Embed Size (px)
Citation preview

BioMed CentralHuman Resources for Health
ss
Open AcceResearchMonitoring and evaluation of human resources for health: an international perspectiveKhassoum Diallo, Pascal Zurn, Neeru Gupta and Mario Dal Poz*Address: Department of Health Service Provision, World Health Organization, Geneva, Switzerland
Email: Khassoum Diallo - [email protected]; Pascal Zurn - [email protected]; Neeru Gupta - [email protected]; Mario Dal Poz* - [email protected]
* Corresponding author †Equal contributors
AbstractBackground: Despite the undoubted importance of human resources to the functions of healthsystems, there is little consistency between countries in how human resource strategies aremonitored and evaluated. This paper presents an integrated approach for developing an evidencebase on human resources for health (HRH) to support decision-making, drawing on a frameworkfor health systems performance assessment.
Methods: Conceptual and methodological issues for selecting indicators for HRH monitoring andevaluation are discussed, and a range of primary and secondary data sources that might be used togenerate indicators are reviewed. Descriptive analyses are conducted drawing primarily on onetype of source, namely routinely reported data on the numbers of health personnel and medicalschools as covered by national reporting systems and compiled by the World Health Organization.Regression techniques are used to triangulate a given HRH indicator calculated from different datasources across multiple countries.
Results: Major variations in the supply of health personnel and training opportunities are found tooccur by region. However, certain discrepancies are also observed in measuring the same indicatorfrom different sources, possibly related to the occupational classification or to the sources'representation.
Conclusion: Evidence-based information is needed to better understand trends in HRH. Althougha range of sources exist that can potentially be used for HRH assessment, the information that canbe derived from many of these individual sources precludes refined analysis. A variety of datasources and analytical approaches, each with its own strengths and limitations, is required to reflectthe complexity of HRH issues. In order to enhance cross-national comparability, data collectionefforts should be processed through the use of internationally standardized classifications (inparticular, for occupation, industry and education) at the greatest level of detail possible.
BackgroundThe importance of sound empirical evidence for informedpolicy decision-making and the monitoring of progresstowards achieving health system goals and human re-
sources for health (HRH) development in particular iswidely recognized. Human resources for health are centralto managing and delivering health services, and in mostcountries account for a high proportion of national
Published: 14 April 2003
Human Resources for Health 2003, 1:3
Received: 2 April 2003Accepted: 14 April 2003
This article is available from: http://www.human-resources-health.com/content/1/1/3
© 2003 Diallo et al; licensee BioMed Central Ltd. This is an Open Access article: verbatim copying and redistribution of this article are permitted in all media for any purpose, provided this notice is preserved along with the article's original URL.
Page 1 of 13(page number not for citation purposes)

Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
budgets assigned to the health sector. Defining preciselyHRH can help to identify opportunities and constraintsand the potential impact of HRH on population health.HRH analysis can also be used as a tool to sensitize polit-ical and social stakeholders to the importance of address-ing workforce issues, contributing to the consideration ofHRH issues on the public and political agenda [1].
Despite the undoubted importance of human resources tothe functions of health systems, there is little consistencybetween countries in how HRH strategies are monitoredand evaluated. In terms of health system inputs, interna-tional assessments of health personnel or other non-mon-etary resources remain less widespread than comparisonsof health care expenditures [2]. The global evidence onpolicy options for health systems tends to be weak. It hasbeen acknowledged that no country has discovered anideal model, and appropriate policies differ widely acrosscountry settings [3].
While each country's situation is unique, a comprehensiveframework for examining the contribution of HRH to theachievement of health system goals can be a useful tooltowards developing evidence-based policy options. TheWorld Health Organization's analytical framework forhealth systems performance assessment describes the roleof HRH in each of four main functions of health systems[4]. While the approaches used to implement this frame-work have been the subject of much scientific and politi-cal controversy [5–7], a general point of consensus is thecritical role of HRH in ensuring that services are deliveredeffectively.
At the same time, despite the high profile accorded toHRH within both the developed and developing worlds,there has tended to be less discourse on broader healthpolicies and the more specific HRH interventions requiredto achieve them. Often HRH policy and planning havebeen simply (and mistakenly) equated with training [8].However, recruitment and retention of HRH may be af-fected by a number of different factors; for one, poorworking conditions may be contributing to both numeri-cal and distributional imbalances in many countries [9].Assessing HRH impacts on the delivery of health care serv-ices should thus also take into account factors exogenousto the health system, including the heterogeneity of la-bour markets and the mechanisms for adjustment be-tween supply and demand for health personnel.
This paper presents an integrated approach for developingan evidence base on HRH to support decision-making.Drawing on the WHO framework for health systems per-formance assessment, we focus on the methods and mate-rials for monitoring HRH inputs. First we examineconceptual and methodological issues for selecting rele-
vant indicators. Then we discuss means for enhancingcross-national comparability. We then critically review themain data sources that might be used to generate indica-tors. Lastly, we touch on statistical applications andpresent some empirical findings for illustrative purposes.
Framework and indicators for HRH assessmentThe WHO framework on health system performance as-sessment is based on the concept of health action, and en-capsulates any set of activities whose primary intent is tomaintain or improve population health, enhance the sys-tem's responsiveness to the expectations of the popula-tion, and assure fairness of financial contributions to thesystem. To achieve these main goals, four functions areperformed by health systems: financing, stewardship,service provision and resource generation (see Fig. 1).
In particular, health system financing refers to the processby which revenues are collected from primary and second-ary sources, accumulated in fund pools and allocated toprovider activities. Stewardship involves the aspects of set-ting, implementing and monitoring the rules for thehealth system; assuring a level playing field for all actorsin the system (particularly purchasers, providers and pa-tients); and defining strategic directions for health systemsas a whole. Service provision is the combination of inputsinto a production process that takes place in a particularorganizational setting and that leads to the delivery of in-terventions. Resource generation refers to the production ofinputs – particularly human resources, knowledge, andphysical resources such as facilities, equipment and con-sumables – for the provision of services. While HRH aredirectly or indirectly related to each of these four func-tions and influenced by them, in this paper we will
Figure 1Framework for the assessment of health systems performance
Inputs•Financial resources•Human resources•Capital stocks•Consumables•Information, knowledge
Functions•Financing•Stewardship•Services provision •Resources generation
Intermediate goal•Effective coverage
Goals•Average level of health•Health inequalities•Responsiveness•Fair financial contributions
Page 2 of 13(page number not for citation purposes)

Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
concentrate on assessing HRH inputs as they pertain tothe latter two.
