Embed Size (px)
Citation preview

Money Follows the Person/ Pathways to Community Living
Care Management Processes
Revised 2/6/2015

Goals of Care Management
Improve individual/family/caregiver’s participation in healthcare decisions and management.Improve individual/family/caregiver’s abilities to self-manage health conditions, medication adherence and participation in health promotion activities.Assist individual/family/caregiver in proactive monitoring, evaluating and problem solving.
Improve collaboration among/between individual/family/caregiver, providers and care managers.
Improve the coordination and continuity of care across the continuum of care.
Improve individual/family/caregiver’s health status, satisfaction and quality of life.
Improve the delivery of cost effective care in the least restrictive environment.
2

Care Management Definition
Care Management is a person centered team based approach
(individual/family/caregiver, care manager, primary care provider/psychiatrist)
which integrates health care and social supports. It is based on a
comprehensive multi-disciplinary assessment that identifies and prioritizes
goals, strengths, problems/risks and barriers to care. A collaborative
comprehensive plan of care is developed and implemented, proactively
monitored and evaluated, following evidence-based guidelines and standards of
care which promotes self-management of health conditions, medication
management, health promotion activities, and assures that identified providers,
services and supports are meeting the needs of the individual/family/caregiver.
Transitions in care are managed with timely follow-up, facilitation of
communication between providers, and individual/family/caregiver with
adjustments to the plan of care.
3(Schraeder, 2012)

4
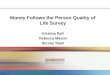
Hospital
Home HealthPharmacy
Behavioral Health
Specialty Care
Long Term Care
Provider(PCP,
psychiatrist)
Person/ Family
CM/CMN
Community Services
Home Transportation
FinanceSupport System
Substance Abuse
Person Centered
(Schraeder, 2012)

Roles of a Care Manager
Assess
Plan
Implement
Monitor
Evaluate
Coach/Educate
Empower
Collaborate
Coordinate
Manage
Document
Advocate
Negotiate
Facilitate
Support
5(Schraeder, 2012)

Care Management ActivitiesAssess health status, goals, strengths, problems/risks, barriers to care, needs and self management abilities of each individual.
Develop and implement with individual/family/caregiver/providers a comprehensive care plan based upon evidenced-based guidelines and standards of care.
Coach, teach and empower individual/family/caregiver to learn and develop abilities to self-manage: health conditions, medications, red flags, and identified problems/risks.
Coordinate and follow-up with formal and informal service providers.
Support individual/family/caregiver to implement plan of care, report challenges/successes, and changes in status.
Collaborate with other disciplines and professions regarding the individual/family/caregiver’s plan of care.
6

Care Management ActivitiesFacilitate communication of pertinent information between providers and with individual/family/caregiver while tracking health status over time with early communication of changes.
Advocate for the individual/family to ensure the correct level and type of care and services are received.
Negotiate with healthcare system and payor sources to obtain necessary services.
Monitor and evaluate effectiveness of the plan of care, teach individual/family/caregiver how to evaluate the effectiveness of their plan of care and revise plan of care to reflect changes in individual’s health status, psychosocial needs, and self-management abilities.
Document individual/family/caregiver and provider contacts.
Manage transitions of care.
7(Schraeder, 2012)

Case StudyMs. Paula Johnson is a 60 year-old Caucasian female, 5’2” and 235 pounds, with a BMI of 43, which is considered heavily overweight. She was admitted to Oak Nut nursing facility 3 years ago after an accident that resulted in a spinal fracture and cord injury at T4-5. She uses a wheelchair for mobility. Her other diagnoses include Type II Diabetes Mellitus (DM), Coronary Artery Disease (CAD) with a previous Myocardial Infarction (MI), and Hypertension (HTN). Her primary language is English and she can read and write. She is of the Catholic faith and likes to attend mass at least once a week. She is not in need of a guardian and her emergency contact person is her sister who lives 4 hours away. She is divorced. She does not have any legal documents in place (no POA or living will). Paula has a 9th grade education and has worked in dry-cleaning intermittently. She was arrested once for shoplifting and on probation for 2 years afterwards. This happened about 25 years ago and she has not been in legal trouble since. She had a bank account in the past, but had difficulty remembering to pay her bills. Her current income is SSDI at $652.85 a month. She is on Medicaid and has no idea if she would qualify for Medicare. She lived independently in the community before her accident.
8

