Embed Size (px)
Citation preview

Molecular Events involving ~ 2 7 ~ ~ ' , p53, HER-2/neu, and ER in Multistep Progression of Breast Cancer
A THESIS SUBMllTED TO THE FACULTY OF
GRADUATE STUDIES IN PARTIAL FULFILLMENT OF
THE REQUIREMENTS FOR THE DEGREE OF MASTER
OF SCIENCE
Submitted by: Ninos Yacoub. B.Sc.
Department of Laboratory Medicine & Pathobiology Faculty of Medicine
University of Toronto Sunnybrook and Women's College Health Sciences Centre

National Library l*l of Canada Bibliothéque nationale du Canada
Acquisitions and Acquisitions et Bibliographie Services services bibliographiques 395 Wellington Street 395. r w Wdlinglm OmwaON K1A ON4 OnawaON K t A W CaMda canada
The author has granted a non- exclusive licence aliowing the National Library of Canada to reproduce, loan, distribute or seii copies of this thesis in microform, paper or electronic formats.
The author retains ownership of the copyright in this thesis. Neither the thesis nor substantial extracts from it may be printed or othenvise reproduced without the author's permission.
L'auteur a accordé une licence non exclusive permettant à la Bibliothèque nationale du Canada de reproduue, prêter, distribuer ou vendre des copies de cette thèse sous la forme de microfiche/film, de reproduction sur papier ou sur format électronique.
L'auteur conserve la propriété du droit d'auteur qui protège cette thèse. Ni la thèse ni des extraits substantiels de celle-ci ne doivent être imprimés ou autrement reproduits sans son autorisation.

ABSTRACT
Despite a wealth of research resources induding tissue cultures. cell lines.
and antibodies. the genetic alterations responsible for the development and
stepwise progression of breast cancer a n still unclear. Cytogenetic and
molecular analyses have failed to identify consistent gene deletions, mutations,
translocations, or amplification in sporadic cases of breast cancer. Earlier work
using monoclonal antibodies has however provided a basis for in vitro
charaderkation of breast cancers by defining a variety of breast cancer-
associated molecular events. These events mediate important functions such as
growth regulation, dl-cell adhesion, differentiation and proteolysis. In this study.
the analysis of some of the most well characterized molecular marken in breast
cancer has shown that rnolecular events involving the Estrogen Reœptor (ER).
~ 2 7 ~ ~ ' . p53 and HER-Zneu are mainly involved in the progression from low
grade disease to high grade disease as assessed by their immunohistochemical
expression. As a result. there seerns to exist a more well defined dissociation
between the mechanism of intraductal progression and the mechanisms involved
in the progression to invasion in breast cancers. Future functional studies of
these individual rnolecular events will lead to a better understanding of the
pathogenesis of breast cancer and of potential targets for rational therapy.

iii
Ac knowkdgements
I would like to gratefully acknowiedge the help and support 1 have reœived
during my graduate training. 1 wouid like to thank Dr. Charies Catzavelos for
accepting me as his first graduate student and providing guidance and support in
both my academic training and research project.
I wold also like to thank al1 members, past and present, of the lab whose
advice and friendship have been invaluable.
I want to gratefully acknowledge the guidance and encouragement I have
received from my wmmittee rnembers: Dr. lan Dubé, Dr. Serge Jothy, Dr. Joyce
Slingerland and Dr. Jorge Filmus, and the additional support I have received from
Dr. Richard Jordan and Dr. Sarrna.
Finally, I would like to thank my parents for their encouragement and
moral support that 1 received during my graduate training.

TABLE OF CONTENTS
Ackno wledgements .......................................................................................... Table of Contents ............................................................................................
.................................................................................................. tist of Tables ................................................................................................. List of Figures
.................................................................................................... List of Plates List of Abbreviations .........................................................................................
1 . INTRODUCTION ..................................................................................
2 . THE MOLECULAR BASIS OF TUMOUR PROGRESSION ...........................
............................................................................... 2.1 Oncogenes 2.2 Tumour-Suppressor Genes ..........................................................
..................................................... 2.3 Genes that Regulate Apoptosis ................................................. 2.4 Genes That Regulate DNA Repair
2.5 Invasion ................................................................................... ........................................ 2.6 General aspects of Multistep Progression
2.7 Molecular Basis of Colon Cancer Progression ..................................
3 . BREAST CANCER PROGRESSION .........................................................
.............................................................................. 3.1 Epidemiology 3.2 Histopathology of Breast Carcinoma ............................................... 3.3 Molecular Events in Breast Cancer Progression ................................
3.3.1 Earl y Morphologie Changes ................................................ .................................................... 3.3.2 Estrogen Receptor (ER)
....................................................... 3.3.3 HER-2heu (c-erbB-2) ............................................................................... 3.3.4 p53
...................................................................... 3.4 Deletional Studies 3.5 Comparative Genomic Hybndization (CGH) .....................................
.................. 3.6 Differentiation-Relationship to Breast Cancer Progression 3.7 Current Models of Breast Cancer Progression ..................................
4 . INVESTIGATION OF MOLECULAR MARKERS IN BREAST CANCER ................................................................................... PROGRESSION
4.1 ~ 2 7 ~ ~ ' Levels in Multistep Breast Cancer Progression .......................
METHODS 4.1.1 Patient population and statistical methods ............................ 4.1.2 Tissue preparation .......................................................... 4.1.3 Aminoalkylsilane (APES) .................................................. 4.1.4 Pre ration of Antibodies & Reagents ................................. Cl p27 ..........................................................................
Secondary Antibody (BA-2000) .......................................... ImmunoPure DAB ........................................................... VECTASTAJN ABC ......................................................... Citrate Buffer Solution ......................................................
4.1.5 lmmunohistochemistry Protocol ..........................................
iii iv vi vii viii ix

RESULTS 4.1.6 Results ......................................................................... 89
........................... 4.2 Molecular Events involving ER . HeNneu. and p53 100 ...................................................................... 4.2.1 Rationale 100
METHODS ............................ 4.2.2 Patient population and statistical methods 701
...................................................... 4.2.3 Imrnunohistochemistry 101 ..................................... 4.2.4 Additional Preparation of Antibodies 102
Her2heu (c-erbB-2) ............................................... 102 ........................................................... E-cadherin 103
ER ..................................................................... 103 p53 .................................................................... 104
RESULTS .......................................................................... 4.2.5 Results 104
DISCUSSION ....................................................................................... 127
FUTURE STUDIES ............................................................................... 154
REFERENCES .................................................................................... 157

vi
LIST OF TABLES
Distribution of histotogic types of breast cancer ............................................ 25
Expression levels of molecules versus morphological subtypes ....................... 65
Clinicopathologic features of the cohort studied ............................................ 75
Tabulation of grade versus patient age in cohort (n=203) ................................ 77
Summary of immunohistochemical results based of ~ 2 7 ~ ~ ' expression ............. 91
Immunohistochemical data on molecules studied in synchronous in situ and invasive carcinoma ........................................................................... 107
........ Imrnunohistochemical data on molecules studied for pure in situ carcinoma 109
immunohistochemical data on molecules studied for pure invasive carcinoma ..... 110
......... lmrnunohistochemical data on molecules studied for metastatic carcinoma 111
Various correlations found between morphological subtypes and molecules studied .................... .. ......................................................................... 114
............. Statistical data for order of molecular events using the McNemar's Test 117
Statistical data for order of molecular events using lnterrnediate Grade ...................................................................................... tumour analysis 137

vii
LIST OF FIGURES
Fiuure
A Genetic Mode! for Colorectal Tumorigenesis ...........................................
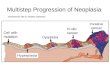
Oiagram showing normal cell maturation pathway .......................................
Diagrams showing possibie developrnent of tumour cells .............................
Morphological continuum mode1 of breast cancer progression .......................
Combination mode1 of breast cancer progression .......................................
Stochastic mode1 of breast cancer progression ..........................................
Analysis of p2pP' protein by immunohistochemistry ..................................
Diagrammatic representation of data for p27'OD' adivity ...............................
Model of Breast Cancer Progression .......................................................
In v h re presentation of breast cancer progression ....................................
Re~resentation of multi~le ~athwav ~oaression in breast cancer ...................

viii
LIST OF PLATES
Plate - 1.
II.
111.
IV.
v.
VI.
VII.
p27'OP1 expression in in M u . invasive and metastatic breast carcinoma ............................................................................................ 95
Top Figure (a) Low grade pure ductal carcinoma in situ (DCISk- ~ 2 7 ~ ~ ' IHC (b) High grade pure dudal carcinoma in situ - p27 IHC
Middle Fqure (a) Low grade ductal carcinoma in situ - ~ 2 7 ~ " IHC (b) Hgh grade dudal aircinoma in s lu --27ffip' IHC (c) L w grade invasive carcinoma - p27 O' IHC (d) High grade invasive caranorna - ~ 2 7 ~ ~ ' IHC
Bottom F@un (a) Low grade ductal carcinoma in situ - ~ 2 7 ~ ' ' IHC (b) High grade dudal carcinoma in situ --27)<ip' IHC (c) LOW grade invasive carcinoma - p27 IHC (d) High grade invasive carcinome - p27@P' IHC (e) Low grade metastatic carcinoma - ~ 2 7 ~ ~ ' IHC (f) High grade metastatic carcinoma - ~ 2 7 ~ " IHC
lntralesional progression of breast cancers.. ................................................ 120 (A) Low grade dudal carcinoma in situ - p27"' IHC (8) Low grade invasive carcinoma - high ~ 2 7 ~ ~ ' IHC (C) High grade invasive carcinoma - low ~ 2 7 ~ ~ ' IHC
lmmunohistochernical expression of Estrogen Receptor (ER) in Breast Cancer.. . 122
Immunohistochemical expression of HER-Uneu (erbB-2) in Breast Cancer.. ...... 122
Immunohistochemical expression of p53 in Breast Cancer .............................. 124
l mmuno histochemical expression of E-cadherin in Breast Cancer.. ................... 1 24
Intraiesional Progression in Breast Cancer using al1 factors studied.. ................. 141

ADH BRCAI BRCA2 CGH CIN cis DCC DCIS OClSG DNA E-cad €CM ER GRi3 HER-2 HG HSR IG IDC IHC INV ILP LG LN LOH MBRGR MET PDWA PsR RER RNA
ix
LIST OF ABBREVlATlONS
Atypical Dudal Hyperplasia Breast Cancer related gene 1 Breast Cancer related gene 2 Comparative Genomic Hybridization CeMcal Intraepithelial Neoplasia Carcinoma in situ Dextran-Coated Charcoal Ductal Carcinoma In situ Dudal Carcinoma In situ Grade Deoxyri bon udeic Acid E-Cadherin Extracellular Matrix Estrogen Receptor Grade (histologie) Human Epithelium Receptor-2 High Grade Homogeneously Staining Regions Intermediate Grade Infiltrating Ductal Carcinoma Immunohistochemistry Invasive lntralesional Progression Low Grade Lyrnph Node Loss of Heterozygosity Modified Bloom-Richardson Grade Metastasis Proliferative Disease without Atypia Progesterone Receptor Replicative Error Ribonudeic Acid

CHAPTER 1
INTRODUCTION

1. INTRODUCTION
Breast cancer is the second most common cause of cancer death in
women overall and the most common cause in women aged 40-59 (Chu et al.,
1996). Despite recent advances in detection and management of this disease,
approximately 40% of patients will ultimately die of metastatic carcinoma
(Dupont and Page. 1985). The genetic alterations responsible for the
development and stepwise progression of breast cancer remain unclear and
there is not a universally accepted model of breast cancer progression. An
understanding of the process by which progression to disseminated disease
occurs is vital to continued improvement in the management of breast cancer
patients. To investigate the mechanisms involved in the development of this
cancer we undertook the series of studies presented herein. We believe that
these studies contribute to Our understanding of breast cancer progression and
provide the basis for further study. We also believe that a closer look into the
potential molecular events underlying both early and later stages of breast
cancer will yield greater insight into the specifics of breast cancer progression
and its future management.

CHAPTER 2
THE MOLECULAR BASIS OF TUMOUR PROGRESSION

2. THE MOLECULAR BASIS OF TUMOUR PROGRESSION
Tumour progression is a multistep process involving the accumulation of
genetic damage leading to progressive deregulation of normal cellular function
and increasingly malignant behavior culminating in the development of
metastases. Cancer is caused by genetic abnomalities that can be induced in
many different ways. Non-lethal genetic damage can results from environmental
agents such as chemicak, radiation, viruses, or it may be inherited in the gerrn
line. The genetic hypothesis of cancer implies that a tumour mass results from
the expansion of a single progenitor cell that has incurred genetic damage from
one or more of these factors. This phenomenon is the basis of the clonal
evolution of tumoun(Fujii et al.. 1996). Originafly, it gave rise to the terms
"initiationn and "promotion" of cancers (Huberman. 7988). These phases do not
however, explain why the tumours continue to develop in a neoplastic manner
after the stimuli have lcng ceased. Shortly after realizing that random genetic
damage occurs in normal tissue, it was shown that certain specific mutations
affecting several classes of genes resulted not only in initiation and promotion of
neoplasms, but also in progression to disseminated metastatic disease. There
are three classes of normal regulatory genes that are the main targets of genetic
damage. These are growth promoting proto-oncogenes, growth inhibiting tumour-
suppressor genes (antioncogenes), and genes that regulate programmed cell
death or apoptosis (Weinberg, 1996). Mutant alleles of protoonwgenes are
considered dominant when they transfomi cells despite the presence of their
normal counterpart gene. In contrast, both normal alleles of the tumour

suppressor genes must be damaged for transformation to occur, thereby acting
in a recessive fashion. Genes that regulated apoptosis may be dominant or
recessive acting and can behave either as oncogenes or tumour suppressor
genes. In addition to the three classes just mentioned, a fourth category of genes
that regulate the repair of damaged DNA is also important for tumour growth and
developrnent. The DNA repair genes nonnally repair non-lethal damage in other
genes, including protooncogenes, turnour suppressor genes, and genes that
regulate apoptosis. An inability to carry out these repain c m predispose the cell
to neoplastic transformation. A mutation in this class of genes would require the
inactivation of both alleles to induce this instability (Johannsdottir et ai., 1999).
DNA repair genes can therefore be considered to behave in a similar fashion to
tumour suppressor genes. Tumour progression involves several distinct phases
that include dysregulation of growth, loss of differentiation, invasion, and
metastasis. Malignant neoplasms have several phenotypic characteristics, such
as excessive growth, invasiveness and metastatic potential. It is becoming more
widely accepted that carcinogenesis is a muttistep process at both the genetic
and phenotypic levels and that progression is guided by a series of sequentially
activated rnolecular factors(Fearon and Vogelstein, 1990). T O gain a further
appreciation of the regulatory function of these classes of genes in the normal
condition, it is necessary to explain in slightly more detail the characteristics of
each class.

2.1 Oncogenes
Protoonwgenes are cellular genes that promote normal growth and
differentiation. Protooncogenes may become oncogenic by retroviral transduction
(v-oncs) or by influences that alter their behavior in situ. thereby converting them
into cellular onwgenes (c-oncs)(Jansen-Durr, 1996). Oncogenes and their
oncoproteins are altered versions of their normal counterparts and are grouped
according to their role in the signal transduction cascade and cell cycle
regulation. There are five major categories of oncogenes: growth factors, growth
factor receptors. proteins involved in signal transduction, nuclear regulatory
proteins, and ce11 cycle regulators (Sherr, 1996). The alteration or activation of
these oncogenes is brought about by two broad categories of change. Firstly,
changes in the structure of the gene subsequently result in the formation of an
aberrant oncoprotein with aberrant function(Yamashita et al., 1993). This may be
triggered by point mutations. Secondly, changes in the regulation of gene
expression may result in amplified or enhanced production of a structurally and
functionally normal growth-promoting protein(Yarnashita, et al.. 1993). This may
be triggered by chromosomal rearrangements that translocate a gene placing it
in the control elements of a different gene. Translocation-induced overexpression
of a protooncogene is best exemplified by Burkitt lyrnphoma(Gerbitz et al.. 1999).
These tumoun involve chromosome 8q24, where the c-myc gene has been
mapped, as well as an immunoglobulin gene-carrying chromosome(Gerbitz, et
al., 1999). At its normal locus, the expression of the myc gene is tightly controlled
and is expressed only during certain stages of the cell cycle(Cole and McMahon,

1999). In Burkitt lymphoma, the most common form of translocation results in the
movement of the c-myc-containing segment of chromosome 8 to chromosome
14q, placing it under the control of the immunoglobulin heavy-chain (IgH)
gene(Gerbit2, et al., 1999). The translocation can render the c-myc gene subject
to relentless stimulation by the adjacent enhancer element of the immunoglobulin
gene or the translocation can cause mutations in the regulatory sequences of the
myc gene(Gerbit2, et al.. 1999). In al1 instances, the coding sequences of the
gene remain intact, and the c-myc gene is constitutively expressed at high
levels(Gerbitz, et ai., 1999) facilitating its oncogenic activity. Another possible
mechanisrn is by gene amplification that may produce several hundred copies of
the protooncogene in the tumour cell. The amplified genes can be readily
detected by observing double minutes and HSR (homogeneously staining
regions) regions in a karyotype or by molecular hybridization with the appropriate
DNA probes(Fegan et al., 1995). The HER-2lneu gene is amplified with resultant
overexpression of its protein product, p185neu'e*B2, in 15-40% of primary human
breast turnours, suggesting a role for this receptor in breast cancer(Hynes and
Stern, 1995). This thesis will investigate the role of the HER-2lneu oncoprotein in
the progression of breast cancer.
2.2 Tumour Suppressor Genes
Unlike protaonmgenes that promote cell growth, the products of tumour
suppressor genes provide the checks and balances necessary for homeostasis.
Similar to mitogenic signals. growth inhibitory signals originate outside the cell

and act via receptors, signal transducers, and cell cycle and nuclear transcription
regulaton to accomplish their effects. Some major categories of tumour
su p pressor genes include ce11 sudace receptors. molecules involved in signal
transduction, and, most im portan tl y, molecules that regulate nuclear transcription
and the ce11 cycle. The first tumour suppressor gene diswvered was Rb(Kaelin,
1997; Lin, 1996). The product of the Rb gene, pRb, is a nuclear phosphoprotein
that plays a key role in regulating the cell cycle(Kaelin, 1997). It is expressed in
every cell type examined, where it exists in an active underphosphorylated and
an inactive hyperphosphorylated state(Kaelin, 1997). In its active state, pRb
serves as a brake on the advancement of cells from the G1 to the S phase of the
ce11 cycle(Kaelin, 1997). When the cells are stimulated by growth factors, the Rb
protein is inactivated by phosphorylation (pRb-P) and the cells clear the G7 to S
checkpoint(Kaelin, 1997; Sherr. 1996). Once the cells enter S phase, they are
committed to divide without additional growth factor stimulation(Kaelin, 1997;
Sherr, 1996). During the ensuing M phase, the phosphate groups are removed
from pRb by cellular phosphatases, thus regenerating the dephosphorylated forrn
of pRb(Sherr, 1996). p53 is another tumour suppressor gene that has been
widely studied in a variety of cancers. It is a nuclear phosphoprotein involved in
several important functions including regulation of the cell cycle (Levine et al.,
1991) and programmed cell death (Shimamura and Fisher, 1996). The
expression pattern of this molecule will be investigated in this thesis to determine
its potential importance in the progression of breast disease.

2.3 Genes that Regulate Apoptosis
It is now appreciated that genes that prevent or induce programmed ceil
death are also important variables in cancer (Wyllie, 1997). A large farnily of
genes that regulate apoptosis has been identified. Antiapoptotic genes include
bci-2 and bcl-xL, whereas others, such as, bax, bad and bcl-xS favour
programmed cell death(Eissa et al., 1999). At least two other genes are key
players in the pathway to apoptosis. Activation of p53 c m up-regulate bax
synthesis and hence, counteract the antiapoptotic action of bcl-2(Fortuno et al.,
1999). The presence of bcl-2 in breast cancer correlates with favorable prognosis
and high tumour differentiation(Bonetti et al.. 1999), although increased levels of
bcl-2 may lead to aberrant accumulation of cells(Del Bufalo et al., 1997; Rochaix
et al., 1999). c-myc can coordinate with bcl-2 in tumourigenesis(Sherr, 1996;
Sierra et al., 1999). c-myc c m trigger proliferation. while bcl-2 can prevent cell
death in a synergistic manner to promote metastasis in breast cancer(Sierra, et
al., 1 999).
2.4 Genes That Regulate DNA Repair
When a strand of DNA is replicating, mismatch repair genes act as "spell
checkers". If, for example, there is an erroneous pairing of G with Tl the
mismatch repair genes correct the defect (Marra and Boland, 1996). Without
these proofreaders, errors slowly accumulate in several genes, including
protooncogenes and tumour suppressor genes. DNA repair genes themselves
are not oncogenic, but they allow mutations in other genes during the process of

normal cell division. Cells with such defects in DNA repair are said to have the
replication e m r (RER) phenotype. which can be readil y documented by
examination of microsatellite sequences in the tumour cell DNA (Allen, 1995;
Eshleman and Markowitz, 1996). Approximately 24% of colorectal tumours
affecting the proximal colon have been found to contain mutations in the
mismatch repair genes of cells leading to the development of an RER
phenotype(Johannsdottir. et al.. 1999). With errors in mismatch repair. there are
expansions and contractions of the microsatellite repeats in tumour cells,
creating alleles not found in normal cells of the same patient. This microsatellite
instability is a charactefistic of mismatch repair genes.
2.5 lnvasion
lnvasion involves a camplex series of mordinated molecular events that
lead to degradation of the basement membrane and escape of neoplastic cells
from their normal anatomic compartments into the surrounding connective tissue,
the extracellular matrix (ECM). Further invasion of the ECM enables the turnour
cells to gain access to blood and lyrnphatic vessels which creates the potential
for dissemination to distant sites and the formation of metastases.
Specific processes contributing to local invasion in cancers include the
following(Edwards and Murphy, 1998):
2.5.1 Disruption of tumour cell-ce11 and cell-rnatnx interaction:

Epithelial (E) cadherins mediate homotypic adhesions in epithelial tissue,
thus serving to keep the epithelial ceHs together(0ka et al., 1993). In several
epithelial tumours, including adenocarcinornas of the colon and breast, there is a
down-regulation of E-cadherin expression(Moll et al., 1993). Presumably, this
down-regulation reduces the abitity of ceils to adhere to each other and facilitates
their detachment from the primary tumour and their advance into the surrounding
tissues. To penetrate the surrounding extracellular matrix, the tumour cells must
first develop a means by which to adhere to the matrix components. There
seems to be a carrelation between the invasiveness and the density of laminin
receptors in carcinomas of the breast and colon facilitating this interaction(Price,
1997). In addition to laminin-specific receptors, tumour cells also express
integrins that can serve as receptors for many components of the extracellular
matrix, including fibronectin, laminin, and collagen(Ziober, 1996).
2.5.2 lncreased ceIl motility:
Locomotion is the next step of invasion, propelling tumour cells through
the degraded basement membranes and the ECM. Migration seems to be
mediated by two categories of molecules: (a) motility factors(Guirguis et al.,
1987; Verhasselt et al., 1992) and (b) cfeavage products of the ECM(Coopman et
al., 1998). Hepatocyte Growth Factor (HGF) is found at the interface of cancer
cells and extracellular matrix, its expression is markedly upregulated in a number
of cancers including breast(Bevig1ia et al., 1997) and can facilitate the scattering
of cells. Cleavage products derived from collagen and proteoglycans, have been

found to have growth-promoting, angiogenic, and chemotactic
activities(Cham bers and Matrisian, 1 997).
2.5.3 Upstream regulation of protease expression:
Invasion of the matrix is not brought about by passive growth pressure,
but rather requires the activation of enzymes specialized for degradation of
matrix components(P~ce, 1997). Tumour cells secrete proteolytic enzymes
themselves in addition to inducing the secretion from other cell types. At the
invading edge of tumours, the balance between proteases and antiproteases is
tilted in favor of proteases(Liotta and Kohn, 1997). A major protease family
includes the matrix metalloproteinases (MMPs) which can cleave collagen fibers
in the ECM(Liotta and Kohn, 1997). MMPs are activated by a molecule called
uPA (urokinase plasminogen activator) which converts plasminogen into its MMP
activating form plasmin(Kwaan. 1992).
2.5.4 lncreased proteolytic activiw
An increase in proteolytic activity comes from the secretion of yet another
class of proteases, the cysteine proteinase cathepsin D(Andreasen, 1 997).
These enzymes act on a large variety of substrates, including fibronectin,
taminin, and proteoglycans(Andreasen, 1 997). Levels of these enzymes are
elevated in several animal and human tumours. Levels of cathepsin D in the
tumour cells and serum seem to be prognostic in patients with breast cancer
(Tetu et al., 1 999; Zheng et al., 1999).

2.5.5 Decreased pmtease inhibitor expression:
Levels of tissue inhibitors of the metalloproteinases (TIMPs) are markedly
reduced in invading tumours favoring the continued degradation of activated
forms of MMPs (Iwata et al., 1995).
2.5.6 Enhanced angiogenesis:
Levels of a vascular endothelial factor (VEGF) have been shown to be
elevated near the invasive front of invading cancers(Folkman, 1994). VEGF
promotes the formation of neovasculature as a preparatory measure for the more
advanced spread of the tumour(Folkman. 1994).
Each step in the invasion sequence is subject to a multitude of influences,
and hence at any point in the sequence, the breakaway cell may not survive.
Studies in mice reveal that although millions of cells are released into the
circulation from the prirnary tumour site, only a small subset of metastasis
actually form(Giavani et al., 1980). The genetic basis for this seeming
inefficiency lies in the fact that tumours are heterogeneous with respect to
invasive and metastatic potential. That is, only certain subclones possess the
right combination of gene products to complete al1 the steps outlined above.

