Embed Size (px)
Citation preview

MondayAM
report 11-23-09
CCWeakness myalgiasarthralgias and fever
HPI
Bring it on
Toxicology
PVL
EKG
Immunology
Urinalysis Endocrine
PathologyMolecular
Microbiology
Microbiology
Heme
TTE
Coags
ROS
LFTs
Problem listPE I
Chemistry
PE II
MedsAllergiesFHSH
CT abdomenCT head
MRI head
Chest X-ray Abdomen X-ray
CT extremboneCT chest
Extremities X-ray
MRI chest MRI abdomen MRI extrembone
US
TEE Lecture
HPIHPI This is a 54 yo caucasian male who was transferred from Maria Parham ED for a several day history of generalized weakness muscle aches with associated subjective fevers (101 F) that started 5 days ago with a sore throat He was in his usual state of health who reports that approximately 3 weeks ago he hurt his back while lifting a heavy television As a result of this injury he began to experience sharp pains that would go down his left leg He was seen in the Maria Parham ED who obtained a MRI spine that revealed a pinched nerve from a possible slipped disc He was referred to an orthopedist in Raleigh who prescribed cyclobenzaprine and physical therapy with good response After that he developed a fever 5 days ago followed closely by myalgias nauseavomiting headaches that converted to migraines and general weakness He presented to Maria Parham again who diagnosed him with the flu gave fluid resuscitation and sent him home However his symptoms continued to a point where he could no longer walk and re-presented at Maria Parham ED for evaluation At that time he was noted by the physician there to have bilateral lower extremity weakness and diminished reflexes Out of concern for possible acute inflammatory demyelinating polyneuropathy (Guillian-Barre syndrome) he was transferred to UNC He also developed swelling and tenderness of the right knee on Sunday He developed a red patchy rash on his elbows 3 weeks ago He also developed purple papules on palms and soles that have worsened over the course of the day
Back
ROSGENERAL +appetite loss +chills no nightsweats mild weight loss due to appetite loss
HEENT +HA +Nauseavomiting + sore throat no vision changes
CHEST no chest pain
LUNGS no SOB no cough no hemoptysis
ABDOMEN no abdominal pain no diarrhea no blood in stools
GU no urinary symptoms no discharge
MSK generalized myalgias and arthralgias back pain
SKIN + jaundice bilateral elbows with red patchy rash with a few pustules petechial rash on right chest medial to mid axillary line purple pustules present on soles of hands and feet
NeuroPsych 3xoriented anxious general weakness
Back
PMH - Medsallergies - FHSHPMH HTN HLD Gilberts Syndrome Osteoarthritis in Neck Low back pain since 3 weeks with radicular pinched nerve at L3-L4 from lifting injury PSHAppendectomy at age 12 Kidney stones lithotripsy x 5 L inguinal hernia repair 2005 Crown lengthening procedure about 1 month to 6 weeks ago and a root canal a few weeks prior to that CURRENT MEDS HCTZ 25mg daily Simvastatin 40 mg daily Skelaxin (metaxalone) 400mg bid (muscle relaxant)ASA 81 mg Etodolac 400mg BID Vitamins E and C
AllergiesNKDA SH No tobacco No ETOH No history of IV drug use No history of sexually transmitted disease Currently working as support analyst at Lab Core in Burlington Lives in Henderson with wife 2 Children
FH 3 Cousin had toe fungus (JUST kidding) Noncontributory Back
PEPE T 987RR 22 HR 115 BP 11668 Sa O2 96 on RA
General Pt in acute distress diaphoretic HEENT Mouth dry no palatal petechia or aphtae yellow sclera no JVD Heme no LADCV S1 S2 rapid regular no murmur no rub no gallopLungs CTAB no wheezes Abdomen soft nontender nondistended +hemorrhoidsSkin Purpule pustules present on soles of hands and feet petechial rash on right chest medial to mid axillary line + jaundice bilateral elbows with red patchy rash with a few pustulesGU no dischargeMSK Decreased strength due to painExtremities R knee effusion no erythema no warmth pulses 2+ throughout Neuro AAOx 3 no focal DTRs 2+ bilaterally sensation intact Babinski negative CNs 2-12 grossly intact
Back
Skin lesions I
Next
Skin lesions II
Next
Skin lesions III
Back
Problem listWeakness
Myalgias
Arthralgias (+ right knee swelling)
Subjective fevers
Tachycardia
Low O2 sats
Jaundice
Headaches
Nauseavomiting
Dehydration
Pain
Skin lesions (elbow palms soles petechia on chest) Back
ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

