Embed Size (px)
Citation preview

Regional Anesthesia 22(2):131-136, 1997
Morphine, Morphine-6-Glucuronide, and Morphine-3-Glucuronide in Cerebrospinal Fluid
and Plasma After Epidural Administration of Morphine
Sigga Kalman, M.D., Ph.D., Kerstin Metcalf, M.D., and Christina Eintrei, M.D., Ph.D.
Background and Objectives. It has been suggested that the potency of epidural mor- phine might be explained by spinal metabolism to the active and potent metabolite morphine-6-glucuronide (M6G). The main objective of this study was to describe the early pharmacokinetics of epidurally administered, morphine with special atten- tion to the appearance of the glucuronated metabolites in cerebrospinal fluid (CSF). Methods. Morphine was administered epidurally to eight patients scheduled for major abdominal surgery. The concentrations of morphine and its 6-glucuronide and 3-glucuronide metabolites were monitored in blood and CSF at 10, 30, 60, and 120 minutes and 10 and 24 hours. Postoperative pain was estimated on a visual analog scale, and analgesia requirements (administered by a patient-controlled techiqne) were recorded. Results. Only traces of the metabolites were found in CSF and in only two patients throughout the 24 hours. Both metabolites appeared rapidly (within 30 minutes) in plasma in all patients and were found in plasma throughout the study period. Morphine concentration peaked in CSF within 30 minutes at a very high level; in plasma, it peaked at 10 minutes. No correlation was seen between initial or later concentrations of morphine in CSF and postoperative pain or morphine requirements. Conclusions. No evidence of spinal metabolism of morphiiie could be found. Rapid distribution of morphine to CSF and plasma occurred after epidural administration. No value of initial CSF morphine concentra- tions for prediction of analgesic requirements could be demonstrated. Reg Anesth 1997: 22: 131-136. Key words: morphine, morphine-6-glucuronide, morphine-3-glucuronide, phar- macokinetics, epidural, cerebrospinal fluid.
From the Department of Anesthesiology, University Hospital, Link6ping, Sweden.
Presented in part at the 23rd Congress of the Scandinavian Society of Anaesthesiologists in Reykjavik, Iceland, June 12-16, 1995. Abstract published in Acta Anaesthesiol Scand 1995:39 (suppl 105): 115.
Supported in part by the Swedish Cancer Society (Grant no. 3127-B92-02xBB).
Accepted for publication July 24, 1996. Reprint requests: Sigga Kalman, Department of Anesthesiol-
ogy, University Hospital, S-581 85 Linkfping, Sweden.
The increased potency of epidurally adminis- tered as compared with systemically administered morphine has not been sufficiently demonstrated with other opioids (1). One explanation for this could be differences in lipophilicity between opoids. With the discovery of the active metabolite morphine-6-glucuronide (M6G), which is a more potent mu agonist than morphine itself (2-4), the question has arisen as to whe the r this active
131

132 Regional Anesthesia Vol. 22 No. 2 March-April 1997
metabolite contributes to analgesia by its presence in the cerebrospinal fluid (CSF) after epidural mor- phine administration and if so, whether it is formed by the metabolism of morphine in the cen- tral nervous system or elsewhere. The possibility of morphine metabolism in the central nervous sys- tem is suggested by results of studies on human brain in vitro (5) and by the finding of morphine metabolites in CSF after intracerebroventricular administration of morphine even though no meta- bolites of morphine were found in plasma (6). That morphine is metabolized in the liver and kidney seems reasonably well documented (7,8), but whether in vivo metabolization in the brain occurs seems uncertain. Mather has proposed that "if sig- nificant metabolism of morphine to analgesically active or antagonistic metabolites takes place on the brain side of the blood-brain barrier then many of the pharmacokinetic notions of morphine and its metabolites based upon plasma analysis really do need re-evaluation"(9).