Different elements should be borne in mind when select-ing and calculating appropriate indicators for HRH mon-itoring and evaluation. From the perspective of humanresources as an input to health action, HRH can be broad-ly defined as "the stock of all individuals engaged in thepromotion, protection or improvement of populationhealth" [4]. This encompasses those working across differ-ent domains of health systems: public and private sectors;clinical, research and public health interventions; preven-tive and curative personal care; etc.
In general terms, a number of criteria have been identifiedas crucial for selecting indicators, including policy rele-vance, reliability, validity, simplicity and ability to aggre-gate/disaggregate information [10,11]. Indicators onHRH are used for various purposes, such as measures ofplanning, implementing, monitoring and evaluating pol-icies. To facilitate both the data collection and analysisprocesses, it is important to focus on a limited and essen-tial number of indicators that are comparable and meas-urable regularly using standard data sources.
A series of components for selecting HRH indicators forthe performance of the services provision and resourcesgeneration functions can be found in Fig. 2. The proposedlist follows the general framework of health system per-formance assessment, classified in terms of the level ofachievement, distribution (equity) and efficiency (pro-ductivity) of HRH [12]. This list is not meant to be exhaus-tive, nor is it necessarily expected that all these indicatorswill be used in any given HRH assessment. This will de-pend on the user's particular circumstances, with the even-tual number reduced to an essential minimum inaccordance with data availability and quality. This basic
basket of indicators is also not intended to be restrictive,and focuses on indicators appropriate for quantitativeanalyses. Other indicators may be used as appropriate inthe context of national and local operations or differenttypes of study designs.
Detailed descriptions of the key indicators, including for-mulas and potential sources for measurement, can befound in the 1. Depending on the data sources and classi-fications used, many of these indicators can bedisaggregated by occupation (physicians, nursing andmidwifery professionals, etc.), by administrative units(districts, provinces or states, etc.) or other sociodemo-graphic characteristics (age, sex, etc.). At the same time, in-dicators for some topics highly relevant to HRH analysismust be further investigated and tested. This includesmeasures of labour relations or dissatisfaction (such aswork stoppages or other absences), regulation of healthprofessions (such as rules to ensure standards of trainingand practice), financing of HRH production (such as fair-ness of financing for training programmes), risk factors tohealth workers (such as susceptibility to violence or tocontracting infectious diseases including HIV/AIDS) andphysical conditions (such as lack of materials or state ofthe workplace).
Indicators of the health service provision functionLevelA range of indicators can be defined to measure specificaspects of the level of HRH as an input to improving theprovision of health services. The starting point of manyHRH assessments is the stock of health personnel. Indica-tors of stock or available supply are usually expressed interms of densities of HRH with regard to the total popula-tion or the population of economically active age. The dis-tinction lies in the capacity of the system versus theallocation of human resources to the system compared tothose available. Skill-mix indicators are also commonlyused to measure various HRH components in relativeterms. These indicators, which can provide a pointer ofthe priorities and capacities of the system, compare onesubgroup to another according to assumed differences inskill levels or skill specializations, such as the ratio of phy-sicians to nurses, or of specialists to generalists.
External migration of health workers, especially highlyskilled ones, has long been recognized as a problem forensuring appropriate coverage of essential services insome countries. The proportions of foreign-born or for-eign-trained among the national HRH stock constitutesimple but informative indicators on the importance ofinternational immigration within the health sector. Onthe other hand, they fail to capture the impact of emigra-tion on sending countries or migratory trajectories amongworkers, which tend to be difficult to measure because of
Figure 2Selected indicators for HRH assessment
Level Distribution Efficiency
Health services provision
� Stock of HRH
� Skills mix
� Migration
� Labour force activity
� Institutional sector
� Earnings
� Distribution of HRH bylocation / gender / other
� Gender gap in earnings
� Provider productivity
Resources generation
� Renewal and loss of HRH
� Education and training
� Distribution of entrantsby location / gender /other
� Training costs
Page 3 of 13(page number not for citation purposes)

Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
a general lack of reliable and comparable data from sourcecountries.
The participation or not of those with a health-related vo-cational background in the labour market, and their ensu-ing participation in the health industry in particular, offerimportant information for health policy purposes. Indica-tors on labour force activities capture three main ele-ments: participation (the proportion of individuals withhealth-related skills currently in the labour force), em-ployment opportunities (the proportion with health-re-lated skills currently employed), and retention (theproportion with health-related skills currently working ina health-related industry). Complementary indicatorsmay include the proportion of health workers engaged ona part-time basis, or the proportion with more than onecurrent job.
Another aspect of labour force activity is the categoriza-tion of institutional sector of the work location, usually aspublic or private sector operations. The public sector in-cludes government-operated facilities and services, whilethe private sector consists of for-profit or not-for-profit ac-tivities implemented by private agents or businesses aswell as nongovernmental organizations and religious orother charitable institutions. However, the distinction isnot always clear-cut, with some health systems havingpublicly-owned facilities staffed mainly by privately oper-ating health workers, or large numbers of health profes-sionals working partly in the private sector and partly inthe public sector (with this arrangement sometimes beingpart of their contract with the latter).
Information on income or wages among health workers isof value when discussing countries' health care financingoptions. In many countries wage costs (salaries, bonusesand other payments) are estimated to represent between65% and 80% of renewable health system expenditures[13,14]. A common indicator is the average annual in-come or occupational earnings. This can be measured ingross or net terms, depending on the nature of the datasource. In order to account for differences in workingtimes, an alternative indicator might be constructed as av-erage hourly wages (gross or net). Other complementaryindicators for assessing monetary incentives could refer tomodes of remuneration (for example, the proportion ofhealth care providers paid by salary, fee-for-service or cap-itation), or multiplicity of sources of remuneration (suchas the proportion of health workers receiving wages fromboth public and private sector jobs).
Distribution (equity)A breakdown of HRH by workers' sociodemographic orother characteristics can offer insight into imbalanceswithin the health workforce. Inequitable occupational
distributions by geographical location and by gender con-stitute the main areas of health policy concern for manycountries. Geographical imbalances, and especially short-ages in rural or poor areas, are reported to have a numberof adverse consequences for health systems performance.Other complementary indicators for assessing equity inthe health workforce include distributions of vacancyrates, turnover rates and relative wage rates by location (orother criteria).
Occupational clustering by gender is regarded as impor-tant not only for assessing equity in human resources op-portunities, but also for health services planning. Adistinctive feature of HRH in many countries is the highproportion of workers who are women. Studies haveshown that increased participation of women in the med-ical field may be accompanied by differences in workingpatterns: female physicians are likely to work fewer hoursthan their male counterparts [15,16] and to present differ-ent styles of care provision that may be reflected in the lev-els of patient participation [17]. Moreover it has beensuggested that certain female-dominated occupations, no-tably in nursing and midwifery, often are not given a mar-ket value commensurate with their skill level, as the workis seen simply as "women's work" [18]. Analysis of genderimbalances in average occupational earnings may revealthe extent to which women and men have equal opportu-nities in career choice. Indices of inequality might also beused to highlight extremes across income distributions,which may be masked when considering averages alone.
