Embed Size (px)
Citation preview
Volume 01 / Issue 02 / September 2013 boa.ac.uk Page 50
Peer-Reviewed Articles
Motion-preserving salvage surgery of the wrist after a scaphoid non-union or scapholunate dissociation
Joseph J Dias
This article looks at salvage surgery of the wrist after a scaphoid fracture non-union or a scapholunate dissociation cause arthritic change in the radioscaphoid joint. All motion-preserving alternatives are discussed. Of the common ones of scaphoid excision and a four-corner fusion or a proximal row carpectomy, in the medium term a proximal row carpectomy retains more physiological movement and therefore better function but long-term results are less certain. In such cases the orthopaedic surgeon must discuss alternatives and tailor a specific solution to the patient.
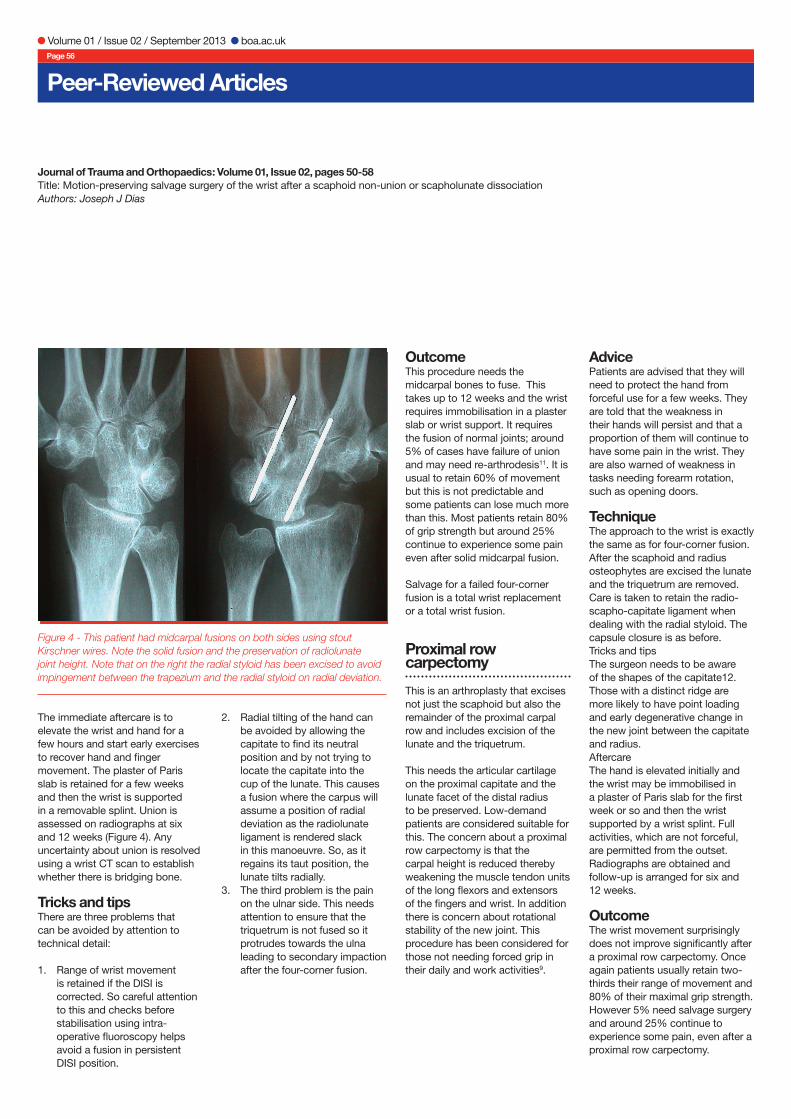
It rapidly extends to involve the articulation between the radial segment of the proximal carpal row and the scaphoid fossa of the distal radius. The next joint to get involved is that between the capitate and the proximal scaphoid with the degeneration slowly progressing (Figure 2). The radiolunate joint and that between the proximal scaphoid and the radius is preserved until very late4.
The symptoms from the degenerative arthritis do not usually reflect the radiological findings. Patients can present with episodic sharp catching or painful giving way, especially on gripping forcefully. Persistent aching is uncommon and, although patients have restricted movement, what is left permits most daily activities. Patients cannot push up taking weight on their palm. Once the symptoms have become intrusive and cannot be managed using non-surgical methods (rest, splints, analgesics NSAIDs or injections), the surgeon needs to consider possible intervention.