The aim of this study was to describe the early pharmacokinetics of epidurally administered mor- phine, with special emphasis on the appearance of the glucuronated metabolites in CSF and plasma. At a later stage in the study, analgesia was supple- mented by systemically administered morphine to determine what influence this would have on con- centrations of metabolites in CSE
Materials and Methods
The investigation was approved by the Ethics Committee of the Faculty of Health Sciences, Uni- versity of Link6ping. Eight patients scheduled for major abdominal surgery, who were expected on clinical grounds to benefit from epidural analgesia in the postoperative period, gave their informed consent to participate.
men was chosen because it forms part of our clini- cal routine. Sampling of CSF and blood was per- formed at 10, 30, 60, and 120 minutes and 10 and 24 hours after the first epidural dose.
General anesthesia was induced at least 60 min- utes after administration of epidural morphine. For induction, fentanyl was given in a dose of 0.003 mg/kg, thiopental was given as required (range, 3.3-5.2 mg/kg), and intubation was facilitated by suxamethonium 1 mg/kg. Anesthesia was main- tained with isoflurane in 65% nitrous oxide, and additional doses of fentanyl were given when needed.
In the postoperative period patients were able to self-administer morphine intravenously 1-mg bolus doses, using a Deltec pump (Pharmacia, Uppsala, Sweden) with a lockout time of 6 minutes. The pump was started in the postoperative ward as soon as possible after arrival of the patient. Admin- istration of intravenous morphine started 2-10 hours after surgery. In the event of nausea or vom- iting, dixyrazin 5 mg (Esucos, UCB, Brussels, Bel- gium) was given intravenously. The pain was eval- uated on a visual analog scale (VAS) before the first patient-controlled injection of morphine and post- operatively at 10 and 24 hours. An additional dose of 4 mg morphine was given epidurally 12 hours after the first epidural injection.
After 24 Hours
On the following day, after completion of the protocol, the position of the catheter in the epidu- ral space was confirmed by injecting mepivacaine 20 mg/mL with epinephrine 5 ].tg/mL in a 5 mL bolus dose to ensure that sensory block was consis- tent with epidural placement of the catheter.
Analysis of Morphine and Metabolites
On the Day of Surgery
A radial artery cannula was inserted for use in blood sampling but also for monitoring blood pressure before, during, and after surgery. Ringer's acetate solution, 1,000 mL, was given intra- venously before introduction of a 16-gauge lumbar epidural catheter with a Tuohy needle by the loss of resistance technique.
A 16-gauge spinal catheter was placed one or two interspaces caudally with use of a 16-gauge Tuohy needle. The intent was to advance both catheters cranially in order to bring their tips to the same level. A uniform 4-rag dose of morphine was given to all patients, regardless of weight; this regi-
Blood samples were immediately centrifuged at 2,500 rpm for 10 minutes at 4~ Plasma was sepa- rated and frozen at -20~ and CSF was frozen. Morphine, M6G, and morphine-3-glucuronide (MBG) were analyzed by high-performance liquid chromatography (10); the lower limit of detection for the metabolites was 1 ng/mL (Department of Clinical Pharmacology, University Hospital, LinkSping).
Statistics
Since the study was exploratory, values are given as median and range. No statistical comparisons were made.

Possible Spinal Metabolism of Epidural Morphine * Kalman et al. 133
R e s u l t s
The patients included three w o m e n and five men, all American Society of Anesthesiologists 1 or 2, of mean age 39 years (range, 25-75 years). Serum creatinine and albumin concentrat ion were within normal limits in all patients. All patients were premedicated with oral f lunitrazepam in doses of 0.5-2 rag, according to the expected requirements in the individual patient. Table 1 lists demographic data, premedication, type of surgery, and total intravenous dose of morphine.
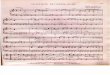
A single 4-mg dose of morphine given epidurally appeared very rapidly in the systemic circulation, as seen in Figure 1. The concentrat ion peaked within 10 minutes in all patients and had declined at 30 minutes. The metabolites M3G and M6G appeared in plasma as rapidly as the parent drug (Fig. 1), but whereas the morphine concentrat ion declined over the next 2 hours, the metabolites remained in plasma at a more constant level.
