Embed Size (px)
Citation preview

PM08CH02-Ebert ARI 13 December 2012 18:55
Molecular Pathophysiology ofMyelodysplastic SyndromesR. Coleman Lindsley1,2 and Benjamin L. Ebert1,2
1Division of Hematology, Brigham and Women’s Hospital, Boston, Massachusetts 02215;email: [email protected] of Medical Oncology, Dana-Farber Cancer Institute, Boston,Massachusetts 02115; email: [email protected]
Annu. Rev. Pathol. Mech. Dis. 2013. 8:21–47
First published online as a Review in Advance onAugust 28, 2012
The Annual Review of Pathology: Mechanisms ofDisease is online at pathol.annualreviews.org
This article’s doi:10.1146/annurev-pathol-011811-132436
Copyright c© 2013 by Annual Reviews.All rights reserved
Keywords
RNA splicing, cytogenetic, epigenetic, mutation
Abstract
The clinicopathologic heterogeneity of myelodysplastic syndromes(MDS) is driven by diverse, somatically acquired genetic abnormali-ties. Recent technological advances have enabled the identification ofmany new mutations, which have implicated novel pathways in MDSpathogenesis, including RNA splicing and epigenetic regulation of geneexpression. Molecular abnormalities, either somatic point mutations orchromosomal lesions, can be identified in the vast majority of MDS casesand underlie specific disease phenotypes. As the full array of molecu-lar abnormalities is characterized, genetic variables are likely to com-plement standard morphologic evaluation in future MDS classificationschemes and risk models.
21
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
IPSS: InternationalPrognostic ScoringSystem
MDS/MPN:myelodysplastic/myeloproliferativeneoplasms
Ring sideroblasts:erythroid precursors,identified on ironstaining of a bonemarrow aspiratesmear, that containfive or more irongranules around atleast one-third of thenucleus
AML: acute myeloidleukemia
MPN:myeloproliferativeneoplasms
INTRODUCTION
Myelodysplastic syndromes (MDS) are aheterogeneous group of clonal hematopoieticdisorders that are characterized by ineffectivehematopoiesis, peripheral blood cytopenias,and a propensity for leukemic transforma-tion. Morphologic dysplasia, identified onexamination of the bone marrow, is a definingfeature of MDS and is an important criterionfor disease classification. The World HealthOrganization (WHO) classification systemcurrently recognizes seven distinct pathologicsubtypes of MDS that are based on thesemorphologic features, the percentage of bonemarrow cells that are blasts, and the numberof affected hematatopoietic lineages (Table 1)(1). The rapidly expanding compendium ofmolecular lesions in MDS may enable majoradvances in diagnosis, estimation of prognosis,and prediction of therapeutic response andmay lead to the development of novel therapiesfor patients with this disease.
With recent technical and scientific ad-vances, molecular abnormalities, includingcopy number abnormalities and point mu-tations, can now be identified in the vastmajority of MDS cases. Metaphase cytogeneticanalysis detects chromosomal abnormalities inapproximately 50% of cases (2, 3), althoughsensitive techniques such as single-nucleotidepolymorphism microarrays (SNP-A) and arraycomparative genomic hybridization (CGH)can identify abnormalities in nearly 80% ofcases (4). Clinical MDS risk stratificationperformed using the International PrognosticScoring System (IPSS) integrates cytogeneticinformation, along with bone marrow blastpercentage and peripheral blood counts, to dis-tinguish four prognostic subgroups (5). Recentanalysis of a large international data set enabledfurther refinement of karyotype information,and it defined 19 distinct cytogenetic categoriesthat distinguish five prognostic subgroups (2).
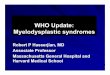
Somatic point mutations can be identified inmore than 50% of MDS cases, including mostthat have a normal karyotype (Figure 1) (6, 7).These emerging genetic data have transformed
our understanding of MDS pathophysiology,implicating new biological pathways and pro-viding a new tool to deconstruct the complexityof MDS phenotypes. Recurrent mutations havebeen identified that alter many essential cellularprocesses, including RNA splicing, epigeneticregulation of gene expression, DNA-damageresponse, and tyrosine kinase signaling. Specificmutations in these pathways are, in some cases,tightly associated with distinct morphologicfeatures or clinical phenotypes. For example,mutations in SF3B1 are associated with thepresence of ring sideroblasts (6, 9), and SRSF2,TET2, and ASXL1 mutations are enriched inthe overlap myelodysplastic/myeloproliferativeneoplasms (MDS/MPN) with markedmyelomonocytic differentiation (6, 10).Combinations of point mutations and chromo-somal abnormalities probably underlie much ofthe clinicopathologic heterogeneity of MDS.
RNA SPLICING
Recurrent somatic mutations in componentsof the spliceosome have recently been identi-fied with whole-genome and whole-exome se-quencing of MDS patient samples (6, 9, 11). As aclass, these mutations are remarkably common;they affect 45–85% of MDS cases, dependingon the morphologic subtype. Splicing muta-tions are generally enriched in diseases charac-terized by morphologic dysplasia, such as MDS,chronic myelomonocytic leukemia (CMML),therapy-related acute myeloid leukemia (t-AML), and AML with myelodysplasia-relatedchanges. By contrast, spliceosome mutationsoccur at low frequency in myeloid diseases with-out dysplasia, including de novo AML and themyeloproliferative neoplasms (MPN) (6). Al-though the molecular consequences of thesegenetic lesions have not been elucidated, theidentification of mutations in multiple genesthat encode components of this enzyme com-plex implicates aberrant splicing in the patho-physiology of many MDS cases.
The spliceosome mediates excision ofintrons and ligation of flanking exons to gen-erate mature messenger RNAs (mRNAs) from
22 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
Table 1 The 2008 World Health Organization classification of myelodysplastic syndromes andmyelodysplastic/myeloproliferative neoplasms (1, 149, 150)
DiseaseCommon
abbreviation Peripheral blood findings Bone marrow findingsRefractory cytopenia withunilineage dysplasia
RCUD Uni- or bicytopenia, blasts <1% Unilineage dysplasia (≥10% of cells in onemyeloid lineage), blasts <5%, ringsideroblasts comprising <15% of erythroidprecursors
• Refractory anemia RA
• Refractory neutropenia RN
• Refractorythrombocytopenia
RT
Refractory anemia withring sideroblasts
RARS Anemia, blasts absent Ring sideroblasts constitute ≥15% of erythroidprecursors, dysplasia limited to erythroidlineage, blasts <5%
Refractory cytopenia withmultilineage dysplasia
RCMD Cytopenia(s),a blasts <1%, no Auerrods, monocytes <1 × 109 liter−1
Dysplasia in ≥10% of cells in more than onemyeloid lineage, blasts <5%, no Auer rods
Refractory anemia withexcess blasts–1
RAEB-1 Cytopenia(s), blasts <5%, no Auerrods, monocytes <1 × 109 liter−1
Dysplasia in ≥1 lineage, blasts 5–9%, no Auerrods
Refractory anemia withexcess blasts–2
RAEB-2 Cytopenia(s), blasts 5–19%,presence or absence of Auer rods,monocytes <1 × 109 liter−1
Dysplasia in ≥1 lineage, blasts 10–19%,presence or absence of Auer rods
Myelodysplastic syndrome,unclassifiable
MDS-U Cytopenias, blasts ≤1% Unequivocal morphologic dysplasia in <10%cells of at least one lineage when accompaniedby a clonal cytogenetic abnormality, blasts<5%
MDS with isolated del(5q) — Anemia, platelet count normal orincreased, blasts <1%
Normal or increased megakaryocytes withhypolobated nuclei, blasts <5%, isolateddel(5q) cytogenetic abnormality, no Auer rods
Chronic myelomonocyticleukemia
CMML Persistent monocytosis (monocytes>1 × 109 liter−1)
Dysplasia in one or more myeloid lineages; ifdysplasia absent, diagnosis can be made if(a) acquired clonal cytogenetic or moleculargenetic lesion is present and (b) monocytosispersists for more than three months and othercauses are excluded; no Philadelphiachromosome or BCR-ABL1 fusion gene; norearrangement of PDGFRA or PDGFRB;blasts <20%
Myelodysplastic/myeloproliferativeneoplasm, unclassifiable
MDS/MPN (a) Clinical, laboratory, morphological features of MDS and <20% bone marrowblasts; (b) prominent myeloproliferative features, including either platelets >450 ×109 liter−1 with associated megakaryocytic proliferation or white blood cells≥13 × 109 without splenomegaly; and (c) no prior MDS or MPN, no BCR-ABL1fusion gene, no rearrangement of PDGFRA or PDGFRB, no isolated del(5q) or 3qabnormalities, no recent exposure to cytotoxic therapy or hematopoietic growthfactors. Alternatively: de novo disease with mixed MDS/MPN features that cannotbe assigned to another category of MDS, MPN, or MDS/MPN
• RARS associated withmarked thrombocytosis
RARS-T
aCytopenias are defined as follows: hemoglobin, <10 g dl−1; absolute neutrophil count, <1.8 × 109 liter−1; platelets, <100 × 109 liter−1.
www.annualreviews.org • Molecular Pathophysiology of MDS 23
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
Karyotype
SF3B1SRSF2
NPM1IDH1/2ETV6
TK pathwayEZH2ASXL1
TET2
U2AF1
TP53
DNMT3A
RUNX1
Figure 1Somatic mutations in 255 cases of myelodysplastic syndrome with a normal karyotype or a −Y karyotype. Among cases with a normalkaryotype or a −Y karyotype, 72% harbor somatic mutations in at least 1 of 17 genes tested. Each column represents one patientsample, and each row corresponds to mutations in a gene or gene family. TK pathway denotes mutations in genes that activate tyrosinekinase signaling (NRAS, KRAS, BRAF, CBL, and JAK2). Modified from Reference 7 with permission; based in part on Reference 8.
precursor mRNA (pre-mRNA) (Figure 2b).Alternative splicing is an evolutionarily con-served mechanism that enables the productionof multiple mRNA and protein isoforms from asingle gene. Deep sequencing of mRNA acrosshuman tissues has revealed that 90–95% ofmultiexon genes undergo alternative splicing,which causes the production of more than100,000 distinct mRNA species from only25,000 protein-coding genes (12, 13). Severaldistinct types of alternative splicing have beenidentified in normal physiology (Figure 2d ).
Exon skipping, whereby an exon and its flankingintrons are excised together from a transcript,is the most common and accounts for 30% to40% of alternative splicing events. Other typesof alternative splicing events include alternative5′ or 3′ splice-site selection, alternative firstor last exon utilization, tandem 3′ UTR (un-translated region) creation, and rarely intronretention. Aberrantly spliced mRNA speciescan be degraded by the nonsense-mediateddecay (NMD) pathway. Abnormal transcriptsthat escape NMD-mediated elimination can be
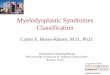
−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−→Figure 2Mutations that affect RNA splicing machinery are common in myelodysplastic syndromes (MDS).(a) Mutations in genes that encode components of the RNA splicing machinery are mutually exclusive andoccur in a range of cytogenetic contexts. Each column represents one sample. Mutations are shown as redbars. Specific karyotypic abnormalities are color coded as follows: red, isolated deletion on the long arm ofchromosome 5 [del(5q)]; green, −7/del(7q) alone or +1 abnormality; blue, isolated +8; yellow, isolateddel(20q); black, complex; white, normal or −Y; orange, unknown. Modified from Reference 8 withpermission. (b) Schematic of RNA splicing showing spliceosome-mediated precursor–messenger RNAprocessing that causes the excision of an intervening intron and ligation of flanking exons. (c) Selectedcomponents of the spliceosome are mutated in MDS. The U1 small nuclear ribonucleoprotein (snRNP)binds to the 5′ splice site (5′ SS), and the U2 snRNP binds to the branch point. The U2 auxiliary factor(U2AF), which is composed of U2AF1 and U2AF2 subunits, binds to the 3′ splice site (3′ SS) andpolypyrimidine tract [Y(n)]. Serine- and arginine-rich proteins bind to the exonic splice enhancer (ESE). Thegenes encoding SF3A1, SF3B1, U2AF1, U2AF2, SF1, SRSF2, and ZRSR2 are mutated in myeloidneoplasms and are shown in red. (d ) Various outcomes of alternative splicing occur in normal physiology,including alternative splice-site selection, exon skipping, and intron retention.
24 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
Pre-mRNA splicing:the process by whichpre-mRNAs areconverted to maturemRNA by excision ofnoncoding sequences(introns) and joining ofcoding sequences(exons)
translated into mislocalized or dysfunctionalproteins that have been implicated in thepathogenesis of cancer and other diseases (14).
The spliceosome consists of core smallnuclear ribonucleoproteins (snRNPs) andnon-snRNP accessory proteins (Figure 2c).Whereas snRNPs are critical to the structuraland enzymatic function of the spliceosome,non-snRNPs are important for structural
assembly, splice-site selection, and coordi-nation of alternative splicing events. Normalpre-mRNA splicing occurs by a series of well-regulated steps, starting with the identificationof appropriate splice sites, followed by assem-bly of the spliceosome complex and catalysisof cleavage and ligation reactions. Splice-siterecognition is mediated by specific interac-tions between spliceosomal components and
a
b
c
d Alternative splice-site selection
U1 snRNP
5' SS
GU Y(n)
Exon skipping or retention
Intron retention
SF3B1SRSF2U2AF1
Karyotype
U2AF2
ZRSR2
SF1
3' SSYAG
U2AF1SRSF2
ESE
U2 snRNP
SF3A1SF3B1
A
www.annualreviews.org • Molecular Pathophysiology of MDS 25
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
Small nuclearribonucleoproteins(snRNPs):RNA-proteincomplexes that makeup part of thespliceosome and areimportant forcatalyzing pre-mRNAprocessing
conserved RNA sequence motifs. The principalcis-acting signals include the 5′ and 3′ splice sites[invariant guanine-uracil (GU) and adenine-guanine (AG), respectively], a polypyrimidinetract (PPT) just upstream of the 3′ splicesite, and an adenine-containing branch pointupstream of the PPT. The pattern of alter-native splicing is regulated in a tissue-specificfashion by the interaction between trans-actingregulatory proteins and these locus-specificcis-acting RNA sequence elements (15).