2.6 General aspects of Multistep Progression
Specific pathological findings and distinct genetic hereditary or somatic
alterations seem to be major factors that are in some way linked to the risk of
developing cancer and, in the latter stages, to the spreading of the disease. In
recent years the model of multistep carcinogenesis of cancer combining specific
pathological findings and distinct genetic alterations has becorne a central
paradigm of cancer biology (Thompson. 1994) (El-Ashry and Lippman, 1994)
(Black, 1994) (Busch, 1990). As early as 1855 Virchow alluded indirectly to
genetics when he noted from cell theory not only 'Omnis cellula e cellula', that al1
cells corne from cells, but also 'Omnis cellulae e cellula ejusdem generis', that al1
cells corne from the cells of the same type. In the case of cancer. a single cell
may be the beginning of the malignant process.
2.7 Moleculai Basis of Colon Cancer Progression
Many current models of tumour progression are based on the linear
paradigm proposed by Vogelstein and colleagues for colon cancer(Fearon and
Vogelstein, 1990). In this model, the risk of invasion increases as lesions
progress along the morphologie spectrum and consequently, in colon cancer,
invasion is seen only in association with high grade precursors, i.e., progression
from low to high grade precursors is required for invasion. The detailed
pathological knowledge of adenorna-carcinoma development in colorectal
carcinogenesis led to investigations into the genetic alterations occurring during
this process. While longitudinal observation of these changes is not feasible,

cross-sectional analyses involving the careful pathological examination of large
numbers of adenornas and carcinomas and the genetic changes associated with
them led to the determination of the sequence of genetic events and their
timing(Cho and Vogelstein, 1992; Fearon and Vogelstein, 1990). Fearon and
Vogelstein detected (a) APC mutation or loss in normal mucosa and
hyperproliferative epithelium, (b) K-RAS mutation in adenoma, (c) DCC loss in
adenoma, increasing in size and with dysplasia, and (d) TP53 loss in invasive
and metastatic cancer(Fearon and Vogelstein, 1990). These studies reinforce the
notion that progression occun as a result of both activation of oncogenes and
inactivation of tumour suppressor genes.
In the studies of colorectal tumourigenesis by Vogelstein and CO-workers,
the findings were that colorectal tumours appear to arise as a result of the
mutational activation of oncogenes coupled with a more predominant mutational
inactivation of tumour suppressor genes (Figure 1 )(Fearon and Vogelstein ,
1990). Second. additional mutations in at least four to five genes are required for
the formation of a malignant tumour and fewer than four are required for
adenoma formation or begin tumours(Fearon and Vogelstein, 1990). Third,
althoug h the genetic alterations often occurred according to a particular
sequence of events, the total number of changes rather than their order is most
important in detennining the tumour's biological properties(Fearon and
Vogelstein, 1990). The model of figure 1 illustrates a linear and biologically
reproducible sequence of events that guides the avolution of the tumour to more

Figure 1. A Genetic Model for Colorectal Tumourigenesis. The three stages of adenomas are defined in Figure 1 initially. These stages represent tumours of increasing size, dysplasia and villous content. A mutation on chromosome 5q is responsible for the development of familial adenomatous polyposis (FAP). This alteration may be responsible for the hyperproliferative epithelium present in t hese patients. Subsequent hypomethylation is present in very srnall adenomas in patients with or without polyposis. Mutations in the ras gene appear to occur in one cell of a preexisting srnall adenoma and through clona1 expansion produces a larger and more dysplastic tumour. The chromosomes most frequently deleted are 18q and 17p. The putative target of the loss event on each chromosome is indicated as well as the relative timing of the chromosome loss event. Tumours continue to progress once carcinomas have formed, and the accumulated loss of suppressor genes on additional chromosomes correlates with the ability of the carcinomas to metastasize and eventually cause death (Fearon, 1 990).

GENE: FAP
Normal Hyperprdiferatwe Epithelium Epithelium
ONA 1
CHROMOSOIVE: 5, 12P 18q i 7 ~ ALTERATION : MUTATION OR LOSS MUTATION LOSS LOSS
K- ra s DCC? ~ 5 3
ALTERATIONS HYPOMETHY iATlOPJ
Early Adenorna
I ntermediate Aden orna
Carcinoma Melastasis Adenoma

and more malignant phenotypes. Although rudimentary, the model does provide
a framework for the study of the independent steps involved in a cornplex human
disease. There are several implications of the model. A pathway can rnight offer
several discrete targets for chemotherapeutic action. In addition, risk increases
as one moves along the morphologie spectrum in which precursors are
considered 'low' risk and invasive lesions 'high' risk aiding in the prognosis and
identification of surgical andlor high nsk candidates. Moreover, the discovery of
genetic changes restricted to neoplastic cells suggests that early-stage colorectal
tumors may be possible, perhaps through the identification of mutant gene
products or through the detection of antibodies made by the patient against the
mutant gene products(Fearon and Vogelstein, 1 990).

CHAPTER 3
BREAST CANCER PROGRESSION

3. BREAST CANCER PROGRESSION
Breast cancer cells differ from normal counterparts in many important
characteristics. These characteristics incfude loss of differentiation, uncontrolled
growth, immortalization, loss of contact inhibition, increased invasive capacity,
the ability to evade the host immune surveillance, the ability to evade the
apoptotic signaling restraints, and induction of neo-angiogenesis(E1-Ashry and
Lippman, 1994) (Thompson, 1994). The presence of a ductal system within the
breast creates an additional cornplexity in the growth and evolution of a
malignant focus. As a result, the progression of the tumour is not as predictable
as in other solid tumour cancers such as colon or cervix. The complexity and
diversity was initially exemplified by epidemiological and histopathological data
compiled from breast cancer patients in a multitude of studies(Page and
Anderson, 1987; Pike et al., 1993; Silverstein, 1997; Thompson, 1 994).
3.1 Epidemiology
In the United States, the incidence of breast cancer has been rising for the
past three decades (Chu, et al., 1996). In 1997, for example, 181,600 new cases
of breast cancer were diagnosed and 44,190 people died of breast cancer during
that year(Chu, et al., 1996). Since then, the incidence and mortality has slightly
decreased (Chu, et al., 1996). A widely quoted statistic is that one in nine women
will develop breast cancer in her lifetime, while one in twenty-five will die from it.
The National Cancer lnstitute of Canada (NCIC) estimates that 18,700 Canadian

women will be diagnosed with breast cancer and that 5.400 will succumb to it in
1999 (Lilia, 1999). In Ontario alone. more than 7,000 new cases are reported and
approximately 2,000 women die each year(Lilia, 1999). Although breast cancer
affects men and women, male patients make up less than one percent of al1
cases (Lilia, 1999). Breast cancer therefore, remains a significant contributor to
morbidity and mortality in the female population. There are several identified risk
factors for breast cancer. The most well characterized is the effect of unopposed
estrogen exposure that is caused by early menarche, late menopause and
nulliparity(Madigan et al., 1995). All of the above associations between
reproductive and menstrual factors and risk of breast cancer point towards
reproductive hormones as possible etiological agents. A large amount of
endocrine biochemical research has been done investigating the roles of various
components of estrogen and other hormones including progesterones, prolactin,
androstenedione, and aetiocholonalone(Helzlsouer et al., 1994; Kostoglou-
Athanassiou et al., 1997). Atypical fobular or ductal hyperplasia and benign
breast disease also rnarginally increase the risk(Page and Dupont. 1990a). Other
risk factors are early exposure to ionizing radiation, long-ten postmenopausal
estrogen-replacement therapy, and possibly alcohol consumption and smoking.
The most important risk factor however, is a family history of breast cancer
(Anderson, 1992). About 5 to 10 percent of al1 breast cancers occur in high risk
families and there are several familial breast cancer syndromes that include the
Li-Fraumeni syndrome characterized by individuals that have inherited a
mutation of the p53 allele(Akashi and Koeffler. 1998), Cowden's disease

characterized by individuals with who have a mutation of a gene on chromosome
1 O(Schweitzer et ai., 1999), and the breast-ovarian cancer syndrome in whom
individuals possess inheritable mutations on the BRCA1 and BRCA2 genes
believed to be involved in mediating the repair of DNA(Miki, 1994).
One of the key studies with regard to predisposing factors in the
development of breast was performed by Page and associates in a study that
evaluated 10,366 benign breast cancer patients and deterrnined their risk for the
development of subsequent cancer (Page et al.. 1978). This study showed that
women with benign proliferative disease had a relative risk of 2x, those with
atypical ductal hyperplasia 4x. and those with ductal carcinoma in situ (DCIS)
1 1 x (Page, et al., 1 978).
3.2 Histopathology of Breast Carcinoma
Breast cancer is believed to originate in the ductal epithelial cells of the
terminal ducts. Malignant transformation is indicated microscopically by the
presence of morphological changes within the individual cells and by the way in
which these cells are arranged in relationship to each other. As long as the
proliferating malignant cells are present within the confinement of the basement
membrane surrounding the ducts, acini. or the covering surface epitheliurn of the
nipple, the tumour is considered as in situ carcinoma. When the basement
membrane is breached and the malignant cells are seen infiltrating the breast
stroma and tissue spaces, the tumour becornes an invasive carcinoma. The

tumour cells in both in situ and invasive carcinoma may be arranged in a variety
of ways or exhibit specific features that are used in providing the basis for the
histological classification of breast carcinoma. In ductal carcinoma in situ (DCIS).
the involved ducts are markedly enlarged and may appear distorted, but they
preserve a welf-defined contour surrounded by a basement membrane. DCIS
accounts for approximately twenty percent of breast cancer(Silverstein and
Poller, 1 995). Invasive ductal carcinoma accounts for approximately ninety
percent of invasive tumours(Page and Anderson. 1987). The majority of invasive
ductal carcinomas contain foci of intraductal carcinoma. In this study, a co-
existence of in situ and invasive disease will be referred to as mixed disease.
Twenty to thirty percent of cases show pure invasive carcinoma with no apparent
in situ components(Page and Anderson, 1987). Breast cancers show a wide
spectrum of behaviour and a number of factors that predict behaviour have been
developed. The principle prognostic factors in invasive breast cancer include
stage, axillary lymph node status, tumour grade, tumour size, steroid hormone
receptor status, and s-phase fraction(Page and Anderson, 1987). Turnour grade
is currently determined by the modified Bloom-Richardson grading systern that
assigns scores for architecture, nuclear grade, and the number of
mitoses(Fentiman and Taylor-Papadimitriou, 1993).
Breast carcinomas display considerable heterogeneity with regard to both
the amount of DClS associated with the invasive component and the spectrum of
grades in both the in situ and invasive component. The variability of breast

cancer can best be illustrated by reference to Table 1, which shows the forms of
breast cancer seen.
Table 1 shows that a considerable amount of genetic diversity must exist
to account for the extreme morphologie heterogeneity of breast cancers seen in
the clinicat setting. Progression in breast cancer is thought to take place via a
series of morphologically definable precursors, including atypical ductal
hyperplasia and ductal carcinoma ni situ (DCIS) that are thought to precede
invasive cancer and the development of metastatic disease. Three phases of
breast cancer progression can be defined. lntraductal progression refers to the
progression from low grade to high grade in situ carcinoma. In addition, there is
the transition from in situ to invasive cancer and progression from low to high
grade invasive carcinoma. It has been assumed that breast cancer follows the
linear paradigm proposed for colon cancer. There is growing molecular evidence
however, to suggest that this is not the case.
3.3 Molecular Events in Breast Cancer Progression
3.3.1 Early Morphologie Changes
Unfortunately, Iittle is known about the evolution of human breast cancer.
lnvestigators have been unable to identify with certainty morphological, cellular or
molecular events that genuinely lead to invasive disease. Epidemiological studies
have shown that certain subsets of these proliferative lesions are statistically
associated with the later development of breast cancer and provide the few clues

Table 1. Represents the distribution of generalized histologie types of breast cancers seen. The majority of breast cancers seen in the clinical setting are of the invasive variety. Invasive tumours are more readily detected mammographically and are often detected by the patient. In situ disease is less common and more dificult to detect. The majority of women who have in situ disease develop ductal carcinoma in situ as opposed to the rarer lobular carcinoma in situ which afflicts the terminal lobular units. (Robbins, Pathologic Basis of Disease 6" Ed.)

Table 1. Distribution of histologic types of breast cancer
Type of Breast Cancer % pop. with disease
In situ carcinoma 15%-30%
Ductal carcinoma in situ 80%
Lobular carcinoma in situ 20%
l nvasive carcinoma 70%-85%
Reference: Robbins, Pathologie Basis of Disease 6th Ed.

we have regarding early breast cancer evolution. In a retfospective study
involving over 10,000 patients, it was shown that hyperplastic, atypical
hyperplastic, and non-invasive neoplastic lesions were associated with 2-fold, 5-
fold, and 10-fold increased relative risks, respectively, of eventually developing
invasive carcinoma (Page et al., 1985). More recent studies have found that
hyperplastic lesions and non-invasive cancer are concurrently present in the
large majority of breasts containing invasive cancer (Kintanar and Raju, 1991).
Together, these studies are consistent with the notion that many invasive breast
cancers arise from hyperplastic lesions. A working hypothesis of breast cancer
evolution has therefore, been suggested based on these studies that show a
progressively increased relative risk of subsequently developing invasive
carcinoma. Ninety percent of breast cancers originate in the duct cells of the
breast(Fentiman and Taylor-Papadimitriou, 1993). It is believed that these normal
duct cells can undergo changes causing them to increase in number and size.
This is known as Usual Hyperplasia or Proliferative (Fibrocystic) Disease
Without Atypia (PDWA)(Kintanar and Raju, 1991 ). As changes continue, some of
the rnorphologic features seen in ductal carcinoma in situ appear, but al1 the
features for this diagnosis are not present. This is known as Atypical Ductal
Hyperplasia (ADH), which represents a pre-rnalignant stage in breast cancer
evolution (Kintanar and Raju, 1991). At a later stage in progression, cells fiII and
distort the ducts and show increasing evidence of malignancy although they
remain contained within the rnamrnary ductaf system. The phases of h yperplasia,
atypical hyperplasia, and in situ carcinoma are thought to be

reversible(Silverstein, 1997). Most women diagnosed with DClS do not appear to
go on to develop clinically apparent invasive breast cancer (perhaps 5-25%,
depending on histologie type. mode of detection, and whether "treatedw by biopsy
alone or lumpectomy with or without radiation)(Silverstein, 1997). The time taken
for cells to undergo these events may Vary from one individual to another. but the
process likely takes yean rather than months or days. It is only through a series
of additional genetic anomalies and continued rnolecular progression that the
lesions acquire malignant potential and develop the in situ and invasive
carcinomas commonly seen. The following pages describe in more detail some
of the more well characterized molecular events involved in breast cancer.
3.3.2 Estrogen Receptor (ER)
The estrogen receptor is a protein responsible for the binding and uptake
of estrogen by normal cells and breast cancer tissue(McCarty et al., 1985).
Studies have suggested a biochemical mechanism for estrogen action. Estrogen
diffuses easily across cytoplasmic membranes and binds to its specific receptor
protein(Pike, et al., 1993). The majority of receptors reside in the nucleus in
loose association with nuclear components. As estrogen binds to its receptor, a
hormone-receptor wmplex with high affinity for nuclear chromatin is
formed(Pike, et al., 1993). This hormone-receptor complex interacts with specific
DNA sequences to mediate transcription of messenger RNA that is then
translated into specific proteins. One of these estrogen-regulated proteins is the
progesterone receptor (PR), which is required for progesterone activity. Other

proteins include growth factors that alter proliferation of the tumour cells or
adjacent stroma1 tissues (Lippman et al.. 1986).
Prognostic factors are very important in breast cancer because they allow
the identification of groups of high risk patients in whom adjuvant therapy may
lead to an improved prognosis. Estrogen (ER) and progesterone (PgR) receptors
have been extensively studied and are now considered prognostic factors in
clinical practice (Wollenweider-Zerargui et al., 1988) (Clark and McGuire, 1988)
(Molino et al., 1992). The presence of these receptors is norrnally detemined by
means of a biochemical technique using dextran-coated charcoal
(DCC)(McCarty, et al., 1985). The availability of monoclonal antibodies that
recognizes ER has led to the development of an immunohistochernistry (IHC)
technique for evaluating the presence of ER protein(Pertschuk et al., 1985).
Unlike the biochemical assay, immunohistochemistry requires only small
quantities of tissue, allowing the heterogeneity of ER distribution and the content
in each cell to be evaluated and is not affected by the level of endogenous
steroids. A number of studies have shown a good carrelation between the two
methods (Patterson et al., 1 990) (Pertschuk, et al., 1985) (McCarty, et al., 1 985)
and another study also demonstrated that the presence in tumour tissue of more
than 10% of cells that are positive at estrogen receptor assay by IHC is a good
index of overall positivity (Molino et al., 1995). Estrogen receptor expression can
be characterized in both invasive and carcinoma in situ. Studies have shown ER
expression in in situ carcinoma correlates with pathologic features of

differentiation and is similar to that of invasive carcinoma (Bur et al., 1991). ER
positivity has been seen in both in situ and invasive disease and has shown an
inverse correlation with grade in 98% of cases studied by other groups (Bur, et
al., 1991). Only a small number of studies have addressed estrogen expression
across low-, intemediate-, and high grade tumours(Leal et al.. 1995; Zafrani et
al., 1994). Not standardization of scoring parameters were followed and cohort
sizes averaged less than 30 cases. The majority of studies have only examined
low- and high grade cases but have shown that the general trend of ER
expression was that of elevated levels in low grade disease and markedly
reduced levels in higher grade disease(Barnes and Masood. 1990; Helin et al..
1989). The greatest limitations of these studies was the wide variability in the
scoring methodology used. Some studies deterrnined ER positivity based on
observation of greater than 0% of cells staining with dark nuclei, while others
chose higher cut-offs of S%(Chaudhuri et al., 1993). 10%(Albonico et al., 1996).
20%(Barnes and Masood, 1990) and 25%(Giri et al., 1989).
3.3.3 HER-2heu (c-erbB-2)
The HER-2lneu oncogene encodes a transmembrane tyrosine kinase
receptor with significant homology to the epiderrnal growth factor receptor
(Press, 1994). HER-Uneu has been widely studied in breast cancer and its
amplification and overexpression in breast cancer tissue has been correlated
with poor prognosis in women(Revillion et al., 1998). HER-2lneu is also amplified
in DCIS, predominantly in high grade lesions (Zafrani, et al.. 1994). In studies

categorizing DClS into low and high grade subtypes. the average incidence of
HER-Uneu overexpression was very low (about 15%)(Bartkova et al.. 1990) and
very hig h (about 75%)(Zafrani, et al.. 1 994). respectively. Intemediate grade
lesions showed intemediate rates of overexpression (approximate average 40%)
in the very few studies categorizing DClS into three histologic grades(Polbr et
al., 1994) (Bobrow et al., 1994). It has been shown by a recent phase III dinical
trial that systemic administration of anti-HER-Uneu antibodies like Heneptin,
alone and in combination with cytotoxic chemotherapy in patients with HER-
Zlneu overexpressing primary breast tumours, can increase the time to
recurrence and overall response rates in metastatic breast cancer (Ross and
Fletcher, 1998). In an attempt to evaluate the reliability and reproducibility of the
immunohistochemical staining of the HER-aneu oncoprotein from paraffin-
embedded material, studies comparing HER-2heu IHC staining and protein
product levels have been performed with good correlation(Liu et al., 1992;
Tannapfel et al., 1996). A variety of studies have demonstrated that a positive
stain can be considered to be specific for HER-Uneu in both invasive and in situ
lesions if (i) there is definitive staining along the tumour cell membrane with no
predominant immunoreactivity inside the tumour cell cytoplasm, (ii) the degree of
irnmunoreactivity is comparable with a positive standard and (iii) the surrounding
normal, non-neoplastic tissue shows no immunoreactivity (Tannapfel, et al.,
1 996). Studies have shown that HER-Uneu overexpression occurs in anywhere
from 24% (An et al.. 1997) to 32% (Houston et al.. 1999) in invasive breast
carcinoma. HER-Zneu overexpression has been previously correlated with high

grade, ER negative invasive lesions(Silverstein and Poller, 1995). In the context
of a model for breast cancer progression, the finding that high levels of HER-
Zneu expression are found in approximately 80% of high grade, cornedo-type
DClS (Allred et al., 1994), are interesting. Although the general trend in HER-
2Ineu expression in the Iiterature has demonstrated that there exists a noticeable
overexpression in higher grade disease, there are studies, using sirnilar scoring
parameters and source of tissue which have shown irregularities in the
expression pattern. Ramachandra et al reports similar levels of HER-Plneu
overexpression in both low- and high grade in situ disease (50% and 62%.
respectively). Another study has reported a decrease in the degree of
overexpression in intermediate grade tumours compared to low grade tumours
(low grade= 1 7%, intemediate grade=l O%)(Leal, et al., 1 995). A major limitation
of both of these studies was their srnall cohort size (approx. ne50).
3.3.4 p53
The nuclear transcription factor p53 is a tumour suppressor gene (Levine,
et al., 1991). It is mutated in about 47% of breast tumours (Baker et al., 1989)
while other investigators have demonstrated mutation rates in 30%-40% of
turnours (Andersen et al., 1993) using immunohistochemical techniques. The p53
gene is the single most wmmonly mutated gene in cancer and functional
homozygous loss of the p53 gene is found in virtually every type of cancer,
including carcinomas of the lung, colon, and breast (Greenblatt et al., 1994).
There are two methods by which the p53 gene is inactivated. Somatic mutations

affect both alleles of p53. while inherited mutations affect one allele of p53 and
predisposes individuals to develop malignant tumours because only one
additional "hitn is needed to inactivate the second, normal, allele (Greenblatt. et
al., 1994). p53 is a negative modulator of cellular proliferation presumably by
negatively affecting transcription of growth stimulatory genes or positively
affecting transcription of growth inhibitory genes. It is thought that p53 functions
on several levels. Normal p53 acts to monitor levels of ONA damage and to shut
down replication if repair is required(Silvestrini et al., 1996). It acts very much like
a "gatekeeper" for the cell cycle(Silvestrini. et al.. 1996). An increase in p53
levels due to DNA damage or hypoxia causes pS3 to bind to DNA and transcribe
a set of target genes(Levine, et al.. 1991). One of these genes is p21 an inhibitor
of the cyclin/CDK complexes(El-Deiry et al., 1993). Such a pause in the cell
cycling is necessary because it allows the cells time to repair the DNA damage
inflicted by the mutagenic agents. p53 also transcribes a gene called GADD4S
(Growth Arrest and DNA Damage), which produces a protein that assists in Gl
arrest and DNA repair(Lane, 1992). If the DNA damage is repaired successfully,
p53 activates a gene called mdm2. whose product serves to down-regulate
levels of p53, thus relieving the cell cycle block (Lane and Hall, 1997). If repair
fails, p53 transcribes a gene called bax which is involved in mediating the
pathway to apoptosis(Basu and Haldar, 1998). The most common mutations that
disable p53 affect its DNA-binding domain, and thus prevent the p53-dependent
transcription of the above mentioned genes allowing for selection of unstable celt
populations(Lane, 1992) (Hartwell, 1992) (Vogelstein and Kinder, 1992). Mutant

p53 gene products fomi tetramers with the nona l p53, thereby decreasing its
ability to regulate cell growth and giving these cells a selective
advantage(Greenblatt, et al.. 1994). It has been demonstrated that one mutant
p53 protein in the tetrameric wmplex is capable of inducing cellular
transformation, presumably by inactivating the remaining normal p53 molecules
in a dominant-negative fashion(Greenb1att. et al.. 1994).
Previous studies have shown that the presence of detectable p53 protein
in breast cancer is correlated with increased tevels of HER-2lneu
oncoprotein(Martinaui et al.. 1993). It has been reported that p53
overexpression as detennined by any antibody is associated with patients' failure
to respond to endocrine therapy (Home et al.. 1996). suggesting a possible
dis ru ption in the estrogen receptor pathways of these turnours. A contentious
issue regarding p53 protein overexpression concems the relationship to p53
mutations. It is generally accepted now that mutation and overexpression are
correlated (Baas et al.. 1994). However, with some discordance in the literature.
a more acceptable t e n to use to interpret p53 activity, is 'stability". Normally.
p53 protein in a cell. has a short half-life (20 minutes)(Greenblatt et al.. 1994)
and cannot be detected by immunohistochemistry. In the presence of mutations.
the half-life of the protein increases and the altered p53 protein can therefore be
detected by this technique. There are no other studies that specifically address
the issue of whether p53 predicts risk of relapse in patients with DClS or the risk
of progression to invasive cancer. Therefore, p53 expression cannot currently be

used to make clinical decisions about the treatment of DCIS. It has been
previously shown that the presence of detectable p53 protein in invasive breast
cancer is significantly correlated with poor tumour differentiation and poor patient
prognosis(Yamashita, et al., 1 993). Another study has shown that mutations
within a highly conserved region of the p53 gene leading to overexpression of the
protein product can occur in early (in situ) phases of breast cancer and this
alteration is maintained during progression from intraductal to invasive cancer
(Davidoff et al., 1991 ). In low grade DCIS, mutations and/or elevated p53 protein
levels are relatively rare, averaging about 5% incidence (Walker et al., 1991). In
contrast, high grade DCIS commonly has p53 alterations averaging about 50%
incidence(Tsuda et al., 1993), which is comparable to the tevels in invasive
breast cancer (Elledge et al., 1993). The majority of data on p53 expression in
breast cancer comes frorn studies that have used low sample sizes (usually less
than 50 cases); a variety of assaying and scoring techniques; and different
source material for assessrnent (paraffin and/or frozen tissue). While the majority
of studies have shown a larger incidence of p53 alteration in high grade disease,
one studies has reported a greater incidence in low grade DCIS (21%) as
compared to high grade counterparts (3%) using immunohistochemistry and a
cohort size of n=23 (Schmitt et al., 1995). To help reduce discrepancies and
overcorne the limitations of these various studies, there is a clearer need in the
literature for a standardized systern for evaluating p53 in breast tissue, which will
eventually help to uncover the role of p53 in cancer progression.

