Embed Size (px)
Citation preview

Pathology Informatics 18Roy E. Lee, Long Phi Le, and John Gilbertson
Contents
18.1 Definition and Scope of Pathology
Informatics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 500
18.2 The Major Components of Pathology
Informatics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 500
18.2.1 The Study of Information . . . . . . . . . . . . . . . . . . 500
18.2.2 The Study of Information Systems . . . . . . . . 500
18.2.3 The Study of Processes and Workflows . . . 501
18.2.4 Information, System, and Process
Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 501
18.3 Pathology Informatics and the
Diagnostics Laboratory . . . . . . . . . . . . . . . . . . 501
18.3.1 Codependency and
Shared Responsibility . . . . . . . . . . . . . . . . . . . . . . 501
18.3.2 Future Trends . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 502
18.4 The Laboratory Information System
and the Diagnostic Process . . . . . . . . . . . . . . . 502
18.4.1 The Total Testing Cycle . . . . . . . . . . . . . . . . . . . 502
18.4.2 Involvement by the LIS . . . . . . . . . . . . . . . . . . . . 502
18.5 Molecular Informatics . . . . . . . . . . . . . . . . . . . . 505
18.5.1 Unique Aspects of Molecular
Informatics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 505
18.6 Pathology Imaging . . . . . . . . . . . . . . . . . . . . . . . . 508
18.6.1 Specific Uses of Digital Imaging . . . . . . . . . . 508
18.6.2 Telepathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 509
18.6.3 Digital Pathology . . . . . . . . . . . . . . . . . . . . . . . . . . . 509
18.6.4 Current Status, Challenges, and Potential of
Digital Pathology . . . . . . . . . . . . . . . . . . . . . . . . . . . 510
18.6.5 Nontraditional Imaging Techniques . . . . . . . 510
18.7 Image Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . 511
18.7.1 Goals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 511
18.7.2 Working Examples . . . . . . . . . . . . . . . . . . . . . . . . . 511
18.7.3 Limitations to Image Analysis on Whole
Slide Images . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 511
18.7.4 Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 512
18.8 Digital Pathology, Image Analysis, and
the Laboratory Information System . . . . 512
18.8.1 Image Orders and Workflow . . . . . . . . . . . . . . . 512
18.8.2 Specimen Identification and Messaging . . . 512
18.8.3 Imaging at Sign Out . . . . . . . . . . . . . . . . . . . . . . . . 513
Further Reading . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 513
R.E. Lee, MD (*)
Pathology and Laboratory Medicine Institute,
The Cleveland Clinic, Cleveland, OH, USA
L.P. Le, MD, PhD � J. Gilbertson, MD
Harvard Medical School, Department of Pathology,
The Massachusetts General Hospital, Boston, MA, USA
L. Cheng, D.Y. Zhang, J.N. Eble (eds.), Molecular Genetic Pathology,DOI 10.1007/978-1-4614-4800-6_18, # Springer Science+Business Media New York 2013
499

18.1 Definition and Scope ofPathology Informatics
• Pathology informatics can be conveniently
defined as the study and management of
pathology information, information systems,
and processes (Table 18.1)
• The definition is based on the observation that
laboratory processes, the data those processes
consume and generate, and the computer
systems that manage that data and those
processes are intimately related
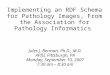
• Informatics is not synonymous with “informa-
tion technology” (IT) or “information services”
(IS) (Fig. 18.1). While informatics teams work
closely with IT/IS groups, the latter tend to be
focused on one component of informatics – the
technical implementation and maintenance of
information systems
18.2 The Major Components ofPathology Informatics
• Pathology informatics implemented at the
Massachusetts General Hospital is based on
four main areas of study: information, infor-
mation systems, processes (workflows), and
management
18.2.1 The Study of Information
• What information is required for a given process
• Measurements of information quality
• Information extraction (e.g., image analysis
and natural language processing)
• Annotation and meta-data
• Information models and architectures
• Programming principles (information
manipulation)
• Human processing and use of information
(e.g., human–computer interaction and user
interface design)
• Decision support principles (Bayes theorem)
• Information exchange and standards: data
standards (e.g., SNOMED, ICD) and messag-
ing standards (e.g., HL7, DICOM)
18.2.2 The Study of InformationSystems
• Laboratory information systems (LIS): archi-
tecture and operations (see below)
• Image management systems (e.g., picture
archival and communication systems [PACS])
• Bioinformatics systems
• Other clinical information systems (CIS):
ADT (admission, discharge, and transfer)
systems, CIS, electronic medical record
Table 18.1 Simplified breakdown of major areas under medical informatics. Because these three areas are often
confused with one another, it is important to define them here. Clinical informatics differs from pathology informatics
mainly in that the type of data and systems cover a scope outside of pathology and laboratory medicine and places less
emphasis on process optimization and redesign. Of note, bioinformatics is the only one of these three areas that explicitly
includes “computational tools” (IT) in its definition. Overall, medical informatics does not necessarily imply the use of
IT; however, in today’s age, IT makes the most sense to use, instead of traditional filing cabinets, and pen and paper
Clinical informatics Pathology informatics Bioinformatics
Concerned with information use in
healthcare by clinicians: clinical
decision support, CPOE, system
design, system implementation (e.g.,
electronic health records and health
information systems)
Concerned with laboratory
information, its systems (e.g.,
laboratory information system), and
associated processes. Pathology
informatics differs from clinical
informatics in that it is the branch of
medical informatics covering
pathology data and the processes and
systems it covers. A greater proportion
is devoted to process optimization,
such as Lean Six Sigma
Associated with “hard-core” number-
crunching algorithms for analysis and
study of data at the DNA, RNA, and
protein levels and less about information
flow and processes. NIH definition
(2000): research, development, or
application of computational tools and
approaches for expanding the user of
biological, medical, behavioral, or
health data, including those to acquire,
store, organize, archive, analyze, or
visualize such data
500 R.E. Lee et al.

