Embed Size (px)
Citation preview

MICROSCOPY RESEARCH AND TECHNIQUE 34:544-553 (1996)
Morphological Changes at Paranodes in IgM Paraproteinaemic Neuropathy J.M. JACOBS Department of Neuropathology, Znstitute of Neurology, London WCl N 3BG, United Kingdom
KEY WORDS ABSTRACT The paranode is one of a number of sites of a specific myelin sheath abnormality found in cases of IgM paraproteinaemic neuropathy. The gammopathy may be malignant or, more frequently, benign, and is often associated with a predominantly demyelinating neuropathy. The circulating paraprotein IgM antibody, usually with kappa light chains, was found in many cases to recognise an antigenic determinant in myelin, identified as myelin-associated glycoprotein (MAG). Other glycoconjugates expressed by Schwann cells may also be recognised by the antibody. MAG is localized to regions of the myelin sheath in which the membranes are uncompacted. The paranode is one such region, and there is evidence that IgM is deposited specifically on the membranes of the terminal loops of the myelin sheath in addition to other MAGassociated regions of the sheath. In many cases the presence of the paraprotein appears not to otherwise affect paranodal organization; in a few it is associated with changes to the termination of the loops on the axolemma and to the associated Schwann cell cytoplasm. These findings do not provide unambiguous evidence that binding of anti-MAG IgM antibodies a t the paranode is a direct cause of demyelination. Whilst localization of the paraprotein closely matches that of MAG, proof is still lacking that the relevant
Neuropathy, Myelin-associated glycoprotein, IgM
antigen is MAG itself. - 8 1996 WileyILiss, he.
INTRODUCTION The paranodal region is one of a number of sites of a
specific myelin sheath abnormality that may be seen in nerve biopsies of patients with neuropathy associated with IgM paraproteinaemia. As a background to the understanding of these changes, it is appropriate to give a brief account of the neuropathy, one of the specific components of the nerve that is involved-myelin-as- sociated glycoprotein-and the possible role of the para- proteins. Reference is made to experimental studies.
PARAPROTEINAEMIA AND ITS ~~ -
~ RELATIONSHIP TO PERIPHERAL NEUROPATHY
Paraproteins are immunoglobulins produced in ex- cess by the monoclonal proliferation of plasma cells or their precursors. In conditions such as multiple my- eloma, certain forms of amyloidosis, Waldenstrom’s macroglobulinaemia, and other lymphoproliferative disorders, there is uncontrolled production of parapro- teins. It has long been known that these disorders may be associated with peripheral neuropathy.
In addition, a much larger group of patients has now been identified in which the presence of monoclonal serum paraproteins is unassociated with evidence of a malignant lymphoproliferative disorder. The term be- nign or nonmalignant gammopathy is used to describe this condition, although Kyle (1984) has suggested that it be called “monoclonal gammopathy of unknown sig- nificance” (MGUS) since long-term follow-up studies have shown that up to 10% of these patients go on to develop a malignant gammopathy. In benign parapro- teinaemia, the level of serum monoclonal proteins (M
protein) is relatively low and may remain unchanged for many years (Kelly, 1985).
An association has been identified between mono- clonal gammopathy and peripheral neuropathy. In a large series of patients referred to a neurological hos- pital, electrophoretic examination of sera revealed a group with benign paraproteinaemia in which there was a disproportionate number of cases of neuropathy (Kahn et al., 1980). In another series of patients with neuropathy of unknown aetiology, Kelly et al. (1981) found monoclonal gammopathy in lo%, whilst the in- cidence was only 2.5% in patients with other recognised causes of neuropathy. The occurrence of monoclonal gammopathy increases with age, and the associated neuropathy is now an important cause of peripheral neuropathy in older patients (Latov, 1988).
The different monoclonal proteins are named accord- ing to the class of their heavy chain; the three of im- portance in the present context are IgG (y), IgA (a) and IgM (k). Each of the monoclonal protein classes may be associated with neuropathy. The relative incidence of IgG, IgA, and IgM varies in the published reports, but in recent papers Yeung et al. (1991) found IgM para- protein in 46 of 63 patients with peripheral neuropathy associated with benign monoclonal neuropathy, and Suarez and Kelly (1993) recorded that 23 of 39 patients had an IgM paraproteinaemia. In most cases the light chain type is kappa; of their 46 cases Yeung et al.
~ ~
Received February 13, 1996; accepted in revised form March 20, 1995. Address reprint request to J.M. Jacobs, Department of Neuropathology, Insti-
tute of Neurology, Queen Square, London WClN 3BG, U.K.
0 1996 WILEY-LISS, INC.

PARANODES IN PARAPROTEINAEMIC NEUROPATHY 545
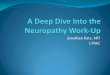
Fig. 1. Electron micrograph of a longitudinal section through the paranodal region of a normal small myelinated fibre. Individual terminal myelin loops are separated by a clear space (arrows). Membranes of the Schwann cell and the axon are separated by a gap with periodic densities or transverse bands (arrowheads). Bar = 0.5 wm.
(1991) found 36 with IgM kappa and 10 with IgM lambda.
The clinical pattern of neuropathy is broadly similar in patients with all classes of paraproteinaemia, al- though the IgA cases are less well documented. The neuropathy is of late onset, slowly progressive, distal sensorimotor, and usually demyelinating. A male pre- ponderance is found among patients with IgM parapro- teins.