3.3.5 E-cadherin (E-cad)
The initial step of cancer invasion and metastasis is the escape of cells
from the primary tumour, involving disruption of normal cell-cell adhesion in the
epithelial tissue(Ne1son et al., 1990). Turnour cell detachment results frorn the
d ysreg ulation of cell ad hesion molecules(0ka. et al., 1 993). E-cad herin (E-cad) is
a subclass of the cadherin family, which consists of functionally related
transmembrane glycoproteins responsible for the ca2'-dependent dl-cel l
adhesion mechanism(0ka. et al.. 1993; Takeichi. 1991). E-cadherin is crucial for
cell-cell epithelial adhesion and epithelial tissue integrity (Nelson, et al.. 1990).
Antibodies raised against cadherins are able to block intercellular adhesion and
promote cell invasion in malignancies. as shown by in vitro models (Behrens et
al., 1989). In poorly differentiated breast cancers, E-cadherin is expressed
weakly or not at all(Moll, et al., 1993). In invasive breast carcinomas with an
intraductal component. the strong E-cadherin expression of the in situ component
complimented the equally prominent and sornewhat heterogeneous expression
of the invasive component(Hashizume et al., 7996; Rasbridge et al., 1993).
Malignant cells in other breast tumoun like lobular carcinoma have typically a
pattern of single-file infiltration and is consistent with low levers of E-cadherin
expression(Rasbridge, et al., 1993). In contrast, ductal carcinomas typically form
infiltrating cohesive islands of cells. sometimes with organization into tubular
structures. consistent with continued E-cadherin expression(Rasbridge, et al.,
1993). Its down-regulation can however favour the formation of an invasive
phenotype and eventual rnetastasis(0ka. et al., 1993). The prognostic

significance of E-cadherin expression in tenns of overall survival in breast
carcinomas has been investigated using immunohistochernistry on both frozen
and paraffin embedded tissue sections and long-terni patient follow-up(Siitonen
et al., 1996; Umbas et al.. 1994). Reduced expression of E-cadherin correlates
with tumour de-differentiation(Shimoyama and Hirohashi. 1991 ) (8ecker et al.,
1994) (Bohm et al.. 1993). high grade(Shimoyama and Hirohashi. 1991) (Umbas,
et al., 1994). stages (Kinsella et al., 1993) (Umbas, et al., 1994). lymph node
invasion (Kinsella, et al.. 1 993). distant metastasis recurrence (Oka. et al., 1 993).
and decreased survival (Umbas, et al., 1994).
3.3.6 p2pp'
The cell cycle is governed by a family of cyclin-dependent kinases (cdks),
and their associated cyclins(Morgan, 1995). ~ 2 7 ~ ~ ' is a cyclin-dependent kinase
inhibitor that regulates the progression of the cell cycle from GI into S phase by
binding to and inhibiting the actions of cyclinlcdk complexes(Polyak et al., 1994)
(Slingerland et al., 1994) (Hengst et al.. 1994). ~ 2 7 ~ ~ ' binding to target cdks is
up-regulated by growth inhibitory cytokines such as transforming growth factor4
(TFG-R), providing an important connection between the extracellular
environment of the cell and its cell cycle controls(Hengst, et al., 1994;
Slingerland, et al.. 1994). Levels of ~ 2 7 " ~ ' are predominantly regulated post-
translationall y by the Ubiquitin degradation system(Pagano. 1 997). Furthermore,
decreased ~ 2 7 " ~ ' levels in tumours do not occur as a resuit of mutations
(Morosetti et al., 1995) (Tanaka et al.. 1997). It has recently been reported that

~ 2 7 ~ ~ ' has a role in regulating drug resistance in solid turnours (St. Croix et al.,
1996). Recently, studies have even implicated ~ 2 7 ~ ~ ' as a key player in the
pathway to apoptosis (Katayose et al., 1997) (Levkau et al., 1998). There have
also been studies which have shown that ~ 2 7 " ~ ' has a role in the regulation of
differentiation in some tissues (Zabludoff et al., 1998). Two lines of evidence
indicate that ~ 2 7 ~ ~ ' suppresses cell proliferation in vivo. Malignant ceIl
transfection with the ~ 2 7 ~ ~ ' gene leads to inhibition of proliferation and cell cycle
arrest in G1 (Polyak, et al., 1994; Toyoshima and Hunter, 1994). Mice lacking the
~ 2 7 " ~ ' gene show an increase in body weight. thymic hypertrophy. and
hyperplasia of pituitary cells. adrenal glands and gonadal organs (Fero et al.,
1998; Kiyokawa et al., 1996).
Drs. Catzavelos, Slingerland and collaborators undertook a study to
determine the prognostic utility of ~ 2 7 ~ ~ ' levels in breast cancer(Catzavelos et
al., 1997). For a new prognostic marker to enter into routine clinical use at least
three criteria must be met (Steeg and Abram, 1997): (a) the marker provides
information independent of and better than conventional pathological criteria. (b)
The marker provides information that can alter treatment decisions. (c) Studies
with the rnarker are reproducible.
The Sunnybrook study(Catzavelos. et al.. 1997). showed that loss of
~ 2 7 ~ ~ ~ ' ( ~ 5 0 % cells positive) was a strong predictor of shorter disease-free
suwival on univariate analysis (p=0.0072, relative risk 2.256). Kaplan-Meier

curves of disease-free survival and survival in patients with low ( 6 0 % cells
positive) venus high ~ 2 7 ~ ~ ' (>50%) showed a significant separation within 2
years of follow-up (P=0.005 and 0.05. respectively) (Catzavelos, et al., 1997). In
a multivariate analysis. ~ 2 7 ~ ~ ' was a strong independent predictor of diminished
disease-free survival (P=O.Ol7OI relative risk 2.3 1 5) (Catzavelos, et al., 1 997).
This study also has shown that ~ 2 7 ~ ~ ' is consistently decreased. with increasing
tumour grade, in primary breast cancer and may be important in tumour
progression (Catzavelos. et al.. 1997). Decreased levels of this protein may
result in loss of sensitivity to negative growth regulatory cytokines and in altered
protiferative potential. difierentiation and intercellular adhesion. This study
concluded that reduction of ~ 2 7 ~ ~ ' protein is a strong predictor of poor outwme
in women with breast cancer and has potential for becoming an independent
prognostic rnarker and rnay therefore be used as part of the routine pathological
assessrnent of patients with breast cancer if these findings were confirmed in a
larger cohort of patients. Concurrent studies by other groups (Porter et al., 1997)
(Tan et a/.. 1997) support results of the Sunnybrook study. These three studies
suggest that alterations in the level of ~ 2 7 ~ ~ ' protein may play a role in breast
cancer progression. The Sunnybrook pilot study however, focused mainly on
invasive carcinomas of the breast and did not address to any great detail ~ 2 7 ~ ' ~ '
levels in relationship to the different stages of breast cancer progression. In
addition to epithelial tumoun, lymphomas(Erlanson et al.. 1998) and
neuroectoderrnal tumours including gliomas (Mizumatsu et al., 1999) have been
used to test ~ 2 7 " ~ ' as a possible prognostic marker.

3.4 Deletional Studies
Loss of heterozygosity (LOH) of polymorphic genetic marken is thought
to reflect the general chromosomal locations of tumour suppressor genes in
which the random loss of one allele (e.g., as may occur with deletions,
nondisjunctions, or recombinational errors such as sister chromatid exchange)
unmasks a mutated and nonfunctional allele on the other chromosome,
conferring a growth advantage leading to clonal expansion of cells with the
alteration(Sratton et al., 1995). In breast tumours, LOH represents the most
frequent type of genetic aberration. LOH has been reported at significantly high
levels in varying proportion of breast cancers at specific chromosomal regions.
such as 1 p, Iq, 3p, 6q, 7p, 11 p, 13q. 16q, 17p. 17q. 18p. 18q and 22q (Aldaz et
al., 1995; Radford et al., 1995a). The incidence of loss varies for different
regions, with the most frequent loss being on 16q and lfp(40%-60%)(Aldaz, et
al., 1995; O'Connell et al., 1994; Radford et al., 1993) while losses in the other
regions are seen in about 15-20% of tumour cases(0'Connell. et al., 1994;
Radford et al., 1995b). Unfortunately, there is considerable variation in the
frequency of LOH at the same locus arnong different researchers (Ali et al.,
1 987) (Chen et al., 1 992).
There are a number of studies that have demonstrated correlations
between LOH and various pathobiological parameters of mainly invasive breast
tumours. For example, LOH on chromosome 17q carrelates with estrogen

receptor-negative cancers (Ito et al.. 1995). Some studies have demonstrated
an association between LOH on 18q and higher tumour grade(Sainsbury et al.,
1987). while others have not (Radford, et al., 1993). Due to small sample size
and multiple techniques used for measunng LOH, statistical biases are
inevitable(Radford, et al.. 1 993) (Radford, et al., 1993). However, such
correlations are useful for generating hypotheses that can be independentty
validated with larger databases using one quantifying procedure.
With the application of sensitive techniques of DNA analysis, it has been
possible to correlate histologic and genetic alterations in small but
uncontaminated microdissected sampies of various histological stages of breast
cancer(6ornstein et al.. 1998; Koreth et al., 1995). This alfows two important
issues in breast cancer progression to be addressed directly: (1) the clonal
relationship between the pre-invasive and invasive lesions at the genetic level;
and (2) the existence of any order of events in which genetic changes may occur
during progression. One study has compared LOH of alleles on chromosome 17
in subtypes cf DClS (Radford, et al., 1993). The data show LOH on 17p in 29%
of the DClS cases that include cornedo. cribiform and mixed DCIS of both high
and low nuclear grades(Radford, et al., 1993). In contrast, LOH at 17q was not
found in the DClS cases, although it was cornmonly observed in other studies of
invasive tumours (Andersen et al., 1992). Therefore, it appears that the genetic
changes on 17p may be important in the initiation of DClS while those on 17q
may be important for either the invasive phenotype or other aspects of later

stages of progression. Another study has compared the incidence of LOH on
1 lq23 in in situ, invasive and metastatic breast cancer(Koreth, et al., 1995).
Although there was some similarity between LOH frequency (or its absence) in in
situ and invasive disease, and in invasive and metastatic lesions, some cases in
this study showed discordance between lesions from the same patient.
Furthermore, it was observed that LOH on 11q23 wuld manifest at any time
during disease progression (Koreth, et al., 1995). These findings lend support to
the stochastic model of breast cancer progression which asserts that the
acquisition of genetic aberrations in the pathways of progression is governed
largely by the laws of probability(Smith et al., 1993). This group also
demonstrated that LOH on 11q23 often occurs in pre-invasive stages, and can
alsc be manifested after the turnour has become metastatic(Koreth, et al., 1995).
Therefore, LOH at 1 lq23 is probably not essential for the invasive phenotype.
Other groups have compared LOH on 1 lq13 in microdissected in situ and
invasive tumours. In every case where the in situ tumour showed LOH, the same
allele was lost in the corresponding invasive tumour (Zhuang et al., 1995). The
authors concluded therefore that their study provided molecular genetic support
for the hypothesis that invasive breast cancer arises from in situ lesions. In more
comprehensive follow-up studies evaluating more than 100 cases of OClS at 14
independent loci across 10 chromosomes, they have since found that more than
80% of pure low grade and high grade DClS contained at least one LOH (often
many more), and that DClS and invasive cancers from the same breasts with
LOH shared the same losses more than 70% of the time(OIConnell et al., ).

Similar findings have been reported recently by other groups (Munn et al., 1995)
(Fujii, et al., 1996) (Radford, et al., 1995b; Zhuang, et al., 1995) including one by
Lakhani, et al, showing genetic refatedness between carcinoma in situ and
synchronous invasive breast cancer(Lakhani et al., 1995). In the majority of
lesions analyzed in al1 these studies, two patterns of LOH were described. The
majority of these studies found correlations between loss of heterozygosity and
the grade of the in situ and associated invasive lesions, by showing similar
percentage losses(Aldaz. et al.. 1995; Radford. et al., 1995b). Some studies
however have shown a pattern for LOH in which there is no change in the in situ
lesion but there are significant deletional events in the associated invasive
lesions(Bose et al., 1998). A study which examined the loss of heterozygosity for
markers on 10q23, found that none of the DClS components studied showed
loss while close to 70% of the invasive components had loss suggesting that a
gene(s) at this locus is important in the transition from in situ to invasive
carcinoma (Bose, et al., 1998).
3.5 Comparative Genomic Hybridization (CGH)
A recently developed technique, comparative genomic hybridization
(CGH), allows analyses of chromosome copy number abnormalities involving
segments of at least 1 OMb (Kallioniemi et al.. 1994). CGH involves hybridizing
differentially labeled genomic DNA from a tumour and a n o n a l cell population to
the same normal metaphase(Pinke1 et al., 1998). It circumvents some of the
difficulties encountered in conventional karyotyping. Through such analyses,

nearly every tumour analyzed revealed increased or decreased DNA sequence
copy number (Kallioniemi, et al.. 1994). The most cornmon regions of increased
copy number in breast cancer as deterrnined by CGH include lq, 8q(Tirkkonen
et al., 1998). l7q22-24(Barlund et al., 1997). and 20ql3(Tanner et al.. 1995).
lncreased copy nurnber at 17q was previously determined through gene
fluorescence in situ hybridization (FISH) analysis to be 50 to 100-fold
amplification of ER862 (HER-2heu) (Kallioniemi et al., 1992), a gene known to
be amplified in a considerable percentage of breast cancers. Amplification at
region 8q24 represents c-myc, another gene known to be amplified in some
breast cancers (Shiu et al., 1993). No candidate gene has yet been identified for
reg ion 20q 1 3 amplification.
Although CGH has defined many amplified chromosomal regions
(amplicons) that are seen in a proportion of breast cancers, the majority of target
genes have not yet been defined. One problem is that the amplified regions are
large chromosomal segments containing many different genes. Because of the
increased copy number of these genes. many may be overexpressed even
though they do not contribute to the malignant phenotype. Regions of decreased
DNA copy nurnber were also observed and include 3p, 6q. 8p. 1 1 p. 12q. 1 3q,
and 17p (Gray et al.. 1994b). For some of these regional losses, candidate
genes exist that may be the target of deletion in the progression to a malignant
phenotype (see LOH above). More specifically, both RB7 (1 3q)(Tamura et al.,
1994)and TP53 (17p)(Lavarino et al.. 1998) have been shown extensively to

undergo deletion in a significant fraction of breast cancers (Cox et al.. 1994).
Interestingly, when both loss and gain of DNA copy nurnber as detemined by
CGH were compared with survival data in a series of node negative breast
tumours, only copy number losses were significant for recurrence and for overall
survival (Isola et al., 1995). However, as is the case with conventional
cytogenetiw, CGH has yet to reveal any characteristic abnormalities that occur
in the majority of breast turnours and in what order the abnorrnalities occur(Gray
et al., 1 994a).
The number of identified genes for which there is clear evidence of a role
in the multistep carcinogenesis of breast cancer is still limited. Most information
is restricted to three oncogenes (c-erbB2(Kallioniemi, et al., 1992; Revillion, et
al., 1998), CCNDl locus(Barnes and Gillett, 1998), and c-myc(Shiu, et al., 1993))
and some turnour suppressor genes (TP53)(Andersen, et al., 1993; Davidoff, et
al., 1991 ; Greenblatt, et al., 1994), with mutations of BRCAl and BRCA2 playing
an important role in the familiar breast cancer syndrome(Miki, 1994). In sporadic
breast cancer it is very dificult to determine whether chromosomal imbalance or
mutations of loss or gain of a whole chromosome or chromosomal arm has an
effect on tumour development. Multiple candidate genes are located at a
chromosornai locus, and the specific participation of a given turnour suppressor
gene is therefore difficult to define. Simultaneous affectation of multiple
chromosomal loci bearing tumour suppressor genes or tumour cell heterogeneity
lead to different patterns of genetic alterations and therefore to differences in

tumour development. Furthemore, the number of irrelevant genetic alterations,
genetic imbalance or background. has yet to be defined(Gray. et al., 1994a).
Studies have shown that an almost identical profile for genetic gains and losses
occur between DClS and invasive carcinoma, fortifying evidence that DClS is a
precursor to invasive carcinoma(Buerger et al., 1999). Some studies have even
suggested a preferential order of certain genetic losses during the progression of
breast cancen(Tirkkmen, et al., 1998). Hot spots of chromosomal deletion
involved in the development of intraductal carcinoma may be able to be
determined to a limited extent by a combination of LOH and CGH. However, it
will be many years before we know the functions of al1 of the genes within the
present amplicons and until that time the relative importance of these genes can
only be speculated in the progression of breast cancer.
3.6 Differentiation - Relationship to Breast Cancer Progression
In studying breast cancer progression, it is important to understand
processes of normal cellular differentiation. In a normal cell, it is believed that an
'inducer' acts on a receptor to cause the sequential expression of a set of genes
whose purpose is to alter the phenotype of a cell such that it is completely
differentiated and specialized(Huberrnan, 1988). Breast epithelial tissue is
thought to arise from pluripotent stem cells that begin to mature after the
interaction of a specific inducer of differentiation with its appropriate cellular
receptor(Fentiman and Taylor-Papadimitriou, 1993). Following this interaction, a
series of cellular signals are transmitted from the receptor to the genome

causing, within a short periad of tirne, the activation and expression of specific
genes. presumably regulatory genes(Fentiman and Taylor-Papadimitriou, 1993).
The products of these early activated genes cause, through positive or negative
controls, a sequential expression of genes that code for the different grawth and
maturation functions, initially causing cell growth and then induction of cell
maturation (differentiation)(Huberrnan, 1988). Figure 2 senres to illustrate the
possible pathway to differentiation that a normal epithelial cell would
take(Huberrnan, 1988).
In this hypothetical modal, Gene A is activated by the inducer. In turn,
Gene A causes the activation of Gene B. Likewise Gene B causes activation of
Gene C, and Gene C activates Gene D, al1 of which code for cell maturation
functions. The product of Gene Dl which is expressed in the later parts of the
maturation pathway causes the suppression of a growth facilitating gene, Gene
G. If the mechanisms are allowed to occur without interference, the resulting
phenotype will be that of a tenninally differentiated cell with nomal function
which does not actively proliferate(Huberrnan. 1988).
In an abnormal situation. Figure 3 shows the possible development of a
tumour cell that is dysregulated. The growth-facilitating gene. Gene G, is
overexpressed because of gene amplification andlor gene restructuring (Section
2.1). Genes A and 6, but not C and Dl are expressed and Gene G is
overexpressed as a tesuit of its location in the pathway. This situation produces

Figure 2. Diagram showing normal cell maturation pathway. The "inducet' of differentiation interacts with its receptor and causes the expression of Gene A, which in turn activates Gene B, which in turn activates Gene C. In turn, Gene C activates Gene D. Gene D inactivates the gene that facilitates growth, Gene G. The resulting situation is expression of Gene A, B, C, and D, al1 of which code for cell maturation functions (e.g., polarity in epithelial cells of ducts), and suppression of the growth facilitating gene, Gene G. The resulting phenotype will be that of a terminally differentiated cell (e.g., milk-producing epithelial cells of the breast).

NORMAL CELL
DIFFERENTIATED STATE

tumour cells that exhibit a partially differentiated phenotype as a result of
interrupted maturation. and continuous cell growth (since gene 0. the gene that
normally causes suppression is not expressed)(Hubennan, 1988). A similar
situation can also occur following a loss of a gene(s) or gene rearrangement in
which a growth factor like a protooncogene rnay become part of the sequence of
the activated genes that code for the maturation functions(Hu berman. 1988).
As cancer progresses, there is gradua1 loss of the differentiation program.
Therefore in low grade forms of breast disease, it can be seen that the cells are
small, and there is to some degree. preservation of the normal architecture. That
is, many of the cells palisade around open spaces in an attempt to form lumens
for subsequent ductal formation, resembling normally growing cells. This is due
to at least a partial retention of the normal differentiation program that these cells
are attempting to follow. As tumoun progress, the cells become less responsive
to extracellular differentiation and growth control signais and lose their
differentiation program. This is evidenced by loss of polarity and changes in
cytoskeletal features that transfomi the shape of the cells(Slade et al.. 1999),
reduced levels of E-cadherin(Gamallo et al., 1993), and reduced levels of integrin
expression(Jonjic et al., 1993). This results in turnours which lack architectural
features characteristic of normal breast tissue.

Figure 3. Diagrams showing possible development of tumour cells. As in Figure 2, the inducer activates Genes A and B, as well as the translocated growth-facilitating gene, Gene G. Because Gene G is not capable of activating Gene C, this gene and Gene D are not expressed. Because of inactivation of Gene D, there is also no suppression of the growth-facilitating gene G as is described in Figure 2. The growth-facilitating gene, Gene G, c m also be overexpressed because of gene amplification or gene restructuring (e.g., activation of a potent promoter). Genes A and B, but not C and D, are expressed and Gene G is overexpressed. This situation produces turnour cells that exhibit a partially differentiated phenotype with enhanced cell growth. Gene G can be amplified in the genome (top diagram) or can be overexpressed (bottom diagram) to accelerate growth.

TUMOUR CELLS
GROWTH
GROWTH

3.7 Current Models of Breast Cancer Progression
There is an unusual degree of genetic heterogeneity and complexity that
has been identified during the progression of breast tumours(Kuukasjarvi et al.,
1997a; Patchefsky et al., 1989). Unlike colon cancers, where there is a
predictable stepwise accumulation of genetic events that lead from precursor
stages to invasion, the genesis of sporadic breast cancer rernains
eiusive(Dairkee and Smith. 1996). Ductal carcinoma in situ (DCIS) has been
considered a direct precursor of invasive ductal breast canmr (IOC)(O'Connell, et
a/., 1994). In a study that looked at genetic changes in intraductal breast cancer
using comparative genomic hybridization(Kuukasjarvi et al., 1997b). it was
revealed that there were identical changes between the in situ and invasive
components in one case, but substantial differences in another. It was the
conclusion of the researchers that a simple linear progression model may not
always account for the DCIS to IDC (ififiltrating ductal carcinoma) transitions that
are seen (Kuukasjafvi, et al., 1997b). In another related study which looked at
progression pathways of metastatic breast cancer, it was revealed that a linear
progression model is unlikely to account for the progression of pnmary tumours
to metastasis based on the genetic composition differences obtained between
the metastatic and prirnary tumours (Kuukasjawi, et al., 1997a).
In other epithelial systems like the colon, skin or cervix, it is believed that
dysplasia can progress over many years from a mild f o m of non-invasive
neoplasm (e.g., CIN-1, cervical intraepithelial neoplasia) through moderate

dysplasia (e-g., CIN-2) to severe dysplasia (e.g., CIN-3), eventually becoming
invasive(Ponten and Gw, 1998). In the breast, epithelial hyperplasia of usual
type, atypical ductal hyperplasia (ADH), and DClS are morphologically identified
lesions that have k e n shown to be associated with a risk of subsequent
development of invasive carcinoma (Jensen et al.. 1993). If the model of the
other epithelial lesions is followed, one would expect ductal epithelium to
progress frorn hyperplasia to low grade DClS and to evolve through moderate
grades to poorly differentiated DClS and then on to a spectrum of invasive
phenotype. Moreover, welt differentiated DCIS usually gives rise to a low grade
carcinoma when it becomes invasive and does not need to evolve through
moderate and severe dysplasia fi nt. If this were the usual mechanism of breast
cancer progression, a mixed differentiation of DClS might be expected in an
individual case as the lesion bewmes less differentiated over time until invasion
occurs. Invasive carcinomas would be associated with high grade DCIS alone.
which is not exclusively observed(Goldstein and Murphy, 1996). Breast cancers
are also unusual, in that tumaurs of similar stage and histology can have very
different clinical outcomes(Hortobagyi, 1998). At one extreme are the patients
who succumb to metastatic disease within a year of diagnosis. At the other
extreme, patients with cancers that appear similar may have 20 yean of disease-
free survival(Hortobagyi 1998). It is likely that this biological heterogeneity
among breast cancers at least partially results from the combination of genetic
lesions present in a given tumour.

Based on these observations, the following models of disease progression
have been considered for defining experimental approaches to investigate the
existence of an emerging order of genetic alterations in breast tumourigenesis.
The Morphological Continuum Model of Breast Cancer Progression
asserts that there is a linear continuity from normal to hyperplasia to atypia as
shown schematically (Figure 4) (Page and Dupont, 1990b). This model proposes
that this morphologic series represents the sequential course of breast tumour
progression(Page and Dupont. 1990b). Consistent with this model is the
discovery of atypias and in situ carcinomatous areas found in tissues adjacent to
most invasive carcinomas(Page and Dupont, 1990b).
Another model suggested by O'Connel1 et al (Figure 5 ) (O'Connell. et al.,
1994) supports the basic concept of progression from precursor lesions. It is
referred to as the Combination Model of breast cancer progression(O'Connel1. et
ai.. 1994). In addition. it proposes that some percentage of cases, invasive
lesions can result from any precursor lesion without necessarily evolving through
an intermediary lesion. It is diffcult to distinguish between the morphological
continuum and the combination models. Evidence that at least some invasive
carcinomas result from progression of atypias andfor ductal carcinomas in situ
cornes from comparative analysis of genetic lesions in invasive carcinomas with
those in adjacent atypias and in situ areas. In most cases. the lesions seen in
the noninvasive components represent a subset of those seen in the invasive

Figure 4. Morphological continuum rnodel of breast cancer progression. In this model, progression is serial and sequential and requires obligate intermediate steps of premalignancy, designated as atypia, and of preinvasive disease, designated as carcinoma in situ.

Normal
Carçinoma In Situ
Invasive Carçinoma
1 Metastatic Disease 1

Figure 5. Corn bination model of breast cancer progression. This model supports the basic concept of progression from precunor lesions. However, it also proposes that some invasive tumours may arise directly from any precunor stage without evolving through additional intermediate steps. DCIS= Ductal Carcinoma in situ.
a= Atypia which have the capacity to progress
b= Atypia which do not progress
c= DClS which has the capacity to progress
d= DClS which remains DClS

Morpliologically

components(Allred, et al., 1994). It is possible, though. to determine whether al1
invasive carcinomas anse via progression of non-invasive lesions. The fact that
some invasive cancers do not have visible adjacent noninvasive lesions suggests
a direct path from morphologically normal cells; however, the absence of
adjacent noninvasive components could potentially result from overgrowth by the
invasive cells (clonal expansion). Furthenore, obtaining direct evidence is
complicated by the fact that atypias and in situ carcinomas are surgically
removed whenever they are found. Therefore, the course that they follow can
only be speculated upon, but not directly wnfined.
The Stochastic Model of breast cancer progression has been proposed to
account for the extreme morphologie and biologic heterogeneity found in breast
cancers (Smith, et al., 1993). It asserts that there are four phenotypes associated
with malignancy: dysregulated proliferation. invasion, angiogenesis, and
metastasis. All of these can be acquired through more than one independent
genetic lesion and therefore it is possible to obtain two hundred and fifty six
different breast cancers (Smith, et al., 1993).
Recognizing the growing heterogeneity of breast cancer lesions. the
model set forth by Smith et al attempts to explain progression using
mathematical models. This model is wmmonly referred to as the Stochastic
Model of breast cancer progression(Figure G)(Smith, et al., 1993). This model
further states that the phenotypic changes required for invasive cancer rnay be

Figure 6. Stochastic rnodel of breast cancer progression. This model accounts for the extreme biological heterogeneity among breast cancers. Numbers 1-4 in each column represent a hypothetical set of 4 genes whose aberrant expression allows the acquisition of the 4 malignant phenotypes indicated. Thus a large variety of combination (256 in this example) are possible. During malignant progression, these genetic lesions are acquired stochastically. Depending on which genelgenes in the set becomes abnormal, the resulting tumour can be more or less aggressive in attaining the indicated phenotype. The rows represent the varying degrees of arbitrary levels of aggressiveness.