Efficiency (productivity)Increasing the productivity of health workers has beenidentified as one of the most cost-effective ways to im-prove health system capacity and performance [19]. Indi-cators of productivity include measures such as the ratioof workers' time spent providing health care services ascompared to non-care services (meetings, travelling, re-porting, etc.), the average number of ambulatory visits perworking hour among providers of direct patient care, orthe average number of immunizations administered perday by a given provider. Such indicators may reflect in partthe intensity of work activities among health care provid-ers, but different values for the indicators may also reflectdifferences in the underlying reality – for example, linkedto the manner in which work is organized or the patternof ailments. Complementary indicators of productivitymay include the average number of hours worked perweek among health workers, the ratio of health workersengaged on a part-time basis versus full-time basis, or theratio of average working time among clinical staff to less-costly support staff.
Page 4 of 13(page number not for citation purposes)

Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
Indicators of the resource generation functionLevelThe proportion of those starting or completing training ina health-related field with respect to the total HRH stockoffers insight into the renewal and loss patterns of thehealth workforce. Monitoring information about en-trants/graduates at health training institutions enables an-ticipation of future HRH supplies in relation to exits dueto retirement or external migration. Such indicators maybe disaggregated by skill specialization, such as the ratioof entrants/graduates of medical programmes versus nurs-ing programmes. In some cases, where information onnumbers of academic entrants/graduates is difficult to ob-tain, a substitute indicator may be used as the proportionof the total HRH stock in the youngest age groups. Thisproxy measure can be used to assess the importance ofageing in the health workforce. However, cross-nationaland cross-occupational comparability may be hinderedby differences in the average duration or age of academictraining, where the number of trainees who eventuallyseek employment in the (national) health sector is low,where the number of workers trained abroad is high, orwhere there is considerable mobility in and out of theworkforce over the active age span.
Assessing the education and training levels of the healthworkforce is a key element for policy-makers. The advanceof complex health systems organizations and medicalknowledge, as well as the introduction of sophisticatedtechnology, mean that improvements in populationhealth and welfare increasingly depend on the degree ofeducational attainment and renewal and maintenance oftechnical capacity among the health workforce. Educa-tion-relevant indicators for HRH assessment include theproportion of health workers with a tertiary-level educa-tional attainment and the proportion having undertakena continuous education course or programme within aspecific period. It should be noted that such indicatorsmay fail to capture the notion of quality of education andtraining and its adequacy regarding the needs of the pop-ulation and the health care system.
Distribution (equity)Equity indicators for resource generation show the pro-portional distribution of new entrants or graduates athealth training institutions according to different criteria– for example, the distribution of health trainees accord-ing to gender, or their distribution in urban versus ruralareas. Monitoring the latter can be especially crucial forassessing policy impacts in terms of imbalances and in-centives for staffing in remote geographical locations.
EfficiencyThe decision to train more students in the field of healthhas important financial consequences. The training costs
per student might be substantial, especially for physiciansand specialists, who must attend medical school for sever-al years to acquire the proper qualifications. Measures ofthe current average and marginal financial cost of trainingallow projections of the total costs of training more stu-dents, and can be used to compare training costs withinand across countries. This can refer to vocational trainingat tertiary-level educational institutions or through con-tinuous education programmes. A complementary effi-ciency indicator could be the attrition rate at healthtraining institutions – that is, the ratio of entrants to grad-uates per academic programme.
Cross-national comparability in HRH monitoringThe range of indicators necessary to describe the profileand monitor the progress of HRH is extensive, integratingmany aspects such as occupation, industry, training andothers. A number of challenges must be faced in enhanc-ing cross-national comparability. The roles of health careworkers vary from country to country, and the professionsalso have different national histories and cultures. It canbe difficult to categorize data when professional bounda-ries are not well defined.
The use of internationally standardized classifications –such as the International Standard Classification of Occu-pations (ISCO), the International Standard IndustrialClassification of all Economic Activities (ISIC), and theInternational Standard Classification of Education(ISCED) [20–22] – can provide the backbone for compar-ing HRH between countries and over time. Classificationsprovide a framework for the description and comparisonof statistics by categorizing items according to sharedcharacteristics. But international classifications are notwidely used in health research, and their potential as toolsfor defining the scope of the health system including hu-man resources and for conducting HRH analyses has gen-erally not been met. Different user areas may havedifferent degrees of interest in the various elements. Stud-ies of health systems and HRH in many countries still ap-ply classifications that are not always comparable withstandardized categorizations, although use of or mappingto ISCO and other international standards is becomingmore widespread. Even when international classificationsare used, they are often not used to full advantage.
The International Labour Office's 1988 revision of theISCO classification system (ISCO-88) pools occupationaltitles into a hierarchical four-digit system that can be ag-gregated to progressively broader groups, representing avalue set with respect to the type of work performed or tobe performed. Occupations are specified according to theprecision needed in major (one-digit level), sub-major(two-digit level), minor (three-digit level) and unit (four-
Page 5 of 13(page number not for citation purposes)

Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
digit level) groups. The basic criteria used to define thesystem of major, sub-major, minor and unit groups arethe "skill level" and "skill specialization" required to carryout the tasks and duties of the occupations [20].
The main occupations of interest with a health care-relat-ed specialization fall within two of the ten major groups:group 2 "professionals" (generally well-trained workers injobs that normally require a university or advanced-leveldegree for recruitment) and group 3 "technicians and as-sociate professionals" (generally requiring skills at a terti-ary non-university educational qualification level).Health practitioners in the professional group includephysicians, nursing and midwifery professionals and oth-er health professionals, such as dentists, pharmacists andveterinarians. Among associate professionals are modernhealth associate professionals (such as medical assistants,dental assistants, physiotherapists, opticians and sanitari-ans), nursing and midwifery associate professionals andtraditional medicine practitioners.
For HRH analysis purposes, it is essential to have jobs clas-sified at least according to the three-digit ISCO-88 level orequivalent. Information at the two-digit level alone doesnot allow distinction of health occupations from other lifesciences occupations. Moreover, different health occupa-tions can be separately identified only at the four-digit lev-el, such as physicians (code 2221) from other healthprofessionals. And certain related occupations aside frommedical and nursing practitioners are likewise identifiableonly at the four-digit level, in particular medical equip-ment operators (code 3133), health and safety inspectors(code 3152) and institution-based personal care workers(code 5132).