Recurrent mutations have been identified ingenes involved in the early steps of U2 snRNPassembly/function (SF3A1, SF3B1, ZRSR2,SRSF2) and 3′ splice-site recognition, includ-ing branch point sequence binding (SF1), PPTbinding (U2AF2), and 3′ splice-site binding(U2AF1). In nearly all instances, mutationsin components of the splicing machinery aremutually exclusive (Figure 2a) (6). Severalgenes are subject to recurrent heterozygousmissense mutations (SF3B1, SRSF2, U2AF1),whereas others display diverse mutation typesthroughout the open reading frame (ZRSR2)(Figure 2c). Further studies will be requiredto clarify which lesions cause a loss of functionand which cause a gain or alteration of proteinfunction.
SF3B1
SF3B1 is the most frequently mutated spliceo-somal gene in MDS, affecting 14–28% of un-selected patients (6, 9, 16, 17). Mutations ofSF3B1 are strongly associated with the presenceof ring sideroblasts. Among MDS patients withring sideroblasts, 50–75% have SF3B1 muta-tions. An SF3B1 mutation has a 98%-positivepredictive value for the presence of ring sider-oblasts, and interestingly, the percentage of ringsideroblasts in a given patient is proportionalto the SF3B1 mutant allele frequency (16).Together, these data support a causal mechanis-tic relationship between SF3B1 mutation andthe generation of ring sideroblasts.
Initial studies found SF3B1 mutations tobe independently associated with prolongedoverall and leukemia-free survival, whereas a
subsequent study concluded that SF3B1 mu-tation status provided no additional prognosticinformation beyond established morphologicrisk categories (9, 16, 18). Compared withMDS without SF3B1 mutation, MDS withSF3B1 mutation are characterized by higherplatelet counts (9, 16–18), lower bone marrowblast counts (9, 16, 17), and higher white bloodcell counts (9, 17).
SF3B1 encodes a subunit of the splicingfactor 3b complex, which, together with theSF3A complex and the U2 small nuclear RNA,constitutes the U2 snRNP. SF3B1 mutationsare heterozygous missense substitutions thatpredominantly affect conserved residues withinthe carboxy-terminal HEAT repeats. Approx-imately 90% of mutations involve five aminoacids: K700 (58%), K666 (11%), H662 (10%),E622 (7%), and R625 (6%). On the basis ofprotein structure prediction algorithms, inves-tigators have suggested that mutated SF3B1 re-mains structurally intact, although presumablywith altered function (9). The nature of SF3B1dysfunction is unclear, however, given that noglobal splicing abnormalities have been iden-tified in MDS with SF3B1 mutations and noexperimental model has been reported.
U2AF1
Mutations in U2AF1, a subunit of the U2snRNP auxiliary factor (U2AF) that binds the3′ splice acceptor site, are present in 8% to 9%of unselected MDS samples (6, 11). In con-trast to SF3B1 mutations, U2AF1 mutations areassociated with an increased rate of progres-sion to AML, despite no difference in medianblast count, IPSS or other clinical parameters.U2AF1 mutations are heterozygous missensesubstitutions within the conserved zinc fingerdomains that predominantly affect amino acidresidue S34 and less commonly residue Q157.Uniparental disomy and mutations or deletionsof the remaining allele are uniformly absent.Functional analysis of the U2AF1 S34 mutatedprotein demonstrated increased splicing activ-ity using in vitro reporter assays (11) and pro-duction of aberrant splice products on the basis
26 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
HSC: hematopoieticstem cell
Epigeneticregulators: factorsthat influence cellularphenotype withoutaffecting the primarynucleotide sequence,often via effects onlocal transcriptionalpotential
5mC:5-methylcytosine
DNMT: DNAmethyltransferase
5hmC: 5-hydroxymethylcytosine
of RNA sequencing and exon arrays (6). In vivo,murine hematopoietic stem cells (HSCs) thatexpress mutant U2AF1 had a reduced compet-itive repopulation capacity (6).
Several studies have identified MDS-specificsplicing patterns in genes that regulate cellgrowth and survival, but it is not clear whetherthese changes are caused by mutations in genesthat encode splicing factors (19, 20). The ob-servation that certain mutations display a closeassociation with specific morphologicsubtypes—such as SF3B1 mutations withrefractory anemia with ring sideroblasts(RARS), RARS associated with marked throm-bocytosis (RARS-T), refractory cytopenia withmultilineage dysplasia and ring sideroblasts(RCMD-RS), and SRSF2 mutations withCMML—suggests unique mechanisms ofaction or context dependence. On the whole,splicing mutations are found in a mutuallyexclusive pattern and are restricted to proteinsinvolved in 3′ splice-site recognition and U2snRNP function. Consequent disruption of 3′
splice-site recognition could cause altered exonutilization or activation of cryptic 3′ splicesites, thereby creating novel protein isoformswith altered function or ectopic expressionof tissue-inappropriate isoforms. Aberrantsplicing may also cause a quantitative reductionof gene expression via the introduction ofpremature stop codons and activation ofnonsense-mediated decay. Moreover, compo-nents of the U2 snRNP interact directly withPolycomb group proteins, which suggests arole for splicing machinery in the epigeneticregulation of gene expression (21).
EPIGENETICS
Alongside genetic lesions that alter the RNAsplicing machinery, mutations in genes that en-code epigenetic regulators are among the mostcommon molecular abnormalities in MDS.These lesions affect genes involved in DNAmethylation and histone modification. Muta-tions in epigenetic regulators have the potentialto cause widespread alterations in transcrip-tional programs that can be maintained through
cell division, which could lead to the establish-ment and persistence of the MDS phenotype.
Mutations in several genes involved inDNA methylation, including DNMT3A andTET2, are commonly identified in MDS. Cy-tosine bases are converted to 5-methylcytosine(5mC) by DNA methyltransferases (DNMTs),primarily in the context of CpG dinucleotidesenriched at the site of gene promoters. In thiscontext, cytosine methylation status reducesgene transcription by recruiting methyl-CpG binding domain–containing repressorcomplexes or by influencing the binding oftranscription factors to promoter elements. Bycontrast, methylation of intragenic sites is asso-ciated with active transcription (22). Patterns ofDNA methylation can be maintained throughsuccessive rounds of cell division but shift sig-nificantly during cellular differentiation (23).
DNMTs are assigned to functional cate-gories on the basis of their de novo (DNMT3Aand DNMT3B) or maintenance (DNMT1)methyltransferase activity. These enzymescooperate to establish initial patterns ofmethylation and regenerate hemimethy-lated DNA during replication. 5mC itselfcan be modified by TET1, TET2, andTET3, paralogous members of a family ofFe(II)- and α-ketoglutarate-dependent dioxy-genases. TET proteins successively oxidize5mC to 5-hydroxymethylcytosine (5hmC),t-formylcytosine (5fC), and 5-carboxycytosine(5caC) (Figure 3a) (24). TETs can act on vari-ous substrates, including fully and hemimethy-lated DNA in CG and non-CG contexts (25).
MDS and secondary AML (sAML) are as-sociated with widespread alterations in DNAmethylation relative to normal hematopoieticprogenitors and de novo AML (26). Althoughthese abnormalities are found even in low-riskMDS, the extent of aberrant promoter hyper-methylation correlates with disease severity,predicts transformation to AML (27), and isindependently associated with reduced overallsurvival (28). These observations suggest an im-portant role for aberrant DNA methylation inMDS pathogenesis and serve as a rationale forthe therapeutic utility of DNMT inhibitors.
www.annualreviews.org • Molecular Pathophysiology of MDS 27
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
5mC
5hmC
5caC
5fC
5mC
5hmC
a
b
TET2
TET2
TET2
mTET2
Figure 3(a) TET proteins successively oxidize 5-methyl-cytosine (5mC) to 5-hydroxymethylcytosine(5hmC), t-formylcytosine (5fC), and5-carboxycytosine (5caC). (b) TET2 mutation(mTET2) causes reduced enzymatic activity anddecreased products of 5mC oxidation.
Two DNMT inhibitors, the nucleo-side analogs 5-azacytidine and 5-aza-2′-deoxycytidine (decitabine), have been approvedfor treatment of MDS in the United States.Treatment with these agents yields overallresponse rates of approximately 40% to 60%,whereas only 5-azacytidine has been shownto prolong overall survival (29, 30). Althoughtreatment with DNMT inhibitors inducesglobal promoter hypomethylation (26), theextent of pretreatment promoter hypermethy-lation does not predict clinical response (28).
DNMT3A
Recurrent mutations in DNMT3A have beenfound in approximately 22% of de novo AML,2% to 8% of unselected MDS, and up to 7%of CMML and primary myelofibrosis (31–34).In MDS, DNMT3A mutations have beenassociated with worsened survival and a shortertime to leukemic transformation (32, 33).Missense, nonsense, and frameshift mutationshave been identified throughout the codingregion of the DNMT3A gene, sometimes in thecontext of copy-neutral loss of heterozygosityor compound heterozygosity, suggesting that
they are loss-of-function mutations (31). How-ever, the most common DNMT3A mutation,which is found in 30% to 60% of cases, isa heterozygous arginine-histidine substitu-tion at position 882, which falls within themethyltransferase domain and reduces in vitroenzymatic activity (35); this type of DNMT3Amutation may confer gain of function or mayhave dominant-negative activity.
Despite the established role of DNMT3Ain DNA methylation, murine HSCs that lackDnmt3a show equivalent global levels of 5mCcompared with the levels in wild-type HSCs(36). Nevertheless, Dnmt3a-deficient HSCsare functionally abnormal; there is a distinctbias to self-renewal versus differentiation, as re-flected by enhanced competitive repopulationpotential following serial transplantation anda diminished contribution to lineage-restrictedprogenitor populations. HSCs that lackDnmt3a show an increase in the expression ofstem cell multipotency–associated genes and aconcomitant decrease in the expression of genesimportant for differentiation. Closer analysesof locus-specific methylation in Dnmt3−/−
HSCs revealed an unexpected combination ofhypo- and hypermethylation. Among the mostrobustly hypomethylated regions in Dnmt3−/−
HSCs are Runx1 and Gata3, both of which haveincreased histone 3 lysine 4 (H3K4) trimethy-lation, augmented expression, and directbinding by Dnmt3a. Similarly, B cells derivedfrom Dnmt3a-deficient HSCs display hy-pomethylation and ongoing expression of stemcell–associated genes, such as Runx1. Thesedata suggest that in murine hematopoiesis,Dnmt3a regulates the balance between self-renewal and differentiation by coordinatingrepression of the stem cell gene-expressionprogram and facilitating differentiation (36).
TET2
TET2 is the most commonly mutated genein MDS (19–26%) (7, 37, 38) and CMMLpatients (42–50%) (39, 40). TET2 mutationsare also frequently present in AML and areenriched in patients with sAML, AML with
28 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
PRC2: Polycombrepressive complex 2
myelodysplasia-related changes (22–24%),patients older than 60 years (29%), and AMLpatients with normal cytogenetics (23–30%)(38, 41, 42). In MDS, TET2 mutations aresimilarly associated with normal cytogeneticsand generally cooccur with mutations in othergenes (7). Although TET2 mutations are apotentially useful negative prognostic factorin AML with normal cytogenetics (41), TET2mutations have no clear prognostic significancein MDS (7, 37, 40, 43, 44).
TET2 mutations are predicted to resultin loss of function and are frequently iden-tified in the context of copy-neutral loss ofheterozygosity and hemizygous or compoundheterozygous mutations. Biochemical studieshave demonstrated reduced levels of 5hmCin the genomic DNA of bone marrow cellsfrom patients with TET-mutated malignancies,which suggests that the catalytic activity ofmutant TET2 protein is compromised (45).This conclusion is supported by targeteddeletion of the Tet2 catalytic domain in miceand the introduction of disease-associatedcatalytic domain mutant TET2 alleles into celllines, both of which demonstrate that deletionor mutation of TET2 decreases productionof 5hmC (Figure 3b) (45–47). Interestingly,patients with low 5hmC levels display a similarclinical phenotype independently of TET2 mu-tation status, which suggests that 5hmC levels,rather than TET2 mutation status per se, maymediate the observed clinical phenotype.
The functional roles of 5hmC and otherTET-dependent products of 5mC oxidationremain incompletely understood. Along with5mC, 5hmC may be an epigenetic mark that di-rectly influences gene transcription via specificinteractions with nuclear factors. TET activityand 5hmC presence appear to be enriched atsites of bivalent histone marks and to influ-ence the recruitment of Polycomb repressivecomplex 2 (PRC2) to target genes (48). Hy-droxymethylcytosine may otherwise indirectlyregulate gene expression as a demethylation in-termediate. Conversion of 5mC to 5hmC couldinhibit the binding or activity of maintenancemethyltransferases, thereby promoting passive,
replication-dependent cytosine demethylation.Alternatively, 5hmC may be an intermediatespecies in active, replication-independentdemethylation. In this model, 5mC undergoessuccessive TET-dependent oxidation to 5fCand 5caC, which are then cleaved to cytosineby the base excision-repair enzyme thymineDNA deglycosylase (49).