Weak D- 1
1 D-3
Aggressive D-4
4x4x4x4=256 different types of breast cancer

acquired in any order and the events are stochastic (govemed by the laws of
probability) (Smith, et al., 1993). In those cases where a cell acquires the ability
to invade before the ability for dysregulated growth, the invasive tumour will not
proceed through an in situ phase. Depending of which gene or genes in the set
becomes abnormal, the resulting tumour can be more or less aggressive in
attaining the indicated phenotype. If for example, a breast cancer cell is
incapable of completing a phenotypic step in the cascade, it will not successfully
metastasize. As an example with reference to Figure 6, mammary cells capable
of extensive and dysregulated growth (D) still require additional changes to
become fully malignant. Likewise, a cell that has gained the capacity for
degrading the basement membrane (1) will not progress if its proliferative activity
is not dysregulated. The resultant phenotypes will differ based on these
characteristic molecular traits and will contribute to the heterogeneous make up
of lesions. In the figure indicated, a large variety of combinations (256 in this
example) are possible. Since the genetic lesions are acquired stochastically, the
degree of aggressiveness (weak to aggressive in figure 6) is dictated by which
genelgenes in the set become abnormal.
At the cellular level, progression is mediated by the differential expression
or lack of expression of molecules involved in regulation of cellular activity. Some
of the best evidence for building a model of progression cornes from studies that
have attempted to characterize various molecules involved in creating the
diverse phenotypic nature of breast lesions. The following table (Table 2) serves
to summarize the growing data for the expression of some of these most well

characterized molecules involved in breast cancer research. The data obtained
thus far is hard to reconcile with a Iinear model of progression that predicts
invasive carcinoma to be a wnsistently later event in the evolution of the
disease. In table 2, positive values indicate the presence of significance
expression while negative values indicate negligible levels of expression of the
respective molecules. A positive value for HER-2lneu refiects overexpression of
the gene. A positive value for p53 indicates stability or mutation of the gene.
Negative values for p ~ 7 ~ ~ ' . ER and E-cadherin indicate reduction in expression
levels, whereas positive values are indicative of up-regulated levels. The table
specifically shows molecular expression venus morphologie subtypes in breast
cancer to be dysregulated.
Although the data in the literature is suggestive of variable expression of
these molecules in different types of cancer, there is still the need for a unifying
study which either confirms or opposes the dynamical expression profiles
indicated in Table 2. Some of the referenced studies had very limited cohort
sizes upon which to draw conclusions (eg. n=12) (Helin, et al., 1989). Low cohori
sizes may lead to misleading conclusions about the expression of a particular
rnolecule. For instance. in contrast to the majority of studies showing p53
alterations in association with higher grade disease, group studying p53
expression in DClS evaluated only 23 cases of breast cancer and observed that
21% of low grade cases should altered p53 levels while only 3% of high grade
turnours should indications of alteration(Schmitt, et al., 1995). Other studies have

Table 2. Represents the cullected tabulation of the expression levels of molecules versus morphological subtypes as determined in a variety of studies involving breast cancer. Positive values indicate the presence of significance expression while negative values indicate negligible levels of expression of the respective molecules. A positive value for HER-2lneu reflects overexpression of the gene. A positive value for p53 indicates stability or mutation of the gene. Negative values for p 2 7 ~ i ~ l , ER and E-cadherin indicate reduction in expression levels, whereas poslive values are indicative of up-regulated levels. The table specifically shows molecular expression versus morphologic subtypes in breast cancer to be dysregulated. The numbers in parenthesis reflect the reference from which the data was obtained. The corresponding references are listed on the bottom sequentially.

Table 2. Expression levels of molecules versus morphological subtypes
LG HG LG HG Molecules DClS DClS INV INV
REFERENCES: (1) van de Vijver et al, 1988 (2) Tsuda et al, 1993 (3) Ravdin et al, 1995 (4) Barns et al, 1990 (5) Helin et al, 1989 (6) Pallis et al. 1992 (7) Walker et al, 1991 (8) Tan et al, 1999 (9) Catzavelos et al, 1997 (10) Tan et al, 1997 (1 1) Siitonen et al, 1996 (12) Gupta et al, 1997

used exclusively frozen or fresh tissue based on the efficacy of their antibodies
and compared their results to other studies using paraffin tissue and different
antibodies. Assay parameters also varied from study to study (Table 2). Some
studies used a combination of techniques to detemine expression levels
including southern blotting(HERZ/neu)(Tsuda, et a 1 993), enzyme
immunoassays(ER)(Pallis et al.. 1992) and single strand conformation
polymorphism(SSCP)(p53)(Tsuda, et al., 1 993). Furthemore, it was not the
specific intention of these studies to address the role of these molecules in the
context of a model for tumour progression. Rather, the studies concentrated on
establishing prognostic or predictive value for a molecule. The studies rarely
examined expression of more than one of these molecular markers at a time, and
in many cases rarely categorized DClS and invasive cancers into low-,
intermediate- and high grades. Even fewer studies have attempted to analyze
the patterns of expression of these molecules in lesions of pure ductal carcinoma
or pure invasive carcinoma. There is growing need for a more focused study
analyzing the expression of molecular markers with the direct intention of
describing in more detail the pathways of progression in breast cancer.
The data extrapolated from the collection of studies on breast cancer
progression in Table 2 suggests that if one considers progression to be a linear
phenomenon in breast, that is. progression strictly from low grade in situ to
higher grade in situ lesions and then on to low grade invasive and high grade
invasive lesions, then it would require accepting that in each stage of

progression, the levels of expression of the molecules mediating the process be
altered more than once. For example, HER-2Jneu expression is low in low grade
DCIS. Evolution to higher grade DCIS is supported by elevated levels of HER-
Pheu, invasion to low grade infiltrating carcinoma is characterized by a reduction
in levels of HER-2/neu, and progression to high grade infiltrating carcinoma is
supported by yet another increase in expression of HER-Uneu. This is the same
sceoario of altered expression that exists in other molecules studied (Table 2).
AIthough there is some evidence explaining the local or temporal fluctuation in
levels of the rnolecule E-cadherin(Hashimoto et al., 1989; Kondapaka et al.,
1997). it is generally believed to be a metabolically costly proœss to radically
alter levels of expression of so many molecules in order to facilitate tumour
progression. If however, the data from Table 2 is grouped according to grade
(highllow) and not morphological subtypes (in situ I invasion), it can be seen that
for al1 molecules in question, only one alteration in the levels of expression is
required to produce the desired phenotype. This can adequately explain
progression from early in situ lesions to later aggressive infiltrating lesions.
Furthermore, this arbitrary grouping of lesions by grade and morphological
subtype may emphasize the existence of divergence in pathways to progression
of breast cancer. That is, there may be a set of molecular conditions which
mediate the progression from low to high grade disease and another set of
molecular conditions which mediate the progression of confined disease (in situ)
to infiltrating forms (invasive). Based on this critical finding of a possible multi-
step progression in breast cancer. my thesis project was to undertake a

molecular study of these markers in DClS and associated invasive cancers in
order to help clarify the problerns just explained.

CHAPTER 4
INVESTIGATION OF MOLECULAR MARKERS IN BREAST
CANCER PROGRESSION

4. INVESTIGATION OF MOLECULAR MARKERS IN BREAST CANCER PROGRESSION
The finding that ~ 2 7 ~ ~ ' levels show an inverse correlation with grade and is
an independent marker of prognosis led us to postulate that a reduction in ~ 2 7 ~ ~ '
levels may play a role in breast tumour progression. In the ~ 2 7 ~ ~ ' prognostic
study, in addition to the above mentioned data, Catzavelos et al noted a
correlation between the grade of the associated in situ and invasive components
and a strong correlation between ~ 2 7 ~ ~ ' levels in these cornponents (p=0.001)
as evidenced by the pattern of expression seen in Figure 7(Catzavelos, et al.,
1997). It was shown that there was a statistically significant association between
low grade DClS and elevated levels of ~ 2 7 ~ ~ ' protein expression. It was also
shown in this study that there was a statistically significant association of high
grade DClS with low levels of expression of the ~ 2 7 ~ ~ ' protein. This was shown
in both the in situ and invasive tumours of the cohort(Catzavelos, et al., 1997).
These findings suggested that progression in breast cancer may not follow
current linear models(Fearon and Vogelstein, IWO). To investigate this, we
performed a study to assess p27KiP' levels in relationship to the various stages of
breast cancer progression using a new cohort of patients which included pure
DCIS, mixed DClS plus invasion, pure invasive carcinoma, and metastatic
disease. The data from this study (Section 4.1 below) supported our hypothesis
and as a result, I extended the study to investigate the most well characterized
molecufar events in breast cancer progression, i.e., those involving ER, p53 and
HER-Uneu in the context of our model (Section 4.2.5 below).

Figure 7. Analysis of ~ 2 7 ~ ' ~ ' protei n by immunohistochemistry. a, lmmunohistochemistry shows high levels of ~ 2 7 " ~ ' protein in low-grade ductal carcinoma in situ (X40 magnification). b, Reduced ~ 2 7 ~ ~ ' protein in high-grade ductal carcinoma in situ . High levels of ~ 2 7 ~ ' ~ ' protein can be seen in the nuclei of adjacent normal ductal epithelial cells (X40 magnification). c, High levels of ~ 2 7 ~ ~ ' protein in well- differentiated invasive ductal carcinoma (X20 magnification). d, Reduced ~ 2 7 ~ ~ ' in high-grade invasive ductal carcinoma. A normal duct within the same field shown high ~ 2 7 ' " ~ ' protein staining (X20 mag nification). (Catzavelos et al, 1 997)


4.1 ~ 2 7 " ~ ' Levels in Multistep Breast Cancer Progression
4.1.1 Patient population and statistical rnethods.
In the work of this thesis, I studied ~ 2 7 ~ ~ ' levels in different stages of
progression in a consecutive series of primary breast cancers seen at
Sunnybrook & Women's College Health Science Center between 1996 and 1998
(n=203). This included 46 cases of pure ductal carcinoma in situ (DCIS) and 1 53
cases of ductal carcinoma in situ associated with invasive carcinoma. ln addition,
I determined ~ 2 7 ~ ' ~ ' levels in the associated lymph node metastases in 52 cases
frorn the latter group. The chi-squared test was used to analyze the statistical
significance between the expression of each molecule and the histological grade
for each table generated (Tables 3a 8 3b). P values e0.05 were considered as
statistically significant. Table 3a and 3b describe various clinicopathologic
characteristics of this whort. ~ 2 7 ~ ' ~ ' levels were determined by
immunohistochemistry and were considered high if 250% of the tumour cells
showed nuclear staining and low if <50% showed nuclear staining as in other
published studies(Catzavelos. et al., 1997; Tan, et al., 1997).
The following tables summarizes the various statistical characteristics of
the cohort studied. The average patient age was 61 years with an average size
of invasive tumour of 2.4cm and 25% of patients had axillary lymph node
metastasis (Table 3a). Based on this, the clinicopathologic features of this cohort
were representative of the population of breast cancer patients admitted to
Sunnybrook. Table 3b shows that in this cohort, 61% of the patients were greater

Table 3a. Represents the tabulation of the clinicopathologic features of the cohort studied (n=203). The average turnour size was made only for cases with an invasive component present.

Table 3a. Clinicopathologic features of the cohort studied
Mixed DClS INVASIVE COHORT DClS + INV ALONE ALONE AVERAGE
n=124 n=48 n=31
Average AGE (yrs.) 61.6 58 63.7 61 -1
AGE Range (yrs.) 28-91 40-93 36-92 28-93
Avg. Turnour Site 2.3cm NIA 2.4cm 2.4cm (size of invasive component)
Tumour Size Range 0.1-1 0.0cm NIA 0.6-9.0cm 0.1-1 0.0cm
Metastatic cases (LN) w 2 6 ) NIA 8(27) 52(25)

Table 3b. Represents tabulation of grade of the lesion versus the patient age in the cohort examined (n=203). The majority of women with breast cancer were greater than 55 years of age (61 %). The data also shows that 21 ?4 of women over the age of 55 develop low grade disease, while only 5% of the women under the age of 55 developed low grade breast neoplasia.

Table 3b. Tabulation of grade venus patient age in cohort (n=203)
AGE MlXED DClS ALONE INVASIVE COHORT AVG AVG AGE DClS + INV ALONE LG IG HG LG IG HG LG IG HG LG IG HG

than 55 years of age and 21% of these had low grade disease, while only 6% of
women less that 55 years of age had low grade disease.
4.1.2 7ïssue preparation.
Tumour tissues were received fresh in the Department of Pathology, were
dissected and block-sized pieces were fixed overnight in neutral buffered
formalin. Following primary fixation the blocks were further trimmed and post-
fixed in formal sublimate (saturated aqueous mercuric chloride and 37%
formaldehyde, 9: 1 ) for approximately 3h. Blocks were then routinely paraffin
embedded according to the processing schedule for breast specimens: placed in
10% formalin for 2hrs at 40°C; an alcohol gradient run: 70%, 80%, 95%. and
100% ethanol for 1 hour each at 40°C except for 100% ethanol which was
processed for 1 hour and 30 minutes twice; next they are processed in a solvent
which is miscible with wax such as toluene (or xylene here) twice for 2 hours at
40°C and finally embedded in wax twice- fold for 1 hour and 30 minutes at 40°C.
The clinico-pathological stage of the tumours was classified according to the
TNM classification system of the International Union against Cancer(Page and
Anderson, 1987). The histological classification of the tumours was based on the
World Health Organization (WHO) criteria and the grading was according to the
criteria of Bloom and Richardson modified by Elston. The histological diagnosis,
tumour size and lymph node status was detenined during routine pathological
assessment. A consecutive section from each sample was stained with

hematoxylin and eosin for histological evaluation by three separate pathologists
(C.C., L.K., 1-M. P.).
4.1 -3 Aminoalkylsilane (APES)
The Aminoaklylsilane (APES) solution was used as a medium for ensuring
maximal adherence of the tissue under examination to the cfear glass slides
locally supplied. The following is the protocol for a successful application of this
medium to al1 slides used under our irnmunohistochemical procedures:
1. Remove Im l of 3-aminopropylriethoxysilane and add it into 50 ml of
acetone in a container wide enough to accept standard 30-slide slide
racks.
2. The staining containers used required the addition of 392ml of acetone
and 8ml of stock Aminoalkylsilane. This represents a 2% APES
solution that is standard on irnmunohistochemical application. This was
prepared fresh for every 60 slides that required APES application.
3. Slides were dipped into this solution for 20 seconds.
4. Slides were then washed twice in pure acetone, dipping for 30
seconds.
5. Slides were finally washed Nice in distilled water. dipping for 30
seconds.
6. Tissue sections were fioated ont0 slides in a water-bath at 37OC for 2
hours.

7. Slides were then plaœd in a 50°C oven for drying overnight or at 37OC
for 48 hours.
The above mentioned procedure was followed with the exception of some
modifications we felt necessary to facilitate the adhesibn of breast tissue to the
slides. Since breast tissue sections are cornposed of large quantities of fat and
connective tissue, these elements make it difficult to adhere the tissue to the
slide under the extremes of microwave treatment. Therefore, we have found that
altering the concentration of the final APES solution from 2% to 6% was
adequate enough to ensure the adherenœ of the larger, more fragile portions of
the tissue to the slide. Attempts at concentrations of IO%, although successful in
adherence of the tissue showed background or "halon-like staining patterns under
ABC (Avidin-Biotin Complex) administration and made for poorly looking and
difficult to assess immunostained slides. An additional modification we used to
further enhance our staining quality was to add a solution of stayOnm to the
water-bath solution from which the sections are obtained and prepared for
placing on sections. This is a gluing medium that is perfectly miscible in water
kept at 37OC and does not contribute to any background staining.
4.1.4 Preparation of Antibodies & Reagents
p2PP1
This monoclonal antibody was purchased from Transduction
laboratories in 150pg aliquots at a concentration of 250 pglml and stored

at -20°C. The following were the storage conditions of the antibody:
0.25mglml in 50% glycerol, 20mM sodium phosphate pH 7.5, 150mM
NaCI, 1.5 mM NaN3, 1 mg/ml BSA. Working aliquots were prepared in
smaller volumes to prevent continued freezelthaw cycles of the stock
solution.
Secondary Anfibody (BA-2000) (Vector Laboratones, CA)
The secondary antibody used is biotin ylated anti-mouse lgG (H+L)
and is affinity purified. The antibody was purchased from Vector
Laboratories and arrived as 1.5mg lyophilised, produced in horse. The
antibody was reconstituted by adding lm1 of distilled water. The resulting
solution had the following composition: 1OmM phosphate, pH 7.8, 0.1 5 M
NaCI, 0.08% sodium azide. lmmunohistochemical grade bovine serum
albumin was added for stabilization. The antibody was stored in a
refrigerator at 4OC. For long-term storage, aliquots of 50pl were frozen at
-20°C in a frost-freezer. If the product is reconstituted as recommended,
the resulting solution will be the same as that provided in the
VECTASTAIN" ABC kits. The recommended concentration range for use
was 2-10 pg/ml. Since the antibody is to be used in tissues that may
contain cross-reacting endogenous immunoglobulins, dilution of the
biotinylated antibody was made in buffers containing serum. The optimal
dilution of the secondary antibody was determined to be 1 :200.

lmmuno~um@ Metal Enhanced DAB Substrate(P1ERCE)
The DAWMetal Concentrate is packaged under nitrogen for long-
term stability. Care was taken to ensure that the solution was not brought
to room temperature as this could affect the quality of the staining. It was
stored at -20°C in a frost-free freezer. For long-terrn storage (over 6
months), it was recommended that the nitrogen content in the mixture be
replenished. This can be accomplished by gently bubbling a slow stream
of nitrogen into the DABlMetal liquid. The associated Stable Peroxide
Buffer was stored at 4OC. The kit utilizes cobalt chloride and nickel chloride
in a special formulation to produce a dark brownlblack precipitate in the
presence of HRP in immunohistochemical applications. The following
preparation was used to create a working solution:
1. The volume of substrate was deterrnined.
2. The DABIMetal Concentrate (10X) was removed from the -20°C
storage. The solution was mixed well by inversion and was not allowed
to come to room temperature.
3. The DABIMetal Concentrate (10X) was diluted with Stable Peroxide
Buffer to a 1X working solution. For example, if 5 ml of substrate was
required. 500~1 of the DABlMetal Concentrate was diluted with 4.5ml of
the Stable Peroxide Buffer.
4. The solutions were mixed well using a Vortex agitator.

Note: hydrogen peroxide was not added. Stable peroxide is already
present at an optimal concentration and bulk hydrogen peroxide
cannot be substituted since adding further amounts will increase the
background staining of the tissue.
5. The 1X working solution was added to the tissue or was blotted until
the desired substrate development.
Note: The 1X solution was stable over many hours. For the best
results, the working solution was stored at 4OC when not in use.
VECTASTAIAP ABC
Avidin is a 68,000 molecular weight glycoprotein with an
extraordinarily high affinity (IO~~M") for the small molecular weight
vitarnin, Biotin. Because this affinity is over one million times higher than
that of antibody for most antigens, the binding of avidin to biotin (unlike
antibody-antigen interactions) is essentially irreversible. In addition to this
high affinity, the BiotinlAvidin System can be effectively exploited because
avidin has four binding sites for biotin and rnost proteins (including
antibodies and enzymes) can be conjugated with several molecules of
biotin. These aspects provide the potential for macromolecular complexes
to be fomed between avidin and biotinylated enzymes.
For convenience, the kit included mixing bottles to prepare working
solutions of reagents. After the buffer and appropriate reagents are added

to the bottle. the drop dispenser tip was inserted into the white opaque cap
in the correct orientation. All bottles have wlour wded labels to minimize
inadvertent use of the wrong mixing borne. In order to prevent
evaporation, the white opaque cap was secured ont0 the bottles when
they were not in use. The entire kit can be kept at 4°C.
A sufficient number of drops were applieâ on the slide to mver the
entire section. The slides were then placed in a humidified chamber
(maximum number of slides: 30) during the incubation period to further
prevent evaporation.
A number of different buffers can be used in the VECTASTAIN~
ABC system. We decided to use the most common one. lOmM sodium
phosphate. pH 7.5 0.9% saline (PBS). The working solutions were
prepared as follows:
Two drops (each drop is approximately 50~1) of REAGENT A
(orange label) were added to 10ml of buffer in the ABC Reagent mixing
bottle. The solution was gently stirred for a short time. Then. two drops of
REAGENT B (brown label) was added to the same mixing bottle. The
solution was mixed immediately using a vortex agitator, and allowed to
stand for approximately 30 minutes while it came to room temperature
before further use.

Citrate Buffer solution
The solution of chcice for immersion of tissue while in the
microwave was citrate buffer. The following is the protowl for a 10mM
Citrate Buffer, pH 6 solution:
Weigh 2.949 of Tri-Sodium Citrate powder from main container and
add to 1 liter of distilled water.
Agitate the solution until al1 noticeable powder grains have been
dissolved in the solution (10 minutes minimum).
Place flask next to a pH meter while still agitating the solution.
Remove using an eye dropper a sufficient amount of I N HCI and
slowly dispense the contents into the mking solution and note pH
meter value.
When enough acid has been added to neutralize the solution to a pH
of 6.00 stop with any additional HCI administration.
Use paraffin wax film to seal the open end of the flask to prevent any
contaminating bodies from entering the solution.
Pour approximately 500ml of solution into the pressure cooker or
enough to ensure immersion of the slides contained in the cooker.

Five paraffin sections were cut for each case in order to ensure
additional stock for experimental reproducibility. ParaffÏn sections of
tumour blocks were deparaffinized with xylene for 5 minutes, rehydrated in
a series of decreasing alcohol concentrations: 100% for 2 minutes. 75%
for 2 minutes, 50% for 2 minutes, and distilled water for 2 minutes. They
were then subjected to microwave treatrnent for 10 min in lOmM citrate
buffer (pH 6.0) 20 cases at a time. The citrate buffer was prepared freshly
and was discarded after every microwave session. In the citrate buffer
solution, a number of boiling chips were added (approximately 10) in order
to reduce the vigorousness of the boil, thereby ensuring maximal tissue
retention on the slides. The slides were placed on plastic slide holders
(holding 20 each) and altogether placed inside a ceramic pressure cooker.
After being placed in a microwave for 2- 1 O minute intervals at full power,
the slides were allowed to cool for 20 minutes at 4OC or 40 minutes at
25OC. Sections were removed and dehydrated by progressively adding
them into increasing concentrations of alcohol (same ethanol
concentrations used as above). The slides were then blocked with 3%
hydrogen peroxide in methanol for 10 minutes in order to block any
endogenous peroxide activity, followed by a wash in normal horse serum
(1:20 dilution) in O.1M solution of Phosphate Buffer Serum (PBS) at pH
6.0. The slides were then marked with a PAP pen (Zymed) encircling the
region of tissue. This procedure creates a hydrophobic barrier around the
slide to ensure that the reagents administered to the slides remain

confined to the areas of tissue. The slides were then transferred ont0 a
hydration chamber five at a time. All slides were not allowed to dry at any
point in the experimental procedure as this is known to have degrading
affects on the staining. Distilled water is added as the slides are set side
by side on the hydration chamber until the last slide is prepared. They
were then incubated overnight at 4OC with the monoclonal antibodies
studied. Approximately 500~1 of solution containing the antibody was
adequate to ensure total coverage of tissue. It some situations it was
necessary to incubate the slides at room temperature (25OC) for 2 hours
which had the same effect as the overnight incubation at lower
temperatures. The following antibody was used in the
irnmunohistochemical assessrnent of patient slides: ~ 2 7 ~ ' ~ ' [Anti
p27fiP'm~b] mouse monoclonal (Transduction Laboratories, KY) at an
optimal dilution of 1 :IO00 as determined in previous studies(Catzavelos, et
a 1997). Slides were then reacted with biotin-labeled anti-mouse IgG
secondary antibody for one hour and incubated with preformed avidin-
biotin-peroxidase cornplex (Vector Laboratories, Burlingame, CA) for an
additional hour. In between the administration of the various reagents, the
slides were washed with a series of PBS-based applications. Metal-
enhanced 3.3'-diaminobenzicline (DAB) substrate (Pierce, Rockford, IL)
was then added in the presence of horseradish peroxidase. After
approximately 5 to 10 minutes of DA8 administration. the slides were
immersed in water to stop the reaction. Sections were then mildly

counterstained with Mayer's hematoxylin. differentiated using an aqueous
solution of lithium carbonate, followed by a wash in 0.075% acid alcohol
(HCI 8 70% ethanol), dehydrated and mounted. The degree of staining
was scored independently by three different pathologists ( C C , I .M.-P.
and L.K.). In negative wntrols the pnmary antibody was replaced by PBS
or an irrelevant monoclonal antibody. Nomal glandular structures present
in most breast carcinoma sections (at least one in each stained slide)
served as positive interna1 wntrols. With routinely fixed paraffin material,
the antibody was successful in most samples. with less than 10% of the
tissues being poorly reactive (probably due to damage during fixation or
tissue processing). Photomicrographs were taken using a ~ei tz@
microscope through a ~odak@ digital DCS400 camera using one blue filter
to enhance contrast and brightness. A composite production of images
was made using Adobe hoto os hop^ 5.0 sofhvare on a ~ o w e r ~ a c @
computer.
4.1 .6 Results
Scoring
In al1 cases analyzed. a value of 4 was scored for cases showing dark
nuclear staining in 75400% of the nuclei assessed; 50.75% of positive
nuclei were given a score of the 3; 2550% nuclear staining was given a
score of 2; and 045% staining was given a value of 1. Statistically it was
later discovered that the swring can be grouped and classified into cases

which were high (staining in >5O% of cells) or low (staining in ~ 5 0 % of
cells). The nuclei of normal ductal epithelial and myoepithelial cells as well
as lymphocytes provided useful intemal positive controls in most sections
evaluated. At least 10 high power fields were exarnined for each case in
order to observe the overall expression of ~ 2 7 ~ ~ ' .
p2pp ' levels in relationship to grade
pure DClS
There were a total of 13 low grade cases. 16 intermediate grade, and 17
high grade cases of pure ductal carcinoma in situ (Table 4). In pure DCIS,
there was an inverse correlation between ~ 2 7 ~ ~ ' protein levels and grade
(p=<0.0139) with low grade lesions showing high ~ 2 7 ~ ' ~ ' levels and high
grade lesions showing low ~ 2 7 " ~ ' levels. 62% of low grade pure DClS
lesions had high ~ 2 7 ~ ~ ' levels, while 82% of high grade pure DCIS lesions
had low levels of expression of ~ 2 7 ~ ~ ' . Intermediate grade turnours
showed predominately a loss of ~ 2 7 ~ ' ~ ' expression (63%) (Table 4).
DCIS + INV
In DClS associated with invasive carcinoma, a similar association
between ~ 2 7 ~ ~ ' levels and grade was found. In al1 but one case, the levels
of were the same in the in situ and invasive components
(p=<0.00006). High ~ 2 7 ~ ~ ' levels were observed for 63% of low grade
DClS and 6 1 % of associated invasive components, respectively. 91 % of

Table 4. Represents a sumrnary of immunohistochemical results based on ~ 2 7 ~ ~ ' expression in three classes of primary turnours and their associated lymph node metastasis where found. The three classes of primary tumour studied were Pure DCIS (Ductal Carcinoma In Situ ) (first table from top), mixed DCIS + INV (invasive carcinoma) (second table), and Pure INV (thinl table). The grades of the associated primary and metastatic lesions are indicated, where 1 = low grade, 2 = intermediate grade, and 3 = high grade. High and Low levels of expression are tabulated versus these grades for each class. The information is presented in the form of n(%), where n represents the number of cases, and % represents its percentage of overall cases. High levels of ~ 2 7 ~ ~ ~ ' expression were found in low grade pure, mixed and metastatic carcinoma, 62%, 63% and 71%. While only 18%, 7% and 14% of high grade pure, mixed and metastatic carcinoma. respectively showed elevated levels of ~ 2 7 ~ ~ ' protein expression.