Even when occupations are classified according to ISCO-88, comparability issues may arise. For example, whilephysicians are unambiguously identified among the pro-fessionals major group (code 2221), the classification ofnurses and midwives is less clear, crossing two majorgroups where they could be recorded: "nursing and mid-wifery professionals" (code 223) or "nursing and mid-wifery associate professionals" (code 323). Thisdistinction was designed to reflect differences in tasks andduties that may be a consequence of differences in workorganization as well as in education and training. In somecountries, the possibility of distinguishing between thetwo typologies of nurses and midwives remains of limitedrelevance; inadequacies in the reporting system orincomparability of the education systems and measures oftechnical capacity may mean that some nursing and mid-wifery jobs do not fit easily into these two categories.
In addition, health systems employ a large number ofworkers with non-health occupational backgrounds, such
as administrators, accountants, drivers and other supportstaff. Capturing this wider range of workers entails consid-eration of occupations across all of the major ISCO-88groups, so further information on industry may be re-quired. The ISIC classification can form a basis for suchanalysis. Using ISIC's latest revision requires informationcompiled at the three-digit level, in order to be able to dis-tinguish the health sector from social work activities [21].
Other relevant classifications include ISCED, a cross-na-tionally comparable instrument for definitions of levelsand fields of education and training [22]; the CentralProduct Classification, covering all goods and servicesthat are produced or traded, including health services[23]; and the International Classification of Status in Em-ployment, designed to facilitate cross-national compara-bility in the production and presentation of statistics onjobs by types of economic risk and levels of authority [24].Using combinations of these classifications when describ-ing HRH it will be possible to identify, for example, em-ployment in non-health activities among those with ahealth-related education, and employment in health ac-tivities with jobs that do not require medical or nursingskills.
In practice, the precision of coding to such standard clas-sification systems will depend largely on the level of spec-ification in the raw data. Accurate occupational, industryand training information is vital in assessing HRH, start-ing with the most basic of indicators on size and compo-sition of the health workforce. Many countries usenational coding systems for occupation and other perti-nent areas. However, data on health workforces are moredirectly comparable once differences in the organizationof national health systems and the educational systemsfor health occupations are attenuated through harmo-nized classifications. Use among all countries of ISCO-88to the greatest detail possible, or mapping of national clas-sifications to this standard, would greatly improve cross-national comparability and facilitate use of health work-force information for informed decision-making.
Potential data sourcesEffective planning and management of HRH depend vital-ly on the availability of high quality and timely statistics.Despite a prevailing view that statistics on HRH are scarce,the sources that potentially can produce information rele-vant to this issue are quite diverse. Routine administrativerecords, censuses and household and establishment sam-ple surveys are among the sources that allow researchersand decision-makers to calculate different indicators ac-cording to their goals and needs. Some of the publishedempirical studies on HRH have drawn on information inhealth-related professional registries [25], national ac-counts gathered by agencies of the United Nations system
Page 6 of 13(page number not for citation purposes)

Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
[26], or records of medical schools and faculties [27].Other research agendas have focused on using demo-graphic census data [28,29], labour force survey findings[30], or specialized surveys of health human resources[31].
Two fundamental challenges for data compilation at theinternational level are to identify appropriate sources andto gain timely access to the data [32]. Frameworks havebeen formulated that can support efforts to coherentlycombine statistics from different sources and for differentunits [33]. However, in many countries, information onthe health workforce is fragmented, and the statistics gen-erated by these various sources have received limited pub-lic dissemination and generally been underused. Even incountries where updated data are available, it may be dif-ficult to establish the size and composition of the healthworkforce because the collection and dissemination ofrepresentative occupational data using the ISCO-88standard at the three- or four-digit level (or other compa-rable national classification) remains less widespread.
Population censusesDemographic census results can be a valuable source forstatistics describing HRH characteristics, in particular ifthey are available as microdatasets. They can provide ac-curate information on the total stock and composition ofthe health workforce as well as differentials by spatialunits (administrative districts, states or provinces, regions,etc.), demographic characteristics (age, sex, migration sta-tus) and other socioeconomic characteristics (educationalattainment, income level, sector of activity). Unlike surveydata, censuses do not suffer from problems of sample siz-es that are too small to allow estimates with the requiredprecision, so they give researchers greater leverage to dis-aggregate indicators for various population and adminis-trative subgroups. On the other hand, due to theirgenerally shorter questionnaires, censuses generally con-tain only limited information on other aspects of labourforce activities valuable for in-depth analyses (such as sec-ondary employment or working hours). They are alsocharacterized by longer periodicity (usually only once eve-ry ten years), and the results therefore are useful primarilyfor describing the structure of HRH, in the context of thestructure of the population, and related long-termchanges.
Many countries have collected information on occupationin their censuses for a long time. However, in manydeveloping countries, especially in Africa, census resultsremain a greatly underused resource for HRH assess-ments, and microdata have not been available. Two mainproblems arise. First, the quality and content of censusdata can vary widely from country to country, and some-times from one census to another within the same coun-
try, making cross-national and time-trend analysesdifficult. For instance, with regard to the last two censusesin Kenya, occupational information was collected in the1989 round but not in 1999. Second, as already men-tioned, where available, it is necessary to have occupation-al information detailed at least at the three-digit ISCO-88classification level or equivalent to obtain separate identi-fication of health workers. Many countries disseminatestatistics only at the one-digit or two-digit level. Even fordeveloped countries, the classifications used for compil-ing many indicators relevant to HRH assessment – such asoccupation, education and industry – differ from onecountry to another [29].
For some countries, analyses of census data can be facili-tated through collaborative research projects aiming toharmonize microdata variables and structures for publicuse. Two main census microdata providers can be identi-fied: the Integrated Public Use Microdata Series (IPUMS)and the African Census Analysis Project (ACAP) [34,35].Such projects process census microdata series in machine-readable form for multiple countries, and help dissemi-nate the relevant documentation for scholarly research.Information on HRH drawing on occupation data is cur-rently available for four out of the six countries for whichmicrodata are disseminated through the IPUMS-Interna-tional project (Kenya, Mexico, United States of Americaand Vietnam) [34]. ACAP has archived census microdatafrom at least six countries with occupation data detailedminimally at the three-digit ISCO level or equivalent(Gambia, Kenya, Mali, Nigeria, South Africa and Ugan-da), with plans to eventually facilitate distribution of thedata with the aid of tools being developed for guided sta-tistical application [35].
Sample surveysRepresentative household or establishment sample sur-veys, such as labour force or facility surveys, can provideuseful information on various aspects of the health work-force. Depending on the sampling frame and implemen-tation, surveys may be representative of the population orhealth service delivery environment, and national gener-alization is possible.
