Embed Size (px)
Citation preview
September 2016
Monthly Infectious Diseases
Surveillance Report
Volume 5, Issue 9
The Monthly Infectious Diseases Surveillance Report is produced by Public Health Ontario (PHO) for the
public health community of Ontario. We welcome feedback by email to: [email protected]. Past issues
and additional information are available online.
In Focus ........................................................................................................................ 2
Significant Reportable Disease Activity .......................................................................... 7
Appendix – Reportable Diseases .................................................................................. 10

Monthly Infectious Diseases Surveillance Report Page 2 of 12
IN FOCUS
Carbapenemase-producing Enterobacteriaceae
Carbapenemase-producing Enterobacteriaceae (CPE) is a gram-negative bacterium that produces an
enzyme capable of breaking down a whole class of beta-lactam agents, including carbapenems, that are
considered last-resort antibiotics.1 Its antibiotic resistance, association with high mortality rates, and
potential to spread rapidly from one location to another make CPE a significant public health concern
worldwide.2 CPE produces different types of carbapenemase enzymes, such as Klebsiella pneumoniae
carbapenemase (KPC), New Delhi metallo-β-lactamase-1 (NDM-1), Verona integron-encoded metallo-β-
lactamase (VIM), and oxacillinase (OXA). Since the KPC producer was first discovered in 1996, CPEs have
spread throughout the world. Endemic areas have been identified, including KPC producers in the
United States, Greece, and Israel; NDM producers in the Indian subcontinent; VIM producers in Greece
and Italy; and OXA producers in North Africa and Turkey.3
CPEs are primarily found in health care settings and as a result, receiving health care in countries where
CPE is endemic is a major risk factor for colonization and/or infection with CPE. CPE can be spread from
person to person, or through contact with contaminated surfaces such as door handles, chairs, and
medical equipment. Recently, acquisition of CPE has also been associated with the use of contaminated
endoscopic retrograde cholangiopancreatography, or ERCP—a procedure used to study the bile ducts,
pancreatic duct, and gallbladder.4,5 It affects patients, residents, and health care workers and can cause
various infections including pneumonia and bloodstream infection. Symptoms of CPE infections may
include fever and chills. In the laboratory, CPE is detected initially by observing increased minimum
inhibitory concentration (MIC) to carbapenems and the presence of carbapenemase genes is confirmed
using PCR testing. Treatment of CPE infections is difficult as currently available antibiotics are not highly
effective. Therefore, prevention and control of CPE is a priority.
Nomenclature
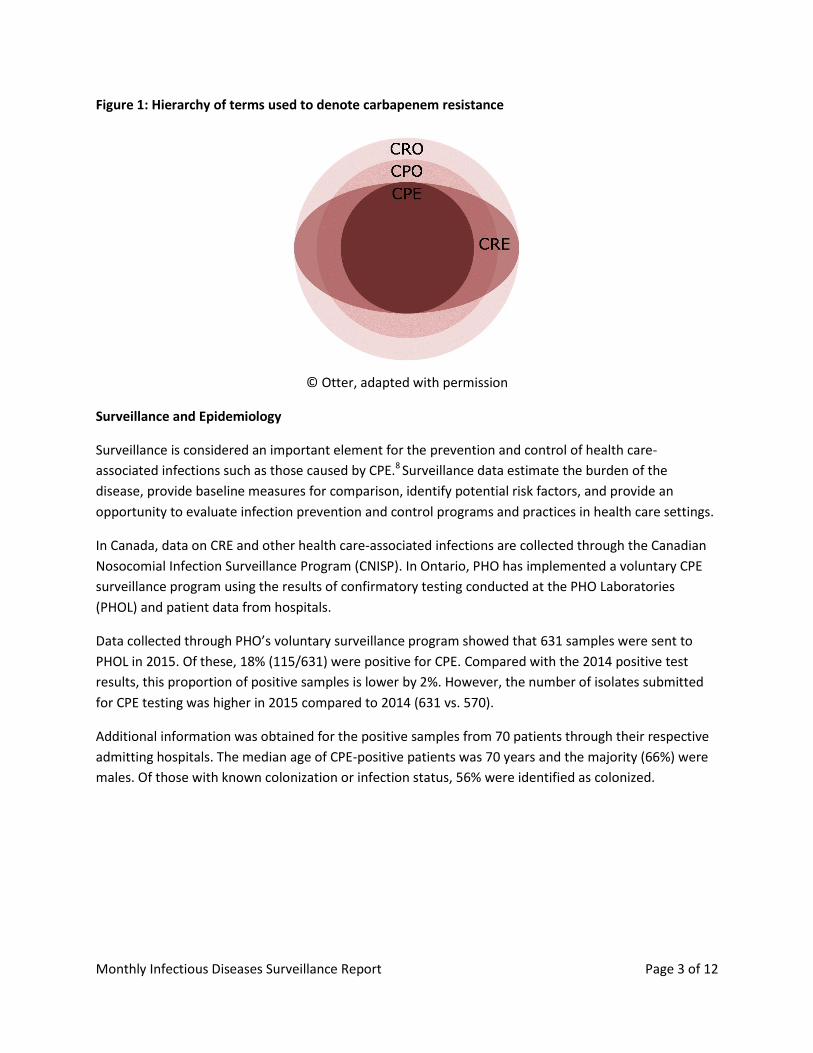
CPE is often confused with carbapenem-resistant Enterobacteriaceae (CRE), carbapenemase-producing
organism (CPO), and carbapenem-resistant organism (CRO). Bacteria that are resistant to carbapenems
are collectively known as CROs. Among the CROs, those that produce carbapenemase are termed CPOs.
CPOs that belong to the Enterobacteriaceae family are also known as CPE. The terms CRE and CPE are
often used interchangeably but, in fact, these bacteria differ in terms of resistant mechanisms. CRE may
be resistant to carbapenem by producing extended-spectrum beta-lactamase (ESBL) or AmpC beta-
lactamase, together with the loss of porins, or by acquiring the genes to produce carbapenemase. The
latter applies to CPE’s mechanism of resistance.6,7 Public Health Ontario (PHO) uses CPE to denote the
organism group (i.e., Enterobacteriaceae) and mechanism of resistance (i.e., acquired carbapenemase).