(EMR)/electronic health record/patient medical
record systems, and financial systems
• System interoperability and connectivity
(interfaces and standards)
• System life cycle (creation, implementation,
maintenance, decommission) of clinical systems
• User training
18.2.3 The Study of Processes andWorkflows
• Process theory (industrial engineering)
• Process analysis, improvement, and valida-
tion: (e.g., business process management
(BPM), failure modes and effects analysis
(FMEA), and Lean Six Sigma)
• People working in systems (e.g., Just Culture)
• Outcomes measurement
• Process modeling and simulation
• Decision support processes
18.2.4 Information, System, andProcess Management
• Pathology informatics involves large, com-
plex, highly integrated, and interconnected
systems supporting hundreds of users and
processes. Successful system development
and implementation and management in the
pathology environment require significant
communication and management skills
– Project management
– System management
– Capital and accounting finance
– Software development management
– Validation studies management
– System selection, implementation, and
maintenance (e.g., total cost of ownership)
– Regulatory compliance
18.3 Pathology Informatics and theDiagnostics Laboratory
18.3.1 Codependency andShared Responsibility
• A modern diagnostic laboratory cannot
function without an effective information
system, and an effective information system
cannot be designed, implemented, or
maintained without a clear understanding of
the operations and missions of the lab. There
are numerous reasons for this:
– The primary product: Accurate, actionable
clinical information, in the form of final-
ized results or “signed out” reports, is the
primary product of pathology labs
– Required inputs: Laboratory operations
depend on access to clinical, patient, spec-
imen, and financial information
– Management of processes: Diagnostic lab-
oratories run complex processes that need
to run efficiently, at low variance, and with
limited failures. The processes must be val-
idated and documented
– Communications: Communication
between the lab and the rest of the clinical
care team (usually through formal orders
and results/reports as well as ad hoc) is
central to the value of the laboratory and
the safety of the patient
– Automation: Automation, standardization,
machine-readable specimen identification
(barcodes), and clear, human- and
Fig. 18.1 The term “informatics” is not synonymous
with information technology. In pathology informatics,
these three major components of pathology information,
information services/technology, and laboratory processes
are intimately linked and related
18 Pathology Informatics 501

machine-readable results/reports have been
shown to improve efficiency, patient
safety, and effective communication
between the lab and the clinic
– Data sharing and interoperability: Pathol-
ogy/laboratory results are used by multiple
downstream information systems
(reporting systems, electronic information
systems, etc.). Studies have shown that the
majority of data in most EMRs originates
in diagnostic laboratories and that most
significant medical decisions depend on
laboratory data
• Each above activity is a shared responsibility
between medical staff, laboratory technical
staff, the information management team, and
information system developers. System devel-
opers must understand the laboratory’s goals,
missions, and customers, and laboratory staff
should understand that the LIS is their best
tool for feedback, quality assurance, and lab-
oratory efficiency/value
18.3.2 Future Trends
• Demographic trends (national and interna-
tional), the explosion of genetic and molecular
testing and digital imaging, and increasing use
clinical decision support systems, workflow
efficiency engines, utilization and value stud-
ies, and the convergence of basic science and
clinical application (all of which will require
high-quality, standardized, machine-readable
laboratory data) will drive increased needs for
sophisticated LIS and pathology informatics
for the foreseeable future
18.4 The Laboratory InformationSystem and the DiagnosticProcess
• Though normally considered a computer sys-
tem, the LIS can be thought of more broadly as
a set of related processes, operations, and pro-
cedures, some or all of which are supported by
one or more computer systems. The primary
goal of an LIS is to support the operations of
a clinical laboratory. It therefore makes sense to
discuss the LIS in terms of laboratory operations
18.4.1 The Total Testing Cycle
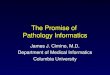
• The total testing cycle (TTC) is a classic, high-
level model of the diagnostic laboratory pro-
cess (Fig. 18.2). The TTC models laboratory
testing as a largely linear process beginning
when testing is first considered by the clinician
and continues through the clinical and labora-
tory processes needed to order the test, collect
and transport the specimen, prepare the spec-
imen for testing, run the test, and through the
interpretation of the test result first by lab staff
and pathologists (which may result in further
testing) and finally by clinicians. The process
is modeled as a cycle because the results of
one test often results in the ordering of others
18.4.2 Involvement by the LIS
• The LIS (and related information systems) is
involved in every step of the TTC
18.4.2.1 Ordering and Order Entry• Ordering is the process through which the
ordering clinician chooses and orders tests or
other laboratory services (such as anatomic
pathology analysis of tissue specimens).
Traditionally done through paper requisitions,
it is increasingly done through computerized
“provider order entry” systems (CPOE).
By interfacing with other systems (the LIS,
test formularies, lab handbooks, etc.),
sophisticated CPOE systems allow clinicians
to search for tests, obtain advice on appropri-
ate test selection and cost, manage utilization,
collect clinical information or clinical justifi-
cation necessary for the laboratory doing the
test, or provide mechanism for the ordering
physician to talk directly to a pathologist
• Order communication and specimen transport
– Orders are passed to the LIS, usually
through an ordering interface, and patient
502 R.E. Lee et al.