The biologic effect of TET2 inactivationon hematopoiesis has been studied usingmultiple independent mouse models (46, 47,50, 51). In all cases, inactivation of Tet2 causedcell-autonomous expansion of hematopoieticstem and progenitor cell (HSPC) populations,enhanced HSC self-renewal and replatingcapacity, and led to a bias toward myelomono-cytic differentiation. Tet2-deficient micedevelop a myeloproliferative phenotype that isreminiscent of human CMML, a disease with ahigh frequency of TET2 mutations. Mice withheterozygous Tet2 deletion (Tet2−/+) exhibit asimilar spectrum of hematopoietic abnormal-ities and a propensity to myeloid malignancies,albeit with delayed kinetics of onset. Together,these data suggest that reduced TET2 activityin human hematopoietic progenitors maycontribute to the establishment of clonal domi-nance and initiation of myeloid transformation.
In patients with TET2-mutated myeloidneoplasms, the mutant allele can be identi-fied in the earliest hematopoietic precursorpopulations (38, 44). However, monoallelicinactivation in isolation does not appear to com-promise functional multipotency, given thatTET2 mutations or 4q24 microdeletions can befound in both the myeloid neoplastic clone andpresumably normal lymphocytes (44, 52). Evenmore provocative is the observation that certainmature lymphoid neoplasms are associatedwith TET2 mutations; in some of these cases,the clonal origin may be traced to a multipotentprogenitor (47, 52). Indeed, close examinationof Tet2-deficient mice demonstrates dysregu-lated lymphopoiesis that is characterized by areduced number of B cells and an increased Tcell compartment that is shifted to an immaturephenotype. Impaired TET2 function in theearliest hematopoietic precursor may cause
www.annualreviews.org • Molecular Pathophysiology of MDS 29
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
2HG:2-hydroxyglutarate
Acquired uniparentaldisomy (alsocopy-neutral loss ofheterozygosity):acquiredhomozygosity, oftenassociated withduplication ofmutations in tumorsuppressors oroncogenes and loss ofthe normal allele
gradual clonal dominance and a predispositionto clonally related multilineage neoplasia.
IDH1 and IDH2
Heterozygous missense mutations in two iso-citrate dehydrogenase genes (IDH1 and IDH2)are found in AML (15–25%) (53, 54) and lessfrequently in MDS (4–12%) (7, 55, 56). Inmyeloid neoplasms, IDH1 and IDH2 muta-tions are mutually exclusive, uniformly monoal-lelic, and associated with a normal karyotype.IDH1 mutations have adverse prognostic valuein MDS (7, 55, 56).
IDH1 and IDH2 encode NADP+-dependent enzymes involved in citratemetabolism that localize to the cytosol and themitochondria, respectively. Mutations mainlyaffect residue R132 of IDH1 and residues R140and R172 of IDH2 and alter catalytic function.Whereas wild-type IDH proteins convertisocitrate to α-ketoglutarate, cancer-associatedIDH1 and IDH2 mutations confer a neomor-phic enzymatic activity that directly convertsα-ketoglutarate to 2-hydroxyglutarate (2HG)(57). 2HG, which is found at high levels incancers harboring IDH1 and IDH2 mutations,is thought to function as an oncometabolitethat can induce genome-wide alterations inhistone and DNA methylation via competitiveinhibition of α-ketoglutarate-dependent en-zymes. AML with IDH1 and IDH2 mutationsare characterized by a distinct pattern ofhypermethylation that is consistent with dis-ruption of TET2-mediated 5mC hydroxylation(42). Similarly, a reduction of IDH activityor an increase in intracellular 2HG interfereswith the function of histone demethylasesand causes increased H3K79 methylation andleukemia-associated HOXA gene expression(58).
EZH2
EZH2 is a member of the PRC2, along withEED, SUZ12, and RBBP4, that repressesgene expression through trimethylation ofH3K27me3 (59). EZH2 mutations in MDS and
other myeloid malignancies cause a loss of en-zymatic function (60, 61). Missense mutationscluster in a C-terminal SET domain, whichis required for methyltransferase activity,whereas various other mutations (missense,nonsense, splice site, insertion/deletions,and frameshift) affect other EZH2 domains,including the cysteine-rich and protein-protein(EED-binding or SUZ12-binding) interactiondomains. By contrast, the heterozygous EZH2mutations found in follicular lymphoma anddiffuse large B cell lymphoma occur predom-inantly at Y641 and confer altered enzymaticfunction, as reflected by increased H3K27trimethylation (62, 63). Disruption of PRC2 inmurine bone marrow, via inactivation of Ezh2,Eed, or Suz12, augments HSC activity; thisfinding is consistent with an early role for lossof EZH2 function in myeloid neoplasia andwith recent reports of rare mutations of PRC2components (EED and SUZ12) and associatedfactors (JARID2) in myeloid malignancies (64).The disparate biologic effects of EZH2 dysreg-ulation suggest that this gene’s dual functionas oncogene and tumor suppressor is contextdependent and determined by hematopoieticlineage and stage of differentiation.
EZH2 mutations occur in 6% of MDScases. This gene is located on the long armof chromosome 7 (7q), and mutations may beassociated with acquired uniparental disomyand, less commonly, 7q deletion (7, 60, 61, 65).EZH2 mutations are more prevalent in lower-risk MDS but are associated with reducedoverall survival, independently of other knownvariables (7). Despite their adverse prognosticimpact, however, EZH2 abnormalities areexceptionally rare in AML, which implicatesmechanisms other than progression to overtleukemia for their negative clinical effect.
ASXL1
ASXL1 is a homolog of the Drosophila ETP(Enhancer of trithorax and Polycomb) groupgene Additional sex combs (Asx). The ASXL1protein contains a C-terminal plant homeo-domain (PHD) finger and several nuclear
30 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
CDR: commondeleted region
receptor coregulator–binding (NR box) motifs.Many proteins that contain PHD fingers areproposed to function as epigenetic readersvia PHD-dependent binding to trimethy-lated lysine residues on histones. Asx and itsmurine homolog Asxl1 regulate homeoticgene expression during embryogenesis byactivating or repressing gene expression in acontext-dependent manner (66).
ASXL1 is among the most frequently mu-tated genes in myeloid neoplasms, includingMDS (10–20%), CMML (40%), AML (5–30%), and MPN (10%) (7, 67–70). The ASXL1gene is localized to 20q11 but falls outside thecommon deleted region (CDR) in MDS associ-ated with deletions in the long arm of chromo-some 20 [del(20q)]. ASXL1 mutations are morecommon in MDS with intermediate-risk cy-togenetics. By contrast, ASXL1 mutations arethree to five times more frequent in AML pa-tients who are older than 60 years, are mutuallyexclusive of mutations in NPM1 in this pop-ulation, and are rarely found in combinationwith FLT3 internal tandem duplications (69).
In a multivariable analysis, ASXL1 mu-tations in MDS are associated with reducedoverall survival and a shorter time to leukemictransformation, independently of existingclinical parameters (7, 70). In AML, the pres-ence of an ASXL1 mutation is also associatedwith reduced overall survival and furtherpredicts a lower rate of complete response toinitial therapy (69). Most ASXL1 mutationsare heterozygous frameshifts or prematurestop codons that are predicted to cause theformation of a truncated protein that lacks theC-terminal PHD finger and nearly all NR boxmotifs (7, 70). It is unknown whether a stableprotein product is expressed from the truncatedalleles and, if so, whether it directly mediatesa disease phenotype via distinct gain of func-tion or dominant-negative activity. Targeteddisruption of mouse Asxl1 results in abnormalhematopoiesis marked by progenitor defects inthe lymphoid and myeloid lineages, althoughthese mice do not exhibit an overt stem cell de-fect or morphologic features of dysplasia (71).
TP53
p53, which is encoded by the TP53 geneon chromosome 17p, is a tumor suppressorthat coordinates the response to diverse cellu-lar stresses, including oncogene activation andDNA damage. In response to these stimuli,p53 can induce cell-cycle arrest, activate DNA-repair pathways, and trigger apoptosis; thesefunctions are mediated largely by its transcrip-tion factor activity. TP53 is mutated or deletedin most human cancers, with an incidence ofgreater than 50% in certain epithelial malig-nancies, including lung and ovarian cancer. Theincidence of TP53 abnormalities among hema-tologic malignancies, however, is relatively lowat approximately 10–20% (72).
Loss-of-function somatic mutations in TP53are present in 4% to 14% of unselected MDScases (7, 73, 74) and at least 20% to 30% inMDS cases that arise after exposure to radia-tion or alkylating agents (75). TP53 mutationsare associated with advanced disease, whichis often marked by severe thrombocytopenia(<50,000), elevated blast count (≥5%), and/ora complex karyotype (7, 76). Nearly 80% of pa-tients with TP53 mutations are categorized inthe IPSS intermediate 2– and high-risk diseasegroups (7). Despite this association with high-risk clinical features, however, TP53 mutationsare still associated with reduced survival afteradjusting for IPSS risk group [hazard ratio (HR)for death = 2.5] (7).
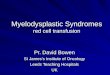
Among MDS patients with complex cyto-genetics, nearly half harbor somatic mutationsin TP53 (Figure 4a). Indeed, the presence ofa TP53 mutation in the context of complexcytogenetics is associated with significantlyreduced overall survival (0.58 versus 2.01 years;P < 0.001). Strikingly, in the absence of TP53mutation, the overall survival of patients witha complex karyotype is equivalent to that ofpatients with a noncomplex karyotype (2.01versus 2.91 years; P = 0.83) (Figure 4b) (7).Adverse prognosis in MDS cases with complexcytogenetics is also associated with the numberof chromosomal abnormalities; patients withmore than three lesions have reduced overall
www.annualreviews.org • Molecular Pathophysiology of MDS 31
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
0
0.2
0.4
0.6
0.8
1.0
0 2 4 6 8 10 12 14
Years
Prob
abili
ty o
f ove
rall
surv
ival Complex karyotype;
TP53 mutation present (n = 26)Complex karyotype;TP53 mutation absent (n = 31)Noncomplex karyotype;TP53 mutation absent (n = 368)
a
b
Karyotype
SF3B1SRSF2
NPM1
IDH1/2ETV6
TK pathwayEZH2ASXL1
TET2
U2AF1
TP53
DNMT3A
RUNX1
Complex karyotype;TP53 mutation present (n =Complex karyotype;TP53 mutation absent (n = Noncomplex karyotype;TP53 mutation absent (n =
Figure 4TP53 mutations are associated with a complex karyotype and reduced overallsurvival. (a) A subset of 439 patients with myelodysplastic syndrome (MDS) (7),including those with TP53 mutation (n = 33) or a complex karyotype (n =57). Each column represents one case, and mutations are represented ascolored bars. Specific karyotypes are color coded as in Figure 2. (b) Survival ofMDS patients with a complex karyotype, either with (n = 26; red line) orwithout (n = 31; blue line) TP53 mutations. Survival of MDS patientsassociated with a noncomplex karyotype and wild-type TP53 (n = 368) isrepresented as a gray line. TK pathway denotes mutations in genes that activatetyrosine kinase signaling. Modified from Reference 7 with permission.
survival compared with patients with threelesions (0.5 versus 1.3 years; P < 0.1) (2).
TRANSCRIPTION FACTORS
Hematopoietic differentiation is driven by theaction of transcription factors, which coordi-
nate dynamic programs of lineage-specific geneexpression (77). Transcription factors are com-monly mutated in hematologic malignanciesaffecting both lymphoid and myeloid lineages,including MDS. On the whole, these mutationsare thought to disrupt normal differentiationand cause aberrant HSC self-renewal, leadingto dominance of the mutated clone. RUNX1and ETV6 are the most commonly mutatedtranscription factor genes in de novo MDS.Somatic mutations in CEBPA are common inAML but are very rare in MDS. Germ-linemutations in GATA2 lead to familial MDS andAML, but somatic mutations are rare.
RUNX1
Among unselected MDS cases, RUNX1 mu-tations are identified in 10% to 20%; there arehigher rates in patients with prior exposure tochemotherapy or radiation and in those withmore advanced disease (7, 78, 79). RUNX1mutations are associated with severe thrombo-cytopenia (<50,000), increased bone marrowblasts (>5%), and decreased overall survivalindependent of IPSS (7, 80). Despite theseadverse prognostic features, RUNX1-mutatedMDS rarely have concurrent TP53 mutations(7, 81); instead, they are instead associated withactivation of the RTK-RAS pathway, possiblyvia mutation of FLT3, NRAS, or NF1 (81).RUNX1 mutations are further associated withdistinct cytogenetic features and more oftenhave chromosome 7 abnormalities (−7/7q−)in the setting of a normal chromosome 5.
RUNX1, also known as AML1 or CBFA2,is located on 21q22 and encodes a com-ponent of a transcriptional regulatory com-plex, core-binding factor (CBF). CBFs are het-erodimeric transcription factors composed ofa DNA-binding α-subunit (RUNX1, RUNX2,or RUNX3), which confers specificity, and anon-DNA-binding β-subunit (CBFB), whichregulates heterodimer stability and affin-ity for DNA. As part of the AML1/ETO(RUNX1/RUNX1T1) translocation, RUNX1was identified in t(8;21) CBF AML. Althoughthis translocation is rare outside of AML, point
32 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
mutations in RUNX1 are identified frequentlyin MDS, AML, and CMML.