Collaborative Care Management
9
Person/Family Centered
Case Contact: Engage Referral
Pre-Transition: Conduct Comprehensive
Assessment
Pre-Transition: Develop
Individualized Plan of Care
Transition: Implement Plan of Care
Transition: Monitor & Evaluate Plan of Care
· Engage Referral
·Conduct Comprehensive Assessment
·Develop Individualized Plan of Care
·Implement Plan of Care
·Provide Self-Management
·Provide Medication Management
·Reinforce Health Promotion
·Coordinate Care/Services
·Provide Transitional Care
·Perform Critical Incident Review
·Facilitate communication across continuum
·Monitor & Evaluate Plan of Care
(Schraeder, 2012)

Case Contact: Engage Referral
10

11
Identification & Referrals
Potential MFP individuals are primarily identified through the following mechanisms:a) Local or Regional Ombudsman
b) Self-Referral from individuals or families
c) Nursing facility or provider staff
d) Other agencies
e) HFS online MFP/Pathways’ referral form
f) SODC closures (DDD specific)
g) Class action lawsuits
11

MFP/Pathways Referral Process
Submission of online referrals starts the MFP process. If there are no issues with the referral data, it will be
routed directly to the agency based on routing rules. If there are issues (e.g. data discrepancies, no RIN),
the referral will be processed by HFS and manually distributed.
Once a referral is passed to an agency for follow-up, it becomes a “Case” in the WebApp. Cases are linked to a individual – meaning a
individual can have multiple cases but all are linked together in CRM/WebApp.
12

MFP/Pathways Referral Process
Initial contacts cannot be entered in CRM without a referral.
New referrals from HFS need to be followed up on within 10 days of receiving the referral.
Referrals can be sent back to HFS if they need follow up from a different state agency.
13
Referrals are entered here:
https://mfp.hfs.illinois.gov/mfpreferral.aspx

Conducting Case (First) Contact
Determine if the referral has a legal guardian. Determine if there is a family member/significant
other who is actively involved in their care. Maintain privacy and confidentiality when meeting
with the referral. Inform referral of the reason for your visit. Describe your role, the MFP/Pathways program
and the type of housing, services and supports available to them in the community. For more information, visit http://www.mfp.illinois.gov/
Provide referral and/or guardian with a copy of the MFP/Pathways brochure and your contact information.
An MFP first contact is considered a face-to-face meeting unless the referral’s guardian is located outside the local area.
14

15
Complete Case Contacts
Click “+” to add a new Case Contact.
The First contact date is shown here.
All Case contacts are listed here. Click the “Name” link to view a contact.

16
Case Contacts: Not in the Facility
If you find out from the institutional care setting staff that the individual you are trying to contact has
become deceased or has moved out of the facility…
Complete a case contact to document this outcome.
This closes the loop on the referral.

Completed when individual indicates he or she would like
to enroll and plans to transition to the community through
MFP/Pathways.
Two original copies must be signed and dated by the
individual (or proxy or guardian) prior to transition in order
for the individual’s transition to be valid for MFP.
One copy is given to individual/guardian
One copy is kept for TC’s file
17
Informed Consent

A individual is enrolled if, and only if, the individual (and/or guardian) has agreed to participate in MFP by signing the Informed Consent document.
The date of the individual’s signature on the Informed Consent is the date of enrollment. (There is no more Form B).
If the individual or guardian no longer wishes to sign the informed consent, document this by completing a new case contact since the individual is no longer “Considering MFP”.
18
Informed Consent = MFP Enrollment

19
Advance to Informed Consent Stage vance to Informed Consent Stage 1. After you have documented that a potential individual is
Considering MFP, you can advance to the next stage of the transition planning process.
2. Click the “Next Stage” button in CRM to advance to the Informed Consent stage (move the blue flag!).

