Embed Size (px)
Citation preview

Montgomery County
Round Table & Luncheon
“Partnering for Action in 2016”March 29, 2016
A Special Round Table Event with All Montgomery County Hospitals and Post Acute Care Providers
Brooke Grove Retirement Village

1. Discuss existing and future collaborative efforts
in Montgomery County between hospitals and
post-acute partners
2. Identify successful strategies for improved
transitions and reduced admissions
3. Participate in smaller round table discussions to
plan collaborative activities
4. Commit to action with community partners to
improve care transitions across the county
Today’s Objectives
2

• Round table sessions
• Life Span & MHA sessions/education
• Hospital meetings
• 911 facilities
• Preferred providers
• Hospital workgroup / VHQC
• HEALTH Partners Coalition
• VHQC Care Transitions Project
• Collaborative funding proposals for improved
care coordination
• Nexus Montgomery
History
3

a. Approx. 125,000 Medicare beneficiaries
a. 13, 30-day readmissions each day
b. 76 admissions each day
c. 78 ED visits each day
d. 15 observation stays each day
b. 18% HHA, 20% SNF, 15% Home, 2%
Hospice
c. >10% - Readmissions occur on Day 1
d. Sepsis
Perspective – What do we know?
Source: Medicare Part A & B Claims Data through Qtr. 2, 2015

Readmissions by Discharge Destination
5
Discharged to: In Montgomery Co. In Maryland
Home 15.7% 17.5%
with/HH 17.2% 19.9%
SNF 17.0% 19.5%
Hospice 2.2% 1.9%

Top 10 Principal Diagnoses Leading to a
30-Day Readmission
6

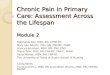
HEALTH Partners Days Until Readmission
7
0
50
100
150
200
250
300
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
HEALTH Partners Days until Readmission Frequency Breakdown (Q4-2014 to Q3-2015)
25% of readmissions occur within 4-5 days of discharge
50% of readmissions occur within 11 days of discharge
11.5% within 1 day of discharge!

a. Readmissions
a. Penalties are a reality! What you do now matters.
b. Quality Outcomes
a. Used to make decisions about care.
c. Improvement Activities
a. Adopting proven interventions
b. Measuring impact
d. Collaboration
a. Working alone doesn’t work.
How are you improving transitions?
8

Pre-Round Table Survey
9
http://www.interact2.net

• Not all answered….
• 7/27 are using INTERACT – most are SNFs
• 1-3 tools (2), 4-8 tools (3), Just starting (1)
• <6 Mths. (2), 6-12 Mths. (1), >12 Mths. (3)
• Tools Used the Most:1. SBAR: 5
2. STOP & WATCH: 4
3. Transfer Form: 4
4. Transfer Checklist: 4
5. Capabilities Checklist: 3
6. QI Tool: 2
7. Hospital Tracking Tool: 2
Results
10

a. Identify opportunities for providers to
embrace similar interventions to impact
care transitions on a larger scale.
b. Measure effectiveness of
interventions/improvement activities.
c. Spread the adoption of successful
interventions across the county.
d. Next level
e. Recognition
Goal
11

• Suburban Hospital
• Adventist Shady Grove Hospital
• Washington Adventist Hospital
• MedStar Montgomery Medical Center
• Holy Cross Hospital
Hospital Sharing
12

13
Partnering For Action in 2016
Montgomery County Round Table
February 10, 2016

SNF/NH Collaboration Historical Perspective
• 2005 the Nursing Home Collaborative was established by Suburban Hospital and included multiple nursing facilities. It was originally initiated out of the Medicine and Family Practice QA Committee as a way to better coordinate the care between facilities. It was a large and productive group as long as common concerns were addressed.
• 2010 Healthcare focus began changing with a focus on readmissions and care coordination. The meeting was transferred to Director of Care Coordination, 2010 to develop inter-facility groups focusing on readmissions
• 2011 Collaborative effort initiated with Hebrew Home from the Charles E Smith Life Community to address readmissions and build more collaborative relationships between the physicians in both entities.
March 28, 2016 14

Lessons Learned
• Building strong relationships is instrumental for safe, smooth transition and lowering risk for hospitalization
• The foundation of the relationship needs to based on Communication, Collaboration and Continuity of Care
March 28, 2016 15