Labour force surveys are the key instruments used by na-tional statistical offices to obtain estimates regarding em-ployment characteristics of the population. The target isusually the adult resident population classified as eitheremployed, unemployed or not being in the labour force(i.e. inactive). Surveys collect information via household-based interviews (in person, by mail or by telephone) ona range of labour force and sociodemographic indicators,such as occupation, work status, wages and earnings, in-dustry and educational attainment. Information on occu-pation among individuals in the labour force is usually
Page 7 of 13(page number not for citation purposes)

Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
processed in terms of the national occupational classifica-tion, which is often based on and sometimes mapped tothe ISCO-88 standard.
Depending on the sampling and instruments used, labourforce surveys may provide statistics on a wider range oftopics than censuses, which usually do not enter intodepth on labour force issues. They cover a more represent-ative population than national health registries, which of-ten focus only on the public sector. Sample surveysgenerally require fewer resources than censuses and can beused periodically to monitor the evolution of HRH andtheir impact on health service provision. Furthermore, de-tailed information of all aspects of health labour marketmobility, job turnover rates, second jobs, etc., can some-times be obtained only through surveys.
Another source highly relevant to HRH assessment is sur-veys of health service delivery points. These are generallydesigned to generate data on the characteristics of healthcare facilities as well as the composition and spatial distri-bution of health workers employed in them. Such surveysare usually completed by means of interviews and/or ex-amination of relevant materials and documents in thesampled facilities. In order to allow generalizations, thesampling frame should be designed to ensure representa-tion across various domains: facility type, urban/rural,public/private, etc.
The main limitations of facility surveys are associated withthe difficulty in some countries of designing a representa-tive sampling frame – due, for instance, to the absence ofan accurate and updated enumeration list of service deliv-ery points. This may be especially true in countries whereregistration and licensing systems of health care providersare poor, or exclude those outside the public health sector.In addition, the sometimes small sample sizes do not al-low for disaggregation of HRH indicators at the subna-tional level. Confidence intervals and likelihood ofstatistical errors may also be large for certain indicatorswhen focusing on specific occupations such as physiciansor nursing and midwifery personnel, or when complete-ness of reporting is low.
While the content and design of sample surveys are highlydiverse across countries and over time, important effortshave been made to harmonize data for public use in somecountries as well as internationally through microdata ar-chives. For example, the Luxembourg Income Study (LIS)undertakes a process to enhance comparability and dis-semination of microdata from labour force and incomesurveys that had already been collected by the central sta-tistical offices across participating countries in the Ameri-cas, Asia, Europe and Oceania [36]. Occupational data
allowing differentiation of health workers are availablefor 18 countries through this source [30].
Routine reportsRoutine administrative reports include information col-lected in an ongoing manner by national ministries (suchas ministries of health, labour or education) and profes-sional associations (such as regulatory or membership-based bodies for physicians, nurses and other health pro-fessionals), as well as other types of continually updatedrecords – for example, registries on entry visas and workpermits for international migrants. These sources are com-monly used in countries to estimate their HRH stock.Some of these estimates can be obtained through interna-tional agencies or institutional federations that compilethem from national sources. Routinely reported data pro-vided by Member States form the basis for the WHO data-base on health personnel [37] and the WHO directory ofmedical schools [38].
Depending on the characteristics and content of each spe-cific registry, information may be obtainable on HRH interms of subnational distribution, skills mix, educationand training, workforce activities, migration trajectories,nationality, gender or age distribution. Their mainstrength lies in the continuous nature of the data collec-tion and processing, even if changes to the underlying reg-ulations and administrative procedures may rendercomparisons difficult over time. Comprehensive datafrom ongoing national records can be a useful comple-ment to periodic censuses and surveys, but are normallynot comparable between countries.
The relevance of such data for reviews of national HRH sit-uations depends on the fraction of the total number of es-tablishments or personnel covered in the country. Inmany countries there is no regular recording of the num-bers and activities of all health personnel, and some em-phasize only the public sector or can have variableaccuracy for rural areas. The direction and magnitude ofbiases from registries' data will depend on their specificcharacteristics. For example, an upward bias will be evi-dent if the system has no mechanisms for the removal ofindividuals from the records upon retirement, externalemigration or death. Another potential issue derives fromthe tendency for some personnel (notably physicians and,to a growing extent, nurses) to practice health care at morethan one location, such as part-time in a public facilityand part-time in the private sector. Unless this situation isreflected, information based on providers' registries canbe subject to bias due to double counting and/or partialcoverage.
Page 8 of 13(page number not for citation purposes)
Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
Analytical techniques and applicationsThe empirical approaches that can be used for HRH anal-ysis are numerous, and the selection of the appropriatetechnique (or techniques) for a given study will dependon many factors, notably the objectives of the study to beconducted, the type of information needed, and the dataavailability and quality. Such approaches can be broadlycategorized as either quantitative or qualitative in nature.
Quantitative applications can range from descriptive tech-niques, such as univariate and bivariate frequency distri-butions of HRH by occupation and other backgroundvariables, to more advanced statistical methods. Summarydescriptives are highly useful for visualizing complex datastructures and integrating data items in graphical or tabu-lar form for presentation. Advanced methods can be usedfor analysing the determinants of a specific HRH matter,involving techniques for testing the effects and interac-tions of certain variables while controlling for the effectsof other variables (covariates). A wide range of models canbe applied, depending on the variables and outcomes ofinterest. This can mean models that yield a single estimat-ed equation with unique correspondence between coeffi-cients and variables, or multiple equations andsubsequent coefficients. They may involve time-seriesanalysis or other types of smoothing techniques for pro-jecting data in time/space based on observed trends.Among the advanced estimation methods for HRH analy-sis found in the published literature are multiple regres-sion (to explain factors affecting the geographicaldistribution of physicians) [39] and proportional hazardmodels (to deal with issues of retention of nurses in thehealth system) [25].
Qualitative methods are techniques for examining non-numeric characteristics of the area of interest. They in-clude the analysis of content from texts, focus group dis-cussions, in-depth interviews and participantobservations. Applications to HRH analysis may be espe-cially pertinent for topics such as regulation of health pro-fessions, labour relations, and worker satisfaction andmotivation (see, for example, [40]).
