-
MOPEDS: Motorized Objects PropellingEthanol Drinking SubjectsA.
BRITTON CHRISTMAS, M.D., RITA A. BRINTZENHOFF, M.D., THOMAS M.
SCHMELZER, M.D.,KAREN E. HEAD, R.N., B.S.N., RONALD F. SING,
D.O.
From the F.H. "Sammy" Ross, Jr. Trauma Center, Department of
Surgery,Carolinas Medical Center, Charlotte, North Carolina
Mopeds are not subject to the same laws and jurisdiction as cars
or motorcycles, including therequirement of a driver's license. We
undertook this study to examine the influence of alcohol(ETOH) on
moped crashes. We retrospectively reviewed adult moped injuries
compared withmotor vehicle crashes (MVCs) and motorcycle crashes
(MCCs) from 1995 through 2006. De-mographics, severity of injury,
mortality, and serum ETOH levels were recorded. Data were an-alyzed
using tbe Student f test for continuous data and the x^ test for
proportional data. Motorvehicle crashes accounted for 7186
admissions. MCC and moped crashes numbered 973 and
113,respectively. Although not statistically significant (P =
0.064), moped crashes yielded the highestmortality (9.7%) compared
with MCCs (8.5%) and MVCs (6.7%). An increased association of
bloodETOH levels witb moped crashes, however, was statistically
significant (P = 0.004). Serum ETOHlevels above 0.05 g/dL were
observed in 1681 MVCs (23.4%), 241 MCCs (24.8%), and 44
mopedcrashes (39%). In tbis study, we discovered tbat moped crashes
demonstrate a significantly higherETOH involvement than either MVCs
or MCCs representing a previously unrecognized publicsafety
risk.
T HE POTENTIAL INFLUENCE of alcohol intoxication ontrauma,
including homicide, assault, and motorvehiele eollisions. has been
well doeumented. In the1997 National Highway Traffie Safety
Administra-tion's (NHTSA) Current Research in Alcohol, it
wasestimated that half of all trauma admissions to U.S.hospitals
involved patients who were injured whileunder the influence of
alcohol.' Speeifieally in 2007,the NHTSA reported that 32 per eent
of all motor ve-hicle collision fatalities, 12,998 deaths, were the
resultof aleohol-intoxieated drivers with a blood
aleoholeoneentration (BAC) of 0.08 g/dL or higher.- The per-centage
of alcohol-related injuries specific to motorcy-cle collisions has
also been doeumented. Soderstromand eoUeagues-* reported in 1993
that 53 per eent ofinjured motorcycle drivers exhibited positive
BAC.
Reeently, we identified another group of intoxieateddrivers that
have yet to be studied: moped drivers.Mopeds are a class of
motorized vehieles with a de-fined engine eapaeity of less than 50
em"' that may notexeeed a speed of 30 miles per hour. Moped
operator
Presented at the 2008 annual meeting of the American Collegeof
Surgeons, October 12-16. 2008, San Francisco, CA.
Address correspondence and reprint requests to A.
BrittonChristmas, M.D.. Department of Surgery, Carolinas
MedicalCenter. P.O. Box 32861, Charlotte, NC 28232. E-mail:
[email protected].
requirements and lieensing laws eurrently vary amongthe states.
Furthermore, in many states, an individualean legally obtain a
moped lieense even if his or herdriver's lieense has been
previously suspended or re-voked. For this reason, these drivers
represent a sub-stantial potential publie safety risk. We undertook
thisstudy to assess the association between moped colli-sions and
drivers' positive serum ethanol levels com-pared with automobile
and motorcycle eollisions.
Methods
We retrospeetively reviewed the reeords of patientsinjured by
motor vehiele eollisions from 1995 to 2006as identified by the
Carolinas Medieal Center traumaregistry database. Carolinas Medieal
Center is a re-gional Level I trauma eenter serving an area of
6147square miles and a population of over three millionresidents of
North Carolina and South Carolina. Dataeolleetion ineluded patient
demographies. Injury Se-verity Seore (ISS), mortality rates, and
serum ethanollevels of all patients admitted to the trauma
servieeafter motor vehicle collisions. These eollisions
wereeategorized as automobile, motoreyele, or moped. Bloodaleohol
eoneentration testing was measured at the timeof presentation for
all persons involved in motor vehieleerashes in eonjunetion with
North Carolina state law. Forthis study, a positive serum ethanol
test was deñned as
304
-
No. 3 MOPEDS
BAC greater than 0.05 g/dL. Data were analyzed usingthe Student
/ test for continuous data and the x" test forproportional data.
