Embed Size (px)
Citation preview

Allogeneic haematopoietic stem-cell transplantationwas developed as a strategy to prevent the bone-marrow toxicity that is caused by intensive chemora-diotherapy regimens (BOX 1a). This approach cures asignificant percentage of patients who have otherwisefatal haematological malignancies1. Reciprocalimmune reactions between donor and recipient are aprincipal feature of allogeneic stem-cell transplanta-tion, and have both deleterious and beneficial conse-quences. Key to these immune reactions are humanleukocyte antigen (HLA) class I and II molecules,which are expressed on the cell surface and presentpeptides for recognition by CD8+ and CD4+ T cells,respectively2. T cells in the graft can react against recip-ient HLA–peptide complexes, leading to graft-versus-host disease (GVHD) in the skin, gastrointestinal tractand/or liver3. Less frequently, residual T cells in thehost react against donor stem cells, leading to graftrejection. The highest risk of GVHD and graft rejec-tion occurs in transplants between HLA-MISMATCHED indi-viduals. However, unless donor T cells are depletedfrom the stem-cell graft, GVHD also frequently occursafter HLA-matched stem-cell transplantation becauseof recognition of minor histocompatibility antigens,which are polymorphic peptides that are displayed byHLA molecules of recipient cells4.
Animal models and human studies of allogeneicstem-cell transplantation show that immunologicalnon-identity between donor and recipient is alsoresponsible for a graft-versus-leukaemia (GVL) effectthat leads to tumour eradication5,6. In humans, recipi-ents of allogeneic stem-cell transplants were found tohave a lower risk of leukaemic relapse than recipients ofSYNGENEIC STEM-CELL TRANSPLANTS or recipients of T-cell-depleted allogeneic stem-cell transplants7,8. The GVLeffect is greatest in the subset of allogeneic-stem-cell-transplant recipients with GVHD, but the risk of relapseis also reduced in patients without GVHD7,9. Thepotency of the GVL effect is illustrated by the use ofdonor-lymphocyte infusion to treat patients withleukaemia who experience a relapse after receiving atransplant. Remarkably, donor-lymphocyte infusioncan induce a durable remission in most patients withchronic myelogenous leukaemia (CML) and in somepatients with acute leukaemia10,11.
The recognition of the GVL effect is now drivingthe evolution of allogeneic stem-cell transplantationtowards an immunotherapeutic approach that doesnot require toxic chemoradiotherapy for tumoureradication. Animal experiments have shown that aless intensive approach, known as NON-MYELOABLATIVE
CONDITIONING, can suppress recipient immunity
MOLECULES AND MECHANISMS OFTHE GRAFT-VERSUS-LEUKAEMIAEFFECTMarie Bleakley and Stanley R. Riddell
The ability of allogeneic bone-marrow cells and peripheral-blood stem cells to cure leukaemiaremains the most striking example of the ability of the human immune system to recognize anddestroy tumours. However, harnessing this ‘graft-versus-leukaemia’ effect to improve outcome forpatients with advanced disease and segregating it from graft-versus-host disease have proven tobe key challenges. The recent identification of molecules that are specifically expressed byleukaemic cells and that can be recognized by T cells has indicated that immunological reactivitycan be targeted. This anticancer specificity of T cells should soon be routinely incorporated intoallogeneic stem-cell transplant regimens to promote tumour eradication.
HLA MISMATCHED
Individuals mismatched (that is,non-identical) at one or morealleles of the human leukocyteantigen (HLA) complex.
SYNGENEIC STEM-CELL
TRANSPLANTATION
Stem-cell transplantationperformed between geneticallyidentical twins.
NATURE REVIEWS | CANCER VOLUME 4 | MAY 2004 | 371
Fred Hutchinson CancerResearch Center,1100 Fairview Avenue,Seattle, Washington 98109, USA.Correspondence to S.R.R.e-mail: [email protected]:10.1038/nrc1365
REVIEWS

NON-MYELOABLATIVE
CONDITIONING
Chemotherapy and/or low-doseirradiation given to prepare apatient for a haematopoieticstem-cell graft from anotherindividual. The purpose is toimmunosuppress the recipient,but the dose ofchemoradiotherapy is notsufficient to irreversibly damagethe patient’s own bone marrow.
PANCYTOPAENIA
The severe reduction in thenumber of red blood cells, whiteblood cells and platelets that isseen after intensivechemotherapy.
HAPLO-IDENTICAL STEM-CELL
TRANSPLANTATION
Stem-cell transplantationperformed between individualswho are genetically identical forhalf of the human leukocyteantigen molecules.
372 | MAY 2004 | VOLUME 4 www.nature.com/reviews/cancer
R E V I E W S
T-cell-depleted HAPLO-IDENTICAL STEM-CELL TRANSPLANTATION
in the subset of recipients that do not express the donorHLA class I molecules that are required to engage NK-cell inhibitory receptors19, and this mechanism has beenrecently reviewed20. Here, we will focus on the identifi-cation of target molecules recognized by T cells thatmight contribute to a GVL effect after HLA-matchedallogeneic stem-cell transplantation, and on the poten-tial to use the adoptive transfer of T cells specific forantigens that are expressed by leukaemia to augmentGVL activity.
Minor histocompatibility antigens HLA molecules alert the immune system to infection bydisplaying peptide derivatives of antigenic proteins atthe cell surface for recognition by T cells. In the settingof allogeneic HLA-matched stem-cell transplantation,endogenous proteins in recipient cells that differ fromthose of the donor, because of genetic polymorphisms,can provide distinct HLA-binding peptides. These serveas minor histocompatibility antigens for donor T cells(BOX 2). The potential for minor histocompatibility anti-gens to be targets for a GVL response after allogeneicstem-cell transplantation was shown in mouse models.In these mice, adoptive transfer of CD8+ cytotoxic T cells (CTLs) that were specific for a single reci-pient minor histocompatibility antigen eradicatedleukaemia21. After allogeneic stem-cell transplantationin humans, both CD8+ and CD4+ T cells that recognizeminor histocompatibility antigens on recipient cells areactivated in vivo and can be isolated for in vitroanalysis22. The potential for CD8+ T cells to recognizehuman leukaemia has been investigated extensively.CD8+ minor-histocompatibility-antigen-specific T-cellclones lyse primary AML and acute lymphoblasticleukaemia (ALL) cells, inhibit the growth of leukaemiccolonies and prevent the engraftment of AML in non-obese diabetic/severe combined immunodeficiency(NOD/SCID) mice. This indicates that the earliestleukaemic progenitors express minor histocompatibilityantigens and are targets for T cells22–24. Unfortunately,some T cells that are specific for minor histocompatibil-ity antigens also recognize non-haematopoietic cells andcan cause GVHD.
Methods have been developed for identifying thepolymorphic genes that encode minor histocompati-bility antigens (BOX 3), and the discovery of these genesis providing insight into the basis for immunogenicity.Individual minor histocompatibility antigens also havethe potential to serve as targets for a GVL effect with-out inducing GVHD. The HLA restriction, encodinggene and/or chromosomal location, and amino-acidsequence of 16 minor histocompatibility antigens havebeen determined (TABLE 1), and this list is expandingrapidly25–41. The immunogenicity of minor histocom-patibility antigens typically results from one or morenucleotide polymorphisms in the homologous donoror recipient genes. This enables the presentation ofpeptides by HLA molecules of recipient cells that aredistinct from those of donor cells. In one instance, aminor histocompatibility antigen was encoded by a
sufficiently to allow allogeneic stem- and immune-cellengraftment12. Clinical trials are now using non-mye-loablative regimens consisting of fludarabine and low-dose chemotherapy or total-body irradiation (BOX 1b).These usually achieve donor-cell engraftment with adecrease in both organ toxicity — PANCYTOPAENIA — andearly mortality, compared with myeloablative regi-mens13–16. Non-myeloablative conditioning makes itpossible to perform bone-marrow transplantation safelyin older patients and those with compromised organfunction, but provides minimal direct antitumour activ-ity. The lack of significant antitumour activity of theseconditioning regimens means that tumour eradicationrelies almost exclusively on the GVL effect that is medi-ated by donor immune cells. Antitumour activity is seenafter non-myeloablative stem-cell transplantation inmany patients, including those with CML, chronic lym-phoblastic leukaemia (CLL), acute leukaemia, multiplemyeloma, lymphoma and renal-cell carcinoma. A sig-nificant fraction of these patients, however, fail torespond or undergo relapse after an initial response13–17.Additionally, GVHD occurs in approximately 50% ofthese patients and contributes to morbidity and mortal-ity13–18. These results demonstrate that the GVL effectcan sometimes replace intensive chemoradiotherapy,but highlight the need for a clearer understanding of theimmunological mechanisms and target molecules thatare required for elimination of malignant cells. Oncethese are understood, strategies to augment the GVLeffect without GVHD can be developed.