and encounter information is sent to the
LIS through an ADT (admission, dis-
charge, and transfer) interface. In some
systems, the LIS prints barcoded containers
in clinic for identification of the specimens;
in other cases, specimen identification is
done by a separate process in the
clinic. Increasingly barcoded specimens
are tracked during transport from the clinic
to the lab
• Accessioning
– Accessioning is the process through which
the laboratory (through the LIS) takes pos-
session of the specimen; verifies patient,
insurance, order, and specimen informa-
tion; reconciles discrepancies; and associ-
ates the specimen(s) with the specific
laboratory processes that will eventually
lead to a diagnostic report. Laboratories
often provide their services for multiple
clinics and hospitals and receive specimens
in many different ways, making accessions
an important and complex process
• Diagnostic processes
– Diagnostic processes (also known as pro-
tocols or workups) define the way the lab
are activities that the lab employs to gener-
ate the information needed to solve the
clinical question at hand. Processes can be
iterative or nested. Depending of the com-
plexity of the diagnostic question, a lab
may employ multiple subprocesses (e.g.,
specimen dissection and description, tissue
processing, embedding, tissue sectioning,
staining, molecular studies, and micro-
scope examination) involving multiple
subdivision of specimens (e.g., parts,
blocks, slides, and aliquots) and even dif-
ferent laboratories in the pathology depart-
ment or at outside institutions (e.g.,
surgical pathology, molecular pathology,
flow cytometry, and reference laboratories)
to fully work up a case. A major role of the
LIS is to organize and keep track of this
complex flow of specimens, processing,
testing, and data. LIS has several mecha-
nisms to do this
• Unique specimen identification, usually
by barcode
• Tracking the physical location of speci-
mens and knowing where each speci-
men should be and where it should go
next (“routing”)
• Protocols defining where specimens
should go (routing) and how they should
be processed/analyzed at each location.
Protocols tend to be specific to specific
specimen types: For example, a breast
Fig. 18.2 The total testing
cycle: The TTC is a model
of the generic clinical
testing process. It begins
with a clinical question and
the decision to test, through
the ordering, specimen
collection and
transportation to the steps
necessary to generate,
interpret, and report results
in lab and communicate
them to the
clinic. Information systems
are involved in virtually
every step in the cycle
18 Pathology Informatics 503

biopsy may have a different route and
may be subjected to different protocols
(e.g., different processing, more slides,
more stains, and fewer images) than
a kidney resection
• Status: Each case and tissue asset in the
LIS is given a status depending on its
completeness in the diagnostic cycle.
Examples include “Accessioned,” “In
histology,” “Final,” and “Signed out”
• Primary or secondary protocols
– Diagnostic processes can be iterative:
The first set of protocols on a tissue biopsy
may be designed to establish the presence (or
absence) of cancer. If cancer is established,
the lab might use other protocols to classify
the cancer using tumor markers. The use
of these secondary protocols can be automa-
tically triggered based on the results of initial
test results (reflex testing) or done on the
order of the pathologist working up the case
• Interpretation and reporting
– In a simple case such as the measurement
of serum electrolytes, results can be
accepted by the LIS from the analyzer and
reported to the clinic (usually via a CIS, see
below) after the test or batch passed quality
assurance. Such test results are usually sent
with minimal interpretive information such
as normal reference ranges. For complex
testing requiring an interpretive report
from the lab (e.g., anatomic pathology),
each report is reviewed by the primary
pathologist for the case who then signs out
each case (usually through electronic sig-
nature) in the LIS
• The pathology report
• In some areas of pathology (such as surgical
pathology, cytology, molecular pathology,
and autopsy), a clinical report is needed to
communicate
– What specimens were received
– What processes/workup were done
– Specific laboratory data or results (e.g.,
“size of tumor” or “number of lymph
nodes dissected”)
– Diagnostic interpretation (e.g., “prostatic
adenocarcinoma, Gleason 3 + 4 ¼ 7”)
– Clinical communications and notes (e.g.,
“interpretation is limited by extensive cau-
tery artifact”)
– In addition, the pathology report contains
information on the pathologists and clini-
cians associated with the case, the clinical
context, diagnostic and procedure codes,
and information used in a wide range of
operational and financial reports as
discussed in the “Postdiagnostic activities”
section below
– The LIS provides a series of tools for the
creation of the pathology report including
the ability to create specific report tem-
plates for different types of cases, word
processing including spell checking,
“quick text,” or “macros” for the inclusion
of standard text by typing short, relatively
simple codes. In many cases, LIS allows
structured data entry in which information
is entered in specific data elements directly
into the system with a defined set of valid
values and stored as discrete data elements
in the database. For example, the College
of American Pathologists tumor templates
are often implemented through a structured
data entry tool in the system, thus
bypassing the use of paper
• Report and result communication
– Laboratory reports created in the LIS are
communicated to clinicians through
a variety of mechanisms including printing
and mailing, dedicated printers in clinical
offices, faxing and, increasingly, secure
Internet/web-based report distribution sys-
tems. However, the great majority of
reports are communicated, via HL7 inter-
faces, to EMR systems and CIS
– The LIS is usually able to display pathol-
ogy reports in a much more sophisticated
way than the EMR. There are two main
related reasons for this: (1) The HL7 inter-
faces that communicate the report cannot
easily communicate formatting informa-
tion (such as tables or font), and (2) EMR
systems tend not to support sophisticated
formatting. This is a significant problem for
laboratory – clinic communication – and
504 R.E. Lee et al.

