Embed Size (px)
Citation preview

Mongolia Health Sector
Achievements and Challenges:
Where Next?
February 2009

2
Health Outcomes
Sector:
• Financing
• Allocation
• Efficiency and Equity
• Health Insurance
Reforms of 2006
Remaining Challenges?
The Current Crisis/Where Next for Health?
Outline

3
Outcomes Good Relative to
Level of Economic Development
Vietnam
Turkey
South Africa
Russian Federation
Mongolia
Malaysia
KazakhstanIndia
Georgia
ColombiaChina
Cambodia
Brazil
Bangladesh
Azerbaijan
Armenia
0
20
40
60
80
100
120
140
160
180
0 5,000 10,000 15,000 20,000
GDP p.c. (constant international US$)
In
fan
t m
ortality
VietnamTurkey
South Africa
Russian Federation
Mongolia
Malaysia
KazakhstanIndia
Georgia
ColombiaChina
Cambodia
Brazil
Bangladesh
Azerbaijan
Armenia
0
50
100
150
200
250
300
0 5,000 10,000 15,000 20,000
GDP p.c. (constant international US$)
Un
der-fiv
e m
ortali
ty r
ate

4
Success in Delivery System
MongoliaUzbekistan
VietnamKyrgyz Republic
Kazakhstan
Cambodia
Azerbaijan
20
40
60
80
100
0 5,000 10,000 15,000 20,000
GDP pc (PPP)
% o
f c
hil
dren
ag
es 1
2-2
3 m
on
th
s
imm
un
ized
for m
easle
s (
20
04
)
Azerbaijan
CambodiaKazakhstan
Kyrgyz
RepublicVietnam
UzbekistanMongolia
20
40
60
80
100
0.00 5,000.00 10,000.00 15,000.00 20,000.00
GDP pc (PPP)
% o
f c
hil
dren
ag
es 1
2-2
3 m
on
th
s
imm
un
ized
for D
PT (
20
04
)

5
Maternal Mortality and Child Delivery
Azerbaijan
BangladeshBolivia
Brazil
Bulgaria ChileChina
Colombia
India
IndonesiaKazakhstan
MexicoMongolia
PhilippinesSouth Africa
Thailand
Vietnam
0
300
600
900
1200
0 5,000 10,000 15,000 20,000
GDP p.c. (international US$)
Matern
al
mortali
ty r
atio
MongoliaUzbekistan
Vietnam
Kyrgyz
Republic
Cambodia
Azerbaijan
0
20
40
60
80
100
0 5,000 10,000 15,000 20,000
GDP pc (PPP)
% o
f t
otal b
irth
s a
tten
ded
by
skille
d h
ealt
h s
taff (
20
00
-0
4)

6
But…Variations in Mortality
(by Income and Geography)
0
10
20
30
40
50
60
70
80
Ula
anbaata
r
Centr
al
Khangai
East
West
Capital ci
ty
Aim
ag
Soum
cente
r
Rura
l
Poore
st
Ric
hest
Mort
alit
y ra
te
IMR
U5M
Source: Data on infant mortality rates (IMR) and
under-five mortality rates (U5MR) from 2005 Middle
Income Countries.

7
Changing Disease Profile
(NCDs & need for primary/secondary prevention)
Source: WHO Gobal Database
Thailand
Sri Lanka South Africa
PhilippinesMalaysia
Indonesia
India
China
Chile
Brazil
Argentina
Mongolia
Uzbekistan
Vietnam
Kyrgyz Republic
Kazakhstan
0
10
20
30
40
50
60
70
80
0 5,000 10,000 15,000 20,000 25,000 30,000
GDP pc (PPP)
Pre
vale
nce
of sm
okin
g a
mong
adult m
ale
s (2
000-0
5)

8
Health Outcomes
Health Sector:
• Financing
• Allocation
• Efficiency and Equity
• Health Insurance
Reforms of 2006
Remaining Challenges?
The Current Crisis/Where Next for Health?
Outline

9
VietnamUzbekistan
Mongolia Sri LankaCambodia
Kazakhstan
IndiaIndonesia
China
0
20
40
60
80
100
120
140
160
180
200
0 1,000 2,000 3,000 4,000 5,000 6,000 7,000 8,000
GDP p.c. (current international US$)
To
tal
healt
h e
xp
en
dit
ure p
.c. (
cu
rren
t U
S$
)
VietnamUzbekistan Russian Federation
Pakistan
Mongolia
Sri Lanka
Cambodia
Kyrgyz Republic
Kazakhstan
India
Indonesia
China
Brazil
Azerbaijan
0.0
2.0
4.0
6.0
8.0
10.0
12.0
0 1,000 2,000 3,000 4,000 5,000 6,000 7,000 8,000 9,000 10,000
GDP p.c. (current international US$)
To
tal h
ealth
exp
. as %
o
f G
DP
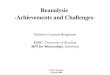
Total Health Expenditure and GDP
Source: Data from World Development Indicators (2006) and WHO Statistical Information System (2006).