Surgical Options
The options the surgeon may consider include advice, debridement of osteophytes, denervation, and partial excision arthroplasty. Excision arthroplasty commonly involves excision of the scaphoid and midcarpal fusion or a proximal row carpectomy. It is very uncommon, in my experience, to need total wrist arthroplasty5 or a full wrist fusion6.
Joseph J Dias
Injury to the wrist is common and usually affects young men. The two injuries that can result in early secondary osteoarthritis are a scaphoid fracture1 that does not heal and a scapholunate dissociation2, which causes instability.
Once degenerative change has set in salvage procedures may be needed if symptoms intrude on the patients’ ability to perform activities of daily living or activities at work.
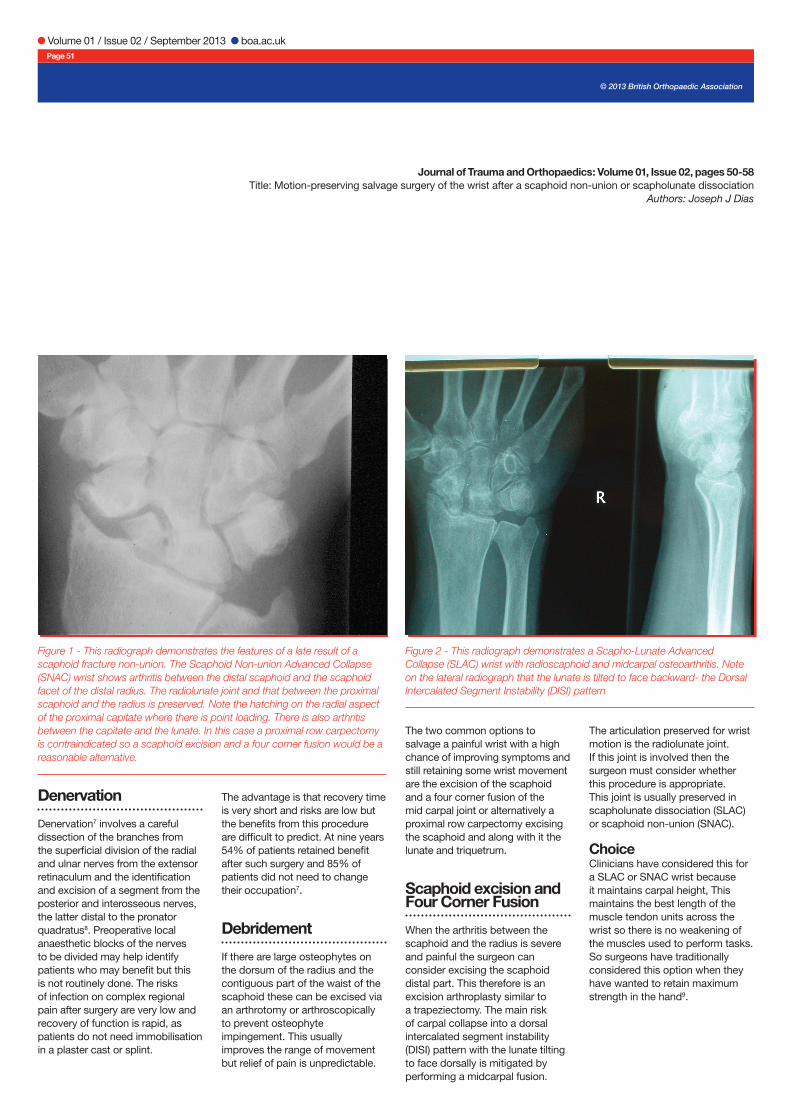
Both injuries disrupt the continuity of the proximal carpal row. This row is then broken into two unequal parts, the smaller radial segment made up of a part or whole of the scaphoid and the longer ulnar segment of the lunate and triquetrum with or without the proximal part of the scaphoid. The extent of degeneration reflects the size of the radial segment of the proximal carpal row, which flexes after the non-union or dissociation. There is point loading between the radial segment of the proximal carpal row and the dorsal rim of the scaphoid facet of the distal radius. This, in a very quick time, leads to loss of joint cartilage. After a scaphoid non-union (Figure 1) there is a loss of wrist cartilage which is noted on wrist radiographs within five years in most patients3. The arthritis initially occurs between the radial segment of the proximal carpal row and the styloid and dorsal rim of the distal radius.