CCWeakness myalgiasarthralgias and fever
HPI
Bring it on
Toxicology
PVL
EKG
Immunology
Urinalysis Endocrine
PathologyMolecular
Microbiology
Microbiology
Heme
TTE
Coags
ROS
LFTs
Problem listPE I
Chemistry
PE II
MedsAllergiesFHSH
CT abdomenCT head
MRI head
Chest X-ray Abdomen X-ray
CT extremboneCT chest
Extremities X-ray
MRI chest MRI abdomen MRI extrembone
US
TEE Lecture
HPIHPI This is a 54 yo caucasian male who was transferred from Maria Parham ED for a several day history of generalized weakness muscle aches with associated subjective fevers (101 F) that started 5 days ago with a sore throat He was in his usual state of health who reports that approximately 3 weeks ago he hurt his back while lifting a heavy television As a result of this injury he began to experience sharp pains that would go down his left leg He was seen in the Maria Parham ED who obtained a MRI spine that revealed a pinched nerve from a possible slipped disc He was referred to an orthopedist in Raleigh who prescribed cyclobenzaprine and physical therapy with good response After that he developed a fever 5 days ago followed closely by myalgias nauseavomiting headaches that converted to migraines and general weakness He presented to Maria Parham again who diagnosed him with the flu gave fluid resuscitation and sent him home However his symptoms continued to a point where he could no longer walk and re-presented at Maria Parham ED for evaluation At that time he was noted by the physician there to have bilateral lower extremity weakness and diminished reflexes Out of concern for possible acute inflammatory demyelinating polyneuropathy (Guillian-Barre syndrome) he was transferred to UNC He also developed swelling and tenderness of the right knee on Sunday He developed a red patchy rash on his elbows 3 weeks ago He also developed purple papules on palms and soles that have worsened over the course of the day
Back
ROSGENERAL +appetite loss +chills no nightsweats mild weight loss due to appetite loss
HEENT +HA +Nauseavomiting + sore throat no vision changes
CHEST no chest pain
LUNGS no SOB no cough no hemoptysis
ABDOMEN no abdominal pain no diarrhea no blood in stools
GU no urinary symptoms no discharge
MSK generalized myalgias and arthralgias back pain
SKIN + jaundice bilateral elbows with red patchy rash with a few pustules petechial rash on right chest medial to mid axillary line purple pustules present on soles of hands and feet
NeuroPsych 3xoriented anxious general weakness
Back
PMH - Medsallergies - FHSHPMH HTN HLD Gilberts Syndrome Osteoarthritis in Neck Low back pain since 3 weeks with radicular pinched nerve at L3-L4 from lifting injury PSHAppendectomy at age 12 Kidney stones lithotripsy x 5 L inguinal hernia repair 2005 Crown lengthening procedure about 1 month to 6 weeks ago and a root canal a few weeks prior to that CURRENT MEDS HCTZ 25mg daily Simvastatin 40 mg daily Skelaxin (metaxalone) 400mg bid (muscle relaxant)ASA 81 mg Etodolac 400mg BID Vitamins E and C
AllergiesNKDA SH No tobacco No ETOH No history of IV drug use No history of sexually transmitted disease Currently working as support analyst at Lab Core in Burlington Lives in Henderson with wife 2 Children
FH 3 Cousin had toe fungus (JUST kidding) Noncontributory Back
PEPE T 987RR 22 HR 115 BP 11668 Sa O2 96 on RA
General Pt in acute distress diaphoretic HEENT Mouth dry no palatal petechia or aphtae yellow sclera no JVD Heme no LADCV S1 S2 rapid regular no murmur no rub no gallopLungs CTAB no wheezes Abdomen soft nontender nondistended +hemorrhoidsSkin Purpule pustules present on soles of hands and feet petechial rash on right chest medial to mid axillary line + jaundice bilateral elbows with red patchy rash with a few pustulesGU no dischargeMSK Decreased strength due to painExtremities R knee effusion no erythema no warmth pulses 2+ throughout Neuro AAOx 3 no focal DTRs 2+ bilaterally sensation intact Babinski negative CNs 2-12 grossly intact
Back
Skin lesions I
Next
Skin lesions II
Next
Skin lesions III
Back
Problem listWeakness
Myalgias
Arthralgias (+ right knee swelling)
Subjective fevers
Tachycardia
Low O2 sats
Jaundice
Headaches
Nauseavomiting
Dehydration
Pain
Skin lesions (elbow palms soles petechia on chest) Back
ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

