Embed Size (px)
Citation preview

RES-000-23-1269
Background Research based on Cox and Klinger’s (e.g., 2004a) model indicates that there are two major cognitive-motivational determinants of drinking: (a) drinkers’ attentional bias for alcohol-related stimuli, which reflects their preoccupation with drinking, and (b) their motivational structure, which prevents them from focusing on and successfully achieving healthy, adaptive goal pursuits as an alternative to drinking alcohol. Attentional-bias training. A prototype of the Alcohol Attention-Control Training Programme (AACTP; Fadardi & Cox, 2004) was previously developed in our laboratory. It was designed to neutralise the cognitive processes involved in the automatic chain of drink-wanting, drink-seeking, and drink-taking behaviours, by helping excessive drinkers gain better control over their distraction by alcohol. Although the AACTP helped drinkers to reduce their alcohol-related distraction, re-directing their attention to alternative goals was not a part of the training. The effects of the AACTP might not endure, especially when the drinker lacks the motivational skills necessary to find emotional satisfaction without alcohol. Thus, the current research evaluated the effectiveness of the AACTP alone and in combination with a motivational intervention aimed at helping drinkers maintain drinking reductions by developing alternative goal pursuits. Motivational counselling. Excessive drinkers’ efforts to reduce their consumption are likely to fail if they lack adaptive motivational strategies for pursuing goals that are incompatible with drinking alcohol (e.g., Correia, 2004). Systematic Motivational Counselling is an individual counselling technique that we previously developed (SMC; Cox & Klinger, 2004b); it uses motivational restructuring components to help alcohol abusers change their maladaptive motivational patterns. Evaluations have shown that SMC reduces alcohol abusers’ alcohol consumption, and that the reduction is mediated by improvements in maladaptive motivation (e.g., Cox et al., 2003). The current research aimed to advance the applicability of the SMC approach by developing and evaluating a brief, cost-effective, SMC-based intervention; we called it Life Enhancement and Advancement Programme (LEAP; see below). Objectives
The objectives of the research were to assess the individual and combined effects of the AACTP and LEAP interventions on reductions in drinking. We also assessed how the reductions in drinking co-varied with a variety of other variables. Method
Participants. Based on the results of a power analysis, a sample size of 247 participants was deemed suitable for this study. Participants were recruited from the following sources: the School of Psychology Community Participant Panel; NHS Community Alcohol Services; newspaper advertisements; posters and fliers that were distributed in GP surgeries and other public places; announcements posted on the Bangor University Intranet; advertisements displayed on local buses; and the School of Psychology Student Participant Panel. After giving their informed consent, participants were randomly assigned to one of four groups: Control Group, AACTP Group, LEAP Group, or Combination Group (AACTP and LEAP). Except for basic demographic information (collected only at baseline) participants in all four groups were administered the full assessment battery at four points: Baseline, Post-Treatment, Three-Month Follow-Up, and Six-Month Follow-Up. The second (“post-treatment”) assessment of the Control Group was timed so that it occurred at the same interval following the first (baseline) assessment as it did for the three intervention groups. The mean number of days that the post-treatment, three-month, and six-
Final Report--13
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
month assessment followed the baseline assessment was 34.92 (SD = 20.63) days, 119.68 (SD = 39.54) days, and 202.64 (SD = 63.17) days, respectively. The mean number of days from the post-treatment assessment to the three-month follow-up was 85.61 (SD = 37.23), and the mean number of days from the three-month follow-up to the six-month follow-up was 81.95 (SD = 45.51). Of the 231 participants included in the final baseline sample, 186 (80.51%), 140 (60.61%), and 120 (52.00%) completed the post-intervention, three-month follow-up, and six-month follow-up assessments, respectively. Of 247 drinkers were tested at baseline, 16 did not meet eligibility criteria and were excluded. The final baseline sample (N = 231; 44.6% males) ranged in age from 18 to 72 years (mean age = 26.95 years, SD = 12.91) years; mean education was 14.97 (SD = 3.32) years. The weekly mean alcohol consumption for males was 55.74 (SD = 53.98) units; for females, it was 28.98 (SD = 35.70) units. Thus, at baseline the males, on average, were drinking at a harmful level, according to the Department of Health’s criterion for harmful drinking among men (50 or more units/week). The females at baseline were, on average, drinking at a hazardous level, according to the Department of Health’s criterion for hazardous drinking among women (between 15 and 35 units/week). On average, participants had drunk 7.89 (SD = 17.48) units of alcohol on their last drinking occasion, which had occurred an average of 3.67 (SD = 7.28) days prior to the baseline assessment. Baseline means and standard deviations of the measures are shown in Table 1 (Appendix II). On mean weekly drinking—the major dependent variable of interest—the four groups were equal at baseline, F(3, 227) = 0.10, p > .05. Assessment
Various indicants of alcohol-specific improvement were assessed, including alcohol consumption (Fadardi, Cox, & Hogan, 2005), alcohol-related problems (Short Inventory of Problems (SIP; Miller et al., 1995), alcohol dependence (Raistrick et al., 1994), situational confidence (Annis & Graham, 1988), and readiness to change (Heather et al., 1993). Additionally, we measured (a) classic, alcohol, and concern-related attentional bias with Stroop tests and (b) motivational structure with the Personal Aspirations and Concerns Inventory (PACI; Cox, Klinger, & Fadardi, 2006). We also measured (a) psychological and social functioning (Self Rating at Intake; SRI, Simpson, 1998), (b) life stressors and social resources (Health and Daily Living Form; HDL, Moos & Moos, 1994), (c) positive affect and negative affect (Positive Affect Negative Affect Schedule; PANAS, Watson, Clark, & Tellegen, 1988), and (d) satisfaction with life (Satisfaction With Life Scale; SWLS; Diener et al., 1985). Finally, we assessed participants’ service utilisation and related characteristics (Client Socio-Demographic and Service Receipt Inventory; CSSRI, Chisholm et al., 2000) as a basis for calculating the cost of care for excessive drinking. For each measure within each domain, widely used measures with established reliability and validity were chosen (see Appendix I). Interventions Alcohol Attention-Control Training Programme (AACTP). The Alcohol Attention-Control Training Programme (AACTP) was designed to help drinkers to become aware of and gain better control over the automatic thoughts related to their drinking. They are guided through a series of systematic, volitional exercises aimed at developing their ability to inhibit their unintentional distraction by alcohol stimuli. The AACTP is based on individualized, hierarchical goal-setting and provides trainees with immediate feedback about their performance.