Volume 01 / Issue 02 / September 2013 boa.ac.uk Page 51
Denervation
Denervation7 involves a careful dissection of the branches from the superficial division of the radial and ulnar nerves from the extensor retinaculum and the identification and excision of a segment from the posterior and interosseous nerves, the latter distal to the pronator quadratus8. Preoperative local anaesthetic blocks of the nerves to be divided may help identify patients who may benefit but this is not routinely done. The risks of infection on complex regional pain after surgery are very low and recovery of function is rapid, as patients do not need immobilisation in a plaster cast or splint.
The advantage is that recovery time is very short and risks are low but the benefits from this procedure are difficult to predict. At nine years 54% of patients retained benefit after such surgery and 85% of patients did not need to change their occupation7.
Debridement
If there are large osteophytes on the dorsum of the radius and the contiguous part of the waist of the scaphoid these can be excised via an arthrotomy or arthroscopically to prevent osteophyte impingement. This usually improves the range of movement but relief of pain is unpredictable.
The two common options to salvage a painful wrist with a high chance of improving symptoms and still retaining some wrist movement are the excision of the scaphoid and a four corner fusion of the mid carpal joint or alternatively a proximal row carpectomy excising the scaphoid and along with it the lunate and triquetrum.
Scaphoid excision and Four Corner Fusion
When the arthritis between the scaphoid and the radius is severe and painful the surgeon can consider excising the scaphoid distal part. This therefore is an excision arthroplasty similar to a trapeziectomy. The main risk of carpal collapse into a dorsal intercalated segment instability (DISI) pattern with the lunate tilting to face dorsally is mitigated by performing a midcarpal fusion.
The articulation preserved for wrist motion is the radiolunate joint. If this joint is involved then the surgeon must consider whether this procedure is appropriate. This joint is usually preserved in scapholunate dissociation (SLAC) or scaphoid non-union (SNAC).
ChoiceClinicians have considered this for a SLAC or SNAC wrist because it maintains carpal height, This maintains the best length of the muscle tendon units across the wrist so there is no weakening of the muscles used to perform tasks. So surgeons have traditionally considered this option when they have wanted to retain maximum strength in the hand9.
Journal of Trauma and Orthopaedics: Volume 01, Issue 02, pages 50-58Title: Motion-preserving salvage surgery of the wrist after a scaphoid non-union or scapholunate dissociation
Authors: Joseph J Dias
Figure 2 - This radiograph demonstrates a Scapho-Lunate Advanced Collapse (SLAC) wrist with radioscaphoid and midcarpal osteoarthritis. Note on the lateral radiograph that the lunate is tilted to face backward- the Dorsal Intercalated Segment Instability (DISI) pattern
Figure 1 - This radiograph demonstrates the features of a late result of a scaphoid fracture non-union. The Scaphoid Non-union Advanced Collapse (SNAC) wrist shows arthritis between the distal scaphoid and the scaphoid facet of the distal radius. The radiolunate joint and that between the proximal scaphoid and the radius is preserved. Note the hatching on the radial aspect of the proximal capitate where there is point loading. There is also arthritis between the capitate and the lunate. In this case a proximal row carpectomy is contraindicated so a scaphoid excision and a four corner fusion would be a reasonable alternative.
© 2013 British Orthopaedic Association

Volume 01 / Issue 02 / September 2013 boa.ac.uk Page 52
Peer-Reviewed Articles
AdvicePatients are told that the scaphoid will be excised and the mid-carpal joint will be fused. They will be immobilised in a plaster cast for a while between six and 12 weeks. Patients are informed that their wrist movement will be reduced and that the procedure does not restore normality. They are warned of the other risks of non-union, mal-alignment of the wrist joint, ulnar sided pain in addition to the usual surgical risks of infection, stiffness, algodystrophy and nerve injury. All other alternatives are discussed and a shared decision is made.
TechniqueMy preference is to do this procedure through a dorsal longitudinal incision centred over the middle finger ray. The extensor retinaculum is divided transversely and the stout septum between the third and fourth extensor retinaculum is divided. This allows the distal part of the retinaculum to be retracted, exposing the Extensor Pollicis Longus tendon and the tendons of the fourth compartment. These are retracted radially and ulnar-wards to expose the dorsum of the wrist capsule.