Immune cells that are implicated in the GVL effectinclude CD8+ and CD4+ T cells, and natural killer (NK)cells. Donor NK cells mediate a potent GVL effectagainst acute myelogenous leukaemia (AML) after
Summary
• Allogeneic stem-cell transplantation, in which donor immune cells transplanted withbone-marrow stem cells recognize and eliminate leukaemia, is now recognized as animmunological modality for cancer therapy.
• New approaches to transplantation take advantage of the allogeneic graft-versus-leukaemia (GVL) effect and facilitate the eradication of malignancies with low andminimally toxic doses of chemotherapy.
• In human leukocyte antigen (HLA)-matched transplant recipients, T-cell responses tominor histocompatibility antigens are responsible for antileukaemic activity, but alsocause graft-versus-host disease (GVHD). The discovery of the polymorphic genes thatencode minor histocompability antigens is now proceeding rapidly and has identified asubset of these antigens that can be targeted for selective destruction of leukaemic cellswithout GVHD.
• Non-polymorphic self-proteins are often overexpressed in leukaemic cells as aconsequence of molecular dysregulation. Many of these proteins are expressed at lowlevels on a limited subset of normal cells, and T cells of sufficient avidity todistinguish malignant cells from normal cells can be identified and might alsocontribute to GVL activity.
• The development of effective methods for isolating and propagating antigen-specific T cells indicates that adoptive T-cell therapy using T cells that are selected forrecognition of leukaemic cells will be a useful adjunct to stem-cell transplantation fortreating or preventing leukaemic relapse.
• Approaches to regulate the fate and migration of adoptively transferred T cells are beingdeveloped and promise to improve the safety and efficacy of T-cell therapy for leukaemia.

NATURE REVIEWS | CANCER VOLUME 4 | MAY 2004 | 373
R E V I E W S
of polymorphism with their X-chromosome homo-logues and are responsible for immunological reactionsin transplants between males and females.
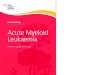
It has been proposed that differential tissue expres-sion of genes that encode individual minor histocom-patibility antigens might serve as a basis for segregatingthe GVL effect from GVHD. T cells that recognizeminor histocompatibility antigens that are onlyexpressed by recipient haematopoietic cells, includingleukaemic cells, could contribute to the elimination ofleukaemia without GVHD. Alternatively, T cells thatrecognize antigens that are expressed by haematopoieticcells as well as epithelium might contribute to both theGVL effect and GVHD (FIG. 1). Studies in a mousemodel of GVHD indicate this paradigm could be overlysimplistic, and that the phenotype and cytokine profileof alloreactive T cells might also determine epithelialinjury. In BONE-MARROW CHIMAERA mice that expressed adisparate major histocompatibility complex (MHC)class I or II molecule only on haematopoietic antigen-presenting cells and not on epithelial cells, transplanta-tion of CD4+ T cells and, to a lesser extent, CD8+ T cellsinduced GVHD that was mediated by the cytokinestumour-necrosis factor and interleukin (IL)-1 (REF. 42).Whether this mechanism operates in GVHD caused byminor-histocompatibility-antigen-specific T cells afterhuman HLA-matched stem-cell transplantationrequires additional study.
Minor histocompatibility antigens selectively expressedin haematopoietic cells. Several human minor histo-compatibility antigens, such as HA-1, HA-2, HB-1 andBCL2A1, are only expressed by haematopoietic cells(TABLE 1) and are being investigated as potential targetsfor a GVL effect25–28,31,32,34. There are conflicting dataconcerning a role for HA-1 in GVHD43–45, but evidenceis accumulating that both HA-1 and HA-2, which arepresented by HLA-A2, are targets for a GVL effect afterallogeneic stem-cell transplantation. One study foundthat recipients who expressed HA-1 and had an HA-1-negative donor had a lower incidence of leukaemicrelapse than HA-1-compatible pairs46. Additional evi-dence has come from analysis of patients who receiveddonor-lymphocyte infusion to treat post-transplanta-tion relapse47,48. An expansion of CD8+ T cells specificfor HA-1 and/or HA-2 was identified in the blood afterdonor-lymphocyte infusion and this coincided withremission of the malignancy. These T cells were isolatedand shown to lyse recipient leukaemic cells and toinhibit leukaemic-cell colony formation in vitro47.
BCL2A1 is a member of the BCL2 family of anti-apoptotic genes that is frequently highly expressed inhaematological malignances and encodes two minorhistocompatibility antigens49. These result from dis-tinct nucleotide polymorphisms in the BCL2A1 geneand are presented by HLA-A*2402 and HLA-B*4403,respectively34. BCL2A1-specific T cells were isolatedfrom transplant recipients and were shown to lyse pri-mary leukaemic cells in vitro34. No increase was seen inthe incidence of GVHD in recipients who carried anantigenic BCL2A1 allele but had an BCL2A1-negative
member of a multigene family that was expressed inrecipient cells, but not donor cells, because of homozy-gous deletion of the gene in the donor33. Severalhuman minor histocompatibility antigens are encodedby Y-chromosome genes, which show significant levels
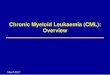
Box 1 | Myeloablative and non-myeloablative stem-cell transplant
Myeloablative allogeneic haematopoietic stem-cell transplantation (panel a indiagram) involves administration of intensive chemotherapy (ovals), often combinedwith total body irradiation (lightning bolts), before the cells are transplanted (day 0).Allogeneic haematopoietic stem cells are typically obtained from bone marrow orfrom the peripheral blood after growth-factor administration. The intensivechemoradiotherapy provides significant antitumour activity, but decreases hosthaematopoiesis and immunity. Engraftment of donor stem cells (allogeneichaematopoietic stem-cell infusion) is essential to rescue the patient from lethalhaematopoietic toxicity. Immunosuppressive drugs, such as cyclosporine andmethotrexate, are administered post-transplantation to prevent graft-versus-hostdisease (GVHD). The main complications of stem-cell transplantation following thismyeloablative regimen are organ damage, due to the intensive cytotoxic therapy,opportunistic infection during the period of profound neutropaenia, and GVHD.The intensive chemoradiotherapy and the graft-versus-leukaemia (GVL) effect ofdonor immune cells both contribute to the eradication of the leukaemia.
During non-myeloablative conditioning (panel b in diagram), fludarabine combinedwith reduced-intensity chemotherapy or low-dose total-body irradiation, areadministered to the patient before the haematopoietic stem cells are transplanted. Thisless intensive conditioning is not myeloablative, but is sufficiently immunosuppressiveto allow engraftment of donor stem cells. Immunosuppressive drugs such ascyclosporine and mycophenolate mofetil are administered both to prevent rejection ofthe transplanted donor cells and to prevent GVHD. The main complications of stem-cell transplantation following this non-myeloablative regimen are GVHD andopportunistic infections that occur as a consequence of immunosuppressive therapy.The GVL effect that is mediated by donor immune cells is solely responsible for theeradication of the leukaemia.
–7 –6 –5 –4 –3 –2 –1 0 +14 +28 +100 +180
–4 –3 –2 –1 0 +14 +28 +100 +180
Pancytopaenia, infection, organ toxicity
GVHD, infection
Allogeneic haematopoietic-stem-cell infusion
Immunosuppression
Mild pancytopaenia
GVHD, infection
Allogeneic haematopoietic-stem-cell infusion
Immunosuppression
a Myeloablative allogeneic haematopoietic-stem-cell transplantation
b Non-myeloablative allogenic haematopoietic-stem-cell transplantation

374 | MAY 2004 | VOLUME 4 www.nature.com/reviews/cancer
R E V I E W S
levels in only a few normal tissues, including testis, thy-mus and hyperplastic tonsils31,32,50. T cells that are specificfor a minor histocompatibility antigen encoded by HB-1and presented by HLA-B*4402 or HLA-B*4403 havebeen isolated after allogeneic stem-cell transplantationand have been found to lyse ALL blast cells. T cells that arespecific for HB-1 might be useful in treating ALL, whichis typically the most resistant leukaemia to a GVL effect31.