Final Report--14
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
Two of the categories of stimuli used in the AACTP are individually presented on a computer monitor and comprise single alcoholic or soft-drink bottles, each of which is surrounded by either a coloured background or border in one of four colours—red, yellow, blue, or green. The participant is required to ignore the content of the pictures and name the surrounding colour as quickly and accurately as possible. There is a third, more difficult category of stimuli, in which pairs of bottles appear simultaneously on the screen. To respond to the pairs of bottles, the participant is instructed to name the outline colour of each non-alcoholic bottle as quickly as possible, while ignoring the alcohol-related part of the stimulus. Each session began with the single stimuli with coloured backgrounds (easiest in the series); proceeded with the single stimuli with coloured outlines (intermediate difficulty); and continued with the paired stimuli (most difficult). After completing each session, the participant was given numerical and graphical feedback: (a) number of errors and mean reaction time (RT) to the alcoholic and non-alcoholic stimuli, and (b) interpretation of the results. The goal was to motivate participants to actively take part in the programme in a meaningful and goal-directed way. Prior to each session, the participant was encouraged to set a goal for decreasing his or her errors and RTs to the coloured dimension of the alcoholic bottles relative to the non-alcoholic ones. The goal was for each participant to improve attentional control until his or her own performance plateau had been reached. However, every effort was made to ensure that participants always terminated the training sessions feeling good about their progress. Life Enhancement and Advancement Programme (LEAP). The aim of the Life Enhancement and Advancement Programme (LEAP) was to help excessive drinkers (a) understand how alcohol consumption is related to mood regulation and affect, (b) achieve their goals more effectively, and (c) lead a satisfying life without excessive use of alcohol. The LEAP included four main components: First, participants learned about the rationale for the LEAP, including the reciprocal relationship between the satisfactions and frustrations that people experience from other areas of their life and their need to use alcohol to regulate their positive and negative affect. They were shown how various factors can influence people’s life satisfaction, such as their feelings of control, knowing what to do to achieve goals, and how realistic their goals were. Second, having taken the PACI at baseline, participants were helped to focus on the components of the LEAP that were relevant to their own motivational patterns when pursuing their goals, especially the goal of reducing their alcohol consumption. Third, participants were helped to develop skills they needed for resolving important concerns by teaching them motivational enhancement techniques and exercises. The techniques included (a) re-evaluating their sources of emotional satisfaction, (b) shifting towards an appetitive motivational style and away from an avoidant one, (c) constructing goal ladders to facilitate mastery of small, interim steps that underlay long-range achievements, and (d) developing skills needed to cope with negative affect and enhance positive affect. Participants were also given worksheets detailing the principles underlying successful goal achievements. Fourth, a summary was prepared of the participant’s progress and his or her plan for continuing the application of the motivational principles to his or her prioritized goals during the next three and six months.
Design. In a 2 X 2 design, the study crossed two levels of AACTP (present, absent) with two levels of LEAP (present, absent). The resulting four groups received only AACTP, only LEAP, both AACTP and LEAP, or neither intervention. Participants were randomly assigned to the four groups. Participants in the AACTP
Final Report--15
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
and LEAP groups received a one-hour session once a week for four weeks. Participants in the Combined Group received both a one-hour AACTP session and a one-hour LEAP session once a week for four weeks. Results
Change scores. Change indices were calculated as follows: (a) changes between Time 1 (baseline) and Time 2 (post-treatment) assessments were calculated by subtracting Time 1 values from Time 2 values (resulting values are indicated by the suffix “1�2” after each change index); (b) changes between Time 1 (baseline) and Time 3 (three-month follow-up) assessments were calculated by subtracting Time 1 values from Time 3 values (the resulting values are indicated by the suffix “1�3” after each change index); (c) changes between Time 1 (baseline) and Time 4 (six-month follow-up) assessments were calculated by subtracting Time 1 values from the Time 4 values (the resulting values are indicated by the suffix “1�4” after each change index). For example, Mean Weekly Drinking 1�2 refers to changes in mean weekly alcohol consumption between Time 1 and Time 2. A negative value indicates a reduction in the index across time; a positive value indicates an increase. The change scores are summarized in Table 2 (Appendix III) and are organized according to the major categories of measures shown in Table 1. Analyses of Variance (ANOVAs) First, a series of exploratory, 2 X 2 ANOVAs were run to assess whether the four groups of participants showed differential improvement on the various indices of outcome at each of the three post-interventions assessments. AACTP (presence/absence) and LEAP (presence/absence) were the between-participants factors, and change scores were the dependent variables. Mean weekly drinking. On mean weekly drinking, there was a significant main effect for AACTP on 1�2 [F(1,182) = 4.78, p = .03] and on 1�3 [F(1,135) = 4.89, p = .029], but not on 1�4 [F(1,116) = 2.26, p = .14]. There was a significant main effect for LEAP on 1�2 [F(1,182) = 3.90, p = .05], on 1�3 [F(1,135) = 6.82, p= .01], and on 1�4 [F(1,116) = 7.90, p = .006]. However, there was not a significant interaction between AACTP and LEAP on 1�2 [F (1, 182) = 0.35, p = .56], on 1�3 [F (1, 135) = 0.96, p = .33], nor on 1�4 [F (1, 116) = 1.83, p = .18]. Thus, both interventions were effective in reducing excessive drinkers’ alcohol consumption; the effects of the two interventions were additive rather than multiplicative; and the effects of LEAP were more enduring than the effects of AACTP. The effect sizes shown in Table 1 corroborate these conclusions.
Alcohol-related problems. On the alcohol-problems total score, there was not a significant main effect for AACTP on 1�2 [F(1,181) = 0.34, p = .56], on 1�3 [F(1,136) = 0.75, p = .39], nor on 1�4 [F(1,116) = 0.10, p = .76]. There were also no significant main effects for LEAP on 1�2 [F(1,181) = 2.11, p = .15], on 1�3 [F(1,136) = 0.14, p = .71], nor on 1�4 [F(1,116) = 0.05, p = .83]. However, there was a significant interaction between AACTP and LEAP on 1�2 [F(1,181) = 4.97, p= .027] and on 1�3 [F(1,136) = 7.62, p = .007], and there was a marginally significant interaction on 1�4 [F(1,116) = 3.71, p = .057]. The effect sizes in Table 1 suggest that both AACTP when delivered alone and LEAP when delivered alone (but not AACTP and LEAP delivered in Combination) reduced participants’ alcohol problems. Additionally, there were significant group effects on the alcohol-problems subscales. Specifically, at several of the time points, LEAP was more effective than AACTP in reducing alcohol-related interpersonal problems, but AACTP was more effective in reducing alcohol-related impulse-control problems. The latter results are consistent with the changes that AACTP and LEAP, respectively, were designed to
Final Report--16
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
target. Situational confidence. Situational confidence reflects drinkers’ confidence in
their ability to resist the urge to drink in various high-risk situations. On the total score, there was a significant main effect for AACTP on 1�2 [F(1,180) = 4.20, p = .042], but not on 1�3 [F(1,136) = 0.25, p = .57] or on 1�4 [F(1,116) = 0.003, p = .96]. There was no significant main effect for LEAP on 1�2 [F(1,180) = 1.61, p = .21], 1�3 [F(1,136) = 0.18, p = .67], or on 1�4 [F(1,116) = 1.64, p = .20], and there was no significant interaction between AACTP and LEAP on 1�2 [F(1,180) = 0.004, p = .95], on 1�3 [F(1,136) = 3.59, p = .06], or on 1�4 [F(1,116) = 1.36, p = .25].The main effect of AACTP indicates that it increased participants’ situational confidence only from baseline to post-treatment. However, Table 1 shows medium or strong effect sizes for each of the three interventions at one or more of the assessment points.