The posterior interosseous nerve is identified as it courses to the dorsum of the wrist. A one-centimetre section is excised from as proximal as the incision permits. Once the nerve is divided the radiocarpal joint is entered distal to the Lister’s tubercle and the capsulotomy extended radially to the styloid. On the ulnar side the incision is oblique through the middle of the dorsal radiotriquetral ligament towards the triquetrum and then distally for one centimetre. The incision into the capsule then goes radially to the scaphoid and the dorsal radially based flap is elevated from the carpal bones fully exposing the mid carpal joint.
The scaphoid is then mobilised and removed using sharp dissection and a periosteal elevator. The palmar ulnar corner of the scaphoid tuberosity can at times cause a problem as it is very strongly attached. Sometimes the scaphoid is large and may need to be divided using Lambotte osteotomes. Bone nibblers are used to complete the excision. When dealing with a SNAC wrist we usually retain the proximal scaphoid. The area is washed and any debris removed.
Attention is turned to the dorsal osteophytes, which are trimmed back, and the radial styloid is trimmed with osteotomes to present a rounded surface and avoid impacting on the trapezium on radial deviation.
Attention is then turned to the mid carpal joint, which is usually unaffected. The surfaces of the capitate, hamate, triquetrum and lunate are cut back to good bleeding bone using a combination of rongeurs, osteotomes and a 4 mm burr. The area is washed to remove debris, and packed with cancellous bone. We prefer to obtain good quality cancellous bone from the patient’s opposite iliac crest. This is morcellised using a bone cutter and packed into the mid carpal joint. The joints are stabilised using 1.1 mm Kirschner wires, with attention being paid to correct any dorsal tilting of the lunate. The position is checked on image intensifier.
Once a satisfactory position is obtained we prefer to hold position using a circular plate (Figure 3). There are many alternative ways of holding the bones in position10 and the surgeon needs to be familiar with a few of these techniques.
The capsule is then closed with a few interrupted sutures. The transverse split in the extensor retinaculum is quickly closed with a running absorbable suture. The wound is infiltrated with a long acting local anaesthetic. The longitudinal skin incision is closed and the wrist bandaged. We routinely apply a plaster of Paris cast on the palmar surface to immobilise the wrist.
Journal of Trauma and Orthopaedics: Volume 01, Issue 02, pages 50-58Title: Motion-preserving salvage surgery of the wrist after a scaphoid non-union or scapholunate dissociationAuthors: Joseph J Dias
Figure 3 - This intra-operative photograph shows the scaphoid excised and the midcarpal joint stabilised with a circular plate.
Volume 01 / Issue 02 / September 2013 boa.ac.uk Page 56
Peer-Reviewed Articles
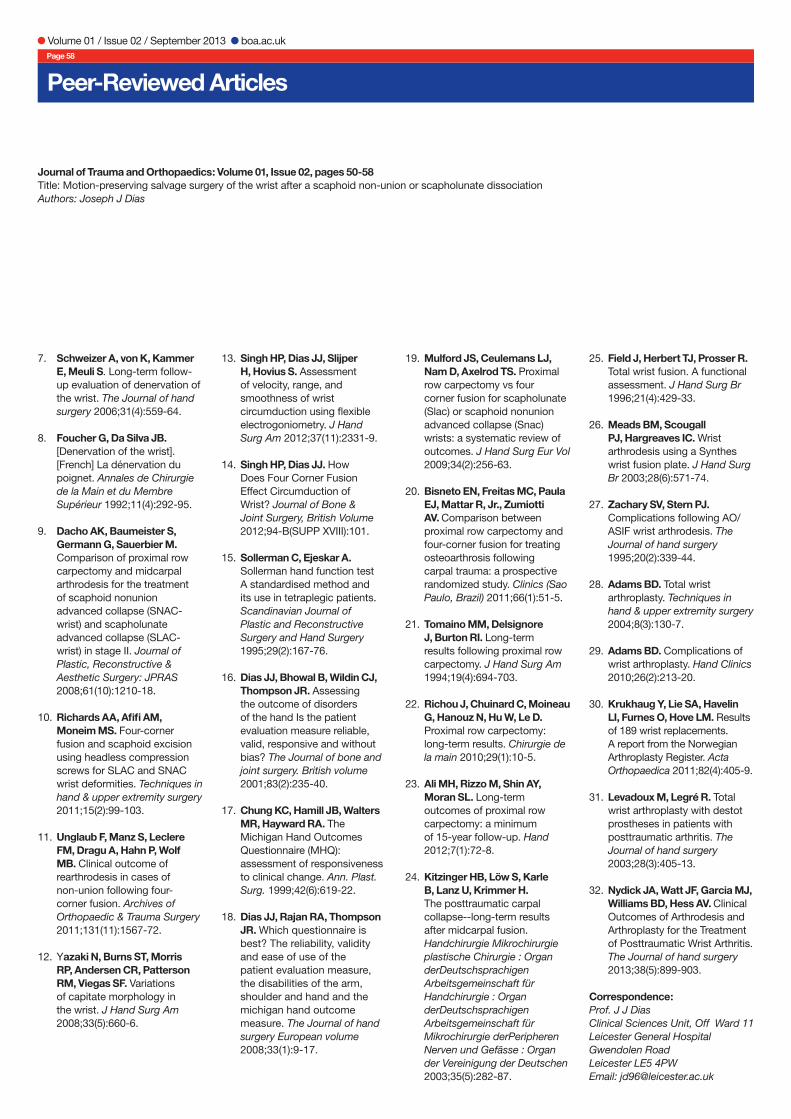
The immediate aftercare is to elevate the wrist and hand for a few hours and start early exercises to recover hand and finger movement. The plaster of Paris slab is retained for a few weeks and then the wrist is supported in a removable splint. Union is assessed on radiographs at six and 12 weeks (Figure 4). Any uncertainty about union is resolved using a wrist CT scan to establish whether there is bridging bone.