Getting to “Yes” Readmissions become a Priority
•Projects have been a collaboration between the two unrelated organizations, each offering different levels of care•Regular meetings were planned between the organizations, meeting sites were alternated•Organizations brought their own perspectives and priorities to the table•Reduction of Readmissions was identified as a priority•Critical stakeholders were identified and an effective choice was made with respect to staff from each organization to focus on Readmissions work. • Both leadership and clinical staff were included
March 28, 2016 16

Why Use INTERACT ?
• INTERACT’s Goal to improve care and reduce the frequency of potentially avoidable transfers to acute hospital aligns perfectly with initiatives currently in place in the acute care hospital settings.
March 28, 2016 17

SBAR Tool: A Great Example on How to Enhance Communication
Situation•Concise statement of the problem•What is happening now?
Background•Brief and pertinent information related to the situation•What had happened?
Assessment•Analysis and consideration of options•What do you see or think is going on?
Recommendation•Suggest/recommend action•What do you want to happen?
March 28, 2016 18

Suburban’s Bundle of Strategies to Prevent Readmissions
• Early Risk Screening
• Identify patients early in admission
• Interdisciplinary Care Planning
• Representative from SNF invited to attend ID rounds
• Patient and Family Education
• Effort to coordinate educational materials between facilities
March 28, 2016 19

Suburban’s Bundle of Strategies to Prevent Readmissions (continued)
• Medication Management
• Participated in Cardinal Grant
• Primary Provider Handoff
• Sent Hospitalists on site visit to SNF
• ED Workgroup
• ED physicians available for consult by phone
March 28, 2016 20

Suburban’s Bundle of Strategies to Prevent Readmissions (continued)
• Transitions of Care
•Case reviews
•Collaboration on pathways
•Transition Guide RNs care planning w/complex patients
•Paper prescriptions for C2-C5 medications
•Warm handoff RN to RN
March 28, 2016 21

Case Management

• Real time notification of every re-admitted patient
• Root Cause Analysis of readmission by nursing
facility
• Monthly meetings to discuss readmissions
– Palliative care consults
• Data from Nursing facilities on readmission rates
• Closing the loop – Outcomes of patients
– Referrals to Home Health
– Notification about potential readmissions after dc
Wish List

• Joint plans of care for frequently readmitted patients
• INTERACT Tools:
– Capabilities Checklist
– Transfer form
Bright colored paper
– SBAR
Direct phone numbers for provider to provider
report
Wish List

For More Information
Jo Cimino, MSN, RN, ACM
Director of Case Management
Phone: 240-826-6532 or 301-891-5326
Fax: 240-826-5264 or 301-891-6275


SNF PARTNERSHIPSCurrent partnership with St. Thomas Moore
Readmission reduction of 5% since beginning of partnership
Infectious Disease MD makes weekly visits to St. Thomas Moore to
evaluate patients that have been discharged from WAH
Facilitation of viewing EMR’s from both entities to increase
communication. All ED MD’s and Pop Health staff have access to
EMR
INTERACT Capabilities list
Implementation of SBAR communication tool
MD to MD
RN to RN

SNF PARTNERSHIPSEMR Access to two ManorCare facilities to launch mid-February
MD to MD calls
RN to RN calls
Dedicated call line at both the facility and at WAH ED
SBAR communication
INTERACT Capabilities list
Physicians at ManorCare facilities all credentialed at WAH
Beginning Bi-Weekly Readmission Reviews first week of February

TRANSFUSION PROGRAM
Developed for SNF’s that do not transfuse patients at
their facilities
Full Time RN M/W/F
Non-emergent transport
Able to take vent and dialysis patients

CONTACT INFO
Zachary Goodling
Manager, Population Health
Washington Adventist Hospital
301-891-6395
Katherine Barmer
Director of Population Health Management
Adventist Healthcare

Improving Population Health through
Community Partnerships
Diana Saladini
Director, Outpatient Services & Population Health
March 29, 2016
31

Focus on The Triple Aim
• Framework developed by the Institute for
Healthcare Improvement (IHI) to optimize health
system performance
– Improving the patient experience of care (including
quality and satisfaction)
– Improving the health of populations
– Reducing the per capita cost of health care.
32
Source: Institute for Healthcare Improvement,
http://www.ihi.org/Engage/Initiatives/TripleAim
March 29, 2016

Develop a Population Health Strategy
33Source: Playbook for Population Health, Advisory Board, 2013
March 29, 2016

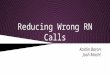
Understand our Population:
Identify High Utilizers
34
Source: HSCRC Inpatient and Outpatient Case Mix Data with CRISP
EID. Data from calendar years 2012-2015
Montgomery County High Utilizers: 3 or More Admissions
March 29, 2016