HPI
Bring it on
Toxicology
PVL
EKG
Immunology
Urinalysis Endocrine
PathologyMolecular
Microbiology
Microbiology
Heme
TTE
Coags
ROS
LFTs
Problem listPE I
Chemistry
PE II
MedsAllergiesFHSH
CT abdomenCT head
MRI head
Chest X-ray Abdomen X-ray
CT extremboneCT chest
Extremities X-ray
MRI chest MRI abdomen MRI extrembone
US
TEE Lecture
HPIHPI This is a 54 yo caucasian male who was transferred from Maria Parham ED for a several day history of generalized weakness muscle aches with associated subjective fevers (101 F) that started 5 days ago with a sore throat He was in his usual state of health who reports that approximately 3 weeks ago he hurt his back while lifting a heavy television As a result of this injury he began to experience sharp pains that would go down his left leg He was seen in the Maria Parham ED who obtained a MRI spine that revealed a pinched nerve from a possible slipped disc He was referred to an orthopedist in Raleigh who prescribed cyclobenzaprine and physical therapy with good response After that he developed a fever 5 days ago followed closely by myalgias nauseavomiting headaches that converted to migraines and general weakness He presented to Maria Parham again who diagnosed him with the flu gave fluid resuscitation and sent him home However his symptoms continued to a point where he could no longer walk and re-presented at Maria Parham ED for evaluation At that time he was noted by the physician there to have bilateral lower extremity weakness and diminished reflexes Out of concern for possible acute inflammatory demyelinating polyneuropathy (Guillian-Barre syndrome) he was transferred to UNC He also developed swelling and tenderness of the right knee on Sunday He developed a red patchy rash on his elbows 3 weeks ago He also developed purple papules on palms and soles that have worsened over the course of the day
Back
ROSGENERAL +appetite loss +chills no nightsweats mild weight loss due to appetite loss
HEENT +HA +Nauseavomiting + sore throat no vision changes
CHEST no chest pain
LUNGS no SOB no cough no hemoptysis
ABDOMEN no abdominal pain no diarrhea no blood in stools
GU no urinary symptoms no discharge
MSK generalized myalgias and arthralgias back pain
SKIN + jaundice bilateral elbows with red patchy rash with a few pustules petechial rash on right chest medial to mid axillary line purple pustules present on soles of hands and feet
NeuroPsych 3xoriented anxious general weakness
Back
PMH - Medsallergies - FHSHPMH HTN HLD Gilberts Syndrome Osteoarthritis in Neck Low back pain since 3 weeks with radicular pinched nerve at L3-L4 from lifting injury PSHAppendectomy at age 12 Kidney stones lithotripsy x 5 L inguinal hernia repair 2005 Crown lengthening procedure about 1 month to 6 weeks ago and a root canal a few weeks prior to that CURRENT MEDS HCTZ 25mg daily Simvastatin 40 mg daily Skelaxin (metaxalone) 400mg bid (muscle relaxant)ASA 81 mg Etodolac 400mg BID Vitamins E and C
AllergiesNKDA SH No tobacco No ETOH No history of IV drug use No history of sexually transmitted disease Currently working as support analyst at Lab Core in Burlington Lives in Henderson with wife 2 Children
FH 3 Cousin had toe fungus (JUST kidding) Noncontributory Back
PEPE T 987RR 22 HR 115 BP 11668 Sa O2 96 on RA
General Pt in acute distress diaphoretic HEENT Mouth dry no palatal petechia or aphtae yellow sclera no JVD Heme no LADCV S1 S2 rapid regular no murmur no rub no gallopLungs CTAB no wheezes Abdomen soft nontender nondistended +hemorrhoidsSkin Purpule pustules present on soles of hands and feet petechial rash on right chest medial to mid axillary line + jaundice bilateral elbows with red patchy rash with a few pustulesGU no dischargeMSK Decreased strength due to painExtremities R knee effusion no erythema no warmth pulses 2+ throughout Neuro AAOx 3 no focal DTRs 2+ bilaterally sensation intact Babinski negative CNs 2-12 grossly intact
Back
Skin lesions I
Next
Skin lesions II
Next
Skin lesions III
Back
Problem listWeakness
Myalgias
Arthralgias (+ right knee swelling)
Subjective fevers
Tachycardia
Low O2 sats
Jaundice
Headaches
Nauseavomiting
Dehydration
Pain
Skin lesions (elbow palms soles petechia on chest) Back
ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