Readiness to change. Readiness-to-change scores were used to assign drinkers to one of the three stages of change (precontemplation, contemplation, action), which indicate the degree to which excessive drinkers are motivated to reduce their alcohol consumption. Numbers were assigned to each stage (1 for Precontemplation, 2 for Contemplation, or 3 for Action) to indicate the stage that each participant was in at each assessment, and then change scores were calculated. There was no significant main effect for AACTP on 1�2 [F(1,181) = 0.25, p = .62], on 1�3 [F(1,135) = 3.31, p = .07], or on 1�4 [F(1,116) = 2.19, p = .14]. There was no significant main effect for LEAP on 1�2 F(1,181) = 3.16, p = .08], but there was a significant main effect for LEAP on 1�3 [F(1,135) = 21.32, p < .001] and on 1�4 [F(1,116) = 11.10, p = .001]. However, there was not a significant interaction between AACTP and LEAP on 1�2 [F(1,181) = 0.77, p = .38], on 1�3 [F(1,135) = 0.06, p = .80], or on 1�4 [F(1,116) = 0.005, p = .95]. As Table 2 indicates, unlike AACTP, LEAP when delivered alone significantly increased participants’ motivation to change. Table 2 shows, moreover, that when LEAP was combined with AACTP, it was associated with even stronger effect sizes.
Adaptive motivation. On adaptive motivation there was no significant main effect for AACTP on 1�2 [F(1,180) = 0.87, p = .35], on 1�3 [F(1,134) = 1.47, p = .23], or on 1�4 [F(1,112) = 0.02, p = .89], and there was no significant main effect for LEAP on 1�2 F(1,180) = 2.83, p = .09], on 1�3 [F(1,134) = 0.12, p = .73], or on 1�4 [F(1,112) = 0.06, p = .81]. There was also no significant interaction between AACTP and LEAP on 1�2 [F(1,180) = 2.08, p = .15], on 1�3 [F(1,134) = 0.02, p = .88], or on 1�4 [F(1,112) = 0.00, p = .99]. Thus, the ANOVA results indicate that neither intervention significantly altered participants’ motivational structure. Stroop interference (classic, alcohol-related, and concern-related). The classic Stroop test was used to measure participants’ general cognitive flexibility; the alcohol Stroop test measured their alcohol attentional bias; and the concern-related Stroop measured their concern-related attentional bias. Regarding classic and alcohol-related attentional interference, at no time point was there a significant main effect for AACTP or for LEAP or a significant interaction between AACTP and LEAP. On the concern-related Stroop, there was no significant main effect for AACTP on 1�2 [F(1,181) = 0.28, p = .60] or on 1�4 [F(1,116) = 0.54, p = .46]; however, the main effect approached significance on 1�3 [F(1,136) = 3.48, p = .06]. There was no significant main effect for LEAP on 1�2 F(1,181) = 0.56, p = .46], on 1�3 [F(1,136) = 0.25, p = .62], or on 1�4 [F(1,116) = 0.001, p = .97]; and there was no significant interaction between AACTP and LEAP on 1�2 [F(1,181) = 0.61, p =
Final Report--17
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
.43], on 1�3 [F(1,136) = 0.04, p = .84], or on 1�4 [F(1,116) = 0.14, p = .71]. The main effect for AACTP that approached significance indicated that the AACTP tended to reduce concern-related interference. Affect variables [satisfaction with life, positive affect (PA) and negative affect (NA), self-confidence, and global depression]. On none of the affect variables—satisfaction with life, PA, NA, self-confidence, or global depression—was there a significant main effect for AACTP or for LEAP or a significant interaction between AACTP and LEAP at any of the time points. Alcohol dependence. There was not a significant main effect for AACTP on 1�2 [F(1,181) = 2.13, p = .15], on 1�3 [F(1,136) = 0.05, p = .83], or on 1�4 [F(1,116) = 0.11, p = .74]. However, there was a significant main effect for LEAP on 1�2 F(1,181) = 6.12, p = .014], but not on 1�3 [F(1,136) = 0.55, p = .46] or on 1�4 [F(1,116) = 0.004, p = .95]. There was no significant interaction between AACTP and LEAP on 1�2 [F(1,181) = 0.21, p = .65], on 1�3 [F(1,136) = 1.74, p = .19], or on 1�4 [F(1,116) = 0.71, p = .40]. The main effect for LEAP on 1�2 indicates that it (when delivered alone and in the Combined Intervention) reduced participants’ dependence on alcohol. There were, however, medium or strong effect sizes for all three of the intervention groups (see Table 2). Economic analysis. A number of health-economic variables were assessed at baseline and the two follow-ups. They included employment status (weeks unemployed in the prior three months); absences from work or study; health-related restricted activity; and family, legal, social, and financial difficulties due to drinking. On drinking-related family, legal, social, and financial difficulties, there was no significant main effect for AACTP on 1�3 [F(1,138) = 0.08, p = .79] or on 1�4 [F(1,115) = 0.005, p = .94]; there was no significant main effect for LEAP on 1�3 [F(1,138) = 0.12, p = .73] or on 1�4 [F(1,115) = 0.16, p = .69]. However, there was a significant interaction between AACTP and LEAP on 1�3 [F(1,138) = 3.88, p = .05] but not on 1�4 [F(1,115) = 2.63, p = .11]. The significant interaction seems to indicate that both AACTP and LEAP reduced these difficulties more when delivered alone than in combination. It is not surprising that the reductions in excessive drinking were not immediately accompanied by economic improvements. Such improvement is likely to be a longer-range consequence of reductions in excessive drinking.
Clinically significant improvement in drinking. Another indicator of public-sector costs of excessive drinking is the societal consequences of harmful and hazardous drinking. Thus, we evaluated clinically significant (Roberts et al., 2000) improvements in participants’ alcohol consumption. At each assessment, participants were categorised according to the Department of Health’s criteria for hazardous or harmful drinking, and improvements in their drinking status across time were evaluated. There was no significant main effect for AACTP on 1�2 [F(1,182) = 2.35, p = .13], on 1�3 [F(1,135) = 0.13, p = .72], or on 1�4 [F(1,116) = 0.78, p = .38]. However, there was a significant main effect for LEAP on 1�2 [F(1,182) = 8.57, p = .004], on 1�3 [F(1,135) = 5.31, p = .023], and on 1�4 [F(1,116) = 17.38, p < .001], but there was no significant interaction between AACTP and LEAP on 1�2 [F (1, 182) = 0.28, p = .60], on 1�3 [F (1, 135) = 0.46, p = .50], or on 1�4 [F (1, 116) = 0.36, p = .55]. The main effect for LEAP showed that it improved participants’ drinking status. Clinically significant reductions in harmful and hazardous drinking have economic implications—in both the short-term and the long-term—for public services for excessive drinking and for individual problem drinkers and society as a whole.
