Embed Size (px)
Citation preview

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
G.L. Drusano, M.D.Co-Director
Ordway Research Institute &Research Physician
New York State Department of Health

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Monte Carlo simulation was invented by Metropolis and von Neumann
This technique and its first cousin Markov Chain Monte Carlo have been used since for construction of distributions (Markov Chain Monte Carlo was actually described as a solution to the “simulated annealing problem” in the Manhattan Project -Metropolis, Metropolis, Teller and Teller)

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
The first use of Monte Carlo simulation for drug dose choice and breakpoint determination was presented on October 15, 1998 at an FDA Anti-Infective Drug Products Advisory Committee
At this time, the drug was presented as “DrugX” but was evernimicin
The ultimate outcome was predicted by the method (but the drug died)

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
What is Monte Carlo simulation, as applied to Infectious Diseases issues?
What are the technical issues?For what is Monte Carlo simulation
useful?

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
What is Monte Carlo simulation?MC simulation allows us to
make use of prior knowledge of how a target population handles a specific drug to predict how well that drug will perform clinically at the dose chosen for clinical trials

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
How is this done?Through use of the mean parameter vector
and covariance matrix, derived from a population PK study, a sampling distribution is set up (think of every body in the world in a bucket from which you randomly select a large number of subjects, each of whom knows their PK parameter values). This allows the peak concentrations, AUC and Time > threshold to be calculated for all the subjects

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
How do we use this to predict the clinical utility of a specific drug dose?1) Identify the goal of therapy (cell kill,organism eradication resistance suppression)2) Identify the sources of variability that affect achieving the goal of therapy
a) PK variability (accounted for by MCS)b) Variability in MIC’s (or EC95, etc)c) Protein binding (only free drug is active)

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
What do we do?As an example, for a drug that is AUC/MIC driven in terms of goal of therapy (e.g. AUC/MIC of 100 for a good microbiological outcome), we can now take the 2000 (or 10000 or whatever) simulated subjects and divide the AUC by the lowest MIC in the distribution, then determine how many achieve the target of 100. This is then repeated with higher MIC values until the target attainment is zero or some low number

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
How does this help evaluate the utility of a specific drug dose?
We have target attainment rates at each MIC value in the organism population distribution. A specific fraction of the organisms have a specific MIC. A weighted average for the target attainment rate (taking an expectation) can be calculated. This value will be the overall “expected” target attainment rate for the outcome of interest for that specific dose.

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Technical Issues

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
What are the factors that may affect the simulation?
►Model mis-specification
►Choice of distribution
►Covariance matrix (full vs diagonal) ►Simulating the world from 6 subjects

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Model Mis-specification

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Model mis-specificationSometimes, data are only
available from older studies where full parameter sets and their distributions were not reported
Some investigators have used truncated models for simulation (1 cmpt vs 2 cmpt)
This may have more effect for some drugs relative to others (β lactams vs quinolones)

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Choice of Distribution

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
There are many underlying distributions possible for parameter values
Frequently, there are insufficient numbers of patients to make a true judgement
One way to at least make the choice rational is to examine how one distribution vs another recapitulates the mean parameter values and measure of dispersion
A quinolone example follows (N vs Log-N)

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Param Pop Mean
Sim Mean
Pop SD
Sim SD Distr
Vol 23.32 22.80 33.51 30.15 LN
Kcp 2.662 2.985 9.591 11.84 LN
Kpc 0.9327 0.7515 12.03 4.388 LN
SCL 6.242 6.252 4.360 4.303 LN

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Param Pop Mean
Sim Mean
Pop SD
Sim SD Distr
Vol 23.32 36.82 33.51 24.23 N
Kcp 2.662 8.926 9.591 6.311 N
Kpc 0.9327 9.914 12.03 7.370 N
SCL 6.242 6.936 4.360 3.817 N

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Here, it is clear that the Log-normal distribution better recaptures the mean parameter values and, in general, the starting dispersion (except Kpc)
However, for AUC distribution generation, it is clear that Log-normal is preferred because it performs better for the parameter of interest (SCL) for both mean value and dispersion
We have seen examples where there is no substantive difference (N vs Log-N)

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Full vs Major DiagonalCovariance Matrix

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
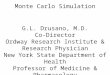
Sometimes, only the population standard deviations are available and only a major diagonal covariance matrix can be formed
Loss of the off-diagonal terms will generally cause the distribution to become broader (see example)
One can obtain an idea of the degree of impact if the correlation among parameters is known (of course if this is known it is likely one would also have the full covariance matrix!)