HPIHPI This is a 54 yo caucasian male who was transferred from Maria Parham ED for a several day history of generalized weakness muscle aches with associated subjective fevers (101 F) that started 5 days ago with a sore throat He was in his usual state of health who reports that approximately 3 weeks ago he hurt his back while lifting a heavy television As a result of this injury he began to experience sharp pains that would go down his left leg He was seen in the Maria Parham ED who obtained a MRI spine that revealed a pinched nerve from a possible slipped disc He was referred to an orthopedist in Raleigh who prescribed cyclobenzaprine and physical therapy with good response After that he developed a fever 5 days ago followed closely by myalgias nauseavomiting headaches that converted to migraines and general weakness He presented to Maria Parham again who diagnosed him with the flu gave fluid resuscitation and sent him home However his symptoms continued to a point where he could no longer walk and re-presented at Maria Parham ED for evaluation At that time he was noted by the physician there to have bilateral lower extremity weakness and diminished reflexes Out of concern for possible acute inflammatory demyelinating polyneuropathy (Guillian-Barre syndrome) he was transferred to UNC He also developed swelling and tenderness of the right knee on Sunday He developed a red patchy rash on his elbows 3 weeks ago He also developed purple papules on palms and soles that have worsened over the course of the day
Back
ROSGENERAL +appetite loss +chills no nightsweats mild weight loss due to appetite loss
HEENT +HA +Nauseavomiting + sore throat no vision changes
CHEST no chest pain
LUNGS no SOB no cough no hemoptysis
ABDOMEN no abdominal pain no diarrhea no blood in stools
GU no urinary symptoms no discharge
MSK generalized myalgias and arthralgias back pain
SKIN + jaundice bilateral elbows with red patchy rash with a few pustules petechial rash on right chest medial to mid axillary line purple pustules present on soles of hands and feet
NeuroPsych 3xoriented anxious general weakness
Back
PMH - Medsallergies - FHSHPMH HTN HLD Gilberts Syndrome Osteoarthritis in Neck Low back pain since 3 weeks with radicular pinched nerve at L3-L4 from lifting injury PSHAppendectomy at age 12 Kidney stones lithotripsy x 5 L inguinal hernia repair 2005 Crown lengthening procedure about 1 month to 6 weeks ago and a root canal a few weeks prior to that CURRENT MEDS HCTZ 25mg daily Simvastatin 40 mg daily Skelaxin (metaxalone) 400mg bid (muscle relaxant)ASA 81 mg Etodolac 400mg BID Vitamins E and C
AllergiesNKDA SH No tobacco No ETOH No history of IV drug use No history of sexually transmitted disease Currently working as support analyst at Lab Core in Burlington Lives in Henderson with wife 2 Children
FH 3 Cousin had toe fungus (JUST kidding) Noncontributory Back
PEPE T 987RR 22 HR 115 BP 11668 Sa O2 96 on RA
General Pt in acute distress diaphoretic HEENT Mouth dry no palatal petechia or aphtae yellow sclera no JVD Heme no LADCV S1 S2 rapid regular no murmur no rub no gallopLungs CTAB no wheezes Abdomen soft nontender nondistended +hemorrhoidsSkin Purpule pustules present on soles of hands and feet petechial rash on right chest medial to mid axillary line + jaundice bilateral elbows with red patchy rash with a few pustulesGU no dischargeMSK Decreased strength due to painExtremities R knee effusion no erythema no warmth pulses 2+ throughout Neuro AAOx 3 no focal DTRs 2+ bilaterally sensation intact Babinski negative CNs 2-12 grossly intact
Back
Skin lesions I
Next
Skin lesions II
Next
Skin lesions III
Back
Problem listWeakness
Myalgias
Arthralgias (+ right knee swelling)
Subjective fevers
Tachycardia
Low O2 sats
Jaundice
Headaches
Nauseavomiting
Dehydration
Pain
Skin lesions (elbow palms soles petechia on chest) Back
ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

ROSGENERAL +appetite loss +chills no nightsweats mild weight loss due to appetite loss
HEENT +HA +Nauseavomiting + sore throat no vision changes
CHEST no chest pain
LUNGS no SOB no cough no hemoptysis
ABDOMEN no abdominal pain no diarrhea no blood in stools
GU no urinary symptoms no discharge
MSK generalized myalgias and arthralgias back pain
SKIN + jaundice bilateral elbows with red patchy rash with a few pustules petechial rash on right chest medial to mid axillary line purple pustules present on soles of hands and feet
NeuroPsych 3xoriented anxious general weakness
Back
PMH - Medsallergies - FHSHPMH HTN HLD Gilberts Syndrome Osteoarthritis in Neck Low back pain since 3 weeks with radicular pinched nerve at L3-L4 from lifting injury PSHAppendectomy at age 12 Kidney stones lithotripsy x 5 L inguinal hernia repair 2005 Crown lengthening procedure about 1 month to 6 weeks ago and a root canal a few weeks prior to that CURRENT MEDS HCTZ 25mg daily Simvastatin 40 mg daily Skelaxin (metaxalone) 400mg bid (muscle relaxant)ASA 81 mg Etodolac 400mg BID Vitamins E and C
AllergiesNKDA SH No tobacco No ETOH No history of IV drug use No history of sexually transmitted disease Currently working as support analyst at Lab Core in Burlington Lives in Henderson with wife 2 Children
FH 3 Cousin had toe fungus (JUST kidding) Noncontributory Back
PEPE T 987RR 22 HR 115 BP 11668 Sa O2 96 on RA
General Pt in acute distress diaphoretic HEENT Mouth dry no palatal petechia or aphtae yellow sclera no JVD Heme no LADCV S1 S2 rapid regular no murmur no rub no gallopLungs CTAB no wheezes Abdomen soft nontender nondistended +hemorrhoidsSkin Purpule pustules present on soles of hands and feet petechial rash on right chest medial to mid axillary line + jaundice bilateral elbows with red patchy rash with a few pustulesGU no dischargeMSK Decreased strength due to painExtremities R knee effusion no erythema no warmth pulses 2+ throughout Neuro AAOx 3 no focal DTRs 2+ bilaterally sensation intact Babinski negative CNs 2-12 grossly intact
Back
Skin lesions I
Next
Skin lesions II
Next
Skin lesions III
Back
Problem listWeakness
Myalgias
Arthralgias (+ right knee swelling)
Subjective fevers
Tachycardia
Low O2 sats
Jaundice
Headaches
Nauseavomiting
Dehydration
Pain
Skin lesions (elbow palms soles petechia on chest) Back
ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

