Embed Size (px)
Citation preview

Mongolia Progress Report
Dr. D. Otgontsetseg, Head of recording and reporting unit, TB surveillance and research department,
NCCD
The ninth Technical Advisory Group and National TB Programme Managers meeting for TB control in the
Western Pacific Region
Manila, Philippines9 -12 December 2014

1962
1964
1966
1968
1970
1972
1974
1976
1978
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
2012
0
1000
2000
3000
4000
5000
6000
0
50
100
150
200
250
300
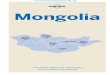
All form TB cases Notification rate
Year
Nu
mb
er
of T
B c
ase
s
No
tific
atio
n r
ate
pe
r 1
00
’00
0
Notified all form TB cases, In Mongolia, 1962-2013
GF project started
DOTS implemented
Nationwide screening

Number of smear positive TB cases, in Mongolia, 1962-2013
19631966
19691972
19751978
19811984
19871990
19931996
19992002
20052008
20110
500
1000
1500
2000
2500
0%
20%
40%
60%
80%
100%
Sputum smear positive TB casesPercent of pulmonary TB casesPercent of SS+ TB cases among pulmonary TB
Year
Nu
mb
er
of S
S+
TB
ca
ses
Pe
rce
nta
ge

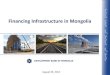
Age distribution of all forms of TB cases, in Mongolia, 2009-2013
0-1 2-7 8-14 15-24 25-34 35-44 45-54 55-64 65+0
400
800
1200
1600
0.0
30.0
60.0
90.0
120.0
2009 2010 20112012 2013 Average rate
Age group
Num
ber
of a
ll fo
rm T
B c
ases
Ave
rage
not
ifica
tion
rate
per
100
’000

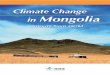
Cure rate among smear positive pulmonary cases Mongolia, 2009-2013 year
2009 2010 2011 2012 201377
78
79
80
81
82
83
84
85
86
84.284.5
8382.6
80.1
cure rate target WHO

Failure and default rate among smear positive pulmonary patients Mongolia, 2009-2013 year
7.1 7.28.1
7.1
9
2.2 2.42.9
44.8
0
2
4
6
8
10
2009 2010 2011 2012 2013
per
cen
t
year
failure default

Major successes The global Millennium Development goal and regional
targets for TB control are likely to be met Increasing Government funding for TB control Revised National TB care guidelines approved by Health
Ministerial order WHO revised definition and reporting framework for
tuberculosis introduced in all levels of TB care – pilot in 2014, starting 2015- will be reported officially
Nationwide TB prevalence survey started in Apr 2014 and field data collection completed in urban areas
Introduction and roll out of GeneXpert

Major challenges
Dependence from external funding – sustainability of the National TB programme after the end of the GF grant
Diagnosis and management of EPTB and TB in children
Early detection and treatment of TB among high risk groups (homeless, alcoholics, migrants)
Increasing rates of default and failure among TB patients in the last two years, especially in Ulaanbaatar city
Lack of awareness of the public about TB

National TB Strategy/Policies
• Timeframe: 2010 - 2015• Targets: by 2015, reduce TB prevalence to 154 per 100
000 and by 2015, reduce TB mortality to 15 per 100 000 • Alignment with WHO End TB strategy: The new National
Stop TB strategy will be developed in 2015• National Health Sector Plan will be end in 2015. National
Strategic Plan to Stop TB 2010-2015 is aligned. • Budgeted• 70% - GF supported project, 30% - government

Laboratory strengthening•LED 2 LED: NRTL and 1 province
A prison hospital and 3 provinces received in Nov 2014
•Xpert 3 GeneXpert –NRTL and 2 provinces
NRTL: Total tested 2659, MTB detected 50.2%, error 3.1%, rif resistance detected 18.6%
•Quality assuranceEQA SSM 36 ZN, 1 LED labs, EQA DST, SSM from RIT, Japan
•Laboratory information management system
Internet-based system www.tubis.mn•TA partners
SRL –RIT, Japan since 2005