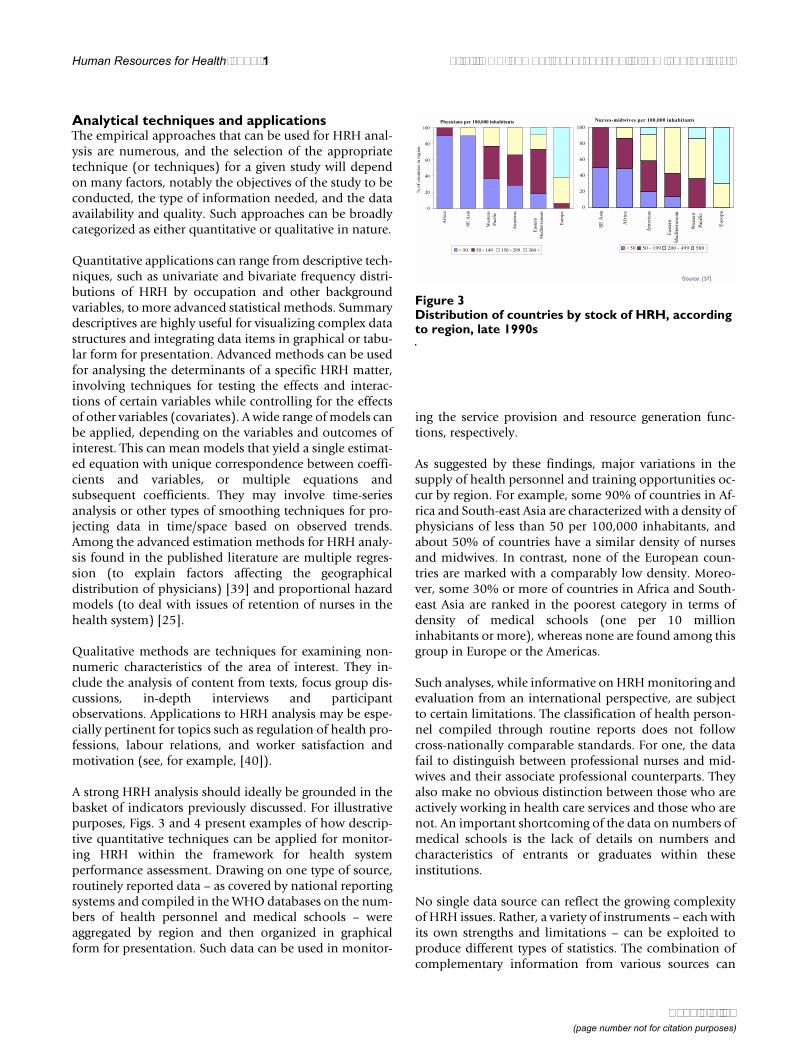
A strong HRH analysis should ideally be grounded in thebasket of indicators previously discussed. For illustrativepurposes, Figs. 3 and 4 present examples of how descrip-tive quantitative techniques can be applied for monitor-ing HRH within the framework for health systemperformance assessment. Drawing on one type of source,routinely reported data – as covered by national reportingsystems and compiled in the WHO databases on the num-bers of health personnel and medical schools – wereaggregated by region and then organized in graphicalform for presentation. Such data can be used in monitor-
ing the service provision and resource generation func-tions, respectively.
As suggested by these findings, major variations in thesupply of health personnel and training opportunities oc-cur by region. For example, some 90% of countries in Af-rica and South-east Asia are characterized with a density ofphysicians of less than 50 per 100,000 inhabitants, andabout 50% of countries have a similar density of nursesand midwives. In contrast, none of the European coun-tries are marked with a comparably low density. Moreo-ver, some 30% or more of countries in Africa and South-east Asia are ranked in the poorest category in terms ofdensity of medical schools (one per 10 millioninhabitants or more), whereas none are found among thisgroup in Europe or the Americas.
Such analyses, while informative on HRH monitoring andevaluation from an international perspective, are subjectto certain limitations. The classification of health person-nel compiled through routine reports does not followcross-nationally comparable standards. For one, the datafail to distinguish between professional nurses and mid-wives and their associate professional counterparts. Theyalso make no obvious distinction between those who areactively working in health care services and those who arenot. An important shortcoming of the data on numbers ofmedical schools is the lack of details on numbers andcharacteristics of entrants or graduates within theseinstitutions.
No single data source can reflect the growing complexityof HRH issues. Rather, a variety of instruments – each withits own strengths and limitations – can be exploited toproduce different types of statistics. The combination ofcomplementary information from various sources can
Figure 3Distribution of countries by stock of HRH, according to region, late 1990s
Nurses-midwives per 100,000 inhabitants
0
20
40
60
80
100
SE
Asi
a
Afr
ica
Am
eric
as
Eas
tern
Med
iter
ran
ean
Wes
tern
Pac
ific
Eu
rop
e
< 50 50 - 199 200 - 499 500 +
Source: [37]
Physicians per 100,000 inhabitants
0
20
40
60
80
100
Afr
ica
SE
Asi
a
Wes
tern
Pac
ific
Am
eric
as
Eas
tern
Med
iter
ran
ean
Eu
rop
e
% o
f co
un
trie
s in
reg
ion
< 50 50 - 149 150 - 299 300 +
Page 9 of 13(page number not for citation purposes)

Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
provide useful and rich information on the profile andother characteristics of the health workforce. Moreover,availability of different types of data sources can also serveas a control for the common information they collect, of-fering means for triangulation [41].
Figure 5 offers an illustration of the uses of triangulationfor data quality control. The same indicator, in this casethe ratio of physicians to nursing and midwifery person-nel (indicator of skills mix), was measured for differentcountries through two different types of data sources:household-based labour force survey data (as compiledthrough the LIS project, see [30]) versus the routinelyreported data. Simple linear regression was then used tocharacterize the relationship between the measures ob-tained from the two sources. Some of the observed dis-crepancies may be related to the occupationalclassification or to the sources' representation. The result-ing parameters could eventually be used as a basis for ad-justing reported numbers to compensate for datadiscrepancies (although before any adjustment is made,the assumptions underlying the evaluation method mustbe carefully considered).
DiscussionThe purpose of this paper was to improve knowledgeabout the information on HRH that researchers and insti-tutions collect and why they do it. A number of indicatorsand data sources were discussed here, focusing on thosebeing used for HRH monitoring and evaluation followingthe WHO framework on Health Systems Performance As-sessment. The indicators were broadly categorized
according to the service provision and resource generationfunctions of health systems. Issues of harmonization ofdata collection and processing methods for enhancingcross-national and time-trend comparability were ad-dressed. Given that the roles and tasks performed by thesame categories of health occupations might vary acrosscountries, the occupational, industrial and educationalclassifications associated with the definition of HRHshould be taken into account when conducting compara-tive analyses. In turn, the selection of an appropriate ana-lytical approach will depend on the policy questions to beaddressed, the resources available and the context of thestudy. Moreover, regardless of the methodology used, theability to track time trends will generally be constrainedby the periodicity of the data sources available.
