Embed Size (px)
Citation preview
BC CDC Public Health Lab
Mel Krajden MD, FRCPCMedical Director,
BCCDC Public Health LaboratoryMedical Head, Hepatitis
BC Centre for Disease Control
Professor, Pathology & Laboratory Medicine, UBC
Targeted, Multiplex or Pan-Diagnostic Molecular Respiratory Testing:What are the lessons learned?
Disclosures:• Grants/contracts to my institution
from Roche, Siemens, Hologic, Boerhinger Ingelheim• Mitigation: most contracts unrelated
and the presentation will provide a public health perspective
BC CDC Public Health Lab
Objectives:• Learn how automation affects quality
and turnaround times• Understand how Lab Developed
Tests (LDTs) and commercial In Vitro Diagnostic Devices (IVDs) can co-exist to improve care
BC CDC Public Health Lab
Nucleic acid testing (NAT) is used for individual and outbreak diagnosis– Local vs central testing
• Targeted tests: FluA• Multiplex tests: FluA/B/RSV– Multiplexes or do sequential multiplex reflex
testing
• Pan-Diagnostic tests:– Simultaneously detect a broad array of
agents e.g., MAGPIX NxTAG Respiratory Pathogen Panel – 22 targets: 19 viral, 3 bacterial
BC CDC Public Health Lab
Factors affecting turnaround time (TAT) • Sample collection/type: NP/lower respiratory!• Sample transport: external/within facility• Testing approach: individual or batched– POC– Hospital/facility– Centralized
• Result reporting:– Electronic – batched or real-time– What is a critical result?
BC CDC Public Health Lab
TAT considerations cont’d:• Timeliness: received/interpreted by the
orderer?–Result actionable, i.e., alter management!
• Justifies/avoids treatment• Justify/avoids an infection control/outbreak response -
cohorting/prophylaxis
–Alter outcome?• Flu A or B – individual/outbreak control• Enterovirus D68 – correlation with AFP• Mycoplasma?• Legionella – identify a common exposure risk?
BC CDC Public Health Lab
TAT considerations summary:• sample quality• transport• assay design• testing location• staffing• operating hours• reporting mechanisms• provider being informed• provider actions• outcomes and costs
BC CDC Public Health Lab
Key testing challenges:Ramanan et al. Clin Micro Reviews Jan 2018
Targeted testing: Syndromic overlap between
bacterial/viral/other illnesses
– Clinician may not order the right test!
• Multiple simultaneous or sequential tests - TAT/costs
• Pan-diagnostic tests are still in the early stages in terms of
comprehensiveness – detect an array of bacterial agents/detect
antimicrobial resistance, etc
– Multiplex/pan-diagnostics highlight clinical complexity e.g.,
co-infections, shedding and colonization
• Is the detected agent clinically relevant?
• Paediatric rhinovirus?
BC CDC Public Health Lab
Key testing challenges cont’d:Multiplex(s) - (e.g., Flu A/B/RSV; Adeno, hMPV, Rhino; ParaFlu 1/2/3/4);
• 1o screen – FluA/B/RSV– Broader panel - simultaneously or reflex - TAT?– Methodology LDT/IVD– Co-infection interpretation– Respiratory infections are seasonal• Summer? Fall? Spring? Peak influenza endemic – 30%
to 50% of samples can be Flu +ve
BC CDC Public Health Lab
Key testing challenges cont’d:Pan-Diagnostic - multiple viral/bact/agents, etcsimultaneously– Decreases time to Dx, may reduce time to Rx →
mortality/hospitalization impacts are inconclusive– Not comprehensive enough → high cost add on• MagPix – increased rate of detection of atypical bact.
– Performance: 80% to 100% sens and 98 to 99% spec – QC/QA not simple
– TAT is affected by: individual vs batched testing– Co-infections, shedding, colonization
BC CDC Public Health Lab
Blaschke et al. Pediatrics 2018 - illustrates clinical and laboratory challenges• In-patients or ER visits from febrile 1 to 90 day old infants
– 4,037/10,964 (37%) underwent resp. viral PCR testing– 2,212 (55%) had respiratory virus, 1,392 (35%) had human rhinovirus– Febrile infants with rhinovirus → more likely to have a bacterial
infection relative to those with non-rhinovirus infections– Risk of UTI or invasive bacterial infection was not significantly different
for those with or without rhinovirus
• Rhinovirus is common in young febrile infants → doesn’t alter the risk for concomitant UTI or invasive bacterial infection– Doing a multiplex/pan-diagnostic does not replace clinical judgement!