Results were considered significant atP < 0.05.
Results
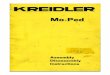
From 1995 through 2006, there were 8272 admissionsfor injuries
caused by motor vehicle collisions. Motorvehicle crashes involving
automobiles or trucks (MVCs)accounted for 7186 admissions (87%),
and motorcyclecrashes (MCCs) and moped crashes (MOPED) num-bered
973 ( 12%) and 113 ( 1 %), respectively (Fig. 1 ). Asexpected, the
mean ISS was slightly lower for MVCs(13.7) compared with MCCs
(16.3) and MOPED (15.8).However, these differences were not
statistically differ-ent. Mortality among the groups was also
similar with6.7 per cent MVCs, 8.5 per cent MCCs, and 9.7 percent
MOPED. Interestingly, alcohol intoxication rates,defined as serum
ethyl alcohol levels greater than 0.05g/dL, varied significantly
among the groups. Although23.4 per cent of automobile/truck
operators and 24.5per cent of motorcycle operators were
intoxicated, 39per cent of moped operators were intoxicated (P
=0.0004) (Table 1 ).
We further compared the motorcycle and mopedgroups. Although
both groups exhibited similar Glas-gow Coma Scale scores, hospital
length of stay, andintensive care unit length of stay, significant
differ-ences were observed with respect to age and BAC.Moped riders
were significantly older (45 ± 14 years)than their motorcycle
counterparts (37 ± 12 years). Asubanalysis of intoxicated riders
demonstrated a sig-nificantly higher BAC in the moped group (0.185
±0.096 g/dL) compared with the motorcycle group(0.122 ± 0.090 g/dL)
(Table 2).
Discussion
The relationship between alcohol use, injuries, andfatalities
after motor vehicle collisions has been welldocumented.'"^ Many
laws have been enacted to protectdrivers and pedestrians from
intoxicated motor vehicleoperators, including convictions for
driving under theinfluence (DUI) with BAC of greater than 0.08
g/dL,license suspension, and eventual license revocation forrepeat
offenders. These laws, however, seldom apply tomoped operators. In
many states, an individual can le-gally obtain a moped license
irrespective of the status ofhis or her driver's license. Some
states do not requirea license at all. As such, repeat offenders
whose drivers'licenses have been suspended or revoked can
continueto operate these motorized vehicles.
In 2(X)6, the NHTSA deinonstrated that drivers witha BAC greater
than 0.08 g/dL involved in a fatal collision
Christmas et al.
Motor Vehicle Collision Admissions N= 8272
305
0 AUTO 87%
• MCC1296
D MOPED 196
Fro. 1. Motor vehicle collision admissions, 1995 to 2006.Auto,
automobile/truck crash. MCC, motor cycle crash. MOPED,moped
crash.
TABLE I. Comparison of Injury Severity, Mortality, andAlcohol
Intoxication by Category of Collision
Automobile Motorcycle Moped F Value
Injury SeverityScore
MortalityAlcohol
intoxication
13.7
6.7%23.4%
16.3
8.5%24.8%
15.8
9.7%39%
0.064O.(X)O4*
* P < 0.05 comparing automobile and motorcycle withmoped.
TABLE 2.Drivers
Comparison between Moped and Motorcycle
MotorcycleMean (SD)
MopedMean (SD) P Value
AgeGCSH LOSICU LOSBAC
37(12)12(5)10(12)6(8)
0.122(0.090)
45 (14)12(5)12(17)6(9)
0.185(0.096)
-
306 THE AMERICAN SURGEON March 2011 Vol. 77
therefore, deereased mortality in the moped groupbeeause, by
definition, these vehicles cannot achievespeeds greater than 30
miles per hour. Although theISS was similar between groups, the
moped group wassignificantly older than the motorcycle group.
Fur-thermore, when the effects of alcohol are introdueed.many
plausible explanadons arise. It is well docu-mented that alcohol
use is associated with deereasedinhibitions and. subsequently, many
other risk faetorsfor injury.̂ Prior studies have shown that
intoxicatedmotoreyelists are much less likely to wear helmets
thansober riders.**- '^ Furthermore, House and
colleagues'°demonstrated that intoxicated drivers are more likelyto
drive at higher speeds and in more hazardous eir-eumstances than
sober drivers. These findings, in com-bination with the impaired
psyehomotor effeets of al-eohol, eould certainly account for the
trend towardinereased mortality in this population.
