! " # $ " %' ! ( $ ) * "!"#$%&'(#)%"Te molecular basis of
lung cancer is complex and heterogenous.
Improvementsinourunderstandingofmolecularalterationsat multiple
levels (genetic, epigenetic, protein expression) and their
functionalsignifcancehavethepotentialtoimpactlungcancer
diagnosis,prognosticationandtreatment.Lungcancersdevelop
throughamultistepprocessinvolvingdevelopmentofmultiple
geneticandepigeneticalterations,particularlyactivation
ofgrowthpromotingpathwaysandinhibitionoftumour
suppressorpathways.Greaterunderstandingofthemultiple biochemical
pathways involved in the molecular pathogenesis of lung cancer is
crucial to the development of treatment strategies
thatcantargetmolecularaberrationsandtheirdownstream
activatedpathways(1).Specificmolecularalterationsthat
drivetumourgrowthandprovidetargetsfortherapyhave
beenbestdefinedinadenocarcinomas(ADC)butthereis
increasinginterestinthemolecularlandscapeofsquamous
cellcarcinoma(SCC)highlightingnewpotentialtherapeutic
targets.Inlungcancerasinothermalignancies,tumourigenesis
relatestoactivationofgrowthpromotingproteins[e!g.,v-Ki-ras2Kirstenratsarcomaviraloncogenehomolog(KRAS),
epidermalgrowthfactorreceptor(EGFR),BRAF,MEK-1,
HER2,MET,ALKandrearrangedduringtransfection(RET)]
aswellasinactivationoftumoursuppressorgenes[e!g!"P53, *%+,('+-$
/)%+%01 %2 +'"0 (-"(,$Wendy A. Cooper1,2, Davld C. L. Lam3, Sandra
A. O'Too|e1,4,5, [obn D.
Mlnna61TlssuePatbo|ogyandDlagnostlcOnco|ogy,Poya|PrlnceA|lredHosplta|,Camperdown,Sydney,NSW,Austra|la,
2Scboo|olMedlclne, Unlverslty ol Western Sydney, NSW, Austra|la,
3Department ol Medlclne, Unlverslty ol Hong Kong, Hong Kong SAP,
Cblna, 4Klngborn Cancer Centre and Garvan |nstltute ol Medlca|
Pesearcb, Dar|lngburst, Sydney, NSW, Austra|la, 5Sydney Medlca|
Scboo|, Unlverslty ol Sydney, NSW, Austra|la, 6Hamon Center lor
Tberapeutlc Onco|ogy Pesearcb, Unlverslty ol Texas Soutbwestern
Medlca| Center at Da||as, Texas,
USA34567386Lungcancersarecharacterisedbyabundantgeneticdiversitywithrelativelyfewrecurrentmutationsoccurringathigh
frequency.However,thegeneticalterationsoftenaffectacommongroupofoncogenicsignallingpathways.Therehave
beenvastimprovementsinourunderstandingofthemolecularbiologythatunderpinslungcancerinrecentyearsand
thishasledtoarevolutioninthediagnosisandtreatmentoflungadenocarcinomas(ADC)basedonthegenotypeof
anindividualstumour.Newtechnologiesareidentifyingkeyandpotentiallytargetablegeneticaberrationsnotonlyin
adenocarcinomabutalsoinsquamouscellcarcinoma(SCC)ofthelung.Lungcancermutationshavebeenidentifedin
v-Ki-ras2Kirstenratsarcomaviraloncogenehomolog(KRS),epidermalgrowthfactorreceptor(EGFR),BRFandthe
parallelphosphatidylinositol3-kinase(PI3K)pathwayoncogenesandmorerecentlyinMEKandHER2whilestructural
rearrangementsinALK,ROS1andpossiblyrearrangedduringtransfection(RET)providenewtherapeutictargets.