Despite the existence of a number of reporting systems(censuses, surveys, routine administrative records, etc.)that can be used to examine HRH issues and theircontributory factors, many of these sources remain under-used and the information on current efforts for analysis isfrequently incomplete. Few available sources have beendesigned with the sole intention of producing informa-tion on HRH. WHO is undertaking work to refine and ex-pand knowledge on HRH issues, including compiling andanalysing statistics from existing sources as well as statis-tics based on specially designed surveys. This strategy in-cludes partnerships with ministries, central statisticalagencies and other data providers, research centres, librar-
Figure 4Distribution of countries by density of medical schools, according to region
Source: [38]
0%
20%
40%
60%
80%
100%
SE
Asia
Afr
ica
Easte
rn
Mediterr
anean
Weste
rn
Pacific
Euro
pe
Am
ericas
% o
f countr
ies in r
egio
n
<2 2 - 5 5 - 10 10 +Population (millions) per medical school:
Figure 5Comparison of the ratio of physicians to nursing and midwifery personnel, according to source of data, 12 countries with developed market and transitional economies
y = 0.59x + 0.19
R 2 = 0.73
0.0
0.2
0.4
0.6
0.8
1.0
1.2
0.0 0.2 0.4 0.6 0.8 1.0 1.2
Ratio from LIS datasets
Ratio
fro
m W
HO
data
set
Sources: [30, 37]
Page 10 of 13(page number not for citation purposes)

Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
ies and public health schools as part of a process ofcapacity building in countries. In particular, four maincollaborative projects are currently being implementedfor the compilation of an evidence base on HRH from aninternational perspective.
The World Health Survey (WHS) is being conducted incollaboration with Member States in more than 70 coun-tries from all regions and levels of development, aiming toprovide a wide range of quantitative information that canbe used to assess population health and health systemsperformance [42]. A module on health occupations wasdeveloped for inclusion in the household-based survey inorder to collect comparable baseline information on thecurrent health workforce for primarily monitoring theservices provision function. A standard questionnaire wasdesigned to identify all adults in the sampled householdswho had ever been trained in a health-related field or en-gaged in the health workforce, with follow-up questionson occupation and training, main work activities, work-place industry and sector, income and methods of remu-neration, migration and other topics. The surveyinstruments were pre-tested in 12 countries in 2002, andfieldwork for the main survey phase will have begun inparticipating countries by early- to mid-2003.
Another project is the development of an electronic data-base called the Global Directory of Health Training Insti-tutions, which will provide information on the status andtrends of health education worldwide. This is an expan-sion of the former listing of medical schools [38],building a wider database that also will include traininginstitutions for other health professions such as nursing,dentistry and pharmacy. It will capture selected character-istics of these institutions, notably the numbers and char-acteristics of entrants and graduates, in order to be able tomeasure a range of indictors for monitoring the resourcegeneration function.
In-depth assessments of human resources for health arebeing conducted in 2002–2003 in six developing coun-tries (Chad, Côte d'Ivoire, Jamaica, Mozambique, Sri Lan-ka and Zimbabwe). The study involves collectingquantitative and qualitative data at the national, institu-tional and individual levels. Four areas are included inthis assessment: regulation of health occupations, healthtraining institutions, health care facilities and health careproviders. In order to ensure national representation of fa-cilities and providers, the guidelines for implementationrecommend the use of complementary list- and area-sam-pling frames for coverage of the range of facility types, es-pecially from the private sector, for which available listsare frequently incomplete [43]. The survey questionnairesare similar to those developed for the WHS and GlobalDirectory of Health Training Institutions, but were
designed to gather more detailed information on profes-sional licensing and registration, labour conditions, sup-ply and demand for health personnel, and other relevanttopics in order to develop short-term and long-term rec-ommendations for HRH policy and planning.
A fourth project is the creation of a meta-database of datasources on HRH. This involves the comprehensive reviewfor all countries of sources of information on human re-sources in health systems, in order to maximize the stockof methods and materials for international analyses onHRH. The task entails an extensive search process usingelectronic library sources and World Wide Web-basedsearches to identify data sources, including general sourc-es such as censuses, labour force surveys and other report-ing systems as mentioned above, with special attention toavailability of statistics on health occupations and labourmarket characteristics. In some cases special tabulationson HRH may be directly requested from countries or fromother international agencies (such as ILO or EUROSTAT).The development of such a database will allow fordistinguishing variables to support consistent cross-coun-try comparisons and within-country in-depthassessments.
As previously mentioned, understanding of the growingcomplexity of HRH issues requires a variety of methodsand materials. Improved coordination of data-gatheringactivities could act as a catalyst for improving theavailability, quality and comparability of data for moni-toring and reporting HRH initiatives. HRH assessmentsshould therefore be constructed as a result of a collabora-tive process between all the health system stakeholders,including health care providers, local and governmentagencies, nongovernmental organizations and interna-tional agencies. It is desirable to further assess to what ex-tent research efforts are concurring, what overlapping mayexist, and how research may be improved by filling gaps.Regarding implementation, ways should be found to en-sure that the data received and used by international or-ganizations are the most recent and accurate, and areprocessed through the use of internationally standardizedclassifications at the greatest level of detail possible.
Competing interestsNone to declare.
Authors' contributionsAll authors contributed to the design and writing of thispaper, and read and approved the final manuscript.
Page 11 of 13(page number not for citation purposes)
Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
Additional material
AcknowledgementsAn earlier version of this paper was presented at the international work-shop on "Human Resources and National Health Systems: Shaping the Agenda for Action", Geneva, 2–4 December 2002. Funding for this research was provided by the World Health Organization. The opinions expressed here are those of the authors, and do not necessarily represent the views of WHO. The authors would like to thank Orvill Adams, Eivind Hoffmann and Suwit Wibulpolprasert for their useful comments.
References1. Dussault G Analysis of human resources situation in health:
why and how? Paper prepared for Intercountry consulting on human re-source development in the health field, Cairo 15–18 February 1999
2. Anell A and Willis M International comparison of health caresystems using resource profiles Bulletin of the World HealthOrganization 2000, 78(6):770-778
3. Feachem R Health systems: more evidence, more debate Bul-letin of the World Health Organization 2000, 78(6):715
4. World Health Organization World health report 2000: healthsystems – improving performance Geneva 2000, [http://www.who.int/whr2001/2001/archives/2000/en/index.htm]
5. Almeida C, Braveman P, Gold MR, Szwarcwald CL, Ribeiro JM, Migli-onico A, Millar JS, Porto S, do Rosario Costa N, Ortun Rubio V, SegallM, Starfield B, Travassos C, Uga A, Valente J and Viacava F Method-ological concerns and recommendations on policy conse-quences of the World Health Report 2000 Lancet 2001,357(9269):1692-1697
6. McKee M Measuring the efficiency of health systems: TheWorld Health Report sets the agenda, but there's still a longway to go BMJ 2001, 323(7308):295-296
7. Ugá AD, de Almeida CM, Szwarcwald CL, Travassos C, Viacava F,Ribeiro JM, do Rosario Costa N, Marchiori Buss P and Porto S Con-siderations on methodology used in the World Health Or-ganization 2000 Report Cadernos de Saúde Pública 2001,17(3):705-712[http://www.scielosp.org/pdf/csp/v17n3/4653.pdf]
8. Martínez J and Martineau T Rethinking human resources: anagenda for the millennium Health Policy and Planning 1998,13(4):345-358
9. Egger D, Lipson D and Adams O Achieving the right balance: therole of policy-making processes in managing human resourc-es for health problems Geneva: World Health Organization 2000,[http://www.who.int/health-services-delivery/disc_papers/Right-bal-ance.pdf] Issues in Health Services Delivery Discussion Paper, no. 2.