Partner Alignment
35
March 29, 2016

Partner Alignment
Open Flow of Communication to:
• Develop/Improve Processes
– Improve Care Transitions
• Warm Handover Process
• Reduce Avoidable Utilization
– Readmissions
• Multi-Disciplinary Case Review of Readmitted Patients
– Emergency Room Visits
• Improve Patient Experience & Outcomes
36
March 29, 2016

Criteria for Community Partners
• Preferred Provider Measures of Performance
– Readmission Rate
– Clinical Service Offerings
– Staffing Ratios
– Cost of Services
– Length of Stay
– Federal Quality Measures
– INTERACT
37
March 29, 2016

QUESTIONS?
38
March 29, 2016

Montgomery County Round Table
Cathy Livingston, LCSW-C
Director, Documentation Quality & Care Transitions
March 29, 2016

Agenda
• Holy Cross Health
• Readmission Prevention Activities
– O/E is better than expected for both hospitals
• Opportunities
40

Holy Cross Health
• Holy Cross Hospital, Silver Spring, MD
– 435 bed acute inpatient facility
• Holy Cross Germantown Hospital, Germantown, MD
– 93 bed acute inpatient facility
• Holy Cross Health Network
41

Holy Cross Health Network
• 4 outpatient health centers
– Silver Spring Aspen Hill
– Gaithersburg Germantown
• 2 primary care practices
• Community health programs
– Chronic disease self-management classes
– Faith Community Nurses
– Community health workers
– Wellness and prevention classes
• Medical adult day care
– Licensed for 35 participants
– Caregiver support groups
42

Readmission Prevention – Discharge Home
• Follow up phone calls: 3 calls in 30 days
– PCP appt., prescriptions filled, discharge instructions, signs & symptoms
• Skilled home care
• Transitional Care Program
• Care Link Program: mental health & substance abuse
• PCP or Health Center follow up appointments
• Payer – complex case management programs
• Pilot – home pharmacy program
43

Readmission Prevention - SNF
• SNF partnerships
• Relationships with 911 area SNFs
• Post-Acute Care Nurse Liaison – Daily contact with SNFs day after transfer
• Daily review of all readmissions
• IPC (hospitalist practice) in SNFs
• Palliative Care & Hospice
44

Current SNF Communication
• SNF on-site liaisons
• Care Finder Pro
• Paper documents at transfer (from both SNF & hosp)
• CRISP
• Direct Email
• Post-Acute Care Nurse phone calls
• We can do better!
45

Opportunities: SNF to hospital• SNF to Hospital
– Sepsis is the leading reason for readmission for HCH
• Prevention, early detection & intervention
• Interact Stop & Watch tool
– Proactive Palliative Care consults prior to the need for transfer
– Collaborate with hospitals for outpatient services rather than inpatient admission. Ex: transfusions, outpatient procedures
– SNF to ED telephone communication
– ED “Treat and Release”
– Appropriate use of Observation Status rather than inpatient admission
– SNF use of Interact Transfer Form & Capabilities checklist
– ED wants Code status, medications, reason for transfer
46

Opportunities: Hospital to SNF
• Hospital to SNF
– Better understanding of SNF capabilities – earlier transfers
– Improved Transfer Summaries
– RN to RN handoff
– MD to MD handoff
– Pre-transfer Medications
• Pre-medicate for pain, anxiety, routine meds due within 2 hours
– Ensure Class II prescriptions accompany the patient
– Ensure MOLST for both ambulance crew & SNF
– Improved hand off communication about end of life decisions made in the hospital
47

Collaboratives
– MHA – Transitions of Care
– Montgomery County Hospitals & VHQC
– H.E.A.L.T.H. Partners
– Payers – complex case management
– Specific hospital/SNF meetings
– Lifespan meetings
48

Potentially Avoidable Utilization
• Prevention Quality Indicators: diagnoses that should be successfully managed in the outpatient setting. Ex: diabetes, hypertension, asthma, COPD, Heart Failure, dehydration, UTIs, bacterial pneumonia
• Readmissions
• Potentially Preventable Complications
49

Care Transitions
• We need to share best practices and learn from each other.
• With the new waiver – either we all succeed or we all fail – collaborative relationships are essential.
• Forums such as these are very helpful – thank you for inviting us to participate.
50