AmplifcationisanothermechanismofactivationofoncogenessuchasMETinadenocarcinoma,fbroblastgrowthfactor
receptor1(FGFR1)anddiscoidindomainreceptor2(DDR2)inSCC.Intriguingly,manyofthesegeneticalternations
areassociatedwithsmokingstatusandwithparticularracialandgenderdiferences,whichmayprovideinsightintothe
mechanismsofcarcinogenesisandroleofhostfactorsinlungcancerdevelopmentandprogression.Teroleoftumour
suppressorgenesisincreasinglyrecognisedwithaberrationsreportedinTP53,PTEN,RB1,LKB11andp16/CDKN2A.
Identificationofbiologicallysignificantgeneticalterationsinlungcancerthatleadtoactivationofoncogenesand
inactivation of tumour suppressor genes has the potential to
provide further therapeutic opportunities. It is hoped that these
discoveries may make a major contribution to improving outcome for
patients with this poor prognosis disease. 9:; 5Lung cancer;
mutation; molecular pathology; oncogene; tumour suppressor gene!
#$%&'( )*+ ,-./012314536789368-: ;%*5
.-:/87:*++?:,-7,9.6/8:,-./:-HR8>9QR74
J-#OS-1Thep16INK4A/RBpathwayregulatescellcycleprogression
fromG1toSphase.RB1isatumoursuppressorgenethat
encodesRBproteinwhichregulatescellcycleG1/Stransition
bybindingthetranscriptionfactorE2F1.RB1wasthefirst
TSGdescribedinlungcancer(121)andisinactivatedin
about90%ofsmallcelllungcarcinomasbutonlyabout
10-15%ofNSCLC(1).InNSCLC,thepathwayismostly
switchedoffthroughalterationsofcyclinD1,CDK4andthe
cyclindependentkinaseinhibitorp16(CDKN2A)(105).
p16INK4AinhibitscyclinD1dependentphosphorylationofRB
protein,therebypreventingcellcycletransitionthroughthe
G1/Scheckpoint(122).p16INK4Aisinactivatedinabout80%
ofNSCLC(123,124)andwasalteredin72%oflungSCCs
examinedbyTCGA,mostlythroughhomozygousdeletion,
methylationorinactivatingmutations(12).Inaddition,there
isoverexpressionofcyclinD1throughgeneamplificationor other
mechanisms in about 40% of NSCLC (123).*%+,('+-$ #-$0,#)"0 )"
L58G8Thepresenceofthesemoleculartargetsasdescribedabovenow defnes
the characteristics of NSCLC, with EGFR mutation and ALK
rearrangements being the most clinically relevant at present (125).
Teprevalenceofthesemutationsvariesinlungcancerarising
frompatientindifferentregions(126).ActivatingEGFR
mutationswerefoundinupto20%ofCaucasianswhileinthe
AsianpopulationstheseEGFRmutationscanbepresentinup
to40%ofpatientswithNSCLC(127).Teseethnicdiference
inNSCLCpropertiesappearstobenotlimitedtothepresence
ofactivatingEGFRmutationsbutisalsoevidentinotherdriver
oncogenicmutationprofles(includingALK,KRS,METetc.),
histologyandhencetumourresponsetotargetedtherapy
treatment(63,126,128).Tepresenceofthesedrivermutations is generally
found to be mutually exclusive to others in the same tumour (126).
