Embed Size (px)
Citation preview

“Molecular Pathologypast present & future”
Thomas Kerr
Principal Healthcare Scientist
Molecular Pathology
Pathology Department
Southern General Hospital

“Molecular Pathologypast present & future”
Thomas Kerr
Principal Healthcare Scientist
Molecular Diagnostics
Genetics
Southern General Hospital

Molecular Pathology ?
• The discipline involved in diagnostic, prognostic and predictive testing on samples (usually tumour) removed from the patient in the course of investigation and treatment of disease.





Laboratory Facility


Molecular pathology
1988: Maura Farquharson
1992 MSc project ISH based
J Clin. Path 1996; “Immunoglobulin light chain mRNA detected by in situ hybridisation in diagnostic fine needle aspiration cytology specimens”
First diagnostic molecular pathology technique Kappa & Lambda ISH

B & T cell lymphoma•H&E morphology
•ICC
•ISH kappa, lambda & EBV
•FISH
•PCR

Lambda ICC

Lambda ISH

IgH clonality by Ceq8000
0 50000
100000 150000 200000 250000
0 50 100 150 200 250 300 350 400
BIGH Fr1 4313A-06.
Size (nt)
Dye Signal
0 1000 2000 3000
0 50 100 150 200 250 300 350 400
BIGH Fr1 4313B-06
Size (nt)
Dye Signal
0 50000
100000 150000 200000 250000
0 50 100 150 200 250 300 350 400
BIGH Fr2 4314A-06
Size (nt)
Dye Signal

TCRgamma clonality by CEQ8000
115
0 50000
100000 150000 200000
0 50 100 150 200 250 300 350 400
TCRGBCLONAL.
Size (nt)
Dye Signal
212
0 25000 50000 75000
100000 125000 150000
0 50 100 150 200 250 300 350 400
TCRGACLONAL
Size (nt)
Dye Signal

TCRgamma polyclonal
0
10000
20000
30000
40000
50000
0 50 100 150 200 250 300 350 400
T C R G A P O L Y .E 0 2 _ 0 6 0 4 0 7 0 8 P Q
Size (nt)
Dye
Sig
nal
05000
1000015000200002500030000
0 50 100 150 200 250 300 350 400
T C R G B P O L Y .E 0 4 _ 0 6 0 4 0 7 0 8 Q 7
Size (nt)
Dye
Sig
nal

Institute of neurological Science

GRI molecular pathology
•HER2 ICC & FISH
•Sarcoma FISH & RT-PCR
•Lymphoma FISH


2002 2003
Resection and Gliadel wafers
No other post-op Rx

1p186
1p226
Normal
Tumour
Normal
Tumour

19q112Normal
Tumour
19q219Normal
Tumour

N040300

• valuable for patient counselling
• useful in deciding intensity of treatment
• can be used clinically to select patients likely to benefit from adjuvant temazolomide treatment.
• can potentially save half of patients from receiving chemotherapy.
MGMT promoter status – clinical relevance

Methylated
M
U
N040300

Predictive & Prognostic markers in Neuro-oncology
• Molecular assays introduced to aid typing & grading of gliomas
• Improved understanding of these tumours at molecular level• Especially presence/absence of combined 1p19q loss in
oligodendroglial tumours, MGMT promoter gene methylation in glioblastoma, EGFR amplification in grade III astrocytic tumours & glioblastoma & IDH mutation analysis
• Now being used to tailor treatment decisions in patients, current therapy combination of surgery, radiotherapy & chemotherapy

49F frontal 60F temp/parietal
1p
19q
1p
19q

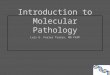
Molecular Haematology 2008
• Microsatellites for Chimaerism testing in post-BMT patients
• BCRABL (t9;22)• PMLRARA (t15;17) in AML• AML/ETO (t8;21) in AML• Chromosome 16 inversion in AML• JAK 2 status in myeloproliferative diseases• FLT3 mutations

Chimaerism

Fiona M Reid April 2011
Purpose of Chimaerism testing post BMT
• To detect an identifiable difference between a patient and their donor
• Ability to measure the proportion of donor present in the blood or bone marrow post transplant

Identification of chimaerism
Microsatellites: Short Tandem Repeats
Prepare DNA from blood or marrow
• PCR
• A number of primer sets in use
• Must identify an “informative “ set of primers

Preparation of DNA: the EZ1

Chimaerism on Lymphoid/Myeloid split
• Blood sample post BMT
• Use CD3 to enrich for Lymphocyte fraction
• Use CD15 to enrich for Myeloid fraction

Automacs Proseparator

Fiona M Reid April 2011
MicrosatellitesFull donor Chimaerism
0
50000
100000
150000
200000
395 400 405 410 415 420 425 430
5 4 4 r.A 0 4 _ 0 7 0 4 2 0 1 2 M Y
Size (nt)
Dye
Sig
nal
400 411.27
412.15
413.22
418.12 420
420.94
421.66
422.74
0
50000
100000
150000
200000
250000
395 400 405 410 415 420 425 430
5 4 4 d .B 0 4 _ 0 7 0 4 2 0 1 2 N 0
Size (nt)
Dye
Sig
nal
400 406.49
407.37
408.49
411.37
412.17
413.25
420
050000
100000150000200000250000
395 400 405 410 415 420 425 430
5 4 4 .C 0 4 _ 0 7 0 4 2 0 1 2 N 2
Size (nt)
Dye
Sig
nal
400407.08
408.48
410.13411.73
413.26
420