Tile concentrat ions of morphine in CSF are shown in Figure 1 for seven of the eight patients (one sample was lost). There are great interindi- vidual variations, but peak concentrat ions were reached rapidly in all patients. The CSF concentra- tion peaked at 10 minutes in the two patients with the highest CSF morphine levels, whereas it peaked at 30 minutes in the other patients. Interindividual variations in morphine concentra- tions were far greater for CSF than for plasma. Glucuronated metabolites were undetectable in CSF in all but two patients. These exceptions were patient 3, who had low concentrat ions of M6G at 2, 10, and 24 hours (2, 3, and 3 ng/mL, respec- tively) and patient 8, who showed similarly low values of M6G at tile same times (1, 2, and 1 ng/mL, respectively). The latter patient also showed M3G in the CSF at 2, 10, and 24 hours (70, 273, and 20 ng/mL, respectively). These two patients did not have the highest initial CSF con- centrations of morphine.
Table 1. Patient Demographics, Type of Surgery, and Total Intravenous Morphine Dose
Total Intravenous Dose Patient Age Height Weight of Morphine (mg) VAS (mm) VAS (mm) No. Sex (y) (cm) (kg) Type of Surgery Given by PCA Pump at 10 h at 24 h
1 F 43 166 57 Ptoctocolectomy, ileoanal pouch 16 70 82 2 M 75 169 75 Low anterior resection of the rectum 7 50 0 3 M 26 189 76 Proctocolectomy, ileoana] pouch 45 50 10 4 F 44 153 42 Proctocolectomy, ileoanal pouch 8 70 20 5 M 25 176 68 lleoanal pouch 14 40 17 6 M 27 178 110 Proctocolectomy, ileoana] pouch 136 20 20 7 F 26 163 63 Correction of ileostomy 9 67 46 8 M 47 178 88 Proctocolectomy, ileoanal pouch 23 60 45
PCA, patient-controlled analgesia; VAS, visual analog score.
Fig. I. Concentrations of nglml morphine in plasma and 10000
cerebrospinal fluid and of morphine-6-glucuronide and m o r p h i n e - 3 - g l u c u r o n i d e lOOO (ng/mL) in plasma at 10, 30, 60, and 120 minutes and 10 and 24 hours after epidural i 0 0 administration of 4 mg mor- phine (at time zero and at 12 hours). Starting time for the patient-controlled analgesic lO pump (PCA) is indicated. Values at 10 and 24 hours depend on a combination of 1 epidural and systemic mor- phine administration. Values arc means.
0 0.17 0.5 1 2 I 10 I 24 Hours
I i J 4 epidural morphine rng
PCA staded 4 mg epldural morp~hine
--O-- plasma morphine - E l - plasn'~ M6G - ~ - plasma M3G
�9 -<>- CSF morphine

134 Regional Anesthesia Vol. 22 No. 2 March-April 1997
Apart f rom the two epidural doses of morph ine (4 mg each), all patients also required fur ther anal- gesics via an in t ravenous pat ient-control led pump. Doses taken over the 24-hour s tudy varied widely (Table 1). Apart f rom one pat ient w h o remained on a venti lator owing to surgical complications and w h o received 136 mg of morph ine (as well as mida- zolam) during the study period, the doses of mor - phine still ranged f rom 7 to 45 mg (median, 14 mg).
No correlat ion was found be tween the 30- m inu t e concentra t ions of m orph i ne in CSF and the VAS score at e i ther 10 or 24 hours, no r was there any correlat ion with the postopera t ive morph ine r equ i remen t (Fig. 2).
Discussion Even though we found very high concentra t ions
of morph ine in the CSF, there were no signs of
metabo l i sm at the spinal level. We found only traces of the two morph ine metabol i tes in CSF and f rom only two patients. This absence of metaboli tes in CSF contrasts wi th the findings of bo th M3G and M6G in CSF after chronic adminis t ra t ion of oral (11,12), epidural (13), or subarachnoid (14) m o r p h i n e and implies that the increase in CSF concentra t ions of the metaboli tes is slow. A lack of metabol i sm to M3G (15,16) and M6G (17) has been repor ted after acute subarachnoid mo rp h in e administrat ion, however , Sandouk et al. (6) found metaboli tes in CSF 1 hou r after subarachnoid adminis t ra t ion of morph ine . The me thod of San- douk et al. for analyzing morph ine and metaboli tes was ra ther elaborate and was quite different f rom the me thod we used (h igh-per formance liquid ch roma tog raphy [ 10,18]), which makes compar i - son difficult. Our findings do not favor the hypo th - esis of a role for M6G in analgesia after acute spinal adminis t ra t ion of morph ine .