In lung ADC among Asians, ALK rearrangement
isseeninupto7%ofpatientswithlungADC(79).Lung
tumoursbearingEML4-ALKrearrangementarenon-responsive
toconventionalchemotherapyorEGFR-tyrosinekinase inhibitors but are
sensitive to a specifc tyrosine kinase inhibitor
namedcrizotinib(129).Basedonourcurrentunderstandingof
therapeuticmoleculartargetsofEGFRmutationandALKgene
rearrangementinNSCLCandtheavailabilityofcorresponding
targetedagents,analgorithmoftestingformoleculartargetsin
NSCLCisproposedasinFigure1,whichrepresentsastepwise
approachtotestingforindividualtargets,beginningwithEGFR
then,ifnegative,ALKfusiongeneorotherpotentialtargetsif
appropriate.AmongNSCLC,adenocarcinomaaccountsforupto80%
ofhistologicalsubtypes(130).Therearepreviousreportsof correlations
between histological subtypes of ADC demonstrating
micropapillaryfeatureswithpresenceofactivatingEGFR
mutations,leadingtothesuggestionsthatthepresenceof
specificmutationsinNSCLCactuallyrepresentheterogeneity
incancerbiologyandalsoresponsetotherapy(131).Giventhe
heterogeneityoflungcancerhistology,however,histological
subtypesaredifficulttobeusedasthesolereliablemarkerfor
guidancetomolecularphenotypingandselectionoftargeted therapy
(132,133).TargetingtherapeuticoncogenicmutationslikeEGFRand
ALKcangivedramaticinitialtreatmentresponseoratleastan initial
stable clinical disease. Te response rate is up to 70% in lung
ADCbearingfavourableactivatingEGFRmutations(134).The median
progression free survival is usually quoted as 9-11 months
withdifferenttyrosinekinaseinhibitors(135,136),after
whichmostpatientswithEGFRmutationswillexperience
diseaseprogressionanddrugresistance.Aproportionofsuch
drugresistanceisattributedtothedevelopmentofasecond mutation,
usually T790M at exon 20 (137). It is hard to explain
theeventuallossofdrugsensitivityintumoursbearingthose !""#$% $' ()*
+")$,-)(% ,.(/0$1 2/ )-/0 ,(/,$% S486favourable EGFR mutations
(exon 19 deletions and L858R) even
withouttheacquisitionofsecondarymutationslikeT790M
orthepresenceofotheruncommonorlessfavourableEGFR
mutations.Thiscouldreflectsuboptimaltherapeutictargeting
andbetterunderstandingonthebiologyofEGFR-related
tumoursignallingandotheroncogenicmutationswillimprove
drugtargetingandgivepatientsbeterpredictionoftherapeutic response
and
prognostication.8%"(+'I)%"ITheidentificationofdrivermutationsinEGFRandALK
heraldedaneweraoftargetedtherapyinlungadenocarcinoma
andadvancedsequencingtechnologiesareprovidingeven
moresophisticatedinsightsintothemolecularaberrations
inoncogenesandtumoursuppressorgenesunderlyinglung
cancer(12,138-142).Thesestudieshaveidentifiedarangeof
potentiallytargetablegeneticaberrationsinlungcancerbut
havealsohighlightedatroublingcomplexityandheterogeneity
whichposessignificantchallengesformoleculardiagnosisand
targetedtreatment.Greaterknowledgeofthemolecularbiology
andgenomiclandscapeoflungcancerofferspromiseforthe
future.Improvementsinoutcomefromlungcancerwillalmost
certainlyrequiretheidentificationofincreasingnumbersof
everrarerdrivermutations,anddiagnosticapproachesthatcan identify
multiple therapeutic targets ofer signifcant advantages.
However,theidentificationofdrivergenomicaberrationsalso
requirestheparalleldevelopmentofefectivetargetedtherapies
andformanyofthesechanges(suchasKRAS)suchtherapies
arenotyetavailable.Resistancetotargetedtherapeuticsisan
increasinglyrecognisedissueintowhichgenomicanalyses
mayprovideimportantmechanisticinsightsunderlyingfuture rational
therapeutic
approaches.3(T"%S+,&0,F,"#IFundingsources:SydneyFoundationforMedicalResearch;
Hong Kong SK Yee Medical Foundation; Cancer Institute NSW
ClinicalResearchFellowship10/1/07;SydneyBreastCancer
Foundation;LifehouseatRoyalPrinceAlfredHospitalGrant; Lung Cancer
SPORE P50CA70907.
Disclosure:WChasreceivedhonorariafromPzerOncology.
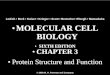
Figure1.Asuggestedalgorithmformoleculartargettestingbasedonunderstandingofrelevantmolecularbiologyinnon-smallcelllungcancer
(NSCLC).Test for alterations in other molecular targets or pathways
e.g. ALK, ROS1, RE1, cME1TtaTKI resistant mutatione.g. T790MECFR
wildtypeTest for ECFR mutationsNSCLC, in particular
adenocarcinomaBiomarker-based personalized therapy for lung
cancerECFR mutantTKI responsive mutatione.g. exon 19 deletion,
L858R, L861QEGFR TKI New generation EGFR- TKI Targeted therapy e.g.
crizotinibe.g. AfatinibFurther research into presence of other
biomarkers:1. To understand the molecular biology of lung cancer2.