It is the IgM paraproteinaemia cases with which this chapter is concerned, and in particular a group of these in which the circulating monoclonal paraprotein anti- body is directed against a component of peripheral nerve myelin. Direct immunohistochemistry was used to demonstrate the presence of IgM on unspecified com- ponents of myelin sheaths in nerve biopsies (Dalakas and Engel, 1981; Meier et al., 1984; Smith et al., 1983; Swash et al., 1979). The pattern of staining is variable; some describe positive staining over the entire myelin sheath (Smith et al., 1983); others find it is limited to the periphery of the myelin sheath and, sometimes, the periaxonal region (Meier et al., 1984). The most con- vincing results are seen using direct immunoperoxi- dase methods on deplasticized semithin sections, when positive reaction product is limited to outer parts of the sheath and sometimes to periaxonal regions (Jacobs and Scadding, 1990; Meier et al., 1984; Mendell et al., 1985). Binding of IgM in patients’ serum to control pe- ripheral nerve tissue (indirect immunostaining) also produces variable staining patterns, but again with de- plasticized resin sections giving the most satisfactory results, with a pattern of staining similar to that seen by direct immunostaining.
An important further step in the study of IgM para- proteinaemic neuropathy, and of particular relevance in this chapter, was the demonstration that the anti- genic determinant in myelin recognised by the anti- body was myelin-associated glycoprotein (MAG) (Braun et al., 1982; Steck et al., 1983). In the majority
of patients with neuropathy associated with IgM para- proteinemia, anti-MAG activity has been demon- strated in the serum (Hafler et al., 1986, Nobile-Orazio et al., 1994; Yeung et al., 1991). Other antigens are recognised by anti-MAG antibodies, and these are dis- cussed below.
Earlier studies failed to detect complement; however, in later reports, colocalization of the monoclonal para- protein with complement components Clq, C3D, and C5 and the terminal membrane complex led to the sugges- tion that demyelination may be mediated by comple- ment (Monaco et al., 1990).
THE PARANODAL REGION AND
GLYCOPROTEIN (MAG) The paranode is the region in which myelin lamellae
terminate on the axolemma as a helical series of loops each containing a small pocket of Schwann cell cyto- plasm. The outermost lamellae terminate nearest to the node of Ranvier. Figure 1 shows a normal paranode of a small myelinated fibre in longitudinal section; in large fibres the organization is more complex, and not all of the lamellae terminate on the axolemma but are stacked on each other producing an appearance “re- sembling ears of barley” (Thomas et al., 1992). Each terminal myelin loop is separated from its neighbour by a gap of 12-14 nm, a distance associated with the presence of MAG in the membranes (Trapp and Quarles, 1982). The junction of the terminal loops and the axolemma is distinguished by a narrow intercellu- lar gap in which periodic densities can be identified (Fig. 1). These “transverse bands,” first described in the central nervous system by Hirano and Dembitzer (1969), are ridges with an oblique orientation.
Figure 2 shows a schematic representation of the ex- pression of MAG, Po, and the neural cell adhesion mol- ecule, N-CAM, at the paranodal region, in Schmidt- Lanterman incisures and in the periaxonal space.
MYELIN-ASSOCIATED

546 J.M. JACOBS
Fig. 2. Diagram of nodal and paranodal regions of a myelinated fibre showing expression of MAG (A), Po (o), and N-CAM (A). A Schmidt-Lanterman incisure is seen to the right. Axon stippled, Schwann cell checkered. (Modified from Martini (1994), with permission of Chapman.)
Myelin-associated glycoprotein (MAG) is a minor com- ponent of both peripheral and central nervous system myelin, constituting about 1% or less of myelin pro- teins (Quarles, 1979). It has a molecular weight of about 100 kD and contains about 30% by weight of carbohydrate. On the basis of cloning studies (Lai et al., 1987; Salzer et al., 19871, MAG is considered to be a member of the immunoglobulin superfamily. It is an integral membrane protein of Schwann cells and oligo- dendroglia (Quarles et al., 19731, probably being unique to the nervous system. Much of the MAG mol- ecule is exposed on the membrane surface and is there- fore readily available to act as an antigen.
MAG was found to be localised to periaxonal mem- branes, noncompacted myelin lamellae at Schmidt- Lanterman incisures, a t the outer mesaxon, and at ter- minal loops of myelin at the paranodes; it was not present in compact myelin (Fig. 2) (Martini and Schachner, 1986; Trapp and Quarles, 1982, 1984). From its distribution MAG was assigned a role in maintaining the separation of membranes at the peri- axonal space, the incisures, the outer mesaxon, and the paranodal myelin loops by preventing compaction of Schwann celUmyelin or Schwann celUSchwann cell membranes. It is probably the size and polarity of the extracellular domain of the MAG molecule at the ex- tracellular side of the Schwann cell membrane that maintains the 12-14 nm gap between it and an ap- posed Schwann cell or axon (Trapp, 1990). The local- ization and potential functions of MAG have been re- viewed by Trapp (1990) and Martini (1994).
IgM anti-MAG antibodies from patients with periph- eral neuropathy recognise a carbohydrate epitope on MAG. This same epitope is also expressed on other gly- coconjugates in the peripheral nervous system such as 19-28 kD glycoproteins (one recently characterized as PMP-22 [Snipes et al., 19921) and glycolipids identified as sulphate-3-glucuronyl paragloboside (SGPG) and sulfated glucuronic acid containing lactosaminyl para- globoside (SGLPG) (Ariga et al., 1987; Chou et al., 1985). These, as well as MAG, must be considered as potential targets for IgM paraproteins. Po glycoprotein,
present in compact myelin (Fig. 2) has also been re- ported as containing the same carbohydrate epitope (Bollensen et al., 1988). Anti-MAG paraproteins have also been shown to bind to other nervous system adhe- sion molecules, including L1 and N-CAM, although re- activity is weaker than for MAG (Steck et al., 1987). These molecules might also be potential targets of the IgM antibody during nerve regeneration when L1 and N-CAM are strongly upregulated in denervated Schwann cells (Martini, 1994).