BC CDC Public Health Lab
To LDT or not LDT, that is the question?
Lab Developed Tests (LDT) are now very feasible:• Advances in molecular biology• Public sharing of sequences• Automated extraction methodologies• Automated and real-time amplification equipment• Standardized master mix backbones and cycling parameters
Report viaLIS
-interfaceor
-manually
LDTs for clinical Dx:• Extensive validation, ongoing reagent QC/QA• Publically reported sequences may not reflect
circulating strain variants• Lab is responsible for automation integration• Can control the test menu, but because of limited
integration → not amenable to simultaneous testing of different agents
Report viaLIS
-interfaceor
-manually
LDTs for clinical Dx cont’d:• Manual components may increase the risk of sample
or amplicon contamination• Instruments illustrated above are conducive to
batching → ↑ TATs• Not amenable to a typical hospital laboratory → need
high-level technical expertise• Per test costs are low → instrument costs/amortized
across all tests • Can be rapidly adapted for novel agent detection
Sample carryover & amplicon contamination• Sample handling• Using the same primer sets over and over• Vector DNA – containing target gene inserts and
other positive controls– Dust and aerosols– NAT reagents, pipets, and tubes– Work surfaces– Instruments– Humans
BC CDC Public Health Lab
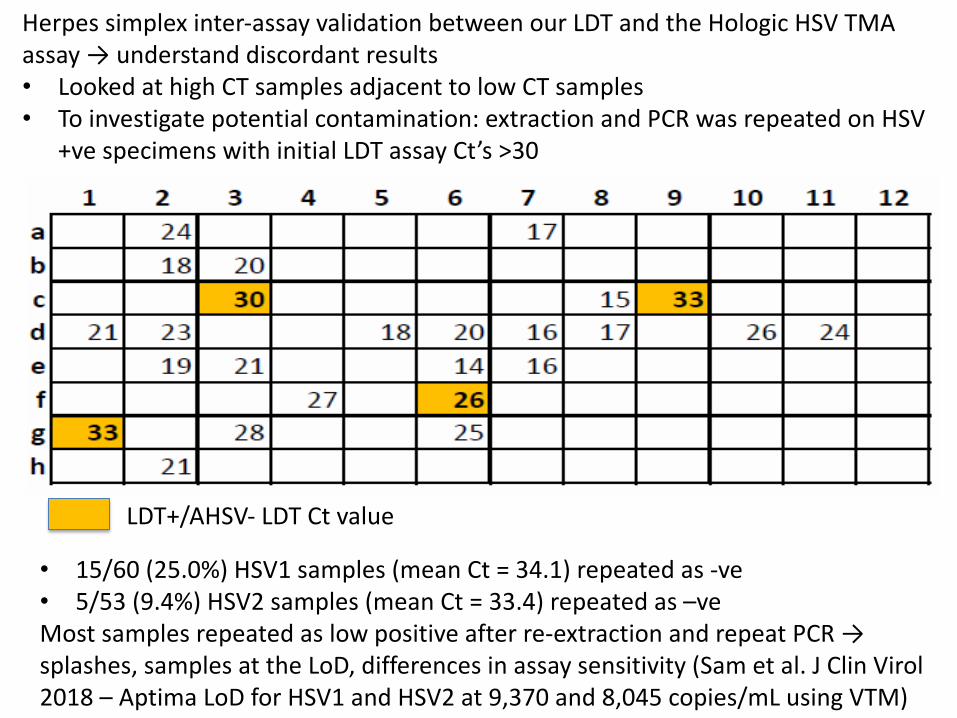
LDT+/AHSV- LDT Ct value
• 15/60 (25.0%) HSV1 samples (mean Ct = 34.1) repeated as -ve• 5/53 (9.4%) HSV2 samples (mean Ct = 33.4) repeated as –veMost samples repeated as low positive after re-extraction and repeat PCR →splashes, samples at the LoD, differences in assay sensitivity (Sam et al. J Clin Virol2018 – Aptima LoD for HSV1 and HSV2 at 9,370 and 8,045 copies/mL using VTM)
Herpes simplex inter-assay validation between our LDT and the Hologic HSV TMA assay → understand discordant results• Looked at high CT samples adjacent to low CT samples• To investigate potential contamination: extraction and PCR was repeated on HSV
+ve specimens with initial LDT assay Ct’s >30
To IVD or not IVD, that is the question?