The RUNX1 protein contains both an N-terminal Runt homology domain that mediatesDNA binding and a C-terminal transactivationdomain that is important for recruitment oftranscriptional cofactors. Pathogenic muta-tions in RUNX1 may be mono- or biallelic and,and as a rule, abolish transactivation of targetgenes (82). Missense mutations predominateand are commonly located in the Runt domain.These mutations cause the loss of DNAbinding with retention of cofactor interactions,which leads to dominant-negative functionalactivity. Frameshift mutations, by contrast, arefound throughout the gene but usually result inloss of the C-terminal transactivation domain(80).
Disease ontogeny influences the distribu-tion of mutations within RUNX1. Whereasmutations in de novo MDS/AML are evenlydistributed throughout the coding region,nearly all RUNX1 mutations in therapy-relatedMDS/AML are localized within the N-terminalRunt domain (80). These two classes of RUNX1mutation, N-terminal missense and C-terminalframeshift, display distinct biological behaviorswhen expressed in murine hematopoietic cells.Mice that are transplanted with bone marrowexpressing a Runt domain–mutated Runx1develop hepatosplenomegaly and myeloprolif-eration with increased bone marrow blasts andmultilineage dysplasia, and have a high rateof transformation to a leukemic phenotype. Incontrast, expression of a C-terminal frameshiftmutation causes leukopenia, marked ery-throid dysplasia, and a lower rate of leukemictransformation (83). Recent data implicatedomain-specific contributions to the patho-genesis of MDS. In a murine model, expressionof C-terminal mutant RUNX1 causes theaccumulation of DNA double-stranded breaksand represses Gadd45a expression, presumablyvia reduction of DNA-damage sensing (84).RUNX1 has been linked to histone modificationvia regulation of proteasomal degradation of theMLL histone methyltransferase. MDS/AML-associated N-terminal mutations cause the loss
of H3K4me3 marks within regulatory regionsof the RUNX1 target gene, PU.1 (85).
Germ-line mutations in RUNX1 cause fa-milial platelet disorder with propensity tomyeloid malignancy (FPD/AML). Individualswith this disease harbor monoallelic RUNX1mutations, most commonly localized to the N-terminal region, and have a clinical phenotypethat is characterized by reduced platelet num-ber and function (86). Approximately one-thirdof patients with FPD/AML develop AML, of-ten after long latency; the median onset of AMLis 33 years of age. Transformation to AML isoften associated with multiple somatic lesions,including acquisition of another mutation in thesecond RUNX1 allele (87).
ETV6
Somatic point mutations in ETV6 (also knownas TEL) have been identified in both MDSand AML at a frequency of 1% to 3%, andheterozygous deletions of the gene also occurrarely (88). In MDS ETV6 mutations predictpoor overall survival independently of the IPSSscore, whereas in AML they are associatedwith an intermediate risk (7, 89). ETV6 is atranscription factor that is expressed widelythroughout hematopoiesis and is required foradult HSC maintenance (90). ETV6 is thetarget of multiple translocations in diversehematologic malignancies, including ETV6-RUNX1 (TEL-AML1) in childhood precursorB cell acute lymphoblastic leukemia, ETV6-PDGFRB in CMML, and rarely ETV6-GOT1or ETV6-MDS2 in MDS (91).
ETV6 abnormalities are thought to con-tribute to disease pathogenesis by variousmechanisms. ETV6 contains a C-terminalDNA-binding (ETS) domain and an N-terminal homodimerization (SAM) domain.When paired with a tyrosine kinase gene,such as ETV6-JAK2, ETV6-PDGFRB, orETV6-FLT3, the ETV6 SAM domain mediateshomodimerization of the fusion oncoprotein,causing constitutive kinase activation andconsequent neoplastic proliferation (92).Fusions with RUNX1, EVI1, or MN1 alter
www.annualreviews.org • Molecular Pathophysiology of MDS 33
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
transcription factor activity and affect the bal-ance between differentiation and self-renewal(93, 94). In many ETV6-RUNX1 leukemias,the nonrearranged ETV6 allele is deleted orinactivated, which suggests that wild-typeETV6 has tumor-suppressor activity (95).
Point mutations in ETV6 are identifiedthroughout the gene and result in a varietyof abnormal full-length or truncated proteins.ETV6 mutations often involve the homodimer-ization or DNA-binding domains and generallycause abrogation of transcriptional repressorfunction (96). Acquired uniparental disomy ofchromosome 12p and loss of heterozygosity areuncommon in the context of ETV6 mutations,and the mutations are generally heterozygous(7, 96). Analysis of primary AML samples,however, reveals that one-third of cases showmarkedly reduced levels of ETV6 protein,despite normal mRNA levels and an absence ofmutation or deletion. Wild-type ETV6 may befurther inhibited by dominant-negative activityof the mutant ETV6 protein, as suggested byanimal models (96).
SIGNALING PATHWAYS
Normal hematopoiesis is critically dependenton appropriate spatiotemporal regulation ofgrowth factors and cytokines that activateintracellular kinase signaling cascades uponbinding to cell-surface receptors. Mutations inthese pathways can cause constitutive signalingor hyperresponsiveness to exogenous stimulisuch as growth factors. As a consequence,affected clones display enhanced proliferation,decreased apoptosis, or alteration of normaldevelopment and growth regulation. Amongmyeloid malignancies, recurrent gain-of-function mutations in receptor and nonrecep-tor tyrosine kinases commonly occur in diseasessuch as AML (FLT3, KIT ), chronic eosino-philic leukemia/hypereosinophilic syndrome(PDGFR, FGFR1), and MPN (MPL, JAK2).
In comparison to AML and MPN, RTKmutations are rare in MDS. For example,FLT3 abnormalities are at least 10-fold morecommon in de novo AML (30%) than in MDS
(2–3%) (97, 98). This small subset of MDS withFLT3 mutations presents as more advanceddisease, more often has a complex karyotypeand RAS mutations, and displays a shorter timeto leukemic transformation (97). Indeed, FLT3mutations are substantially more commonin sAML arising in the setting of preexistingMDS (12%) than in MDS as a whole (98).Similarly, the frequency of KIT mutations,although rare overall, is twice as high in sAMLthan in MDS (1.5% versus 0.7%) (98).
RAS Family
Some MDS cases bear activating mutationsin the RAS family of proto-oncogenes, whichencode small guanosine triphosphatases thatare activated by cell-surface receptors andregulate signaling cascades that are critical forcell growth and survival. NRAS mutations havebeen identified in approximately 10% of MDScases, whereas KRAS mutations are presentin only 1% to 2% (98). NRAS mutations arestrongly associated with severe thrombocy-topenia and increased bone marrow blasts (7),and acquisition of an NRAS mutation maypresage a transformation to acute leukemia(99). Although NRAS mutations are associatedwith inferior outcomes when considered alone(100), they do not provide significant prog-nostic value independent of the other knownclinical variables (7). Downstream members ofthe RAS/RAF/MEK pathway are rarely mu-tated in MDS. BRAF mutations occur in <1%of cases and have clinical implications that areprobably similar to those of NRAS mutations(7, 101).
CBL
CBL encodes a multidomain adaptor proteinwith E3 ubiquitin ligase activity that negativelyregulates RTK signaling by modulating re-ceptor degradation. CBL mutations have beenidentified in up to 15% of both CMML andjuvenile myelomonocytic leukemia ( JMML)patients but less than 3% of MDS and AMLcases (7, 102). CBL mutations are mutually
34 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
exclusive of other recurrent mutations insignaling pathway components, includingFLT3, KIT, NRAS/KRAS/BRAF, and JAK2(7, 103). Although rare in MDS and AML,they are associated with CBF abnormalities,namely t(8;21) and inversion of chromosome16 [inv(16)] (103).
Most CBL mutations affect the linker regionbetween the tyrosine kinase–binding domainand the RING finger domain, which causesreduced E3 ubiquitin ligase activity (104).Mutations are frequently biallelic and areassociated with acquired uniparental disomyof chromosome 11q, which suggests that thewild-type CBL allele has tumor-suppressoractivity (105). Furthermore, the most commonCBL mutations possess dominant-negativeproperties, as they inhibit the E3 ubiquitinligase activity of wild-type CBL and its paralogCBL-B and enhance cellular sensitivity tocytokines and growth factors, including TPO,SCF, FLT3-L, and IL-3 (104). This mecha-nism appears to underlie the myeloproliferativephenotype of Cbl-deficient mice, which de-pends on the presence of exogenous FLT3ligand.
JAK2
Activating mutations in JAK2, which mostcommonly lead to the substitution V617F,occur rarely in MDS but more commonly inMPN, including polycythemia vera (>95%),essential thrombocythemia (50%), and myelofi-brosis (60%). The clinical phenotype of thesemutations is mediated by exaggerated activa-tion of signaling pathways that are otherwiseregulated by hematopoietic growth factors,including erythropoietin, thrombopoietin, andgranulocyte colony-stimulating factor. Amongcases of RARS-T, approximately 50% possessthe JAK2V617F mutation (106) and 70% harborSF3B1 mutations (9). The presence of concur-rent JAK2V617F and SF3B1 mutations, which areindividually associated with myeloproliferativeand myelodysplastic features, respectively, pro-vides a plausible genetic basis for the compositeMDS/MPN phenotype of RARS-T.
Other Genes Involvedin Kinase Signaling
Mutations in other genes that are involved insignal transduction pathways occur at a low fre-quency in MDS. PTPN11, which encodes theSHP2 protein tyrosine phosphatase that reg-ulates growth factor–dependent proliferationand differentiation in hematopoietic progeni-tors, is mutated in 10% to 15% of JMML andin less than 1% of MDS (7, 107). ReducedSHP2 expression in CD34+ progenitors pro-motes proliferation and impairs myeloid anderythroid differentiation (108). Rare somaticmutations in GNAS also occur in MDS (<1%)(7). GNAS encodes the Gsα-subunit of a het-erotrimeric G protein–coupled receptor, andmutations in this gene are associated with al-teration of JAK/STAT signaling and are impli-cated in nonhematopoietic malignancies (109).
CYTOGENETICS
Acquired cytogenetic abnormalities are re-ported in approximately 40% to 50% of denovo MDS (2, 3, 5). Disease karyotype isuseful for the diagnosis of MDS as a marker ofclonality and is a powerful predictor of overalland leukemia-free survival that is incorporatedinto the IPSS score. The specific genes withincytogenetic lesions that contribute to diseasepathophysiology have been challenging toidentify, but the genetic dissection del(5q) hasbegun to elucidate the molecular consequencesof this heterozygous chromosomal deletion.
del(5q)
Interstitial deletions of chromosome 5q arethe most common chromosomal abnormalitiesin MDS; they are identified in 10% to 15%of patients (3, 91). Patients with del(5q) MDSare clinically heterogeneous and fall into twobroad categories on the basis of clinicopatho-logic features, prognosis, and response tospecific therapy. Although 5q deletions areuniformly hemizygous, sequencing and CGHanalysis have failed to reveal point mutations or
www.annualreviews.org • Molecular Pathophysiology of MDS 35
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
microdeletions of the retained 5q alleles (110),nor has copy-neutral loss of heterozygositybeen identified at 5q (4, 111). The absenceof homozygous genetic inactivation of geneswithin the 5q CDRs suggests that the patho-genesis of MDS with hemizygous 5q deletionmay be caused by haploinsufficiency or bysilencing of classical tumor suppressors byepigenetic mechanisms.
Some patients with del(5q) display an ag-gressive disease course marked by an increasedrisk of transformation to acute leukemia anda relatively short overall survival (112). ThisMDS subtype commonly arises in the context ofprior therapy with alkylating agents and/or ra-diation and is often accompanied by additionalcytogenetic abnormalities and TP53 mutation(75, 113). Indeed, patients with del(5q) inthe context of multiple other karyotype ab-normalities demonstrate a substantially lowerlikelihood of complete response to lenalido-mide therapy compared with patients whohave isolated del(5q) (3% versus 67%) (114).Beyond chromosomal complexity, factors asso-ciated with adverse prognosis include deletionof the extreme telomeric and centromeric re-gions of 5q and heterozygous mutations in the5q35 genes NPM1 or MAML1 (115). Studies ina mouse model implicate hemizygous deletionor mutation of NPM1 in MDS pathogenesis.In this model, NPM1 functions as a haploin-sufficient tumor suppressor in the developmentof multilineage hematopoietic neoplasms(116).
MDS patients in whom del(5q) is the solekaryotypic abnormality have a relatively favor-able prognosis (5). Included among this lower-risk subset are patients with the 5q− syndrome.This syndrome was initially described as aclonal hematopoietic disorder characterized bymacrocytic anemia, normal or elevated plateletcount, hypolobated micromegakaryocytes, andan isolated del(5q) on initial diagnostic evalua-tion (117). Bona fide 5q− syndrome has a lowbone marrow blast percentage (<5%), a female-to-male ratio of 2:1, and a relatively low risk oftransformation to AML compared with otherMDS subtypes (5–16% versus 30–45%).
A region that spans 1.5 Mb at 5q32-q33was defined as the CDR for the 5q− syndrome(118). A subset of genes within this region areexpressed at haploinsufficient levels in CD34+
cells of patients with del(5q) (119). Systematicfunctional screening of all candidate geneswithin the 5q33 CDR provided the first evi-dence for the importance of haploinsufficientgene expression in the pathogenesis of 5q−MDS (120). Ribosomal protein S14 (RPS14)haploinsufficiency appears to be principallyresponsible for the characteristic erythroidphenotype of the 5q− syndrome (120). Re-duced expression of RPS14 causes selectiveimpairment of erythropoiesis with relativepreservation of megakaryopoiesis. Forcedexpression of RPS14 in hematopoietic pro-genitors purified from patients with the 5q−syndrome rescues their erythropoietic defect.