HNK-1 (anti-Leu-7) is an experimentally produced mouse monoclonal IgM antibody that is raised against a human T cell line and recognizes a subset of human lymphocytes including natural killer cells (Chou et al., 1986). HNK-1 resembles anti-MAG antibodies in bind- ing to carbohydrate determinants expressed on SGPG, SGLPG, MAG, and other cell adhesion molecules in- cluding L1, N-CAM, and J1. The highly antigenic epitopes shared by these nervous system glycoproteins have been identified as sulfated glucuronyl glycolipids (Ilyas et al., 1984). Studies of sera from patients with IgM paraproteinaemic neuropathy have shown hetero- geneity of the fine specificity of anti-MAG antibodies that may influence their pathogenic effects (Ilyas et al., 1990).
In studies of the localisation of the neural adhesion molecules L1, N-CAM, and MAG in developing nerve, it was concluded that L1 and N-CAM are involved in initial Schwann-axon interactions (Mirsky et al., 19861, with MAG beginning to be expressed once my- elination had begun and L1 and N-CAM expression had ceased (Martini and Schachner, 1986). During my- elination in nerve development, MAG is expressed at the axon-Schwann cell surface and in the first few non- compacted turns of the Schwann cell membrane. Pre- sumably MAG is also expressed at these sites in remy- elination following demyelination, where it would also be a potential target of anti-MAG IgM antibody.
Recent studies provide rather conflicting evidence of the importance of MAG. In in vitro studies with trans- fected Schwann cells underexpressing MAG, a propor- tion of axons did not myelinate (Owens and Bunge,

547 PARANODES IN PARAPROTEINAEMIC NEUROPATHY
1991). On the other hand, in mice, with a null mutation in the mag locus, that are totally deficient in MAG the degree of myelination and compaction was normal, al- though the organization of the periaxonal regions was partially impaired (Li et al., 1994; Montag et al., 1994).
MAG was found to have an inhibitory effect upon neurite outgrowths of developing cerebellar neurons (Mukhopadhyay et al., 1994) and of neurons of a neu- roblastoma cell line (McKerracher et al., 1994). In pe- ripheral neurons, the effect of MAG varied with age of the cells, causing inhibition of neurite outgrowth in adult dorsal root ganglion (DRG) cells but promoting their outgrowth in DRG cells from newborn animals (Mukhopadhyay et al., 1994).
PATHOLOGY OF NEUROPATHY ASSOCIATED WITH IgM PARAPROTEINAEMIA
All reports of the neuropathy describe it as a demy- elination with varying degrees of axonal loss. Strong evidence of demyelination has been provided by nerve conduction studies, with reduced conduction velocities, conduction block, and dispersion in many cases. In pathological studies, thinly myelinated fibres, some- times associated with onion bulb formations, are de- scribed (Fig. 3). It is not an inflammatory disease, al- though inflammatory cells have been reported in a few cases (Vital et al., 1991). Few papers report the nerve fibre appearances in any detail, perhaps because the major interest has been in the binding of IgM to the fibres. Postmortem studies of one case (Mendell et al., 1985) suggested a primary axonal disease with second- ary demyelination and remyelination. In one case of Jacobs and Scadding (1990) there was evidence of ax- onal atrophy with many fibres having low g ratios (small axon diameter relative to myelin sheath thick- ness). Examination of teased fibres in this case showed evidence of secondary demyelination (paranodal, or more extensive) along some “original” atrophic fibres, although a greater number of fibres showed primary de- and remyelination. In assessing the possible role of IgM antibodies in causing demyelination, it is clearly important to know whether demyelination is primary or secondary.
Widening of the periodicity of myelin lamellae, due to an increase in the distance separating the intrape- riod line interfaces, is a very distinctive finding in bi- opsies from neuropathies associated with IgM parapro- teinaemia. Figure 4 illustrates a site of increased periodicity of myelin. Granular material is seen on the external surface of the Schwann cell membrane and at the widened mesaxon, a site associated with MAG, causing a widening at the intraperiod line when the membranes compact to form myelin; the cytoplasmic surface is unaffected, and there is normal formation of the major dense line.
Part of the myelin widening process includes the in- creased separation of terminal loops in the paranodal region (Jacobs and Scadding, 1990). First demon- strated by Sluga (1970), wide myelin has been a con- sistent finding in IgM paraproteinaemic neuropathy both of malignant (Propp et al., 1975) and benign type (Jacobs and Scadding, 1990; Lach et al., 1993; Monaco
et al., 1990; Meier et al., 1984; Mendell et al., 1985; Smith et al., 1983; Vital et al., 1989; Yeung et al., 1991) and may be considered as almost specific for these neu- ropathies (Vital et al., 1989). Widened myelin was also described in the experimental model of paraprotein neuropathy in the chick (Tatum, 1993) (see Experimen- tal Studies).