Although all antibiotic resistant organisms are concerning, CPE receives particularly greater attention as
carbapenemase genes found in these organisms are able to easily move from one species to another,
thus having a much higher potential to spread. Figure 1 provides a visual representation of the hierarchy
of terms.
Monthly Infectious Diseases Surveillance Report Page 3 of 12
Figure 1: Hierarchy of terms used to denote carbapenem resistance
© Otter, adapted with permission
Surveillance and Epidemiology
Surveillance is considered an important element for the prevention and control of health care-
associated infections such as those caused by CPE.8 Surveillance data estimate the burden of the
disease, provide baseline measures for comparison, identify potential risk factors, and provide an
opportunity to evaluate infection prevention and control programs and practices in health care settings.
In Canada, data on CRE and other health care-associated infections are collected through the Canadian
Nosocomial Infection Surveillance Program (CNISP). In Ontario, PHO has implemented a voluntary CPE
surveillance program using the results of confirmatory testing conducted at the PHO Laboratories
(PHOL) and patient data from hospitals.
Data collected through PHO’s voluntary surveillance program showed that 631 samples were sent to
PHOL in 2015. Of these, 18% (115/631) were positive for CPE. Compared with the 2014 positive test
results, this proportion of positive samples is lower by 2%. However, the number of isolates submitted
for CPE testing was higher in 2015 compared to 2014 (631 vs. 570).
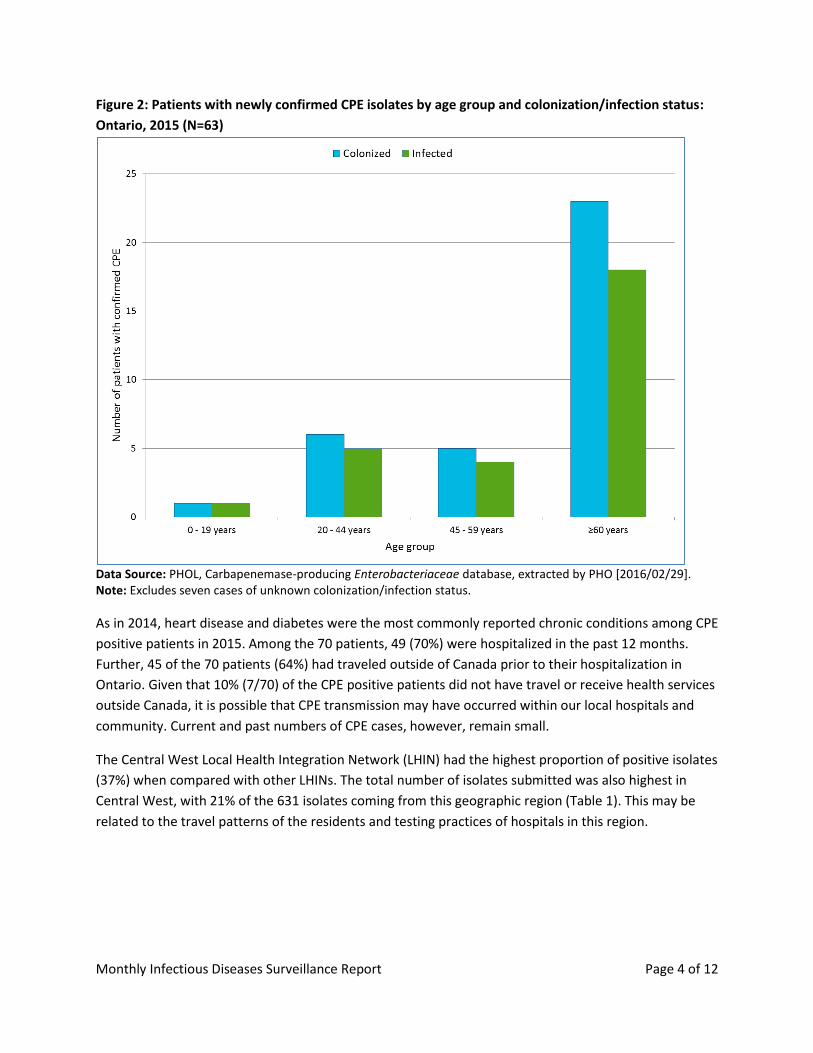
Additional information was obtained for the positive samples from 70 patients through their respective
admitting hospitals. The median age of CPE-positive patients was 70 years and the majority (66%) were
males. Of those with known colonization or infection status, 56% were identified as colonized.
Monthly Infectious Diseases Surveillance Report Page 4 of 12
Figure 2: Patients with newly confirmed CPE isolates by age group and colonization/infection status:
Ontario, 2015 (N=63)
Data Source: PHOL, Carbapenemase-producing Enterobacteriaceae database, extracted by PHO [2016/02/29]. Note: Excludes seven cases of unknown colonization/infection status.
As in 2014, heart disease and diabetes were the most commonly reported chronic conditions among CPE
positive patients in 2015. Among the 70 patients, 49 (70%) were hospitalized in the past 12 months.
Further, 45 of the 70 patients (64%) had traveled outside of Canada prior to their hospitalization in
Ontario. Given that 10% (7/70) of the CPE positive patients did not have travel or receive health services
outside Canada, it is possible that CPE transmission may have occurred within our local hospitals and
community. Current and past numbers of CPE cases, however, remain small.