Release of Information
At the time of receiving informed consent, determine if the individual has any family/friends/ significant others that they want to be part of the transition planning process.
If someone is identified, have the individual sign a release of information to permit you to speak with that person(s).
Also, obtain a release of information for formal and/or informal providers involved in the individual’s care.
This release of information can be uploaded as an attachment in CRM.
20

Case Note
21

Pre-Transition
22

Comprehensive Assessment
Assessment is the first essential function of the care management process.
Assessment is an organized, multidimensional process by which the care manager, through interaction with the individual, significant others, guardian, healthcare providers, review of facility record, agency assessments, and Medicaid claims data, collects and analyzes in-depth information on domains including demographics; individual’s goals, likes or dislikes; cognition/comprehension; diagnoses; substance use; utilization; medications; health; social history; functional status; safety issues, and; self-management skills.
23

Assessment: Key Sources
Individual Institutional record Nursing facility staff Family members, friends, and/or guardian Health and service providers Agency assessments Medicaid claims summary
24

Institutional Record
Face/Diagnosis Sheet Medication List Progress Notes MDS Nursing Assessments Labs Diagnostic Procedure Results Other Service Provider Reports
25

Medicaid Claims Summary
Institutional Visits by Day Diagnosis Groupings Prescription Groupings Procedure Groupings Facility Services Received Provider Frequency Institutional Admissions Institutional Discharges
26

27
Example of Institutional Visits

Example of Diagnosis Groupings
28

Example of Institutional Admissions & Discharges
29

Includes social and financial history, major diagnoses, sensory needs/impairments, individual goals
Required to be completed before transition Add information as needed both pre- and post-transition Click the “Plus (+)” to add a Face Sheet
30
Face Sheet (Form F)

Required to be completed before transition Must have prescriptions ready for when individual
transitions UIC clinical staff, pharmacists, institutional care
setting staff can assist when needed Provide the individual with a copy of his/her
Medications and Supplies List Add/Update information as needed both pre- and
post-transition by updating existing list
31
Medications and Supplies (Form G)
TIP: Review the list during monthly home visits. Update it in CRM and print a new list for individual
with each medication change.

Poll Question
Identify key sources for gathering information for your assessment.
Answer options Individual Institutional record Nursing facility staff Family members, friends, and/or guardian Medicaid claims summary
32

Completely updated questions and format 80 questions 10 domains
Required to be completed prior to transition and must be operational on first day of transition
Identifies potential risks and plans to address known risks
Should include everything the TC will be doing to structure and maintain a safe transition
33
Risk Assessment/Inventory (Forms H&I)

Risk Assessment/Inventory (Forms H&I) Physical Health
Behavioral & Emotional Health
Substance Abuse
Self-Harm or Harm to Others
Cognition
Medication, Laboratory, & Utilization
Functional
Environment
Interpersonal & Social Supports
Engagement, Self-Management & Recovery
34

35
Begin Risk Assessment/Inventory1. Click the “+”
2. Click Save.
3. Click on Risk Assessment

36
Complete Risk Assessment/Inventory
1. Select a Domain
2. Check the box if this Question is a Risk for the individual.
3. Describe why it is a risk
4. Complete pre- and post-transition plan.
5. Click Save and continue to complete remaining questions and domains until progress bar shows
100% complete.
Note: If question is not a risk, click Save and continue to next question. Always click save
or Update after each question. You can close the window and
return to it later.

Risk Stratification Criteria Persons are identified as high risk transitions who have
(based on recent literature): Coronary Artery Disease (CAD), Chronic Obstructive Pulmonary Disease
(COPD), Congestive Heart Failure (CHF) and hospitalized within the past 12 months prior to transition.
Acute Myocardial Infarction (AMI), Dementia, Arthritis, Atrial Fibrillation, Cancer, Renal Failure, Diabetes, Osteoporosis, Serious Mental Illness, Cerebrovascular Accident (CVA), Substance Abuse, and hospitalized twice within the past 24 months prior to transition.
Persons are identified from MFP data review as high risk for reinstitutionalization/mortality who have: Diabetes, medication risks, require additional supports to live in
the community, pre-transition emergency room visit/hospitalization within 12 months of transition, and post-transition hospitalization.
37

Risk Assessment/Inventory Process
Identify risks in each risk domain Discuss risks with individual or guardian Prioritize risks requiring immediate action Develop plan with individual or guardian to manage risks
Focus on techniques that will increase individual’s knowledge of his/her chronic conditions, enhance self management strategies, and coordinate services across health care settings while identifying and addressing barriers and gaps in care.
Incorporate evidence based practice research into plan. Review plan at least monthly Revise plan based on changes to individual’s level of
care
38

Poll Question
Identify risks and related domains for Paula. Answer Options
Functional: Difficulty managing finances. Environmental: Requires adaptive equipment for mobility. Physical Health: Multiple chronic diseases. Physical Health: Requires a special diet. Interpersonal and Social Supports: Lack of peer support.
39