Table 4. Surnmary of immunohistochemical results based of p27kipl expression
Pure DClS GRADE 1 2 3
n(%) n(%) n(%) High p27 8(62) 6(37) 3(18) Low p27 5(38) lO(63) 14(82)
DClS + INV OClS GRADE INV GRADE 1 2 3 1 2 3
n(%) n(%) n(%) n(%) n(%) n(%) High p27 17(63) 16(28) 4(9) 19(61) 15(28) 2(5) Low p27 lO(37) 41(72) 39(91) 12(38) 38(71) 41(95)
PURE INV GRADE 1 2 3
n(%) n(%) n(%) High p27 2(40) 2(29) 1(10) Low p27 3(60) 5(71) 9(90)
LN METASTASES GRADE 1 2 3
n(%) n(%) n(%) High p27 S(71) 2(9) 3(14) Low p27 2(28) 21(91) 19(86)

high grade DClS and 91% of associated invasive components showed low
levels of ~ 2 7 " ~ ' expression. Intemediate grade lesions showed a loss of
expression of p27'@' in 72% of the DCIS component and 71% of invasive
components of the disease.
pure invasive
Low ~ 2 7 ~ ~ ' expression was observed for 90% of high grade pure invasive
carcinoma, white only 60% of low grade lesions showed low ~ 2 7 " ~ ' levels.
71 % of intermediate grade lesions displayed low ~ 2 7 ~ ~ ' levels as
determined immunohistochemically.
Lymph Node Metastases
In the 41 cases where positive nodes were examined, high ~ 2 7 " ~ ' levels
were associated with low grade metastases and low levels were
associated with high grade metastatic disease. There was a highly
statistically significant correlation between ~ 2 7 ~ ~ ' levels in the NI situ, the
invasive and the metastatic lesions (p=0.0007). 71% of low grade lymph
node metastases had high levels of ~ 2 7 ~ ~ ' expression and 86% of high
grade nodal metastases had low levels of ~ 2 7 " ~ ' expression.
correlation between grade of in situ and invasive components
A strong correlation between the grade of the in situ and invasive
components was observed (p=0.0001). E.g . , low grade ductal carcinoma

in situ disease was neariy always seen associated with low grade invasive
disease.
correlation between grade of pnmary and metastatic components
There was a good correlation between grade in al1 three wmponents
(p=0.02). E.g.. a low grade DCIS lesion was associated with low grade
invasive prîmary tumour and low grade histology in the nodal metastasis.
Table 4 serves to summarize the immunohistochemicaI results obtained
for each class of tumour studied: pure DCIS, pure invasive. and mixed
DCIS with synchronous invasive carcinoma.
The following page also includes the Plate figure (Plate 1) showing the
microscopic immunohistochemical detection of ~ 2 7 ~ ~ ' . Plate I is separated into
three sections: the top figure shows expression in in situ disease alone, the
middle figure shows expression in in situ carcinoma associated with invasive
carcinoma (mixed disease) and the bottom figure shows lymph node metastatic
breast cancer. expression variable levels of ~ 2 7 ~ ~ ' .
4.1.7 Analysis
In the following pages. Figure 8 shows a diagrammatic representation of
our findings. These findings suggested that ~ 2 7 ~ ~ ' levels are wnsistently
reduced in the progression from low to high grade disease in pure DCIS. as well

Plate I Top figure. (a) lmmunohistochemical expression of ~ 2 7 ~ ~ ' in low grade pure ductal carcinoma in situ (DCIS) and (b) high grade pure ductal carcinoma in situ showing a loss of ~ 2 7 ~ ' ~ ' expression in the high grade component of the disease. Middle figure. (a) lmmunohistochemical expression of ~ 2 7 ~ ~ ~ ' in low grade ductal carcinoma in situ and associated (c) low grade invasive components (IDC). showing high levels of ~ 2 7 ~ ~ ' expression. (b) and (d) are high grade in situ and invasive components. respectively both showing lowered ~ 2 7 ~ ~ ' protein levels. Bottom figure. (a to d) identical expression pattern to rniddle figure, (e) low grade metastatic carcinoma showing high levels of ~ 2 7 ~ ~ ' staining and (f) high grade lymph node metastatic carcinoma (MET) showing low
Kipl levels of p27 staining. For al1 cases involved, ~ 2 7 ~ ~ ' staining is nuclear and the dark brown stain is scored as high. The monoclonal antibody used in this study had very high specificity to and showed no cross reactivity with cytoplasmic features. ~ 2 7 ~ ~ ' was consistently decreased, with increasing tumour grade. in prirnary breast cancer as well as in the metastatic forms. (X20 Magnification)

PLATE l
~ 2 7 Pure OCIS
Mixed OCiS + INV - . , . - *::-*y . - < ..-". . 6 s . .- -- ,. . -- .. . ,:iy$. ;: - :.?* a-,.. * . <
~ 2 7 ~ i x d DCS + INV + MET

Figure 8. Diagrammatic representation of data for p27kip' activity. Low grade lesions (left) of pure DCIS, mixed DCIS and invasive carcinoma. and metastases demonstrated consistently high levels of ~ 2 7 ~ ~ ' expression as judged by nuclear staining intensities. In cornparison, diffuse and minimal staining was consistently observed for high grade (right) lesions. Additionally, the levels of ~27 '~ ' staining were significantly similar in al1 morphologic subtypes of the same grade: pure h situ (DCIS), mixed synchronous in situ and invasive carcinoma, and lymph node metastases. Since the greatest variation in ~27 '~ ' staining levels were seen with respect to the grade of the tumours, ~ 2 7 ~ ~ 9 s suspected to be a molecule involved in the complex process leading to loss of differentiation of a tumour with minimal involvernent in the processes leading to invasion to other rnorphologic subtypes as judged immunohistochemically. LG DCIS= Low Grade Ductal Carcinoma in situ . HG DCIS= High Grade Ductal Carcinoma in situ . LG IDC= Low Grade lnfiltrating Ductal Carcinoma. HG IDC= High Grade lnfiltrating Ductal Carcinoma. LG LN met= Low Grade Lymph Node metastasis. HG LN met= High Grade Lymph Node metastasis. Dashed line indicates possible progression pathway.

LG DClS HG DClS
No loss of p27
No loss 1 of p27
LG DCIS @ 4 p27 - 00
LG IDC ,, INO loss
- -
LG LN met - - - - - - - - + HG LN met

as in lesions with mixed DClS and invasive carcinoma and pure invasive
carcinoma. In the progression from low to high grade disease. the predominant
features observed are increased proliferative index as judged by the abundance
of cells and decreased differentiation status as determined by nuclear grade (size
and morphology), loss of polarity of cells, apparent loss of adhesion to basement
membrane. and loss of architectural tissue organization (few to no tubular
structures).
In normal breast, there is formation of ducts and lobules containing acinar
units. This is dependent on the coordinate expression of cell-cell and ceIl-matrix
adhesion molecules. chiefly E-cadherin and the integrin family, respectively.
~ 2 7 ~ ~ ' has been shown to be important for differentiation in a number of studies.
~ 2 7 ~ ' ~ ' levels are increased in breast cancer cells engineered to overproduce E-
cadherin, providing the link between ceIl-cell adhesion and the cell
cycle(Levenberg et al.. 1999; St. Croix. et al.. 1996). It is likely that this is true
during differentiation. Another means by which proliferation may be suppressed
during differentiation is through integrin mediated increase in p27'<jP1
levels(Fornaro et al., 1999). Detachment of cells frorn the rnatrix results in a loss
of integrin signaling, that results in upregulation of ~ 2 7 " ~ ' and arrest at the GiIS
transition (Fang et al.. 1996). Overexpression of the integrin-linked kinase (ILK)
has been shown to be associated with unregulated levels of ~ 2 7 ~ ~ ' as well as
en hanced G 1 cyclin dependant kinase activity(Radeva et al.. 1 997). Ad hesion
dependant G1 arrest, accompanied by elevated levels of ~ 2 7 " ~ ' has also been

shown by others(Polyak, et al., 1994). In addition, we have observed that ~ 2 7 ~ ~ '
levels are normally high in normal breast epithelium further supporting these
findings.
During tumour progression, the tumour cells increase in size, develop
nuclear atypia (vesicular chromatin, multiple nucleoli) and increased numbers of
mitotic figures are observed. Low grade breast cancers retain elements of their
normal differentiation program and attempt to recapitulate normal breast tissue
by forming tubules in invasive lesions and cribriform spaces in in situ lesions. It
has been shown that there is a decrease in E-cadherin expression and
downregulation of integrins during this process(Jonjic, et al., 1993; Siitonen, et
al., 1996; Ziober, 1996). In view of the above mentioned relationship between
~ 2 7 ~ ' ~ ' and E-cadherin it is possible that loss of E-cadherin and changes in
intracellular adhesion my influence ~ 2 7 " ~ ' levels or vice versa.
4.2 Molecular Events involving ER, HER-Zneu and pS3
4.2.1 Rationale
Our data on ~ 2 7 ~ ~ ' in in situ and invasive disease supported our initial
hypothesis that breast cancer progression is not linear. To further investigate the
mechanism of breast cancer progression, I undertook a further analysis of soma
of the most well characterized events in breast cancer: loss of ER expression,
amplification of HER-2lneu and overexpression of p53 protein product. A cohort

of patients was re-estabfished and an immunohistochemical assessment of the
following molecules was performed on the entire cohort of pnmary carcinomas:
p53, HER-21neu. Estrogen Receptor (ER), and E-cadherin. The cohort was
subdivided into cases exhibiting pure ductal carcinoma in situ (DCIS), mixed
DClS & synchronous invasive carcinoma, and pure invasive carcinoma. The
study was then broadened to investigate the expression of these molecules in a
subset of cases h m the cohort that displayed axillary lymph node metastases.
4.2.2 Patient population and statistical rnethods.
Our study included 203 resected breast carcinomas from 203 female
patients (same cohort as ~ 2 7 " ~ ' progression study) (mean age: 61.1 years,
range: 28 - 91 years) attending the Sunnybrook and Women's College Health
Science Center between 1996 and 1998. A subset of 44 of these patients had
stage II breast cancer with axillary lymph node metastasis at diagnosis. The
same materials and technical procedures were used in this study as were used in
the p27fiP' progression study. In addition to the chi-squared test. the McNemarls
statistical test (Table 9) using one degree of freedom for a normal distribution
was performed on these factors in an attempt to determine a putative order of
molecular events by evaluating the power of their various expression relative to
each other.
4.2.3 lmmunohistochemistry.

The following additional antibodies were used in the immunohistochemical
assessrnent of patient slides: HER-2lneu (NCL-CBl l] mouse monoclonal (Novo
Castra Laboratories, UK) at an optimal dilution of 1 part antibody to 200 parts
PBS (1:200); p53 [Ab-2, Pab1801] mouse monoclonal IgG1-kappa (Calbiochem
Laboratories, CA) at an optimal dilution of 1:200. Human Estrogen Receptor
[NCL-ER-6F11J mouse monoclonal lgGl (Novo Castra Laboratories, UK) at an
optimal dilution of 1 50. and XE-Cadhenn [HECD-1 ] mouse monoclonal lgG1-
kappa (Zymed Laboratories, CA) at an optimal dilution of 1 : 100. Using a single
cohort, a single operator and a single imrnunohistochemical technique (section
4.1.4), information was gathered and analysed about the distribution and
possible association of the above mentioned molecules reported as informative
in the study of breast cancer progression.
4.2.4 Additional Prepara tion of An tibodies
HER-2heu (c-erb8-2)
This HER-2lneu antibody (Novo Castra Laboratories, UK) reacts to
the interna1 domain of the c-erbB-2 cornplex. The antibody was
reconstituted with 1ml or O.1ml of sterile distilled water as indicated on the
via1 label. Unopened lyophilised antibody was stored at 4OC. Under these
conditions, there is no significant loss in product pefiormance. The
reconstituted antibody was stable for at least two months when stored at
4OC. For long tem storage, aliquots of 25pl of the antibody were made

and stored at -20°C using a frost fieezer. Repeated freezing and thawing
were avoided. Working preparations were made on the day of use.
E-cadhefln
The XE-cadherin [HECD-11 (Zymed Laboratories, CA) antibody was
supplied lyophilised in phosphate-buffered saline, 1 .O% bovine serum
albumin. According to the Company, the antibody was purified by
ammonium sulfate precipitation and anion exchange chromatography and
was very specific to membrane-bound E-cadherin molecules. 100pg of
antibody were received. The antibody was rewnstituted with 50jd of
distilled water to yield a concentration of 2 mglml. For 2-8OC storage, 0.1 %
of NaN3 and 1.0% bovine serum albumin was added. Othewise, the
aliquots of 1 Opl were placed in a -20°C frost freezer until required.
ER
The ER antibody (Novo Castra Laboratories, UK) reacts with the N-
terminal domain of human estrogen receptor (ER, 67dkD). It was
purchased as a lm1 solution in wncentrated form. The buffer included 2
mglml bovine serum albumin in phosphate buffered saline containing
0.1% sodium azide. The solution was stored at 2-8OC and it was not
recommended that aliquots of this antibody be frozen.

The epitope recognized by the mAB 1801 (Calbiochem
Laboratories, CA) lies between amino acids residues 46-55 of human p53.
It was supplied as a 100pg purified antibody lyophilised from a volatile
buffer with 1OOug of BSA (Bovine Serum Albumin). It was resuspended
with sterile phosphate buffer saline (PBS), pH 7.4 or alternatively the
option was given to resuspend it using 20mM Tris-saline (20mM Tris
containing 0.1 5 M NaCI), pH 7.4, to yield a final concentration of 100ug/ml.
The antibody was resuspended at 4OC with occasional gentle mixing for at
least two hours. The antibody was stored at 4OC until reconstituted. then
was stored in aliquots at -20°C or at 4OC with 0.1 % azide. Repeat freezing
and thawing was avoided for this antibody.
4.2.5 Results
Scoring
In al1 cases examined, Estrogen Receptor expression was scored
positive (high) for cases in which greater than 10% of the nuclei showed
dark staining for the receptor. p53 alterations were scored high if greater
than 5% of the nuclei observed had a dark staining pattern. HER-2lneu
overexpression was scored as high in cells which had greater than 10% of
their plasma membrane darkly stained for the receptor. An average
obseivation of 10 high-power fields was made before a score was
recorded for each of the markers. The nuclei of normal ductal epithelium,
myoepithelial cells, endothelial cells as well as lymphocytes provided

useful intemal positive controls in most of the sections examined. The
swring was made independently by three pathologists with a concordance
rate of 90% for al1 cases examined. In cases for which discrepancies
existed in the assessment between the pathologists, a review of the
sections in the presence of al1 three pathologists was made and a decision
as to the final score was deterrnined by consent. The following paragraphs
surnmarize the observations. with references to tables and figures.
The tables of results in the following pages were generated based
on the statistical analysis of the immunohistochemical data obtained.
There are four tables in total. For each table there are two numbers n(%),
the first number represents the actual nurnber of cases and the second
number in parenthesis represents the percentage relative to the entire
cohort. The MBRGR column (Table 5, 6b, 7) represents the Modified
Bloom Richardson-Grading system used to grade the cases. The DClSG
column (Table 6a) represents the Ductal Carcinoma In situ Grade.
Table 5 represents the immunohistochemical and statistical data
obtained for cases in which both an in situ and synchronous invasive
component of the disease were present (n=124). High levels of ER
expression were observed for 93% of low grade DClS and 94% of
associated invasive components. While only 58% of high grade DClS and
51% of high grade invasive lesions demonstrated ER positivity; HER-

2lneu was overexpressed in 100% of low grade mixed lesions while only
44% of high grade DClS and 42% of high grade invasive lesions showed
overexpression; none of the low grade tumours showed p53
overexpression (as reflected in stable p53 overexpression correlation with
point mutations (Baas. et al., 1994)). while 33% of high grade tumours
showed appreciably high levels of stable p53 overexpression.
Table 6a represents the analysis of cases which presented only
ductal carcinoma in situ (n=46). ER positivity was detected in 85% of low
grade tumours and only 24% of high grade lesions; HER-2lneu
overexpression was detected in only 8% of low grade disease and 71% of
high grade disease; p53 overexpression was not detect in low grade
lesions and was detected in 29% of high grade lesions. Table 6b
represents the analysis of cases which presented only an invasive
component of the cancer (n=30). ER positivity was detected in 67% of low
grade disease and only 23% of high grade lesions; HER-Zlneu
overexpression was not detected in any low grade purely invasive lesion
while 38% of high grade lesions showed signs of overexpression; p53
mutated protein was not detect in low grade lesions and was detected in
38% of high grade lesions.
Table 7 represents a sub-set of tumours which had lymph node
metastases obtained from cases found in both the mixed (Table 5) and

Table 5. Represents the immunohistochemical and statistical data obtained for cases in which both an in situ and synchronous invasive component of the disease were present (n=127). High levels of ER expression were observed for 93% of low grade DCIS and 94% of associated invasive components. While only 58% of high grade DCIS and 51% of hig h grade invasive lesions demonstrated ER positivity; HER- Uneu was amplified in 100% of low grade mixed lesions while only 44% of high grade DCIS and 42% of high grade invasive lesions were amplified; none of the low grade tumours showed p53 overexpression (as refleded in stable p53 overexpression correlation with point mutations(6aas et al, 1994), while 33% of high grade tumours showed appreciably high levels of stable p53 overexpression.

Table 5. Immunohistochemical data on molecules studied (in situ and invasive) carcinoma
MOLECUL€ Dcls TOTAL INV TOTAL P MBRGR 1 2 3 1 2 3
n=27 n=57 n=43 127 n=31 n=53 n=43 127 n(%) n(%) n(%) n("/o) n(%) n(%)
ER HlGH 25(93) 4477) 25(58) 94 29(94) 39(74) 22(51) 90 0-00006 LOW 2(7) 13(23) 18(42) 33 2(6) 14(26) 21(48) 37
HER-2 HlGH O(0) 12(21) 19(44) 31 O(0) 12(23) 18(42) 30 0.00006 LOW 27(100) 45(79) 24(56) 96 31(100) 41(77) 25(58) 97
~ 5 3 HlGH O(0) 3(5) 14(33) 17 O(0) 3(6) 14(33) 17 0.00006 LOW 27(100) 5 4 9 5 ) 29(67) 110 31 (100) SO(94) 29(67) 110

Table 6a. Represents the analysis of cases which presented only ductal carcinoma in situ (n=46). ER positivity was detected in 85% of low grade tumours and only 24% of high grade lesions; HER-2heu overexpression was detected in only 8% of low grade disease and 71% of high grade disease; p53 overexpression was not detect in low grade lesions and were detected in 29% of high grade lesions.
Table 6b. Represents the analysis of cases which presented only an invasive component of the cancer (n=30). ER positivity was detected in 67% of low grade disease and only 23% of high grade lesions; HER-%eu overexpression was not detected in any low grade purely invasive lesion while 38% of high grade lesions showed signs of overexpression; p53 mutated protein was not detect in low grade lesions and was detected in 38% of high grade lesions.

Table 6a. Immunohistochemical data on molecules studied for pure In situ carcinoma
MOLECULE PURE DClS TOTAL P OClSG 1 2 3
ER HlGH 1 l(85) 9(56) 4(24) 24 0.0085 LOW 2(15) 7(44) 13(76) 22
~ 5 3 HlGH O(0) 2(13) 5(29) 7 0.0244 LOW 13(100) 14(88) 12(71) 39
Table 6b. lrnmunohistochemical data on molecules studied for pure invasive carcinoma
MOLECULE PURE INV lotAt P MBRGR 1 2 3
ER HlGH 4(67) 7(64) 3(23) LOW 2(33) 4(36) lO(77)
HlGH O(0) 2(18) 5(38)
P~~ LOW ô(100) Q(82) 8(62)

Table 7. Represents a sub-set of tumours which had lymph node metastases obtained from cases found in both the mixed (Table 5) and invasive only (Table 7) categories (n=52). In Table 7, it can be noted that 71 % of the low grade lymph node metastasis showed high levels of ER positivity, while none of the low grade metastatic cases showed either HER-2heu overexpression or p53 mutations. Overexpression of H ER- 2heu and p53 mutations were detected in 27% and 32% of high grade metastatic cases. Interestingly, there was one case from the mhort in which the cancer cells could be seen penetrating a vessel walf. In another region, a single epithelial ceil from a high grade lobular carcinoma was seen partially embedded in a lymphatic vessel with a trail of additional cells nearby.

Table 7. lmmunohistochemical data on molecules studied for metastatic carcinoma
MOLECULE METASTASIS TOTAL MBRGR 1 2 3
HlGH O(0) 4(17) 6(27) 10 HER-2 LOW 7(ioo) is(s3) i s ( n ) 42
HlGH O(0) 6(26) 7(32) 13 LOW 7(100) 17(74) 15(68) 39

invasive only (Table 7) categories (n=44). In Table 7, it can be noted that
71 % of the low grade lymph node metastasis showed high levels of ER
positivity, while none of the low grade metastatic cases showed either
HER-2heu overexpression or p53 mutations. Overexpression of HER-
Uneu and p53 mutations were detected in 27% and 32% of high grade
metastatic cases. Interestingly, there was one case from the cohort in
which the cancer cells could be seen penetrating a vessel wall. In another
region. a single epithelial cell from a high grade lobular carcinoma was
seen partially embedded in a lymphatic vessel with a trail of additional
cells nearby.
Table 8 is a summary of the various associations that have been
found between the different stages studied (morphological subtypes of
DCIS, INV and MET) and the molecular expression of the factors under
investigation ( Inv Grade was also included in the correlation analysis).
The data used to determine the association was obtained from the
irnmunohistochemical experiments carried out. The first column describes
the various associations found between the in situ and invasive ( DCISI
INV ) components with the parameters studied (Grade and molecules).
The second column describes the existence of correlation between the
invasive and metastatic phases of cancer ( INVIMET ) with the parameters
studied. Finally, the last column describes any significant relationships
found between the in situ and metastatic components with relation to the

Table 8 is a summary of the various associations that have been found between the different stages studied (morphological subtypes of DCIS, INV and MET) and the molecular expression of the factors under investigation ( Inv Grade was also included in the correlation analysis) using the chi-squared test. The data used to determine the association was obtained from the immunohistochemical experiments carried out. The first column describes the various associations found between the in situ and invasive (DCISI IW) cornponents with the parameters studied (Grade and molecules). The second column describes the existence of correlation between the invasive and metastatic phases of cancer (1 NVIMET) with the parameters studied. Finally, the last column describes any significant relationships found between the in situ and metastatic components with relation to the studied parameters. There was a hig hly significant association found by using the chi-squared test between the grades of the DCIS, INV and MET forms of the disease (p=0.0001, p-0.0001 and p=0.0207, respectively) as noted in Table 8. Similarly in al1 the molecules, there was significant association in the expression profiles between the DCIS and INV components (p=0.0001) and the INV and MET components (avg. p=0.004) and good association between the DCIS and MET (avg. p=0.0019) except with respect to ER that did not reach statistical significance.

Table 8. Various associations found between morphological subtypes and molecules studied
DClS 1 INV INV 1 MET DClS / MET P
GRADE 0.0001 0.0001 0.0207
Chi-squared test used to establish correlations of grade and molecular expression at the various lesional stages (DCIS, INV and MET)

studied parameten. There was a hig hly significant association found by
using the chi-squared test between the grades of the DCIS, INV and MET
forms of the disease (p=0.0001, p=0.0001 and p=0.0207, respectively) as
noted in Table 8. Similarly in al1 the molecules, there was significant
association in the expression profiles between the DClS and INV
components (p=0.0001) and the INV and MET components (avg. p=0.004)
and good association between the DCIS and MET (avg. p=0.0019) except
with respect to ER that did not reach statistical significance. The
relationship between DCIS ER expression and metastatic (MET) ER
expression was only suggestive of a correlation (p=0.1344) and did not
meet statistical significance possibly due to the smaller cohort size of the
lymph node metastatic cases ( n a ) . A significant trend is still noted, in
that ER expression between DCIS components and MET components
correlate with 86.5% confidence (p=0.1344).
Table 9 represents statistical data obtained for the analysis of order
for the molecular events using the McNemar's test. The likelihood of order
is summarized in the pathway diagram on the bottom. General findings
indicate that loss of ~ 2 7 % ~ ' and loss of ER status are earlier events
(pc0.00006) than HER-Uneu overexpression and p53 mutations. Table 1 0
represents order analysis based on characteriration of intermediate grade
tumours. The analysis showed that loss of ~ 2 7 ~ ~ ' and loss of ER status
were among the earliest rnolecular changes as judged by an alteration in

Table 9. Represents statistical data obtained for the analysis of order for the molecular events using the McNemar's test. The McNemar's test using a 2 by 2 table to compare in pairs the number of molecules with either high "+" or low '-" expression values. It is a common test used to generate a normal distribution and is a variation of the X2. Each table generated will have four numbers in four cells representing the Frequency of occurrence. Arbitrarily, if the top left cell is labeled 'a', top right cell labeled 'b', bottom left cell labeled 'c' and bottom right cell labeled 'd', the following formula will govern the calculation of the z-statistic which will later be used to determine a p-value:
There is no informative data obtained from variables that agree, +1+ and -1-, therefore variable 'a' and 'd' are not utilized in the McNemar's test. Using a statistical chart for a normal distribution using one degree of freedom (Munro et al, 1997), a p-value was obtained from the corresponding Zc figure calculated. The likelihood of order is summarized in the pathway dia ram (bottom figure). General findings indicate that loss of p2#'p1 and los5 of ER status are earlier events (p<0.00006) than HER-2Ineu overexpression and p53 mutations.

Table 9. Statistical data for order of molecular events using the McNemafs Test
TABLE OF p27 BY ER ~ 2 7 ER
Freauencv + - Total + -
Total
TABLE OF p27 BY H E M ~ 2 7 HER2
Frequency Total +
Total 51 66 117 zc=2.17 P=0.030 Order: D ~ ~ > H E R ~
TABLE OF p27 BY p53
Frequency Total +
1
Total 25 92 117
TABLE OF ER BY HER2 ER HER2
Freauencv + - Total . + O
Total 51 66 117
TABLE OF ER BY p53 ER ~ 5 3
Frequency + O
Total
Total 58 59 Il7
TABLE OF HERZ BY p53
Frequency +
Total 25 92
Total 51 66 117

the expression pattern (% altered expression) seen in intemediate grade
tumours. The data supports a putative order predicted by the McNemar's
test.
The following Plate figures (Plate 11, III, IV. VI VI) are photographic
composites generated to illustrate the expression each molecule studied
with respect to the morphologie subtypes in breast cancer and to illustrate
their correlation with out proposed hypothesis for turnour progression. All
images were taken at the same magnification of 20X using a Leitz
~ e t z l a p microscope and a brief surnmary of the findings is presented for
each molecule in the form of figure legends found in the following series of
pages.