Monaco et al. (1990) observed a correlation between the numbers of fibres with abnormally spaced myelin and the extent of deposition of terminal-complement complex. They suggested that the abnormally spaced myelin might be due to an influx of intracellular water after damage by the terminal-complement complex. An earlier paper by King and Thomas (1984) had also sug- gested that the widening was a physicochemical change, perhaps due to binding of specific immunoglo- bulins, leading to overhydration. However, there is now little doubt that widening is associated with the deposition of IgM on myelin. Positive immunostaining for anti-MAG antibody in semithin sections corre- sponded to regions of myelin widening in adjacent ul- trathin sections (Mendell et al., 1985). Although rarely remarked upon in other reports, clumps of granular material, sometimes of considerable size, were clearly seen in continuity with similar material at widened lamellae in several cases (Jacobs and Scadding 1990; Jacobs, unpublished observations) (see Fig. 8). Immu- noelectron microscopy was used to demonstrate IgM kappa paraprotein in regions of myelin widening (Lach et al., 1993).
The incidence of wide myelin varies greatly from one case to another but may affect over 80% of myelinated fibres (Jacobs and Scadding, 1990). It is frequently ob- served in the outermost layers of the myelin sheath (Lach et al., 1993; Meier et al., 1984; Melmed et al., 1983; Pollard et al., 1985; Vital et al., 1989). A number of reports describe wide myelin in fibres that are prob- ably remyelinating (Meier et al., 1984; Mendell et al., 1985). However, it is also identified in fibres that are not remyelinating (King and Thomas, 19841, and Ja- cobs and Scadding (1990) found wide myelin in “origi- nal” atrophic fibres. There are few references to other sites of myelin widening. King and Thomas (1984) noted that wide myelin was more common in the nodal region. In the chick model (see Experimental Studies) Tatum (1993) described IgM deposition at nodes and Schmidt-Lanterman incisures, although these were only demonstrated by light microscopy.
The distribution of widened lamellae at paranodes and Schmidt-Lanterman incisures and in periaxonal regions and external mesaxons found by Jacobs and Scadding (1990) very precisely matches that of the dis- tribution of MAG. However, there were other locations, not corresponding to recognised sites of MAG, where deposited material likely to represent IgM was identi- fied. These include the external surface of the Schwann cell, beneath the basement membrane, and the com- pact myelin, particularly the outermost lamellae. These sites may be associated with glycoconjugates previously referred to that are also recognised by MAG antibodies.
In electron microscope studies of longitudinal sec- tions Jacobs and Scadding (1990) found an increase in

Fig. 3. Semithin resin section from a nerve biopsy of a case of IgM anti-MAG paraproteinaemic neuropathy showing thinly myelinated fibres characteristic of a demyelinating neuropathy (arrows). Arrow- heads indicate small onion bulbs. Bar = 50 pm.
Fig. 4. Electron micrograph from a case of IgM anti-MAG para- proteinaemic neuropathy showing a transverse section through an internodal region. Myelin lamellae of normal periodicity are Been to the left. The external surface of the Schwann cell and the external mesaxon are coated with granular material (arrowheads); this also extends into the first and second lamellae of compact myelin. There is normal formation of the major dense line (arrow), but the intraperiod
line is markedly widened. Bar = 0.1 pm. (Reproduced from Jacobs and Scadding (19901, with permission of Springer-Verlag.)
Fig. 5. Electron micrographs of longitudinal sections at nodes/ paranodes of myelinated fibres from three different cases of IgM anti- MAG paraproteinaemic neuropathy. a,b The space between individ- ual terminating myelin loops is widened and granular material is visible in the gap which narrows on approaching the axolemma (ar- rows). Transverse bands are present. In panel a, terminal loops arise from myelin of normal periodicity. In panel b, the widened gap is continuous with myelin of increased periodicity (wide myelin). Bar = 0.5 pm.

PARANODES IN PARAPROTEINAEMIC NEUROPATHY 549
the spacing between terminal myelin loops as they ap- proach the axolemma at the paranodal region (Fig. 5a,b); in general, this change did not appear to affect the other specializations at the paranodal regions such as the transverse bands.
Further studies on four cases of monoclonal IgM anti- MAG paraproteinaemic neuropathy (Jacobs and Scad- ding, 1990; Jacobs, unpublished) allow a more detailed description of these paranodal changes. All of the nerve biopsies showed evidence of demyelination and remy- elination. Most of the nodes examined from each biopsy were from fibres of small size; some were probably re- myelinating. Because of the relatively small numbers of nodes from each nerve that could be examined in lon- gitudinal section by electron microscopy, it is not pos- sible to give precise incidences (compared with unaf- fected nodes) of the various paranodal changes. The main nodal abnormality was the increased separation of adjacent terminal loops. This often extended back just to the point at which the myelin becomes noncompacted (Fig 5a), but in some fibres the widened gap was con- tinuous with “internodal” myelin of increased period- icity-“wide myelin” (Fig 5b). On approaching the ax- olemma the widened membranes narrowed down to the normal 12-14 nm gap immediately before terminating (Fig. 5a,b). Finely granular material could be seen within the gap. Not all paranodes showed this increase in terminal loop separation; in general, the more severe the demyelination, the greater the number of paranodes affected. OfZen, both paranodes at a node of Ranvier were abnormal, although in a few only one paranode was affected (Fig. 6).