Feedback for clinical management +/- prognostication!"#$%&' ")
*+"$&,-, .-/0&/01 2"' 31 4#55' 3 6,7"80$ 9:;<
S487SOTisamemberoftheRocheAustraliaMolecularPathology
AdvisoryBoard.Theauthorsdeclarenootherconflictsof
interest7,2,$,"(,I1.LarsenJE, MinnaJD.
Molecularbiologyoflungcancer:clinical implications. Clin Chest Med
2011;32:703-40.2.Lynch TJ, Bell DW, Sordella R, et al. Activating
mutations in the epidermal
growthfactorreceptorunderlyingresponsivenessofnonsmall-celllung
cancer to geftinib. N Engl J Med
2004;350:2129-39.3.WeinsteinIB.Cancer.Addictiontooncogenes-theAchilleshealofcancer.
Science 2002;297:63-4.4.Sequist LV, Heist RS, Shaw AT, et al.
Implementing multiplexed genotyping
ofnon-small-celllungcancersintoroutineclinicalpractice.AnnOncol
2011;22:2616-24.5.YipPY,YuB,CooperWA,etal.PatternsofDNAmutationsandALK
rearrangementinresectednodenegativelungadenocarcinoma.JTorac Oncol
2013;8:408-14.6.LiuP,MorrisonC,WangL,etal.Identificationofsomaticmutations
innon-smallcelllungcarcinomasusingwholeexomesequencing.
Carcinogenesis 2012;33:1270-6.7.Ding L, Getz G, Wheeler DA, et al.
Somatic mutations afect key pathways in lung adenocarcinoma. Nature
2008;455:1069-75.8.Govindan R, Ding L, Grifth M, et al. Genomic
landscape of non-small cell lung cancer in smokers and
never-smokers. Cell 2012;150:1121-34.9.Ju YS, Lee WC, Shin JY, et
al. A transforming KIF5B and RET gene fusion
inlungadenocarcinomarevealedfromwhole-genomeandtranscriptome
sequencing. Genome Res
2012;22:436-45.10.KohnoT,IchikawaH,TotokiY,etal.KIF5B-RETfusionsinlung
adenocarcinoma. Nat Med
2012;18:375-7.11.LipsonD,CapelletiM,YelenskyR,etal.IdentifcationofnewALKand
RETgenefusionsfromcolorectalandlungcancerbiopsies.NatMed
2012;18:382-4.12.CancerGenomeAtlasResearchNetwork.Comprehensivegenomic
characterization of squamous cell lung cancers. Nature
2012;489:519-25.13.Hammerman PS, Sos ML, Ramos AH, et al. Mutations
in the DDR2 kinase
geneidentifyanoveltherapeutictargetinsquamouscelllungcancer. Cancer
Discov 2011;1:78-89.14.Downward J. Targeting RS signalling pathways
in cancer therapy. Nat Rev Cancer
2003;3:11-22.15.KarnoubAE,WeinbergRA.Rasoncogenes:splitpersonalities.NatRev
Mol Cell Biol
2008;9:517-31.16.RielyGJ,KrisMG,RosenbaumD,etal.Frequencyanddistinctive
spectrum of KRS mutations in never smokers with lung
adenocarcinoma. Clin Cancer Res
2008;14:5731-4.17.RodenhuisS,SlebosRJ.Clinicalsignifcanceofrasoncogeneactivationin
human lung cancer. Cancer Res
1992;52:2665s-9s.18.SchmidK,OehlN,WrbaF,etal.EGFR/KRAS/BRAFmutations
inprimarylungADCandcorrespondinglocoregionallymphnode metastases.