IVDs for clinical Dx – commercial test:• Most assay validation, reagent QC/QA rests with
the manufacturer• Manufacturer should adjust for circulating strain
variants → tests are proprietary• Responsible for instrument integration• Automated reflex testing, mixed test menus are
possible – huge advancement!• IVDs & LDTs on the same platform
Abbott; Becton Dickinson; Hologic; Roche; etc→ integrated extraction, amplification and
reporting instruments able to do LDTs and IVDs
IVDs for clinical Dx cont’d:• Automation may reduce the risk of sample or
amplicon carryover/contamination• Some of the instruments enable random access• Amenable to hospital laboratories – less need
high-level technical expertise relative to LDTs• Amortize the instrument across the full array of all
tests including LDTs• Can be rapidly adapted for novel agent detection
Abbott; Becton Dickinson; Hologic; Roche; etc→ integrated extraction, amplification and
reporting instruments able to do LDTs and IVDs
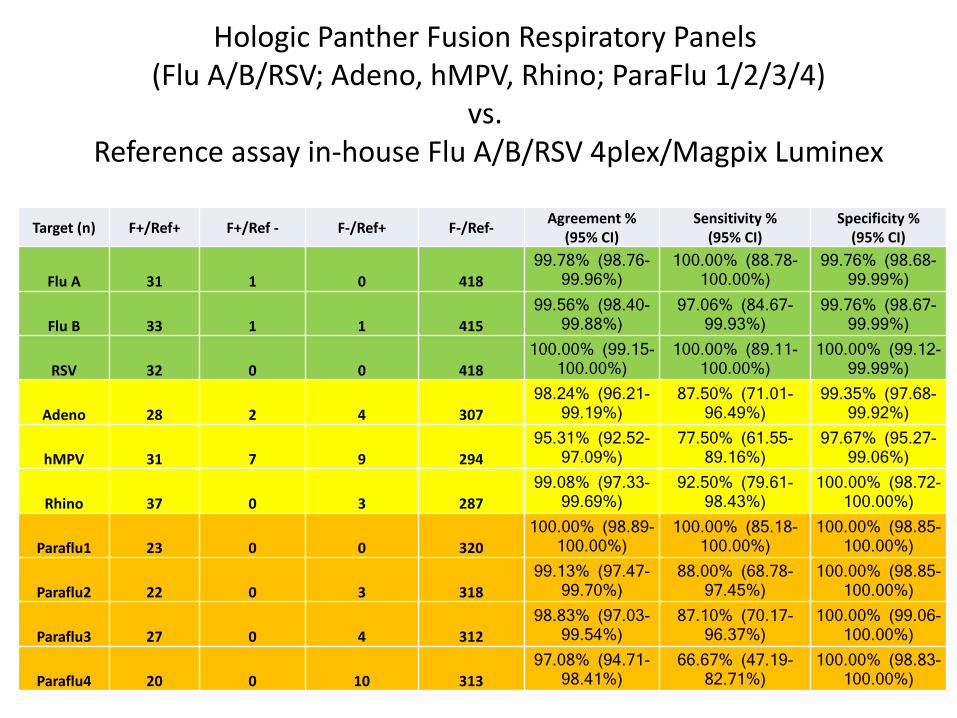
Hologic Panther Fusion Respiratory Panels(Flu A/B/RSV; Adeno, hMPV, Rhino; ParaFlu 1/2/3/4)
vs.Reference assay in-house Flu A/B/RSV 4plex/Magpix Luminex
Target (n) F+/Ref+ F+/Ref - F-/Ref+ F-/Ref- Agreement %(95% CI)
Sensitivity %(95% CI)
Specificity % (95% CI)
Flu A 31 1 0 41899.78% (98.76-
99.96%)100.00% (88.78-
100.00%)99.76% (98.68-
99.99%)
Flu B 33 1 1 41599.56% (98.40-
99.88%)97.06% (84.67-
99.93%)99.76% (98.67-
99.99%)
RSV 32 0 0 418100.00% (99.15-
100.00%)100.00% (89.11-
100.00%)100.00% (99.12-
99.99%)
Adeno 28 2 4 30798.24% (96.21-
99.19%)87.50% (71.01-