PMH - Medsallergies - FHSHPMH HTN HLD Gilberts Syndrome Osteoarthritis in Neck Low back pain since 3 weeks with radicular pinched nerve at L3-L4 from lifting injury PSHAppendectomy at age 12 Kidney stones lithotripsy x 5 L inguinal hernia repair 2005 Crown lengthening procedure about 1 month to 6 weeks ago and a root canal a few weeks prior to that CURRENT MEDS HCTZ 25mg daily Simvastatin 40 mg daily Skelaxin (metaxalone) 400mg bid (muscle relaxant)ASA 81 mg Etodolac 400mg BID Vitamins E and C
AllergiesNKDA SH No tobacco No ETOH No history of IV drug use No history of sexually transmitted disease Currently working as support analyst at Lab Core in Burlington Lives in Henderson with wife 2 Children
FH 3 Cousin had toe fungus (JUST kidding) Noncontributory Back
PEPE T 987RR 22 HR 115 BP 11668 Sa O2 96 on RA
General Pt in acute distress diaphoretic HEENT Mouth dry no palatal petechia or aphtae yellow sclera no JVD Heme no LADCV S1 S2 rapid regular no murmur no rub no gallopLungs CTAB no wheezes Abdomen soft nontender nondistended +hemorrhoidsSkin Purpule pustules present on soles of hands and feet petechial rash on right chest medial to mid axillary line + jaundice bilateral elbows with red patchy rash with a few pustulesGU no dischargeMSK Decreased strength due to painExtremities R knee effusion no erythema no warmth pulses 2+ throughout Neuro AAOx 3 no focal DTRs 2+ bilaterally sensation intact Babinski negative CNs 2-12 grossly intact
Back
Skin lesions I
Next
Skin lesions II
Next
Skin lesions III
Back
Problem listWeakness
Myalgias
Arthralgias (+ right knee swelling)
Subjective fevers
Tachycardia
Low O2 sats
Jaundice
Headaches
Nauseavomiting
Dehydration
Pain
Skin lesions (elbow palms soles petechia on chest) Back
ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

PEPE T 987RR 22 HR 115 BP 11668 Sa O2 96 on RA
General Pt in acute distress diaphoretic HEENT Mouth dry no palatal petechia or aphtae yellow sclera no JVD Heme no LADCV S1 S2 rapid regular no murmur no rub no gallopLungs CTAB no wheezes Abdomen soft nontender nondistended +hemorrhoidsSkin Purpule pustules present on soles of hands and feet petechial rash on right chest medial to mid axillary line + jaundice bilateral elbows with red patchy rash with a few pustulesGU no dischargeMSK Decreased strength due to painExtremities R knee effusion no erythema no warmth pulses 2+ throughout Neuro AAOx 3 no focal DTRs 2+ bilaterally sensation intact Babinski negative CNs 2-12 grossly intact
Back
Skin lesions I
Next
Skin lesions II
Next
Skin lesions III
Back
Problem listWeakness
Myalgias
Arthralgias (+ right knee swelling)
Subjective fevers
Tachycardia
Low O2 sats
Jaundice
Headaches
Nauseavomiting
Dehydration
Pain
Skin lesions (elbow palms soles petechia on chest) Back
ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Skin lesions I
Next
Skin lesions II
Next
Skin lesions III
Back
Problem listWeakness
Myalgias
Arthralgias (+ right knee swelling)
Subjective fevers
Tachycardia
Low O2 sats
Jaundice
Headaches
Nauseavomiting
Dehydration
Pain
Skin lesions (elbow palms soles petechia on chest) Back
ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Skin lesions II
Next
Skin lesions III
Back
Problem listWeakness
Myalgias
Arthralgias (+ right knee swelling)
Subjective fevers
Tachycardia
Low O2 sats
Jaundice
Headaches
Nauseavomiting
Dehydration
Pain
Skin lesions (elbow palms soles petechia on chest) Back
ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Skin lesions III
Back
Problem listWeakness
Myalgias
Arthralgias (+ right knee swelling)
Subjective fevers
Tachycardia
Low O2 sats
Jaundice
Headaches
Nauseavomiting
Dehydration
Pain
Skin lesions (elbow palms soles petechia on chest) Back
ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Problem listWeakness
Myalgias
Arthralgias (+ right knee swelling)
Subjective fevers
Tachycardia
Low O2 sats
Jaundice
Headaches
Nauseavomiting
Dehydration
Pain
Skin lesions (elbow palms soles petechia on chest) Back
ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