RPS14 encodes a core ribosomal proteinthat is important for 18S precursor ribosomalRNA (pre-rRNA) processing and 40S riboso-mal subunit formation. Inherited heterozygousloss-of-function mutations in at least 10 differ-ent ribosomal protein genes, including RPS19and RPS24, cause Diamond–Blackfan anemia(DBA), a rare congenital syndrome character-ized by hypoplastic anemia and macrocytosis(121). In both DBA and del(5q) MDS, hap-loinsufficiency of ribosomal genes impairs pre-rRNA processing and ribosome biogenesis andactivates the p53 pathway (122, 123). Indeed,erythroid precursors display selective inductionof p53, activation of p53 target gene expres-sion, and cell-cycle arrest (123). Pharmacologicor genetic inactivation of p53 rescues the pro-genitor defect in mouse models of the 5q−syndrome (123, 124), which demonstrates themechanistic importance of p53 induction in thesetting of ribosomal protein haploinsufficiency.
An analysis of the repertoire of noncodingRNA species in bone marrow from MDS pa-tients identified several microRNAs (miRNAs)with dysregulated expression. Two in partic-ular, miR-145 and miR-146a, are abundantlyexpressed in normal hematopoietic progenitorpopulations, show specifically reduced expres-sion in del(5q) MDS, and are localized to 5q.
36 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
Depletion of both miR-145 and miR-146a inmurine HSPCs results in thrombocytosis andmegakaryocyte dysplasia, which are mediatedin part by upregulation of the miR-145 andmiR-146a target genes TIRAP and TRAF6and consequently increased IL-6 secretion(125). Further analysis suggested that miR-145normally acts via repression of the transcriptionfactor FLI1 to regulate megakaryocyte anderythroid differentiation. Coordinate loss ofmiR-145 and RPS14 in CD34+ progenitorscauses preferential megakaryocyte differentia-tion, reduced erythroid colony formation, andHSPC expansion, thereby recapitulating keyfeatures of the 5q− syndrome. Consistent withthis mechanism is the finding that patients withdel(5q) MDS and decreased miR-145 levelsshow reciprocally increased expression of FLI1.Forced reexpression of miR-145 in CD34+ cellspurified from MDS patients promoted normal-ization of the megakaryocyte/erythroid colonyratio in patients with hemizygous del(5q), butnot in patients with 5q diploidy (126).
Current evidence suggests that the clini-cal phenotype of the 5q− syndrome representsthe composite effects of multiple genes withinthe 5q33 CDR. Most patients, however, har-bor deletions of substantially larger regions of5q. As such, other genes localized to 5q out-side the CDRs probably contribute to the clin-ical and phenotypic heterogeneity of patientswith del(5q) MDS. APC, located on 5q23 anddeleted in the vast majority of del(5q) MDS,encodes a negative regulator of β-catenin sig-naling. Mouse models demonstrate that het-erozygous inactivation of Apc causes decreasedstem cell activity in secondary transplants and amyeloproliferative/MDS phenotype (127).
Lenalidomide has been approved by the USFood and Drug Administration for the treat-ment of low-risk MDS with del(5q). Amongthese patients, lenalidomide induces a com-plete cytogenetic response in 50% to 60%,while 55% to 70% achieve transfusion inde-pendence (128, 129). Even in patients withcomplete cytogenetic remission, however, thedel(5q) clone persists in CD34+CD38−CD90+
stem cells that may mediate eventual disease
progression (130). The presence of rare diseasesubclones with TP53 mutations in pretreatmentbiopsies is associated with relative resistance tolenalidomide and may predict a reduced dura-tion of treatment response (113, 131).
Monosomy 7; del(7q)
Chromosome 7 abnormalities, such as mono-somy 7 or interstitial deletion of chromosome7q, are present in approximately 10% of denovo MDS and nearly 50% of MDS thatarises after exposure to alkylating agents (3,132). When present as sole abnormalities,chromosome 7 lesions are associated withreduced overall survival compared to a normalkaryotype. Isolated monosomy 7 is associatedwith worse prognostic features than interstitialdel(7q) (2). CDRs at 7q22 and 7q32–34 havebeen delineated in an attempt to identify keytumor-suppressor genes (133). A murine modelwith conditional hematopoietic deletion of aregion syntenic to the 7q22 CDR did not have ahematopoietic phenotype (134). Homozygousdeletion of MLL5, a histone lysine methyltrans-ferase localized within the 7q22 CDR, resultsin altered HSC homeostasis and impairedrepopulating capacity (135). While somaticmutations in MLL5 have not been identifiedin myeloid neoplasms, reduced expression ofMLL5 is independently associated with adverseprognosis in AML. EZH2 is localized to 7q36,and EZH2 mutations can occur in the settingof 7q uniparental disomy. Deletions of 7q andsome cases of acquired uniparental disomy,however, are not associated with EZH2 muta-tions or do not include the EZH2 gene, whichindicates that one or more additional 7q genesare likely to be important drivers of MDS (60).
Trisomy 8
Trisomy 8 is the sole cytogenetic abnormalityin approximately 5% of MDS cases and is as-sociated with an intermediate prognostic riskand a median overall survival of 23 months (3,136). Gain of chromosome 8 appears to rep-resent a late event in MDS pathogenesis; it
www.annualreviews.org • Molecular Pathophysiology of MDS 37
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
occurs in myeloid-restricted progenitors andis absent from the CD34+CD38−CD90+ stemcell compartment that is thought to containthe disease-initiating clone (137). Hematopoi-etic progenitors that harbor trisomy 8 expresshigher levels of antiapoptotic genes and are re-sistant to apoptotic stimuli, which suggests apossible mechanism of clonal advantage (138).Patients with trisomy 8 MDS often demon-strate an oligoclonal expansion of CD8+ T cellsthat are reactive to aneuploid HSPCs and havea higher rate of hematologic response to im-munosuppressive therapy (139). Furthermore,patients with trisomy 8 MDS who respondto immunosuppressive therapy overexpressWilms tumor 1 (WT1) and generate a T cell an-titumor response against WT1 epitopes (140).
3q, i(17q)
Abnormalities that involve chromosome 3q,including inversions, translocations, and dele-tions, are identified rarely in MDS but havebeen integrated into the latest cytogeneticscoring system as “poor” risk due to theirassociation with short overall survival (2, 3).t(3q) and inv(3q) usually involve the MDS1and EVI1 locus (MECOM) at 3q26 and causeincreased expression of EVI1, which in turncauses increased proliferation and impaireddifferentiation of HSPCs (141). In a mousemodel, overexpression of the EVI1 transcrip-tion factor causes an MDS phenotype (142),at least in part by interfering with the functionof the hematopoietic transcription factorsRUNX1, GATA1, and PU.1 (91).
The isochromosome 17q [i(17q)] abnormal-ity confers intermediate cytogenetic risk andis associated with a distinctive myeloprolifera-tive/myelodysplastic phenotype characterizedby severe anemia, leukocytosis, pseudo–Pelger–Huet neutrophils, a hypercellular bonemarrow, megakaryocytic hyperplasia, and thepresence of micromegakaryocytes (143, 144).Although i(17q) is associated with the loss ofone TP53 allele, the remaining TP53 alleleis uniformly unmutated, which suggests that
additional genes on chromosome 17 may beimportant for disease pathogenesis (144).
del(20q), del(12p), del(11q), −Y
Patients with isolated del(20q) and del(12p) areconsidered to be in the same “good” cytogeneticrisk group as patients with a normal karyotype,with median overall survivals of 5 to 6 yearsand 6 to 9 years, respectively. Isolated −Y anddel(11q) fall within the most favorable “verygood” risk group and are associated with pro-longed overall and leukemia-free survival (2, 3).Among these abnormalities, del(20q) has beenthe most intensely studied, but within the CDR,no gene has been conclusively linked with MDSpathogenesis. The ASXL1 gene, mutated in10% to 20% of MDS, is localized to 20q11 butfalls just outside the del(20q) CDR. L3MBTL1,located within the CDR at 20q13, encodes aPolycomb protein and has been implicated ingenomic instability (145). The ETV6 gene, lo-cated at 12p13, and the CBL gene, located at11q23, are recurrently mutated in MDS and liewithin regions that are deleted in some cases ofMDS (103, 146).
CONCLUSION
The clinical heterogeneity of MDS reflectsthe diversity of molecular abnormalities thatdrive disease pathogenesis. Technologicaldevelopments have enabled the identificationof many new genetic lesions in MDS patientsand provided profound insights into diseasepathogenesis. The full impact of genetics onMDS, however, has not yet been fully realized.Molecular factors may soon be integrated intodiagnostic criteria and clinical managementalgorithms, as specific mutations distinguishdisease subtypes and provide prognostic infor-mation not captured by current risk assessmentmodels. For each individual patient, prognosisand therapeutic response will depend not onlyon features of a readily identified dominantclone but also on features of distinct geneticsubclones that coexist in the bone marrow.
38 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
At present, the diagnosis of MDS reliesheavily on accurate assessment of the presenceand extent of morphologic dysplasia in the bonemarrow. The range of dysplastic features iswide, and no single unifying finding is presentin the majority of cases (147). Interobserveragreement about dyshematopoietic features issometimes problematic, and many patients lackthe most distinctive pathologic features, suchas ring sideroblasts or an excess of myeloidblasts (148). Although morphologic evaluationremains the backbone of diagnostic pathology,the presence of characteristic mutations mayclarify the diagnosis of MDS in a patient withrefractory cytopenias and borderline morpho-logic features. Furthermore, sensitive molecu-lar testing of the peripheral blood may proveuseful either diagnostically or as a means tomonitor response to therapy, without the needfor a bone marrow biopsy.
Clinical management of MDS dependscritically on the reliable ascertainment of dis-ease prognosis. While minimally symptomatic
patients with low-risk disease may be observedexpectantly, patients with higher-risk diseaseare treated with disease-modifying medicaltherapies or with allogeneic stem cell trans-plantation, which remains the only potentiallycurative treatment. Optimal timing of trans-plant requires the balancing of disease-specificprognosis and the risk of transplant-relatedmorbidity and mortality.
MDS classification schemes and risk mod-els are likely to be improved by inclusion ofgenetic variables and, ultimately, reconfiguredinto subtypes with a common molecular basisand a more consistent clinical phenotype. Withthe identification of the full suite of mutationsthat are recurrently mutated in MDS, insightsinto disease biology and improved animal mod-els will hopefully accelerate the developmentof new therapeutic agents. In the future, clin-ical variables, pathologic features, and geneticinformation will be integrated for prospectiverisk stratification and the choice of specific ther-apies for the treatment of MDS patients.
SUMMARY POINTS
1. MDS is a clinically heterogeneous collection of clonal myeloid neoplasms whose patho-genesis is driven by diverse, somatically acquired genetic abnormalities.
2. Diagnosis and classification of MDS rely on accurate assessment of the presence andextent of morphologic dysplasia in the bone marrow. As molecular abnormalities arecharacterized more fully, genetic variables will be integrated into disease classificationschemes and risk models.
3. Chromosomal abnormalities are present in approximately 50% of de novo MDS;metaphase cytogenetic analysis is the only genetic test that is currently in routine clinicaluse. Investigators have defined 19 distinct cytogenetic categories that classify 5 prognosticsubgroups.
4. Somatic point mutations can be identified in more than 70% of MDS, including mostcases with a normal karyotype.
5. Point mutations are powerful predictors of clinical phenotype; they predict prognosisindependently of existing clinical variables.
6. Among myeloid neoplasms with morphologic dysplasia, mutations in genes that encodecomponents of the RNA splicing machinery are frequently identified and are mutuallyexclusive.
www.annualreviews.org • Molecular Pathophysiology of MDS 39
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
7. Mutations that affect epigenetic regulation of gene expression, including DNA methy-lation and posttranslational histone modification, are common in MDS.
8. Acquired TP53 mutations are associated with a consistent phenotype, including a poorprognosis independent of established clinicopathologic variables, a complex karyotype,high bone marrow blast percentage, and thrombocytopenia.
DISCLOSURE STATEMENT
The authors are not aware of any affiliations, memberships, funding, or financial holdings thatmight be perceived as affecting the objectivity of this review.
LITERATURE CITED
1. Brunning R, Orazi A, Germing U, Le Beau M, Porwit A, et al. 2008. Myelodysplastic syn-dromes/neoplasms, overview. See Ref. 151, pp. 88–93
2. Presents a largeanalysis of chromosomalabnormalities in MDSthat defines 19 distinctcytogenetic categoriesthat classify fiveprognostic subgroups.