is slowly being mitigated by improved
interfaces and support for open, standard-
ized file formats such as the portable docu-
ment format (PDF)
• Alerts, preliminary reports, addenda, and
amendments
• In addition to the standard results and pathol-
ogy reports, LIS provides other mechanisms
for communications between lab and clinic
– Alerts: Usually used to communicate lab
results that fall in predefined “critical
ranges,” alerts can be implemented as font
or formatting changes in the report (or
EMR), automated paging or direct phone
calls to the ordering or responsible physician
– Preliminary reports: can be used for
a variety of purposes, for example, to notify
the clinic that a case result will be delayed
– Addenda: an addition to a signed out report
that adds new data (but usually does not
change the clinical impact of the diagnosis
reported in the signed out report)
– Amendment: a mechanism for changing
a signed out report with information that
could have significant clinical impact.
Because of the potential clinical impact,
amendments are usually issued with some
form of active clinical alert (vide supra)
• Postdiagnostic activities
• After result reporting or report sign out, the LIS
continues to manage data, reports, and speci-
mens. Typical postdiagnostic activities include
– Management of cases for clinical conferences
– Management of specimens: clinical archives
for specimens, aliquot, blocks, and slides.
The archive time frame can range from
days to years depending on the importance
of the specimen and the cost associated with
storage. In many cases, specimen archiving
is mandated by law
– Management reports: The LIS in a large
hospital or practice will generate hundreds
of reports needed for management and con-
trol of lab operations, workload, efficiency,
and finance
– Billing reports: The LIS generates reports
that include the information needed to bill
for lab services. Typically, these reports are
passed to billing systems that use the data
to validate charges and generate actual
invoices that are passed to third-party
payers, lab clients, or patients
– Reports to registries, research databases,
and regulatory agencies. Examples include
reports to cancer registries, enterprise
research databases that provide de-
identified clinical data to researchers, and
regulatory and certification agencies
18.5 Molecular Informatics
• Molecular studies have become commonplace
in virtually all aspects of pathology, especially
in areas such as microbiology and anatomic
pathology. Molecular testing includes a wide
range of modalities, mostly in the form of
single gene tests from commercial vendors
and laboratory-developed tests. Multigene or
genomic level testing and sequencing will
become more widespread as the technology
becomes more affordable and the practice of
personalized medicine becomes more routine
• Molecular informatics as a subset of pathol-
ogy informatics focused on the flow of infor-
mation through a molecular laboratory,
starting from test ordering through reporting,
and has substantial similarities and significant
differences compared to informatics in tradi-
tional clinical and anatomic pathology labora-
tories, especially in data storage requirements
(Table 18.2)
18.5.1 Unique Aspects of MolecularInformatics
18.5.1.1 Samples, Analytes, and Testing• Sample types of varying quantity and quality
that need to be accessioned and tracked as
assets
– Blood: useful for germ line testing or
blood-related diseases; typically yields suf-
ficient quantity and high-quality material
– Fresh/frozen tissue: similar to blood but
often not routinely available
18 Pathology Informatics 505