…identify one or two items that many
could embrace throughout the county?
• High impact for issues that have wide-spread
opportunity
…measure our collective efforts?
• To show the impact of efforts across the
spectrum of care - processes
Wouldn’t it be nice if we could…
51

Spread out!
• Do not sit with others from your organization
• Interact with people from different
organizations
Share
• Use the guided questions to talk about
opportunities
Participate
• Volunteer to take notes, share and report
out to the larger group
Mini-Round Table Discussions
52

At tables
1. Find question sheet in packet
2. Identify note taker at each table
3. Discuss each question – the more sharing
the better
4. Report-out
5. Collect notes from each table
6. Identify themes
7. Next steps
Round Table Sharing
53

Volunteers from mini-table conversations
a. Ideas shared that sparked more interest?
b. Successful interventions shared?
c. INTERACT Tools conversation, ideas?
d. What opportunities were identified?
e. Needs/expectations related to partners?
f. Data collection insights?
Report Out
54

• Next Steps
1. Learn about HEALTH Partners
2. Learn about the Nursing Home
Improvement Network
• Commitment to Action Form
• Online Community
• Future County Meetings
• Round Table
• Conference Calls, etc.
Committing to ACTION
55

H.E.A.L.T.H. PartnersMontgomery County Post-Acute Care
Providers Roundtable With Local Hospitals
Presented by:
Mary Joseph RN, BC, CPHQ
Primary Care Coalition
301-628-3458
February 9,2016

About the Primary Care Coalition (PCC)
57
Vision: A community in which all residents have the opportunity to live healthy livesMontgomery County: A model for providing access to high quality, efficient care for all
Mission: Develop and coordinate a community-based health care system that strives for universal access and equity for low-income, uninsured, and ethnically diverse community members.

H.E.A.L.T.H. Partners
2011• Partnered with DHHS Aging and Disabilities; Holy Cross Hospital;
Housing Opportunities Commission; PCC to improve care transitions for dual eligible patients in Montgomery County
2013• Coalition formed with Delmarva • 16 organizations and residents of Holly Hall• Access to hospital Medicare admission and readmission data • Small tests of change
2014 • Over 20 organizations represented • Change from Delmarva to VHQC• Spread other senior housing units
2015• Continued monthly meetings and small tests of change• Pharmacy MTM outcome study
58

H.E.A.L.T.H. Partners
59
Purpose:
• Build and sustain a community coalition with a focus on improving
transitions of care
• Encourage person-centered and person-directed models of care by
providing a platform for the patient and family voice
• Collaborate and encourage efforts of organizations with shared
visions
• Advance public policies that furthers the vision
• Share Best Practices in caring for community residents
Mission:
To improve the transition of care from hospital to community for
residents of the region, thereby reducing preventable readmissions to
acute care hospitals.

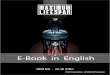
First Site-Holly Hall
96 units/112 Residents
On site resident counselor
60
Race
• African American 49%
• Asia 18%
• White 32%
• Middle Eastern 1%
Age
• < 60 years 17%
• > 60 years 83%
Ethnicity
• Hispanic 22%
• Non-Hispanic 78%
Disabilities:
• Medically Frail 42%
• Physical Disability 29%
• Psychological/Neurological 16%
• Cognitive 10%

Interventions/Tests of Change
61

Data
62
• The H.E.A.L.T.H partners community (Montgomery
County) has approximately 127,434 Medicare
beneficiaries.
• VHQC provides part A & B claims data and ongoing
analysis for communities to assist with the identification of
improvement opportunities.
• Readmissions
• Admissions
• ED visits
• # of days from discharge to readmission
• Top Diagnoses
• Specific Focus Areas

Resident Engagement
• Resident Meeting
• Resident Brochure
• Resident Interviews
63

Medication Therapy Management
64
• Pharmacist services provided by ALFA Specialty
Pharmacy

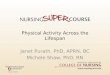
EMS InterventionsDaily notification
65
New Hampshire Ave Incident
Shift Date 808/09/2014
Incident Date Time Call Type Unit Apartment Location
14-0090550 08/09/2014 19:02:58 26-A-11 A716 310 10120 New Hampshire Ave.
2014 EMS Visits Holly Hall
2012-2013 Average = 4 per Month
Building 1/14 2/14 3/14 4/14 5/14 6/14 7/14 8/14 9/14 10/14 11/14 12/14 Total
10100 3 2 4 2 3 3 5 2 1 1 2 4 32
10110 0 2 2 0 0 1 1 0 1 2 1 3 13
10210 0 0 0 0 4 1 1 2 0 2 2 0 12
Total 3 4 6 2 7 5 7 4 2 5 5 7 57
EMS Visits by Building (2012-2014)
Building Apartments EMS
2012/100 Apartments
EMS
2012/100 Apartments
EMS
2012/100 Apartments
Arcola Towers 141 28 23 48
Elizabeth House 160 23 25 38
Forest Oaks 175 32 33 75
Waverly House 158 46 34 46
Holly Hall 96 55 45 63
Bauer Park 142 13 17
Town Center 112 13 20
Monthly Stats