Final Report--18
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
Regression Analyses Next, a series of regression analyses were run to assess the relative effects of AACTP and LEAP on changes in mean weekly drinking (MWD) while considering all of the time points simultaneously. Because time was included as a variable in the analyses, only participants who completed all four assessments were included. For this reason, the results might give a different impression than those with the ANOVAs. However, for the initial analyses, we wished to consider the advantages and disadvantages of each analytic strategy before committing ourselves to a particular one. In the regression analyses, we additionally considered, (a) whether individual-difference variables [age, gender, executive control functioning (ECF, as measured by classic Stroop interference)] moderated the impact of AACTP and of LEAP on MWD, and (b) whether reductions in MWD produced by AACTP and LEAP were mediated by reductions in alcohol attentional bias or motivational structure (or by both variables). Our first objective was to determine the relative effects on MWD of AACTP and LEAP alone and in combination (Combined Intervention). The following models were tested in which the predictors were AACTP alone (present, absent), LEAP alone (present, absent), and Combined Intervention (present, absent): MWD = AACTP + LEAP.......................................................(A) versus MWD = AACTP + LEAP + Combined...................................(B) The formula used for testing the difference between R2 based on f predictors and R2 based on r predictors (where the r predictors are a subset of the f predictors) was:
, where is the r2 for the full model. N: total number
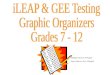
of cases (Howell, 2007 p. 523). The results indicated that Model A was highly significant, F(3,353) = 7.472, p < .0005), and Model B was a significantly better predictor of MWD than Model A, F(1,388) = 22.2, p < .0005. Thus, as Figure 1 shows, both AACTP and LEAP alone reduced MWD, but the Combined Intervention was more effective than either AACTP or LEAP alone.
Final Report--19
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
Figure 1. Mean weekly drinking (MWD) change scores indicating reductions in alcohol consumption across time separately for the four groups of participants. We next examined whether the effects of the three interventions varied across time. The baseline model was: MWD = Time + AACTP + LEAP + Combined....................................................(C) It was compared with these models: MWD = Time + AACTP + LEAP + Combined + Time*AACTP.........................(D) MWD = Time + AACTP + LEAP + Combined + Time*LEAP............................(E) MWD = Time + AACTP + LEAP + Combined + Time*Combined......................(F) Models D, E, and F were highly significant, but none of them was significantly better than Model C (ps > 0.36). However, Model C was significantly better than Model B, F(1,387) = 3.74, p = .05. Thus, we conclude that although there were fluctuations in MWD across time, the improvements resulting from the three interventions were stable across time. Next, we compared Model C with an expanded model that included Age, Gender, and classic Stroop interference change scores. The comparison was between: MWD = Time + AACTP + LEAP + Combined....................................................(C) and MWD = Time + AACTP + LEAP + Combined + Age + Gender + Classic Stroop …………………………………………………………………............................(G)
Final Report--20
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
Model G was a highly significant predictor of MWD, F(7,345) = 7.213, p < .0005; Model G was a highly significant improvement over Model C, F(3,384) = 8.660, p < .0005; and Model G was a highly significant improvement over an alternative baseline model that used feedforward regression and included Time, Age, Gender, and Classic Stroop as the predictor variables, F(3,384) = 7.339, p < .0005. The total variance that Model G accounted for was small (R2 = .13), indicating that much of the variance in MWD was either due to noise or had to be accounted for by other—as yet unspecified—variables. The standardised beta coefficients for the AACTP, LEAP, and Combined interventions were equivalent (-.217, -.243, and -.256, respectively) and larger than the coefficients for the other variables, except for Age (-.247). Thus, of the variables considered, the interventions were the most important determinant of reductions in MWD. Finally, we asked whether (a) reductions in WMD produced by AACTP were mediated by reductions in alcohol attentional bias, and (b) reductions in WMD produced by LEAP were mediated by improvements in motivational structure. The following pairs of models were tested: MWD = alcohol attentional bias....................................................................(H) MWD = alcohol attentional bias + AACTP...................................................(I) and MWD = motivational structure........................................................................(J) MWD = motivational structure + LEAP.........................................................(K) Comparison within the two pairs of models allowed us to test whether (a) AACTP accounted for variance in MWD beyond that accounted for by alcohol attentional bias, and (b) LEAP accounted for variance in MWD beyond that accounted for by motivational structure. Neither Model H, F(1, 355) = 1.063, p = .303, nor Model I, F(2,354) = 0.915, p = .401, was significant; thus, it was not meaningful to compare the two models. Both Model J, F(1,349) = 7.128, p = .008), and Model K, F(2,348) = 6.646, p = .001, were highly significant. However, Model K was not a significantly better predictor of MWD than was Model J, F(1,347) = 1.422, p = .23. Thus, we conclude that reductions in MWD produced by LEAP were due to improvements in motivational structure—a result that supports our theoretical hypothesis.
Activities and Outputs � Sixteen presentations were delivered at international professional conferences. � Two symposia at international professional conferences were organised and
chaired. � Fifteen scientific papers were published in refereed professional journals. � Four book chapters were published. � One book was commissioned. � Software was developed for delivering the AACTP. � A self-help LEAP manual was written. � Software for calculating mean weekly drinking was developed.
Final Report--21
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
Impacts � International networks (with colleagues in the Czech Republic, Germany, Iran,
and the Netherlands) were established for implementing the training and conducting additional research.
� The AACTP generated extensive publicity worldwide. � Numerous excessive drinkers who heard about the research have conducted us
asking for a copy of the computerized AACTP. Future Research Priorities In order to further develop the research programme, an ESRC grant application (“Bilateral Netherlands: An Evaluation of Neurocognitive and Neurofeedback Training for Excessive Drinking)) has been submitted.
Word Count 4,624 Words
Final Report--22
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
References Annis, H. M., & Graham, J. M. (1988). Situational Confidence Questionnaire: User's
Guide. Unpublished manual, Addiction Research Foundation, Toronto, Canada.
Miller, W.R., Tonigan, J.S. & Longabaugh, R. (1995). The Drinker Inventory of Consequences (DrInC): An Instrument for Assessing Adverse Consequences of Alcohol Abuse. Project MATCH Monograph Series, Vol. 4. DHHS Publication No. 95-3911. Rockville, MD: National Institute on Alcohol Abuse and Alcoholism.
Chisholm, D., Knapp, M. R. J., Knudsen, H. C., Amaddeo, F., Gaite, L., & Van Wijngaarden, B. (2000). Client Socio-demographic and Service Receipt Inventory - European Version : development of an instrument for international research. British Journal of Psychiatry, 177, 28-33.
Cox, W. M., Heinemann, A. W., Miranti, S. V., Schmidt, M., Klinger, E., & Blount, J. P. (2003). Outcomes of Systematic Motivational Counseling for substance use following traumatic brain injury. Journal of Addictive Diseases, 22(1), 93-110.