– Body fluids: varying quantity and quality of
material
– Formalin-fixed paraffin-embedded (FFPE)
tissue: standard specimen in most anatomic
pathology laboratories; varying quantity and
quality affected by age of tissue and degree
of formalin fixation which leads to cross-
linking and fragmentation of nucleic acids
• Various analytes/substrates derived from the
initial specimen which contribute different
information (DNA, mRNA, noncoding
RNA); one specimen may yield multiple
molecular derivatives or assets, which may
be challenging for tracking
• The means of testing, data analysis, interpre-
tation, and reporting vary according to
whether the target mutations are germ line
(inherited as in familial diseases) or somatic
(acquired after fertilization as in cancer)
• Various types ofmutations to be detectedwhich
would command different testing modalities
– Single-nucleotide polymorphisms (SNP) or
single-nucleotide variants (SNV)
– Small insertions and deletions (indels)
– Copy number variations (CNV)
– Structural rearrangements (translocations,
inversions)
– Epigenetics (DNA methylation)
– Several types of data may be obtained from
the same molecular derivative
18.5.1.2 Data Types• Qualitative (e.g., base substitution/insertion/
deletion, translocation between two gene
partners, and positive detection of a band on
a gel)
• Quantitative (e.g., fragment size, copy number
change, somatic mutation at a low allele fre-
quency in a tumor specimen, HIV viral load
testing, and bcr-abl testing for minimal resid-
ual disease in chronic myelogenous leukemia)
• May be very complex with multiple muta-
tions/changes detected for one sample
18.5.1.3 Interpretation of Results• Various forms of results output: PCR gel
image, fragment capillary electrophoresis
tracings, fluorescently probed tissue slides
viewed under microscopy, quantitative real-
time PCR data based on interpolation of stan-
dard curves, copy number profile from
genome-wide copy number analysis, and
sequence data from capillary electrophoreto-
grams or pyrograms
Table 18.2 Example comparisons of data storage requirements between anatomic, clinical, and molecular pathology.
Numbers are in uncompressed files and, although not necessarily exact, serve to illustrate the differences in magnitude of
data storage between themselves
Category Test/entity Data storage requirements
Anatomicpathology
Annual storage needs on AP
LIS
<1 TB per year, assuming 100,000 cases per year
Pathology imaging Depends on compression scheme, scanning magnification, amount of
tissue on slide, number of focal planes per virtual slide, and number of
slides per case. A major academic institution generating over 2,000 slides
per day could easily consume over 33 TB per month (surgical pathology
only – excluding cytology)
Clinicalpathology
Blood banking: transfusion
service
�21 GB/year added to database (assuming 60,000 cases/year)
Clinical labs <1 GB/year (assuming volume of 100,000 cases per year)
Molecularpathology
aCGH �70 MB per case (text only)
�275–300 MB/case (if image file included)
Sanger sequencing �400–500 KB per amplicon (�400–600 bp lengths each, and including
both *.ab1 files for forward and reverse primer reactions)
Next-generation sequencing
(exome only)
�13 GB (Illumina HiSeq platform) per run
Next-generation sequencing
(whole genome)
�500–600 GB (Illumina HiSeq platform) per run
506 R.E. Lee et al.

• Various utility of results: diagnosis, prognosis,
and therapeutic significance
• Most one target (single nucleotide or single
gene)-based assays are interpreted in a binary
(positive or negative) fashion or quantitatively
(if signal is present, then disease is present with
burden relative to level of detection); these
interpretations tend to be “static” in nature that
is based on prior established knowledge about
recurrent mutations and their functional effects
• Assays testing for the entire sequence of a
gene (whole gene sequencing) or with
genome-wide scope (array comparative geno-
mic hybridization)may detect variants that have
not been previously described in addition to
ones that are recurrent and have known conse-
quences; new variants require extensive
literature search, cross-checking with mutation
databases, in silico modeling, and population
statistics to further characterize their meaning
(benign, likely benign, of unknown signifi-
cance, likely pathogenic, pathogenic); often,
data on these new mutations are incomplete or
lacking, requiring a classification of “unknown
significance”; variants of unknown significance
may need to be reclassified as new studies
reveal their functional relevance; therefore,
whole gene or genome-wide tests require
“dynamic” interpretation
• Detected rare variants may be private for
a certain family or subpopulation; testing of
additional members may yield added informa-
tion for linkage analysis and proper classifica-
tion of the variants
• Molecular testing which has traditionally
relied on test interpretation for one individual
based on known variants will have to adopt
population-based interpretation to yield the
most meaning out of genetic information
(e.g., what proportion of cancer patients with
a particular gene mutation)
18.5.1.4 Data Curation/Archiving• As molecular testing becomes more complex,
involving many genes and genome-wide
coverage, data curation/archiving is imperative
• Processes should be in place to easily
capture molecular results from instruments,
annotations/interpretations from molecular
pathologists/geneticists, findings from clini-
cians (phenotype), and all other laboratory/
radiological data
• A comprehensive collection of structured
medical testing and clinical phenotype data
affords the ability to easily query for popula-
tion-based statistics and clinical genotype cor-
relation to classify variants of unknown
significance
• Structured data should also be collected
throughout the test workflow for sample track-
ing, quality assurance, quality control, and
process management
18.5.1.5 Reporting• Reports from the molecular pathology labora-
tory may include both qualitative and quanti-
tative elements
• Reporting mutations or genetic changes
should be based on standardized nomenclature
so that recipients from other institutions may
comprehend the test results
• Results may be simple as in a single-base
substitution or complex involving
a multitude of mutations detected in
a genome-wide manner; results may be inter-
related (e.g., expression or methylation data
for a gene that was also sequenced at the DNA
level) and should be correlated to make sense
of the observations
• Molecular data particularly those resulting
from genome-wide studies will require clever
visualization tools to quickly navigate through
complex datasets; a simple text-based report
may not be sufficient
• Reporting of variants may require documenta-
tion of references and primary literature which
should be archived with the laboratory muta-
tion database; references and interpretations
may change as more functional data are
accumulated
18.5.1.6 Workflow in a MolecularPathology Laboratory IsComplex
• Molecular tests usually require multiple pro-
cesses handled by multiple personnel
18 Pathology Informatics 507