The identification of haematopoietic-restrictedminor histocompatibility antigens such as HA-1, HA-2,HB-1 and BCL2A1 is crucial for combining targetedimmunotherapy with allogeneic stem-cell transplan-tation. The subset of patients who undergo allogeneicstem-cell transplantation and are appropriately discordant with their donors for these known minorhistocompatibility antigens could benefit from inter-vention to augment T-cell responses. However, it willbe essential to molecularly characterize additionalminor histocompatibility antigens that are expressedin haematopoietic cells to broadly apply targetedimmunotherapy. Ideal minor histocompatibility anti-gens would be derived from proteins that are not onlyselectively expressed on haematopoietic cells, includ-ing leukaemia cells, but are also necessary for cellfunction. This should minimize the potential forleukaemia cells to evade T-cell recognition by losingexpression of the antigen. One approach that mighthasten the discovery of targetable minor histocompat-ibility antigens is to use array analysis to identify genesthat are selectively expressed by haematopoietic andleukaemic stem cells. This subset of genes would thenbe further characterized to detect nucleotide poly-morphisms that encode non-synonymous amino-acidsubstitutions51. Bioinformatic techniques could thenbe used to predict which polymorphic peptides are
donor, indicating that BCL2A1 might be a useful targetfor segregating the GVL effect from GVHD34.
The HB-1 gene is a polymorphic gene of unknownfunction that is highly expressed in B-cell malignancies,including ALL and lymphoma, but is expressed at low
BONE-MARROW CHIMAERA
These occur after allogeneichaematopoietic-stem-celltransplantation. In chimaeras,the bone marrow andhaematopoietic cells are derivedfrom the donor (one genotype),whereas the remaining cells inthe body are all derived from thehost (a second genotype).
Box 3 | Methods for identifying minor histocompatibility antigen genes
High-performance liquid chromatography (HPLC) and mass spectrometryPeptides are eluted from class I molecules and fractionated by microcapillary HPLC to identify fractions that contain theepitope recognized by cytotoxic T lymphocytes (CTLs). These fractions are analysed by tandem mass spectrometry toidentify the single peptide sequence. Databases are then searched to identify a candidate gene that contains a codingsequence corresponding to the identified peptide.
cDNA expression cloningA cDNA library is prepared from RNA from antigen-positive cells. These cDNAs are cloned into an expression vectorand co-transfected with a plasmid encoding the human leukocyte antigen (HLA)-restricting allele into COS cells. Thetransfected cells are then screened by co-culture with T cells that are specific for minor histocompatibility antigen toidentify those that stimulate T-cell cytokine production. Positive cells are subcloned to identify those that expresses thecDNA encoding the antigenic epitope. The antigenic epitope is then localized by transfecting truncated deletions of thegene into COS cells or by prediction algorithms for HLA–peptide binding.
Genetic-linkage analysisGenetic-linkage analysis uses cell lines from large pedigrees, such as the Centre d’Etude Polymorphism Humain referencefamilies, that have been mapped for polymorphic genetic markers. Cell lines are transfected with cDNA encoding therelevant class I HLA-restricting allele and evaluated for recognition by minor-histocompatibility-antigen-specific CTLs.Pairwise linkage analysis is used to identify the chromosomal region that regulates the expression of the minorhistocompatibility antigen. The draft sequence of the human genome has improved the use of this method for identifyingcandidate genes.
Polymorphic-peptide screeningPolymorphic sequences of candidate proteins are screened using prediction algorithms for HLA–peptide binding.Candidate peptides are then pulsed onto antigen-presenting cells to assess T-cell recognition.
Box 2 | Mechanisms for generating minor histocompatibility antigens
Minor histocompatibility antigens arise as a consequence of the normal cellularmechanisms for processing and presenting foreign antigens to T cells. Peptides that resultfrom the proteolytic degradation of endogenous proteins are transported by the peptidetransporter into the endoplasmic reticulum (ER), where they can bind to humanleukocyte antigen (HLA) molecules, and pass through the Golgi apparatus so that theycan be presented at the cell surface as a complex with HLA. In the setting of allogeneicstem-cell transplantation, polymorphisms in the recipient genome can result in theexpression of proteins and peptides that are distinct from those in the donor cells, and thedisplay of peptides that can therefore be recognized as foreign by donor T cells. Minorhistocompatibility antigens are generated by nucleotide polymorphisms in the codingsequences of genes that lead to differences in the amino-acid sequences of homologousproteins between donor and recipient cells. This can result in altered proteosomalcleavage, peptide transport, HLA binding, or T-cell receptor (TCR) contact, causingdonor T cells to recognize these antigens as foreign.
Nucleotidepolymorphism
Peptide transport
HLA binding TCR contact
Proteosomal cleavage
ERGolgi T cell

NATURE REVIEWS | CANCER VOLUME 4 | MAY 2004 | 375
R E V I E W S
in vitro studies showing that SMCY-specific CD8+
T cells incubated with male skin caused a histologicalinjury that was consistent with severe GVHD54.
T-cell responses to minor histocompatibility antigensthat are expressed at lower levels on epithelia could beassociated with a lesser degree of GVHD, so targetingsuch antigens to induce a GVL effect might be accom-plished safely. For example, CD8+ CTLs that are specificfor a minor histocompatibility antigen encoded by the Y-chromosome gene UTY were isolated from an allo-geneic-stem-cell-transplant recipient without GVHD39.UTY transcripts are present at low levels in most non-haematopoietic tissues, but UTY-specific CTLs fail to lyseskin fibroblasts or stromal cells in vitro. This indicates thatthe level of UTY expression in non-haematopoietic cellscould be insufficient to induce GVHD39. However, UTYis highly expressed by leukaemia cells, and UTY-specificCTLs eliminate leukaemia in NOD/SCID mice24,39.Moreover, there is a substantial level of polymorphismbetween UTY and its X-chromosome homologue, andepitopes that are presented by other HLA alleles havebeen defined. So, UTY might serve as a general target inmale recipients of stem-cell transplants who have femaledonors. Of interest, male recipients who receive stem-cell transplants from female donors have a decreasedrisk of leukaemic relapse, compared with otherdonor–recipient gender combinations — even aftercontrolling for the presence of GVHD. This finding isconsistent with a contribution of Y-chromosome-encoded minor histocompatibility antigens to a selectiveGVL effect55. As additional minor histocompatibilityantigens are discovered, it will be important to examinewhether the level of expression in non-haematopoietictissues is a determining factor in the risk of GVHD.
likely to be generated by proteosomal processing andbind to common HLA molecules, and the candidatepeptides evaluated for immunogenicity52.