Clin Cancer Res
2009;15:4554-60.19.KosakaT,YatabeY,EndohH,etal.Mutationsoftheepidermalgrowth
factorreceptorgeneinlungcancer:biologicalandclinicalimplications.
Cancer Res
2004;64:8919-23.20.MaoC,QiuLX,LiaoRY,etal.KRSmutationsandresistancetoEGFR-TKIs
treatment in patients with non-small cell lung cancer: a
meta-analysis of 22 studies. Lung cancer
2010;69:272-8.21.ShigematsuH,LinL,TakahashiT,etal.Clinicalandbiologicalfeatures
associatedwithepidermalgrowthfactorreceptorgenemutationsinlung
cancers. J Natl Cancer Inst
2005;97:339-46.22.TamIY,ChungLP,SuenWS,etal.Distinctepidermalgrowthfactor
receptorandKRASmutationpatternsinnonsmallcelllungcancer
patientswithdifferenttobaccoexposureandclinicopathologicfeatures.
Clin Cancer Res
2006;12:1647-53.23.SubramanianJ,GovindanR.Moleculargeneticsoflungcancerinpeople
who have never smoked. Lancet Oncol
2008;9:676-82.24.RekhtmanN,PaikPK,ArcilaME,etal.Clarifyingthespectrumofdriver
oncogenemutationsinbiomarker-verifiedsquamouscarcinomaoflung:
lackofEGFR/KRASandpresenceofPIK3CA/AKT1mutations.Clin Cancer Res
2012;18:1167-76.25.Linardou H, Dahabreh IJ, Kanaloupiti D, et al.
Assessment of somatic k-RS
mutationsasamechanismassociatedwithresistancetoEGFR-targeted
agents:asystematicreviewandmeta-analysisofstudiesinadvancednon-small-celllungcancerandmetastaticcolorectalcancerLancetOncol
2008;9:962-72.26.Ihle NT, Byers LA, Kim ES, et al. Efect of KRS
Oncogene Substitutions
onProteinBehavior:ImplicationsforSignalingandClinicalOutcome.J Natl
Cancer Inst
2012;104:228-39.27.PrenzelN,FischerOM,StreitS,etal.Theepidermalgrowthfactor
receptorfamilyasacentralelementforcellularsignaltransductionand
diversifcation. Endocr Relat Cancer 2001;8:11-31.28.Scaglioti GV,
Selvaggi G, Novello S, et al. Te Biology of epidermal growth factor
receptor in lung cancer. Clin Cancer Res
2004;10:4227s-32s.29.YardenY,SliwkowskiMX.UntanglingtheErbBsignallingnetwork.Nat
Rev Mol Cell Biol
2001;2:127-37.30.SordellaR,BellDW,HaberDA,etal.Gefitinib-sensitizingEGFR
mutationsinlungcanceractivateanti-apoptoticpathways.Science
2004;305:1163-7.31.GreulichH,ChenTH,FengW,etal.Oncogenictransformationby
inhibitor-sensitive and -resistant EGFR mutants. PLoS Med
2005;2:e313.32.JiH,LiD,ChenL,etal.TheimpactofhumanEGFRkinasedomain
mutationsonlungtumorigenesisandinvivosensitivitytoEGFR-targeted
therapies. Cancer Cell 2006;9:485-95.33.Dahabreh IJ, Linardou H,
Siannis F, et al. Somatic EGFR mutation and gene copy gain as
predictive biomarkers for response to tyrosine kinase inhibitors in
nonsmall cell lung cancer. Clin Cancer Res 2010;16:291-303.34.Okabe
T, Okamoto I, Tamura K, et al. Diferential constitutive activation
of the epidermal growth factor receptor in nonsmall cell lung
cancer cells bearing EGFR gene mutation and amplifcation. Cancer
Res
2007;67:2046-53.35.EberhardDA,GiacconeG,JohnsonBE.Biomarkersofresponseto
epidermalgrowthfactorreceptorinhibitorsinnonsmall-celllungcancer
workinggroup:standardizationforuseintheclinicaltrialsetting.JClin
Oncol 2008;26:983-94.36.Russell PA, Barnet SA, Walkiewicz M, et al.