Some types of paranodal change were noted only in the biopsy from the patient with the highest (30.8 g/l; normal 0.6-2.8 g/l) circulating levels of anti-MAG IgM. Thus, at some paranodes in this biopsy, the gap sepa- rating the terminating membranes did not narrow on approaching the axolemma, and the deposited granular material appeared to have spread to occupy spaces be- tween the terminal loops and the axolemma (Fig. 7a- c); in this case the cytoplasm in the terminal loops often appeared abnormal, with loss of organelles (Fig. 74. Sometimes all of the terminal loops were widely sepa- rated; in other cases perhaps only the outermost or the innermost loops were affected (Fig. 8). Very occasion- ally, the terminal loops appeared to have lifted off from the axolemma (Fig. 8).
In occasional fibres (that were possibly remyelinat- ing), widened myelin lamellae were seen to terminate at regions distant from the paranode, where again the loops were widely separated and transverse bands were visible (Fig. 9). Parts of Schmidt-Lanterman incisures with widened intraperiod lines are seen in this figure; the adjacent myelin also has increased periodicity.
Changes at the node of Ranvier itself were infre- quent. Schwann cell cytoplasm had sometimes re- tracted away from the node. Occasionally, increased density of organelles was noted in the axons of fibres with the paranodal changes.
EXPERIMENTAL STUDIES Early attempts to produce demyelination experimen-
tally were unsuccessful. It was later found that human
IgM antibody did not cross-react with rodent MAG. MAG is present in all species, but there is interspecies variation in antibody recognition of the molecule. The most suitable species for this type of study were found to be cats and chickens (O’Shannessy et al., 1985). In- traneural injection of cat nerve with human serum con- taining IgM paraprotein with anti-MAG activity caused demyelination, but the pathology did not resem- ble that of the human neuropathy; in particular, no wide myelin was found (Hays et al., 1987; Willison et al., 1988).
Passive transfer of human IgM anti-MAG parapro- teins into chicks (Tatum, 1993) caused demyelination and remyelination, and human IgM was demonstrated on myelin sheaths. By light microscopy, immunoperox- idase methods showed IgM deposition on most myelin sheaths; in transverse section some fibres showed a discontinuous crescent-shape distribution consistent with its localisation over Schmidt-Lanterman in- cisures; and longitudinal sections showed IgM deposi- tion in nodes of Ranvier and at incisures. Electron mi- croscopy showed widening of the periodicity of outer myelin lamellae, but paranodal changes were not noted.
It is of interest that intraneural injection of antibod- ies against sulfoglucuronyl paragloboside (SGPG) in the rat produced demyelination with vesiculation and loosening of the outer myelin lamellae (Maeda et al., 1991), a pattern of demyelination not described in the IgM anti-MAG neuropathies. SGPG is one of the gly- coconjugates that is recognised by IgM antibodies from patients with neuropathy. The sulfated glucuronic acid-containing glycolipids have been shown to be present in myelin and glial-associated membranes and in axolemma (Ariga et al., 1990). In the rat, anti-SGPG antibodies do not cross-react with MAG, therefore, the target antigens are likely to be sulfated glucuronyl gly- colipids.
THE ROLE OF MAG IN PERIPHERAL NEUROPATHY ASSOCIATED WITH
IgM PARAPROTEINAEMIA Does the abnormal appearance of the paranode in
IgM-associated demyelination provide any clue to the possible role of the paraprotein in this neuropathy?
There is good evidence that the paraprotein is a di- rect cause of demyelination, although this issue re- mains controversial. That some relationship exists be- tween anti-MAG paraproteins and neuropathy seems likely because of the high frequency of their associa- tion; and MAG is clearly a potential target. Further compelling evidence comes from the most successful of the experimental studies involving passive transfer of human IgM to chicks (Tatum, 1993). No correlation between antibody titre and degree of nerve pathology has been shown (Gosselin et al., 1991; Vital et al., 19891, although it must be pointed out that antibody titres in serum probably do not reflect levels in nerve tissue. The inconsistent clinical effects of lowering cir- culating paraprotein levels by plasmapheresis (Yeung et al., 1991) do not lend support to a causative role for the paraprotein, although this is not a strong argument since plasmapheresis is not always successful even in

550 J.M. JACOBS
Fig. 6. Electron micrographs as in Fig. 5. The myelin lamellae to the left terminate normally; on the right the distance between adja- cent terminating myelin loops is increased. Bar = 1 pm.
Fig. 7. Electron micrographs as in Fig. 5. a: At this parancde myelin lamellae appear to terminate over an extended region. Bar = 1
pm. b At higher power nearest to the node, granular material lies between terminal loops near to the axolemma (arrow). Bar = 0.5 pm c: Further distant from the node a mass of granular material lies between empty looking terminal loops and the axolemma (arrow). Bar = 0.6 km.

PARANODES IN PARAPROTEINAEMIC NEUROPATHY 551
Fig. 8. Electron micrographs as in Fig. 5 . Terminal loops near to the node appear to have lifted off from the axolemma (arrowheads). Large amounts of granular material are present within the myelin lamellae (arrows). The gaps between innermost terminating lamellae (to the left) are not widened. Bar = 1 pm.
Fig. 9. Electron micrographs as in Fig. 5. Unusual termination of myelin loops at some distance from the node, showing features to be found at paranodes (i.e., increased separation of adjacent myelin loops); transverse bands are seen. Curved arrows indicate widening of the intraperiod lines a t a Schmidt- Lankrman incisure; adjacent myelin has increased periodicity. Bar = 1 pm.
conditions in which circulating antibody is known to be the causative agent.