Minor histocompatibility antigens with broad tissueexpression. It might not be possible to usehaematopoietic specific minor histocompatibility anti-gens as targets for therapy in all recipients of stem-celltransplants. Enhancing the GVL effect by targetingminor histocompatibility antigens that are expressedon both leukaemic cells and epithelial cells could stillbe beneficial, but might be associated with some levelof GVHD. Preliminary data indicate that the level ofexpression of the minor histocompatibility antigen onepithelial cells might determine the risk of GVHD. Forexample, T-cell responses to the HA-8, UGT2B17 andSMCY minor histocompatibility antigens, which areall very highly expressed on epithelial cells, have beenassociated with GVHD. Recipients who were positivefor the ubiquitously expressed HA-8 minor histocom-patibility antigen and received a transplant from an HA-8-negative donor developed acute GVHDmore frequently than recipients of transplants fromHA-8-compatible donors53. T cells specific for theUGT2B17 minor histocompatibility antigen, which isabundantly expressed in the gastrointestinal tract andliver, were isolated from a patient with protracted liverand intestinal GVHD33. Larger numbers of T cells thatwere specific for minor histocompatibility antigensencoded by SMCY — a Y-chromosome gene that ishighly expressed in epithelia — were detected in maleswith GVHD who received stem-cell transplants fromfemale donors, compared with males that did notdevelop GVHD44. This finding is consistent with
Table 1 | Human minor histocompatibility antigens
Minor HLA Gene/chromosome Peptide Tissue Identification technique Referenceshistocompatibility restriction sequence distributionantigen
HA-1 HLA A201 KIAA0223/19p13 VLHDDLLEA Haematopoietic HPLC with mass spectometry 25
HA-1 HLA B60 KIAA0223/19p13 KECVLHDDL Haematopoietic Polymorphic-peptide screening 26
HA-2 HLA A201 MYOG1/7 YIGEVLSV Haematopoietic HPLC with mass spectometry 27,28
HA-3 HLA A1 LBC/15q24-25 VTEPGTAQY Ubiquitous HPLC with mass spectometry 29
HA-8 HLA A201 KIAA0020/9 RTLDKVLEV Ubiquitous HPLC with mass spectometry 30
HB-1 HLA B44 5q32 EEKRGSLHVW Haematopoietic, cDNA-expression cloning 31,32especially B-cellleukaemias
UGT2B17 HLA 2902 UGT2B17/4q13 AELLNIPFLY Ubiquitous cDNA expression cloning 33
BCL2A1 HLA A24 BCL2A1/15q24.3 DYLQYVKQI Haematopoietic Genetic-linkage analysis 34
BCL2A1 HLA B4403 BCL2A1/15q24.3 KEFEDDIINW Haematopoietic Genetic-linkage analysis 34
HY B7 HLA B702 SMCY SPSVDKARAEL Ubiquitous HPLC with mass spectometry 35
HY A2 HLA A201 SMCY FIDSYICQV Ubiquitous HPLC with mass spectometry 36
HY A1 HLA A101 DFFRY IVDCLTEMY Ubiquitous HPLC with mass spectometry 37
HY B60 HLA B60 UTY RESEESVSL Ubiquitous cDNA-expression cloning 38
HY B8 HLA B8 UTY LPHNHTDL Ubiquitous cDNA-expression cloning 39
HY DQ5 HLA DQ5 DBY HIENFSDIDMGE Ubiquitous cDNA-expression cloning 40
HY DRB3 HLA DRB3 RPS4Y VIKVNDTVQI Not reported cDNA-expression cloning 41
HLA, human leukocyte antigen; HPLC, high-performance liquid chromatography.

376 | MAY 2004 | VOLUME 4 www.nature.com/reviews/cancer
R E V I E W S
protein-expression profiles of leukaemic cells willidentify additional candidates in this category. At pre-sent, WT1 and proteinase 3 represent the antigens inthis class that are closest to being used clinically.
WT1 is a zinc-finger transcription factor that is cru-cial for urogenital development62. WT1 is highlyexpressed in most leukaemias and might contribute toleukaemogenesis by blocking differentiation. However,it is also expressed at low levels in some normal tissues,including CD34+ haematopoieitic progenitors, renalpodocytes, Sertoli cells of the testis and granulosa cellsof the ovary63. T cells that can recognize WT1 are pre-sent at low frequency in normal donors and there is littleevidence for the endogenous generation of WT1-specific T cells after allogeneic stem-cell transplantation64.WT1-specific T cells, however, can be expanded fromnormal donors in vitro by stimulation with dendritic cellsthat have been pulsed with synthetic WT1 peptidesselected by prediction algorithms for HLA–peptide binding56,65,66. Such WT1-specific T cells lyse humanleukaemic cells in vitro, inhibit leukaemia colony forma-tion and impair engraftment of human leukaemic cells inNOD/SCID mice67 , but do not recognize normal CD34+
CELLS. These findings show that WT1-specific T cellsmight distinguish malignant from normal cells, based onthe level of WT1 expression.
Proteinase 3 is a primary-granule serine protease thatis a target of autoantibodies in patients who haveWEGENER’S GRANULOMATOSIS68. Proteinase 3 is predominantly
Leukaemia-associated proteins The lower incidence of leukaemia relapse after allo-geneic stem-cell transplantation compared with syn-geneic transplantation appropriately focused attentionon T-cell responses to minor histocompatibility anti-gens as mediators of GVL activity. However, other typesof protein expressed by leukaemic cells have emerged asprospective targets for a GVL effect, including non-polymorphic proteins that are overexpressed or aber-rantly expressed in leukaemic cells as a consequence ofmolecular dysregulation. In many cases, these proteinsalso seem to contribute to the malignant phenotype andare absent or expressed at low levels on normal cells,making them attractive for targeted immunotherapy.
Proteins that are overexpressed by leukaemic cells.Non-polymorphic proteins, such as Wilms’ tumour 1(WT1), proteinase 3, survivin, telomerase reversetranscriptase, CYPB1 and immature laminin recep-tor, are expressed by leukaemic cells at much higherlevels than by normal cells, and are being investigatedas targets for T cells56–61. The expression of these pro-teins on some normal tissues could restrict the reper-toire of reactive T cells that are present in vivobecause of SELF-TOLERANCE mechanisms. However, byoptimizing T-cell culture conditions, it has been pos-sible to isolate rare T cells from normal donors withsufficient avidity for self-antigens to recognizeleukaemic cells. It is likely that analysis of gene- and
SELF-TOLERANCE
The normal lack of animmunological response toautologous or self-antigens. Abreakdown of self-tolerance canresult in autoimmunity.
CD34+ CELLS
The CD34+ glycoprotein is a cell-surface marker of earlyhaematopoietic progenitor cells.
WEGENER’S GRANULOMATOSIS
A rare disorder that ischaracterized by chronicinflammation of blood vesselsand granulomas in the nasalpassages, lungs and kidneys. Thisdisorder is associated withantibodies directed against theproteinase enzyme ofneutrophils.
Skin Stomach,intestines
Liver Fibroblasts
Epithelial tissues
Neutrophil Antigen-presentingcell
Macrophage T cell
Haematopoietic system Leukaemia
T cell responding tobroadly expressed minor histocompatibilityantigen
T cell responding to haematopoietic-restricted minor histocompatibilityantigen
GVHD GVL
Figure 1 | Separating the graft-versus-leukaemia effect from graft-versus-host disease. Donor T cells that arespecific for minor histocompatibility antigens that are broadly expressed by both haematopoietic and epithelial cells of therecipient are believed to cause graft-versus-host disease (GVHD). These T cells could also contribute to the graft-versus-leukaemia (GVL) effect if leukaemic cells express the minor histocompatibility antigens that are recognized by the T cells.Donor T cells that are specific for minor histocompatibility antigens that are selectively expressed by haematopoietic cellscould induce a GVL response without GVHD.

NATURE REVIEWS | CANCER VOLUME 4 | MAY 2004 | 377
R E V I E W S
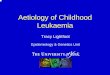
Adoptive T-cell therapyOnce minor histocompatibility antigens and leukaemia-associated antigens are discovered, the challenge will beto use this information to augment the GVL effect afterallogeneic stem-cell transplantation. One approach is touse adoptive T-cell therapy, in which donor T cells thatare specific for antigens expressed by leukaemic cells areisolated and expanded in vitro, and then infused into thetransplant recipient to establish a potent immuneresponse against the cancer (FIG. 2). The adoptive transferof donor T cells that specifically recognize viral antigenshas been effective in preventing cytomegalovirus (CMV)and Epstein–Barr virus (EBV) disease after allogeneicstem-cell transplantation, without causing GVHD75–77,and autologous tumour-reactive T cells have been trans-ferred to successfully treat patients with melanoma78,79.There are advantages and disadvantages of targeting eachof the distinct classes of leukaemia antigens, and pilotclinical trials will be needed to identify the most effectivetargets for therapy (TABLE 2). Furthermore, to use thisapproach in the clinic, it is necessary to optimize strate-gies for isolating and expanding donor T cells that arespecific for relevant antigens, to define the conditionsthat promote efficient cell persistence and migration tothe tumour, and to ensure that transferred T cells do notcause toxicity to normal tissues.
expressed in normal promyelocytes, but is aberrantlyexpressed in CML cells and some subsets of AML69. CD8+
T cells specific for an HLA-A2-binding peptide (PR-1)from proteinase 3 have been isolated from normal donorsand lyse CML and AML cells in vitro57. T cells specific forPR-1 also inhibit leukaemic, but not normal, formationof CD34+ cell colonies in vitro70, although studies ofantileukaemic activity in NOD/SCID mice have not beenreported. Both high- and low-avidity T cells can be iso-lated from normal individuals, depending on the peptideconcentration that is used for stimulation71, and only Tcells with high avidity show antileukaemic activity72. Onlylow-avidity T cells specific for PR-1 were isolated fromuntreated patients with CML, indicating that the T-cellrepertoire might be depleted of high-avidity T cells by theexpanding tumour72.