2. Schanz J, Tuchler H, Sole F, Mallo M, Luno E, et al. 2012. New comprehensive cytogeneticscoring system for primary myelodysplastic syndromes (MDS) and oligoblastic acute myeloidleukemia after MDS derived from an international database merge. J. Clin. Oncol. 30:820–29
3. Haase D, Germing U, Schanz J, Pfeilstocker M, Nosslinger T, et al. 2007. New insights into theprognostic impact of the karyotype in MDS and correlation with subtypes: evidence from a core datasetof 2,124 patients. Blood 110:4385–95
4. Gondek LP, Tiu R, O’Keefe CL, Sekeres MA, Theil KS, Maciejewski JP. 2008. Chromosomal lesionsand uniparental disomy detected by SNP arrays in MDS, MDS/MPD, and MDS-derived AML. Blood111:1534–42
5. Greenberg P, Cox C, LeBeau MM, Fenaux P, Morel P, et al. 1997. International scoring system forevaluating prognosis in myelodysplastic syndromes. Blood 89:2079–88
6. Reports the spectrumof mutations that affectRNA splicing machineryin MDS. 6. Yoshida K, Sanada M, Shiraishi Y, Nowak D, Nagata Y, et al. 2011. Frequent pathway mutations
of splicing machinery in myelodysplasia. Nature 478:64–69
7. Demonstrates thatsomatic point mutations(TP53, EZH2, ETV6,RUNX1, ASXL1)predict poor prognosisin MDS.
7. Bejar R, Stevenson K, Abdel-Wahab O, Galili N, Nilsson B, et al. 2011. Clinical effect of pointmutations in myelodysplastic syndromes. N. Engl. J. Med. 364:2496–506
8. Bejar R, Stevenson KE, Caughey BA, Abdel-Wahab O, Steensma DP, et al. 2012. Validation of aprognostic model and the impact of mutations in patients with lower-risk myelodysplastic syndromes.J. Clin. Oncol. 30:3376–82
9. Reports that SF3B1mutations are stronglyassociated with the ringsideroblast morphology.
9. Papaemmanuil E, Cazzola M, Boultwood J, Malcovati L, Vyas P, et al. 2011. Somatic SF3B1mutation in myelodysplasia with ring sideroblasts. N. Engl. J. Med. 365:1384–95
10. Bacher U, Haferlach T, Schnittger S, Kreipe H, Kroger N. 2011. Recent advances in diagnosis, molecularpathology and therapy of chronic myelomonocytic leukaemia. Br. J. Haematol. 153:149–67
11. Graubert TA, Shen D, Ding L, Okeyo-Owuor T, Lunn CL, et al. 2012. Recurrent mutations in theU2AF1 splicing factor in myelodysplastic syndromes. Nat. Genet. 44:53–57
12. Pan Q, Shai O, Lee LJ, Frey BJ, Blencowe BJ. 2008. Deep surveying of alternative splicing complexityin the human transcriptome by high-throughput sequencing. Nat. Genet. 40:1413–15
13. Wang ET, Sandberg R, Luo S, Khrebtukova I, Zhang L, et al. 2008. Alternative isoform regulation inhuman tissue transcriptomes. Nature 456:470–76
14. David CJ, Manley JL. 2010. Alternative pre-mRNA splicing regulation in cancer: pathways and programsunhinged. Genes Dev. 24:2343–64
15. Will CL, Luhrmann R. 2011. Spliceosome structure and function. Cold Spring Harb. Perspect. Biol. 3:181–203
40 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
16. Malcovati L, Papaemmanuil E, Bowen DT, Boultwood J, Porta Della MG, et al. 2011. Clinical signif-icance of SF3B1 mutations in myelodysplastic syndromes and myelodysplastic/myeloproliferative neo-plasms. Blood 118:6239–46
17. Damm F, Thol F, Kosmider O, Kade S, Loffeld P, et al. 2011. SF3B1 mutations in myelodysplasticsyndromes: clinical associations and prognostic implications. Leukemia 26:1137–40
18. Patnaik MM, Lasho TL, Hodnefield JM, Knudson RA, Ketterling RP, et al. 2012. SF3B1 mutations areprevalent in myelodysplastic syndromes with ring sideroblasts but do not hold independent prognosticvalue. Blood 119:569–72
19. Maratheftis CI, Bolaraki PE, Giannouli S, Kapsogeorgou EK, Moutsopoulos HM, Voulgarelis M. 2006.Aberrant alternative splicing of interferon regulatory factor 1 (IRF-1) in myelodysplastic hematopoieticprogenitor cells. Leuk. Res. 30:1177–86
20. Caudill JS, Porcher JC, Steensma DP. 2008. Aberrant pre-mRNA splicing of a highly conserved cellcycle regulator, CDC25C, in myelodysplastic syndromes. Leuk. Lymphoma 49:989–93
21. Isono K, Mizutani-Koseki Y, Komori T, Schmidt-Zachmann MS, Koseki H. 2005. Mammalianpolycomb-mediated repression of Hox genes requires the essential spliceosomal protein Sf3b1. GenesDev. 19:536–41
22. Ball MP, Li JB, Gao Y, Lee J-H, LeProust EM, et al. 2009. Targeted and genome-scale strategies revealgene-body methylation signatures in human cells. Nat. Biotechnol. 27:361–68
23. Meissner A, Mikkelsen TS, Gu H, Wernig M, Hanna J, et al. 2008. Genome-scale DNA methylationmaps of pluripotent and differentiated cells. Nature 454:766–70
24. Ito S, Shen L, Dai Q, Wu SC, Collins LB, et al. 2011. Tet proteins can convert 5-methylcytosine to5-formylcytosine and 5-carboxylcytosine. Science 333:1300–3
25. Tahiliani M, Koh KP, Shen Y, Pastor WA, Bandukwala H, et al. 2009. Conversion of 5-methylcytosineto 5-hydroxymethylcytosine in mammalian DNA by MLL partner TET1. Science 324:930–35
26. Figueroa ME, Skrabanek L, Li Y, Jiemjit A, Fandy TE, et al. 2009. MDS and secondary AML displayunique patterns and abundance of aberrant DNA methylation. Blood 114:3448–58
27. Jiang Y, Dunbar A, Gondek LP, Mohan S, Rataul M, et al. 2009. Aberrant DNA methylation is adominant mechanism in MDS progression to AML. Blood 113:1315–25
28. Shen L, Kantarjian H, Guo Y, Lin E, Shan J, et al. 2010. DNA methylation predicts survival and responseto therapy in patients with myelodysplastic syndromes. J. Clin. Oncol. 28:605–13
29. Silverman LR, Demakos EP, Peterson BL, Kornblith AB, Holland JC, et al. 2002. Randomized controlledtrial of azacitidine in patients with the myelodysplastic syndrome: a study of the cancer and leukemiagroup B. J. Clin. Oncol. 20:2429–40
30. Fenaux P, Mufti GJ, Hellstrom-Lindberg E, Santini V, Finelli C, et al. 2009. Efficacy of azacitidine com-pared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes:a randomised, open-label, phase III study. Lancet Oncol. 10:223–32
31. Ley TJ, Ding L, Walter MJ, McLellan MD, Lamprecht T, et al. 2010. DNMT3A mutations in acutemyeloid leukemia. N. Engl. J. Med. 363:2424–33
32. Walter MJ, Ding L, Shen D, Shao J, Grillot M, et al. 2011. Recurrent DNMT3A mutations in patientswith myelodysplastic syndromes. Leukemia 2:1153–58
33. Thol F, Winschel C, Ludeking A, Yun H, Friesen I, et al. 2011. Rare occurrence of DNMT3A mutationsin myelodysplastic syndromes. Haematologica 96:1870–73
34. Abdel-Wahab O, Pardanani A, Rampal R, Lasho TL, Levine RL, Tefferi A. 2011. DNMT3A mutationalanalysis in primary myelofibrosis, chronic myelomonocytic leukemia and advanced phases of myelopro-liferative neoplasms. Leukemia 25:1219–20
35. Yan X-J, Xu J, Gu Z-H, Pan C-M, Lu G, et al. 2011. Exome sequencing identifies somatic mutations ofDNA methyltransferase gene DNMT3A in acute monocytic leukemia. Nat. Genet. 43:309–15
36. Challen GA, Sun D, Jeong M, Luo M, Jelinek J, et al. 2012. Dnmt3a is essential for hematopoietic stemcell differentiation. Nat. Genet. 44:23–31
37. Langemeijer SMC, Kuiper RP, Berends M, Knops R, Aslanyan MG, et al. 2009. Acquired mutations inTET2 are common in myelodysplastic syndromes. Nat. Genet. 41:838–42
38. Reports thatmutations in TET2 arecommon in myeloidneoplasms and presentin HSCs.38. Delhommeau F, Dupont S, Valle Della V, James C, Trannoy S, et al. 2009. Mutation in TET2
in myeloid cancers. N. Engl. J. Med. 360:2289–301
www.annualreviews.org • Molecular Pathophysiology of MDS 41
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
39. Kohlmann A, Grossmann V, Klein H-U, Schindela S, Weiss T, et al. 2010. Next-generation sequencingtechnology reveals a characteristic pattern of molecular mutations in 72.8% of chronic myelomonocyticleukemia by detecting frequent alterations in TET2, CBL, RAS, and RUNX1. J. Clin. Oncol. 28:3858–65
40. Abdel-Wahab O, Mullally A, Hedvat C, Garcia-Manero G, Patel J, et al. 2009. Genetic characterizationof TET1, TET2, and TET3 alterations in myeloid malignancies. Blood 114:144–47
41. Metzeler KH, Maharry K, Radmacher MD, Mrozek K, Margeson D, et al. 2011. TET2 mutationsimprove the new European LeukemiaNet risk classification of acute myeloid leukemia: a Cancer andLeukemia Group B study. J. Clin. Oncol. 29:1373–81
42. Figueroa ME, Abdel-Wahab O, Lu C, Ward PS, Patel J, et al. 2010. Leukemic IDH1 and IDH2mutations result in a hypermethylation phenotype, disrupt TET2 function, and impair hematopoieticdifferentiation. Cancer Cell 18:553–67
43. Kosmider O, Gelsi-Boyer V, Cheok M, Grabar S, Valle Della V, et al. 2009. TET2 mutation is anindependent favorable prognostic factor in myelodysplastic syndromes (MDSs). Blood 114:3285–91
44. Smith AE, Mohamedali AM, Kulasekararaj A, Lim Z, Gaken J, et al. 2010. Next-generation sequencingof the TET2 gene in 355 MDS and CMML patients reveals low-abundance mutant clones with earlyorigins, but indicates no definite prognostic value. Blood 116:3923–32
45. Ko M, Huang Y, Jankowska AM, Pape UJ, Tahiliani M, et al. 2010. Impaired hydroxylation of 5-methylcytosine in myeloid cancers with mutant TET2. Nature 468:839–43
46. Ko M, Bandukwala HS, An J, Lamperti ED, Thompson EC, et al. 2011. Ten-eleven-translocation 2(Tet2) negatively regulates homeostasis and differentiation of hematopoietic stem cells in mice. Proc.Natl. Acad. Sci. USA 108:14566–71