Correia, C. J. (2004). Behavioral economics: Basic concepts and clinical applications. In W. M. Cox & E. Klinger (Eds.), Handbook of motivational counseling: Concepts, approaches, and assessment (pp. 49-64). Chichester, United Kingdom: Wiley.
Cox, W. M., Klinger, E. (2004a). A motivational model of alcohol use: Determinants of use and change. In W. M. Cox & E. Klinger (Eds.), Handbook of motivational counseling: Concepts, approaches, and assessment (pp. 121-138). Chichester, United Kingdom: Wiley.
Cox, W. M., Klinger, E. (2004b). Systematic Motivational Counseling: The Motivational Structure Questionnaire in action. W. M. Cox & E. Klinger (Eds.), Handbook of motivational counseling: Concepts, approaches, and assessment (pp. 217-237). Chichester, United Kingdom: Wiley.
Cox, W. M., Klinger, E. & Fadardi, J. S., (2006). Personal Aspirations and Concerns Inventory. Unpublished questionnaire, Bangor University.
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). Satisfaction With Life Scale. Journal of Personality Assessment, 49, 71-75.
Fadardi, J. S., & Cox, W. M. (2004). Alcohol Attention Control Training Programme (AACTP). Bangor University: Unpublished software.
Fadardi, J. S., Cox, W. M., & Hogan, L. M. (2006). Drinking Record Questionnaire. Unpublished questionnaire, Bangor University.
Heather, N., Rollnick, S., & Bell, A. (1993). Predictive validity of the Readiness to Change Questionnaire. Addiction, 88, 1667-1677.
Howell, D. C. (2007). Fundamental statistics for the behavioral sciences. Belmont, CA: Wadsworth.
Moos, R. H., Cronkite, R. C., Billings, A. G., & Finney, J. W. (1988). Health and Daily Living Form Manual. Palo Alto: Stanford University and VA Medical Centers.
Raistrick, D., Bradshaw, J., Tober, G., et al. (1994). Development of the Leeds Dependence Questionnaire (LDQ): A questionnaire to measure alcohol and opiate dependence in the context of a treatment evaluation package. Addiction, 89, 563-572.
Final Report--23
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
Roberts, L. J., Neal, D. J,, Kivlahan, D. R,, Baer, J. S,, & Marlatt, G. A. (2000). Individual drinking changes following a brief intervention among college students: Clinical significance in an indicated preventive context. Journal of Consulting & Clinical Psychology, 68, 500-505.
Simpson, D. (1998). Self-Rating at Intake. Unpublished questionnaire, Texas Christian University.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063-1070.
Final Report--24
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
Appendix I Measures Administered
Drinking Record Questionnaire (DRQ, Fadardi, Cox, & Hogan, 2006).
The DRQ measures the frequency of participants’ typical (usual) and atypical (e.g., binge) drinking weeks. For each type of week, participants indicate the type of beverage(s) that they drank, the percentage of alcohol by volume (ABV%) of each beverage, and the quantity of each beverage drunk. Quantity X Frequency indices of each kind of weekly drinking are then calculated. The primary index is mean weekly drinking (MWD).
Short Inventory of Problems (SIP; Miller et al., 1995). The SIP measures problems associated with the excessive consumption of alcohol. The SCQ yields a total score and scores on five subscales.
Leeds Dependence Questionnaire (LDQ, Raistrick et al., 1994). The LDQ has 10 questions that measure the severity of alcohol dependence.
Situational confidence. The Situational Confidence Questionnaire (SCQ; Annis & Graham, 1988) is based on the concept of self-efficacy in drink-related situations. Participants are asked to imagine themselves in various situations, and for each to indicate how confident they are that they will be able to resist the urge to drink in that situation. The SCQ yields a total score and scores on eight subscales.
Readiness to Change Questionnaire (RTCQ, Heather et al., 1993). The RTCQ was used to measure participants’ stated intentions to change their drinking during the next three months. RTC scores are used to assign drinkers to one of three stages of change: precontemplation, contemplation, or action.
Classic, alcohol, and concern-related Stroop tests. The classic Stroop test was administered to participants as a measure of their general cognitive flexibility. Their attentional bias for alcohol and concern-related stimuli was measured with the alcohol and concern-related Stroop tests. The concern-related words (e.g., health, friends, money, work) represented the life areas in which participants most often have concerns. Concern-related interference scores were used to determine whether improvements due to the AACTP were alcohol-specific or were generalised to other personally relevant concerns.
To avoid potential practice effects, two parallel versions of the Stroop test were created, and the order in which they were administered at each assessment point was counterbalanced. The basic specifications were as follows: The classic Stroop test consisted of colour words that were either congruent (red in red) or incongruent (red in blue) with the font in which they appeared. The alcohol- and concern-related and emotionally neutral words were selected in a similar manner to prior studies. The three categories of words were selected so as to control for relevant dimensions, such as word frequency and length and semantic relatedness.
The colour-naming trials were presented via a computer. Especially for this project, we developed a programme in a shockwave environment that enabled us to administer the Stroop tests. The stimuli were presented on a 20” colour monitor. A standard keyboard was used on which four of the keys were tagged with colour patches corresponding to the four correct responses; this was used as the input device. Each word was presented in a mixed-randomised order, one at a time in red, yellow, blue, or green. The participant was instructed to name as quickly as possible the colour of each word while ignoring the word’s meaning. Colour-naming latencies were automatically recorded. Prior to the experimental trials, the participant was given practice trials to control for “warm-up” effects. Alcohol-interference and
Final Report--25
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
Final Report--26
concern-interference scores were calculated, respectively, by subtracting each participant’s mean reaction time to the neutral stimuli from his or her mean reaction time to the alcohol-related or concern-related words. Classic Stroop interference was calculated by subtracting mean reaction time to the congruent stimuli from that to the incongruent stimuli.
Motivational structure. Motivational structure was measured with the Personal Aspirations and Concerns Inventory (PACI; Cox, Klinger, & Fadardi, 2005). The PACI was developed and computerised especially for use in this project. It was designed as an improvement over its predecessor, the Personal Concerns Inventory (PCI). Specifically, the PACI focuses both on participants’ concerns and their aspirations rather than only on their concerns, as does the PCI. On the PACI, respondents describe their aspirations and concerns in various life areas and name the resolution that they wish to find for each concern. Rating scales allow motivational indices to be derived.
Although various indices can be derived from the PACI to depict respondents’ motivational structure, a Value X Expectancy approach was deemed most appropriate for the current study. According to Value*Expectancy formulations (e.g., Klinger & Cox, 2004; Van Eerde & Thierry, 1996), a person’s motivation, or commitment, to pursue a goal is determined by two factors: the value that the person attributes to goal attainment and the person’s expectancy (subjective probability) of being able to attain it. In the simplest form of Value*Expectancy theory, goal commitment should be determined by the product of value times expectancy. Accordingly, a person’s motivation can be characterized as adaptive to the extent that the person’s reported commitment to pursuing different goals corresponds to the Value*Expectancy product for each goal. Based on the results of a Principal Component Analysis, a PACI value index was calculated for each goal of each participant as Value = [MEAN (Happiness, Sadness, Enjoyment, Approach)], and a PACI expectancy index was calculated as Expectancy = [MEAN (Control, Know What To Do, Expected Chances of Success)]; then, the Value index was multiplied by the Expectancy index to obtain a Value*Expectancy index for each goal. Each participant’s Commitment ratings were correlated with his or her Value*Expectancy indices, and the resulting motivational coefficient (called “adaptive motivation”) was used as the index of motivation for each participant.