• Sample tracking and quality control check-
points are needed to successfully operate
a high-volume molecular laboratory, particu-
larly for high-throughput tests
• Automation should be applied as much as
possible to ensure testing accuracy and
consistency and to enable the allocation of
human resources for other intellectually
demanding tasks
• Digitization should be implemented where
possible to increase workflow efficiency
(e.g., digital document management to
achieve a paperless operation)
18.5.1.7 Future Issues• The arrival of next-generation sequencing into
the clinical molecular laboratories will push
the limits of current molecular informatics
systems
• All aspects of molecular informatics
(accessioning, workflow, sample tracking,
data curation, results interpretation, reporting,
and so forth) will be further taxed with the
increased data burden and complexity of
high-throughput sequencing
• Next-generation sequencing allows the con-
current testing of many genetically barcoded
samples for many targets, yielding billions of
bases of information (gigabytes to terabytes of
information)
• Next-generation sequencing as a single testing
modality may potentially detect point muta-
tions, indels, copy number, gene expression,
structural rearrangements, and methylation
status all in one assay
• Operation of a next-generation sequencing
laboratory will require not only molecular
informatics for routine laboratory operation
but also a multitude of other informatics
disciplines for successful implementation:
Bioinformatics and biostatistics for analysis
and interpretation, medical informatics for
genotype–phenotype correlation and reporting,
and information technology and information
systems support to provide the infrastructure
for the data and computation demands of
next-generation sequencing
18.6 Pathology Imaging
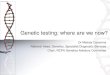
• Digital imaging is used extensively in the
pathology laboratory (Fig. 18.3)
• The main reasons for digitization
– Documentation of specimens
– Digital management of documents
– Visualization of data
– Communication (e.g., telepathology)
– Computation (e.g., image analysis)
– The ability to use multispectral (nonwhite)
light for analysis
18.6.1 Specific Uses of Digital Imaging
• Documentation of gross and autopsy speci-
mens, microbiology plates, gels, gram stains,
urine sediment, and microscope fields in
histopathology, cytology, hematology, and
parasitology
Fig. 18.3 Current versus digital workflows:
Predigitization (blue), digitization (green), and postdigi-
tization (yellow) steps are shown. This picture illustrates
how every step in the process is important – errors or
tissue folds on the slide will affect each upcoming step
508 R.E. Lee et al.

• Document management
• Display of complex data, such as flow
cytometry
• Telepathology
• Diagnostic image analysis or image-based
diagnostic decision support; for example,
automated Pap smear screeners
• The use of multiple, specific wavelengths of
light, as inmultiple target FISH or quantum dots
18.6.2 Telepathology
• Telepathology is a mechanism for laboratory
to laboratory communications that allows dig-
ital images created at one site to be viewed and
interpreted at another. Virtually, any lab oper-
ation (from grossing to electron microscopy)
can be managed through telepathology
• Fundamental requirements
– Ability to digitize the specimen at the
sending site
– A network that can support the
communication
– Ability to display at the receiving site
18.6.2.1 Three Main Types ofTelepathology
• Static
– Relatively small, single fields are captured
and sent through the network. Static
telepathology is useful when the diagnostic
material can be meaningfully imaged in
a limited number of discrete fields and/or
the when the diagnostic request is to confirm
a specific finding. It has been used
effectively in microbiology, parasitology,
and Pap cytology (confirmation of the
output of an automated screener)
• Robotic
– A video camera is connected to a robotic
microscope. An operator at a distant site
operates the robotic microscope and views
the video images. In some implementation,
a high-resolution still camera is also attached
to the microscope, allowing the operator to
capture and view high-fidelity images.While
robotic systems require relatively high
bandwidth, they have been used successfully
to support remote hospitals for both routine
pathology and frozen section diagnosis
• Whole slide imaging
– As the name implies, all of the tissue on
a microscope slide is digitized at high reso-
lution and is stored on a server as a complex,
compressed “pyramid” file that saves the
whole slide image at multiple resolutions
(or “levels”) roughly corresponding to the
resolutions one would see under a
microscope with 4x, 10x, 20x, and 40x
objective lens and 10x oculars. Each level
is divided into multiple, small “tiles” that
can be independently sent from the server
to the remote client system. The pathologist
is initially presented with a low-resolution
“thumbnail” image and “pan and zoom”
into and around the image by clicking on
the image, with the server presenting only
the image data needed to render the area of
the slide the pathologist is looking at (very
much like “Google Maps”). While an
entire whole slide image may be large
(0.3–10 GB), the pathologist tends to do
most of their examination at low resolution;
therefore, a relatively small percentage of
the image data (or “tiles”) is sent over the
network to be displayed
18.6.3 Digital Pathology
• There is increasing interest in the potential,
large-scale implementation of whole slide
imaging for primary diagnosis. This process,
known as digital pathology, has
predigitization, digitization, and postdigi-
tization phases, each of which impacts image
quality and each of which needs to be consid-
ered if large-scale digital pathology is to be
successful in clinical practice
18.6.3.1 Predigitization• In pathology, imaging begins as the
physiochemical process of fixing and processing
tissue, cutting tissue sections, placing them on
slides, and staining them with a variety of
18 Pathology Informatics 509