The paranodal changes described here neither con- firm nor refute the concept of a causal role for the cir- culating paraprotein in neuropathy. Although in some fibres the presence of paraprotein did not otherwise appear to affect paranodal or nodal organization, there was occasional evidence that the deposition of granular material is associated with changes at the paranodes that may represent the beginnings of demyelination. This was particularly the case in the nerve of a patient with very high levels of IgM, although the degree of demyelination in this nerve was less striking than that of nerves from other patients with much less circulat-
ing IgM paraprotein. Any alteration affecting the man- ner in which myelin loops terminate at the axolemma could certainly produce a functional change, since this specialized junctional region probably isolates the in- ternodal axolemma from rapid changes occurring at the node (Rosenbluth, 1984).
Since demyelination occurs in IgM paraprotein- aemias without anti-MAG activity and also in IgA and IgG gammopathies, a number of different mechanisms of demyelination are probably involved. Only the IgM paraproteinaemic neuropathies seem to show the spe- cific wide myelin abnormality, although how this leads to demyelination is still not clear. The vesiculation and loosening of myelin seen after experimental injection of

552 J.M. J A
anti-SGPG serum, another nerve glycoconjugate (see Experimental Studies), suggests a different process of demyelination from that seen in IgM neuropathies. Lit- tle is known of mechanisms of demyelination, but all are of interest since they are important and unique examples of antibody-mediated demyelination occur- ring in man.
ACKNOWLEDGMENTS I am grateful to Miss Hilary Ayling for her technical
expertise and to Mr. Steven Durr for the photography.
REFERENCES Ariga, T., Kohriyama, T., Freddo, L., Latov, N., Saito, M., Kon, K.,
Ando, S., Suzuki, M., Hemling, ME., Rinehart, K.L., Kusunoki, S., and Yu, R.K. (1987) Characterization of sulfated glucuronic acid containing glycolipids reacting with IgM M-proteins in patients with neuropathy. J. Biol. Chem., 262:848-853.
Ariga, T., Kusunoki, S., Asano, K., Oshima, M., Asano, M.A., Man- nen, T., and Yu, R.K. (1990) Localization of sulfakd glucuronyl glycolipids in human dorsal root and sympathetic ganglia, Brain
Bollensen, E., Steck, A.J., and Schachner, M. (1988) Reactivity with the peripheral myelin glycoprotein Po in serum from patients with monoclonal IgM gammopathy and polyneuropathy. Neurology, 38 1266-1270.
Braun, P.E., Frail, D., and Latov, N. (1982) Myelin-associated glyco- protein is the antigen for a monoclonal IgM in polyneuropathy. J. Neurochem., 39:1261-1265.
Chou, K.H., Ilyas, A.A., Evans, J.E., Quarles, R.H., and Jungalwala, F.B. (1985) Structure of a glycolipid reacting with monoclonal IgM in neuropathy and with HNK-1. Biochem. Biophys. Res. Commun.,
Chou, D.K.H., Ilyas, A.A., Evane, J.E., Costello, C., Quarles, R.H., and Jungalwala, F.B. (1986) Structure of sulfated glucuronyl gly- colipida in the nervous system reacting with HNK-1 antibody and some IgM paraproteins in neuropathy. J. Biol. Chem., 261:11717- 11725.
Dalakas, M., and Engel, W.K. (1981) Polyneuropathy with mono- clonal gammopathy. Studies of 11 patients. Ann. Neurol., 1045-52.
Gosselin, S., Kyle, R.A., and Dyck, P.J. (1991) Neuropathy associated with monoclonal gammopathies of undetermined significance. Ann. Neurol., 30:54-61.
Hafler, D.D., Johnson, D., Kelly, J.J., Panitch, H., Kyle, R., and Weiner, H.L. (1986) Monoclonal gammopathy and neuropathy: My- elin-associated glycoprotein reactivity and clinical characteristics. Neurology, 36:75-78.
Hays, A.P., Latov, N., Takatsu, M., and Sherman, W.H. (1987) Exper- imental demyelination of nerve induced by serum of patients with neuropathy and an anti-MAG IgM M-protein. Neurology, 37:242- 256.
Hirano, A., and Dembitzer, H.M. (1969) The transverse bands as means of access to the p e r i a ~ o ~ l space of the central myelinated nerve fiber. J. Ultrastruct. Res., 28141-149.
Ilyas, A.A., Quarles R.H., Macintosh, T.D., Dobersen, M.J., Trapp, B.D., Dalakas, M.C., and Brady, R.O. (1984) IgM in a human neu- ropathy related to paraproteinemia binds to a carbohydrate deter- minant in the myelin-associated glycoprotein and to a ganglioside. Proc. Natl. Acad. Sci. U.S.A., 81:1225-1229.
Ilyas, A.A., Chou, D.K.H., Jungalwala, F.B., Costello, C., and Quarles, R.H. (1990) Variability in the structural requirements for binding of human monoclonal anti-myelin-associated glycoprotein immunoglobulin M antibodies and HNK-1 to sphingoglycolipid an- tigens. J. Neurochem., 55594-601.
Jacobs, J.M., and Scadding, J.W. (1990) Morphological changes in IgM paraproteinaemic neuropathy. Acta Neuropathol., 80:77-84.
Kahn, S.N., Riches, P.G., and Kohn, J. (1980) Paraproteinemia in neurological disease: Incidence, associations, and classification of monoclonal immunoglobulins. J. Clin. Pathol., 33617-621.
Kelly, J.J. (1985) Peripheral neuropathies associated with mono- clonal proteins: A clinical review. Muscle Nerve, 8138-150.
