Embed Size (px)
Citation preview

Monocyte Deactivation and Its Reversal in a Patient WithChemotherapy-Induced Leukopenia and Severe Systemic Infection
Halvard Bonig, MA, MD, Dieter Korholz, MD,* Christiane Lex, MD, Sonja Wolfel,and Ulrich Gobel, MD
Background. Serious infections constitute amajor problem for patients with cancer, andnew approaches must be found in dealing withthese. The pathophysiology of neutropenic in-fection is not well understood, although there issome evidence that, as in sepsis in the primarilyimmunocompetent host, a pro- and an antiin-flammatory phase can be discriminated. In therecent literature is described a series of nonneu-tropenic patients with sepsis in whom inter-feron-g was successfully administered duringthe immunoparalytic phase, a concept thatmight possibly be extended to immunocompro-mised hosts. Procedure. A 14-year-old patientwith RAEB-T/hypoplastic M2 and chemo-therapy-induced neutropenia developed a se-vere infection and continued to deteriorateclinically despite maximum supportive mea-sures, including broad antibacterial and anti-fungal coverage. On the basis of monocyte de-
activation this patient was considered to be inthe immunoparalytic phase of sepsis and con-sequently treated with 60 µg/m2 of interferon-gper day for 10 days. Results. The patient madea rapid clinical recovery, and biochemicalmarkers of infection improved promptly. At thesame time, the fraction of activated monocytesnormalized rapidly and stably. We hypothesizethat treatment with interferon-g effected thisrapid restoral of monocyte activation and thatmonocyte reactivation might have contributedto the patient’s prompt recovery from his severeinfection. Interferon-g treatment was well toler-ated. Conclusions. Immunostimulation with in-terferon-g might prove to be a valuable adju-vant treatment for patients with chemotherapy-induced neutropenia during the rare scenario ofinfection with immunoparalysis. Med. Pediatr.Oncol. 34:39–42, 2000. © 2000 Wiley-Liss, Inc.
Key words: monocyte deactivation; leukopenia; neutropenia infection
INTRODUCTION
With improved supportive therapies, care for the im-munocompromised patient is becoming an increasinglycommon problem in modern medicine. Be the immuno-suppression iatrogeneic, congenital, or infection-induced,among the many therapeutic challenges in these patients,infections are the major ones despite remarkable ad-vances in antimicrobial drugs. Thus new immunomodu-lating therapies must be developed that will further im-prove the outcome for immunodeficient patients with in-fection.
Systemic infection in the primarily immunocompetentindividual is currently looked at as a biphasic event [1].Whereas the first phase is dominated by proinflammatorycytokines, the second is characterized by what is com-monly termed “immunoparalysis,” i.e., monocyte deac-tivation and a predominance of immunosuppressive me-diators such as interleukin-10 (IL-10). This hypothesisfinds support in experimental data showing that mono-cytes stimulated with lipopolysaccharide will first secretethe proinflammatory cytokine tumor necrosis factor-a(TNF-a). As a counterregulation, in a second phase theautocrine induction of IL-10 was observed, which then
suppressed the production of proinflammatory cytokines[2]. Again in in vitro studies, it was later shown that theIL-10-induced failure to clear microorganisms can beovercome by interferon-g even in the presence of IL-10[3].
The intensity particularily of the latter phase of sepsisappears to determine the outcome for the patient. Thusvarious groups have demonstrated a significantly pooreroutcome in terms of survival for patients with elevatedIL-10 serum levels or monocyte deactivation [1,4–7].Consequently, Do¨cke et al. [8] have devised a treatmentprotocol according to which primarily immunocompetentpatients with less than 30% activated monocytes wereconsidered immunoparalytic and were treated with inter-feron-g. A rapid improvement was observed in the ma-jority of patients, both clinically and in terms of mono-
Department of Pediatric Hematology and Oncology, Heinrich-HeineUniversity Medical Center, Du¨sseldorf, Germany
*Correspondence to: Dieter Ko¨rholz, MD, Department of PediatricHematology and Oncology, Heinrich-Heine University Medical Cen-ter, Moorenstraße 5, D-40225 Du¨sseldorf, Germany.
Received 13 April 1998; Accepted 3 August 1999
Medical and Pediatric Oncology 34:39–42 (2000)
© 2000 Wiley-Liss, Inc.