Tricks and tipsThere are three problems that can be avoided by attention to technical detail:
1. Range of wrist movement is retained if the DISI is corrected. So careful attention to this and checks before stabilisation using intra-operative fluoroscopy helps avoid a fusion in persistent DISI position.
2. Radial tilting of the hand can be avoided by allowing the capitate to find its neutral position and by not trying to locate the capitate into the cup of the lunate. This causes a fusion where the carpus will assume a position of radial deviation as the radiolunate ligament is rendered slack in this manoeuvre. So, as it regains its taut position, the lunate tilts radially.
3. The third problem is the pain on the ulnar side. This needs attention to ensure that the triquetrum is not fused so it protrudes towards the ulna leading to secondary impaction after the four-corner fusion.
OutcomeThis procedure needs the midcarpal bones to fuse. This takes up to 12 weeks and the wrist requires immobilisation in a plaster slab or wrist support. It requires the fusion of normal joints; around 5% of cases have failure of union and may need re-arthrodesis11. It is usual to retain 60% of movement but this is not predictable and some patients can lose much more than this. Most patients retain 80% of grip strength but around 25% continue to experience some pain even after solid midcarpal fusion.
Salvage for a failed four-corner fusion is a total wrist replacement or a total wrist fusion.
Proximal row carpectomy
This is an arthroplasty that excises not just the scaphoid but also the remainder of the proximal carpal row and includes excision of the lunate and the triquetrum.
This needs the articular cartilage on the proximal capitate and the lunate facet of the distal radius to be preserved. Low-demand patients are considered suitable for this. The concern about a proximal row carpectomy is that the carpal height is reduced thereby weakening the muscle tendon units of the long flexors and extensors of the fingers and wrist. In addition there is concern about rotational stability of the new joint. This procedure has been considered for those not needing forced grip in their daily and work activities9.
AdvicePatients are advised that they will need to protect the hand from forceful use for a few weeks. They are told that the weakness in their hands will persist and that a proportion of them will continue to have some pain in the wrist. They are also warned of weakness in tasks needing forearm rotation, such as opening doors.
TechniqueThe approach to the wrist is exactly the same as for four-corner fusion. After the scaphoid and radius osteophytes are excised the lunate and the triquetrum are removed. Care is taken to retain the radio-scapho-capitate ligament when dealing with the radial styloid. The capsule closure is as before.Tricks and tipsThe surgeon needs to be aware of the shapes of the capitate12. Those with a distinct ridge are more likely to have point loading and early degenerative change in the new joint between the capitate and radius.AftercareThe hand is elevated initially and the wrist may be immobilised in a plaster of Paris slab for the first week or so and then the wrist supported by a wrist splint. Full activities, which are not forceful, are permitted from the outset. Radiographs are obtained and follow-up is arranged for six and 12 weeks.