In contrast to WT1, there is evidence that the numberof T cells that are specific for PR-1 is increased in CMLpatients who have been treated with interferon-γ (IFN-γ)or allogeneic stem-cell transplantation, and their pres-ence correlates with complete remission73. Furthermore,T cells that are specific for PR-1 are more frequentlyidentified in CML patients who are treated with IFN-γ,compared with those on imatinib, which could berelated to the upregulation of proteinase 3 expressionthat is induced by IFN-γ74.
a Isolation of T cells
Donor Recipient e Adoptive transfer
T cell
Antigen- presenting cell
b In vitro stimulation of T cells
d T-cell cloning and expansion
c Selection of leukaemia- reactive T cells
70
60
50
4030
20
10
0
Spe
cific
lysi
s (%
)
Effector to target ratio100 101 102 103 104
100
101
102
103
104
Cytokine
CD
8
CytotoxicityCapture T cells, based on cytokine profile Tetramer staining
Figure 2 | Adoptive immunotherapy with donor T cells to augment the graft-versus-leukaemia response. a | T cells areobtained from the human leukocyte antigen (HLA)-identical donor before haematopoietic stem-cell transplantation. b | Thesedonor T cells can be primed to recognize leukaemia-associated or minor histocompatibility antigens by in vitro culture usingspecialized antigen-presenting cells. Alternatively, donor T cells that are primed in vivo to antigens that are expressed by therecipient’s leukaemic cells can be isolated from the recipient’s blood using similar stimulation protocols. c | Donor T-cell lines arescreened to identify those with specific cytotoxic activity against the recipient’s leukaemic cells. T-cell clones are selected by cell-sorting techniques that capture T cells based on T-cell cytokine production in response to antigen stimulation, tetramer staining,or by limiting-dilution cloning. d | T-cell clones of the desired specificity are expanded in culture using intermittent T-cell-receptorstimulation and cytokines to promote cell growth. e | The expanded T cells are adoptively transferred into the patient aftertransplantation to augment the graft-vesus-leukaemia effect and prevent or treat cancer relapse.

378 | MAY 2004 | VOLUME 4 www.nature.com/reviews/cancer
R E V I E W S
These include prolonged culture, the application ofexcessive doses of cytokines in vitro and the absence ofa CD4+ HELPER T-CELL RESPONSE in vivo76,90. Factors that havebeen shown to promote T-cell expansion and survivalinclude the addition of cytokines such as IL-2 or IL-15,CO-STIMULATION THROUGH CD28 and transferring T cellswhen the recipient is LYMPHOPENIC and HOMEOSTATIC78,79,91.Systematic studies in animal models and clinical trialsare likely to provide further insights into ways that T-cell persistence can be improved.
T cells must not only survive in vivo, but must alsohome to sites of residual leukaemia. T-cell migration isinfluenced by the expression of adhesion moleculesand chemokine receptors, which is in part determinedby signals during T-cell priming92. The signals thatpromote T-cell homing to cancer sites need to be fur-ther characterized, but gene transfer might be used tointroduce the desired homing receptors. For therapy ofleukaemia, it is essential that transferred T cellsmigrate to the bone marrow, and this might beenhanced by expressing the chemokine receptorCXCR4, the ligand of which — SDF1 — is producedby marrow stromal cells93. However, leukaemia cellsare also present at other sites, such as the skin. So, theintroduction into a subset of leukaemia-reactive T cellsthat express CLA1 — which is naturally expressed byCD8+ T cells specific for herpes simplex virus (HSV)and orchestrates their transport to cutaneous sites ofvirus reactivation — might be effective in reducingleukaemia recurrence in the skin94.
Safety of T-cell therapy for leukaemia. The adoptivetransfer of T cells for leukaemia therapy has thepotential to cause GVHD when targeting minor histo-compatibility antigens, or to cause toxicity to normaltissues when targeting leukaemia-associated proteinsthat are also expressed by some normal cells.Moreover, if gene transfer is used to engineer T-cell-specificity or homing, this would impose the addi-tional risk of insertional oncogenesis95. A certain levelof GVHD or toxicity to normal tissues might beacceptable, providing that the therapy is effective ineliminating residual leukaemia or treating recurrence.It would be desirable, however, to be able to eliminatetransferred T cells if serious toxicity developed.
The introduction of a conditional suicide gene,such as the HSV thymidine-kinase (tk) gene — whichrenders dividing cells susceptible to ganciclovir — hasbeen effective for controlling GVHD after polyclonal-donor-lymphocyte infusion to treat relapse or EBVlymphoproliferation in recipients of stem-cell trans-plants96. However the viral tk protein is immunogenic,which often leads to the premature elimination oftransferred effector cells97. An alternative suicide gene,based on the expression of a chimeric human FASprotein that can be multimerized to activate apoptosisby administration of a synthetic non-toxic drug, hasbeen developed98. This suicide gene is effective ineliminating both proliferating and non-proliferatingcells in vitro and in vivo and, as it encodes a humanprotein, might be less immunogenic99.
Isolation and expansion of donor T cells. Donor T cellsthat are specific for the HA-1, BCL2A1, HB-1, andUTY minor histocompatibility antigens, and for cer-tain leukaemia-associated antigens such as PR-1, areamplified in some recipients of stem-cell transplants.Such T cells could be isolated post-transplantationand expanded in vitro for adoptive transfer, to mag-nify the endogenous response and potentially improvethe GVL effect. However, it would be preferable to iso-late T cells directly from the donor before transplanta-tion and administer them as part of the stem-cellgraft, or early post-transplantation when the tumourburden is low. Early therapy might be especiallyimportant after non-myeloablative stem-cell trans-plantation, because of the limited antitumour activityof the conditioning regimen.
Specialized culture conditions that involve den-dritic cells that have been pulsed with peptides ortransfected with the gene that encodes the antigen havebeen developed to isolate donor T cells that are specificfor leukaemia-associated minor histocompatibility ornon-polymorphic antigens80–82. The selection of anti-gen-specific T cells before therapy would be preferred,to avoid infusing other potential alloreactive T cellsthat might cause GVHD, and could be accomplishedthrough T-cell subcloning or by flow cytometry usingpeptide–MHC tetramers or cytokine-capturemethods83,84. Techniques are now well-established forthe isolation of human T-cell clones and individualclones can be expanded to several billion cells usingappropriate culture methods22,76,85,86. Although cultureconditions for the isolation and expansion of T cellsfor GVL therapy are available, novel strategies to generate tumour-specific T cells might prove moreefficient. One promising approach is to engineertumour-antigen-specific T cells, which express trans-genes that encode the T-cell-receptor α- and β-chainsfrom previously isolated leukaemia-reactive T-cellclones87–89. This strategy has been successful for gener-ating antigen-specific T cells that are effective in mousemodels of adoptive immunotherapy.
Cell transfer, persistence, and migration. The optimalregimen for promoting persistence of transferred T cells in humans has not yet been defined. However,studies of T-cell transfer for prevention of CMV andEBV infections in stem-cell transplant recipients, and ofautologous melanoma-specific T cells, have identifiedfactors that might interfere with T-cell persistence.
CD4+ HELPER T-CELL RESPONSE
The subset of peripheral T cellsthat express the CD4glycoprotein on the cell surfaceare called helper T cells. HelperT cells recognize peptideantigens presented on the cellsurface in association with majorhistocompatibility complex class II molecules, and secretecytokines that orchestrateresponses by other immunecells, including CD8+ T cells andB cells.
CD28 CO-STIMULATION
T cells require several signals forfull activation. Engagement ofthe T-cell receptor by human-leukocyte-antigen–peptidecomplexes provides a first signalthat is required, but notsufficient, for T-cell activation.A second signal, or co-stimulation, is provided byengagement of other molecules,including CD28, which binds toCD80 (B7.1) and CD86 (B7.2)on antigen-presenting cells.
LYMPHOPAENIC
A state of having a subnormallevel of circulating lymphocytes.
HOMEOSTATIC REGULATION
The tendency to correctabnormal levels of cells ormolecules by feedbackregulation. For example, inresponse to lymphopaenia,homeostatic mechanisms drivethe expansion of residuallymphocytes to restorelymphocyte numbers to normallevels.