47. Shows that TET2mutations are present insome mature lymphoidneoplasms.
47. Quivoron C, Couronne L, Valle Della V, Lopez CK, Plo I, et al. 2011. Tet2 inactivation resultsin pleiotropic hematopoietic abnormalities in mouse and is a recurrent event during humanlymphomagenesis. Cancer Cell 20:25–38
48. Wu H, D’Alessio AC, Ito S, Wang Z, Cui K, et al. 2011. Genome-wide analysis of 5-hydroxymethylcytosine distribution reveals its dual function in transcriptional regulation in mouse em-bryonic stem cells. Genes Dev. 25:679–84
49. He Y-F, Li B-Z, Li Z, Liu P, Wang Y, et al. 2011. Tet-mediated formation of 5-carboxylcytosine andits excision by TDG in mammalian DNA. Science 333:1303–7
50. Li Z, Cai X, Cai C-L, Wang J, Zhang W, et al. 2011. Deletion of Tet2 in mice leads to dysregulatedhematopoietic stem cells and subsequent development of myeloid malignancies. Blood 118:4509–18
51. Moran-Crusio K, Reavie L, Shih A, Abdel-Wahab O, Ndiaye-Lobry D, et al. 2011. Tet2 loss leads toincreased hematopoietic stem cell self-renewal and myeloid transformation. Cancer Cell 20:11–24
52. Viguie F, Aboura A, Bouscary D, Ramond S, Delmer A, et al. 2005. Common 4q24 deletion in four casesof hematopoietic malignancy: early stem cell involvement? Leukemia 19:1411–15
53. Mardis ER, Ding L, Dooling DJ, Larson DE, McLellan MD, et al. 2009. Recurring mutations found bysequencing an acute myeloid leukemia genome. N. Engl. J. Med. 361:1058–66
54. Paschka P, Schlenk RF, Gaidzik VI, Habdank M, Kronke J, et al. 2010. IDH1 and IDH2 mutations arefrequent genetic alterations in acute myeloid leukemia and confer adverse prognosis in cytogeneticallynormal acute myeloid leukemia with NPM1 mutation without FLT3 internal tandem duplication. J. Clin.Oncol. 28:3636–43
55. Thol F, Weissinger EM, Krauter J, Wagner K, Damm F, et al. 2010. IDH1 mutations in patients withmyelodysplastic syndromes are associated with an unfavorable prognosis. Haematologica 95:1668–74
56. Patnaik MM, Hanson CA, Hodnefield JM, Lasho TL, Finke CM, et al. 2012. Differential prognosticeffect of IDH1 versus IDH2 mutations in myelodysplastic syndromes: a Mayo Clinic study of 277 patients.Leukemia 26:101–5
57. Ward PS, Cross JR, Lu C, Weigert O, Abel-Wahab O, et al. 2011. Identification of additional IDHmutations associated with oncometabolite R(−)-2-hydroxyglutarate production. Oncogene 31:3491–98
58. Xu W, Yang H, Liu Y, Yang Y, Wang P, et al. 2011. Oncometabolite 2-hydroxyglutarate is a competitiveinhibitor of α-ketoglutarate-dependent dioxygenases. Cancer Cell 19:17–30
59. Beisel C, Paro R. 2011. Silencing chromatin: comparing modes and mechanisms. Nat. Rev. Genet. 12:123–35
42 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
60. Ernst T, Chase AJ, Score J, Hidalgo-Curtis CE, Bryant C, et al. 2010. Inactivating mutations of thehistone methyltransferase gene EZH2 in myeloid disorders. Nat. Genet. 42:722–26
61. Makishima H, Jankowska AM, Tiu RV, Szpurka H, Sugimoto Y, et al. 2010. Novel homo- and hemizy-gous mutations in EZH2 in myeloid malignancies. Leukemia 24:1799–804
62. Morin RD, Johnson NA, Severson TM, Mungall AJ, An J, et al. 2010. Somatic mutations altering EZH2(Tyr641) in follicular and diffuse large B cell lymphomas of germinal-center origin. Nat. Genet. 42:181–85
63. Yap DB, Chu J, Berg T, Schapira M, Cheng S-WG, et al. 2011. Somatic mutations at EZH2 Y641act dominantly through a mechanism of selectively altered PRC2 catalytic activity to increase H3K27trimethylation. Blood 117:2451–59
64. Score J, Hidalgo-Curtis C, Jones AV, Winkelmann N, Skinner A, et al. 2012. Inactivation of poly-comb repressive complex 2 components in myeloproliferative and myelodysplastic/myeloproliferativeneoplasms. Blood 119:1208–13
65. Nikoloski G, Langemeijer SMC, Kuiper RP, Knops R, Massop M, et al. 2010. Somatic mutations of thehistone methyltransferase gene EZH2 in myelodysplastic syndromes. Nat. Genet. 42:665–67
66. Fisher CL, Lee I, Bloyer S, Bozza S, Chevalier J, et al. 2010. Additional sex combs–like 1 belongs tothe enhancer of trithorax and polycomb group and genetically interacts with Cbx2 in mice. Dev. Biol.337:9–15
67. Boultwood J, Perry J, Pellagatti A, Fernandez-Mercado M, Fernandez-Santamaria C, et al. 2010. Fre-quent mutation of the polycomb-associated gene ASXL1 in the myelodysplastic syndromes and in acutemyeloid leukemia. Leukemia 24:1062–65
68. Gelsi-Boyer V, Trouplin V, Roquain J, Adelaıde J, Carbuccia N, et al. 2010. ASXL1 mutation is associatedwith poor prognosis and acute transformation in chronic myelomonocytic leukaemia. Br. J. Haematol.151:365–75
69. Metzeler KH, Becker H, Maharry K, Radmacher MD, Kohlschmidt J, et al. 2011. ASXL1 mutationsidentify a high-risk subgroup of older patients with primary cytogenetically normal AML within theELN favorable genetic category. Blood 118:6920–29
70. Thol F, Friesen I, Damm F, Yun H, Weissinger EM, et al. 2011. Prognostic significance of ASXL1mutations in patients with myelodysplastic syndromes. J. Clin. Oncol. 29:2499–506
71. Fisher CL, Pineault N, Brookes C, Helgason CD, Ohta H, et al. 2010. Loss-of-function additional sexcombs–like 1 mutations disrupt hematopoiesis but do not cause severe myelodysplasia or leukemia. Blood115:38–46
72. Peller S, Rotter V. 2003. TP53 in hematological cancer: low incidence of mutations with significantclinical relevance. Hum. Mutat. 21:277–84
73. Wattel E, Preudhomme C, Hecquet B, Vanrumbeke M, Quesnel B, et al. 1994. p53 mutations are associ-ated with resistance to chemotherapy and short survival in hematologic malignancies. Blood 84:3148–57
74. Kita-Sasai Y, Horiike S, Misawa S, Kaneko H, Kobayashi M, et al. 2001. International prognostic scoringsystem and TP53 mutations are independent prognostic indicators for patients with myelodysplasticsyndrome. Br. J. Haematol. 115:309–12
75. Christiansen DH, Andersen MK, Pedersen-Bjergaard J. 2001. Mutations with loss of heterozygosityof p53 are common in therapy-related myelodysplasia and acute myeloid leukemia after exposure toalkylating agents and significantly associated with deletion or loss of 5q, a complex karyotype, and a poorprognosis. J. Clin. Oncol. 19:1405–13
76. Kaneko H, Misawa S, Horiike S, Nakai H, Kashima K. 1995. TP53 mutations emerge at early phase ofmyelodysplastic syndrome and are associated with complex chromosomal abnormalities. Blood 85:2189–93
77. Novershtern N, Subramanian A, Lawton LN, Mak RH, Haining WN, et al. 2011. Densely intercon-nected transcriptional circuits control cell states in human hematopoiesis. Cell 144:296–309
78. Steensma DP, Gibbons RJ, Mesa RA, Tefferi A, Higgs DR. 2005. Somatic point mutations inRUNX1/CBFA2/AML1 are common in high-risk myelodysplastic syndrome, but not in myelofibrosiswith myeloid metaplasia. Eur. J. Haematol. 74:47–53
79. Chen C-Y, Lin L-I, Tang J-L, Ko B-S, Tsay W, et al. 2007. RUNX1 gene mutation in primary myelodys-plastic syndrome—the mutation can be detected early at diagnosis or acquired during disease progressionand is associated with poor outcome. Br. J. Haematol. 139:405–14
www.annualreviews.org • Molecular Pathophysiology of MDS 43
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
80. Harada H, Harada Y, Niimi H, Kyo T, Kimura A, Inaba T. 2004. High incidence of somatic mutationsin the AML1/RUNX1 gene in myelodysplastic syndrome and low blast percentage myeloid leukemiawith myelodysplasia. Blood 103:2316–24
81. Niimi H, Harada H, Harada Y, Ding Y, Imagawa J, et al. 2006. Hyperactivation of the RAS signalingpathway in myelodysplastic syndrome with AML1/RUNX1 point mutations. Leukemia 20:635–44
82. Matheny CJ, Speck ME, Cushing PR, Zhou Y, Corpora T, et al. 2007. Disease mutations in RUNX1and RUNX2 create nonfunctional, dominant-negative, or hypomorphic alleles. EMBO J. 26:1163–75
83. Watanabe-Okochi N, Kitaura J, Ono R, Harada H, Harada Y, et al. 2008. AML1 mutations inducedMDS and MDS/AML in a mouse BMT model. Blood 111:4297–308
84. Satoh Y, Matsumura I, Tanaka H, Harada H, Harada Y, et al. 2012. C-terminal mutation of RUNX1attenuates the DNA-damage repair response in hematopoietic stem cells. Leukemia 26:303–11
85. Huang G, Zhao X, Wang L, Elf S, Xu H, et al. 2011. The ability of MLL to bind RUNX1 and methylateH3K4 at PU.1 regulatory regions is impaired by MDS/AML-associated RUNX1/AML1 mutations. Blood118:6544–52
86. Ho CY, Otterud B, Legare RD, Varvil T, Saxena R, et al. 1996. Linkage of a familial platelet disorder witha propensity to develop myeloid malignancies to human chromosome 21q22.1–22.2. Blood 87:5218–24
87. Preudhomme C, Renneville A, Bourdon V, Philippe N, Roche-Lestienne C, et al. 2009. High frequencyof RUNX1 biallelic alteration in acute myeloid leukemia secondary to familial platelet disorder. Blood113:5583–87
88. Akagi T, Ogawa S, Dugas M, Kawamata N, Yamamoto G, et al. 2009. Frequent genomic abnormalitiesin acute myeloid leukemia/myelodysplastic syndrome with normal karyotype. Haematologica 94:213–23
89. Haferlach C, Bacher U, Schnittger S, Alpermann T, Zenger M, et al. 2012. ETV6 rearrangementsare recurrent in myeloid malignancies and are frequently associated with other genetic events. GenesChromosomes Cancer 51:328–37
90. Hock H, Meade E, Medeiros S, Schindler JW, Valk PJM, et al. 2004. Tel/Etv6 is an essential andselective regulator of adult hematopoietic stem cell survival. Genes Dev. 18:2336–41
91. Bejar R, Levine R, Ebert BL. 2011. Unraveling the molecular pathophysiology of myelodysplastic syn-dromes. J. Clin. Oncol. 29:504–15
92. Vu HA, Xinh PT, Masuda M, Motoji T, Toyoda A, et al. 2006. FLT3 is fused to ETV6 in a myelopro-liferative disorder with hypereosinophilia and a t(12;13)(p13;q12) translocation. Leukemia 20:1414–21
93. Schindler JW, Van Buren D, Foudi A, Krejci O, Qin J, et al. 2009. TEL-AML1 corrupts hematopoieticstem cells to persist in the bone marrow and initiate leukemia. Cell Stem Cell 5:43–53
94. Lierman E, Cools J. 2007. ETV6 and PDGFRB: a license to fuse. Haematologica 92:145–4795. Romana S, Poirel H, Leconiat M, Flexor M, Mauchauffe M, et al. 1995. High frequency of t(12;21) in
childhood B-lineage acute lymphoblastic leukemia. Blood 86:4263–6996. Barjesteh van Waalwijk van Doorn–Khosrovani S, Spensberger D, de Knegt Y, Tang M, Lowenberg B,
Delwel R. 2005. Somatic heterozygous mutations in ETV6 (TEL) and frequent absence of ETV6 proteinin acute myeloid leukemia. Oncogene 24:4129–37
97. Bains A, Luthra R, Medeiros LJ, Zuo Z. 2011. FLT3 and NPM1 mutations in myelodysplastic syndromes.Am. J. Clin. Pathol. 135:62–69
98. Bacher U, Haferlach T, Kern W, Haferlach C, Schnittger S. 2007. A comparative study of molecularmutations in 381 patients with myelodysplastic syndrome and in 4,130 patients with acute myeloidleukemia. Haematologica 92:744–52
99. van Kamp H, de Pijper C, Verlaan–de Vries M, Bos JL, Leeksma CH, et al. 1992. Longitudinal analysisof point mutations of the N-ras proto-oncogene in patients with myelodysplasia using archived bloodsmears. Blood 79:1266–70
100. Constantinidou M, Chalevelakis G, Economopoulos T, Koffa M, Liloglou T, et al. 1997. Codon 12ras mutations in patients with myelodysplastic syndrome: incidence and prognostic value. Ann. Hematol.74:11–14
101. Christiansen DH, Andersen MK, Desta F, Pedersen-Bjergaard J. 2005. Mutations of genes in the receptortyrosine kinase (RTK)/RAS-BRAF signal transduction pathway in therapy-related myelodysplasia andacute myeloid leukemia. Leukemia 19:2232–40
44 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
102. Loh ML, Sakai DS, Flotho C, Kang M, Fliegauf M, et al. 2009. Mutations in CBL occur frequently injuvenile myelomonocytic leukemia. Blood 114:1859–63
103. Reindl C, Quentmeier H, Petropoulos K, Greif PA, Benthaus T, et al. 2009. CBL exon 8/9 mu-tants activate the FLT3 pathway and cluster in core binding factor/11q deletion acute myeloidleukemia/myelodysplastic syndrome subtypes. Clin. Cancer Res. 15:2238–47
104. Sanada M, Suzuki T, Shih L-Y, Otsu M, Kato M, et al. 2009. Gain-of-function of mutated C-CBLtumour suppressor in myeloid neoplasms. Nature 460:904–8
105. Dunbar AJ, Gondek LP, O’Keefe CL, Makishima H, Rataul MS, et al. 2008. 250K single nucleotidepolymorphism array karyotyping identifies acquired uniparental disomy and homozygous mutations,including novel missense substitutions of c-Cbl, in myeloid malignancies. Cancer Res. 68:10349–57
106. Malcovati L, Porta Della MG, Pietra D, Boveri E, Pellagatti A, et al. 2009. Molecular and clinical featuresof refractory anemia with ringed sideroblasts associated with marked thrombocytosis. Blood 114:3538–45
107. Loh ML, Martinelli S, Cordeddu V, Reynolds MG, Vattikuti S, et al. 2005. Acquired PTPN11 mutationsoccur rarely in adult patients with myelodysplastic syndromes and chronic myelomonocytic leukemia.Leuk. Res. 29:459–62
108. Li L, Modi H, McDonald T, Rossi J, Yee J-K, Bhatia R. 2011. A critical role for SHP2 in STAT5activation and growth factor–mediated proliferation, survival, and differentiation of human CD34+
cells. Blood 118:1504–15109. Furukawa T, Kuboki Y, Tanji E, Yoshida S, Hatori T, et al. 2011. Whole-exome sequencing uncovers
frequent GNAS mutations in intraductal papillary mucinous neoplasms of the pancreas. Sci. Rep. 1:161110. Graubert TA, Payton MA, Shao J, Walgren RA, Monahan RS, et al. 2009. Integrated genomic anal-
ysis implicates haploinsufficiency of multiple chromosome 5q31.2 genes in de novo myelodysplasticsyndromes pathogenesis. PLoS ONE 4:e4583
111. Heinrichs S, Kulkarni RV, Bueso-Ramos CE, Levine RL, Loh ML, et al. 2009. Accurate detection ofuniparental disomy and microdeletions by SNP array analysis in myelodysplastic syndromes with normalcytogenetics. Leukemia 23:1605–13
112. Kantarjian H, OBrien S, Ravandi F, Borthakur G, Faderl S, et al. 2009. The heterogeneous prognosisof patients with myelodysplastic syndrome and chromosome 5 abnormalities: How does it relate to theoriginal lenalidomide experience in MDS? Cancer 115:5202–9
113. Mollgard L, Saft L, Treppendahl MB, Dybedal I, Nørgaard JM, et al. 2011. Clinical effect of increasingdoses of lenalidomide in high-risk myelodysplastic syndrome and acute myeloid leukemia with chromo-some 5 abnormalities. Haematologica 96:963–71
114. Ades L, Boehrer S, Prebet T, Beyne-Rauzy O, Legros L, et al. 2009. Efficacy and safety of lenalidomidein intermediate-2 or high-risk myelodysplastic syndromes with 5q deletion: results of a phase 2 study.Blood 113:3947–52
115. Jerez A, Gondek LP, Jankowska AM, Makishima H, Przychodzen B, et al. 2012. Topography, clinical,and genomic correlates of 5q myeloid malignancies revisited. J. Clin. Oncol. 30:1343–49
116. Sportoletti P, Grisendi S, Majid SM, Cheng K, Clohessy JG, et al. 2008. Npm1 is a haploinsufficientsuppressor of myeloid and lymphoid malignancies in the mouse. Blood 111:3859–62
117. Van den Berghe H, Cassiman JJ, David G, Fryns JP, Michaux JL, Sokal G. 1974. Distinct haematologicaldisorder with deletion of long arm of no. 5 chromosome. Nature 251:437–38
118. Boultwood J, Fidler C, Strickson AJ, Watkins F, Gama S, et al. 2002. Narrowing and genomic annotationof the commonly deleted region of the 5q− syndrome. Blood 99:4638–41
119. Boultwood J, Pellagatti A, Cattan H, Lawrie CH, Giagounidis A, et al. 2007. Gene expression profilingof CD34+ cells in patients with the 5q− syndrome. Br. J. Haematol. 139:578–89
120. Performs afunctional analysis ofthe 5q− syndrome CDRthat implicates RPS14haploinsufficiency as acontributor to theclinical phenotype.