OutcomeThe wrist movement surprisingly does not improve significantly after a proximal row carpectomy. Once again patients usually retain two-thirds their range of movement and 80% of their maximal grip strength. However 5% need salvage surgery and around 25% continue to experience some pain, even after a proximal row carpectomy.
Figure 4 - This patient had midcarpal fusions on both sides using stout Kirschner wires. Note the solid fusion and the preservation of radiolunate joint height. Note that on the right the radial styloid has been excised to avoid impingement between the trapezium and the radial styloid on radial deviation.
Journal of Trauma and Orthopaedics: Volume 01, Issue 02, pages 50-58Title: Motion-preserving salvage surgery of the wrist after a scaphoid non-union or scapholunate dissociationAuthors: Joseph J Dias

Volume 01 / Issue 02 / September 2013 boa.ac.uk Page 57
Salvage for a failed proximal row carpectomy is a capitate hemi-replacement or a total wrist fusion.
So on the current evidence whether the patient is offered one or the other procedure very often comes down to the preference of the surgeon.
Outcomes in comparison
We investigated the function of the wrist and hand after a four-corner fusion and proximal row carpectomy and found that pain relief was comparable but the axis of wrist movement13 14 was parallel to that of the normal wrist after a proximal row carpectomy and was more vertical after a four-corner fusion. Function as assessed by the timed Sollerman hand function test15 was better and quicker after a proximal row carpectomy but tasks needing forearm rotation were more compromised after a proximal row carpectomy. We used two patient reported outcome questionnaires, the Patient Evaluation Measure16 and Michigan Hand Questionnaire17
18. Both have been validated for wrist disorders. Patient were more satisfied, and had better pain relief and function after a proximal row carpectomy. A systematic review of the literature comparing the two techniques demonstrated no difference between the two techniques although the risk of delayed arthritis in the joint between the capitate and radius was much greater after a proximal row carpectomy19. Another study comparing the two procedures in 20 patients also found no difference20.
At six years after a proximal row carpectomy in 23 patients, patients had 61% of range and 79% of strength21. Another study in 24 patients at 10 years found similar range and strength but noted radiographic arthritis in 52%22. But at 15 years 46 of 61 patients had persistent pain and were dissatisfied and arthritis between the capitate and radius was observed on radiographs and 12 of 61 (19.6%) needed full wrist fusion23.
After midcarpal fusion 37 patients were reviewed at 8 years and had range and strength that was similar to that seen after a proximal row carpectomy but 10/37 (27%) had developed radiolunate arthritis24. However, after either of these two procedures my clinical experience is that the need for further surgery after a successful operation is very low.
Other options: Total Wrist Fusion, Total Wrist Arthroplasty
In those patients with persisting disabling pain after these motion-preserving procedures or in those where the extent of arthritis precludes these operations, the surgeon may consider a total wrist arthroplasty or total wrist fusion. Both these procedures improve pain.
Fusion of the wrist gives more certain control of wrist pain but has a profound impact on the function of the arm6 25 26. The risks of fusion surgery are well established27. Non-union is unlikely but complications were noted: 50 of 71 (70%) wrists fused, with reoperation to remove the fusion plate needed in 20%. Eighteen wrists were left with permanent problems. 55 of 71 (77%) wrists fused had a stable pain-free wrist after a total wrist fusion27. Total wrist fusion is a reliable procedure but has a high problem rate and 1:4 will continue to have problems.
The other alternative is to perform a total wrist arthroplasty. Total wrist arthroplasty has evolved over recent decades and we now have experience and information on indications, techniques, complications and their salvage28-30. As our knowledge and experience of wrist arthroplasty in patients with post-traumatic arthritis increase31 32 this may become the intervention of choice especially when motion-preserving procedures fail.
Conclusion
We found that patients with a proximal row carpectomy had restricted movement, but retained the dart-throwing axis. Patients having a scaphoid excision and four-corner midcarpal fusion lost the dart-throwing axis of movement. There was nearly 65% loss of area of circumduction compared to the opposite wrist. Peak strength was similar after each of these operations. Patients reported better outcomes (PEM, MHQ) after a proximal row carpectomy but took longer to perform activities requiring forearm rotation. Based on our findings, a proximal row carpectomy is better, at least in the medium term.