10
Composition of Public Funding
Health Insurance small and
payroll contributions come from
only 20% of members
Has it added more funding to the
health sector?
How will declining economy and
declining employment change
this?
How does it link to Health
Insurance protection?
0
20
40
60
80
2006
Insurance
Budget
Other

11
Decline of Health Insurance Coverage Continue?
SHI coverage by beneficiary category
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
Flat-rate contribution
Payroll contribution
Government subsidy
Source: MOWSL

12
Resource AllocationComposition of MOH budget allocation, 2006
Secondary and
tertiary hospitals
51%
Primary providers
and pharmacies
28%
Public health
institutions and
agencies
9%
Administration
3%
Sport-related
expenditures
3%
Other
6%
Source: MOH. Secondary and tertiary hospitals include clinical hospitals, district hospitals, aimag and city
hospitals, and other referral hospitals. Primary providers and pharmacies include soum and inter-soum hospitals,
family group practices, and pharmacies (reimbursed by HIF). The largest component of ‘Other’ is the government
subsidized health insurance contribution for some households.

13
Variations across Geographic Areas (Aimag)
2006 MOH allocation to aimags p.c.
0 10,000 20,000 30,000 40,000 50,000 60,000
UlaanbaatarOrkhon
BayanUlgiiKhuvsgul
UvurkhangaiSelenge
KhovdArkhangai
Darkhan-UulBayankhong
DornodUmnugobi
TuvSukhbaatarDornogobi
BulganZavkhan
DundgobiKhentii
UvsGobiAltai
Gobi
Source: MOH and Regional GDP data from 2006 Statistical Yearbook.

14
Too Many Beds and Hospitals
Thailand
Sri Lanka
Philippines
Malaysia
Indonesia
Colombia
ChinaChileBrazil
Argentina
Azerbaijan
Cambodia
Kazakhstan
Kyrgyz RepublicUzbekistan
Mongolia
0
20
40
60
80
100
120
0 5,000 10,000 15,000 20,000 25,000 30,000
GDP pc (PPP)
Hosp
ital beds
per
10,0
00
Source: Data from 2006 World Health Report (WHO)

15
Too Many Physicians
Source: Data from 2006 World Health Report (WHO)
Thailand
South Africa
Russia
Philippines
Mexico
Malaysia
Indonesia
Colombia
ChinaBrazil
Argentina
Azerbaijan
Cambodia
Kazakhstan
Kyrgyz Republic
Uzbekistan
Mongolia
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
0 5,000 10,000 15,000 20,000
GDP pc (PPP)
Ph
ysic
ian
s p
er 1
,00
0 p
op
.

16
Health Outcomes
Health Sector:
• Financing
• Allocation
• Efficiency and Equity
• Health Insurance
Reforms of 2006
Remaining Challenges?
The Current Crisis/Where Next for Health?
Outline

17
2006 Health Reforms
1. Full budgetary financing for primary care (FGPs and soum hospitals)
2. Move to financing line items to package of services From budgetary financing for fixed costs and health insurance financing for variable costs for
secondary and tertiary hospitals, towards a model where the financing split is determined by type
(or „package‟) of service
Will need to pool funds to make this work
3. Capitation payment (payment per „covered‟ individual) for FGPs and introduction of capitation-based financing for
variable costs of soum hospitals
4. Hospitals case-based payment (“DRGs”) (fixed payment rate for different types of „cases‟) for most services provided by secondary and
tertiary hospitals
5. Hospital Autonomization provisions for state-owned health facilities to use financial surpluses for the improvement of
working environment and social protection of their health personnel.

18
Health Outcomes
Health Sector:
• Financing
• Allocation
• Efficiency and Equity
• Health Insurance
Reforms of 2006
Remaining Challenges?
The Current Crisis/Where Next for Health?
Outline

19
Outcomes
Maternal Mortality Rate by Province, 2006
80-120
>161
<39

20
Demand Side:
OOPs and Informal Payments: How High?
55%
74%
43%
2%
81%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Cambodia
(2000)
China
(2001)
Indonesia
(2001)
Thailand
(2000)
Vietnam
(1992)
Share of Informal Payments Among Users in Health Services (%)

21
Supply Side
Governance of SHI and the Pooling of Funds• Changes in the current fragmentation of funding and purchasing of services. This includes full pooling of public funds across
sources of revenues such as general budget and health insurance revenues, and development of a real single payer for services
Basic Benefits Package by the new single payer, the Health Insurance Fund (HI Fund)
• New package was developed in 2005 but not fully implemented
Refinement of new Provider Payment systems• new capitation model for FGPs and the case-mix payment per admission system for hospitals
Rationalization and Modernization of Hospital Sector• Collaboration and an eventual consensus across multiple actors in the hospital sector in the capital city. There are several sub-
sectors including the city (9 district hospitals), the MOH (MOH facilities), “parallel system” hospitals (e.g., Defense, Railroads and other large state-financed organizations),, and the private sector (an estimated 10% of all admissions)
• A hospital facility strategy to identify end-results of hospital optimization and selection of a model for implementing this process to achieve end-results. Different implementation models exist including the network model (Estonia), administrative fiat model (Kazakhstan, Moldova), and public-private partnerships (Armenia)
Civil Service Reforms across all sectors including Health• And/or improved autonomization of hospital facilities creating flexibility of inputs and improving accountability mechanisms

22
Impact of New Economic Crisis
Insurance Coverage Decline?
Increased Utilization Rates?
Increased OOPs?
Need for More Government
Revenues for Health sector?
Issues across geographic
areas?
What Else? What Have We
Missed?
…
…
…
…
…