cyte activation, which was expressed as percent HLA-DR+ cells within the CD14+ cell population.
There are today no systematic data available on mono-cyte activation and the effects of immunoregulatory cy-tokines in neutropenic infection in vivo. There is someevidence, however, that the regulation is somewhat simi-lar to that in nonneutropenic patients. Recently a strongcorrelation between elevated serum IL-10 levels and theprobability of succumbing to sepsis and multiorgan fail-ure was demonstrated in patients after allogeneic bonemarrow transplantation [10]. We report here for the firsttime on the adjuvant immunostimulatory treatment withinterferon-g of a patient with chemotherapy-induced leu-kopenia and severe infection.
MATERIALS AND METHODSCytokines
Interferon-g (Imukin) was purchased from Thomae(Biberach/Riß Germany) and administered by subcuta-neous injection at 2PM for 10 days (termed days 1–10).
Blood Counts
EDTA-blood was drawn daily around 9AM from acentral venous line, and blood counts were performed bya fully automatic blood cell counter (Coulter).
C-Reactive Protein (CRP)
Heparinized blood samples were drawn daily around 9AM from a central venous line, and CRP was measured byfully automatic standard laser nephelometry (Boehringer,Mannheim, Germany). At our institution, the range ofnormal for CRP is 0–1 mg/dl.
Serum Cytokine Levels
Heparinized blood samples were drawn daily around 9am from a central venous line, and plasma concentrationsof IL-10 and interferon-g were measured using commer-cially available ELISA kits (Laboserv, Gießen, Ger-many) and an automatic ELISA reader as described pre-viously [11]. Previous studies have established IL-10 lev-els below the detection limit of 5 pg/ml to be normal forhealthy human controls [12]. For a series of bone marrowrecipients, a more sensitive ELISA was used (detectionlimit 0.2 pg/ml), and even here values were generallybelow the limit of detection [10].
Monocyte Activation
Heparinized blood samples were drawn daily around 9AM from a central venous line. The cell suspension waslabeled with fluorescence-bound anti-CD14 and anti-HLA-DR antibodies (Becton-Dickinson, Heidelberg,Germany). Erythrocytes were cleared with BDLysis, andthe cells were analyzed by flow cytometry (FACScan;Becton-Dickinson) as described previously [13]. Mono-
cyte activation was calculated as percentage of HLA-DR+ cells within the CD14+ cell fraction [8]. Monocyteactivation of 30% was calledmonocyte deactivation[1, 8].
CASE REPORT
A 14 year-old-male patient had been dignosed withRAEB-T/hypoplastic M2 6 weeks before and had beenenrolled on the AML-BFM93 protocol [14]. Previously awell child, he was currently undergoing his inductionchemotherapy. Concurrently he became leukopenic (na-dir 0 cells/ml) and a few days into this became ill, de-veloped temperatures up to 40.6°C and CRP [5 mg/dl onday −8 (day 8 before the onset of interferon-g treat-ment)]. On the first day of this febrile episode, bloodcultures drawn from two lumina of the central line grewgram-positive cocci (Gemella morbilorum, an a-hemo-lyzing streptococcus). After initiation of therapy, culturesremained sterile at all times. A few days later,Clos-tridium difficile was found in the intestine and treatedwith oral vancomycin, furthermore, from the patient’ssputum and stools,Candida glabratawas isolated. Overthe course of 8 days, the patient continued to deterioratedespite broad antibacterial and antifungal treatment withteicoplanin, piperacillin/tazobactam, which were re-placed by imipenem/cilastatin after 2 days, metronidazol,and amphotericin B, initially in a conventional prepara-tion, which was later exchanged for a liposomal formu-lation. Although his clinical examination upon admissionhad been grossly normal, he went on to develop rhonchiover both lung bases after 6 days (day 2 before inter-feron-g treatment). On that day the chest X-ray film wasnormal, but a repeat scan 2 days later showed bilateralbasal infiltrates. At this point, the patient was most seri-ously ill, with a Karnowsky performance status#20. Hewas severely dyspnoeic and required continuous oxygeninsufflation via binasal cannulae to maintain adequateoxygenation (transcutaneous O2 saturation >90%). TheCRP had by this time reached 35 mg/dl, and the leuko-cyte count had slowly crept up to 1,300/ml. With a viewto this patient’s poor state of health, no diagnostic bron-choscopy was performed at this point, but a CT scantaken 1 week after the chest film showed patchy infil-trates suggestive of fungal pneumonia. This was provedby CT-guided transthoracic fine-needle lung biopsy tohave indeed been a fungus, namely,Aspergillussp. Itdeveloped some weeks after the episode under discus-sion, the patient having remained free of infection in theinterval.