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Mean = 139.6
Median = 120.2
SD = 82.4
95% CI = 41.2-348.8
Mean = 140.4
Median = 121.4
SD = 83.5
95% CI = 40.7-351.4
0 200 400 600 800 1000Levofloxacin 750 mg AUC-Full Covariance Matrix
0
100
200
300
400
500
600
700
800
900
1000
Co
un
t
0.00
0.02
0.04
0.06
0.08
0.10
Pro
po
rtion
pe
r Ba
r

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Simulating the WorldFrom 6 Subjects

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Obviously, the robustness of the conclusions are affected by the information from which the population PK analysis was performed
If the “n” is small, there may be considerable risk attendant to simulating the world
One of the underlying assumptions is that the PK is reflective of that in the population of interest – care needs to be taken and appropriate consideration given to the applicability of the available data to the target population

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
But, in the end, something is probably better than nothing, so simulate away, but interpret the outcomes conservatively
How many simulations should be done?- Answer: as always, it depends
To stabilize variance in the far tails of the distribution (> 3 SD), it is likely that one would require > 10000 simulations

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Utility of Monte Carlo simulation, a non-exhaustive list:
►Determination of drug dose to attain a specific endpoint
►Determination of a breakpoint

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Required Factors for Rational Dose/Drug Comparison/Breakpoint Determination
1. Pharmacodynamic Target
2. Population Pharmacokinetic Modeling
3. Target Organism(s) MIC, EC50 (or EC90) Distribution
4. Protein Binding Data

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
What About Emergence of Resistance as an Endpoint?

P. aeruginosaP. aeruginosa outcome outcome studiesstudies
Rf in vitro Rfin vivo MIC (g/mL) MBC (g/mL)
2.35x10-6 2.2x10-6 0.8 1.6


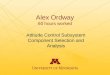
Peripheral (thigh)Compartment (Cp)
Central Blood Compartment (Cc)IP
injection
kcp kpc
+ Bacteria(XT/R)
f(c)
dCc= kaCa+kpcCp-kcpCc-keCc
dt
ke
dXS=KGS x XS x L - fKS(CcH ) x XS
dtdXR= KGR x XR x L- fKR(Cc
H ) x XR
dt
Kmax CcH
C H
50+CcH
f(CcH)=
Y1=XT=XS+XR
Y2=XR
[4]
[5]
[6]
[7]
[8]
, =K and = S,R
[2]
L = (1- (XR + XS)/POPMAX)
[9]
dCp = kcpCc - kpc Cp
dt
[3]
dCa= -kaCa
dt[1]

KmaxGS
0.117
KmaxGR
0.163
KmaxKS
94.01
KmaxKR
12.16
HKS
6.26
HKR
2.37
C50KS
123.5
C50KR
129.8
KmaxG -maximum growth rate (hr-1) in the presence of drug
KmaxK -maximum kill rate (hr-1)
C50K -drug concentration (g/mL) to decrease kill rate by half
HK -rate of concentration dependent kill
Popmax -maximal population size
Mean Parameter Estimates of the Model.Mean Parameter Estimates of the Model.
Popmax = 3.6 x 1010

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
All regimens were simultaneously fit in a large population model
The displayed graph is the predicted-observed plot for the total population after the Maximum A-posteriori Probability (MAP) Bayesian step

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
All regimens were simultaneously fit in a large population model
The displayed graph is the predicted-observed plot for the resistant population after the Maximum A-posteriori Probability (MAP) Bayesian step

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense


Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
In this experiment, a dose was selected to generate an exposure that would prevent emergence of resistance
As this was at the limit of detection, the measured population sometimes had “less than assay detectable” for the colony count
These were plotted at the detection limit

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
We were able to determine how the overall (sensitive plus resistant) population responds to pressure from this fluoroquinolone
More importantly, we were able to model the resistant subpopulation and choose a dose based on simulation to suppress the resistant mutants
The prospective validation demonstrated that the doses chosen to encourage and suppress the resistant mutants did, indeed, work
The identified AUC/MIC breakpoint was 157 – is this value predictive for the clinic?