Table 2. Concentrations (mg/mL) of Morphine, Morphine-6-Glucuronide, and Morphine-3-Glucuronide in Plasma and Cerebrospinal Fluid
Time (h) After Epidural Administration 0.17 0.50 1 2 10 24
Morphine Plasma 34 (32-44) 20 (11-29) CSF 974 (331-10,474) 1544 (527-5,950
M6G Plasma 0 (0-12) 4 (0-20) csP o (o-o) o (o-o)
M3G Plasma 38 (0-114) 121 (73-140) CSF 0 (0-0) 0 (0-0)
11 (7-19) 5 (2-8) 36 (5-75) 9 (5-56) 1389 (290-3,829) 646 (180-2,311) 70 (37-1,113) 23 (0-69)
7 (0-16) 4 (0-11) 17 (0-48) 6 (0-62) 0 (0-0) 0 (0-2) 0 (0-3) 0 (0-3)
135 (76-164) 92 (59-117) 156 (84-290) 122 (75-182) 0 (0-0) 0 (0-70) 0 (0-273) 0 (0-20)
Values are given as median and range. M6G, morphine-6-glucuronide; M3G, morphine-3-glucuronide; CSF, cerebrospinal fluid.
Fig. 2. Correlation of concentration of morphine (ng/mL) in cerebrospinal fluid 30 minutes after epidu- ral administration of 4 mg morphine with postoperative morphine demand in mil- ligrams per kilogram of body weight (n = 7).
Postoperative morphine mg / kg
1,4 t 1,2 o
1
,8
, 6 o
,4
'2 i 0
0
o
o
o
o
i . . . . i . . . . i . . . . i ,
1000 2000 3000 4000 �9 " i . . . . i . . . . i
5000 6000 7000 Morphine ng / ml

Possible Spinal Metabolism of Epidural Morphine �9 Kalman et al. 135
The rapid passage of epidural morphine to the CSF was an unexpected finding, because pharma- codynamic studies have shown a late onset of anal- gesia (19). This rapid passage was previously demonstrated by Drost et al. (20), who found mor- phine in CSF after 2 minutes and peak values after 40 minutes. One plausible explanation for the rapid passage to CSF as found by us and by Drost et al. could be our common technique, which includes dural puncture (placing the CSF sampling catheter) before administration of morphine, ht vitro studies have indicated that the passage through the dura may be enhanced by puncture of this tissue (21). We used a technique in which tile hole in the meningeal tissue was plugged with an epidural catheter, left in place throughout the study, which should at least decrease the leakage. The concentrations of morphine found in CSF were high and as found previously, were 40-200 times those in plasma (22,23).
The difference in results regarding the occur- rence of metabolites in CSF could be explained by differences in the duration of morphine adminis- tration (acute or chronic). Plasma concentrations of the metabolites are quite high and were to some extent maintained over time (Fig. 1). The concen- tration gradient across the blood-brain barrier should favor transport of metabolite. Diffusion of a drug across the blood-brain barrier is dependent on the concentration gradient from plasma to brain of the unbound fraction and on lipid solubility, degree of ionization, pH, molecular conformation, and molecular size. A net extraction of morphine from plasma to the brain has been demonstrated in sheep (7). Active transport ht vitro by chorionic villi is recognized for morphine (24) but to our knowl- edge has not been identified for the metabolites. The pH of CSF is a little lower than that of blood. The pH could perhaps change the configuration of the metabolites by changing polarity or may cause trapping of metabolites in the CSF and result in increasing concentrations of metabolites in CSF with time. Recent reports suggest that the metabo- lites exist i n conformational equilibrium between extended and folded forms, depending on whether the medium is of high or low polarity (25). The folded form produces a less polar molecule, which should favor transport over membranes (a medium of low polarity). The molecular weight of mor- phine is 285.33, in contrast to those of M6G, which is 497.5, and M3G, which is 461.5, indicating slower transport for the metabolites.