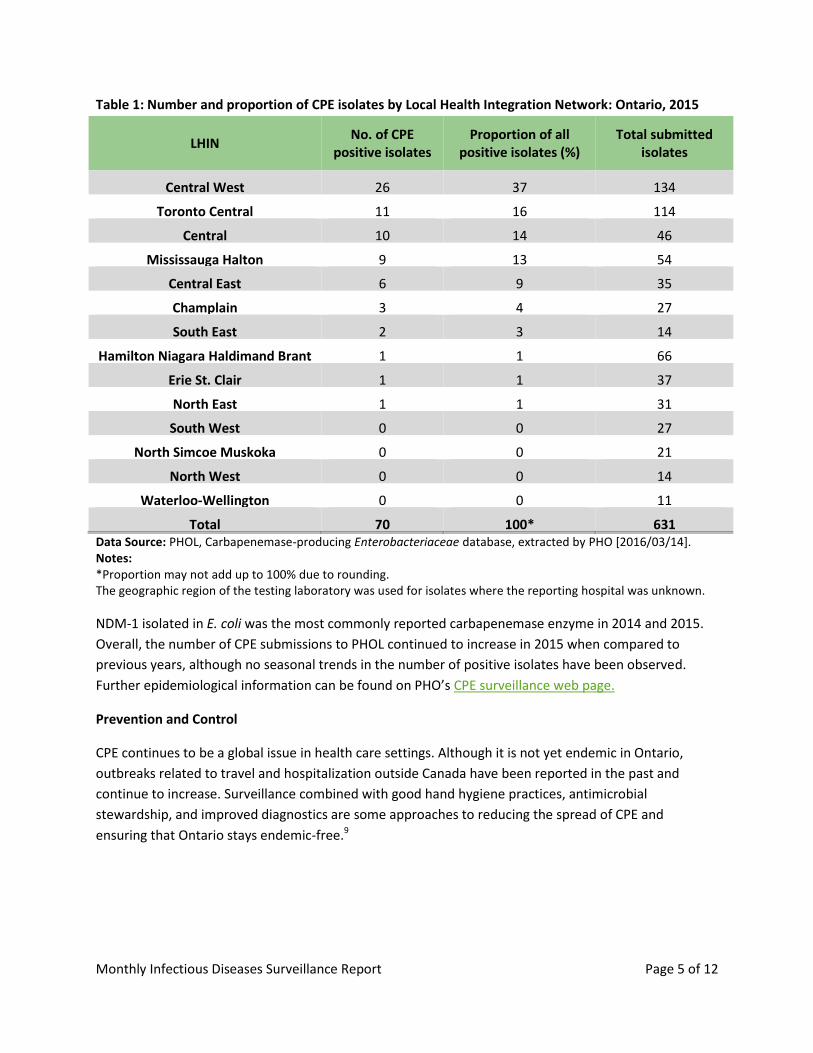
The Central West Local Health Integration Network (LHIN) had the highest proportion of positive isolates
(37%) when compared with other LHINs. The total number of isolates submitted was also highest in
Central West, with 21% of the 631 isolates coming from this geographic region (Table 1). This may be
related to the travel patterns of the residents and testing practices of hospitals in this region.
Monthly Infectious Diseases Surveillance Report Page 5 of 12
Table 1: Number and proportion of CPE isolates by Local Health Integration Network: Ontario, 2015
LHIN No. of CPE
positive isolates Proportion of all
positive isolates (%) Total submitted
isolates
Central West 26 37 134
Toronto Central 11 16 114
Central 10 14 46
Mississauga Halton 9 13 54
Central East 6 9 35
Champlain 3 4 27
South East 2 3 14
Hamilton Niagara Haldimand Brant 1 1 66
Erie St. Clair 1 1 37
North East 1 1 31
South West 0 0 27
North Simcoe Muskoka 0 0 21
North West 0 0 14
Waterloo-Wellington 0 0 11
Total 70 100* 631 Data Source: PHOL, Carbapenemase-producing Enterobacteriaceae database, extracted by PHO [2016/03/14]. Notes: *Proportion may not add up to 100% due to rounding. The geographic region of the testing laboratory was used for isolates where the reporting hospital was unknown.
NDM-1 isolated in E. coli was the most commonly reported carbapenemase enzyme in 2014 and 2015.
Overall, the number of CPE submissions to PHOL continued to increase in 2015 when compared to
previous years, although no seasonal trends in the number of positive isolates have been observed.
Further epidemiological information can be found on PHO’s CPE surveillance web page.
Prevention and Control
CPE continues to be a global issue in health care settings. Although it is not yet endemic in Ontario,
outbreaks related to travel and hospitalization outside Canada have been reported in the past and
continue to increase. Surveillance combined with good hand hygiene practices, antimicrobial
stewardship, and improved diagnostics are some approaches to reducing the spread of CPE and
ensuring that Ontario stays endemic-free.9
Monthly Infectious Diseases Surveillance Report Page 6 of 12
References:
1. Eshetie S, Unakal C, Gelaw A, Ayelign B, Endris M, Moges F. Multidrug resistant and
carbapenemase producing Enterobacteriaceae among patients with urinary tract infection at
referral Hospital, Northwest Ethiopia. Antimicrobial Resistance and Infection Control. 2015;4:12.
Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4407313
2. Lyman M, Walters M, Lonsway D, Rasheed K, Limbago B, Kallen A. Notes from the field:
Carbapenem-resistant Enterobacteriaceae Producing OXA-48-like Carbapenemases — United
States, 2010–2015. Morbidity and Mortality Weekly Report. 2015;64(47);1315-6. Available from:
https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6447a3.htm. Erratum in: Morbidity and
Mortality Weekly Report. 2015; 64(48);1350. Available from:
https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6448a6.htm
3. Nordman P, Gniadkowski M, Giske CG, Poirel L, Woodford N, Miriagou V et al. Identification and
screening of carbapenemase-producing Enterobacteriaceae. Clinical Microbiology and Infection.
2012;18:432-8.