Because neutrophil engraftment had not helped im-prove the patient’s dismal state of health, at this point theauthors decided to measure monocyte activation and se-rum IL-10 and, should these be deranged, to enroll thispatient on a compassionate protocol with interferon-g ashad previously been described by Do¨cke et al. for non-
40 Bonig et al.
neutropenic patients [8]. Informed consent was obtainedfrom the patient’s parents.
Treatment with 60mg/m2 (equivalent to 1.8 × 106
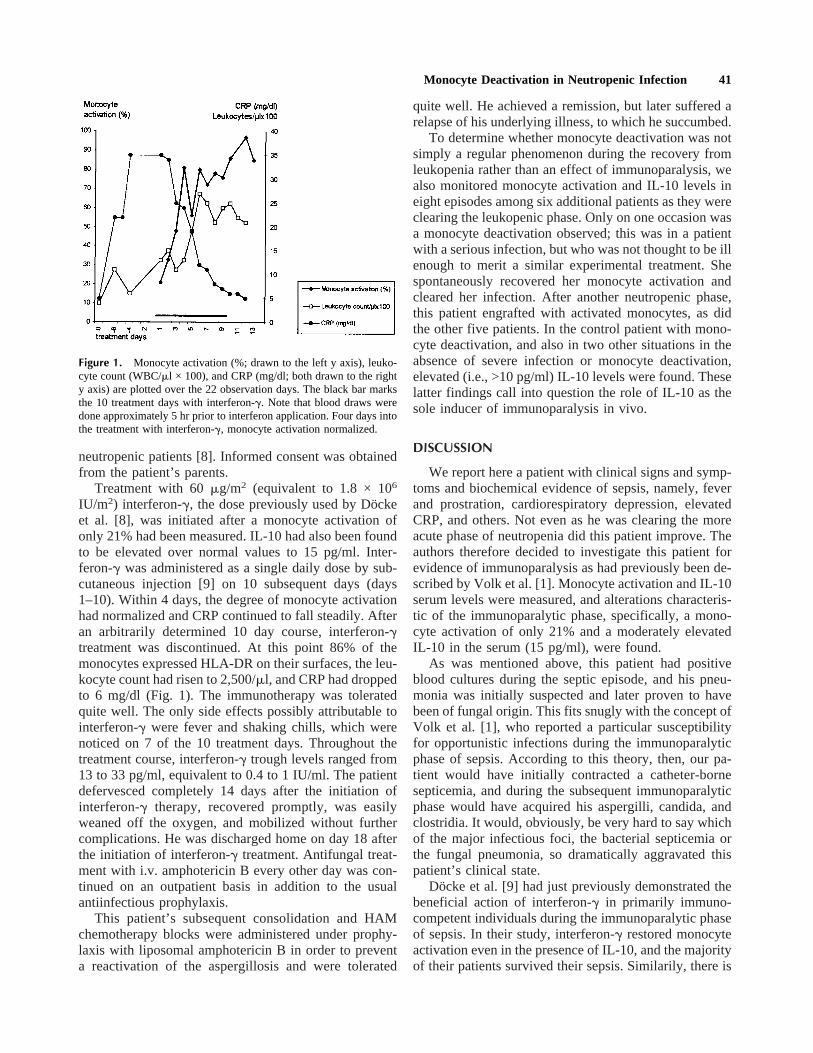
IU/m2) interferon-g, the dose previously used by Do¨ckeet al. [8], was initiated after a monocyte activation ofonly 21% had been measured. IL-10 had also been foundto be elevated over normal values to 15 pg/ml. Inter-feron-g was administered as a single daily dose by sub-cutaneous injection [9] on 10 subsequent days (days1–10). Within 4 days, the degree of monocyte activationhad normalized and CRP continued to fall steadily. Afteran arbitrarily determined 10 day course, interferon-gtreatment was discontinued. At this point 86% of themonocytes expressed HLA-DR on their surfaces, the leu-kocyte count had risen to 2,500/ml, and CRP had droppedto 6 mg/dl (Fig. 1). The immunotherapy was toleratedquite well. The only side effects possibly attributable tointerferon-g were fever and shaking chills, which werenoticed on 7 of the 10 treatment days. Throughout thetreatment course, interferon-g trough levels ranged from13 to 33 pg/ml, equivalent to 0.4 to 1 IU/ml. The patientdefervesced completely 14 days after the initiation ofinterferon-g therapy, recovered promptly, was easilyweaned off the oxygen, and mobilized without furthercomplications. He was discharged home on day 18 afterthe initiation of interferon-g treatment. Antifungal treat-ment with i.v. amphotericin B every other day was con-tinued on an outpatient basis in addition to the usualantiinfectious prophylaxis.