Rapid passage to the systemic circulation after epidural administration of morphine has been reported in studies in which plasma levels of morphine were equivalent to concentrations
reached after a similar intramuscular injection of morphine (19,26).
The position of the epidural catheter was checked after 24 hours by injecting a small dose of local analgesic, which resulted in adequate sen- sory block. The response to the local analgesic test dose has proved to be a useful predictor of effec- tive epidural opioid analgesia (27) and indicates that the positioning of the epidural cathether was adequate. We did not confirm the position of the subarachnoid catheter by roentgenography. Part of the interpatient variability in CSF morphine levels could be explained by variability in the dis- tance of the CSF sampling site from the epidural catheter tip.
No correlation was found between initial con- centrations of morphine in CSF and postoperative morphine requirements. These results are consis- tent with findings during chronic administration of morphine (13).
Even though we found very high concentrations of morphine in CSF, there were no signs of metabolism at the spinal level. The passage of the morphine metabolites M6G and M3G into the CSF is relatively slow. These results suggest that neither subarachnoid formation of M6G nor transport of M6G across the blood-brain barrier contributes to the potency or duration of analgesia produced by acute epidural administration of morphine.
Acknowledgments
The authors thank Gunilla Graffner.for skillful analysis and Professor ,&ke Bertler for valuable dis- cussions and comments on the manuscript.
References
1. Geller E, Chrubasik J, Graf R, Chrubasik S, Schulte- M6nting J. A randomized double-blind compari- son of epidural sufentanil versus intravenous sufentani] or epidural fentanyl analgesia after major abdominal surgery. Anesth Analg 1993: 76: 1243-1250.
2. Pasternak GW, Bodnar R J, Clark JA, Inturrisi CE. Morphine-6-glucuronide, a potent mu agonist. Life Sci 1987: 41: 2845-2849.
3. Paul D, Standifer KM, Inturrisi CE, Pasternak GW. Pharmacological characterization of morphine-6- glucuronide, a very potent morphine metabolite. J Pharmacol Exp Ther 1989: 251: 477-483.
4. Shimomura K, Kamata O, Ueki S, Ida S, Oguri K, Yoshimura H, Tsukamoto H. Analgesic effect of morphine glucuronides. Tohuku J Exp Med 1971: 105: 45-52.

136 Regional Anesthesia Vol. 22 No. 2 March-April 1997
5. Wahlstr6m A, Winblad B, Bixo M, Rane A. Human brain metabolism of morphine and naloxone. Pain 1988: 35: 121-127.
6. Sandouk P, Serfie A, Scherrmann JM, Langlade A. Bourre riM. Presence of morphine metabolites in human cerebrospinal fluid after intracerebroven- tricular administration of morphine. Eur J Drug Metab Pharmacokinet 1991: Special No 3: 166-171.
7. Sloan PA, Mather LE, McLean CF, Rutten AJ, Nation RL, Milne RW, Runciman WB, Somogyi AA. Phys- iological disposition of Lv. morphine in sbeep. Br J Anaesth 1991: 67: 378-386.
8. Milne RW, Sloan PA, McLean CF, Mather LE, Nation RL, Runciman WB, Rutten A J, Somogyi AA. Dis- position of morphine and its 3- and 6-glucuronide metabolites during morphine infusion in the sheep. Drug Metab Dispos 1993: 21:1151-1156.
9. Mather LE. The clinical effects of morphine pharma- cology. Reg Anesth 1995: 20: 263-282.
10. Svensson JO. Determination of morphine, mor- phine-6-glucuronide and normorphine in plasma and urine with high-performance liquid chro- matography and electrochemical detection. J Chromatog 1986: 75: 174-178.