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
For P aeruginosa and the suppression of resistance target, 750 mg of levofloxacin achieves the goal with a 61.2% probability
The levofloxacin nosocomial pneumonia trial cannot be examined for validation-a second drug was added for Pseudomonas aeruginosa
Simulation from Alan Forrest’s data for cipro (400 mg IV Q8h) shows a target attainment of 61.8% and 24.8% for 200 mg IV Q12h

Fluoroquinolone Fluoroquinolone Pharmacodynamics: Duration of Pharmacodynamics: Duration of
TherapyTherapyPerc
ent
of
Pati
ents
Rem
ain
ing
Cult
ure
-posi
tive
Days of therapy
AUC/MIC <125
AUC/MIC 125-250
AUC/MIC >250
100
75
50
25
0
0 2 4 6 8 10 12 14
Forrest et al AAC 1993;37:1073-1081

Suppression of Emergence of Resistance: Suppression of Emergence of Resistance:
A Pharmacodynamic SolutionA Pharmacodynamic SolutionIs Monte Carlo Simulation Predictive?
Peloquin studied 200 mg IV Q 12 h of ciprofloxacin in nosocomial pneumonia - P aeruginosa resistance rate 70% (7/10 - pneumonia only) - 77% (10/13 - all respiratory tract)
Monte Carlo simulation with a resistance suppression target (AUC/MIC = 157) predicts suppression in 24.8%
Fink et al studied ciprofloxacin in nosocomial pneumonia at a dose of 400 mg IV Q 8 h - P aeruginosa resistance rate 33% (12/36)
Monte Carlo simulation at this dose predicts suppression in 61.8% & resistance emergence in 38.2%
Peloquin et al Arch Int Med 1989;1492269-73 Fink et al AAC 1994;38:547-57

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Breakpoint Determination

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Breakpoint?

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-SenseThe same type analysis can be
employed for antivirals(A Prospective Validation to Show
the Approach Works!)

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
GW420867X is a NNRTI Population PK was
performed for each dose Three 1000-subject MC
simulations were performed
EC50 values were corrected for protein binding and the difference between EC50 and EC90
Fraction of patients with trough free drug > EC90
was determinedDrusano et al Antimicrob Agents Chemother 46:913-916

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Drusano et al Antimicrob Agents Chemother 46:913-916

Monte Carlo SimulationMonte Carlo SimulationSense and Non-Sense Sense and Non-Sense
Overall ConclusionsOverall Conclusions MCS is useful for rational breakpoint determination MCS allows insight into the probability that a specific
dose will attain its target This has been prospectively validated The technique rests upon certain assumptions and is as
reliable as the assumptions Care needs to be taken when applying the method,
particularly as regards applicability of the population studied and population size, among other issues

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
WE CAN DO BETTER AND WE SHOULD!– As an aside, I have trying since the early 1980’s to
interest the infectious diseases community in pharmacodynamic modeling, notably WITHOUT SUCCESS!
– WELL!

Days0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
Log
10 P
lasm
a H
IV-1
RN
A fr
om B
asel
ine,
cop
ies/
mL
-4.5
-4.0
-3.5
-3.0
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
0.5
PlaceboGW420867X 50mg GW420867X 100mg GW420867X 200mg
George→

Days0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
Log
10 P
lasm
a H
IV-1
RN
A fr
om B
asel
ine,
cop
ies/
mL
-4.5
-4.0
-3.5
-3.0
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
0.5
PlaceboGW420867X 50mg GW420867X 100mg GW420867X 200mg

The Role of Monte Carlo The Role of Monte Carlo Simulations in Antimicrobial Simulations in Antimicrobial
PharmacologyPharmacology The AUC of levofloxacin
in ELF is slightly more variable than in plasma
Target attainment is higher in Plasma than in ELF up to 0.5 mg/L
After 1.0 mg/L, ELF rates are higher
This may explain some “unexpected” successes

The Role of Monte Carlo The Role of Monte Carlo Simulations in Antimicrobial Simulations in Antimicrobial
PharmacologyPharmacologyAn Expectation taken over the MIC
distribution of 404 strains of Pseudomonas aeruginosa for the ELF AUC distribution yielded an overall target attainment of 65.6%
An Expectation taken over the MIC distribution of 404 strains of Pseudomonas aeruginosa for the Plasma AUC distribution yielded an overall target attainment of 67.1%

The Role of Monte Carlo The Role of Monte Carlo Simulations in Antimicrobial Simulations in Antimicrobial
PharmacologyPharmacology Conclusions (cont’d)Conclusions (cont’d)
The distribution range provides insight into why some patients may respond sub-optimally to a specific dose of drug while others respond when they “should not”
The effect of inflammation on drug penetration is not accounted for in this model
Examination of ELF penetration with active inflammation needs to be undertaken

The Role of Monte Carlo The Role of Monte Carlo Simulations in Antimicrobial Simulations in Antimicrobial
PharmacologyPharmacology
Let us examine target attainment with a robust population PK analysis (n = 272)
Preston et al published a 272 patient study of levofloxacin (500 mg QD) use in community-acquired infections (JAMA 1998;279:125-129)
This Population PK analysis was employed
Target Attainment to Evaluate Dose

The Role of Monte Carlo The Role of Monte Carlo Simulations in Antimicrobial Simulations in Antimicrobial
PharmacologyPharmacology
What About Breakpoint Determination?