Correlation of mutation status
andsurvivalwithpredominanthistologicsubtypeaccordingtothenew
IASLC/ATS/ERSlungadenocarcinomaclassificationinstageIII(N2) !""#$%
$' ()* +")$,-)(% ,.(/0$1 2/ )-/0 ,(/,$% S488patients. J Torac Oncol
2013;8:461-8.37.Tokumo M, Toyooka S, Kiura K, et al. Te
relationship between epidermal
growthfactorreceptormutationsandclinicopathologicfeaturesinnonsmall
cell lung cancers. Clin Cancer Res 2005;11:1167-73.38.Yoshida K,
Yatabe Y, Park JY, et al. Prospective validation for prediction of
geftinibsensitivitybyepidermalgrowthfactorreceptorgenemutationin
patients with non-small cell lung cancer. J Torac Oncol
2007;2:22-8.39.Yamamoto H, Toyooka S, Mitsudomi T. Impact of EGFR
mutation analysis in non-small cell lung cancer. Lung cancer
2009;63:315-21.40.MarchettiA,ArdizzoniA,PapottiM,etal.Recommendationsforthe
analysisofALKgenerearrangementsinnonsmall-celllungcancer:a
consensusoftheItalianAssociationofMedicalOncologyandtheItalian
Society of Pathology and Cytopathology. J Torac Oncol
2013;8:352-8.41.WuJY,WuSG,YangCH,etal.Lungcancerwithepidermalgrowthfactor
receptorexon20mutationsisassociatedwithpoorgefitinibtreatment
response. Clin Cancer Res
2008;14:4877-82.42.OhtsukaK,OhnishiH,FujiwaraM,etal.Abnormalitiesofepidermal
growth factor receptor in lung squamous-cell carcinomas,
adenosquamous
carcinomas,andlarge-cellcarcinomas:tyrosinekinasedomainmutations
arenotrareintumorswithanadenocarcinomacomponent.Cancer
2007;109:741-50.43.Heist RS, Sequist LV, Engelman JA. Genetic
changes in squamous cell lung cancer: a review. J Torac Oncol
2012;7:924-33.44.BalakMN,GongY,RielyGJ,etal.NovelD761Yandcommonsecondary
T790Mmutationsinepidermalgrowthfactorreceptormutantlung
adenocarcinomas with acquired resistance to kinase inhibitors. Clin
Cancer Res
2006;12:6494-501.45.EngelmanJA,ZejnullahuK,MitsudomiT,etal.METamplifcationleads
to geftinib resistance in lung cancer by activating ERBB3
signaling. Science 2007;316:1039-43.46.Davies H, Bignell GR, Cox C,
et al. Mutations of the BRF gene in human cancer. Nature
2002;417:949-54.47.Brose MS, Volpe P, Feldman M, et al. BRF and RS
mutations in human lung cancer and melanoma. Cancer Res
2002;62:6997-7000.48.Marcheti A, Chen TH, Richards WG, et al.
Clinical features and outcome
ofpatientswithnonsmall-celllungcancerharboringBRFmutations.J Clin
Oncol 2011;29:3574-9.49.Naoki K, Chen T, Richards W, et al.
Missense mutations of the BRF gene in human lung adenocarcinoma.