11. D'Honneur G, Gilton A, Sandouk P, Scherrmann JM, Duvaldestin P. Plasma and cerebrospinal fluid concentrations of morphine and morphine glu- curonides after oral morphine. Anesthesiology 1994: 81: 87-93.
12. Wolff T, Samuelsson H, Hedner T. Morphine and morphine metabolite concentrations in cere- brospinal fluid and plasma in cancer pain patients after slow-release oral morphine administration. Pain 1995: 62: 147-154.
13. Samuelsson H, Hedner T, Venn R, Michalkiewicz A. CSF and plasma concentrations of morphine and morphine glucuronides in cancer patients receiv- ing epidural morphine. Pain 1993: 52: 179-185.
14. Bigler D, Broen Christensen C, Eriksen J, Jensen N- H. Morphine, morphine-6-glucuronide and mor- phine-3-glucuronide concentrations in plasma and cerebrospinal fluid during long-term high- dose intrathecal morphine administration. Pain 1990: 41: 15-18.
15. Ionescu TI, Drost RH, Roelofs JMM, Winckers EKA, Taverne RHT, van Marls AA, van Rossum JM. The pharmacokinetics of intradural morphine in major abdominal surgery. Clinic Pharmacokinet 1988: 14: 178-186.
16. Caute B, Monsarrat B, Gouardhres C, Verdie JC, Lazorthes Y, Cros J, Bastide R. CSF morphine lev-
els after lumbar intrathecal administration of iso- baric and hyperbaric solutions for cancer pain. Pain 1988: 32: 141-146.
17. Hanna MH, Peat S J, Woodham M, Knibb A, Fung C. Analgesic efficacy and CSF pharmacokinelics of intrathecal morphine-6-glucuronide: Compari- son with morphine. Br J Anaesth 1990: 64: 547-550.
18. Svensson JO, Rane A, S~iwe J, Sj6qvist F. Determina- tion of morphifie, morphine-3-glucuronide and (tentatively) morpbine-6-glucuronide in plasma and urine using ion-pair high-performance liquid chromatography. J Chromatog 1982: 230: 427-432.
19. Rawal N, Sj6strand U, Dahlstr6m B. Postoperative pain relief by epidural morphine. Anesth Analg 1981: 60: 726-731.
20. Drost RH, Ionescu TI, Taveme RHT, van Lingen G, van Rossum JM, Maes RAA. Pharmacokinetics of morphine in cerebrospinal fluid and plasma after epidural administration in man. Arzneimit- telforschung 1988: 38: 1632-1634.
21. Bernards CM, Kopacz D J, Michel MZ. Effect of nee- dle puncture on morphine and lidocaine flux through the spinal meninges of the monkey in vitro. Implications for combined spinal-epidural anesthesia. Anesthesiology 1994: 80: 853-858.
22. Gustafsson LL, Grell AM, Garle M, Rane A, Schildt B. Kinetics of morphine in cerebrospinal fluid alter epidural administration. Acta Anaesthesiol Scand 1984: 28: 535-539.
23. J6rgensen BC, Andersen HB, Engquist A. CSF and plasma morphine after epidural and intrathecal application. Anesthesiology 1981: 55:714-715.
24. Takemori AE, Stenwick MW. Studies on the uptake of morphine by the choroid plexus hl vitro. J Phar- macol Exp Ther 1966:154: 586-594.
25. Carrupt P-A, Testa B, Bechalany A, El Tayar N, Descas P, Perrissoud D. Morphine 6-glucuronide and morphine 3-glucuronide as molecular chameleons with unexpected lipophilicity. J Med Chem 1991: 34: 1272-1275.
26. Nordberg G, Hedner 1", Mellstrand T, Borg L. Phar- macokinetics of epidural morphine in man. Eur J Clin Pharmacol 1984: 26: 233-237.
27. Weitz S, Drasner K. Local anesthetic test dose as a predictor of effective epidural opioid analgesia. Anesthesiology 1995: 83: 96-100.
28. Standl T, Beck H. Radiological examination of the intrathecaI position of microcatheters in continu- ous spinal anaesthesia. Br J Anaesth 1993: 71: 803-806.