Self-Rating at Intake (SRI, Simpson, 1998). The SRI (with nine subscales) measures psychological functioning, social functioning, and motivation for treatment.
Health and Daily Living (HDL) Form (Moos & Moos, 1994). The HDL measures life stressors and social resources.
Positive affect and negative affect. Affect was measured with the Positive Affect Negative Affect scale (PANAS; Watson, Clark, & Tellegen, 1988), which yields separate PA and NA scores.
Satisfaction with Life Scale (SWLS, Diener, Emmons, Larsen, & Griffin, 1985). The SWLS is a 5-item instrument designed to measure the person’s global self-appraisal of his or her life.
Client Socio-Demographic and Service Receipt Inventory (CSSRI, Chisholm et al., 2000). The CSSRI identifies service utilisation and related characteristics of people, as a basis of calculating costs of care.
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
App
endi
x II
B
asel
ine
Mea
sure
s Ta
ble
1. M
eans
and
stan
dard
dev
iatio
ns o
f all
mea
sure
s at b
asel
ine
for t
he e
ntir
e sa
mpl
e an
d th
e fo
ur g
roup
s. M
easu
re
Entir
e Sa
mpl
e (N
=231
) C
ontro
l (N
=55)
A
AC
TP (N
=56)
LE
AP
(N=6
1)
AA
CTP
+ L
EAP
(N=5
9)
Alco
hol M
easu
res
Am
ount
: Typ
ical
Wee
k
Am
ount
: Aty
pica
l Wee
k
Wee
ks A
bstin
ent
Yea
rs H
eavy
Drin
king
M
ean
Wee
kly
Drin
king
7.
24 (3
.02)
2.
26 (1
.59)
2.
89 (3
.16)
3.
19 (6
.42)
40
.57
(46.
38)
7.
40 (3
.29)
1.76
(1.3
5)a,
b
3.20
(3.2
6)
2.74
(5.6
2)
38.7
7 (4
5.09
)
6.71
(2.9
3)
2.43
(1.7
3)a
2.43
(1.7
3)
4.54
(7.6
9)
39.6
9 (4
6.93
)
7.
75 (3
.12)
2
.08
(1.2
8)c
2.08
(1.2
8)
2.67
(6.1
6)
40.4
6 (4
4.29
)
7.
07 (2
.69)
2.76
(1.8
2)b,
c
2.76
(1.8
2)
2.75
(5.9
2)
43.1
8 (5
0.08
)
Shor
t Inv
ento
ry o
f Pro
blem
sPh
ysic
al
Inte
rper
sona
l In
trape
rson
al
Impu
lse
Con
trol
Soci
al R
espo
nsib
ility
To
tal S
core
2.
17 (2
.03)
1.
03 (1
.99)
2.
03 (2
.20)
2.
06 (1
.86)
2.
46 (2
.32)
9.
68 (8
.27)
2.
09 (2
.23)
0.
78 (1
.85)
1.
78 (2
.06)
2.
15 (2
.01)
2.
38 (2
.46)
9.
11 (8
.85)
2.
07 (2
.13)
0.
89 (1
.55)
2.
09 (2
.31)
2.
07 (1
.75)
2.
32 (2
.10)
9.
39 (8
.05)
2.
31 (1
.85)
1.
30 (2
.20)
2.
40 (2
.24)
1.
84 (1
.66)
2.
87 (2
.41)
10
.67
(8.1
7)
2.
17 (1
.94)
1.
14 (2
.27)
1.
82 (2
.18)
2.
19 (2
.04)
2.
22 (2
.30)
9.
45 (8
.12)
Si
tuat
iona
l Con
fiden
cePl
easa
nt E
mot
ions
U
nple
asan
t Em
otio
ns
Urg
es &
Tem
ptat
ions
Po
sitiv
e So
cial
Situ
atio
ns
Soci
al T
ensi
on
Soci
al P
robl
ems a
t Wor
k Te
stin
g Pe
rson
al C
ontro
l Ph
ysic
al D
isco
mfo
rt SC
Q T
otal
Sco
re
4.
80 (1
.16)
4.
09 (1
.39)
3.
86 (1
.51)
2.
84 (1
.41)
4.
09 (1
.40)
4.
51 (1
.43)
4.
04 (1
.50)
5.
03 (1
.14)
4.
16 (1
.05)
4.
93 (1
.01)
4.
25 (1
.47)
4.
05 (1
.45)
3.
00 (1
.47)
4
.44
(1.3
8)a
4.65
(1.4
3)
4.06
(1.5
8)
5.15
(1.1
1)
4.32
(1.0
6)
4.
52 (1
.26)
3.
88 (1
.41)
3.
79 (1
.45)
2.
79 (1
.32)
3.58
(1.4
1)a,
b
4.13
(1.5
4)
3.77
(1.5
5)
4.73
(1.2
3)
4.00
(1.0
5)
4.
82 (1
.04)
4.
03 (1
.36)
3.
93 (1
.41)
2.
73 (1
.39)
4.
05 (1
.37)
4.
55 (1
.32)
4.
05 (1
.32)
4.
98 (1
.10)
4.
14 (0
.98)
4.
92 (1
.28)
4.
22 (1
.34)
3.
66 (1
.72)
2.
83 (1
.48)
4
.31
(1.3
4)b
4.69
(1.3
9)
4.28
(1.5
3)
5.26
(1.0
8)
4.26
(1.0
8)
Read
ines
s To
Cha
nge
-0
.08
(9.6
5)
-1.3
8 (8
.73)
0.
80 (9
.27)
1.
39 (9
.39)
-1
.21
(10.
94)
Fina
l Rep
ort--
27
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
Stro
opC
lass
ic In
terf
eren
ce
Alc
ohol
Inte
rfer
ence
C
once
rn In
terf
eren
ce
Stro
op T
otal
Err
ors
10
5.25
(93.
73)
16.
76 (7
4.46
) 2
1.50
(92.
49)
6.1
2 (6
.39)
97
.36
(98.
23)
14.9
6 (5
1.97
) 22
.43
(84.
35)
4.65
(4.3
2)
12
5.78
(95.
76)
15.
67 (8
4.18
)
33.1
8 (1
03.1
4)
5.4
8 (6
.14)
90
.83
(71.
96)
17.3
8 (7
6.24
) 11
.97
(82.
39)
5.90
(6.3
2)
10
7.82
(105
.33)
18
.83
(82.
05)
19.3
9 (9
9.80
) 8.
32 (7
.73)
Ad
aptiv
e M
otiv
atio
n 0
.55
(0.3
4)
0.65
(0.2
6)
0.5
1 (0
.31)
0.