technologies (e.g., histochemical staining,
immunohistochemical staining, and fluorescent
in situ hybridization [FISH] staining). These
techniques remain as the most important part
of the imaging process
• Traditionally, these techniques have been
highly manual, with a high variance from
slide to slide that is detrimental to the down-
stream digitization process. Increasingly,
however, automation has been developed for
each step of the process (processing, embed-
ding, staining, coverslipping – there is even
work on automated tissue sectioning)
18.6.3.2 Digitization• Over the past 10 years, automated devices have
been developed to digitize (or “scan”) whole
slides rapidly, automatically, and at high fidel-
ity. Current high-end devices can automatically
scan a slide in approximately 1 min at a spatial
sample period of approximately 1.5 mm(similar to the resolution of a microscope with
a 40x lens). Image quality and system through-
put (the number of slides successfully scanned
per hour) are dependent on the quality of
the prediagnostic image phase (vide supra)
18.6.3.3 Postdigitization• After image capture, the images are stored on
a server and prepared for viewing and inter-
pretation as discussed in the telepathology
section above. Parameters that affect image
quality include the amount of compression,
the quality of the pathologist’s monitor dis-
play, and the viewing environment
18.6.4 Current Status, Challenges, andPotential of Digital Pathology
• Digital pathology is in the early phases of
development and implementation. There are
still significant challenges as well as large,
potential rewards
• Imaging consumes precious time and disrupts
histology workflow
– Current high-end scanners can scan a slide
in approximately one minute (a rate that
has been decreasing rapidly). However, if
one considers that a large lab might gener-
ate 2,500 sides per day and that the standard
histology process involves a large amount
batching, it is clear that imaging the major-
ity of the lab’s slide will require a large
number of scanners and potentially
a change to a nonbatched, continuous flow
histology operation
• Cost and profitability
– Digital pathology requires significant capi-
tal, and profitability has yet to be proven
– Scanners, servers, networks, monitors,
potential infrastructural changes to the lab,
and theworkstations in the pathologist office
when combined in to become prohibitively
expensive, and no one has yet demonstrated
a model with a clear return on investment
• Regulation and validation
– While use of WSI for second opinion con-
sultation and intraoperative consultation
seems to be established, the current opinion
of the FDA is that whole slide imaging
systems will likely be regulated as class
three devices when used for primary diag-
nosis; significantly, there is no consensus of
the testing necessary to prove the safety
and efficacy of WSI in primary diagnosis
and therefore no mechanism to get devices
cleared for this application
• The potential of digital pathology
– Despite the significant challenges, digitiz-
ing the majority of histopathology slides
automatically and at high fidelity has obvi-
ous potential. It would allow laboratories to
apply network connectivity and computa-
tional power – the driving forces of inno-
vation and efficiency in the modern
world – to anatomic pathology
18.6.5 Nontraditional ImagingTechniques
• In addition to WSI and digital pathology,
pathology labs are beginning to examine the
use of techniques developed in radiology or
endoscopy
510 R.E. Lee et al.

– Virtopsy (virtual autopsy): the use of CT
and other radiology tools as adjunct to the
autopsy
– Specimen CT: potentially to evaluate mar-
gins or large tissue volumes
– In vivo microcopy (for the epithelial/
endothelial surface of hollow organs and
vessels)
– Multitissue section, high resolution, and
three-dimensional reconstruction
18.7 Image Analysis
18.7.1 Goals
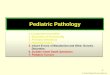
• The goal of imaging analysis is to assist the
laboratory and pathologist when making
morphology-based decisions such as ruling in
or out specific diagnosis, measuring the
quality of the slides and stains, counting
structures such as mitoses or tumor size, or
standardizing tumor grade. Image analysis
can also be used to improve the digital pathology
viewing experience of the pathology by, for
example, registering the images of two adjacent
tissue sections so that they can be viewed and
navigated in tandem (Fig. 18.4)
18.7.2 Working Examples
• While diagnostic image analysis on whole slide
images is in its infancy, the use of image anal-
ysis in automated Pap screening is a mature
technique that is used by hundreds of laborato-
ries on millions of specimens each year
18.7.3 Limitations to Image Analysison Whole Slide Images
18.7.3.1 Data Size• A typical whole slide image represents giga-
bytes of data in uncompressed form, placing a
huge data load on any computational process
Fig. 18.4 Basic image analysis techniques: (a) Once the
tissue section is stained and imaged, the digital slide can
undergo a variety of manipulations for image analysis,
such as (b) sharpening; (c) segmentation, in which an
anatomical or histological structure is separated from
the rest of the image via automated algorithms; and
(d) classification, in which the segmented regions of the
image is identified/associated with a specific anatomic or
medical entity
18 Pathology Informatics 511