Plate II. Intralesional progression of breast cancers p27 Kipl
IHC stain. (A) A section of low grade ductal carcinoma in situ showing higher ~ 2 7 ~ ~ ' staining cells in the central region (inset arrow) and lower staining in peripheral cells (outset arrow). (6) and (C) show one case of low grade invasive carcinoma with high levels of ~ 2 7 ~ ~ ' (B) as compared to lower levels of ~ 2 7 ~ ~ ~ ' in a higher grade portion of the lesion (C) surrounding a normal duct (N). (X20 Magnification)

PLATE Il

Plate III. Immunohistochemical expression of Estrogen Receptor (ER) in low and high grade fonns of ductal carcinoma in situ associated with synchronous invasive carcinoma. In both the low grade ductal carcinoma in situ and low grade invasive carcinoma. Estrogen Receptor expression is high. The nuclei of the low grade cells are equally darkly staining for the molecule in the in situ and invasive components. Conversely, the high grade forms of the disease have minimal to no staining in the high grade nuclei of both in situ and invasive components. (X20 Magnification)
Plate IV. Imrnunohistochemical expression of HER-Uneu (erb-B2) in both low and high grade forms of ductal carcinoma in situ associated with synchronous invasive carcinoma. There is little to no staining in the membranes of low grade in situ and low grade invasive forms of the disease. In contrast, the high grades forms of the disease have abundant HER-2heu staining consistent with overexpression of the receptor in these rnorphologic su btypes. (X20 Magnification)

PLATE III
PLATE IV

Plate V. Immunohistochemical expression of pS3 in both low and high grade forms of ductal carcinoma in situ associated with synchronous invasive carcinoma. There is little p53 staining observed in the low grade forms of both in situ carcinoma and invasive carcinoma. Conversely, the high grade forms show considerably more staining of p53 in both components, in situ carcinoma and invasive carcinoma. This indicates a stabilization of the p53 protein in these forms of the disease. In a study of medullary carcinoma of the breast, researchers demonstrated that immunohistochemical analysis of p53 using antibodies correlated 100% with p53 mutational analysis, proposing excellent agreement between the results of the different analytical techniques, and thereby the validity of immunohistochemical interpretation of p53 activity (Cremoux et al, 1999). (X20 Magnification)
Plate VI. Immunohistochemical expression of Ecadherin in both low and high grade forms of ductal carcinoma in situ associated with synchronow invasive carcinoma. In this study, normal breast ducts and acini strongly expressed E- cadherin a epithelial cellcell boundaries. No positive reaction was observed in lymphocytes, fibroblasts, or adipose tissue. In breast tumour cells and tissues, E-cadherin was variously distributed. In in situ ductal carcinomas, E-cadherin expression resembled that of normal breast. In higher grades of invasive ductal carcinoma, the positive immunoreaction decreased with tumour dedifferentiation. In tumours of intermediate differentiation, Ecadherin expression was heterogeneous. Not al1 the cells were stained and positive cells exhibited abnormal patterns of staining, wlh only focal and punctuate positivity on cytoplasmic borders and cell boundaries. (X20 Magnification)

PLATE V
PLATE VI

DISCUSSION

5. DISCUSSION
Progression in breast cancer appears to be a more cornplex process than
other cancer types and any model that attempts to undentand this process must
be able to explain the marked morphologic. molecular and biologic heterogeneity
observed in this disease. Although some of the models proposed address many
important issues, there is a considerable amount of data that is difficult to
explain. It is difficult to understand how certain events such as decreased levels
of ~ 2 7 ~ ~ ~ ' . loss of ER expression, mutation of p53 and overexpression of HER-
2fneu can occur in high grade in situ lesions but not in low grade invasive
cancers if one believes that breast cancer progression follows linear models.
The overall aim of the studies presented was to investigate key molecular
events in breast cancer to determine their relationship to the spectrum of
morphologic subtypes (DCIS, invasive and metastases) observed in breast
cancer progression. In addition. we investigated relationships between the grade
of the in situ and associated in invasive carcinomas as well as between the
primary tumours and synchronous metastases. One of major limitations of many
studies investigating breast cancer progression has been the lack of correlation
with al1 stages of progression(Gupta et el., 1997). Accordingly, we have studied
the full spectrum of pure in situ carcinoma, mixed in situ and invasive
carcinomas, pure invasive carcinomas and metastatic lesions. We show that in
many respects. breast cancer differs from other cancers that have been shown to

follow traditional linear models of tumour progression(Fearon and Vogelstein,
1990). A diagrammatic representation of our data and hypothetical model is
shown in Figure 9 and further evidence for its validity is presented below.
1 The molecular events studied occur in the same sequence in the progression fmtn low to high graâe in situ, invasive and metastatic lesions
The molecular events studied were detected using immunohistochemistry
which is the most widely used method for the assessment of ER status and
~ 2 7 ~ ' ~ ' levels(McCarty, et al., 1985; Patterson, et al., 1990; Pertschuk, et al.,
1985). Although fluorescence in situ hybridization (FISH) and differential PCR
are considered most accurate for the identification of HER-Uneu amplification,
immunohistochemistry is a well accepted alternative and most widely used
technique for this assessment(Corbett et al., 1990). A recent study observed that
HER-2heu gene amplification can be predicted accurately by IHC with a
confidence of 95.5% (Kerns et al.. 1993).The best rnethod for the assessrnent of
p53 mutations is direct sequencing(Si1va et al., 1999). Although some studies
have shown discordance as high as 25% between the identification of stable p53
protein and mutational status(Sjogren et al., 1996). a sufficient number have
shown sufficient correlation for immunohistochemistry to be an acceptable
alternate in the appropriate context(Andersen, et al.. 1993; Soussi. 1997). Based
on the eficacy of the antibodies used and the wide support from past literature, a
confident interpretation of molecular expression from our data was possible.

Figure 9. Model of Breast Cancer Progression. The model depicted above represents the summarized imrnunohistochemical findings for the molecules studied and how they can best be integrated into a cogent pathway of breast cancer progression. Lesions are separated into Low Grade (left) and High Grade (right) subtypes as well as pure in situ (top row), mixed synchronous in situ 8 invasive (middle row) and lymph node metastases (bottom row). Intermediate Grade tumours have been omitted from the representation for clarity purposes. ER= Estrogen Receptor, E-cad= E-cadherin, Dashed arrows represent hypothesized progression pathways. $ represents a loss of the molecular marker as judged immunohistochemically. ++ represents amplification. mut
represents mutations. LG= Low Grade. HG= High Grade. LN met= breast cancer metastatic to lymph nodes. Alterations in molecular status of al1 studied molecules are obsewed in the progression of the lesions from lower grades to higher grades. The order of molecular activity with respect to each molecule is presented. E-cad is outlined to indicate an observational trend in expression without statistical data. A thickened arrow leading to HG LN met represents a biased avenue of progression in this cfass of lesions.

+p27 +ER HER2+* ~ 5 3 " " ~ + in situ
I l
1
Q " , O g
E' in situ + invasive
\d LN mets

5.1.1 ER
We have demonstrated that ER expression is lost in 48% of cases of pure
DCIS. 93% of low grade in situ lesions and 55% percentage of high grade
lesions were ER positive which suggests that ER receptor expression is lost in
the transition from low to high grade in situ carcinoma. Invasive carcinomas
showed loss of ER in 53% of cases and, as in in situ carcinomas, this occurred in
the progression from low to high grade lesions. Similar findings were seen in
metastatic lesions that showed high levels of ER expression in low grade, and
loss in high grade metastases. There was a strong correlation between levels of
ER expression in the in situ and that of adjacent invasive carcinoma. Our findings
are in agreement with studies investigating ER expression in in situ and invasive
breast carcinoma (Barnes and Masood. 1990; Malafa et al.. 1990).
5.1.2 UER-Zneu
Our results indicate that 30% of in situ lesions have HER-2heu
overexpression and that this is seen in 71% of high grade in situ lesions.
Previous studies have shown rates of between 40 and 60% for al1 in situ
carcinomas and rates of 55400% for high grade subtypes (Schirnmelpenning et
al. ). Therefore. while the overall incidence is lower than reported, the incidence
in high grade lesions is similar. In contrast, only 30% of invasive carcinomas
showed overexpression of this gene and this in a similar rnanner was correlated
with high grade morphology. Furthemore, the same trend was seen in metastatic
lesions with HERZIneu overexpression in high grade lesions. These findings

suggest that HER-Wneu overexpression occurs in the transition from low to high
grade lesions in in situ. invasive and metastatic lesions. In mked cases, there
was a significant correlation between the presence of overexpression in the in
situ and associated invasive components.
The fact that high grade DCIS, which is a presumed precursor of invasive
carcinoma, has a much higher incidence (80%) of HER-21neu overexpression
than invasive cancers (25030%) is surprising. One possible explanation for this
finding is that many of the comedo-type (high grade) DClS cases do not progress
to invasive cancer. This interpretation is consistent with the combination
model(O'Connell, et al., 1994)of breast cancer progression but not the
morphological continuum model(Page and Dupont, 1990b). An alternative
possibility is that some invasive breast cancers occur without passing through a
high grade DClS stage altogether. This interpretation is consistent with the
stochastic mode1 (Smith, et al., 1993). Finally, a third possibility is that those
DClS cases which are high grade but lack expression of HER-Uneu are the ones
most likely to become invasive.
5.1.3 p53
Our results show evidence of stable p53 protein in 15%, 23% and 13% of
pure DCIS, pure invasive and mixed cases, respectively. The results are slightly
lower than those of previous studies (Sawan et al., 1992). It has been reported
however, that in other studies the rate of p53-positive breast carcinomas was

found to be ranging from 12% to 23% (Tnidel et al., 1992) (Martinaui, et al..
1993). This discrepancy could reflect differences in the fixation of the tissues
studied or it could be related to the epitope of reactivity to specific antibodies
used. In this study, the PAb 1801 antibody was used which is the same antibody
used in a larger study showing the independent prognostic value of p53 in
predicting overall survival in a group of node negative patients (Home, et al.,
1996). There are however two additional antibodies developed against p53 that
researchen have commonly used, D07(Fernando et al.. 1995) and p53-BP-
12(Horne, et al., 1996). PAb 1801 is known to react with the amino-terminal
portion of the p53 molecule. which is just proximal to the central region, and is
most frequently affected by point mutations.
There was a strong correlation between the presence of stable p53 protein
in the in situ, associated invasive components and metastatic lesions in mixed
cases. This result concun with the study performed by Davidoff et al which
showed that specific mutations of p53 were highly consenred in both intraductal,
invasive and metastatic components (Davidoff, et al., 1991). It was also seen in
our study that stable p53 protein was expressed in both the in situ and invasive
components of the same tumour (mainly high grades). p53 immunostaining
correlated strongly with grade, and p53-positively scored tumours tended to be
negative for ER status and to be of high grade implicating a possible dissociation
to hormonal stimulus. Evidence of p53 mutations was found almost exclusively in
high grade in situ, invasive and metastatic lesions suggesting that these also

occur in the transition from low to high grade disease as observed in the events
discussed above.
S. 1.4 E-cadhenii
Preliminary data investigating E-cadherin expression show a similar trend
to the molecular events discussed above. The study has shown that E-cadherin
levels are high in low grade in situ. invasive and metastatic carcinomas. In
addition, in mixed cases. there is a correlation of E-cadherin expression in the in
situ, invasive and metastatic components. This is an intriguing observation in
light of accumulated data suggesting that down regulation of E-cadherin as a key
event in invasion(Mareel et al., 1991 ; Siitonen, et al., 1996). If the data from other
literature is correct, one would expect to see differential expression of E-cadhetin
between in situ and invasive cancer. In cases of low grade DCIS that have high
levels of E-cadherin and invade, we see high levels of expression in both the in
situ and invasive cornponents. One possible explanation, is that prior to invasion,
the cells immediately adjacent the basement membrane, downregulate levels of
E-cadherin, detach from their neighboun, and invade through the basement
membrane into the surrounding stroma where subsequently, upregulation of E-
cadherin levels ensue and the cells f o n tubules as seen in low grade lesions.
There is some evidence for unstable E-cadherin expression which may locally or
temporarily diminish as in the embryo(Nose et al.. I W O ) . Furthermore, it has
been reported that highly metastatic cells have an unstable E-cadherin

expression that varies easily depending on cell culture conditions(Hashirnoto, et
al., 1989).
5.1 -5 Order of rnolecular events
Based on the statistical data obtained for the differential expression of the
molecules studied and by using the McNemarls test (Table 9'- lt7) & IO) , it was
possible to predict an order of operation of the molecular events in cancer
progression and to integrate the findings into our proposed model. With respect
to each of the other molecules studied, both techniques used to determine order
in the following pages show that ~ 2 7 ~ ~ ' expression is presumed to be
downregulated initial1 y, followed by estrogen receptor status loss, HER-2lneu
overexpression and finally mutant p53 protein product overexpression. The most
striking feature of the observation is that the molecular events occur in the same
order in progression of pure ductal carcinoma in situ as compared to invasive
carcinomas ieading to further supporting evidence of the idea that DClS are
direct precursors of invasive breast cancer. In Table 9, the McNemarJs showed
that satisfactory certainty of order for al1 molecules could not be fully obtained.
The analysis shows that the relationship between ~ 2 7 " ~ ' and ER could not be
established with p~O.05. Furthermore, the refationship of order between ER and
HER-21neu could also not be made with certainty. However, the test does
demonstrate that loss of ~ 2 7 ~ ~ ' expression occurs before HER-2lneu
amplification (p=0.03) and before any p53 mutational events (p<0.00006).
Furthermore, loss of ER and HER-Uneu amplification occurs before p53

mutations with p<0.00006 level of confidence. In spite of some elements not
being able to meet statistical significance, the data suggests that loss of either
~ 2 7 " ~ ' or ER ocairs before HER-Zneu amplification and p53 mutation as
depicted at the bottom of Table 9. An increase in the size of the cohort, resulting
in an increase in the power of the study, should be able ta bring to statistical
significance those elernents in this analysis which now only shown a strong
tendency. The second line of statistical evidence of order comes from the
assumption that intermediate grade tumours from our cohort represent a stage
that is intermediate not only in histologic and morphologie appearance, but rather
it is also an interrnediary stage in the developmental processes which drive
differentiation. Therefore, this stage can be considered a chronologicai
intermediate between low grade and high grade carcinoma. Table 10 represents
a tabulation of al1 intermediate grade (IG) tumours found in our cohort versus the
expression of molecules studied. For each molecule, the percentage of cases
with altered expression as compared to their low grade counterparts was
tabulated at the intermediate stage. Theoretically, any molecule which
dernonstrated a significant alteration suggests that the change more likely
occurred between the stages of low grade disease and intermediate grade
disease, and therefore relatively early in the chronological series of events. The
results of the tabulation have shown that loss of ~ 2 7 " ~ ' (68.8% of IG cases)
occurs before the loss of estrogen receptor (27.5% of IG cases) and ER loss
likely occurs prior to HER-2lneu amplification (18.8% of IG cases). while stable
p53 overexpression occur last (8.8% of IG cases).

Table 10. Represents the statistical tabulation of the number of Intermediate Grade cases which showed altered levels of immunohistochemical expression of the studied molecules. This analysis can give preliminary insight into an order of molecular events with respect to one another. The number of cases expressing high LEVELS (indicated by a '+' sign) of each molecule were deterrnined and scored. In a similar manner, the number of cases expressing low LEVELS (indicated by a '-' sign) of each molecule were determined and scored. The scores were collected from each morphologie subtype of tumour, DCIS + INV, DCIS ALONE, and INV ALONE. A COHORT average was established for al1 intermediate grade cases (n=80). For each molecule the ratio of the lower number of cases to the higher number of cases was tabulated (% ALTERED EXPRESSION). The largest of these figures represents the molecule which is most frequently involved in altered expression and therefore most probably occurring first. The results indicated that loss of p27 expression occurs prior to loss of ER status prior to HER-2 overexpression prior to stable p53 overexpression. The data supports the putative order predicted by the McNemar's test (Table 9).

Table 1 O. Statistical data for order of molecular events using Intermediate Grade turnour analysis
MOLECULE LEVELS DCIS + INV DCIS ALONE INV ALONE COHORT % ALTERED + = high n=53 n=16 n=l 1 n=80 EXPRESSION - = low

5.2 Correlation between the gredo of the in situ and associated invasive component in mixed cases
In cases with both an in situ and invasive camponent, we found a
significant correlation between the grade of these wmponents (p<O.OOl). This
finding supports the contention that the invasive component arises from the
associated in situ component and indicates that the propensity for invasion is to a
significant degree independent of intraductal progression, i.e.. progression from
low to high grade in situ carcinoma. This is in contrast to linear models in which
invasion is only associated with high grade precursors(Fearon and Vogelstein.
1990). For example. invasion is only associated with high grade intraepithelial
lesions in the cervix(Ponten and Guo. 1998) and high grade dysplasia in the
colon(Fearon and Vogelstein, 1990). These findings suggest that the molecular
pathways involved in the progression from low to high grade precursors in these
two cancers are closely linked to those mediating invasion and that progression
of precursors is essential for invasion to occur. In contrast. in breast cancer. the
molecular pathways appear to bel to a significant degree independent in that
invasion occurs in many cases from low grade DCIS. This is supported by the
fact that in most series, low grade invasive lesions are seen in approximately 20-
30% of breast cancer cases(Page and Anderson, 1987). while intermediate
grade invasive lesions are seen in approximately 3040%(Page and Anderson,
1987) and high grade invasive lesions in approxirnately 40-50%(Page and
Anderson, 1987).

The separation of invasion and in situ progression creates considerable
potential for heterogeneity with regard to the balance of the in situ and invasive
components. The eventual phenotype, is generated by the timing of invasion
and intraductal progression. At one end of the spectrum. if invasion ocairs early
in progression, there is little or no associated in situ carcinoma. On the other
hand, if invasion is a late event, there is extensive intraductal disease with a
small invasive wmponent. A spectrurn of associations can be observed between
the ends of the spectrum. This contributes to the extensive heterogeneity seen in
breast cancer. Cancers which follow a linear model (cervical or colon cancer).
where progression is linear along a single molecular and morphologie pathway
have a relatively narrow phenotypic spectrum. These findings corroborate those
of other authors who perfoned a similar study on the association of the grade of
DCIS and invasive carcinoma (Goldstein and Murphy, 1996).
5.3 Intralesional progression
Approximately 20% of the entire cohort consisted of cases which showed
signs of intralesional progression from low to high grade disease. This represents
progression from low to high grade lesions within the same tumour and indicates
that many cancers progress through recognizable precursors as opposed to de
novo progression. Plate VI t shows an example dernonstrating intralesional
progression in a case of DCIS. There is an area of low grade DCIS (arrow)
showing high ~ 2 7 ~ ~ ' levels, high ER expression and minimal mutant p53
overexpression or HER-2Jneu overexpression. Just adjacent to it is an area of

Plate VIL Intralesional progression was again noted in many cases from the cohort as evidenced by differential antibody staining within the same lesion. This plate illustrates the contrasting expression pattern seen using various antibodies on one particular case of intralesional progression. The H&E slide confirms the heterogeneous rnorphology of this case. The arrow indicates low grade portion of lesion, while the surrounding region is higher grade. In the p27 image. both low grade (dark staining regions) and higher grade (lighter staining regions) can be seen. In contrast, for p53, the low grade component is seen to have very little staining for mutated protein while the surrounding higher grade component has approximately 20 to 30% of cells with darkly stained nuclei. ER positive cells are abundant in the low grade portion of the lesion as determined by the intensity of the staining, while the higher grade regions contain lower overall levels of staining. HER-2 expression is markedly increased in the high grade portions of the lesion and the low grade region seems to be largely negative for HER-2 overexpression. (X40 Magnification)

PLATE VI1

histologically higher grade OClS showing decreased ~ 2 7 ~ ~ ' levels, HER-Zneu
overexpression and stable p53 protein. Plate II illustrates intralesional
progression with regard to ~ 2 7 ~ ~ ' levels (page 120). Panel A shows an in situ
lesion with a low grade area in the center of the duct surrounded by a higher
grade component. ~ 2 7 ~ ~ ' levels are high in the low grade area and are
decreased in the higher grade cornponent. Panels B and C are from the same
case and illustrate low grade invasive carcinoma with high levels of ~ 2 7 ~ ~ ' and
an area of high grade carcinoma showing decreased ~ 2 7 ' " ~ ' levels. N represents
a normal duct. These cases demonstrate intralesional progression in both in situ
and invasive disease. The observation of intralesional progression indicates that
in some cases, the in situ carcinorna progresses through the spectrum of grades
rather than moving frorn low grade in situ to invasive disease.
5.4 Ovewiewandirnplications
The rnolecular evenh studied here suggest that their roles lie mainly in the
processes that promote increases in cellular proliferation and loss of
differentiation rather than invasion. Although as discussed below, links between
these processes rnay occur. A decrease in the level of ~ 2 7 ~ ~ ' removes one of
the key inhibitory signals to the cell cycle potentially resulting in, increased
proliferative activity and tumour growth. In addition, as indicated above, ~ 2 7 ~ ' ~ '
plays an important role in differentiation and therefore a decrease in ~ 2 7 ~ ' ~ '
levels may contribute to the loss of differentiation seen in tumour progression.

Loss of ER receptor expression occun in the progression from low to high
grade disease and correlates with increased growth as estrogen independent
mechanisms of growth stimulation increase. The role of reduced ER levels in
other aspects of progression is not clear.
Overexpression of HER-2heu has been shown to induce growth in
tumour cells and this is consistent with its role as a growth factor receptor. HER-
2lneu amplification may also play a role in promoting cell motility and recently
has been shown to upregulate VEGF and promote angiogenesis(Petit et a/.,
1997). These functions may enhance the ability of tumour cells overexpressing
HER-2lneu to spread, invade and metastasize and offer another reason for its
association with a poorer prognosis. While the role of angiogenesis in the
dissemination of invasive carcinoma is becoming increasing more
established[Kodama, 1999 #157; Brown. 1999 #153; Heffelfinger, 1996 #154;
Horak, 192 #160], its role in situ carcinomas has not been entirely
clear(Heffe1finger et al., 1996). lnfiltrating breast carcinomas measuring > or =
0.5cm in sire are more likely to demonstrate metastasis(Saiz et al., 1999). It has
however. been shown recently. that angiogenesis is essential for the initial
processes of invasion which is consistent with the finding that the "angiogenic
switch" is observed in the preinvasive stage in al1 tumour systems
studied(Folkman. 1994; Kodama et al.. 1999; Pluda, 1997). Furthemore.
staining of microvessels with antibodies to factor VIII-related antigen has
revealed nonneovascularized as well as neovascutarized carcinoma in situ in

the same histologic section(Weidner et al., 1991). Thus molecular events
involving HER-Wneu may both contribute not only to progression from low to high
grade lesions, but also to some degree in invasion and metastasis(Petit. et al.,
1997).
p53 norrnally induces apoptosis in response to genetic
damage(Greenblatt, et al.. 1994). Mutations abrogate this function and not only
allow uncontrolled growth, but the propagation of genetic damage that increases
genetic instability. Recently, it has been shown that p53 mutations cause an
upregulation of VEGF and promote angiogenesis(Gasparini et al., 1993).
Therefore mutations of p53 may contribute to progression by increasing growth
and by inducing angiogenesis(Folkrnan, 1994) in a analogous fashion to HER-
2lneu overexpression.
Our findings show a correlation between the grade of primary tumour and
the associated metastases suggesting that to some degree, metastasis is
independent of grade. However, both in our study and in the literature, grade is
strongly correlated with the propensity for metastasis (Saiz, et al., 1999;
Urdiales-Viedma et al., 1986) and the molecular events studied are strongly
implicated in the metastatic process. We were able to define a subset of low
grade cases that metastasized despite the absence of the molecular events
studied. This suggests that these tumoun metastasize by mechanisms other
than those studied(Kondapaka, et al., 1997) and also underscores the fact that

there may be different molecular pathways to achieve the same end result. A
possible explanation for the increased propensity for invasion associated with
increasing grade is that the molecular changes studied above are associated
with an increased growth rate and increased size which is dependant on
angiogenesis for a blood supply (see above)(Saiz, et al., 1999). The increased
blood supply provides potential access for systemic dissemination and
metastasis. ln addition, as discussed above, HER-2fneu overexpression(Petit, et
al., 1997) and p53 mutations(Folkman, 1994) may upregulate angiogenesis and
thereby provide additional increase in the risk of metastasis.
Figure 10 is a schematic depiction of a possible order of lesional formation
in breast cancer progression. Hyperplastic lesions, which have been shown to
have clonal genetic abnormalities, aquire additional genetic abnormalities and
develop atypia as demonstrated in previous studies(Allred. et al., 1994;
O'Connell, et al., 1994). With further genetic darnage, these lesions progress to
the in situ stage that, in general, is low grade. If at this point. a subclone of
turnour cells acquire the capacity to invade, there will be a low grade invasive
component. The earlier this event occurs. the less the amount of associated in
situ carcinoma. If invasion is a late event, there will be extensive associated
DCIS. At this point. a number of events can occur. Progression of the in situ
cornponent can continue to higher grades, progression of the invasive
component can occur to higher grade lesions or a component of the low grade
invasive component can aquire the capacity to metastasize. In addition, the

Figure 10. ln vivo representation of breast cancer progression. Precursors of carcinoma can lead to the development of Low Grade DClS within the ductal system of a breast. The low grade disease can either progress to a low grade invasive tumour existing and growing in the STROMA or it may progress by losing differentiation status and develop a higher grade more aggressive in situ lesions. In some cases studied, a spectrum of grades was discovered in the in situ lesions leading to the phenomenon of intralesional progression and heterogeneity. High Grade (HG) invasive carcinoma can develop from the in situ lesion and subsequently set up lymph node metastases (HG Met). Although observed less frequently, but in a similar manner, Low Grade (LG) invasive carcinoma can lead to low grade metastatic disease (LG Met) where if present for a number of years may lead to high grade metastatic carcinoma.

DUCT \ ;ion al Progression
I HG Invasion
HG Invasion
LYMPH NODES

higher grade invasive cornpanent may also metastasite. It is also possible that
invasion does not occur from the low grade, but rather from the high grade in situ
lesion. There are innumerable combinations of the possible events and this
generates the marked heterogeneity observed in breast cancer(Patchefsky, et
al., 1989).
It has recently k e n shown that loss of heterozygosity may be found in
normal tissue adjacent to invasive tumoun suggesting that direct progression
rnay occur from normal to invasive carcinoma(Deng et al., 1996) in some
tumours. This has been used to explain the finding of pure invasive carcinoma
without identifiable in situ carcinoma. Another possible explanation is that the
precursor lesions are overgrown by the tumour cells with a growth advantage. It
is however, possible that progression from precursors can occur along multiple
pathways as outlined in Figure 1 i in the next page.
Our data demonstrates that the molecular events studied show a specific
and consistent pattern in relationship to the stages of breast cancer progression
and our hypothesis is that other key genetic events in breast cancer progression,
for example those involved in apoptosis(Eissa, et al., 1999), will follow a similar
pattern.