48 (0
.41)
0.
55 (0
.34)
Se
lf-Ra
ting
at In
take
A
ggre
ssiv
e A
mbi
tious
A
sser
tive
Cal
m
Con
fiden
t D
omin
ativ
e Ea
sygo
ing
Ener
getic
H
appy
O
utgo
ing
Succ
essf
ul
0.
83 (0
.91)
2.
67 (1
.01)
2.
29 (1
.01)
2.
46 (1
.08)
2.
37 (1
.12)
1.
61 (1
.19)
2.
94 (1
.00)
2.
41 (1
.04)
2.
68 (1
.00)
2.
61 (1
.11)
2.
19 (0
.94)
0.
60 (0
.76)
2.
87 (0
.88)
2.
18 (0
.95)
2.
40 (1
.20)
2.
29 (1
.12)
1.
69 (1
.14)
2.
85 (1
.03)
2.
42 (1
.05)
2.
69 (0
.88)
2.
49 (1
.03)
2.
22 (0
.92)
0.
89 (0
.99)
2.
66 (1
.12)
2.
20 (1
.00)
2.
43 (1
.02)
2.
34 (1
.21)
1.
54 (1
.26)
2.
95 (0
.86)
2.
45 (1
.11)
2.
55 (1
.16)
2.
68 (1
.18)
2.
25 (0
.98)
0.
89 (0
.95)
2.
41 (0
.97)
2.
26 (0
.91)
2.
39 (1
.05)
2.
57 (0
.99)
1.
56 (1
.13)
2.
98 (1
.07)
2.
41 (1
.01)
2.
75 (1
.06)
2.
57 (1
.09)
2.
18 (0
.94)
0.
93 (0
.89)
2.
76 (1
.02)
2.
49 (1
.17)
2.
61 (1
.07)
2.
27 (1
.14)
1.
68 (1
.24)
2.
95 (1
.04)
2.
37 (1
.02)
2.
69 (0
.90)
2.
69 (1
.15)
2.
10 (0
.96)
H
ealth
& D
aily
Liv
ing
Se
lf-C
onfid
ence
G
loba
l Dep
ress
ion
13.7
4 (4
.15)
2
7.98
(12.
22)
13
.75
(3.8
3)
24.
98 (1
1.83
)
13
.66
(4.6
8)
30.
66 (1
1.45
)
13
.56
(3.7
5)
27.
57 (1
2.66
)
14
.00
(4.3
9)
28.
66 (1
2.47
)
PAN
AS P
ositi
ve A
ffect
33.3
7 (7
.46)
33
.76
(7.1
8)
33.0
5 (8
.34)
33
.35
(7.1
4)
33.3
1 (7
.35)
PA
NAS
Neg
ativ
e Af
fect
24.0
6 (8
.23)
23
.43
(7.4
0)
24.5
7 (9
.04)
23
.07
(7.4
2)
25.1
7 (8
.95)
Sa
tisfa
ctio
n W
ith L
ife
21
.13
(7.1
7)
22.0
6 (6
.61)
20
,41
(7,8
8)
21.2
5 (6
.78)
20
.85
(7.4
4)
Leed
s Dep
ende
ncy
Que
stio
nnai
re
13
.00
(8.2
1)
13.2
4 (8
.72)
12
.91
(8.0
8)
12.9
5 (7
.68)
12
.93
(8.6
0)
Not
e.W
eekl
y M
ean
Drin
king
was
mea
sure
d in
uni
ts o
f alc
ohol
. SIP
= S
hort
Inve
ntor
y of
Pro
blem
s. LD
Q =
Lee
ds D
epen
denc
y Q
uest
ionn
aire
. SC
Q =
Situ
atio
nal C
onfid
ence
Que
stio
nnai
re. R
TCQ
= R
eadi
ness
to C
hang
e Q
uest
ionn
aire
. HD
L =
Hea
lth &
Dai
ly L
ivin
g Fo
rm. P
AN
AS
= Po
sitiv
e A
ffec
t & N
egat
ive
Aff
ect S
ched
ule.
SW
L =
Satis
fact
ion
with
Life
scal
e. S
uper
scrip
t let
ters
den
ote
sign
ifica
nt d
iffer
ence
s bet
wee
n gr
oups
(p<.
05).
Fina
l Rep
ort--
28
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
App
endi
x II
I C
hang
e Sc
ores
and
Eff
ect S
izes
Ta
ble
2: M
ean
(SD
) cha
nges
in th
e m
ajor
var
iabl
es a
cros
s tim
e an
d co
rres
pond
ing
effe
ct si
zes (
Coh
en’s
d).
V
aria
ble
Con
trol
AA
CTP
LE
AP
Com
bine
d M
ean
Wee
kly
Dri
nkin
g 1�
2 1�
3 1�
4
-1.4
2 (1
1.63
), d
= .1
2 1
.01
(12.
17),
d =
.08
-2.0
6 (1
0.21
), d
= .2
0
-1
0.46
(31.
42),
d =
.33
-14.
19 (2
4,61
), d
= .5
8 -1
2.87
(21,
84),
d =
.59
-
9.77
(20.
58),
d =
.47
-16.
10 (2
7.04
), d
= .6
0 -1
7.81
(24.
44),
d =
.73
-1
4.96
(19.
71),
d =
.76
-21.
98 (4
1.35
), d
= .5
3 -1
8.38
(20.
24),
d =
.91
Shor
t Inv
ento
ry o
f Pr
oble
ms
1�2
1�3
1�4
0
.76
(5.5
5), d
= .1
4 -1
.48
(5.0
6), d
= .2
9 -1
.27
(5.5
2), d
= .2
3
-1
.17
(3.7
2), d
= .3
1 -3
.35
(5.3
1), d
= .6
3 -3
.05
(5.6
2), d
= .5
4
-1
.76
(4.5
2), d
= .3
9 -4
.57
(7.4
2), d
= .6
2 -3
.63
(7.1
1), d
= .5
1
-0
.63
(4.6
6), d
= .1
4 -1
.00
(4.5
0), d
= .2
2 -1
.17
(5.1
6), d
= .2
3 Si
tuat
iona
l Con
fiden
ce1�
2 1�
3 1�
4
0.
04 (0
.63)
, d =
.06
0.22
(0.8
3), d
= .2
7 0.
15 (0
.88)
, d =
.17
0.
32 (0
.87)
, d =
.37
0.58
(0.9
0), d
= .6
4 0.
36 (1
.02)
, d =
.35
0.
22 (0
.95)
, d =
.23
0.43
(0.8
7), d
= .4
9 0.
58 (0
.99)
, d =
.59
0.
48 (1
.04)
, d =
.46
0.24
(0.8
4), d
= .2
9 0.
38 (0
.78)
, d =
.49
Read
ines
s To
Cha
nge
1�
2 1�
3 1�
4
0.
09 (0
.81)
, d =
.11
-0
.16
(0.9
3), d
= .1
7
-0.1
2 (0
.99)
, d =
.12
0.