ChemistrySodium 140
Potassium 39Chloride 104
CO2 30BUN 39
Creatinine 154 (GFR 45) Stage 3Glucose 115
Calcium 8Magnesium 18Phosphorus 4
CK 134CK-MB 36
Troponin 048
Protein 53Albumin 27
LD 687 Back
LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

LFTs
Bilirubin 42 (direct 12)AST 234ALT 435AP 113GGT 65
Back
Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Coags
INR 15PTT 332
Back
Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Heme
CBC 97 (peak 4days later 172)Platelets 73
HampH 121345
Back
Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Urinalysis
Urine sodium lt5FeNa 0
UAWBC 6
LE+Prot 1+RBC 17
Back
Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Endocrine
TSH 353Cortisol normal
Back
Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Immunology
CRP gt45HIV negative
Hepatitis BC negativeANA negative
ANCA negativeRF negative
Glomerular basement membrane -Ab negative
Back
Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Microbiology
BC (33)MRSA (community acquired)
Took 3 days to clear BCs
UC (MRSA)
Vitrous fluid negative 2+PMN
Knee + L34 disk negative (50000 cells 95 neutrophils)
Back
MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

MolecularMicrobiology
Toxoplasma negativeEBV negativeCMV negativeVZV negativeHSV negative
Chlamydia negativeGC negative
Back
Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Toxicology
Back
Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Pathology
Back
DiagnosisSynovium right knee biopsy
- Acute and chronic synovitis
EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

EKG
Sinustachycardia
Back
TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

TTE
EF 55No vegetations
Back
TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

TEE
No vegetations
Back
Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Renal US
No hydronephrosis or nephrolithiasis
Back
PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

PVL
No DVT
Back
Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Chest x-ray
1 Diffuse patchy opacities identified bilaterally consistent with mild pulmonary edema versus infection 2 Question small bilateral pleural effusions versus overlying soft tissue
Back
CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

CT head
No acute intracranial abnormality is identified
Back
MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

MRI spine
Back
Cervical spineIMPRESSION Multilevel degenerative disk disease No abnormal cord signal or enhancement
Thoracic spineIMPRESSION Unremarkable pre-and postcontrast MRI of the thoracic spine
Lumbar spineIMPRESSION Increased STIR signal and enhancement involving theposterior elements from L3 through L5 as well as the dorsalepidural space at this region This could be related to inflammatory changes from recent lumbar puncture versus aninfectious process No drainable fluid collections or masseffect in the spinal canal is present
MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