Role of Monte Carlo Simulation for Dose Choice Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectivesfor Clinical Trials of Anti-Infectives
Required Factors for Rational Dose/Drug Comparison
1. Pharmacodynamic Goals of Therapy
2. Population Pharmacokinetic Modeling
3. Target Organism(s) MIC Distribution
4. Protein Binding Data in Animal and Man

Use of Simulation:Use of Simulation:Overall ConclusionsOverall Conclusions
Simulation can also allow insight into drug penetration into specialized spaces
The variability in penetration may help explain therapeutic failures at an “adequate” drug dose
Simulation is a powerful technique that should be used more widely

The Role of Monte Carlo The Role of Monte Carlo Simulations in Antimicrobial Simulations in Antimicrobial
PharmacologyPharmacologyMonte Carlo simulation for a suppression of
resistance for a 750 mg once-daily levofloxacin dose demonstrates target attainment 61.2% of the time, when an expectation is taken over the 404 strains of P aeruginosa shown previously
We cannot use the levofloxacin nosocomial pneumonia study for validation, because in this study, a second drug was added when P aeruginosa was detected

The Role of Monte Carlo The Role of Monte Carlo Simulations in Antimicrobial Simulations in Antimicrobial
PharmacologyPharmacologyHowever, simulations were also performed from the
data of Forrest et al (Antimicrob Agents Chemother 1993:37:1065-1072) for ciprofloxacin
These data were derived from patients with nosocomial pneumonia
Doses of 200 mg Q 12 h and 400 mg Q 12 h were simulated
Target attainments for suppression of resistance were 24.8% and 61.8%, respectively

Monte Carlo SimulationMonte Carlo SimulationSense and Non-SenseSense and Non-Sense
Drug Penetration Distribution

Levofloxacin Penetration into Epithelial Levofloxacin Penetration into Epithelial Lining Fluid (ELF) as Determined by Lining Fluid (ELF) as Determined by
Population Pharmacokinetic Modeling and Population Pharmacokinetic Modeling and Monte Carlo SimulationMonte Carlo Simulation
G.L. Drusano, S.L. Preston, M.H. G.L. Drusano, S.L. Preston, M.H. Gotfried, L.H. Danziger and K.A. RodvoldGotfried, L.H. Danziger and K.A. Rodvold
AAC 2002;46:586-589AAC 2002;46:586-589

The Role of Monte Carlo The Role of Monte Carlo Simulations in Antimicrobial Simulations in Antimicrobial
PharmacologyPharmacologyIt is important to ascertain the ability of drugs to
penetrate to their site of action, in this case, the ELF
Determination by penetration ratio often provides a biased estimate of penetration because of system hysteresis (penetration ratio changes with time)
We wished to employ population modeling and Monte Carlo Simulation to examine the penetration of levofloxacin into ELF

Levofloxacin Pulmonary Penetration Levofloxacin Pulmonary Penetration 95% Confidence Bounds - ELF95% Confidence Bounds - ELF
100
90
80
70
60
50
40
30
20
10
00 5 10 15 20
25 Time (hours)
Conce
ntr
ati
on (
mg/L
)
ELF

Levofloxacin Pulmonary Penetration Levofloxacin Pulmonary Penetration 95% Confidence Bounds - Plasma95% Confidence Bounds - Plasma
30
25
20
15
10
5
00 5 10 15 20 25
Time (hours)
Conce
ntr
ati
on (
mg/L
)
Plasma

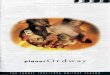
Steady State for a 750-mg Dose
Derived from Population Mean Parameter Estimates.
Penetration Ratio (ELF/Plasma) = 1.161
Time (h)
Conce
ntr
ati
on (
µg/L
)
Plasma
ELF
20
10
00 5 10 15 20 25
Levofloxacin Pulmonary Levofloxacin Pulmonary PenetrationPenetration

Levofloxacin PulmonaryPenetrationLevofloxacin PulmonaryPenetrationELF/Plasma RatioELF/Plasma Ratio
Penetration Ratio Distribution by Monte Carlo Simulation
Mean 3.18
Median 1.43
St. Dev. 5.71
95% CI 0.143 - 19.12
61% > 1.0

The Role of Monte Carlo The Role of Monte Carlo Simulations in Antimicrobial Simulations in Antimicrobial
PharmacologyPharmacology
Population modeling avoids the issue of system hysteresis and should be the preferred method of analysis for penetration studies
Levofloxacin penetrates well into the ELF with a mean penetration ratio exceeding 1.0
Use of Monte Carlo simulation displays the variability in penetration
Conclusions