10. Gravitz M Méthodes des sciences sociales. Paris: Editions Dalloz 1996, 11. Sadana R, Mathers CD, Lopez A, Murray CJL and Iburg K Compar-
ative analyses of more than 50 household surveys on healthstatus Geneva: World Health Organization 2000, [http://www-nt.who.int/whosis/statistics/discussion_papers/pdf/paper15.pdf] Glo-bal Program on Evidence for Health Policy Discussion Paper Series,no. 15.
12. Scientific Peer Review Group on Health Systems Performance As-sessment Final Report Geneva 2002, [http://www.who.int/health-systems-performance/sprg/report_of_sprg_on_hspa.htm]
13. Kolehamainen-Aiken R-L Decentralization and human resourc-es: implications and impact Human Resources for HealthDevelopment 1997, 2(1):1-14
14. Saltman RB and Von Otter C Implementing planned markets inhealth care: balancing social and economic responsibilityBuckingham: Open University Press 1995,
15. Hojat M, Gonnella J and Xu G Gender comparisons of youngphysicians' perceptions of their medical education, profes-sional life, and practice: a follow-up study of Jefferson Medi-cal College graduates Academic Medicine 1995, 70(4):305-312
16. Reamy J and Pong R Physician workforce composition by gen-der: the implications for managing physician supply Paper pre-sented at 4th FICOSSER General Conference, Cuernavaca, Mexico 28–30July 1998
17. Higginbotham E Celebrating women in opthtalmology Archivesof Ophtalmology 1998, 116(9):1227-1228
18. Salvage J and Heijnen S Nursing in Europe: a resource for betterhealth Geneva: World Health Organization Regional Publications 1997,WHO European Series, no. 74.
19. HRH data: guidelines and data requirements for a human re-sources for health information system [http://hrhtoolkit.foru-mone.com/mstr_hrh_data/mstr_hrh_data.pdf]
20. International Labour Office International Standard Classifica-tion of Occupations: ISCO-88 Geneva 1990, [http://www.ilo.org/public/english/bureau/stat/class/isco.htm]
21. United Nations Statistics Division International Standard Indus-trial Classification of All Economic Activities: ISIC Rev. 3.1New York 2002, [http://unstats.un.org/unsd/cr/registry/regcst.asp?Cl=17]
22. United Nations Educational Scientific and Cultural Organization In-ternational Standard Classification of Education: ISCED1997 Paris 1997,
23. United Nations Statistics Division Central Product Classification:CPC version 1.1 New York 2002, [http://unstats.un.org/unsd/stat-com/doc02/cpc.pdf]
24. International Labour Office International Classification of Statusin Employment: ICSE-93 Geneva 1993,
25. Holmas H Keeping nurses at work: a duration analysis HealthEconomics 2002, 11:493-503
26. Wharrad H and Robinson J The global distribution of physiciansand nurses Journal of Advanced Nursing 1999, 30(1):109-120
27. Lambert TW, Goldacre MJ and Parkhouse J Doctors who qualifiedin the UK between 1974 and 1993: age, gender, nationality,marital status and family formation Medical Education 1998,32(5):533-537
28. Johnston G and Wilkinson D Increasing inequitable distributionof general practitioners in Australia, 1986–96 Australian andNew Zealand Journal of Public Health 2001, 25(1):66-70
29. Organisation for Economic Co-operation and Development Thecontribution of census data to improving statistics onemployment in health care Paper presented at OECD Health DataNational Correspondents Meeting, Paris 2002, 25-26
30. Gupta N, Diallo K, Zurn P and Dal Poz M Human resources forhealth: an international comparison of health occupationsfrom labour force survey data Syracuse, NY: Syracuse University2002, [http://www.lisproject.org/publications/liswps/331.pdf] Luxem-bourg Income Study Working Paper Series, no. 331.
31. Kazanjian A and Pagliccia N Identifying the population of healthmanagers in one Canadian province: a two-stage approachEvaluation and Program Planning 1996, 19(1):95-102
32. United Nations Population Division Measuring international mi-gration; many questions, few answers Paper presented at UnitedNations Population Division Coordination Meeting on International Migra-tion, New York 2002, 11-12
33. Hoffmann E Developing labour account estimates: issues andapproaches In Household accounting: experiences in concepts and com-pilation. Vol. 2 Household satellite extensions. New York: United NationsStatistics Division 2000, 21-40 Studies in Methods, series F, no. 75
34. Integrated Public Use Microdata Series [http://www.ipums.umn.edu]
35. African Census Analysis Project [http://www.acap.upenn.edu] 36. Luxembourg Income Study [http://www.lisproject.org] 37. WHO estimates of health personnel: physicians, nurses,
midwives, dentists and pharmacists (around 1998) [http://www3.who.int/whosis/health_personnel/health_personnel.cfm]
38. World directory of medical schools [http://www.who.int/health-services-delivery/med_schools/index.htm]
39. Wilkinson D and Symon B Inequitable distribution of generalpractitioners in Australia: estimating need through the Rob-in Hood Index Australia and New Zealand Journal of Public Health2000, 24:71-75
Additional file
Click here for file[http://www.biomedcentral.com/content/supplementary/1478-4491-1-3-S1.pdf]
Page 12 of 13(page number not for citation purposes)

Human Resources for Health 2003, 1 http://www.human-resources-health.com/content/1/1/3
Publish with BioMed Central and every scientist can read your work free of charge
"BioMed Central will be the most significant development for disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
40. Newman K and Maylor U The NHS Plan: nurse satisfaction,commitment and retention strategies Health Services Manage-ment Research 2002, 15(2):93-105
41. Galin P Guía para optimizar la utilización de la informacióndisponible sobre empleo en el sector salud In Relaciones labo-rales en el sector salud (Edited by: Dal Poz M, Galin P, Novick M, VarellaT) Quito: Organización Panamericana de la Salud 2000, 19-89
42. WHS: World Health Survey home page [http://www3.who.int/whs]
43. World Health Organization Assessment of human resources forhealth: survey instruments and guide to administration Gene-va 2002,
Page 13 of 13(page number not for citation purposes)





