Cancer Res
2002;62:7001-3.50.PaikPK,ArcilaME,FaraM,etal.Clinicalcharacteristicsofpatients
withlungadenocarcinomasharboringBRAFmutations.JClinOncol
2011;29:2046-51.51.FalchookGS,LongGV,KurzrockR,etal.Dabrafenibinpatientswith
melanoma, untreated brain metastases, and other solid tumours: a
phase 1 dose-escalation trial. Lancet
2012;379:1893-901.52.MarksJL,GongY,ChitaleD,etal.NovelMEK1mutationidentifiedby
mutational analysis of epidermal growth factor receptor signalling
pathwar genes in lung adenocarcinoma. Cancer Res
2008;68:5524-8.53.SadiqAA,SalgiaR.METasapossibletargetfornonsmall-celllung
cancer. J Clin Oncol 2013;31:1089-96.54.Bean J, Brennan C, Shih JY,
et al. MET amplifcation occurs with or without
T790MmutationsinEGFRmutantlungtumorswithacquiredresistance to
geftinib or erlotinib. Proc Natl Acad Sci USA
2007;104:20932-7.55.CappuzzoF,MarchettiA,SkokanM,etal.METincreasedgenecopy
numbernegativelyaffectssurvivalofsurgicallyresectednonsmall-cell
lung cancer patients. J Clin Oncol
2009;27:1667-74.56.OnozatoR,KosakaT,KuwanoH,etal.ActivtionofMETbygene
amplifcation or by splice mutations deleting the juxtamembrane
domain in primary resected lung cancers. J Torac Oncol
2009;4:5-11.57.GoH,JeonYK,ParkHJ,etal.HighMETgenecopynumberleadsto
shorter survival in patients with non-small cell lung cancer. J
Torac Oncol 2010;5:305-13.58.Beau-Faller M, Ruppert AM, Voegeli AC,
et al. MET gene copy number in non-small cell lung cancer:
molecular analysis in a targeted tyrosine kinase inhibitor naive
cohort. J Torac Oncol 2008;3:331-9.59.Luterbach B, Zeng Q, Davis
LJ, et al. Lung cancer cell lines harboring MET
geneamplifcationaredependentonMetforgrowthandsurvival.Cancer Res
2007;67:2081-8.60.TzaharE,WatermanH,ChenX,etal.Ahierarchicalnetworkfo
interreceptorinteractionsdeterminessignaltransductionbyNeu
differentiationfactor/neuregulinandepidermalgrowthfactor.MolCell
Biol 1996;16:5276-87.61.Graus-PortaD, BeerliRR, DalyJM, etal .
ErbB-2, thepreferred
heterodimerizationpartnerofallErbBreceptors,isamediatoroflateral
signaling. EMBO J 1997;16:1647-55.62.Heinmller P, Gross C, Beyser
K, et al. HER2 status in non-small cell lung cancer: results from
patient screening for enrollment to a phase II study of herceptin.
Clin Cancer Res
2003;9:5238-43.63.ShigematsuH,TakahashiT,NomuraM,etal.Somaticmutationsofthe
HER2 kinase domain in lung adenocarcinomas. Cancer Res
2005;65:1642-6.64.StephensP,HunterC,BignellG,etal.Lungcancer:intragenicERBB2
kinase mutations in tumours. Nature
2004;431:525-6.65.TomizawaK,SudaK,OnozatoR,etal.Prognosticandpredictive
implicationsofHER2/ERBB2/neugenemutationsinlungcancers.Lung Cancer
2011;74:139-44.66.PereraSA, Li D, Shi mamuraT, etal . HER2YVMAdri
vesrapi d
developmentofadenosquamouslungtumorsinmicethataresensitive
toBIBW2992andrapamycincombinationtherapy.ProcNatlAcadSci
2009;106:474-9.67.EngelmanJA,LuoJ,CantleyLC.Theevolutionofphosphatidylinositol
3-kinasesasregulatorsofgrowthandmetabolism.NatRevGenet
2006;7:606-19.68.CullyM,YouH,LevineAJ,etal.BeyondPTENmutations:thePI3K
pathwayasanintegratorofmultipleinputsduringtumorigenesis.NatRev
Cancer
2006;6:184-92.69.BrognardJ,ClarkAS,NiY,etal.Akt/ProteinkinaseBisconstitutively
active in non-small cell lung cancer cells and promotes cellular
survival and resistance to chemotherapy and radiation. Cancer Res
2001;61:3986-97.70.Tsurutani J, West K, Sayyah J, et al. Inhibition
of the phosphatidylinositol
3-kinase/Akt/mammaliantargetofrapamycinpathwaybutnottheMEK/ERKpathwayatenuateslaminin-mediatedsmallcelllungcancercellular
survivalandresistancetoimatinibmesylateorchemotherapy.CancerRes
2005;65:8423-32.71.PapadimitrakopoulouV.DevelopmentofPI3K/AKT/MTORpathway
!"#$%&' ") *+"$&,-, .-/0&/01 2"' 31 4#55' 3 6,7"80$
9:;<
S489inhibitorsandtheirapplicationinpersonalizedtherapyfornon-small-cell
lung cancer. J Torac Oncol 2012;7:1315-26.72.Vivanco I, Sawyers CL.