Figure 11. Representatlon of multiple pathway progression in breast cancer. The following figure is an attempt to illustrate the varied complexity of breast cancer evolution and progression. As illustrated, normal epithelium may give rise diredly to invasive carcinoma (de novo) ( i ) or may go through the normal pathways of precursor progression to invasion ( ii ). Alternatively, and most commonly, tumours will develop a spectrum of in situ and invasive lesions ( iii ) The red component of the figure represents the stages investigated in this study. It is believed that the transformation from a non- invasive, confined in situ tumour to an invasive, motile and more aggressive form is a key transitory step in the progression from a potentially curable disease to an otherwise predictably fatal one.

NORMAL
1
LG DCIS 1 i LGINV 1
1 HG DCIS / HG INV
1 LGINV 1-1 H G I N V ~

5.5 lmpact on patient can,
The findings also suggest that the designation of in situ lesions as "early"
or "low risk" and invasive cancer as "high risk" may be inaccurate in breast
cancer. In some respects, the tumour celfs in high grade DClS have changes
associated with high grade invasive carcinomas despite their inability to invade
the basement membrane. Therefore, although high grade DClS has no risk of
metastasis per se, when a high grade DClS tumour does invade, the invasive
tumour will already have undergone significant molecular changes that increase
the risk of systemic spread. Furthermore. high grade in situ lesions have been
shown to have associated angiogenesis which increases the chance of
metastatic dissemination if invasion occurs. Thus our findings indicate that
prognosis may be detennined not only by the presence of invasion and
progression of the invasive component, but may also be influenced by the
degree of intraductal progression.

CHAPTER 6
FUTURE STUDIES

6. FUTURE STUDIES
This thesis describes a subset of rnolecular events and their relationship
to key stages in breast cancer progression. Simultaneous analyses of several
different genetic alterations in tumour samples can be achieved only by using
techniques such as laser capture microdissection(Bornstein, et al.. 1998)
followed by microsatellite analysis of loss of heterozygosity(Amari et al.. 1 999) or
comparative genomic hybridization(Roy1ance et al.. 1 999). We have
microdissected specific stages of progression in over 200 cases and have
extracted DNA from these lesions. We have established microsatellite analysis
for the key loci deleted in breast cancer and plan to study a subset of cases
which show evidence of intralesional progression to determine molecular
reiationships between the different stages observed within the same tumour.
Currently, although numerous studies investigating LOH in breast cancer have
been performed(Amari, et al., 1999; Gonzalez et al.. 1999; Hampl et al.. 1999).
there is considerable confusion about the role of these events in breast cancer
progression. We may be able to better define the relationship between these
deletional events and the key stages of breast cancer progression in a manner
analogous to the study outlined above. Events that are essential for invasion will
be seen in a small proportion of pure in situ carcinomas and in al1 invasive
lesions. In our study. using ~ 2 7 ~ ~ ~ ' as an example. we see a high proportion of
cases of low grade DClS with high ~ 2 7 ~ ~ ' levels and the same proportion of low
grade invasive carcinomas with high ~ 2 7 " ~ ' levels. This suggests that in a

subset of cases, decreased ~ 2 7 ~ ~ ' is not essential for the procass of invasion.
The focus of future studies will be in deciphering in more detail the genetic and
molecufar basis for invasive progression of breast cancer.
Breast cancer is a heterogeneous malignancy in which the prognosis varies. not
only with the extent of disease, but also with its biologic behavior. For this
reason, the prognostic assessrnent of patients with breast cancer has become
increasingly important, and additional variables are needed to give
supplernentary information that can lead to a better understanding of the biology
of mammary carcinoma and help in the choice of the correct treatment. We used
different factors known to be important in breast cancer progression to develop a
hypothetical model of breast cancer progression. We have learned that breast
tumour progression is bimodal with some tumours developing an early invasive
phenotype while others continue to grow to higher grades as a noninvasive.
poorly differentiated entity. The separation of invasion from intraductal
progression creates two potential routes of progression (birnodal) and the
eventual phenotype is determined both by the timing of invasion in relation to
intraductal progression, as well as, progression of the invasive component. This
indicates that, in contrast to cancers that show linear progression(Fearon and
Vogelstein, 1990). the degree of intraductal progression makes a significant
contribution to prognosis. It is also apparent that the tumour cells in high grade in
situ carcinomas show changes associated with high grade invasive carcinomas
despite their inability to invade the basement membrane(Gupta, et al., 1997).

This. in addition to the fact that invasion at this stage leads to a high grade
invasive carcinoma, also suggests that these lesions may not be early or low risk
as in cancers that follow the linear paradigm. The validation and further
development and refinement of our theory of progression may one day afford
more information on tumour aggressiveness and provide currently unrealized
modalities for therapeutic action.

REFERENCES
Akashi, M., and Koeffier, H. (1998). "Li-Fraumeni syndrome and the role of the p53 tumor suppressor gene in cancer susceptibility."Clin Obstet Gynecol 41, 172-199.
Albonico, G., Querzoli, P., Feretti, S., Magri, E., and Nenci, 1. (1996). "Biophenotypes of breast carcinoma in situ defined by image analysis of biological parametersnPath Res Pract 192, 1 17-1 23.
Aldaz, C., Chen, T., Sahin, A., Cunningham, J., and Bondy, M. (1995). "Comparative allelotype of in situ and invasive human breast cancer: high frequency of microsatellite instability in lobular breast carcinomas."Cancer Res 55,3976-3981.
Ali, I., Lidereau, R., Theillet, C., and Calahan, R. (1987). "Reduction to homozygosity of genes on chromosome 1 in human breast neoplasia."Science 238, 185-1 88.
Allen, J. (1 995). "Molecular biology of colon polyps and colon cancer." Seminars in Surgical Oncology. 1 1, 399405.
Allred, O., O'Connell, P., Fuqua, S., and Osborne, C. (1994). "lmmunohistochemicaI studies of early breast cancer."Br. Cancer Res. Treat. 32, 13-1 8.
Amari, M., Suzuki, A., Moriya. T., Yoshinaga, K.. Amano, G., Sasano, H., Ohuchi, N., Satomi, S., and Horii, A. (1999). "LOH analyses of premalignant and malignant lesions of human breast: frequent LOH in 8p, 16q, and 17q in atypical ductal h yperplasia."Oncol Rep 6, 1 277-1 280.
An, H., Niederacher, D., Dominik, S., Kuschel, B., Yan, H., Dall, P., Schnurch, H., Bender, H., and Beckmann, M. (1997). "int-2 and cerbB-2 gene amplification detected in 70 frozen human breast carcinomas b y quantitative polymerase chain reactionl'Anticancer Research 17, 31 33- 31 36.

Andersen, T., Gaustad, A., and Ottestad, L. (1992). "Genetic alterations of the tumour suppressor gene regions 3p, 1 1 p. l3q.l7p, and 179 in human breast carcinomas."Genes Chromosomes Cancer 4, 1 13-1 21.
Andersen, T., Holm, R., Nesland, J., Heimdal, K., Ottestad, L., and Borresen, A. (1 993). "Prognostic signifiant of TP53 alterations in breast carcinoma."Br J Cancer 68,540-548.
Anderson, D. (1 992). "Familial versus sporadic breast cancer."Cancer 70, 1 740- 1 746.
Andreasen, P. (1 997). "The urokinase-type plasminogen activator system in cancer metastasis: a review."lnt J Cancer 72, 1.
Baas, I., Mulder, J.-W., Offerhaus, G., Vogelstein, B., and Hamilton. S. (1 994). "An evaluation of six antibodies for immunohistochernistry of mutant p53 gene product in archival colorectal neoplasrns." J. Pathol. 172, 5-1 2.
Baker, S., Fearon, E., and Nigro, J. (1989). "Chromosome 17 deletions and p53 mutations in colorectal carcinomas."Science 244,217.
Barlund, M., Tirkkonen, M., Forozan, F., Tanner, M., Kallioniemi, O., and Kallioniemi, A. (1997). "lncreased copy number at 17q22-q24 by CGH in breast cancer is due to high-level amplification of two separate reg ions. "Genes Chromosomes Cancer 20,372-376.
Barnes, D., and Gillett, C. (1998). "Cyclin D l in breast cancer."Breast Cancer Res Treat 52, 1 -1 5.
Barnes, R., and Masood, S. (1990). "Potential value of hormone receptor assay in carcinoma in situ of breast."Am J Clin Pathol94, 533.
Bartkova, J., Barnes, D., Millis, R., and Gullick, W. (1990). "lmmunohistochemicaI demonstration of c-erbB-2 protein in mammary ductal carcinoma in situ."Human Pathol21, 1 1 64-1 1 67.

Basu, A., and Haldar, S. (1998). "The relationship between Bc12, Bax and p53: consequences for cell cycle progression and cell death."Mol Hum Reprod. 4, 1 099-1 1 09.
Becker, K., Atkinson, M., and Reich, U. (1994). "E-cadherin gene mutations provide clues to diffuse type gastnc carcinomas."Cancer Res 54, 3845- 3852.
Behrens, J.. Marcel, M., Von Roy, F.. and Birchmeier, W. (1989). "Dissecting tumour cell invasion: epithelial cells acquire invasive properties after the loss of uvomorulin-mediated cell-cell adhesion ." J Ce11 Biol 108, 2435- 2447.
Beviglia, L., Matsumoto, K., Lin. C., Ziober, B., and Kramer, R. (1997). "Expression of the c-MeüHGF receptor in human breast carcinoma: correlation with tumor progression."lnt J Cancer 74. 301 -309.
Black, D. (1 994). "The genetics of breast cancer."Eur J Cancer 30A, 1957-1 961.
Bobrow, L., Happerfield, L., Gregory, W., Springall, R., and Millis, R. (1994). "The classficiation of ductal carcinoma in situ and its association with biological markerswSemln Diagn Pathol 1 1 , 1 99-207.
Bohm, M., Totzeck, B., Birchmeier, W., and Wieland, 1. (1993). "Difference of E- cadherin expression levels and paterns in primary and metastatic human lung cancer" Clin Exp Metastasis 1 2, 55-62.
Bornstein, S., Willenberg, H., and Scherbaum, W. (1998). "[Progress in rnolecular medicine: "laser capture microdissection"]."Med Klin 93, 739- 743.
Bose, S., Wang, S. I., Terry, M. B., Hibshoosh, H., and Panons, R. (1 998). t'Allelic loss of chromosme lOq23 is associated with tumour progression in breast carinomanOncogene 17. 123-1 27.

Bouetti, C., Nizzoli, R., Naldi, N., Guazzi, A., Camisa, R., Bella, M., and Cocconi, G. (1999). "Bcl-2 expression on fine-needle aspirates from primary breast carcinoma: correlation with other biologic factors."Cancer 87,224-230.
Buerger, H., Otterbach, F., Simon, R., Poremba, C., Diallo, R., Decker, T., Riethdorf, L., Brinkschmidt, C., Dockhorn-Dwomiczak, B., and Boecker, W. (1 999). "Comparative genomic h ybridization of ductal carcinoma in situ of the breast-evidence of multiple genetic pathways."J Pathol 187, 396-402.
Bur, M. E., Zimarowski, M. J., Schnitt, S. J., Baker, S., and Lew, R. (1991). "Estrogen Receptor: lmmunohistochemistry in Carcinoma In Situ of the BreastNCancer 69,1174-1 181.
Busch, H. (1990). "The final common pathway of cancer: presidential address."Cancer Research 50,4830-4838.
Catzavelos, C., Bhattacharya, N., Ung, Y. C., Wilson, J. A., Roncari, L., Sandhu, C., Shaw, P., Yeger, H., Morava-Protzner, I., Kapusta, L., Franssen, E., Pritchard, K. I., and Slingerland, J. M. (1997). "Decreased levels of the cell-cycle inhibitor p27kipl protein: Prognostic implications in primary breast cancer"3, 227-230.
Chambers, A., and Matrisian, L. (1997). "Changing view of the role of matrix metalloproteinases in metastasis."J Nat1 Cancer lnst 89, 1260.
Chaudhuri, B., Crist, K., Mucci, S., Malafa, M., and Chaudhuri, P. (1993). "Distribution of estrogen receptor in ductal carcinoma in situ of the breast."Surgery 113, 134-137.
Chen, L., Kurisu, W., Ljung, B., Goldman, E., Moore, O., and Smith, H. (1992). "Heterogeneity for allelic loss in human breast cancer."JNCI 84, 506-51 0.
Cho, K., and Vogelstein. B. (1992). "Genetic altemations in the adenoma- carcinoma sequence."Cancer 70, 1727-1 731.

Chu, K., Tarone, R., and Kessler, L. (1 996). "recent trends in U.S. breast cancer incidence, survival, and mortality rates."J. Nat1 Cancer lnst 88, 1571-1 579.
Clark, G., and McGuire, W. (1988). "Steroid receptors and other prognostic factors in primary breast cancer."Semin Oncol (supp.) 15, 20-25.
Cole, M., and McMahon, S. (1999). "The Myc onwprotein: a critical evaluation of transactivation and target gene regulation."Oncogene 18,291 6-2924.
Coopman, P., Do, M., Thompson, E., and Mueller, S. (1998). "Phagocytosis of cross-linked gelatin matrix by human breast carcinoma ceffs correlates with their invasive capacity."Clin Cancer Res 4, 507-51 5.
Corbett, I., JA, H., and B. A. (1990). "NCL-CB1 1 : A new monoclonal antibody recognizing the intemal domain of the c-ehB-2 oncogene protein, effective for use on fonnalin fixed, paraffin embedded tissue"Journa1 of Pathology 161, 15-25.
Cox, L., Chen, G., and Lee, E. Y.-H. P. (1 994). "Tumor suppressor genes and their roles in breast cancer."Breast Cancer Res Tmat 32, 19-38.
Dairkee, S. H., and Smith, H. S. (1996). "Genetic Analysis of Breast Cancer Progression ." Journal of Mammary Gland Biology and Neoplasia 1, 1 39- 151.
Davidoff, A. M., Kerns, B.-j. M., Iglehart, J- D., and Marks, J. R. (1991). "Maintenance of p53 alterations throughout Breast Cancer Progression."Cancer Research 51,2605-261 0.
Del Bufalo, D., Biroccio. A., Leonetti, C., and Zupi, G. (1997). "Bcl-2 overexpression enhances the metastatic potential of a human breast cancer line."FASEB J 11,947-953.
Deng, G., Lu, Y., Zlotnikov, G., Thor, A., and Smith. H. (1996). "Loss of heterozygosity in normal tissue adjacent to breast carcinomas."Science 274,2057-2059.

Dupont, W., and Page, D. (1985). "Risk factors for breast cancer in women with proliferative breast disease."New England Journal of Medicine 31 2, 146- 151.
Edwards, D., and Murphy, G. (1 998). "Proteases- invasion and more."Nature 394, 527-528.
Eissa, S.. Labib, R., Khalifa, A., Swelam, N., Khalil. F., and El-Shenawy, A. (1 999). "Regulators of apoptosis in human breast cancer."Clin Biochem 32, 323 -326.
El-Ashry, D., and Lippman, M. (1994). "Molecular biology of breast carcinoma." World J Surg 18, 12-20.
El-Deiry, W., Tokino, T., Velculescu, V., Levy, D., Parsons, R., Trent, J., Lin, D., Mercer, W., Kinzler. K., and Vogelstein, B. (1993). "WAFI , a potential mediator of p53 tumor suppression."Cell75,817-825.
Elledge, R., Fuqua, S., Clark, G., Pujol, P., and Allred, D. (1993). "The role and prognostic significance of p53 gene alterations in breast cancer."Breast Cancer Res Treat 27,95-102.
Erlanson, M.. Portin, C., Linderholm. B., Lindh, J., Roos, G., and Landberg, G. (1998). "Expression of cyclin E and the cyclin-dependent kinase inhibitor p27 in malignant lymphomas-prognostic implications."Blood 92, 770-777.
Eshlernan, J., and Markowitz, S. (1996). "Mismatch repair defects in human carcinogenesis."Hum Mol Genet 5, 1489-1494.
Fang, F., Orend, O., Watanabe, H., Hunter, T., and Ruoslahti, E. (7996). "Dependence of CyclinE-CDK2 Kinase Activity on Cell Anchorage."Science 271,499-502.
Fearon, E., and Vogelstein, B. (1990). "A Genetic Model for Colorectal Tumorigenesis"Cell61, 759-767.

Fegan, C., White, D.. and Sweeney. M. (1 995). C m y c amplification. double minutes and homogenous staining regions in a case of AML."Br J Haematol90,486-488.
Fentiman, 1.. and Taylor-Papadimitriou, J. (1993). "Breast Cancer VOLUME 18: CSHL press."Cancer Surveys 18.
Fernando, S., Wu, X.. McKenzie, P., and Johnson, S. (1995). "lmmunohistochemicaI detection of p53 protein expression in mammary carcinoma: a study of 80 cases."Pathology 27,365-369.
Fero, M.. Randall. E., Gurley, K., Roberts, J.. and Kemp, C. (1998). "The murine gene p27Kipl is haplo-insufficient for tumor suppression."Nature 396, 177-1 80.
Folkman. J. (1 994). "Angiogenesis and breast cancer." Journal of Clinical Oncology 1 2,44 1 -443.
Fornaro, M.. Tallini. G., Zheng, D., Flanagan. W.. Manzotti. M., and Languino, L. (1999). "P27(kipl) acts as a downstream effector of and is coexpressed with the beta 1 C integrin in prostatic adenocarcinorna." J Ciin lnvest 103, 321 -329.
Fortuno, M., Zalba, G., Ravassa, S., D'Elom. E., Beaumont, F., Çortuno, A., and Diez, J. (1 999). "p53-mediated upregulation of BAX gene transcription is not involved in Bax-alpha protein overexpression in the left ventricle of spontaneously hypertensive rats."Hypedension 33, 1 348-1 352.
Fujii, H., Marsh. C.. Cairns, P., Sidransky. D., and Gabrielson. E. (1996). "Genetic divergence in the clonal evolution of breast cancer-"Cancer Res 56, 1493-1497.
Gamallo, C., Palacios, J., and Suarez, A. (1993). "Correlation of E-cadherin expression with differentiation grade and histological type in breast carcinomal'Am J Pathol143, 1 731 -1 742.

Gasparini, G., Weidner, N., Maluta, S., Pona, F., Boracchi. P:, Meuetti, M., Testolin, A., and Bevilacqua. P. (1993). "lntratumoral microvessel density and p53 protein: correlation with metastasis in head-and-neck squamous- cell carcinoma ."/nt. J. Cancer 55, 739-744.
Gerbitz, A., Mautner. J., Geltinger, C., Hortnagel, K., Christoph, B., Asenbauer, H., Klobeck, G., Polack. A., and Bornkamm, G. (1999). "Deregulation of the proto-oncogene c-myc through t(8;22) translocation in Burkitt's lymphorna."Oncogene 18,1745-1 753.
Giavazzi, R., Alessandri, G., Spreafico, F., Garattini, S., and Mantovani, A. (1 980). "Metastasizing capacity of tumour cells from spontaneous metastases of transplanted murine tumours."Br J Cancer 42,462-472.
Giri, D., Dundac. S., and Nottingham, J. (1989). "Oestrogen receptors in benign epithelial lesions and intraductal carcinomas of the breast: an immunohistolog ical stud y."Histopathology 1 5, 575-584.
Goldstein, N., and Murphy, T. (1996). "Intraductal Carcinoma Associated with Invasive Carcinoma of the Breastl'Anatomic Pathology 106, 31 2-31 8.
Gonzalez, R., Silva, J.. Dominguez, G., Garcia, J., Martinez, G., Vargas, J., Provencio, M., Espana, P., and Bonilla, F. (1999). "Detection of loss of heterozygosity at RADSI, RA052, RAD54 and BRCAl and BRCA2 loci in breast cancer: pathological correlations."Br J Cancer 81, 503-509.
Gray, J., Collins, C., Henderson, I., Isola, J., Kallioniemi, A., Kallioniemi, O., Nakamura, H., Pinkel. D., Stokke. T., and Tanner, M. (1994a). "Molecular cytogenetics of human breast cancer."Cold S p h g Ha& Symp Quant Bi01 59,645-652.
Gray, J., Collins, C., Henderson, I., Isola, J., Kallioniemi, A., Kallioniemi, O.-P., Nakamura, H., Pinkel, D., Stokke, T., Tanner, M., and Waldman, F. (1 994b). "Molecular Cytogenetics of Human Breast Cancer.", 645-652.
Greenblatt, M., Bennett, W., Hollstein. M., and Harris, C. (1994). "Mutations in the p53 Tumor Suppressor Gene: Clues to Cancer Etiology and Molecular PathogenesisWCancer Research 54,48554878-

Guirguis, R., Margulies, I., Taraboletti, G.. Schiffmann, E., and Liotta, L. (1987). "Cytokine-induced pseudopodial protrusion is coupled to tumour cell migration."Nature 329, 261 -263.
Gupta, S., Douglas-Jones, A.. Fenn, N.. Morgan, J., and Mansel, R. (1997). '.The Clinical Behaviour of Breast Carcinoma 1s Probably Determined at the Preinvasive Stage (Ductal Carcinoma In Situ)"Cancer 80, 1740-1 745.
Hampl, M., Hampl. J., Reiss. G.. Schackert, G., Saeger. H., and Schackert, H. (1 999). "Loss of heterozygosity accumulation in primary breast carcinomas and additionally in wrresponding distant metastases is associated with poor outcorne."C/in Cancer Res 5, 141 7-1 425.
Hartwell, L. (1992). "Defects in a cell cycle checkpoint may be responsible for the genomic instability of cancer cells."Ce// 543, 546.
Hashimoto, M.. Niwa, O., Nitta. Y.. Takeichi, M.. and Yokoro, K. (1989). "U nstable expression of E-cad herin ad hesion molecufes in metastatic ovarian tumor cells."Jpn J Cancer Res 80,459-463.
Hashizume, R., Koizumi, H., and Ihara. A. (7996). "Expression of B-catenin in normal breast tissue and breast carcinoma: a comparative study with epithelial cadherin and a-catenin."Histopathology 29, 139-1 46.
Heffelfinger, S., Yassin, R., Miller, M.. and Lower. E. (1996). "Vascularity of proliferative breast disease and carcinoma in situ correlates with histological features."Clin Cancer Res 2, 1873-1 878.
Helin, H.. Helle, M.. Kallioniemi, O.-P., and Isola. J. (1989). "Immunohistochemical determination of estrogen and progesterone receptors in human breast carcinoma: correlation with histopathology and DNA flow cytometry."Cancer 63, 1 76 1 -1 767.
Helzlsouer, K.. Alberg, A.. Bush, T., Longcope, C., Gordon. G., and Cornstock, G. (1994). "A prospective study of endogenous hormones and breast cancer."Cancer Detect Prev 18, 79-85.

Hengst, L., Dulic, V., Slingerfand. J., Lees, E., and Reed, S. (1994). "A cell cycle regulated inhibitor of cyclin dependant kinases."Proc. NatLAcad. Sci. 91, 5291 -5294.
Horne, G., Anderson, J., Tiniakos, D., Mclntosh, G., Thomas, M., Angus, B.. Henry, J., Lennard, T., and Home, C. (1 996). "P53 protein as a prognostic indicator in breast carcinoma: a wmparison of four antibodies for immunohistochemistrynBntish Journal of Cancer 73,29-35.
Hortobagyi, G. (1 998). "Treatment of Breast Cancer." The New England Journal of Medicine 339, 974-984.
Houston, S., Plunkett, T., Barnes, D-, Smith, P., Rubens, R., and Miles, D. (1 999). "Overexpression of c-erbB2 is an independent marker of resistance to endocrine therapy in advanced breast cancer."British Journal of Cancer 79, 1 220-1 226.
Huberman, E. (1 988). "The potential role of cell differentiation in carcinogenesisWin Carcinogenesis , 247-258.
Hynes, N., and Stern, D. (1995). "The biology of erbB-2IneulHER-2 and its role in cancei'Biochim. Biophys. Acta 1 198, 165-1 84.
Isola, J., Kallioniemi, O., Chu, L., Fuqua, S., Hilsenbeck, S., Osborne, C., and Waldman, F. (1 995). "Genetic aberrations detected by comparative genomic hybridization predict outcome in node-negative breast cancer."Am J Path 147, 905-91 1.
Ito, I., Yoshimoto, M., Iwase, T., Watanabe, S., Katagiri, T., Harada, Y., Kasumi, F., Yasuda. S., mitomi, t., Emi. M., and Nakamura, Y. (1995). "Association of genetic alterations on chromosome 17 and loss of hormone receptors in breast cancer."Br. J. Cancer 71,438441.
Iwata, H., Kobayashi, S., Iwase, H., and Okada, Y. (1995). "The expression of MMPs and TlMPs in human breast cancer tissues and importance of their balance in cancer invasion and metastasis."Nippon Rinsho 53, 1805-1 81 0.

Jansen-Durr, P. (1996). "How viral oncogenes make the cell cycle."Trends Genet 12,270-275.
Jensen, R., Dupont, W., and Page. D. (1993). "Diagnostic criteria and cancer risk of proliferative breast lesions." J Ce// Biochem 17, 59-64.
Johannsdottir, J., Bergthorsson, J., Gretarsdottir, S., Kristjansson, A., Ragnarsson, G- , Jonasson. J., Egilsson, V., and Ingvarsson, S. (1999). "Replication error in colorectal carcinoma: association with loss of heterozygosity at mismatch repair loci and clinicopathological variables."Anticancer Res 19, i 821 -1 826.
Jonjic, N., Lucin, K., Krstulja, M., Iternicka, 2.. and Mustac, E. (1993). "Expression of Beta-1 lntegrins on Tumor Cells of Invasive Ductal Breast Carcinoma."Path. Res. Pract. 189, 979-984.
Kaelin, W. (1997). "Recent insights into the functions of the retinoblastoma susceptibility gene product."Cancer lnvest 15, 243.
Kallioniemi, A., Kallioniemi, O.-P., Kurisu, W., Thor, A., Chen, L., Smith, H., Waldman, F., Pinkel, D., and Gray, J. (1992). "ERBB2 amplification in breast cancer analyzed by Ruoresence in situ hybridization."Proc Natl Acad Sei 89,532 1 -5325.
Kallioniemi, A.. O-Pl K., Piper, J., Tanner, M., Stokke, T., Chen, L.. Smith, H., Pinkel, D., Gray, J., and Waldman. F. (1994). "Detection and mapping of arnplified DNA sequences in breast cancer by comparative genomic hybridization."Proc Natl Acad Sei 91, 21 56-2160.
Katayose. Y., Kim, M.. Rakkar, A., Li. Z., Cowan. K., and Seth, P. (1997). "Promoting apoptosis: a novel activity associated with the cyclin- dependent kinase inhibitor p27"Cancer Research 57, 5441-5445.
Kerns, B., Jordan, P., Huper, G., Marks, J., Iglehart, J., and JL, L. (1993). "Assessment of c-erbB-2 Amplification By Irnmunohistochemistry ln Paraffin-Embedded Breast Cancer"Modem Pathology 6,673-678-

Kinsella, A., Green, B., Lepts, G.. Hill, C., Bowie, G., and Taylor, B. (1993). "The role of the cell adhesion molecule E-cadherin in large bowel tumour cell invasion and metastasisuBr J Cancer 67, 904-909.
Kintanar, E., and Raju. U. (1991). "Further delineation of patterns of atypical ductal hyperplasia (ADH): an analysis of ADH patterns associated with intraductal and invasive breast carcinorna."Modem Pathol4.
Kiyokawa, H., Kineman, R., manova-Todorova, K., Soares, V., Hohan , E., Ono, M., Khanam, D., Hayday, A., Frohman, L., and Koff, A. (1996). "Enhanced growth of mice lacking the cyclin-dependent kinase inhibitor function of p27kipl ."CeIl 85, 721 -732.
Kodama, J., Seki, N., Tokumo, K., Hongo, A., Miyagi, Y., Yoshinouchi, M., Okuda, H., and K u ~ o , T. (1999). "Vascular endothelial growth factor is implicated in early invasion in cervical cancer."Eur J Cancer 35,485-489.
Kondapaka, S., Fridman, R., and Reddy, K. (1997). "Epidermal growth factor and amphiregulin up-regulate matrix metafloproteinase-9 (MMP-9) in human breast cancer cells."lnt J Cancer 70, 722-726.
Koreth, J., Bethwaite, P. B., and McGee, J. O. D. (1995). "Mutation at chromosome 11q23 in hurnan non-familial breast cancer: a microdissection microsatellite analysis." J. Pathol. 17 6, 1 1-1 8.
Kostog lou-Athanassiou, I., Ntalles, K., Gogas, J., Markopoulos, C., Alevizou- Terzaki, V., Athanassiou. P., Georgiou. E., and Proukakis, C. (1997). "Sex hormones in postmenopausal women with breast cancer on tamoxifen."Hom Res 47, 1 16-1 20.
Kuukasjarvi, T., Karhu, R., Tanner, M., Kahkonen, M., Schaffer, A., Nupponen, N., Pennanen, S., Kallioniemi, A., Kallioniemi, O., and Isola, J. (1997a). "Genetic heterogeneity and clonal evolution underlying development of asynchronous metatasis in human breast cancer."Cancer Research 57, 1 597-1 604.