New format – no additional data entry required. Required to be completed before transition and after Risk
Inventory has been completed. Printable report available in CRM. TC reviews completed
Risk Assessment/Inventory. Edit as needed. Involve individual/guardian to achieve the best possible
outcome and keep it person centered. Document agreement and have individual/guardian sign
the mitigation plan. Upload signed copy to CRM and provide
individual/guardian with a copy. Evaluate effectiveness of plan during follow-up visits.
40
Mitigation Plan (Form J)

Mitigation PlanningTransition Coordinator activities: Involve the individual and/or caregiver in every step of mitigation
plan development. Prioritize risks based on the level of each risk, the individual’s
readiness to change and the individual’s ability to self manage identified problem areas.
Establish goals and activities based upon the individual’s preferences.
Provide individual and/or caregiver with guidelines for self-management techniques.
Create a “notebook” where the individual and caregivers can keep guides, logs, notes or questions to discuss with various providers or CM.
Determine contact schedule and who will conduct the coaching, supporting, collaborating, monitoring, and evaluating.
41

Example Mitigation Plan
42

Example Mitigation Plan
43

New format – no longer one page (includes Personal Resource List – Form L).
Completion required prior to transition and must be operational on first day of transition.
Back-up providers should be identified for all critical services.
Individual and/or primary caregiver(s) should be educated on how to use the back-up plan in different scenarios.
Printable version available in CRM. Provide individual and/or caregiver(s) with a copy.
44
24 Hour Back-Up Plan (Form K)

Federal requirement. If not completed prior to transition, then transition will not count for MFP.
Must be completed prior to transition scanned and uploaded to the CRM or faxed to UIC.
Complete one week to 30 days prior to transition, no earlier. If individual refuses, contact Farris Watson at
[email protected] for more information. Second QoL Survey: conducted by UIC College of Nursing at
“First Follow-Up” (about 11-12 months post-transition OR by DDD)
Third QoL Survey: conducted by UIC College of Nursing at “Second Follow-Up” (about 2 years post-transition OR by DDD)
45
Quality of Life Survey Important

UIC Case Review All pre-transition documentation should be completed prior to
requesting a case review. A case review is completed by UIC prior to transition and sent to all
parties involved in the individual’s transition. Including Managed Care Organization (MCO) staff
A case review call is scheduled and occurs within 60 days prior to the individual transitioning. (If individual does not transition within 60 days after the completion of case review, then another case review will be scheduled.)
The case review will cover Medicaid claims data, risk inventory and mitigation plan, and risk status and risk categorization.
A list of clinical questions and action plan items will be included in the case review.
This is the time to ask questions regarding the individual’s diagnoses, medications, or other necessary supports and services.
46

Poll Question What mitigation strategies would be in your service plan
to address the identified risk of limited social support with an individual diagnosed with Major Depressive Disorder.
Answer options Arrange and monitor caregiver services. Provide contact numbers to peer support groups in
the community. Arrange transportation as needed. Arrange weekly counseling session with a mental
health provider.
47

Transition
48

Completed on the day of transition or within 2 business days post-transition
Starts MFP 365 day clock of eligibility Records date of transition Records housing information, new address,
county and appropriate waiver, state plan and demonstration services.
49
Transition (Form C)

Implementation of Mitigation Plan: Day of Transition
Transition Coordinator activities: Be present on the day of transition both at the nursing facility and at
the individual’s new residence. Obtain agreed upon medication supply and/or prescriptions from the
nursing facility. Ensure all medical supplies and furniture were delivered to individual’s
new residence. Ensure all utilities and the emergency medical response unit are in
working condition. Review medication chart and the 24-hour back-up plan with individual. Arrange for personal assistant, homemaker, family member/friend,
and/or home health nurse to be present at the new residence.
50

Case Note
51

Post-Transition
52

Implementation of Mitigation Plan: First Week After TransitionTransition Coordinator activities: Conduct at least one face-to-face visit within the first week after
transition. Determine if there are any outstanding or new issues and/or changes
to the individual’s condition. Determine if individual has enough medications and is taking her
medications as prescribed. Inquire about the individual’s satisfaction with caregiver services. Review dates of upcoming provider appointments. Determine follow-up schedule with individual. (Intense monitoring is
typically required the first eight weeks after transition and again after an emergency room visit or hospitalization.)
53