96.49%)99.35% (97.68-
99.92%)
hMPV 31 7 9 29495.31% (92.52-
97.09%)77.50% (61.55-
89.16%)97.67% (95.27-
99.06%)
Rhino 37 0 3 28799.08% (97.33-
99.69%)92.50% (79.61-
98.43%)100.00% (98.72-
100.00%)
Paraflu1 23 0 0 320100.00% (98.89-
100.00%)100.00% (85.18-
100.00%)100.00% (98.85-
100.00%)
Paraflu2 22 0 3 31899.13% (97.47-
99.70%)88.00% (68.78-
97.45%)100.00% (98.85-
100.00%)
Paraflu3 27 0 4 31298.83% (97.03-
99.54%)87.10% (70.17-
96.37%)100.00% (99.06-
100.00%)
Paraflu4 20 0 10 31397.08% (94.71-
98.41%)66.67% (47.19-
82.71%)100.00% (98.83-
100.00%)
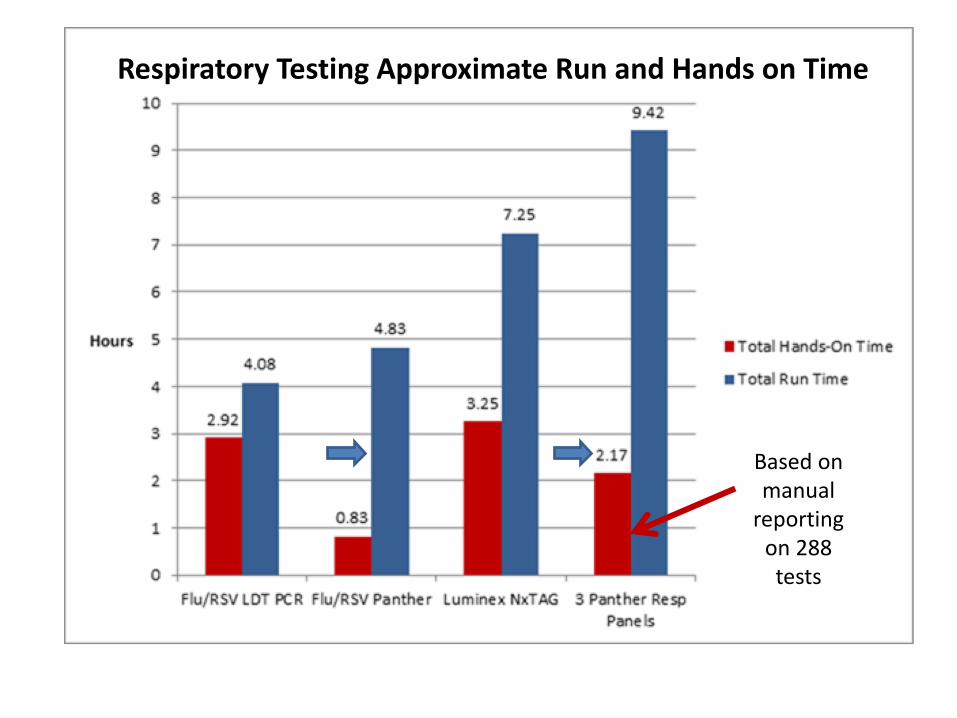
Respiratory Testing Approximate Run and Hands on Time
Based onmanual
reportingon 288 tests
• High-throughput automated NAT → akin to automated serology platforms are here → revolutionize ID diagnostics
• Commercial integrated platforms that can do targeted and multiplexed IVDs and LDTs will replace piecemeal automation• Reduce labour costs, streamline testing and reporting
and will improve testing quality• Ability to do both IVDs and LDTs creates a more flexible
test menu, amortizes instrument costs and improves the ability to rapidly respond to novel agents
• Pan-diagnostic panels still need to become more comprehensive before they can fully replace traditional microbial diagnostics and justify their cost for many clinical conditions…
• Research on cost-effectiveness and health outcome impact of these approaches
Acknowledgements Brian AukYin ChangMichael ChanTracy ChanRon ChowDiane EislerKingsley GunadasaBecky HickmanAgatha JassemMarko KrywruchkoKaren MooderVirology lab
BC CDC Public Health Lab
Thank You!