Fiona M Reid April 2011
MicrosatellitesMixed Chimaerism
0
50000
100000
150000
380 390 400 410 420 430 440
P E N T A E A .A 1 0 _ 0 8 0 5 1 5 1 2 5 8
Size (nt)
Dye
Sig
nal
385.38
386.41
387.42
424.89
425.91
0
50000
100000
150000
200000
380 390 400 410 420 430 440
P E N T A E B .B 1 0 _ 0 8 0 5 1 5 1 2 5 9
Size (nt)
Dye
Sig
nal
405.69
406.71
420.15
421.17
0
50000
100000
150000
200000
380 390 400 410 420 430 440
P E N T A E D .D 1 0 _ 0 8 0 5 1 5 1 2 5 D
Size (nt)
Dye
Sig
nal
386.40
387.44
405.62
406.70
420.09
421.16
424.91
425.98

Recommendations from the molecular pathology review group on the future of molecular pathology testing in
Scotland. (2010)
•The Calman review of genetics in relation to healthcare in Scotland
•Better health better care action plan
•Better cancer care action plan
•Clinical trials
•SPAN & Scottish cancer group networked approach to HER2 FISH testing

Conclusions & recommendations
A molecular pathology service should be developed and run as a NSD supported consortium, mirroring the Scottish genetics laboratory consortium for diagnosis of constitutional genetic abnormalities.
To ensure the stability of the services, equity of access and service development
Linked to the Scottish cancer taskforce, cancer networks and Scottish medicines consortium so that there is early coordinated planning for new testing.

Laboratory Facility

Targeted therapies
• Therapeutic monoclonal antibodies
• Small molecules

Therapeutic monoclonal antibodies
• Target specific antigens on proteins-extracellular growth factors eg transmembrane receptors
• Monoclonal antibodies end with the stem “mab” e.g. cetuximab which targets EGFR

Small molecules
• Penetrate the cell membrane to interact with targets inside a cell
• Interfere with the enzymatic activity of the target protein
• End with the stem “ib”, the agent has inhibitory properties e.g. imatinib in CML

Cost
• Targeted therapies £20000 per patient per year
• Molecular test EGFR £50

= Differentoutcome
s
Differentoutcome
s
Current Treatment is the Same for Most Patients
Outcomes can vary widely
=
Patients Treatment
+Disease
+
Different treatment outcomes affect patients’ safety, survival and quality of life

The Alternative:Personalized Healthcare
(PHC)Tailors treatment to
the patient
• Molecular diagnostic testing can stratify patients according to their specific genetic makeup and/or the nature of their disease or condition
• This approach improves drug safety, may increase patient survival, and may improve quality of life

Personalized Healthcare Provides benefits for all
stakeholders
Improvedbenefit to risk ratio
Patient
Efficient use ofhealthcare budgets
Payer
Informedtreatment decisions
Healthcare provider

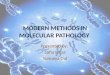
Near to mid-term genomics and oncology portfolioPlatform consolidation; Pharma driven focus on oncology
• RMD is committed to expanding the oncology menu in order to remain competitive in the oncology IVD market.

Biomarker Test Disease Therapeutic
Class Drug(s)
cobas® BRAF Mutation Test
Metastatic Melanoma BRAF Inhibitors RG7204 (PLX
4032), Zelboraf
cobas® KRAS Mutation Test
Colorectal Cancer
Anti-EGFR Monoclonal
Antibodies (mAb)
Anti-EGFR mAbTherapies,
cetuximab, panitumumab
cobas® EGFR Mutation Test
Non-Small Cell Lung Cancer (NSCLC)
Anti-EGFR Tyrosine Kinase Inhibitors
Erlotinib, Gefitinib
Current Cobas® Oncology PortfolioClinically validated biomarker tests on one
platform

cobas® 4800 Oncology TestsWorkflow Overview

Melanoma Progression
• Melanoma is the most aggressive
form of skin cancer originating
in the melanocytes.
• 197,000 people worldwide are diagnosed with melanoma each
year
50

BRAF Mutation TestDesigned to identify metastatic melanoma patients
who may benefit from BRAF inhibitors
• The cobas®4800 BRAF V600 Mutation Test– Is designed to determine mutation status of the BRAF gene– Is the companion diagnostic used in the clinical trials for
RG7204 (also known as PLX4032), an oral inhibitor of mutated BRAF co-developed by Roche Pharmaceuticals and Plexxikon. BRIM2 +3 clinical trials (>2,000 patients)~ Roche kit is the ONLY clinically validated kit.
– RG7204 has shown strong clinical activity in metastatic melanomas harboring the BRAF V600E mutation; clinical data suggests that patients with wild-type BRAF do not respond or respond adversely.