4. Kola A, Piening B, Pape U-F, et al. An outbreak of carbapenem-resistant OXA-48-producing
Klebsiella pneumonia associated to duodenoscopy. Antimicrobial Resistance and Infection
Control. 2015;4:8. doi:10.1186/s13756-015-0049-4. Available from:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4374528
5. Newson L. Patient: ERCP. [Internet]. Leeds, UK: EMIS Group; 2016. Available from:
http://patient.info/health/ercp
6. Otter J. Do you know your CRO from your CPO from your CRE from your CPE? 2013; Jul 13. In:
Reflections on Infection Prevention and Control blog [Internet]. Available from:
https://reflectionsipc.com/2013/07/24/do-you-know-your-cro-from-your-cpo-from-your-cre-
from-your-cpe/
7. Wong T. Carbapenem resistant Enterobacteriaceae: epidemiology, clinical impact and laboratory
diagnosis. Presented at the Annual Congress of the British Columbia Society of Laboratory
Science, Whistler BC, April 2014. [cited 9 September 2016] Available from:
http://www.bcsls.net/pages/documents/April2014ABCsofCREs-Presentation_000.pdf
8. Ontario Agency for Health Protection and Promotion (Public Health Ontario), Provincial
Infectious Diseases Advisory Committee. Best practices for surveillance of health care-associated
infections in patient and resident populations, 3rd ed. Toronto, ON: Queen’s Printer for Ontario;
2014. [cited 9 September 2016]. Available from:
http://www.publichealthontario.ca/en/eRepository/Surveillance_3-3_ENGLISH_2011-10-
28%20FINAL.pdf
9. Ontario Agency for Health Protection and Promotion (Public Health Ontario). ASP 101: What is
antimicrobial stewardship. Toronto, ON: Queen’s Printer for Ontario: Toronto; 2014. [Cited 9
September 2016]. Available from:
https://www.publichealthontario.ca/en/eRepository/What_is_Antimicrobial_Stewardship_2014
Monthly Infectious Diseases Surveillance Report Page 7 of 12
SIGNIFICANT REPORTABLE DISEASE ACTIVITY
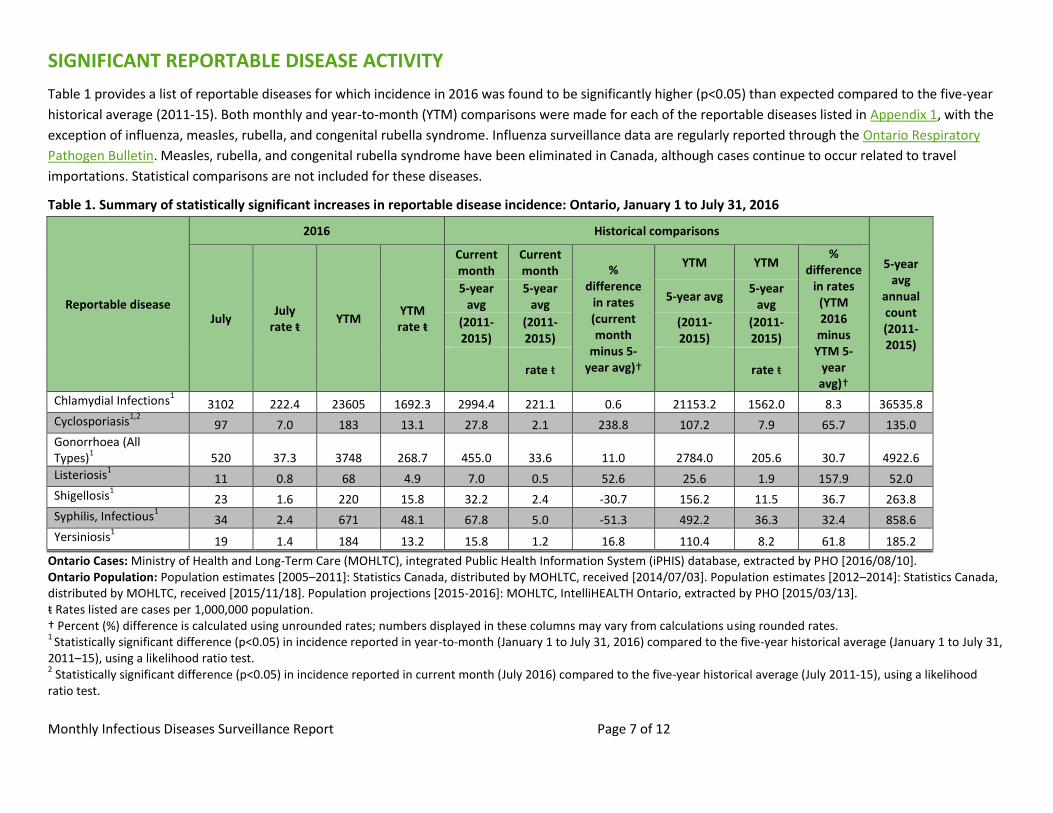
Table 1 provides a list of reportable diseases for which incidence in 2016 was found to be significantly higher (p<0.05) than expected compared to the five-year
historical average (2011-15). Both monthly and year-to-month (YTM) comparisons were made for each of the reportable diseases listed in Appendix 1, with the
exception of influenza, measles, rubella, and congenital rubella syndrome. Influenza surveillance data are regularly reported through the Ontario Respiratory
Pathogen Bulletin. Measles, rubella, and congenital rubella syndrome have been eliminated in Canada, although cases continue to occur related to travel
importations. Statistical comparisons are not included for these diseases.
Table 1. Summary of statistically significant increases in reportable disease incidence: Ontario, January 1 to July 31, 2016
Reportable disease
2016 Historical comparisons
5-year avg
annual count (2011-2015)
July July
rate ŧ YTM
YTM rate ŧ
Current month
Current month %
difference in rates (current month
minus 5-year avg)†
YTM YTM %
difference in rates
(YTM 2016
minus YTM 5-
year avg)†
5-year avg
5-year avg
5-year avg 5-year
avg
(2011-2015)
(2011-2015)
(2011-2015)
(2011-2015)
rate ŧ
rate ŧ
Chlamydial Infections1 3102 222.4 23605 1692.3 2994.4 221.1 0.6 21153.2 1562.0 8.3 36535.8
Cyclosporiasis1,2
97 7.0 183 13.1 27.8 2.1 238.8 107.2 7.9 65.7 135.0
Gonorrhoea (All Types)
1 520 37.3 3748 268.7 455.0 33.6 11.0 2784.0 205.6 30.7 4922.6
Listeriosis1 11 0.8 68 4.9 7.0 0.5 52.6 25.6 1.9 157.9 52.0
Shigellosis1 23 1.6 220 15.8 32.2 2.4 -30.7 156.2 11.5 36.7 263.8
Syphilis, Infectious1 34 2.4 671 48.1 67.8 5.0 -51.3 492.2 36.3 32.4 858.6
Yersiniosis1 19 1.4 184 13.2 15.8 1.2 16.8 110.4 8.2 61.8 185.2
Ontario Cases: Ministry of Health and Long-Term Care (MOHLTC), integrated Public Health Information System (iPHIS) database, extracted by PHO [2016/08/10]. Ontario Population: Population estimates [2005–2011]: Statistics Canada, distributed by MOHLTC, received [2014/07/03]. Population estimates [2012–2014]: Statistics Canada, distributed by MOHLTC, received [2015/11/18]. Population projections [2015-2016]: MOHLTC, IntelliHEALTH Ontario, extracted by PHO [2015/03/13]. ŧ Rates listed are cases per 1,000,000 population. † Percent (%) difference is calculated using unrounded rates; numbers displayed in these columns may vary from calculations using rounded rates. 1
Statistically significant difference (p<0.05) in incidence reported in year-to-month (January 1 to July 31, 2016) compared to the five-year historical average (January 1 to July 31, 2011–15), using a likelihood ratio test. 2 Statistically significant difference (p<0.05) in incidence reported in current month (July 2016) compared to the five-year historical average (July 2011-15), using a likelihood
ratio test.