18.7.3.2 Histology Artifact• Standard, largely manual histology processes
result in:
– Tissue sections with variable thickness and
that are rotated, translated, folded, and
twisted
– Staining can be highly variable
18.7.4 Techniques
• Histochemistry
– Though not normally considered part of
image analysis, histochemical, immunohis-
tochemical, and FISH staining is an
extremely powerful tool for tissue segmen-
tation and structure classification (vide
infra)
18.7.4.1 Averaging and Sharpening• These are basic techniques, usually applied
across the entire image, to remove noise
(averaging) or sharpen edges. Done by
applying appropriate filters to either the spatial
or the color space
18.7.4.2 Segmentation• The separation of meaningful structures
in the image (usually anatomic or disease
structures, such as separating bone from soft
tissue); segmentation is done by applying
“morphologic” or color “operators” that look
for specific shapes, textures, and colors in
image. Operators usually begin with a basic
shape (e.g., a blue circle of a given size) and
then apply “erosion,” “dilation,” or color vari-
ation programs to find similar structures
18.7.4.3 Classification• Classification is the identification/association
of specific objects or regions (identified
through segmentation) with specific anatomic
or medical entities (such as cancer cells and
blood vessels)
18.7.4.4 Registration• An image analysis technique important in dig-
ital pathology registration allows WSI from
two adjacent tissue sections (which have
been independently rotated, translated, and
twisted in the histology process) to overlay
on the same screen
18.7.4.5 Pipelining• A typical image analysis process would
involve histology staining, imaging, averaging
and sharpening, segmentation, classification,
and, potentially, registration in a “pipeline”
and creating the completed analysis
18.8 Digital Pathology, ImageAnalysis, and the LaboratoryInformation System
• As the main workflow engine of the pathology
lab, the LIS has a major role in the future
implementation of large-scale digital pathol-
ogy and image analysis
18.8.1 Image Orders and Workflow
• LIS has the capacity to include imaging and
image analysis as part of the workflows (routes
and protocols) defined in the LIS for specific
specimen types and clinical questions. For
example, the current protocol for a breast core
biopsy might call for placing the entire core in
a single block, process with a specific protocol,
cut ten levels from the block and stain level 1, 5,
and 10 with H&E, save the remainder for
potential immunohistochemistry, and send the
case to the breast pathologist on service.
This could be extended to including imaging
level 1, 5, and 10 at high resolution on a specific
slide scanner
18.8.2 Specimen Identification andMessaging
• LIS barcodes and HL7 messages between the
scanner and the LIS will manage and allow the
scanner to identify slides and the appropriate
imaging orders on each slide
512 R.E. Lee et al.

18.8.3 Imaging at Sign Out
• Incorporation of imaging at sign out by inte-
grating images into the standard sign out
workflow
Further Reading
Baron JM, Dighe AS. Computerized provider order entry
in the clinical laboratory. J Pathol Inf. 2011;2:35.
Buesa RJ. Adapting lean to histology laboratories. Ann
Diagn Pathol. 2009;13:322–33.
Butte AJ. Translational bioinformatics applications in
genome medicine. Genome Med. 2009;1:64.
Cankovic M, Varney RC, Whiteley L, Brown R,
D’Angelo R, Chitale D, et al. The Henry Ford produc-
tion system: LEAN process redesign improves service
in the molecular diagnostic laboratory: a paper from
the 2008 William Beaumont hospital symposium on
molecular pathology. J Mol Diagn. 2009;11:390–9.
Cowan DF. Informatics for the clinical laboratory:
a practical guide. New York: Springer; 2003.
Gabril MY, Yousef GM. Informatics for practicing ana-
tomical pathologists: marking a new era in pathology
practice. Mod Pathol. 2010;23:349–58.
Gilbertson J, Yagi Y. Histology, imaging and new diag-
nostic work-flows in pathology. Diagn Pathol.
2008;3(Suppl 1):S14.
Glenn TC. Field guide to next-generation DNA
sequencers. Mol Ecol Resour. 2011;11:759–69.
Gomah ME, Turley JP, Lu H, Jones D. Modeling complex
workflow in molecular diagnostics: design specifica-
tions of laboratory software for support of personal-
ized medicine. J Mol Diagn. 2010;12:51–7.
Guidi GC, Lippi G, Solero GP, Poli G, Plebani M. Man-
aging transferability of laboratory data. Clin Chim
Acta. 2006;374:57–62.
Paszko C, Pugsley C. Considerations in selecting a labo-
ratory information management system (LIMS). Am
Lab. 2000;32:38.
Sinard JH. Practical pathology informatics: demystifying
informatics for the practicing anatomic pathologist.
New York: Springer; 2006.
Stephan C, Kohl M, Turewicz M, Podwojski K, Meyer
HE, Eisenacher M. Using laboratory information man-
agement systems as central part of a proteomics data
workflow. Proteomics. 2010;10:1230–49.
Tuthill M. Automating anatomic pathology.
Implementing an AP solution that integrates with
your hospital’s LIS can improve workflow and produc-
tivity. Health Manag Technol. 2008;29:18, 20.
Weinstein RS, Graham AR, Richter LC, Barker GP,
Krupinski EA, Lopez AM, et al. Overview of
telepathology, virtual microscopy, and whole slide
imaging: prospects for the future. Hum Pathol.
2009;40:1057–69.
Wilbur DC. Digital cytology: current state of the art
and prospects for the future. Acta Cytol. 2011;55:
227–38.
18 Pathology Informatics 513