If pain relief is inadequate the surgeon can consider either a wrist arthroplasty or a full wrist fusion using a custom fusion plate.
In summary, wrist salvage surgery for post-traumatic pain due to degenerative change needs to be specifically tailored to each patient. There are many surgical options and good shared-decision-making and technical execution are the key to obtaining a satisfactory outcome.
Of the two procedures that preserve motion, the proximal row carpectomy is superior in the medium term as it retains the natural axis of wrist movement. But late reviews suggest that 1:4 cases will continue to have or develop wrist pain after either of these two common motion-preserving procedures.
References
1. Hidaka Y, Nakamura R. Progressive patterns of degenerative arthritis in scaphoid nonunion demonstrated by three-dimensional computed tomography. J Hand Surg Br 1998;23(6):765-70.
2. Watson HK, Ballet FL. The SLAC wrist: scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9(3):358-65.
3. Mack GR, Bosse MJ, Gelberman RH, Yu E. The natural history of scaphoid non-union. J Bone Joint Surg Am 1984;66(4):504-09.
4. Moritomo H, Tada K, Yoshida T, Masatomi T. The relationship between the site of nonunion of the scaphoid and scaphoid nonunion advanced collapse (SNAC). J Bone Joint Surg Br 1999;81(5):871-76.
5. Anderson M, Adams B. Total wrist arthroplasty. Hand Clinics 2005;21(4):621-30.
6. Houshian S, Schrøder HA. Wrist arthrodesis with the AO titanium wrist fusion plate: a consecutive series of 42 cases. J Hand Surg Br 2001;26(4):355-59.
Journal of Trauma and Orthopaedics: Volume 01, Issue 02, pages 50-58Title: Motion-preserving salvage surgery of the wrist after a scaphoid non-union or scapholunate dissociation
Authors: Joseph J Dias
© 2013 British Orthopaedic Association
Volume 01 / Issue 02 / September 2013 boa.ac.uk Page 58
Peer-Reviewed Articles
7. Schweizer A, von K, Kammer E, Meuli S. Long-term follow-up evaluation of denervation of the wrist. The Journal of hand surgery 2006;31(4):559-64.
8. Foucher G, Da Silva JB. [Denervation of the wrist]. [French] La dénervation du poignet. Annales de Chirurgie de la Main et du Membre Supérieur 1992;11(4):292-95.
9. Dacho AK, Baumeister S, Germann G, Sauerbier M. Comparison of proximal row carpectomy and midcarpal arthrodesis for the treatment of scaphoid nonunion advanced collapse (SNAC-wrist) and scapholunate advanced collapse (SLAC-wrist) in stage II. Journal of Plastic, Reconstructive & Aesthetic Surgery: JPRAS 2008;61(10):1210-18.
10. Richards AA, Afifi AM, Moneim MS. Four-corner fusion and scaphoid excision using headless compression screws for SLAC and SNAC wrist deformities. Techniques in hand & upper extremity surgery 2011;15(2):99-103.
11. Unglaub F, Manz S, Leclere FM, Dragu A, Hahn P, Wolf MB. Clinical outcome of rearthrodesis in cases of non-union following four-corner fusion. Archives of Orthopaedic & Trauma Surgery 2011;131(11):1567-72.
12. Yazaki N, Burns ST, Morris RP, Andersen CR, Patterson RM, Viegas SF. Variations of capitate morphology in the wrist. J Hand Surg Am 2008;33(5):660-6.
13. Singh HP, Dias JJ, Slijper H, Hovius S. Assessment of velocity, range, and smoothness of wrist circumduction using flexible electrogoniometry. J Hand Surg Am 2012;37(11):2331-9.
14. Singh HP, Dias JJ. How Does Four Corner Fusion Effect Circumduction of Wrist? Journal of Bone & Joint Surgery, British Volume 2012;94-B(SUPP XVIII):101.
15. Sollerman C, Ejeskar A. Sollerman hand function test A standardised method and its use in tetraplegic patients. Scandinavian Journal of Plastic and Reconstructive Surgery and Hand Surgery 1995;29(2):167-76.