Monthly Infectious Diseases Surveillance Report Page 8 of 12
Bacterial Sexually Transmitted Infections (STIs)
Compared to the five-year historical averages, there were statistically significant increases in the YTM
incidence of all three bacterial STIs (chlamydia, gonorrhea, and infectious syphilis) reported between
January 1 and July 31, 2016. During this period, laboratory-confirmed cases of chlamydia increased 8.3%
(from 1,562.0 to 1,692.3 cases per 1,000,000 population), gonorrhea cases increased 30.7% (from 205.6
to 268.7 cases per 1,000,000 population), and cases of infectious syphilis increased 32.4% (from 36.3 to
48.1 cases per 1,000,000 population).
The potential causes for these concurrent provincial increases in bacterial STIs are under active
investigation and are likely multifactorial. PHO will continue to monitor the epidemiology of bacterial
STIs in Ontario in subsequent months.
Listeriosis
The YTM incidence rate for listeriosis for 2016 was significantly higher than the average for the same
period in the previous five years. From January 1 to July 31, 2016, 68 cases of listeriosis were reported
compared to an expected average of 26 cases. The increase observed in the first half of 2016 can be
attributed to two separate outbreaks that began in 2015. Certain Dole and PC Organics brands of pre-
packaged leafy green products were implicated in the first outbreak and Neilson brand partly skimmed
chocolate milk was implicated in the second. Additional details about these outbreaks are available in
the June 2016 and July 2016 issues of this report.
Shigellosis
Incidence rates for shigellosis continued to be higher than expected in the first half of 2016. The YTM
incidence rate for 2016 was significantly higher than the average for the same period in the previous five
years. From January 1 to July 31, 2016, 220 cases of shigellosis were reported compared to an expected
average of 156 cases. However, the number of cases reported in July indicates that this sustained
increase in incidence may be waning with 23 cases reported in 2016 compared to 32 cases on average in
July in the preceeding five years. The source of the increase observed in 2015 through to the first half of
2016 was described in the May 2016 issue of this report. PHO continues to collaborate with public
health units (PHUs) affected by this increase to identify risk factors, at-risk populations, and prevention
and control measures.
Yersiniosis
A statistically significant increase in the YTM incidence rate of reported cases of yersiniosis was
observed. From January to July 2016, 184 cases of yersiniosis were reported compared to an expected
average of 110 cases. The cause of the increase is unknown at this time; however, the monthly rate was
not significantly above expected in July with 19 cases reported in 2016 compared to 16 cases on average
in July in the preceeding five years. The information available does not suggest that the increase is due
to a single source outbreak. PHO continues to monitor trends and investigate this increase to identify
potential clustering.

Monthly Infectious Diseases Surveillance Report Page 9 of 12
Cyclosporiasis
Statistically significant increases in both the monthly and the YTM incidence rates of cyclosporiasis were
observed in July 2016. From January to July 2016, 183 cases of cyclosporiasis were reported compared
to an expected average of 107 cases; of the 183 cases, 97 occurred during the month of July, when only
28 cases would be expected. An Outbreak Investigation Coordinating Committee (OICC) was activated
on July 15 to investigate non-travel cases of cyclosporiasis cases. The investigation is ongoing and the
source of this increase has not been identified.