MRI head
Next
MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

MRI head
Back
CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

CT chestabdomenpelvis
IMPRESSION
1 Distal position of right PICC line as above 2 Splenic and renal hypodensities are indeterminant given size3 Trace pelvic fluid Gas within bladder may be secondary to Foley placement 4 Mild splenomegaly
Back
Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Endocarditisbull Infectious Endocarditis (IE) an infection of
the heartrsquos endocardial surfacebull Classified into four groups
ndash Native Valve IEndash Prosthetic Valve IEndash Intravenous drug abuse (IVDA) IEndash Nosocomial IE
Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Further Classificationbull Acute
ndash Affects normal heart valves
ndash Rapidly destructivendash Metastatic focindash If not treated usually
fatal within 6 weeks
Organisms Staphylococcus aureus Streptococcus pyogenes Streptococcus pneumoniae
bull Subacutendash Often affects damaged
heart valvesndash Indolent naturendash If not treated usually
fatal by one year
OrganismsStreptococcus viridansEnterococcus
Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Infective Endocarditis
bull Gram negative organismsndash P aeruginosa most commonndash HACEK - slow growing fastidious organisms that
may need 3 weeks to grow out of culturebull Haemophilus spbull Actinobacillusbull Cardiobacteriumbull Eikenellabull Kingella
Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Infective Endocarditis
bull Case rate may vary between 2-3 cases 100000 to as high as 15-30100000 depending on incidence of iv drug abuse and age of the populationndash 55-75 of patients with native valve endocarditis (NVE)
have underlying valve abnormalitiesbull MVPbull Rheumaticbull Congenitalbull ASH orbull iv drug abuse
Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Infective Endocarditis
bull Adult populationndash Rheumatic Heart Disease
bull 20 ndash 25 of cases of IE in 1970rsquos amp 80rsquosbull 7 ndash 18 of cases in recent reported seriesbull Mitral site more common in womenbull Aortic site more common in men
ndash Congenital Heart Diseasebull 10 ndash 20 of cases in young adultsbull 8 of cases in older adultsbull PDA VSD bicuspid aortic valve (esp in mengt60)
Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Infective Endocarditis
bull Intravenous Drug Abusendash Risk is 2 ndash 5 per ptyearndash Tendency to involve right-sided valves
bull Distribution in clinical seriesndash 46 ndash 78 tricuspidndash 24 ndash 32 mitralndash 8 ndash 19 aortic
ndash Underlying valve normal in 75 ndash 93ndash S aureus predominant organism (gt50 60-70
of tricuspid cases)
Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Clinical Features I
bull Interval between index bacteremia amp onset of sxrsquos usually lt 2 weeks
bull May be substantially longer in early PVE
bull Fever most common signbull May be absent in elderlydebilitated pt
bull Murmur present in 80 ndash 85bull Generally indication of underlying lesionbull Frequently absent in tricuspid IE
bull Changing murmur
Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Clinical Features II
bull Acutendash High grade fever and
chillsndash SOBndash Arthralgias
myalgiasndash Abdominal painndash Pleuritic chest painndash Back pain
bull Subacutendash Low grade feverndash Anorexiandash Weight lossndash Fatiguendash Arthralgias
myalgiasndash Abdominal painndash NV
Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Petechiae1Nonspecific2Often located on extremities
or mucous membranes
Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Janeway Lesions
Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Janeway Lesions
1 More specific2 Erythematous blanching macules 3 Nonpainful4 Located on palms and soles
Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Splinter Hemorrhage
Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Splinter Hemorrhages
1 Nonspecific2 Nonblanching3 Linear reddish-brown lesions found under the nail bed4 Usually do NOT extend the entire length of the nail
Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Oslerrsquos Nodes
1 More specific2 Painful and erythematous nodules3 Located on pulp of fingers and toes4 More common in subacute IE
Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Subconjunctival Hemorrhages
Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Rothrsquos Spots
Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Complications
bull Four etiologiesndash Embolicndash Local spread of infectionndash Metastatic spread of infectionndash Formation of immune complexes ndash
glomerulonephritis and arthritis
Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Embolic Complications
bull Occur in up to 40 of patients with IE
bull Strokebull Myocardial Infarction
ndash Fragments of valvular vegetation or vegetation-induced stenosis of coronary ostia
bull Ischemic limbsbull Hypoxia from pulmonary embolibull Abdominal pain (splenic or renal infarction)
Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Septic Pulmonary Emboli
bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