16. Dias JJ, Bhowal B, Wildin CJ, Thompson JR. Assessing the outcome of disorders of the hand Is the patient evaluation measure reliable, valid, responsive and without bias? The Journal of bone and joint surgery. British volume 2001;83(2):235-40.
17. Chung KC, Hamill JB, Walters MR, Hayward RA. The Michigan Hand Outcomes Questionnaire (MHQ): assessment of responsiveness to clinical change. Ann. Plast. Surg. 1999;42(6):619-22.
18. Dias JJ, Rajan RA, Thompson JR. Which questionnaire is best? The reliability, validity and ease of use of the patient evaluation measure, the disabilities of the arm, shoulder and hand and the michigan hand outcome measure. The Journal of hand surgery European volume 2008;33(1):9-17.
19. Mulford JS, Ceulemans LJ, Nam D, Axelrod TS. Proximal row carpectomy vs four corner fusion for scapholunate (Slac) or scaphoid nonunion advanced collapse (Snac) wrists: a systematic review of outcomes. J Hand Surg Eur Vol 2009;34(2):256-63.
20. Bisneto EN, Freitas MC, Paula EJ, Mattar R, Jr., Zumiotti AV. Comparison between proximal row carpectomy and four-corner fusion for treating osteoarthrosis following carpal trauma: a prospective randomized study. Clinics (Sao Paulo, Brazil) 2011;66(1):51-5.
21. Tomaino MM, Delsignore J, Burton RI. Long-term results following proximal row carpectomy. J Hand Surg Am 1994;19(4):694-703.
22. Richou J, Chuinard C, Moineau G, Hanouz N, Hu W, Le D. Proximal row carpectomy: long-term results. Chirurgie de la main 2010;29(1):10-5.
23. Ali MH, Rizzo M, Shin AY, Moran SL. Long-term outcomes of proximal row carpectomy: a minimum of 15-year follow-up. Hand 2012;7(1):72-8.
24. Kitzinger HB, Löw S, Karle B, Lanz U, Krimmer H. The posttraumatic carpal collapse--long-term results after midcarpal fusion. Handchirurgie Mikrochirurgie plastische Chirurgie : Organ derDeutschsprachigen Arbeitsgemeinschaft für Handchirurgie : Organ derDeutschsprachigen Arbeitsgemeinschaft für Mikrochirurgie derPeripheren Nerven und Gefässe : Organ der Vereinigung der Deutschen 2003;35(5):282-87.
25. Field J, Herbert TJ, Prosser R. Total wrist fusion. A functional assessment. J Hand Surg Br 1996;21(4):429-33.
26. Meads BM, Scougall PJ, Hargreaves IC. Wrist arthrodesis using a Synthes wrist fusion plate. J Hand Surg Br 2003;28(6):571-74.
27. Zachary SV, Stern PJ. Complications following AO/ASIF wrist arthrodesis. The Journal of hand surgery 1995;20(2):339-44.
28. Adams BD. Total wrist arthroplasty. Techniques in hand & upper extremity surgery 2004;8(3):130-7.
29. Adams BD. Complications of wrist arthroplasty. Hand Clinics 2010;26(2):213-20.
30. Krukhaug Y, Lie SA, Havelin LI, Furnes O, Hove LM. Results of 189 wrist replacements. A report from the Norwegian Arthroplasty Register. Acta Orthopaedica 2011;82(4):405-9.
31. Levadoux M, Legré R. Total wrist arthroplasty with destot prostheses in patients with posttraumatic arthritis. The Journal of hand surgery 2003;28(3):405-13.
32. Nydick JA, Watt JF, Garcia MJ, Williams BD, Hess AV. Clinical Outcomes of Arthrodesis and Arthroplasty for the Treatment of Posttraumatic Wrist Arthritis. The Journal of hand surgery 2013;38(5):899-903.
Correspondence: Prof. J J DiasClinical Sciences Unit, Off Ward 11Leicester General HospitalGwendolen RoadLeicester LE5 4PWEmail: [email protected]
Journal of Trauma and Orthopaedics: Volume 01, Issue 02, pages 50-58Title: Motion-preserving salvage surgery of the wrist after a scaphoid non-union or scapholunate dissociationAuthors: Joseph J Dias





