Monthly Infectious Diseases Surveillance Report Page 10 of 12
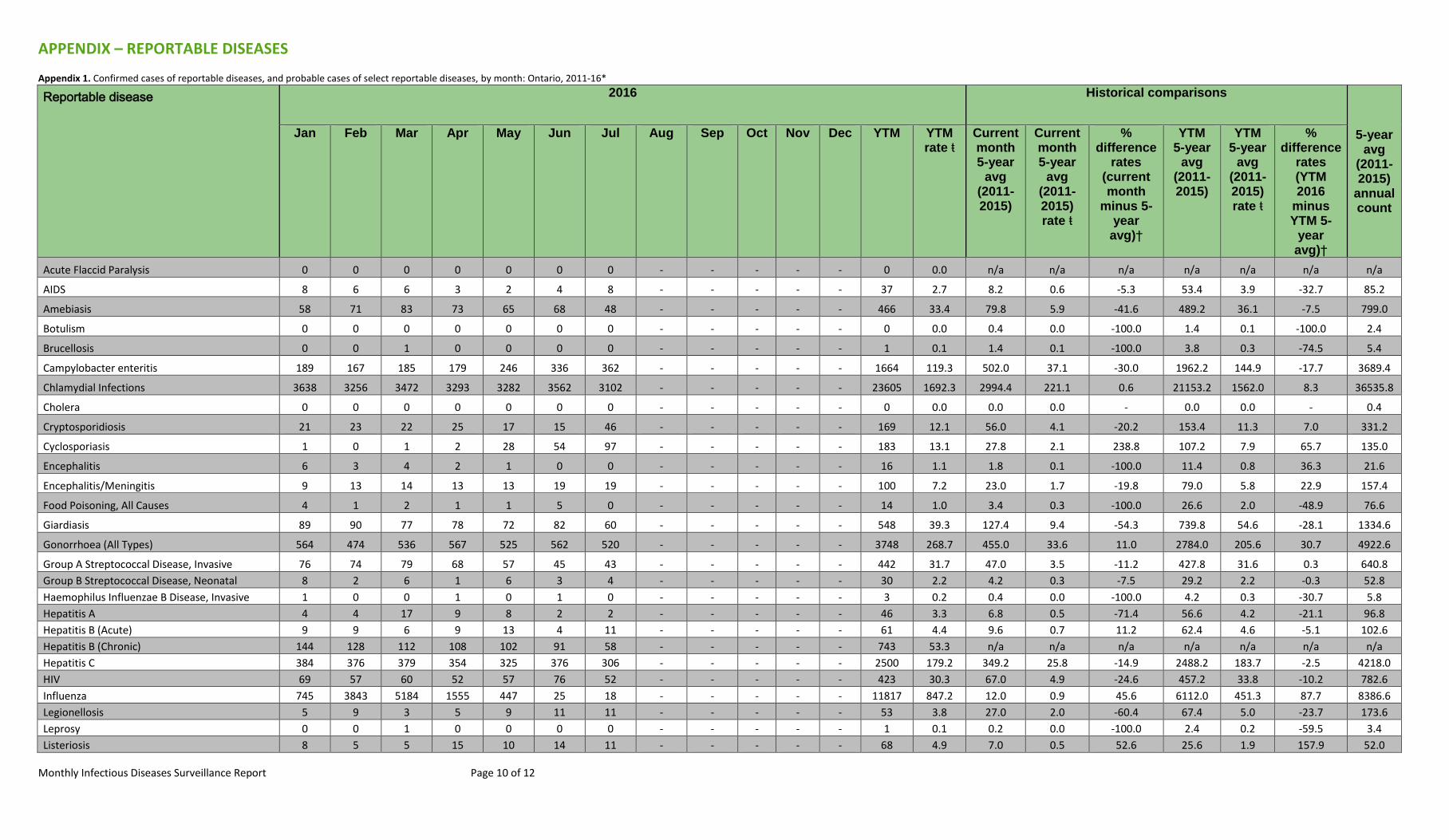
APPENDIX – REPORTABLE DISEASES
Appendix 1. Confirmed cases of reportable diseases, and probable cases of select reportable diseases, by month: Ontario, 2011-16*
Reportable disease 2016 Historical comparisons
5-year avg
(2011-2015)
annual count
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec YTM YTM rate ŧ
Current month 5-year
avg (2011-2015)
Current month 5-year
avg (2011-2015) rate ŧ
% difference
rates (current month
minus 5-year
avg)†
YTM 5-year
avg (2011-2015)
YTM 5-year
avg (2011-2015) rate ŧ
% difference
rates (YTM 2016
minus YTM 5-
year avg)†
Acute Flaccid Paralysis 0 0 0 0 0 0 0 - - - - - 0 0.0 n/a n/a n/a n/a n/a n/a n/a
AIDS 8 6 6 3 2 4 8 - - - - - 37 2.7 8.2 0.6 -5.3 53.4 3.9 -32.7 85.2
Amebiasis 58 71 83 73 65 68 48 - - - - - 466 33.4 79.8 5.9 -41.6 489.2 36.1 -7.5 799.0
Botulism 0 0 0 0 0 0 0 - - - - - 0 0.0 0.4 0.0 -100.0 1.4 0.1 -100.0 2.4
Brucellosis 0 0 1 0 0 0 0 - - - - - 1 0.1 1.4 0.1 -100.0 3.8 0.3 -74.5 5.4
Campylobacter enteritis 189 167 185 179 246 336 362 - - - - - 1664 119.3 502.0 37.1 -30.0 1962.2 144.9 -17.7 3689.4
Chlamydial Infections 3638 3256 3472 3293 3282 3562 3102 - - - - - 23605 1692.3 2994.4 221.1 0.6 21153.2 1562.0 8.3 36535.8
Cholera 0 0 0 0 0 0 0 - - - - - 0 0.0 0.0 0.0 - 0.0 0.0 - 0.4
Cryptosporidiosis 21 23 22 25 17 15 46 - - - - - 169 12.1 56.0 4.1 -20.2 153.4 11.3 7.0 331.2
Cyclosporiasis 1 0 1 2 28 54 97 - - - - - 183 13.1 27.8 2.1 238.8 107.2 7.9 65.7 135.0
Encephalitis 6 3 4 2 1 0 0 - - - - - 16 1.1 1.8 0.1 -100.0 11.4 0.8 36.3 21.6
Encephalitis/Meningitis 9 13 14 13 13 19 19 - - - - - 100 7.2 23.0 1.7 -19.8 79.0 5.8 22.9 157.4
Food Poisoning, All Causes 4 1 2 1 1 5 0 - - - - - 14 1.0 3.4 0.3 -100.0 26.6 2.0 -48.9 76.6
Giardiasis 89 90 77 78 72 82 60 - - - - - 548 39.3 127.4 9.4 -54.3 739.8 54.6 -28.1 1334.6
Gonorrhoea (All Types) 564 474 536 567 525 562 520 - - - - - 3748 268.7 455.0 33.6 11.0 2784.0 205.6 30.7 4922.6
Group A Streptococcal Disease, Invasive 76 74 79 68 57 45 43 - - - - - 442 31.7 47.0 3.5 -11.2 427.8 31.6 0.3 640.8
Group B Streptococcal Disease, Neonatal 8 2 6 1 6 3 4 - - - - - 30 2.2 4.2 0.3 -7.5 29.2 2.2 -0.3 52.8
Haemophilus Influenzae B Disease, Invasive 1 0 0 1 0 1 0 - - - - - 3 0.2 0.4 0.0 -100.0 4.2 0.3 -30.7 5.8
Hepatitis A 4 4 17 9 8 2 2 - - - - - 46 3.3 6.8 0.5 -71.4 56.6 4.2 -21.1 96.8
Hepatitis B (Acute) 9 9 6 9 13 4 11 - - - - - 61 4.4 9.6 0.7 11.2 62.4 4.6 -5.1 102.6
Hepatitis B (Chronic) 144 128 112 108 102 91 58 - - - - - 743 53.3 n/a n/a n/a n/a n/a n/a n/a
Hepatitis C 384 376 379 354 325 376 306 - - - - - 2500 179.2 349.2 25.8 -14.9 2488.2 183.7 -2.5 4218.0
HIV 69 57 60 52 57 76 52 - - - - - 423 30.3 67.0 4.9 -24.6 457.2 33.8 -10.2 782.6