Kelly, J.J., Jr., Kyle, R.A., O'Brien, P.C., and Dyck, PJ., (1981) Prev- alence of monoclonal protein in peripheral neuropathy. Neurology,
Res., 51957-64.
128383-388.
3 1: 1480-1483.
COBS
King, R.H.M., and Thomas, P.K. (1984) The occurrence and signifi- cance of myelin with unusually large periodicity. Ada Neuro- pathol., 63:319-329.
Kyle, R.A. (1984) Benign monoclonal gammopathy: A misnomer. - - - - JAMA, 251:1849.
Lach, B., Rippstein, P., Atack, D., Afar, D.E.H., and Gregor, A. (1993) Immunoelectron microscopic localization of monoclonal IgM anti- bodies in gammopathy associated with peripheral demyelinative neuropathy. Acta Neuropathol., 85:298-307.
Lai, C., Brow, M.A., Nave, K.-A., Noronha, A.B., Quarles R.H., Bloom, F.E., Milner, R.J., and Sutcliffe, J.G. (1987) Two forms of lB236/myelin-associated glycoprotein, a cell adhesion moleeule for p t n a t a l neural development, are produced by alternative splicing. Proc. Natl. Acad. Sci. U.S.A., 844337-4341.
Latov, N. (1988) Peripheral neuropathy and monoclonal gammopathy in ageing. In: Peripheral Nerve Changes in the Elderly, Vol 1. New Issues in Neurosciences. Basic and clinical approaches. P.K. Thomas, ed. Thieme Medical Publishers, New York. pp. 205-212.
Li, C., Tropak, M.B., Gerlai, R., Clapoff, S., Abramov-Newerly, W., Peterson, A., and Roder, J. (1994) Myelination in the absence of myelin-associated glycoprotein. Nature, 369747-750.
Maeda, Y ., Bigbee, J.W., Maeda, R., Miyatani, N., Kalb, R.G., and Yu, R.K. (1991) Induction of demyelination by intraneural injection of antibodies against sulfoglucuronyl paragloboside. Exp. Neurol.,
Martini, R. (1994) Expression and functional roles of neural cell sur- face molecules and extracellular matrix components during devel- opment and regeneration of peripheral nerves. J. Neurocq-tol., 23
Martini, R., and Sehachner, M. (1986) Immunoelectron microscope localization of neural cell adhesion molecules (Ll, N-CAM and MAG) and their shared carbohydrate epitope and myelin basic pro- tein in developing sciatic nerve. J. Cell Biol., 103:2439-2448.
McKerracher, L., David, S., Jackson, D.L., Koffis, V., Dunn, R.J., and Braun, P.E. (1994) Identification of myelin-associated glycoprotein as a major myelin-derived inhibitor of neurite growth. Neuron, 13:
Meier, C., Vandevelde, M., Steck, A., and Zurbriggen, A. (1984) De- myelinating polyneuropathy associated with monoclonal IgM-para- proteinaemia. J. Neurol. Sci., 63:353-367.
Melmed, C., Frail, D., Duncan, I., Braun, P., Danoff, D., Finlayson, M., and Stewart, J. (1983) Peripheral neuropathy with IgM kappa monoclonal immunoglobulin directed against myelin-associated glycoprotein. Neurology, 331397-1405.
Mendell, J.R., Sahenk, Z., Whitaker, J.N., Trapp, B.D., Yates, A.J., Griggs, R.C., and Quarles, R.H. (19%) Polyneuropathy and IgM monoclonal gammopathy: Studies on the pathogenetic role of anti- myelin-associated glycoprotein antibody. Neurology, 17243 -254.
Mirsky, R., Jessen, K., Schachner M., and Goridis, C. (19861 Distri- bution of the adhesion molecules N-CAM and L1 on peripheral neu- rons and glia in adult rats. J. Neurocytol., 15:799-815.
Monaco, S., Bonetti, B., Ferrari, S., Moretto, G., Nardelli, E., Tedesco, F., Mollnes, T.E., Nobile-Orazio, E., Manfredini, E., Bonazzi, L., and Rizzuto, N. (1990) Complement-mediated demyelination in patients with IgM monoclonal gammopathy and polyneuropathy. N. Engl. J.
Montag, D., Giese, K.P., Bartsch, U., Martini, R., Lang, Y., Bluth- mann, H., Karthigasan, J., Kimhner, D.A., Wintergerst, E.S., Nave, K.-A., Zielasek, J., Toyka, K.V., Lipp, H.-P., and Sehachner, M. (1994) Mice deficient for the myelin-associated glycoprotein show subtle abnormalities in myelin. Neuron, 13229-246.
Mukhopadhyay, G., Doherty, P., Walsh, F.S., Crocker, P.R., and Fil- bin, M.T. (1994) A novel role for myelin-associated glycoprotein as an inhibitor of axonal regeneration. Neuron, 13:757-767.
Nobile-Orazio, E., Manfredini, E., Carpo, M., Meucci, N., Monaco, S., Ferrari, S., Bonetti, B., Cavaletti, G., Gemignani, F., Durelli, L., Barbieri, S., Allaria, S., Sgarzi, M., and Scarlato, G. (1994) Fre- quency and clinical correlates of anti-neural antibodies in neurop- athy associated with IgM monoclonal gammopathy. Ann. Neurol., 36:416-424.
O'Shannessy, D.J., Willison, H.J., Inizuka, T., Dobersen, M.J., and Quarles, R.H. (1985) The species distribution of nervous system antigens that react with antimyelin-associated glycoprotein anti- bodies. J. Neuroimmunol., 9255-268.