Reach the unreached• Active case finding: among high risk populations – prisoners,
homeless, medical workers, pregnant women, people living with HIV
• Passive case finding: adults by smear examination and X-ray, children tuberculin skin test and X-ray
• Contact investigation: family members of smear positive patients, children, MDR-TB – target 100%, in practice – 86%
• TB-HIV: screening of people living with HIV for TB by Gene Xpert, all new and relapse TB cases (16 years old and above) tested for HIV. So far 181 HIV cases are reported, out of them 31 are co- infected
• Child TB: Operational research on contact investigation, strategy on child TB will be developed in 2015

Surveillance• Quality of surveillance system
–Use of national unique ID –Paper and internet based reporting: on time by paper; some difficulties using internet-based system due to internet connection
• New case definition roll out– WHO revised definition and reporting
framework for tuberculosis introduced in all levels of TB care – pilot in 2014, starting 2015- will be reported officially

Surveillance• e-R&R
– Internet based reporting – ‘tubis’; – Update of the system based on WHO new
definitions– 90% of TB reporting units use ‘tubis’ platform
• Analysis and usage of data at national and sub-national levels– Analysis data at the national level on monthly,
quarterly and annual basis – Limited capacity at the sub-national level

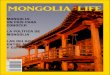
Notified (n=1375) and died (n=325) MDR-TB cases Mongolia, 2003-2013
0
50
100
150
200
250
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
nu
mb
er
year
notified died
started GF supported MDRTB + pilot project

Treatment success for MDRTB patients Mongolia , 2006-2010
2007 2008 2009 2010 20110
10
20
30
40
50
60
70
80
90
75
85.1
71.677.2
68
success death failure WHO target

Number of XDR-TB cases
XDRTB Pre XDRTB 2009 3 22010 10 12011 6 272012 12 92013 3 132014 6 6
total 40 58
out of them:
Died 30
Address unclear 4
Refused 2
Waiting on treatment 2
2 nd line treatment continued 1
Cured 1

PMDT
•Plan vs universal coverage–In 2014 planned 219 MDR-TB and 81 PDR patients to enroll in treatment
•Barriers–Lack of social support for MDR-TB patients–Lack of experienced health providers ( high turn over of staff)–Lack of management of side effects–Some MDR-TB patients refuse to receive treatment due to various reasons (religious, co-morbidities etc.)

PMDT: Priority actions–Strengthening management of MDR-TB patients (counseling, follow up of patients, capacity building of TB providers)–Establishment of patient support groups in collaboration with MATA –Treatment of XDR-TB patients with financial support of the GF–DRS planned in 2015–TB prevalence survey results to be analyzed–Advocacy to include MDR-TB drugs in Government budget

Bold policies and supportive systems
•TB care financing and social protection–TB care financed by the Government–No health insurance coverage for TB services–No specific social protection services for TB patients–Within general social protection system TB patients (especially employed) may receive disability benefits for certain period
•Strengthening notification mechanism–An estimated 15-20% of diagnosed TB cases are not notified –Supportive supervision should be strengthened–Strengthen internet based reporting and recording
•Drug regulations – Progress since drug regulation meeting in March 2014
–New drugs for MDR-TB were included in national essential drug list–Drug information is in the process of revision in internet-based system

Patient centred care: involvement of patients and civil society
• Community mobilization activities– Patient support groups will be established by
MATA with financial support of Stop TB Partnership
• CBO involvement and their role– MATA: lunch DOT and home DOT– World vision: TB services for prisoners,
homeless – TB Coalition: advocacy for local governments

Patient centred care: involvement of patients and civil society
• Involvement of patient groups in TB control – In the process of establishment
• Forms of social support to TB patients (incentives? TB Pension? Reimbursement of costs related to care like transportation costs?)– Transportation cost only for MDR-TB patients (GF)– Within general social protection system TB patients
(especially employed) may receive disability benefits for certain period

Thank you for your attention