27 (0
.89)
, d =
.30
0.07
(0.8
1), d
= .0
9 0.
15 (0
.83)
, d =
.18
0.
44 (0
.93)
, d =
.47
0.49
(0.8
7), d
= .5
6 0.
47 (1
.01)
, d =
.47
0.
39 (0
.97)
, d =
.40
0.79
(0.8
6), d
= .9
2 0.
71 (0
.86)
, d =
.83
Adap
tive
Mot
ivat
ion
1�2
1�3
1�4
-0.0
6 (0
.30)
, d =
.20
-0
.06
(0.3
7). d
= .1
6
-0.0
1 (0
.33)
, d =
.03
-0.0
3 (0
.43)
, d =
.07
0
.04
(0.4
2), d
= .0
0
-0.0
0 (0
.41)
, d =
.00
0.1
4 (0
.53)
, d =
.26
-0
.08
(0.5
8), d
= .1
4
-0.0
3 (0
.39)
, d =
.08
-0.0
1 (0
.40)
, d =
.03
0.01
(0.4
0), d
= .0
3
-0.0
2 (0
.34)
, d =
.06
Stro
opC
lass
ic In
terf
eren
ce
1�2
1�3
1�4
-1
3.61
(88.
35),
d =
.15
-24.
55 (8
1.62
), d
= .3
0 -2
6.23
(69.
04),
d =
.40
-2
4.69
(121
.94)
, d =
.20
-49.
23 (1
43.4
7), d
= .3
4
-25.
35 (1
24.2
8), d
= .2
0
-3
.56
(115
.97)
, d =
.03
6.1
3 (9
5.92
), d
= .0
6 -1
2.66
(76.
81),
d =
.16
-0
.20
(117
.74)
, d =
.002
-3
1.77
(107
.49)
, d =
.30
-33.
93 (1
23.1
1), d
= .2
8
Fina
l Rep
ort--
29
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC

RES-000-23-1269
Alco
hol I
nter
fere
nce
1�2
1�3
1�4
Con
cern
Inte
rfer
ence
1�
2 1�
3 1�
4
-6
.90
(91.
55),
d =
.07
14.0
3 (6
2.85
), d
= .2
2 9
.82
(74.
48),
d =
.13
-2
7.44
(76.
54),
d =
.36
-4.
89 (8
6.92
), d
= .0
6 -1
5.32
992
.57)
, d =
.17
-1
7.36
(93.
82),
d =
.19
-24.
33 (9
7.79
), d
= .2
5 -
12.7
7 (1
07.3
0), d
= .1
2
-23.
65 (1
04.6
4), d
= .2
3 -4
5.00
(124
.64)
, d =
.36
-35.
97 (1
09.4
6), d
= .3
3
-2
2.81
(111
.69)
, d =
.20
-9.
27 (1
18.3
9), d
= .0
8 -4
6.02
(114
.10)
, d =
.40
-5
.07
(96.
81),
d =
.05
0.75
(125
.79)
, d =
.006
-2
2.94
(86.
71),
d =
.26
-1.3
6 (1
06.4
3), d
= .0
1 -1
2.52
(95.
37),
d =
.13
-7.
40 (8
7.92
), d
= .0
8
-24.
15 (1
15.8
7), d
= .2
1 -3
1.29
(101
.70)
, d =
.31
-29.
70 (1
06.8
3), d
= .2
8Le
eds D
epen
denc
e Q
uest
ionn
aire
1�2
1�3
1�4
-
0.02
(4.6
6), d
= .0
04
-1.5
4 (6
.55)
, d =
.24
-1.7
3 (7
.57)
, d =
.23
-1
.50
(5.4
3), d
= .2
8 -3
.05
(4.9
5), d
= .6
2 -3
.25
(7.1
1), d
= .4
6
-2
.28
(4.8
7), d
= .4
7 -3
.57
(6.8
0), d
= .5
3 -2
.90
(7.2
0), d
= .4
0
-3
.05
(5.9
2), d
= .5
2 -2
.48
(4.1
3), d
= .6
0 -2
.25
(5.3
8), d
= .4
2 Po
sitiv
e Af
fect
1�
2 1�
3 1�
4 N
egat
ive
Affe
ct
1�2
1�3
1�4
0.
13 (6
.49)
, d =
.02
2.10
(6.6
5), d
= .2
4 1.
76 (5
.66)
, d =
.31
-1
.16
(6.3
9), d
= .1
8 -2
.16
(7.3
7), d
= .2
9 -2
.65
(5.0
6), d
= .5
2
0.
21 (6
.65)
, d =
.03
-0.5
7 (6
.65)
, d =
.09
0.31
(6.4
4), d
= .0
5
-0.0
4 (4
.44)
, d =
.01
-2.2
6 (5
.88)
, d =
.38
-2.3
3 (6
.75)
, d =
.35
1.
56 (4
.93)
, d =
.32
1.22
(6.8
5), d
= .1
8 1.
60 (7
.16)
, d =
.22
-0.6
1 (5
.89)
, d =
.10
-0
.74
(8.2
9), d
= .0
9
-2.2
5 (6
.05)
, d =
.37
1.
00 (5
.51)
, d =
.18
2.11
(6.1
4), d
= .3
4 1.
35 (7
.91)
, d =
.17
-0.2
9 (6
.33)
, d =
.05
-1
.83
(7.6
3), d
= .2
4
-0.9
6 (8
.39)
, d =
.11
Satis
fact
ion
with
Life
1�
2 1�
3 1�
4
0.
27 (4
.23)
, d =
.06
2.87
(5.3
3), d
= .5
4 1.
38 (5
.97)
, d =
.23
0.
67 (3
.85)
, d =
.17
0.84
(3.3
4), d
= .2
5 1.
03 (4
.35)
, d =
.24
1.
20 (4
.20)
, d =
.29
2.24
(4.0
4), d
= .5
5 2.
93 (4
.83)
, d =
.61
1.
85 (5
.11)
, d =
.36
2.34
(6.0
5), d
= .3
9 2.
28 (6
.93)
, d =
.33
Dri
nkin
g D
iffic
ultie
s 1�
3 1�
4
-0
.16
(0.9
2), d
= .1
7
-0.1
5 (1
.19)
, d =
.13
-0
.49
(1.1
2), d
= .4
4 -0
.53
(1.0
6), d
= .5
0
-0
.47
(1.2
9), d
= .3
6 -0
.45
(1.2
7), d
= .3
5
-0
.03
(1.2
4), d
= .0
2 -0
.04
(1.6
8), d
= .0
2
Not
e. C
ohen
’s d
; sm
all e
ffec
t siz
e =
0.2-
0.3;
med
ium
eff
ect s
ize
= ap
prox
imat
ely
0.5;
larg
e ef
fect
size
= 0
.8 a
nd h
ighe
r.
Fina
l Rep
ort--
30
To cite this output: Cox, W. et al (2009). Effects of Attentional and Motivational Training on Reducing Excessive Drinking: Full Research Report ESRC End of Award Report, RES-000-23-1269. Swindon: ESRC