Although DUI laws have become more stringent,some authors
estimate that only three to five arrests areactually made for every
1000 DUI episodes. ' ' Of greateoneern is that for those who are
ultimately arrestedand convieted, mopeds offer an alternative mode
oftransportation with fewer restrictions and
regulations.Furthermore, the BAC of moped drivers is
significantlyhigher than motorcycle drivers. The ability to
remainconscious with a BAC approaehing 0.200 g/dL impliesprior
development of high aleohol tolerance, depen-deney, and likely
reeidivism.'- Because there are cur-rently no laws in effeet to
prevent potential recidivistsfrom operating mopeds. they will
likely continue to doso until either severe injury or behavior
modificationoccurs. Similar to Li and colleagues,^ we reiterate
thatdrinking behavior persists across activity domains.
Theassociation, therefore, is less likely to be a causai
re-lationship and is more likely the result of
behaviorpatterns.
As in any elinieal study, our study has several lim-itations.
First, this is a single-institutional study thathas not been
subjected to muld-institutional analysis.Seeond. we acknowledge
potendal deficiencies in anytrauma registry database. We recognize
that data entryis subject to human error and potendal omissions. It
isalso possible that the BACs reeorded in our registrymay aetually
be lower than the BACs at the time ofinjury. We recognize that
potential delays, particularlyfor patients transferred from
regional facilities, allowmore time for metabolism and,
subsequently, mayyield lower BACs. Furthermore, in this
retrospectivestudy, we have no way to verify that every patient
un-derwent BAC testing at the time of arrival. At present.
we do not have license suspension or revoeadon data onthe moped
drivers idendfied in this study.
Conclusion
In this study, we diseovered a greater associationbetween moped
collisions and positive serum ethanollevels eompared with
automobile and motorcycle eol-lisions. Although we strongly suspeet
that many of theseriders are drunk driving recidivists, we do not
havelicense suspension data. The next step in studying thispublie
health issue is to obtain reeords from the De-partment of Motor
Vehicles to confirm the nationwidetrends of DUI recidivism in moped
operators. With thisinformation, we hope to gain support in our
effort torevise current moped laws and to close a potentialloophole
for DUI recidivists.
REFERENCES
1. National Highway Traffic Safety Administration.
Currentresearch in alcohol. Ann Emerg Med 1997:30:817-9.
2. National Highway Traffic Safety Administration. US
De-partment of Transportation. Traffic Safety Facts: 2(X)8
Data.Washington. DC: National Highway Traffic Safety
Administration;2008.
3. Soderstrom CA, Dischinger PC, Ho SM. Soderstrom MT.Alcohol
use, driving records, and crash culpability among injuredmotorcycle
drivers. Accid Anal Prev 1993:25:711-6.
4. Zador P. Alcohol-related relative risk of fatal driver
injuriesin relation to driver age and sex. J Stud Alcohol
1991:52:302-10.
5. Hingson R, Heeren T, Winter M. Lowering state legal
alcohollimits to 0.08%: the effect on fatal motor vehicle crashes.
Am JPublic Health 1996;86:1297-9.
6. Ricci G, Majori S, Mantovani W, et al. Prevalence of
alcoholand drugs in urine of patients involved in road accidents. J
PrevMed Hyg 2008 ;49:89-95.
7. Li G, Shahpar C, Soderstrom CA. Baker SP. Alcohol use
inrelation to driving records among injured bicyclists. Accid
AnalPrev 2000:32:583-7.
8. Luna GK, Maier RV. Sowder L. et al. The influence of eth-anol
intoxication on outcome of injured motorcyclists. J
Trauma1984:24:695-700.
9. Shankar BS, Ramzy AI, Soderstrom CA, et al. Helmet
use,patterns of injury, medical outcome, and costs among
motorcycledrivers in Maryland. Accid Anal Prev 1992:24:38.5-96.
10. House EG, Waller PF, Stewart JR. Blood alcohol level
andinjury traffic crashes. Proceedings of American Association
forAutomotive Medicine. 1982;26:349-73.
11. Hingson R, Howland J, Heeren T, et al. Effects of
legalpenalty changes and laws to increase drunken driving
convictionson fatal accident crashes. Bull N Y Acad Med
1988:64:662-7.
12. Runge JW, Pulliam CL. Carter JM, Thomason MH. En-forcement
of drunken driving laws in cases involving injuredintoxicated
drivers. Ann Med 1996:27:66-72.
-
Copyright of American Surgeon is the property of Southeastern
Surgical Congress and its content may not be
copied or emailed to multiple sites or posted to a listserv
without the copyright holder's express written
permission. However, users may print, download, or email
articles for individual use.