Implementation of Mitigation Plan:OngoingTransition Coordinator activities: Coordinate and ensure individual is receiving
necessary services such as home health care for diabetes management.
Collaborate with community and health care providers.
Monitor caregiver’s ability to safely assist individual in transferring and managing ADLs/IADLs.
Coach individual on the development of self management skills and educate on symptom identification (e.g., checking and logging blood sugar readings).
Establish medication and nutritional goals and monitor progress.
Re-assess individual’s needs, risks and strengths after any health changes.
54

Monitoring & EvaluationMonitoring Assess individual’s status and responding quickly to physiological,
behavioral or other changes. Conduct visits on a regular basis. Address individual’s ongoing needs, identifies new needs, and
follows up on progress towards care plan goals.
Evaluation Conduct on a regular basis. Evaluate and adjust mitigation plan to reflect changes to individual’s
status and ability to self-managed. Identify successful and unsuccessful interventions. Involve individual and/or family members in revising care plan to
meet his/her changing needs.
55(Schraeder & Shelton, 2011)

Monitor & EvaluateTransition Coordinator activities:
Assess for changes in health status and/or medications.
Assess for utilization of emergency room, hospital, and/or physician visits.
Provide resources, equipment and services: Were ordered services delivered? Are services appropriate and
meeting individual’s needs? What gaps in services exist? Are there any new needs? Is durable medical equipment in
working order? Inspect and confirm it is being used by individual appropriately.
Monitor safety and social support.
Assess housing situation. Is housing appropriate and
meeting needs? Does individual enjoy living in her
new residence? Does individual feel safe and
secure?
Assess overall satisfaction with community living.
Monitor development of self-management strategies (i.e., medication management).
56

Update Documentation Face Sheet
Add any new diagnoses. Medication List
Add new medications and/or remove medication discontinued by medical provider(s). Provide individual with a printed copy of the medication list.
Risk Assessment/Inventory Determine if there are any changes to risk inventory domains.
Mitigation Plan Determine if new goals and/or strategies are needed.
24-Hour Back-Up Review contacts on back-up plan and add new contacts as
needed. Notes
Document notes with every individual contact. Document notes throughout the entire transition process.
57

UIC 30-day Post-Transition Follow-Up
TC and UIC clinical consultant will arrange a time around thirty days after transition to discuss individual’s adjustment to community living. Collaborating agencies, including MCO staff, are invited.
TC will provide an update on the individual’s first month in the community.
Discussion points may include: Status of action plan items established in transition plan, Status of follow-up with medical providers, Changes to medication regimen, Identification of critical incidents, Discuss unforeseen issues/risks, Discuss strengths, goals, likes/dislikes, etc.
58

Poll Question
Name other activities you would conduct during your follow-up visits with Paula.
Answer options Determine if Paula has enough medications and diabetic
supplies. Discuss level of satisfaction with personal care assistants. Create goals and discuss progress in meeting them. Discuss any changes from provider appointments.
59

Is completed when a new risk assessment/inventory is completed
that requires a change in the Mitigation Plan when there is a change in residence address when there is a change in waiver or demonstration
services when there are calls for emergency back-up (e.g., If a
TC finds a individual had to use their back-up plan for transportation, caregiver, meal services, or emergency ambulance transport).
60
Post-Transition Update (Form E)

Occurs anytime a individual is no longer enrolled A individual is no longer eligible or interested in
transitioning. Once a transitioned individual has been
re-institutionalized for 30 days. Occurs only if an Informed Consent has been signed
61
Disenrollment/Withdrawal (Form D)

Re-transition after Re-institutionalization
If a individual was re-institutionalized for greater than 30 days after transition and before his/her MFP graduation date, then he/she is eligible to re-transition with MFP and use the remainder of the days left on his/her MFP clock.
62

63
Re-Enrollment: Post 365 Days
If an individual completes 365 days in the community and has been re-institutionalized in a qualified institution (e.g., nursing facility) for 90 days or more, then TC can start a new record for the individual, complete the enrollment and transition process again.

In Summary Transition coordinators have a vital
and complex role in success of individuals transitioning to the community from institutional care settings.
64

Questions
65

References
66
See handout: Care Management Coordination bibliography