Owens, G.C., and Bunge, P.P. (1991) Schwann cells infected with a recombinant retrovirus expressing myelin-associated glycoprotein antisense RNA do not form myelin. Neuron, 7565-575.
Pollard, J.J., Mcleod, J.G., and Feeney, D. (1985) Peripheral neurop-
113~221-225.
1-28.
805-811.
Med., 322649-652.

PARANODES IN PARAPROTEINAEMIC NEUROPATHY 553
athy in IgM kappa paraproteinaemia. Clinical and ultrastructural studies in 2 patients. Clin. Exp. Neurol., 21:41-54.
Propp, R.P., Means, E., Deibel, R., Sherer, G., and Barron, K. (1975) Waldenstrom's macroglobulinemia and neuropathy. Neurology, 25:
Quarles, R.H. (1979) Glycoproteins in myelin and myelin related membranes In: Complex Carbohydrates of the Nervous System. R.A. Margolis and R.K. Margolis, eds. Plenum Press, New York, pp. 203-233.
Quarles, R.H., Everly, J.C., and Brady, R.O. (1973) Evidence for the close association of a glycoprotein with myelin in rat brain. J. Neu- rochem., 21:1177-1191.
Rosenbluth, J. (1984) Membrane specialization at the nodes of Ran- vier and paranodal and juxtanodal regions of myelinated central and peripheral nerve fibers. In: The Node of Ranvier. J.C. Zagoren and S. Federoff, eds. Academic Press Inc., Orlando, FL, pp. 31-67.
Salzer, J.L., Holmes, W.P., and Colman, D.R. (1987) The amino acid sequences of the myelin-associated glycoproteins: Homology to the immunoglobulin gene superfamily. J. Cell Biol., 1M957-965.
Sluga, E. (1970) Uber eine Entmarkungsneuropathie bei T-G Para- proteinihie Wien. Klin. Wochenschr., 82667.
Smith, I.S., Kahn, S.N., Lacey, B.W., King, R.H.M., Eames, R.A., Whybrew, D.J., and Thomas, P.K. (1983) Chronic demyelinating neuropathy associated with benign IgM paraproteinaemia. Brain, 106169-195.
Snipes, G.J., Suter, U., Welcher, A.A., and Shooter, E.M. (1992) Char- acterization of a novel peripheral nervous system myelin protein (PMP-22/SR13). J. Cell Biol., 117:225-238.
Steek, A.J., Murray, N., Meier, C., Page, N., and Perruisseau, G. (1983) Demyelinating neuropathy and monoclonal IgM antibody to myelin-associated glycoprotein. Neurology, 33:19-23.
Steck, A.J., Murray, N., Dellagi, K., Brouet, J.-C., and Seligmann, M. (1987) Peripheral neuropathy associated with monoclonal IgM an- tibody. Neurology, 22:764-767.
Suarez, G.A., and Kelly, J.J., Jr. (1993) Polyneuropathy associated with monoclonal gammopathy of undetermined significance: Fur-
980-988.
ther evidence that IgM-MGUS neuropathies are different than I&- MGUS. Neurology, 43A304-1308.
Swash, M., Perrin, J., and Schwartz, M.S. (1979) Significance of im- munoglobulin deposition in peripheral nerve in neuropathies asso- ciated with paraproteinemia. J. Neurol. Neurosurg. Psychiatry, 42:
Tatum, A.H. (1993) Experimental paraprotein neuropathy, demyeli- nation by passive transfer of human IgM antimyelin-associated gly- coprotein. Ann. Neurol., 33:502-506.
Thomas, P.K., Landon D.N., and King, R.H.M. (1992) Diseases of peripheral nerves. In: Greenfield's Neuropathology, 5th ed. J. Hume Adams and L.W. Duchen, eds. Edward Arnold, London, pp.
Trapp, B.D. (1990) Myelin-associated glycoprotein. Location and po- tential function. Ann. N. Y. Acad. Sci., 60529-43.
Trapp, B.D., and Quarles, R.H. (1982) Presence of the myelin-associ- ated glycoprotein correlates with alterations in the periodicity of peripheral myelin. J. Cell Biol., 92:877-882.
Trapp, B.D., and Quarles, R.H. (1984) Immunocytochemical localiza- tion of the myelin-associated glycoprotein. Fact or artefact? J. Neu- roimmunol., 6231-249.
Vital, A., Vital, C., Julien, J., Baquey, A., and Steck, A.J. (1989) Polyneuropathy associated with IgM monoclonal gammopathy. Acta Neuropathol., 79160-167.
Vital, A., Latinville, D., Aupy, M., Dumas, P., and Vital, C. (1991) Inflammatory demyelinating lesions in two patients with IgM monoclonal gammopathy and polyneuropathy. Neuropathol. Appl. Neurobiol., 17415-420.
Willison, H.J., Trapp, B., Bacher, J.D., Dalakas, M.C., Griffin, J.W., and Quarles, R.H. (1988) Demyelination induced by intraneural injection of human anti-myelin associated glycoprotein antibodies. Muscle Nerve, 11:1169-1176.
Yeung, K.B., Thomas, P.K., King, R.H.M., Waddy, H., Will. R.G., Hughes, R.A.C., Gregson. N.A., and Leibowitz, S. (1991) The clin- ical spectrum of peripheral neuropathies associated with benign monoclonal IgM, IgG and IgA paraproteinaemia. J. Neurol., 238:
179-183.
1116-1245.
383-391.