Table 2 | Advantages and disadvantages of candidate antigens
Class of target Advantages Disadvantages
Minor histocompatibility T cells have high avidity for Limited to allogeneic antigens antigen; both CD8+ and CD4+ transplantation; limited
T cells recognize antigen; number of definedpotentially multivalent response antigens; potential for GVHD
Overexpressed normal Broad applicability for different T cells have low avidityproteins types of cancer for antigen; potential
for toxicity to normaltissues
GVHD, graft-versus-host disease.

NATURE REVIEWS | CANCER VOLUME 4 | MAY 2004 | 379
R E V I E W S
transfer that can be used to augment the GVL effect with-out GVHD. Ideally, the clinical applications of non-mye-loablative stem-cell transplantation and T-cell therapywill merge into a cohesive strategy that begins by engi-neering the stem-cell graft to remove subsets of donor T cells that cause GVHD100,101, and to add donor T cellsspecific for defined minor histocompatibility and/orleukaemia-associated antigens that promote a GVL effect.The need for additional infusions of leukaemia-reactive T cells could be determined by molecular monitoring todetect minimal residual disease102.
Future directionsThe outcome of allogeneic stem-cell transplantation hasimproved over the past decade, in large part because ofadvances in supportive care. However, leukaemic relapseand complications from GVHD remain importantcauses of failure. The focus in the field is increasinglyshifting towards the use of less intensive chemoradio-therapy and reliance on the GVL effect of donor T cellsfor leukaemia eradication. Further improvements inallogeneic stem-cell transplantation are likely to beachieved by defining strategies such as adoptive T-cell
1. Appelbaum, F. R. The current status of hematopoietic celltransplantation. Annu. Rev. Med. 54, 491–512 (2003).
2. Klein, J. & Sato, A. The HLA system. N. Engl. J. Med. 343,702–709 (2000).
3. Vogelsang, G. B., Lee, L. & Bensen-Kennedy, D. M.Pathogenesis and treatment of graft-versus-host diseaseafter bone marrow transplant. Annu. Rev. Med. 54, 29–52(2003).
4. Falkenburg, J. H., van de Corput, L., Marijt, E. W. &Willemze, R. Minor histocompatibility antigens in humanstem cell transplantation. Exp. Hematol. 31, 743–751(2003).
5. Barnes, D. W. H., Corp, M. J., Loutit, J. F. & Neal, F. E.Treatment of murine leukemia with x-rays and homologousbone marrow. Br. Med. J. 32, 626–627 (1956).
6. Weiden, P. L. et al. Antileukemic effect of graft-versus-hostdisease in human recipients of allogeneic-marrow grafts. N. Engl. J. Med. 300, 1068–1073 (1979).
7. Horowitz, M. M. et al. Graft-versus-leukemia reactionsafter bone marrow transplantation. Blood 75, 555–562(1990).
8. Marmont, A. M. et al. T-cell depletion of HLA-identicaltransplants in leukemia. Blood 78, 2120–2130 (1991).
9. Passweg, J. R. et al. Graft-versus-leukemia effects in T lineage and B lineage acute lymphoblastic leukemia. BoneMarrow Transplant. 21, 153–158 (1998).
10. Kolb, H. J. et al. Graft-versus-leukemia effect of donorlymphocyte transfusions in marrow grafted patients.European Group for Blood and Marrow TransplantationWorking Party Chronic Leukemia. Blood 86, 2041–2050(1995).
11. Collins, R. H. Jr et al. Donor leukocyte infusions in 140patients with relapsed malignancy after allogeneic bonemarrow transplantation. J. Clin. Oncol. 15, 433–444 (1997).
12. Storb, R. et al. Stable mixed hematopoietic chimerism inDLA-identical littermate dogs given sublethal total bodyirradiation before and pharmacologicalimmunosuppression after marrow transplantation. Blood89, 3048–3054 (1997).
13. Khouri, I. F. et al. Nonablative allogeneic hematopoietictransplantation as adoptive immunotherapy for indolentlymphoma: low incidence of toxicity, acute graft-versus-hostdisease, and treatment-related mortality. Blood 98,3595–3599 (2001).
14. Champlin, R. et al. Harnessing graft-versus-malignancy:non-myeloablative preparative regimens for allogeneichaematopoietic transplantation, an evolving strategy foradoptive immunotherapy. Br. J. Haematol. 111, 18–29(2000).
15. Maloney, D. G. et al. Allografting with nonmyeloablativeconditioning following cytoreductive autografts for thetreatment of patients with multiple myeloma. Blood 102,3447–3454 (2003).
16. Maris, M. B. et al. HLA-matched unrelated donorhematopoietic cell transplantation after nonmyeloablativeconditioning for patients with hematologic malignancies.Blood 102, 2021–2030 (2003).
17. Childs, R. et al. Regression of metastatic renal-cellcarcinoma after nonmyeloablative allogeneic peripheral-blood stem-cell transplantation. N. Engl. J. Med. 343,750–758 (2000).
18. Mielcarek, M. et al. Graft-versus-host disease afternonmyeloablative versus conventional hematopoietic stemcell transplantation. Blood 102, 756–762 (2003).
19. Ruggeri, L. et al. Effectiveness of donor natural killer cellalloreactivity in mismatched hematopoietic transplants.Science 295, 2097–2100 (2002).
20. Parham, P. & McQueen, K. L. Alloreactive killer cells:hindrance and help for haematopoietic transplants. NatureRev. Immunol. 3, 108–122 (2003).
21. Fontaine, P. et al. Adoptive transfer of minorhistocompatibility antigen-specific T lymphocytes eradicatesleukemia cells without causing graft-versus-host disease.Nature Med. 7, 789–794 (2001).Shows that it is possible in a murine transplant modelto eradicate leukaemia by the adoptive transfer ofCD8+ T cells specific for a single minorhistocompatibility antigen.
22. Warren, E. H., Greenberg, P. D. & Riddell, S. R. Cytotoxic T-lymphocyte-defined human minor histocompatibilityantigens with a restricted tissue distribution. Blood 91,2197–2207 (1998).
23. Falkenburg, J. H. et al. Growth inhibition of clonogenic leukemicprecursor cells by minor histocompatibility antigen-specificcytotoxic T lymphocytes. J. Exp. Med. 174, 27–33 (1991).
24. Bonnet, D., Warren, E. H., Greenberg, P. D., Dick, J. E. &Riddell, S. R. CD8+ minor histocompatibility antigen-specificcytotoxic T lymphocyte clones eliminate human acutemyeloid leukemia stem cells. Proc. Natl Acad. Sci. USA 96,8639–8644 (1999).A minor subset of human leukaemia cells exhibitstem-cell properties and can establish leukaemichaematopoiesis in immunodeficient mice. This studyshows that leukaemic stem cells express minorhistocompatibility antigens and can be eradicated byCD8+ cytotoxic T cells.
25. den Haan, J. M. et al. The minor histocompatibility antigenHA-1: a diallelic gene with a single amino acidpolymorphism. Science 279, 1054–1057 (1998).
26. Mommaas, B. et al. Identification of a novel HLA-B60-restricted T cell epitope of the minor histocompatibilityantigen HA-1 locus. J. Immunol. 169, 3131–3136 (2002).
27. den Haan, J. M. et al. Identification of a graft versus hostdisease-associated human minor histocompatibility antigen.Science 268, 1476–1480 (1995).Describes the use of peptide elution, high-performance liquid chromatographic fractionation andmass spectrometry to identify the molecular structureof the first human minor histocompatibility antigen.
28. Pierce, R. A. et al. The HA-2 minor histocompatibility antigenis derived from a diallelic gene encoding a novel humanclass I myosin protein. J. Immunol. 167, 3223–3230 (2001).
29. Spierings, E. et al. The minor histocompatibility antigen HA-3 arises from differential proteasome-mediated cleavageof the lymphoid blast crisis (Lbc) oncoprotein. Blood 102,621–629 (2003).
30. Brickner, A. G. et al. The immunogenicity of a new humanminor histocompatibility antigen results from differentialantigen processing. J. Exp. Med. 193, 195–206 (2001).
31. Dolstra, H. et al. Recognition of a B cell leukemia-associatedminor histocompatibility antigen by CTL. J. Immunol. 158,560–565 (1997).
32. Dolstra, H. et al. A human minor histocompatibility antigenspecific for B cell acute lymphoblastic leukemia. J. Exp.Med. 189, 301–308 (1999).
33. Murata, M., Warren, E. H. & Riddell, S. R. A human minorhistocompatibility antigen resulting from differentialexpression due to a gene deletion. J. Exp. Med. 197,1279–1289 (2003).