Technology
• Care2Care
• Provides a patient-centered record including
– Essential care elements
– Barriers to care and self-management goals
• Facilitates optimal outcomes as the patient moves through
the continuum of care
• Community Health Gateway
• Web and call center solution
• Easy to understand discharge instructions & medication
information
• Help in navigating healthcare and community services
• Increased community collaboration
66

Successes
• Community Engagement
• Over 60% of residents have signed release of
information
• Hospital transitional care teams working
together
• EMS notification and follow-up
• MTM with positive outcomes on 20 residents in
several housing sites
• Introduction of technology to assist in personal
health management
67

Maryland - Virginia Nursing Home Improvement Network

1. Decrease the use of unnecessary
antipsychotic medication
2. Prevent and reduce healthcare associated
infections
3. Increase mobility of long-stay residents
4. Improve quality measures
5. Decrease potentially avoidable
hospitalizations
Nursing Home
Improvement Network Goals
69

1. Learning from both colleagues and experts
2. National Nursing Home Quality Care
Collaborative
3. Change package tools and resources
4. Consultation with VHQC quality consultants
5. Plan-Do-Study-Act (PDSA) cycles to test
improvement strategies and tactics
A Collaborative Approach
70

1. Flexible, no-cost structure for improvement
2. Quality Assurance Performance Improvement
(QAPI) tools and resources
3. Latest strategies and techniques from
successful colleagues and QI experts
4. Intervention development ideas and assistance
5. Support for participation in other QI initiatives
Benefits of Participation
71

Organizational quality goals
Quality Assurance and
Performance Improvement
(QAPI)
The Partnership to Improve
Dementia Care
Advancing Excellence
CMS Nursing Home Action
Plan
MD All Payer Model
Maryland-Virginia
Nursing Home
Improvement
Network
Aligning QI Efforts
72

1. Form an interdisciplinary QI team
2. Complete the QAPI self-assessment
3. Utilize a data-driven and proactive
approach to quality improvement
4. Develop and apply strategies for
implementing QAPI and overall quality
5. Participate in network activities
6. Actively share best practices with other
facilities
Your Commitment
73

1. Prepare data reports and facilitate analysis
to support overall quality improvement
2. Provide consultation by qualified staff and
faculty with expertise in quality improvement
3. Share best practices and evidence-based
tools and resources to support overall quality
improvement
4. Develop and facilitate collaboration using
workshops and peer mentoring
VHQC Commitment
74

Contact VHQC
Sheila McLean,
Program Director
804.289.5345
Linda Harris,
Improvement Consultant
804.289.5340
Theresa Mandela,
Improvement Consultant
804.289.5352
30
This material was prepared by VHQC, the Medicare Quality Innovation Network Quality Improvement Organization for Maryland and Virginia, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services.
The contents presented do not necessarily reflect CMS policy. VHQC/C.2.HAC/2/5/2016/2378

a. H.E.A.L.T.H. Partners
b. Nursing Home Improvement Network
c. Commitments for Action
a. Submit green sheet
b. Join NHIN
c. Join HEALTH Partners (yellow charter)
d. Join VHQC’s Online Community (flyer)
d. Participate in next sessions, calls and
activities…stay tuned!
Next Steps
76

Save the Date
Toolkit 2016: Build on you Emergency
Preparedness Program
Monday, June 6th
8:00-4:30
Holy Cross Hospital Auditoriums
Region V Emergency Response
Hospital-SNF Workshop
77

This material was prepared by VHQC, the Medicare Quality Innovation Network Quality Improvement Organization for Maryland Virginia,
under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services.
The contents presented do not necessarily reflect CMS policy. VHQC/C.3.CT/2/8/2016/2379
Questions?
78
• Please complete your session evaluation
• Submit action forms at registration.
• Thank you, Brook Grove, for hosting & lunch!
• Enjoy networking throughout lunchtime.