Influenza 745 3843 5184 1555 447 25 18 - - - - - 11817 847.2 12.0 0.9 45.6 6112.0 451.3 87.7 8386.6
Legionellosis 5 9 3 5 9 11 11 - - - - - 53 3.8 27.0 2.0 -60.4 67.4 5.0 -23.7 173.6
Leprosy 0 0 1 0 0 0 0 - - - - - 1 0.1 0.2 0.0 -100.0 2.4 0.2 -59.5 3.4
Listeriosis 8 5 5 15 10 14 11 - - - - - 68 4.9 7.0 0.5 52.6 25.6 1.9 157.9 52.0
Monthly Infectious Diseases Surveillance Report Page 11 of 12
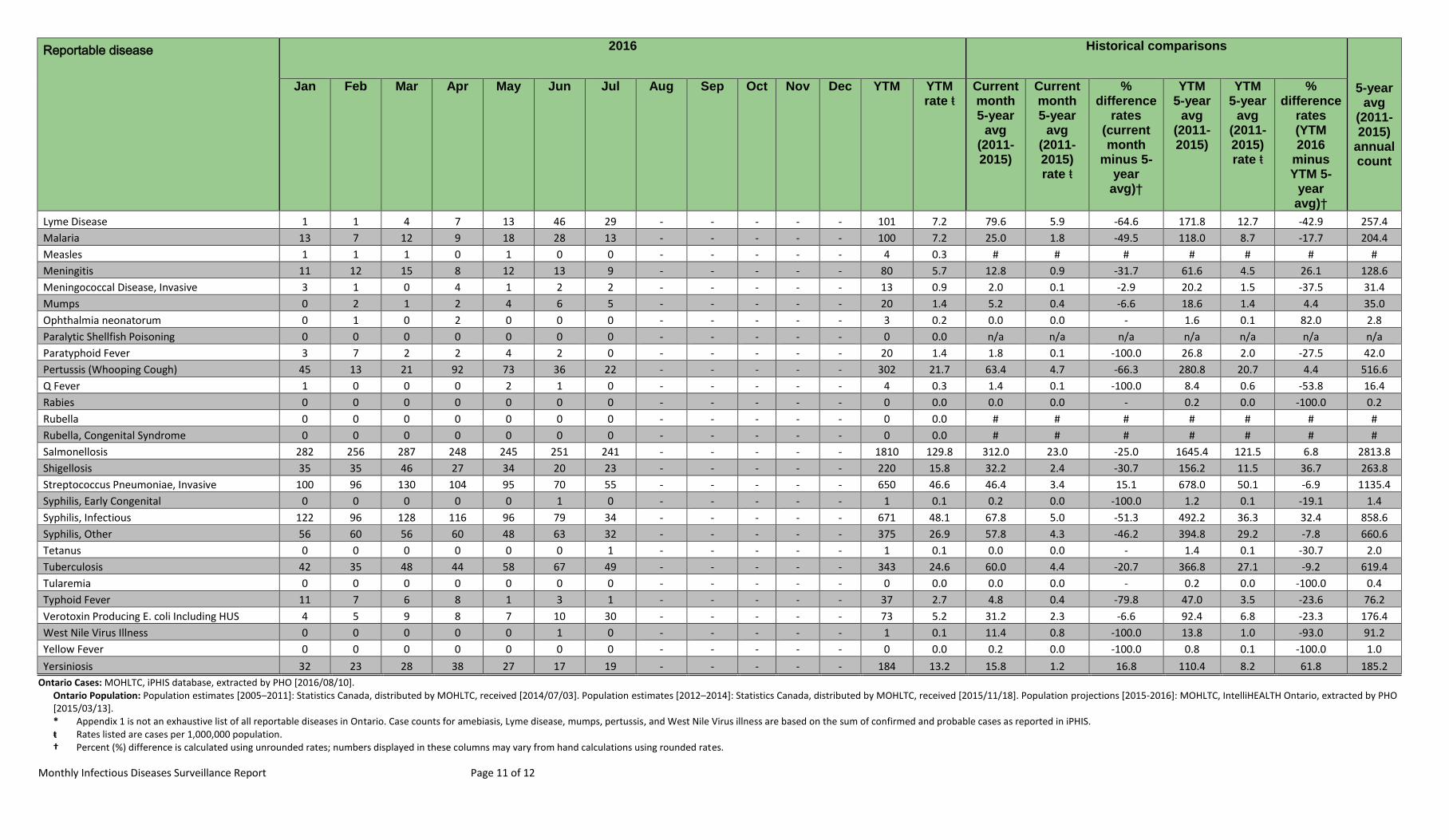
Reportable disease 2016 Historical comparisons
5-year avg
(2011-2015)
annual count
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec YTM YTM rate ŧ
Current month 5-year
avg (2011-2015)
Current month 5-year
avg (2011-2015) rate ŧ
% difference
rates (current month
minus 5-year
avg)†
YTM 5-year
avg (2011-2015)
YTM 5-year
avg (2011-2015) rate ŧ
% difference
rates (YTM 2016
minus YTM 5-
year avg)†
Lyme Disease 1 1 4 7 13 46 29 - - - - - 101 7.2 79.6 5.9 -64.6 171.8 12.7 -42.9 257.4
Malaria 13 7 12 9 18 28 13 - - - - - 100 7.2 25.0 1.8 -49.5 118.0 8.7 -17.7 204.4
Measles 1 1 1 0 1 0 0 - - - - - 4 0.3 # # # # # # #
Meningitis 11 12 15 8 12 13 9 - - - - - 80 5.7 12.8 0.9 -31.7 61.6 4.5 26.1 128.6
Meningococcal Disease, Invasive 3 1 0 4 1 2 2 - - - - - 13 0.9 2.0 0.1 -2.9 20.2 1.5 -37.5 31.4
Mumps 0 2 1 2 4 6 5 - - - - - 20 1.4 5.2 0.4 -6.6 18.6 1.4 4.4 35.0
Ophthalmia neonatorum 0 1 0 2 0 0 0 - - - - - 3 0.2 0.0 0.0 - 1.6 0.1 82.0 2.8
Paralytic Shellfish Poisoning 0 0 0 0 0 0 0 - - - - - 0 0.0 n/a n/a n/a n/a n/a n/a n/a
Paratyphoid Fever 3 7 2 2 4 2 0 - - - - - 20 1.4 1.8 0.1 -100.0 26.8 2.0 -27.5 42.0
Pertussis (Whooping Cough) 45 13 21 92 73 36 22 - - - - - 302 21.7 63.4 4.7 -66.3 280.8 20.7 4.4 516.6
Q Fever 1 0 0 0 2 1 0 - - - - - 4 0.3 1.4 0.1 -100.0 8.4 0.6 -53.8 16.4
Rabies 0 0 0 0 0 0 0 - - - - - 0 0.0 0.0 0.0 - 0.2 0.0 -100.0 0.2
Rubella 0 0 0 0 0 0 0 - - - - - 0 0.0 # # # # # # #
Rubella, Congenital Syndrome 0 0 0 0 0 0 0 - - - - - 0 0.0 # # # # # # #
Salmonellosis 282 256 287 248 245 251 241 - - - - - 1810 129.8 312.0 23.0 -25.0 1645.4 121.5 6.8 2813.8
Shigellosis 35 35 46 27 34 20 23 - - - - - 220 15.8 32.2 2.4 -30.7 156.2 11.5 36.7 263.8
Streptococcus Pneumoniae, Invasive 100 96 130 104 95 70 55 - - - - - 650 46.6 46.4 3.4 15.1 678.0 50.1 -6.9 1135.4
Syphilis, Early Congenital 0 0 0 0 0 1 0 - - - - - 1 0.1 0.2 0.0 -100.0 1.2 0.1 -19.1 1.4
Syphilis, Infectious 122 96 128 116 96 79 34 - - - - - 671 48.1 67.8 5.0 -51.3 492.2 36.3 32.4 858.6
Syphilis, Other 56 60 56 60 48 63 32 - - - - - 375 26.9 57.8 4.3 -46.2 394.8 29.2 -7.8 660.6
Tetanus 0 0 0 0 0 0 1 - - - - - 1 0.1 0.0 0.0 - 1.4 0.1 -30.7 2.0
Tuberculosis 42 35 48 44 58 67 49 - - - - - 343 24.6 60.0 4.4 -20.7 366.8 27.1 -9.2 619.4
Tularemia 0 0 0 0 0 0 0 - - - - - 0 0.0 0.0 0.0 - 0.2 0.0 -100.0 0.4