”

•
Colorectal Cancer Progression
• Incidence in the UK: ~70 cases per 100,000
• >95% of colorectal cancers arise from the glandular
epithelium that lines the gut (adenocarcinomas)

•
cobas® KRAS Mutation Test Designed to help identify colorectal patients who
are unlikely to benefit from anti-EGFR mAb therapies
cobas® KRAS Mutation Test:
• Is designed to determine mutation status of the KRAS oncogene
• Colorectal cancer tumors with KRAS mutations are unresponsive to anti-EGFR therapies1
• When combined with other clinical data, this information will help physicians identify colorectal cancer patients who may not benefit from
anti-EGFR mAb therapies
1. Amado et al. J Clin Oncol 2009;26:16261634

•
cobas® KRAS Mutation Test Designed to help identify colorectal patients who are
unlikely to benefit from anti-EGFR mAb therapies
cobas® KRAS Mutation Test:
• Is designed to determine mutation status of the KRAS oncogene
• Colorectal cancer tumors with KRAS mutations are unresponsive to anti-EGFR therapies1
• When combined with other clinical data, this information will help physicians identify
colorectal cancer patients who may not benefit from anti-EGFR mAb therapies
1. Amado et al. J Clin Oncol 2009;26:1626163455

Non-small cell lung cancer Overview
• Lung cancer is the most frequently diagnosed cancer and the leading
cause of cancer-related deaths worldwide: ~106,000 new cases of
advanced lung cancer per year in the UK, France, Spain, Italy and
Germany combined.
• NSCLC is the most prevalent and accounts for approximately 85% of all
cases.
• Prognosis for patients with NSCLC is poor with a 5-year survival rate of
only 15%.

•
Non-small Cell Lung Cancer Therapy Options - Overview
• Treatment of cancer is guided by disease stage:
• early stages: primary treatment is surgical resection
• locally advanced or metastatic disease:
• platinum-based chemotherapy
• targeted therapy
• anti-EGFR (cetuximab, panitumumab)
• tyrosine kinase inhibitors: erlotinib (Roche Tarceva® and gefitinib (AstraZenaca Iressa®)
• anti-VEGF (Roche Avastin®)

Non-small Cell Lung Cancer Role of EGFR
• EGFR is a receptor tyrosine kinase located on the cell surface
of epithelial cells.
• EGFR is linked to several signaling pathways including the
RAS/MAPK pathway and the PI3K/Akt pathway.
• In normal cells, these pathways are tightly regulated and are
activated only when a specific ligand (such EGF) binds to the
receptor.
• In cancer cells, EGFR gene mutations activate the kinase in the absence of a ligand leading
to abnormal cell proliferation and tumor formation.
58

cobas® EGFR Mutation Test Designed to help identify NSCLC patients who
may benefit from anti-EGFR TKI therapy
cobas® EGFR Mutation Test:
• Is designed to detect mutations in the EGFR gene in NSCLC tumor tissue
• Test results will help physicians identify NSCLC patients who may benefit from anti-
EGFR tyrosine kinase inhibitor therapy

Next Generation Sequencing
• High throughput, low cost (?) sequencing technology
• Human Genome Project started in 1990 and took 13
years to complete
• It was an international collaboration which cost $3 billion
and used traditional Sanger sequencing
• Today you could sequencing the human genome in
~month using NGS
• Target is the $1000 genome

Next Generation Sequencing
• Many NGS techniques, chemistries and instruments
now available
• Personal genome machines (PGMs) are affordable
bench-top instruments e.g. Ion Torrent
• NGS allows you to look at many genes or regions of the
genome, from many patients, simultaneously
• NGS has multiple applications and will replace many of
the molecular tests currently available in the lab

Ion Torrent

The present: small (and a little odd looking)

Ion Torrent Personal Genome Machine
• Bench-top NGS instrument from Life Technologies.
• Purchase the Comprehensive Cancer Panel from Life Technologies which targets exons within 409 oncogenes and tumour suppressor genes.
• Requires 10ng of input DNA from FFPE tissue.
• Produces amplicons of between 125-175bp and has 16,000 primers in 4 tubes.
• From DNA extraction to results is less than 24 hours, and the laboratory process is almost fully automated

The future: bigger and better
• What is bigger and better?
• Bigger is looking at more genes, better is improving the
patients diagnosis and treatment in doing so
• How do we do bigger and better?
• By sequencing the entire exome, every single base of
each coding exon in the genome
• In the future it will be cheaper and easier to sequence
the whole exome for every patient

NGS: the future

NGS: the future

NGS: the future
• Life Technologies claim the Ion proton will sequence the
entire human genome in 8 hours


Acknowledgements
• Maura Farquharson
• Willie Stewart
• Molecular pathology team SGH
• Nicola Williams, Jane Duncan, Rachel Ellis
• Aly Grant (Roche)

Information
• CRUK stratified medicine
• www.mycancergenome.com
• Life technologies ion torrent