Kuukasjarvi, T., Tanner, M., Pennanen, S., Karhu, R., Kallioniemi, O., and Isola, J. (1 997b). "Genetic changes in intraductal breast cancer detected by comparative genornic hybridization."Ame~an Journal of Pathology 150, 1465-1471.
Kwaan, H. (1992). "The plasminogen-plasmin system in malignancy."Cancer Metastasis Rev 11,291 -31 1.
Lakhani, S., Collins, N., Sloane, J., and Stratton. M. (1995). "Loss of heterozygosity in lobular carcinoma in situ of the breast."J Clin Pathol48, 74-78.
Lane, D. (1 992). "p53, Guardian of the genome."Nature 358, 15.
Lane, D., and Hall, P. (1997). "MDM2-arbiter of p53's destruction."Trends Biochem Sci 22, 372-374.
Lavarino, C., Corletto, V., Menelani, A., Della Torre, G., Bartoli, C., Riva, C., Pierotti, M., Rilke, F., and Pilotti, S. (1998). "Detection of TP53 mutation, loss of heterozygosity and DNA content in fine-needle aspirates of breast carcinoma."Br J Cancer 77, 1 25-1 30.
Leal. C., Schmitt, F., Bento, M., Maia, N., and Lopes, C. (1995). "Ductal carcinoma in situ of the breast. Histotogic categorization and its relationship to ploidy and immunohistochemical expression of hormone receptors, p53 and c-erbB-2 proteinXancer 75, 2123-31.
Levenberg, S., Yarden, A., Kam, Z., and Geiger, B. (1999). "p27 is involved in N- cadherin-rnediated contact inhibition of cell growth and S-phase entry . "Oncogene 1 8,869-876.
Levine, A., Mornand. J-, and Finlay, C. (1991). "The p53 tumour suppressor gene."Nature 351,453.
Levkau, B., Koyama, H., Raines, E., Cluman, B., Herren, B., Orth, K., Roberts, J., and Ross, R. (1998). "Cleavage of p2lcipI/wafl and p27kip1

mediates apoptosis in endothelial cells through activation of Cdk2: role of a caspace cascade"Mol Ce11 1,553-563.
Lilia, M. (1 999). "Chronological Age Should not Influence Management Decisions"GenatricsdAging 2, 8-23.
Lin, S C . (1996). "Genes in the Rb pathway and their knockout in rnice."Semin Cancer Biol7, 279.
Liotta, L., and Kohn, E. (1997). "Invasion and metastasis. In Holland, JF et al (eds): Cancer Medicine, 4th ed. Baltimore, Williams & Wilkins, 1997", 165.
Lippman, M., Dickson, R., Bates, S., Knabbe, C., Huff, K., Swain, S., McManaway, M., Bronzert, O., Kasid, A., and Gelrnan, E. (1986). "Autocrine and paracrine growth regulation of human breast cancer."Cancer 50,2265-2268.
Liu, E., Thor, A., and He, M. (1992). '@The HER2 (c-erbB-2) oncogene is frequently amplified in in situ carcinomas of the breast."Oncogene 7, 1027-1 032.
Madigan, M., Ziegler, R., Benichou, J.. Byrne, C., and Hoover, R. (1995). "Proportion of breast cancer cases in the United States exlained by well- established risk factors." J. Nat1 Cancer lnst 87, 1681 -1 685.
Malafa, M., Chaudhuri, B., and Thomford, N. (1990). "Estrogen receptors in ductal carcinoma in situ of the breast."Amencan Surgeon 56,436.
Mareel, M., Behrens, J., Birchmeier, W., De Bruyne, G., Vleminckx, K., and Hoogewijw, A. (1991). "Down-regulation of E-cadherin expression in Madin-Darby canine kidney (MDCK) cells inside tumors of nude mice."lnt J Cancer 47,922-928.
Marra, G., and Boland, C. (1996). "DNA Repair and colorectal cancer."Gastmenteml Clin North Am 25,755.

Martinani, M., Crivelli, F., Zampatti, C., and Martinani, S. (1993). "Relationship between p53 expression and other prognostic factors in human breast carcinoma. An immunohistochemical study."Am. J. Clin. Pathol., 100, 21 3- 21 7.
McCarty, K. J., Miller, L., and Cox, E. (1985). "Estrogen receptor analysis. Correlation of biochemical and immunohistochemical methods using monoclonal antireceptor antibodiesNArch Path Lab Med 109, 71 6-721.
Miki, Y. (1994). "A strong candidate for the breast and ovarïan cancer susceptibility gene BRCAI ."Science 266,66.
Mizurnatsu, S., Tamiya, T., Ono, Y., Abe, T., Matsumoto, K., Furuta, T., and Ohmoto, T. (1999). "Expression of cell cycle regulator p27Kip1 is correlated with survival of patients with astrocytoma."Clin. Cancer Res. 5, 551 -557.
Molino, A., Micciolo, R., and Turaua, M. (1995). "Estrogen receptors in 699 primary breast cancers: a cornparison of immunohistochemical and biochemical methods."Breast Cancer Res and Tmat 34,22 1 -228.
Molino, A., Turaza. M., and Bonetti, A. (1992). "Estrogen and progesterone receptors in breast cancer: correlation with clinical and pathological features and with prognosis."Oncology 49, 82-88.
Moll, R., Mitre, M., Frixen, U., and Birchmeier, W. (1 993). "Differential loss of E- cadherin expression in infiltrating ductal and lobular breast carcinomas"Am J Pathol143, 1731-1 742.
Morgan, D. (1 995). "Principles of Cdk regulation."Nature 374, 1 31 -1 34.
Morosetti, R., Kawamata, N., Gombart, A., Miller, C., Hatta, Y., Hirama, T., Said, J., Tomonaga, M., and Koeffier, H. (1995). "Alterations of the p271kipl gene in non-Hodgkin's lymphomas and adult T-cell leukemia/lymphoma"Blood 86, 1924-1 930.

Munn, K., Walker, R., and Varley, J. (1995). "Frequent alterations of chromosome 1 in ductal carcinoma in situ of the breast."Oncogene 10, 1653-1 657.
Nelson, W.. Shore, E., Wang, A.. and Hammerton, R. (1990). "Identification of a membrane-cytoskeletal wmplex containing the cell adhesion molecule uvornorulin (E-cadherin). ankyrin and fodrin in Madin-Darby canine kidney epithelial cellsn J Ce11 Bi01 11 0, 349-357.
Nose, A., Tsuji, K., and Takeichi, M. (1990). "Localkation of specificity deterrnining sites in cadherin cell adhesion molecules."Cell61, 147-1 55.
O'Connell, P., Pekkel, V., Fuqua, S., Osborne, C., and Allred, 0. "Genetic evidence that hyperplasias and in situ carcinomas are precurson of invasive breast cancer. Tubmitted .
OIConnell, P., Pekkel, V., Fuqua, S., Osborne, C. K., and Allred, D. C. (1994). "Molecular genetic studies of early breast cancer evolution"8reast Cancer Research and Treatment 32,5-12.
Oka, H., Shiozaki, H., Kobayashi, K., Inoue, M., Tahara, H.. Kobayashi, T., Takatsuka, Y., Matsuyoshi, N., Hirano, S., Takeichi, M., and Mori. T. (1993). "Expression of E-Cadherin Cell Adhesion Molecules in Human Breast Cancer Tissues and Its Relationship to Metastasis"Cancer Research 53, 1696-1 701.
Pagano, M. (1997). "Cell cycle regulation by the ubiquitin pathway."FASEB J 11, 1067-1 075.
Page, O., and Anderson, T. (1987). "Diagnostic Histopathology of the Breast. Churchill Livingstone: New York.".
Page, D., and Dupont, W. (1990a). "Premalignant conditions and marken of elevatied risk in the breast and their management."Surg Clin North Am 70, 831-851.

Page, D., Dupont, W., Rogers. L., and Rados, M. (1985). "Atypical hyperplastic lesions of the female breast. A long term follow up study."Cancer 55, 2698-2708.
Page, D., Vander Zwagg, R., Rogers, L., Williams, L., Walker, W., and Hartmann, W. (1978). "Relation between wmponent parts of fibrocystic disease complex and breast cancer." JNCI 61,1055-1 063.
Page, D. L., and Dupont, W. D. (1990b). "Anatomical markers of human premalignancy and risk of breast cancer."Cancer 66,1326-1 335.
Pallis, L., Wilking, N., and Cedermark, B. (1992). "Receptors for estrogen and progesterone in breast carcinoma in-situ."Anticancer Res 12, 21 13-21 15.
Patchefsky, A., Schwartz, G., Finkelstein, S., Prestipino, A., Sohn, S., and Singer, J. (1 989). "Heterogeneity of intraductal carcinoma of the breastNCancer 63, 731 -741.
Patterson, D., Reid, C., and Anderson, T. (1990). "Assessment of oestrogen receptor content of breast carcinoma by irnmunohistochemical techniques on fixed and frozen tissue and by biochemical ligand binding assay."J Clin Pathol43,46-51.
Pertschu k, L., Eisenberg , K., and Carter, A. (1 985). "lmmunohistologic localization of estrogen recepton in breast cacner with monoclonal antibodiesXancer 55, 151 3-1 51 8.
Petit, A., Rak, J., Hung, M., Rockwell, P., Goldstein, N., Fendly, B., and Kerbel, R. (1997). "Neutralizing antibodies against epidermal growth factor and ErbB-2lneu receptor tyrosine kinases down-regulate vascular endothelial growth factor production by tumor cells in vitro and in vivo: angiogenic implications for signal transduction therapy of solid tumors."Am J Pathol 151, 1523-1 530.
Pike, M., Spicer, D., Cahmoush, L., and Press, M. (1993). "Estrogens, progestogens, normal breast cell proliferation, and breast cancer risk"Epidemiol Rev 15, 1 7-35.

Pinkel, D., Segraves, R., Sudar, O., Clark, S., Poole, I., Kowbel, D., Collins, C., Kuo, W., Chen, C., Zhai, Y., Dairkee, S., Ljung. B., Gray, J., and Albertson, D. (1998). "High resolution analysis of DNG wpy number variation using comparative genomic hybridization to microarrays."Nat Genet 20, 207-21 1.
Pluda, J. (1 997). "Tumor-associated angiogenesis: mechanisms, clinical implications. and therapeutic strategies."Semin Oncol 24, 203-21 8.
Poller, O., Silverstein, M., and Galea, M. (1994). "Ductal carcinoma in situ of the breast: a proposal for a new simplified histological classification association between cellular proliferation and c-erb-6-2 protein expression."Modem Pathol7,257-262.
Polyak, K., Kato, J., Solomon, M., Sherr, C., Massague, J., Roberts, J., and Koff, A. (1 994). "p27Kip1, a cyclin-Cdk inhibitor, links transforming growth factor-beta and contact inhibition to cell cycle arrest."Genes Dev 8,9022.
Ponten, J., and Guo, Z. (1998). "Precancer of the human cervix."Cancer Surv 32,201 -229.
Porter, P., Malone, K., Heagerty, P., Alexander, G., Gatti, L., Firpo, E., Daling, J., and Roberts, J. (1997). "Expression of cell-cycle regulaton p27kipl and cyclin El alone and in wmbination, correlate with survival in Young breast cancer patients."Nature Medicine 3,222-225.
Press, M. (1994). "Sensitivity of Her-2heu antibodies in archival tissue samples: Potential sources of error in immunohistochemical studies of oncogene expression. "Cancer Research 54,2771 -2777.
Price, J. (1 997). "Biochemistry of cancer dissemination. Crit. Rev."Biochem Mol Bi01 32, 175.
Radeva, G., Petrocelli, T., Behrend, E., Leung-Hagesteijn, C., Filmus, J., Slingerland. J., and Dedhar, S. (1997). "Overexpression of the integrin- linked kinase promotes anchorage-independent cell cycle progression."J Bi01 Chem 272, 1 3937-1 3944.

Radford, D., Fair, K., and Philips. N. (1995a). "Allelotyping of ductal carcinoma in situ of the breast: deleteion of loci on 8p.1 3q,16q11 7p, and l?q."Cancer Res 55,3399-3405.
Radford, D., Fair, K., Thompson, A., Ritter, J.. Holt, M., Steinbrucck, T., Wallace, M., Wells, S., and Donis-Keller, H. (1993). "Allelic loss on chromosome 17 in ductal carcinoma in situ of the breastTancer Res. 53, 2947-2950.
Radford, D., Philips. N., and Fair, K. (1995b). "Allelic loss and the progression of breast cancer."Cancer Res 55,5180-5183.
Rasbridge, S., Gillett, C., Sampson, S., Walsh, F., and Millis, R. (1993). "Epithelial (E-) and Placental (P-) cadherin cell adhesion rnolecule expression in breast acarcin~rna.'~Joumal of Pathology 169, 245-250.
Revillion, F., Bonneterre, J., and Peyrat, J. (1 998). "ER662 oncagene in human breast cancer and its clinical significance."Eur J Cancer 34, 791 -808.
Rochaix, P., Krajewski, S., Reed, J., Bonnet, F., Voigt, J., and Brousset, P. (1 999). "ln vivo patterns of Bcl-2 family protein expression in breast carcinomas in relation to apoptosis."J Pathol187,410415.
Ross, J., and Fletct~er, J. (1998). "The HER-2lneu oncagene in breast cancer: prognostic factor, predictive factor, and target for therapy."Stern Celk 16, 41 3-428.
Roylance, R., Gorman, P., Harris, W., Liebmann, R., Barnes, O., Hanby, A., and Sheer, D. (1 999). "Comparative genornic hybridization of breast tumors stratified by histological grade reveals new insights into the biological progression of breast cancer."Cancer Res 59, 1433-1 436.
Sainsbury, J., Farndon, J., Needham, G., Malcolm, A., and Harris, H. (1987). "Epidermal growth factor receptor status as predictor of early recurrence of and death from breast cancer"Lancet 1, 1398-1402.

Saiz, E., Toonkel, R., Poppiti, R. J., and Robinson, M. (1999). "Infiltrathg breast carcinoma smaller than 0.5 centimeters: is lymph node dissection necessary?"Cancer 85,2206-221 1.
Sawan, A., Randall, B., Angus, B., Wright, C., Henry. J., Ostrowski, J., Hennessey, C., Lennard, T., Corbett, I., and Home, C. (1992). "Retinoblastoma and p53 gene expression related to relapse and survivat in human breast cancer: an immunohistochemical study." J. Pathol. 168, 23-28.
Schimmelpenning, H., Eriksson, E., and Pallis, L. (1992). "lmmunohistochemicaI c-erb-B-2 proto-oncogene expression and nuclear DNA content in human mammary carcinoma in situnAm J Clin Pathol97, S48452.
Schmitt, F., Leal, C., and Lopes, C. (1995). "p53 protein expression and nuclear DNA content in breast intraductal proliferations."J Pathol176, 233-241.
Schweitzer, S., Hogge, J.. Grimes, M., Bear, H., and de Paredes, E. (1 999). "Cowden disease: a cutaneous marker for increased risk of breast cancer."AJR Am J Roentgen01 l72,M9-351.
Sherr, C. (1 996). "Cancer cell cycle"Science 274, 1672.
Shimamura, A., and Fisher, D. (1996). "Minireview. p53 in life and death."Clin Cancer Res 2,435440-
Shimoyama, Y., and Hirohashi, S. (1991). "Expression of E- and P-cadherin in gastric carcinomas."Cancer Res 51,2185-21 92.
Shiu, R., Watson, P.. and Dubik, D. (1993). "c-myc oncogene expression in estrogen-dependent and -independent breast cancer."Clin Chem 39, 353- 355.
Sierra, A., Castellsague, X., Escobedo, A., Moreno. A., Drudis, T., and Fabra, A. (1 999). "Synergistic cooperation between c-Myc and Bcl-2 in lymph node progression of T l human breast carcinomas."Breast Cancer Res Treat 54, 39-45.

Siitonen, S., Kononen, J., Helin, H., Rantala, I., Holli, K., and Isola, J. (1996). "Red uced E-cad herin expression is associated with invasiveness and unfavorable prognosis in breast cancer."Am J Clin Patholl05, 394-402.
Silva, J., Gonzalez, R., Dominguez, G., Garcia, J., Espana, P., and Bonilla, F. (1 999). "TP53 gene mutations in plasma DNA of cancer patients."ûenes Chromosomes Cancer 24, 160-1 61.
Silverstein, M. (1997). "Ductal Carcinoma In Situ of the Breast: Epidemiology and Natural History of Ductal Carcinoma in Situ; Williams 8 Wilkins. Baltimore, Marylanci."Chapter 4, 32-33.
Silverstein, M., and Poller, 0. (1 995). "Prognostic classification of breast ductal carcinoma-in-situWLancet 345, 1 1 54-1 1 57.
Silvestrini, R., Daidone, M. G., Benini, E., Faranda, A., Tomasic, G., Boracchi, P., Salvadori, 6-1 and Veronesi, U. (1996). "Validation of p53 accumulation as a predictor of distant metastasis at 10 years of follow-up in 1400 Node- negative Breast Cancers"Clinica1 Cancer Research 2, 2007-201 3.
Sjogren, S., Ignanas, M., Holmberg, L., Norberg, T., Nordgren, H., and Lindgren, A. (1996). "The p53 gene in breast cancer: prognostic versus immunohistochemistry ."J Nat1 Cancer lnst 88, 1 500.
Slade, M., Coope, R., Gomm, J., and Coombes, R. (1999). "The human marnmary gland basement membrane is integral to the polarity of luminal epithelial cells."Exp Ce11 Res 247,267-278.
Slingerland, J., Hengst, L., Pan, C., Alexander, D., Stampfer, M., and Reed, S. (1 994). "A novel inhibitor of cyclin-Cdk activity detected in Transforming Growth Factor B-arrested epithelial cellsnMal.Cell Biol. 14, 3683-3694.
Smith, H., Lu, Y., Deng, G., Martinez, O., Krams, S., Ljung, B.-M., Thor, A., and Lagios, M. (1993). "Molecular aspects of early stages of breast cancer progression" J. Ce// Biochem 1 70 , 144-1 52.

Soussi, T. (1 997). '7he p53 tumour suppressor gene: from molecular biology to clinical investigation. In: Klijn JG. editor. Prognostic and predictive value of p53. Amsterdam (The Netherlands): Elsevier", 3-22.
Sratton, M., Collins, N., Lakhani. S., and Sloane, J. (1995). "Loss of heterozygosity in ductal carcinoma in situ of the breast."J Pathol175, 195- 201.
St. Croix, B.. Florenes, V., Rak. J., Flanagan, M., Bhattacharya, Nel Slingerland, J., and Kerôel. R. (1996). "Impact of the cyclindependent kinase inhibitor p27kip1 on resistance of tumour cells to anti-cancer agentsWNature Med 2, 1204-1 21 O.
Steeg . P., and Abram, J. (1 997). "Cancer prognostics:past, present and p27"Nature Medicine 3, 1 52-1 54.
Takeichi, M. (1 991 ). "Cadherin cell adhesion recepton as a morphogeneic regulator."Science 251, 1451 -1 455.
Tamura, G., Maesawa. C., Suzuki, Y., Kashiwaba, M., Ishida, M., Saito, K., and Satodate. R. (1 994). "1 mproved detection of loss of heterozygosity at retinoblastoma gene locus in human breast carcinoma."Pathol /nt 44, 34- 38.
Tan, P.. Cady. B., Wanner, M., Worland. P., Cukor, B.. Magi-Galluui. C., Lavi, P., Draetta. G.. Pagano, M.. and Loda. M. (1 997). "The cell cycle inhibitor p27 is an independent prognostic marker in small invasive breast carcinomaWCancer Research 57, 1259-1 263.
Tanaka. C., Yoshimoto, K., Yang, P., Kimura, T., Yamada, S., Moritani, M., Saro. T.. and Itakura. M. (1997). "Infrequent mutations of p27kipl gene and trisomy 12 in a subset of hurnan pituitary adenomasWJ. Clin Endocrinol Metab 82, 3141 -3147.
Tannapfel, A., Kuhn, R., Kessler, H., and Wittekind, C. (1 996). "Expression of c- erbB2 oncogene product in different tumours and its standardised e~aluation.~~Analytica/ Cellular Pathology 10, 149-1 60.

Tanner, M., Tirkkonen, M., Kallioniemi, A., Holli, K., Collins, C., Kowbel, O., Gray, J., Kallioniemi, O., and Isola, J. (1995). "Amplification of chromosomal region 20qI 3 in invasive breast cancer: prognostic irnplications."Clin Cancer Res 1,1455- 1 46 1 .
Tetu, B., Brisson, J., Lapointe, H., Wang, C., Bernard, P., and Blanchette, C. (1999). "Cathepsin D expression by cancer and stroma1 cells in breast cancer: an immunohistochemical study of 1348 cases."Breast Cancer Res Treat 55, 137-1 47.
Thompson, W. (1994). "Genetic epidemiology of breast cancerTancer 74, 279- 288.
Tirkkonen, M., Tanner, M., Karhu, R., Kallioniemi, A., Isola, J., and Kallioniemi, 0. (1998). "Molecular cytogenetics of primary breast cancer by CGH."199821, 177-184.
Toyoshima, H., and Hunter, T. (1994). "p27, a novel inhibitor of G1 cyclin-Cdk protein kinase activity, is related to p21 ."Ce// 78, 67-74.
Trudel, M., Mulligan, L., Cavernee, W., Margolese, R., Cote, J., and Gariepy, G. (1 992). "Retinoblastoma and p53 gene product expression in breast carcinoma"Hurn. Pathol. 23, 1388-1 394.
Tsuda, H., Iwaya, K., Fukutomi, T., and Hiroshashi, S. (1993). "p53 mutations and c-erbB-2 amplification in intraductal and invasive breast carcinomas of hig h histologic grade." Jpn. J Cancer Res 84, 394-40 1.
Umbas, R., Isaacs, W., and Bringuier, P. (1994). "Decreased E-cadherin expression is associated with poor prognosis in patients with prostate cancer" Cancer Res 54,3929-2933.
Urdiales-Viedma, M., Nogales-Fernandez, F., Martos-Padilla, S., and Sanchez- Cantalejo, €. (1986). "Correlation of histologic grade and lymph node status with some histopathologic discriminants in breast cancer."Tumon 72,43-51.

Verhasselt, 8., Van Damme, J., van Larebeke, N., Put, W., Bracke, M., De Potter, C., and Mareel, M. (1992). "lnterieukin-1 is a motility factor for human breast carcinoma cells in vitro: additive effect with interleukin- 6."Eur J Ce11 Biol59,449-457.
Vogelstein, B., and Kinzler, K. (1992). "p53 Function and dysfunction."Cell 70, 523.
Walker, R., Dearing, S., Lane, 0.. and Varley, J. (1991). "Expression of p53 protein in infiltrating and in situ breast carcinornas."J Patholl65, 203-2 1 1 .
Weidner, N., Semple, J., and Welch, W. (1 991 ). "Tumor angiogenesis and metastasis-Correlation in invasive breast cancer."N Engl J Med 324, 1-8.
Weinberg. R. (1 996). "How cancer arisesnSci Am 275,62.
Wollenweider-Zerargui, L., Barrelet, L., and Wong, Y. (1988). "The predictive value of estrogen and progesterone receptor concentrations on the clincal behaviour of breast cancer in women."Cancer 57,1171 -1 180.
Wyllie, A. (1 997). "Apoptosis and carcinogenesis."Eur J Ce11 Bi01 73, 189.
Yamashita, H., Kobayashi, S., Iwase, E., Itoh, Y., Kuzushima, T., Iwata, H., Itoh, K., Haito, A., Yarnashita, T., Masaoka, A., and Andkumra, N. (1993). "Analysis of oncogenes and tumour suppressor genes in hurnan breast cancer" Jpn. J. Cancer Res. 84,87 1-878.
Zabludoff, S., Csete, M., Wagner, R., Yu, X., and Wold, B. (1998). "p27kip1 is expressed transiently in developing myotomes and enhances myogenesis"Ce1l Growth Differ 9, 1-1 1.
Zafrani, B., Leroyer, A., and Fourquet, A. (1 994). "Mammographically detected ductal in situ carcinoma of the breast analysed with a new classification. A study of 127 cases: correlation with estrogen and progesterone receptors,

p53 and cerbB-2 proteins. and proliferative adivity."Semin Diagn Pathol 11,208-214.
Zheng, W., Looi, L., and Cheah, P. (1999). "A cornparison of the pattern of cathepsin-D expression in fibroadenoma. fibrocystic disease, preinvasive and invasive ductal breast carcinoma."Pathology 31, 247-25 1 .
Zhuang, Z., Merino, M. J., Chuaqui. R., Liotta. L.. and Emmert-Buck, M. R. (1 995). "Identical allelic loss on chromosome 1 1 q 1 3 in microdissected in situ and invasive human breast cancer."Cancer Res. 55, 467-471.
Ziober, B. (1996). "Laminin-binding integrins in tumor progression and metastasis."Smin Cancer Biol7, 1 19.