Typhoid Fever 11 7 6 8 1 3 1 - - - - - 37 2.7 4.8 0.4 -79.8 47.0 3.5 -23.6 76.2
Verotoxin Producing E. coli Including HUS 4 5 9 8 7 10 30 - - - - - 73 5.2 31.2 2.3 -6.6 92.4 6.8 -23.3 176.4
West Nile Virus Illness 0 0 0 0 0 1 0 - - - - - 1 0.1 11.4 0.8 -100.0 13.8 1.0 -93.0 91.2
Yellow Fever 0 0 0 0 0 0 0 - - - - - 0 0.0 0.2 0.0 -100.0 0.8 0.1 -100.0 1.0
Yersiniosis 32 23 28 38 27 17 19 - - - - - 184 13.2 15.8 1.2 16.8 110.4 8.2 61.8 185.2
Ontario Cases: MOHLTC, iPHIS database, extracted by PHO [2016/08/10]. Ontario Population: Population estimates [2005–2011]: Statistics Canada, distributed by MOHLTC, received [2014/07/03]. Population estimates [2012–2014]: Statistics Canada, distributed by MOHLTC, received [2015/11/18]. Population projections [2015-2016]: MOHLTC, IntelliHEALTH Ontario, extracted by PHO [2015/03/13]. * Appendix 1 is not an exhaustive list of all reportable diseases in Ontario. Case counts for amebiasis, Lyme disease, mumps, pertussis, and West Nile Virus illness are based on the sum of confirmed and probable cases as reported in iPHIS. ŧ Rates listed are cases per 1,000,000 population. † Percent (%) difference is calculated using unrounded rates; numbers displayed in these columns may vary from hand calculations using rounded rates.

Monthly Infectious Diseases Surveillance Report Page 12 of 12
# Historical comparison data are not provided for measles, rubella, and congenital rubella syndrome because these diseases have been eliminated in Canada. However, as these diseases remain endemic in other countries, imported and import-related cases continue to occur in Ontario. n/a Acute Flaccid Paralysis and Paralytic Shellfish Poisoning became reportable in Ontario in December 2013. No historical data are available for comparisons. Also, a provincial case definition for chronic hepatitis B was released in January 2012. Please note that chronic and acute hepatitis B case counts are not mutually exclusive and should not be added to obtain a total for hepatitis B cases in Ontario. Historical comparisons are not available as cases of chronic hepatitis B may have been entered using varying criteria prior to this time.
Does not include cases for which the Ministry of Health and Long-Term Care was selected as the Diagnosing Health Unit or cases with a Disposition Description set to “DOES NOT MEET” or “ENTERED IN ERROR.”
Differentials in year-over-year comparisons are reflective of changes in disease incidence and changes in the size of the population.
Statistical tests comparing rates were not performed when the YTM rate in previous years was zero.
Case counts for tuberculosis and AIDS are based on diagnosis date and not episode date. HIV case counts are based on encounter date. Case counts for all other diseases are based on episode date.