34. Akatsuka, Y. et al. Identification of a polymorphic gene,BCL2A1, encoding two novel hematopoietic lineage-specific minor histocompatibility antigens. J. Exp. Med. 197,1489–1500 (2003).
35. Wang, W. et al. Human H-Y: a male-specifichistocompatibility antigen derived from the SMCY protein.Science 269, 1588–1590 (1995).
36. Meadows, L. et al. The HLA-A*0201-restricted H-Y antigencontains a posttranslationally modified cysteine thatsignificantly affects T cell recognition. Immunity 6, 273–281(1997).
37. Pierce, R. A. et al. Cutting edge: the HLA-A*0101-restrictedHY minor histocompatibility antigen originates from DFFRYand contains a cysteinylated cysteine residue as identifiedby a novel mass spectrometric technique. J. Immunol. 163,6360–6364 (1999).
38. Vogt, M. H. et al. UTY gene codes for an HLA-B60-restricted human male-specific minor histocompatibilityantigen involved in stem cell graft rejection: characterizationof the critical polymorphic amino acid residues for T-cellrecognition. Blood 96, 3126–3132 (2000).
39. Warren, E. H. et al. The human UTY gene encodes a novelHLA-B8-restricted H-Y antigen. J. Immunol. 164,2807–2814 (2000).
40. Vogt, M. H. et al. The DBY gene codes for an HLA-DQ5-restricted human male-specific minor histocompatibilityantigen involved in graft-versus-host disease. Blood 99,3027–3032 (2002).
41. Spierings, E. et al. Identification of HLA class II-restricted H-Y-specific T-helper epitope evoking CD4+ T-helper cells inH-Y-mismatched transplantation. Lancet 362, 610–615(2003).
42. Teshima, T. et al. Acute graft-versus-host disease does notrequire alloantigen expression on host epithelium. NatureMed. 8, 575–581 (2002).
43. Goulmy, E. et al. Mismatches of minor histocompatibilityantigens between HLA-identical donors and recipients and thedevelopment of graft-versus-host disease after bone marrowtransplantation. N. Engl. J. Med. 334, 281–285 (1996).
44. Mutis, T. et al. Tetrameric HLA class I-minorhistocompatibility antigen peptide complexes demonstrateminor histocompatibility antigen-specific cytotoxic Tlymphocytes in patients with graft-versus-host disease.Nature Med. 5, 839–842 (1999).
45. Lin, M. T. et al. Absence of statistically significant correlationbetween disparity for the minor histocompatibility antigen-HA-1 and outcome after allogeneic hematopoietic celltransplantation. Blood 98, 3172–3173 (2001).
46. Murata, M. et al. No significant association between HA-1incompatibility and incidence of acute graft-versus-hostdisease after HLA-identical sibling bone marrowtransplantation in Japanese patients. Int. J. Hematol. 72,371–375 (2000).
47. Marijt, W. A. et al. Hematopoiesis-restricted minorhistocompatibility antigens HA-1- or HA-2-specific T cellscan induce complete remissions of relapsed leukemia. Proc.Natl Acad. Sci. USA 100, 2742–2747 (2003).Regression of leukaemia after donor-lymphocyteinfusion correlated temporarily with large in vivoexpansion of CD8+ cytotoxic T cells specific for HA-1and HA-2.
48. Kircher, B. et al. Induction of HA-1-specific cytotoxic T-cellclones parallels the therapeutic effect of donor lymphocyteinfusion. Br. J. Haematol. 117, 935–939 (2002).
49. Nagy, B. et al. Abnormal expression of apoptosis-relatedgenes in haematological malignancies: overexpression ofMYC is poor prognostic sign in mantle cell lymphoma. Br. J.Haematol. 120, 434–441 (2003).
50. Dolstra, H. et al. Bi-directional allelic recognition of thehuman minor histocompatibility antigen HB-1 by cytotoxic T lymphocytes. Eur J. Immunol. 32, 2748–2758 (2002).
51. Phillips, R. L. et al. The genetic program of hematopoieticstem cells. Science 288, 1635–1640 (2000).
52. Nielsen, M. et al. Reliable prediction of T-cell epitopes usingneural networks with novel sequence representations.Protein Sci. 12, 1007–1017 (2003).
53. Akatsuka, Y. et al. Disparity for a newly identified minorhistocompatibility antigen, HA-8, correlates with acute graft-versus-host disease after haematopoietic stem celltransplantation from an HLA-identical sibling. Br. J.Haematol. 123, 671–675 (2003).

380 | MAY 2004 | VOLUME 4 www.nature.com/reviews/cancer
R E V I E W S
54. Dickinson, A. M. et al. In situ dissection of the graft-versus-host activities of cytotoxic T cells specific for minorhistocompatibility antigens. Nature Med. 8, 410–414(2002).
55. Randolph, S. S., Gooley, T. A., Warren, E. H., Appelbaum, F.R. & Riddell, S. R. Female donors contribute to a selectivegraft versus leukemia effect in male recipients of HLAmatched related hematopoietic cell transplants. Blood 103,347–352 (2004).
56. Gao, L. et al. Selective elimination of leukemic CD34+
progenitor cells by cytotoxic T lymphocytes specific forWT1. Blood 95, 2198–2203 (2000).
57. Molldrem, J. et al. Targeted T-cell therapy for humanleukemia: cytotoxic T lymphocytes specific for a peptidederived from proteinase 3 preferentially lyse humanmyeloid leukemia cells. Blood 88, 2450–2457(1996).
58. Andersen, M. H. et al. Spontaneous cytotoxic T-cellresponses against survivin-derived MHC class I-restricted T-cell epitopes in situ as well as ex vivo in cancer patients.Cancer Res. 61, 5964–5968 (2001).
59. Arai, J. et al. Identification of human telomerase reversetranscriptase-derived peptides that induce HLA-A24-restricted antileukemia cytotoxic T lymphocytes. Blood 97,2903–2907 (2001).
60. Maecker, B. et al. The shared tumor-associated antigencytochrome P450 1B1 is recognized by specific cytotoxic T cells. Blood 102, 3287–3294 (2003).
61. Siegel, S. et al. Induction of cytotoxic T-cell responsesagainst the oncofetal antigen-immature laminin receptor forthe treatment of hematologic malignancies. Blood 102,4416–4423 (2003).
62. Scharnhorst, V., van der Eb, A. J. & Jochemsen, A. G. WT1 proteins: functions in growth and differentiation. Gene273, 141–161 (2001).
63. Inoue, K. et al. Aberrant overexpression of the Wilms tumorgene (WT1) in human leukemia. Blood 89, 1405–1412(1997).
64. Rezvani, K. et al. Functional leukemia-associated antigen-specific memory CD8+ T cells exist in healthy individuals andin patients with chronic myelogenous leukemia before andafter stem cell transplantation. Blood 102, 2892–2900(2003).
65. Ohminami, H., Yasukawa, M. & Fujita, S. HLA class I-restricted lysis of leukemia cells by a CD8+ cytotoxicT-lymphocyte clone specific for WT1 peptide. Blood 95,286–293 (2000).
66. Azuma, T. et al. Identification of a novel WT1-derived peptidewhich induces human leucocyte antigen-A24-restrictedanti-leukaemia cytotoxic T lymphocytes. Br. J. Haematol.116, 601–603 (2002).
67. Gao, L. et al. Human cytotoxic T lymphocytes specific forWilms’ tumor antigen-1 inhibit engraftment of leukemia-initiating stem cells in non-obese diabetic-severe combinedimmunodeficient recipients. Transplantation 75, 1429–1436(2003).
68. Williams, R. C. Jr et al. Epitopes on proteinase-3 recognizedby antibodies from patients with Wegener’s granulomatosis.J. Immunol. 152, 4722–4737 (1994).
69. Dengler, R. et al. Immunocytochemical and flow cytometricdetection of proteinase 3 (myeloblastin) in normal andleukaemic myeloid cells. Br. J. Haematol. 89, 250–257(1995).
70. Molldrem, J. J. et al. Cytotoxic T lymphocytes specific for anonpolymorphic proteinase 3 peptide preferentially inhibitchronic myeloid leukemia colony-forming units. Blood 90,2529–2534 (1997).