120. Ebert BL, Pretz J, Bosco J, Chang CY, Tamayo P, et al. 2008. Identification of RPS14 as a 5q−syndrome gene by RNA interference screen. Nature 451:335–39
121. Narla A, Ebert BL. 2010. Ribosomopathies: human disorders of ribosome dysfunction. Blood 115:3196–205
122. McGowan KA, Pang WW, Bhardwaj R, Perez MG, Pluvinage JV, et al. 2011. Reduced ribosomal proteingene dosage and p53 activation in low-risk myelodysplastic syndrome. Blood 118:3622–33
123. Dutt S, Narla A, Lin K, Mullally A, Abayasekara N, et al. 2011. Haploinsufficiency for ribosomal proteingenes causes selective activation of p53 in human erythroid progenitor cells. Blood 117:2567–76
www.annualreviews.org • Molecular Pathophysiology of MDS 45
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
124. Barlow JL, Drynan LF, Hewett DR, Holmes LR, Lorenzo-Abalde S, et al. 2010. A p53-dependentmechanism underlies macrocytic anemia in a mouse model of human 5q− syndrome. Nat. Med. 16:59–66
125. Starczynowski DT, Kuchenbauer F, Argiropoulos B, Sung S, Morin R, et al. 2010. Identification ofmiR-145 and miR-146a as mediators of the 5q− syndrome phenotype. Nat. Med. 16:49–58
126. Kumar MS, Narla A, Nonami A, Mullally A, Dimitrova N, et al. 2011. Coordinate loss of a microRNAand protein-coding gene cooperate in the pathogenesis of 5q− syndrome. Blood 118:4666–73
127. Lane SW, Sykes SM, Al-Shahrour F, Shterental S, Paktinat M, et al. 2010. The Apcmin mouse has alteredhematopoietic stem cell function and provides a model for MPD/MDS. Blood 115:3489–97
128. List A, Dewald G, Bennett J, Giagounidis A, Raza A, et al. 2006. Lenalidomide in the myelodysplasticsyndrome with chromosome 5q− deletion. N. Engl. J. Med. 355:1456–65
129. Fenaux P, Giagounidis A, Selleslag D, Beyne-Rauzy O, Mufti G, et al. 2011. A randomized phase 3 studyof lenalidomide versus placebo in RBC transfusion-dependent patients with low-/intermediate-1-riskmyelodysplastic syndromes with del5q. Blood 118:3765–76
130. Tehranchi R, Woll PS, Anderson K, Buza-Vidas N, Mizukami T, et al. 2010. Persistent malignant stemcells in del(5q) myelodysplasia in remission. N. Engl. J. Med. 363:1025–37
131. Jadersten M, Saft L, Pellagatti A, Gohring G, Wainscoat JS, et al. 2009. Clonal heterogeneity in the5q− syndrome: p53 expressing progenitors prevail during lenalidomide treatment and expand at diseaseprogression. Haematologica 94:1762–66
132. Christiansen DH, Andersen MK, Pedersen-Bjergaard J. 2004. Mutations of AML1 are common intherapy-related myelodysplasia following therapy with alkylating agents and are significantly associ-ated with deletion or loss of chromosome arm 7q and with subsequent leukemic transformation. Blood104:1474–81
133. Le Beau MM, Espinosa R, Davis EM, Eisenbart JD, Larson RA, Green ED. 1996. Cytogenetic andmolecular delineation of a region of chromosome 7 commonly deleted in malignant myeloid diseases.Blood 88:1930–35
134. Wong JCY, Zhang Y, Lieuw KH, Tran MT, Forgo E, et al. 2010. Use of chromosome engineering tomodel a segmental deletion of chromosome band 7q22 found in myeloid malignancies. Blood 115:4524–32
135. Heuser M, Yap DB, Leung M, de Algara TR, Tafech A, et al. 2009. Loss of MLL5 results in pleiotropichematopoietic defects, reduced neutrophil immune function, and extreme sensitivity to DNA demethy-lation. Blood 113:1432–43
136. Schanz J, Steidl C, Fonatsch C, Pfeilstocker M, Nosslinger T, et al. 2011. Coalesced multicentric analysisof 2,351 patients with myelodysplastic syndromes indicates an underestimation of poor-risk cytogeneticsof myelodysplastic syndromes in the international prognostic scoring system. J. Clin. Oncol. 29:1963–70
137. Nilsson L, Astrand-Grundstrom I, Anderson K, Arvidsson I, Hokland P, et al. 2002. Involvement andfunctional impairment of the CD34+CD38−Thy-1+ hematopoietic stem cell pool in myelodysplasticsyndromes with trisomy 8. Blood 100:259–67
138. Sloand EM, Pfannes L, Chen G, Shah S, Solomou EE, et al. 2007. CD34 cells from patients with trisomy8 myelodysplastic syndrome (MDS) express early apoptotic markers but avoid programmed cell deathby up-regulation of antiapoptotic proteins. Blood 109:2399–405
139. Sloand EM, Mainwaring L, Fuhrer M, Ramkissoon S, Risitano AM, et al. 2005. Preferential suppressionof trisomy 8 compared with normal hematopoietic cell growth by autologous lymphocytes in patientswith trisomy 8 myelodysplastic syndrome. Blood 106:841–51
140. Sloand EM, Melenhorst JJ, Tucker ZCG, Pfannes L, Brenchley JM, et al. 2011. T cell immune responsesto Wilms tumor 1 protein in myelodysplasia responsive to immunosuppressive therapy. Blood 117:2691–99
141. Nucifora G, Laricchia-Robbio L, Senyuk V. 2006. EVI1 and hematopoietic disorders: history and per-spectives. Gene 368:1–11
142. Buonamici S, Li D, Chi Y, Zhao R, Wang X, et al. 2004. EVI1 induces myelodysplastic syndrome inmice. J. Clin. Investig. 114:713–19
143. McClure RF, Dewald GW, Hoyer JD, Hanson CA. 1999. Isolated isochromosome 17q: a distinct typeof mixed myeloproliferative disorder/myelodysplastic syndrome with an aggressive clinical course. Br.J. Haematol. 106:445–54
46 Lindsley · Ebert
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08CH02-Ebert ARI 13 December 2012 18:55
144. Kanagal-Shamanna R, Bueso-Ramos CE, Barkoh B, Lu G, Wang S, et al. 2012. Myeloid neoplasmswith isolated isochromosome 17q represent a clinicopathologic entity associated with myelodysplas-tic/myeloproliferative features, a high risk of leukemic transformation, and wild-type TP53. Cancer118:2879–88
145. MacGrogan D, Kalakonda N, Alvarez S, Scandura JM, Boccuni P, et al. 2004. Structural integrity andexpression of the L3MBTL gene in normal and malignant hematopoietic cells. Genes Chromosomes Cancer41:203–13
146. Streubel B, Sauerland C, Heil G, Freund M, Bartels H, et al. 1998. Correlation of cytogenetic, molecularcytogenetic, and clinical findings in 59 patients with ANLL or MDS and abnormalities of the short armof chromosome 12. Br. J. Haematol. 100:521–33
147. Germing U, Strupp C, Giagounidis A, Haas R, Gattermann N, et al. 2012. Evaluation of dysplasiathrough detailed cytomorphology in 3,156 patients from the Dusseldorf Registry on myelodysplasticsyndromes. Leuk. Res. 36:727–34
148. Orazi A, Czader MB. 2009. Myelodysplastic syndromes. Am. J. Clin. Pathol. 132:290–305149. Vardiman J, Bennett J, Bain B, Baumann I, Thiele J, Orazi A. 2008. Myelodysplastic/myeloproliferative
neoplasm, unclassifiable. See Ref. 151, pp. 85–86150. Orazi A, Bennett J, Germing U, Brunning R, Bain B, Thiele J. 2008. Chronic myelomonocytic leukemia.
See Ref. 151, pp. 76–79151. Swerdlow SH, Carrigo E, Harris NL, Jaffe ES, Pilori SA, et al., eds. 2008. WHO Classification of Tumours
of Haematopoietic and Lymphoid Tissues. Lyon, Fr.: IARC
www.annualreviews.org • Molecular Pathophysiology of MDS 47
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08-FrontMatter ARI 17 December 2012 9:46
Annual Review ofPathology:Mechanisms ofDisease
Volume 8, 2013Contents
Pathogenesis of Langerhans Cell HistiocytosisGayane Badalian-Very, Jo-Anne Vergilio, Mark Fleming,
and Barrett J. Rollins � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 1
Molecular Pathophysiology of Myelodysplastic SyndromesR. Coleman Lindsley and Benjamin L. Ebert � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �21
The Role of Telomere Biology in CancerLifeng Xu, Shang Li, and Bradley A. Stohr � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �49
Chromosome Translocation, B Cell Lymphoma,and Activation-Induced Cytidine DeaminaseDavide F. Robbiani and Michel C. Nussenzweig � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �79
Autophagy as a Stress-Response and Quality-Control Mechanism:Implications for Cell Injury and Human DiseaseLyndsay Murrow and Jayanta Debnath � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 105
Pathogenesis of Antineutrophil Cytoplasmic Autoantibody–AssociatedSmall-Vessel VasculitisJ. Charles Jennette, Ronald J. Falk, Peiqi Hu, and Hong Xiao � � � � � � � � � � � � � � � � � � � � � � � � � 139
Molecular Basis of Asbestos-Induced Lung DiseaseGang Liu, Paul Cheresh, and David W. Kamp � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 161
Progressive Multifocal Leukoencephalopathy: Why Grayand White MatterSarah Gheuens, Christian Wuthrich, and Igor J. Koralnik � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 189
IgA Nephropathy: Molecular Mechanisms of the DiseaseJiri Mestecky, Milan Raska, Bruce A. Julian, Ali G. Gharavi,
Matthew B. Renfrow, Zina Moldoveanu, Lea Novak, Karel Matousovic,and Jan Novak � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 217
Host Responses in Tissue Repair and FibrosisJeremy S. Duffield, Mark Lupher, Victor J. Thannickal,
and Thomas A. Wynn � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 241
v
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.

PM08-FrontMatter ARI 17 December 2012 9:46
Cellular Heterogeneity and Molecular Evolution in CancerVanessa Almendro, Andriy Marusyk, and Kornelia Polyak � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 277
The Immunobiology and Pathophysiology of Primary Biliary CirrhosisGideon M. Hirschfield and M. Eric Gershwin � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 303
Digital Imaging in Pathology: Whole-Slide Imaging and BeyondFarzad Ghaznavi, Andrew Evans, Anant Madabhushi,
and Michael Feldman � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 331
Pathological and Molecular Advances in PediatricLow-Grade AstrocytomaFausto J. Rodriguez, Kah Suan Lim, Daniel Bowers,
and Charles G. Eberhart � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 361
Diagnostic Applications of High-Throughput DNA SequencingScott D. Boyd � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 381
Pathogenesis of the Viral Hemorrhagic FeversSlobodan Paessler and David H. Walker � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 411
Skeletal Muscle Degenerative Diseases and Strategies for TherapeuticMuscle RepairMohammadsharif Tabebordbar, Eric T. Wang, and Amy J. Wagers � � � � � � � � � � � � � � � � � � � 441
The Th17 Pathway and Inflammatory Diseases of the Intestines,Lungs, and SkinCasey T. Weaver, Charles O. Elson, Lynette A. Fouser, and Jay K. Kolls � � � � � � � � � � � � � � 477
Indexes
Cumulative Index of Contributing Authors, Volumes 1–8 � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 513
Cumulative Index of Article Titles, Volumes 1–8 � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 517
Errata
An online log of corrections to Annual Review of Pathology: Mechanisms of Disease articlesmay be found at http://pathol.annualreviews.org
vi Contents
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
21-4
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Con
nect
icut
on
02/2
4/13
. For
per
sona
l use
onl
y.