This patient’s subsequent consolidation and HAMchemotherapy blocks were administered under prophy-laxis with liposomal amphotericin B in order to preventa reactivation of the aspergillosis and were tolerated
quite well. He achieved a remission, but later suffered arelapse of his underlying illness, to which he succumbed.
To determine whether monocyte deactivation was notsimply a regular phenomenon during the recovery fromleukopenia rather than an effect of immunoparalysis, wealso monitored monocyte activation and IL-10 levels ineight episodes among six additional patients as they wereclearing the leukopenic phase. Only on one occasion wasa monocyte deactivation observed; this was in a patientwith a serious infection, but who was not thought to be illenough to merit a similar experimental treatment. Shespontaneously recovered her monocyte activation andcleared her infection. After another neutropenic phase,this patient engrafted with activated monocytes, as didthe other five patients. In the control patient with mono-cyte deactivation, and also in two other situations in theabsence of severe infection or monocyte deactivation,elevated (i.e., >10 pg/ml) IL-10 levels were found. Theselatter findings call into question the role of IL-10 as thesole inducer of immunoparalysis in vivo.
DISCUSSION
We report here a patient with clinical signs and symp-toms and biochemical evidence of sepsis, namely, feverand prostration, cardiorespiratory depression, elevatedCRP, and others. Not even as he was clearing the moreacute phase of neutropenia did this patient improve. Theauthors therefore decided to investigate this patient forevidence of immunoparalysis as had previously been de-scribed by Volk et al. [1]. Monocyte activation and IL-10serum levels were measured, and alterations characteris-tic of the immunoparalytic phase, specifically, a mono-cyte activation of only 21% and a moderately elevatedIL-10 in the serum (15 pg/ml), were found.
As was mentioned above, this patient had positiveblood cultures during the septic episode, and his pneu-monia was initially suspected and later proven to havebeen of fungal origin. This fits snugly with the concept ofVolk et al. [1], who reported a particular susceptibilityfor opportunistic infections during the immunoparalyticphase of sepsis. According to this theory, then, our pa-tient would have initially contracted a catheter-bornesepticemia, and during the subsequent immunoparalyticphase would have acquired his aspergilli, candida, andclostridia. It would, obviously, be very hard to say whichof the major infectious foci, the bacterial septicemia orthe fungal pneumonia, so dramatically aggravated thispatient’s clinical state.
Docke et al. [9] had just previously demonstrated thebeneficial action of interferon-g in primarily immuno-competent individuals during the immunoparalytic phaseof sepsis. In their study, interferon-g restored monocyteactivation even in the presence of IL-10, and the majorityof their patients survived their sepsis. Similarily, there is
Figure 1. Monocyte activation (%; drawn to the left y axis), leuko-cyte count (WBC/ml × 100), and CRP (mg/dl; both drawn to the righty axis) are plotted over the 22 observation days. The black bar marksthe 10 treatment days with interferon-g. Note that blood draws weredone approximately 5 hr prior to interferon application. Four days intothe treatment with interferon-g, monocyte activation normalized.