71. Molldrem, J. J., Lee, P. P., Wang, C., Champlin, R. E. &Davis, M. M. A PR1-human leukocyte antigen-A2 tetramercan be used to isolate low-frequency cytotoxic Tlymphocytes from healthy donors that selectively lysechronic myelogenous leukemia. Cancer Res. 59,2675–2681 (1999).
72. Molldrem, J. J. et al. Chronic myelogenous leukemiashapes host immunity by selective deletion of high-avidityleukemia-specific T cells. J. Clin. Invest. 111, 639–647(2003).
73. Molldrem, J. J. et al. Evidence that specific T lymphocytesmay participate in the elimination of chronic myelogenousleukemia. Nature Med. 6, 1018–1023 (2000).MHC-class-I–peptide tetramers were used to showthat CD8+ T cells specific for proteinase 3 — a proteinexpressed in normal myeloid differentiation andoverexpressed in chronic myeloid leukaemia — areexpanded in patients with leukaemia that respond tointerferon-α therapy or allogeneic stem-celltransplantation.
74. Burchert, A. et al. Interferon-α, but not the ABL-kinaseinhibitor imatinib (STI571), induces expression of myeloblastin and a specific T-cell response in chronic myeloid leukemia. Blood 101, 259–264 (2003).
75. Riddell, S. R. et al. Restoration of viral immunity inimmunodeficient humans by the adoptive transfer of T cellclones. Science 257, 238–241 (1992).
76. Walter, E. A. et al. Reconstitution of cellular immunity againstcytomegalovirus in recipients of allogeneic bone marrow bytransfer of T-cell clones from the donor. N. Engl. J. Med.333, 1038–1044 (1995).
77. Heslop, H. E. et al. Long-term restoration of immunityagainst Epstein–Barr virus infection by adoptive transfer ofgene-modified virus-specific T lymphocytes. Nature Med. 2,551–555 (1996).
78. Dudley, M. E. et al. Cancer regression and autoimmunity inpatients after clonal repopulation with antitumourlymphocytes. Science 298, 850–854 (2002).Shows that the use of non-myeloablativechemotherapy to induce lymphopaenia allows fordramatic in vivo expansion and clonal repopulation ofadoptively transferred T cells specific fordifferentiation antigens expressed in melanoma. Thistherapy was associated with tumour regression andautoimmune destruction of normal melanocytes insome patients.
79. Yee, C. et al. Adoptive T cell therapy using antigen-specificCD8+ T cell clones for the treatment of patients withmetastatic melanoma: in vivo persistence, migration, andantitumour effect of transferred T cells. Proc. Natl Acad. Sci.USA 99, 16168–16173 (2002).
80. Mutis, T. et al. Efficient induction of minor histocompatibilityantigen HA-1-specific cytotoxic T-cells using dendritic cellsretrovirally transduced with HA-1-coding cDNA. Biol. BloodMarrow Transplant. 8, 412–419 (2002).
81. Osman, Y. et al. Generation of bcr–abl specific cytotoxic T-lymphocytes by using dendritic cells pulsed with bcr-abl(b3a2) peptide: its applicability for donor leukocytetransfusions in marrow grafted CML patients. Leukemia 13,166–174 (1999).
82. Osman, Y. et al. Dendritic cells stimulate the expansion ofPML–RARα specific cytotoxic T-lymphocytes: itsapplicability for antileukemia immunotherapy. J. Exp. Clin.Cancer Res. 18, 485–492 (1999).
83. Yee C. et al. Isolation of high avidity melanoma-reactiveCTL from heterogeneous populations using peptide-MHC tetramers. J. Immunol. 162, 2227–2234 (1999).
84. Becker C. et al. Adoptive tumor therapy with T lymphocytesenriched through an IFN-γ capture assay. Nature Med. 7,1159–1162 (2001).
85. Brodie, S. J. et al. In vivo migration and function oftransferred HIV-1-specific cytotoxic T cells. Nature Med. 5,34–41 (1999).
86. Lu, J. et al. Interleukin 15 promotes antigen-independent invitro expansion and long-term survival of antitumourcytotoxic T lymphocytes. Clin. Cancer Res. 8, 3877–3884(2002).
87. Cooper, L. J., Kalos, M., Lewinsohn, D. A., Riddell, S. R. &Greenberg, P. D. Transfer of specificity for humanimmunodeficiency virus type 1 into primary human Tlymphocytes by introduction of T-cell receptor genes. J. Virol. 74, 8207–8212 (2000).
88. Stanislawski, T. et al. Circumventing tolerance to a humanMDM2-derived tumor antigen by TCR gene transfer. NatureImmunol. 2, 962–970 (2001).
89. Heemskerk, M. H. et al. Redirection of antileukemicreactivity of peripheral T lymphocytes using gene transfer ofminor histocompatibility antigen HA-2-specific T-cellreceptor complexes expressing a conserved alpha joiningregion. Blood 102, 3530–3540 (2003).
90. Dudley, M. E. & Rosenberg, S. A. Adoptive-cell-transfertherapy for the treatment of patients with cancer. NatureRev. Cancer 3, 666–675 (2003).
91. Brentjens, R. J. et al. Eradication of systemic B-cell tumorsby genetically targeted human T lymphocytes co-stimulatedby CD80 and interleukin-15. Nature Med. 9, 279–286 (2003).
92. Sallusto, F. & Lanzavecchia, A. Understanding dendritic celland T-lymphocyte traffic through the analysis of chemokinereceptor expression. Immunol. Rev. 177, 134–140 (2000).
93. Mohle, R. et al. The chemokine receptor CXCR-4 isexpressed on CD34+ hematopoietic progenitors andleukemic cells and mediates transendothelial migrationinduced by stromal cell-derived factor-1. Blood 91,4523–4530 (1998).
94. Koelle, D. M. et al. Expression of cutaneous lymphocyte-associated antigen by CD8+ T cells specific for a skin-tropicvirus. J. Clin. Invest. 110, 537–548 (2002).
95. Hacein-Bey-Abina, S. et al. A serious adverse event aftersuccessful gene therapy for X-linked severe combinedimmunodeficiency. N. Engl. J. Med. 348, 255–256 (2003).
96. Bonini, C. et al. HSV-TK gene transfer into donorlymphocytes for control of allogeneic graft-versus-leukemia.Science 276, 1719–1724 (1997).
97. Riddell, S. R. et al. T-cell mediated rejection of gene-modified HIV-specific cytotoxic T lymphocytes in HIV-infected patients. Nature Med. 2, 216–223 (1996).
98. Thomis, D. C. et al. A Fas-based suicide switch in human T cells for the treatment of graft-versus-host disease. Blood97, 1249–1257 (2001).
99. Berger, C. et al. Pharmacologically regulated Fas-mediateddeath of adoptively transferred T cells in a nonhumanprimate model. Blood 103, 1261–1269 (2003).
100. Chen, B. J., Cui, X., Sempowski, G. D., Liu, C. & Chao, N. J.Transfer of allogeneic CD62L- memory T cells without graft-versus-host disease. Blood 103, 1534–1541 (2003).
101. Anderson, B. E. et al. Memory CD4+ T cells do not inducegraft-versus-host disease. J. Clin. Invest. 112, 101–108(2003).
102. Hughes, T. P. et al. Frequency of major molecular responsesto imatinib or interferon α plus cytarabine in newlydiagnosed chronic myeloid leukemia. N. Engl. J. Med. 349,1423–1432 (2003).
AcknowledgementsWork in the authors’ laboratory is supported in part by grants fromthe National Institutes of Health and the Leukemia and LymphomaSociety. We thank past and present members of the Programme inImmunology for helpful discussions, and W. Hilliker for assistance inpreparation of the manuscript.
Competing interests statementThe authors declare that they have no competing financial interests.
Online links
DATABASESThe following terms in this article are linked online to:Cancer.gov: http://cancer.gov/acute lymphoblastic leukaemia | acute myelogenous leukaemia |chronic lymphoblastic leukaemia | chronic myelogenousleukaemia | melanoma | multiple myeloma | renal-cell carcinoma LocusLink: http://www.ncbi.nlm.nih.gov/LocusLink/BCL2A1 | CD34 | CLA1 | CXCR4 | HA-1 | HA-2 | HA-8 | HB-1 |IFN-γ | proteinase 3 | SDF1 | SMCY | UGT2B17 | UTY | WT1
FURTHER INFORMATIONInternational Bone Marrow Transplant Registry:www.ibmtr.orgInternational Histocompatibility Working Group:www.ihwg.orgAccess to this interactive links box is free online.