bull Heart failurendash Extensive valvular damage
bull Paravalvular abscess (30-40)ndash Most common in aortic valve IVDA and S aureusndash May extend into adjacent conduction tissue causing
arrythmiasndash Higher rates of embolization and mortality
bull Pericarditisbull Fistulous intracardiac connections
Local Spread of Infection
Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Modified Duke Criteria2 Major OR 1 Major + 3 Minor OR 5 Minor
Major (microbiology) a)typical organisms x 2 blood cultures (eg Strep viridans S bovis HACEK S aureus or enterococcus) with no primary source b)persistent bacteremia (gt12 hours) c)33 or 34 positive blood cultures
Major (valve) a)echo w vegetationb)b) new valve regurgitation
Minor a)predisposing cardiac condition or IDU b)fever gt 38degC (1004degF)c)vascular phenomenon (arterial emboli mycotic aneurysm intracerebral bleed conjunctival hemorrhage Janeway lesions)d)immune phenomenon (glomerulonephritis Osler nodes Roth spots positive rheumatoid factor)e)positive blood culture not meeting above criteria and f)echo--abnl but not diagnostic
Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Antibiotic Therapy
bull Effective antimicrobial treatment should lead to defervescence within 7 ndash 10 days
bullEmpiric acute endocarditis [nafcillin or oxacillin 2g IV q4h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg IV q12h + gentamicin 1mgkg IV q8h]
bullEmpiric subacute endocarditis [ampicillinsulbactam 3g IV q 6h + gentamicin or tobramycin 1mgkg IV q8h] OR [vancomycin 15mgkg q12h + [ceftriaxone 2g IV q12hOR gentamicintobramycin 1 mgkg IV q8h]
Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Bacteremia Risk Related to Dental Procedures
Estimated cumulative exposure of 5370 minutes of bacteremia month related to chewing food and oral hygiene measure Vs 6-30 minutes of bacteremia associated with single tooth extraction (Guntheroth 1984)
Tooth brushing twice daily for 1 year has estimated IE risk 154000 times greater than single tooth extraction (Roberts 1999)
Cumulative exposure to bacteremia over 1 year may be as high as 56 million times greater than that from a single tooth extraction (Roberts 1999)
Prophylactic Therapy
Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Cardiac Conditions for which IE Prophylaxis Recommended for Dental Procedures
bull Prosthetic Cardiac Valve
bull Previous Infective Endocarditis
bull Congenital Heart Disease (CHD)
bull Unrepaired Cyanotic CHD Including Palliative Shunts and Conduits
bull Completely Repaired CHD with Prosthetic Material or Device whether by Surgery or by Catheter Intervention during the first 6 months after the procedure
bull Repaired CHD with Residual Defects at the Site or Adjacent to the Site of a Prosthetic Patch or Prosthetic Device (which Inhibit Endothelialization)
bull Cardiac Transplant Recipients who Develop Valvulopathy
bull All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Endocarditis Prophylaxis NOT Recommended
bull ldquoProbably Innocent Murmurrdquo never evaluated by cardiologist but getting SBE prophylaxis ldquojust in caserdquo
bull Genitourinary or Gastrointestinal Tract Procedures
IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

IE Prophylaxis Dosing for Dental Procedure
bull Oral Administer 30-60 minutes prior to procedure
bull Amoxicillin 50 mgkg (maximum 2 grams)bull Clindamycin 20 mgkg (maximum 600 milligrams)bull Cephalexin or equivalent 1st2nd Generation Cephalosporin 50mgkg (max 2 grams)bull Azithromycin or Clarithromycin 15 mgkg (max 500 mg)
bull IVor IM Administer 30-60 minutes prior to procedure
bull Ampicillin 50 mgkg (maximum 2 grams)bull Cephazolin or Ceftriaxone 50 mgkg (maximum 1 gram)bull Clindamycin 20 mgkg (maximum 600 mg)
First choice unless allergic
Wilson W Taubert KA Gerwitz M et al Circulation 2007115
Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Thank you
Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Infective Endocarditis
bull Pathologyndash NVE infection is largely confined to leafletsndash PVE infection commonly extends beyond valve
ring into annulusperiannular tissuebull Ring abscessesbull Septal abscessesbull Fistulaebull Prosthetic dehiscence
ndash Invasive infection more common in aortic position and if onset is early
Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Infective Endocarditis
bull Pathogenesis
Endothelial damage
Platelet-fibrin thrombi
Microorganism adherence
Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Pathophysiology
1 Turbulent blood flow disrupts the endocardium making it ldquostickyrdquo
2 Bacteremia delivers the organisms to the endocardial surface
3 Adherence of the organisms to the endocardial surface
4 Eventual invasion of the valvular leaflets
Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Endocarditis Prophylaxis NOT RecommendedNegligible-risk Category(No greater risk than the general population)1048708 Isolated secundum atrial septal defect1048708 Surgical repair of atrial septal defect ventricular septaldefect or patent ductus arteriosus (without residuabeyond 6 mo)1048708 Previous coronary artery bypass graft surgery1048708 Mitral valve prolapse without valvar regurgitation1048708 Physiologic functional or innocent heart murmurs1048708 Previous Kawasaki disease without valvar dysfunction1048708 Previous rheumatic fever without valvar dysfunction1048708 Cardiac pacemakers (intravascular and epicardial) andimplanted defibrillatorsAmerican Heart Association SBE Guidelines- JAMA 19972771794
Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy

Infectious Bacterial EndocarditisProphylaxis No Longer Recommendedfor the Following Conditions1048708 Ventricular Septal Defect1048708 Ostium Primum Atrial Septal Defect1048708 Pulmonary Stenosis1048708 Aortic StenosisInsufficiency1048708 Mitral Valve Prolapse with Valve Regurgitation1048708 Patent Ductus Arteriosus1048708 Coarctation of Aorta1048708 Rheumatic Heart Disease1048708 Hypertrophic Cardiomyopathy












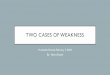



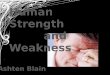
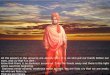





![[Critica] Apple's Weakness](https://img.pdfslide.us/doc/110x75/54b2dc494a7959d10e8b456b/critica-apples-weakness.jpg)