Monocyte Deactivation in Neutropenic Infection 41

at least some evidence for the existance of the immuno-paralytic phase of sepsis in patients with chemotherapy-induced neutropenia. Thus, for patients after allogeneicbone marrow transplantation, the authors have recentlyshown a correlation between elevated IL-10 serum levelsand the risk of succumbing to infections and multiorganfailure [10]. In summary, this patient was critically ill,and he fulfilled the criteria of “immunoparalysis,” whichpredicted an untoward outcome. Thus, the authors de-cided to treat him with interferon-g. We hypothesize thatthe rapid monocyte reactivation was largely attributableto this experimental therapy, which might thus have as-sisted this patient’s rapid recovery: The markedly higherdegree of monocyte activation might have contributed tothe clearance of microorganisms. The defervescence af-ter day 14 might have been due more to the discontinuedinterferon-g treatment than to the clearing infection.Clinical and experimental trials must attempt to establishthe safety and efficacy of interferon-g as an immuno-stimulatory drug during the immunoparalytic phase ofsepsis in the immunocompromised host.
ACKNOWLEDGMENTS
We acknowledge the excellent work of the medicaland nursing staff on the pediatric oncology ward and theproficient technical assistance of Ms. A. Klein-Vehneand Ms. P. Genutt. D.K. and H.B. are supported by DFGSonderforschungsbereich 506; H.B. and C.L. are sup-ported by Elterninitiative Kinderkrebsklinik e.V.
REFERENCES
1. Volk HD, Reinke P, Krausch D, et al. Monocyte deactivation—rationale for a new treatment strategy in sepsis. Intens Care Med1996;22:S474–S481.
2. Platzer C, Meisel C, Vogt K, Platzer M, Volk HD. Upregulation
of monocytic IL-10 by tumor necrosis factor-alpha and cAMPelevating drugs. Int Immunol 1994;7:517–523.
3. Donnelly RP, Freeman SL, Hayes MP. Inhibition of IL-10 expres-sion by IFN-gamma up-regulates transcription of TNF-alpha inhuman monocytes. J Immunol 1995;145:3762–766.
4. Hummel M, Docke WD, Friedel N, von Baehr R, Hetzer R, VolkHD. Monitoring of the cellular immune system in patients withbiventricular assist devices awaiting cardiac transplantation. ClinTransplant 1994;8:59–66.
5. Docke WD, Syrbe U, Meinicke A, et al. Improvement of monoyticfunction–a new therapeutic approach in sepsis? In: Reinhart K,Eyrich K, Sprung CL, editors. Update in intensive care and emer-gency medicine. Berlin: Springer; 1994. p 473–488.
6. Westendorp RGJ, Langermans JAM, Huizinga TWJ, et al. Geneticinfluence on cytokine production and fatal menigococcal disease.Lancet 1997;349:170–173.
7. Munoz C, Carlet J, Fitting C, Misset B, Bleriot JP, Cavaillon JM.Dysregulation of in vitro cytokine production by monocytes dur-ing sepsis. J Clin Invest 1991;88:1747–1754.
8. Docke WD, Randow F, Syrbe U, et al. Monocyte deactivation inseptic patients: restoration by IFN-gamma treatment. Nature Med1997;3:678–681.
9. Amluish A, Urba W, Longo D. The determination of an immu-nologically active dose of interferon-gamma in patients withmelanoma. J Clin Oncol 1988;6:434–445.
10. Hempel L, Ko¨rholz D, Nußbaum P, Bo¨nig H, Burdach S, Zintl F.High interleukin 10 serum levels are associated with fatal outcomein patients after bone marrow transplantation. Bone MarrowTransplant 1997;20:365–368.
11. Korholz D, Banning U, Bo¨nig H, et al. The role of interleukin-10(IL-10) in IL-15-mediated T-cell responses. Blood 1997;90:4513–4521.
12. Rutella S, Rumi C, Testa U, et al. Inhibition of lymphocyte blas-togenic response in healthy donors treated with recombinant hu-man granulocyte-stimulating factor (rhG-CSF): possible role oflactoferrin and interleukin-1 receptor antagonist. Bone MarrowTransplant 1997;20:355–364.
13. Korholz D, Kunst D, Hempel L, et al. Humoral immunodeficiencyin patients after bone marrow transplantation. Bone MarrowTransplant 1996;18:1123–1130.
14. Ritter J, Creuzig U, Schellong G. Treatment results of three con-secutive German childhood AML trials. Leukemia 1992;6S2:59–62.
42 Bonig et al.