Te phosphatidylinositol 3-Kinase-AKT pathway in human cancer. Nat
Rev Cancer
2002;2:489-501.73.YamamotoH,ShigematsuH,NomuraM,etal.PIK3CAmutationsand
copy number gains in human lung cancers. Cancer Res
2008;68:6913-21.74.EngelmanJA,ChenL,TanX,etal.EffectiveuseofPI3KandMEK
inhibitorstotreatmutantK-rasG12DandPIK3CAH1047Rmurinelung cancers.
Nat Med
2008;14:1351-6.75.KawanoO,SasakiH,EndoK,etal.PIK3CAmutationstatusinJapanese
lung cancer patients. Lung cancer
2006;54:209-15.76.JiM,GuanH,GaoC,etal.Highlyfrequentpromotermethylationand
PIK3CAamplificationinnon-smallcelllungcancer(NSCLC).BMC Cancer
2011;11:147.77.MalangaD,ScrimaM,DeMarcoC,etal.ActivatingE17Kmutationin
thegeneencodingtheproteinkinaseAKT1inasubsetofsquamouscell
carcinoma of the lung. Cell Cycle
2008;7:665-9.78.KoivunenJP,MermelC,ZejnullahuK,etal.EML4-ALKfusiongene
andefficacyofanALKkinaseinhibitorinlungcancer.ClinCancerRes
2008;14:4275-83.79.SodaM,ChoiYL,EnomotoM,etal.Identificationofthetransforming
EML4-ALKf usi ongenei nnon- smal l - cel l l ungcancer. Nature
2007;448:561-6.80.ChoiYL,TakeuchiK,SodaM,etal.Identifcationofnovelisoformofthe
EML4-ALKtransforminggeneinnon-smallcelllungcancer.CancerRes
2008;68:4971-6.81.Choi YL, Soda M, Yamashati Y, et al. EML4-ALK
mutations in lung cancer that confer resistance to ALK inhibitors.
N Engl J Med 2010;363:1734-9.82.Shaw AT, Solomon B. Targeting
anaplastic lymphoma kinase in lung cancer. Clin Cancer Res
2011;17:2081-6.83.RikovaK,GuoA,ZengQ.Globalsurveyofphosphotyrosinesignaling
identifes oncogenic kinases in lung cancer. Cell
2007;131:1190-203.84.TakeuchiK,ChoiYL,TogashiY,etal.KIF5B-ALK,anovelfusion
oncokinaseidentifiedbyanimmunohistochemistry-baseddiagnostic system
for ALK-positive lung cancer. Clin Cancer Res
2009;15:3143-9.85.SodaM,TakadaS,TakeuchiK,etal.AmousemodelforEML4-ALK-positive
lung cancer. Proc Natl Acad Sci USA
2008;105:19893-7.86.SolomonB,Varella-GarciaM,CamidgeDR.ALKgenerearrangements.
Anewtherapeutictargetinamolecularlydefnedsubsetofnon-smallcell lung
cancer. J Torac Oncol 2009;4:1450-4.87.Selinger CI, Rogers TM,
Russell PA, et al. Testing for ALK rearrangement in lung
adenocarcinoma-a multicenter comparison of immunohistochemistry and
fuorescent in situ hybridization. Mod Pathol 2013. [Epub ahead of
print].88.RodigSJ,Mino-KenudsonM,DacicS,etal.Uniqueclinicopathologic
features characterize ALK-rearranged lung adenocarcinoma in the
Western population. Clin Cancer Res
2009;15:5216-23.89.SakairiY,NakajimaT,YasufukuK,etal.EML4-ALKfusiongene
assessmentusi ngmetastati cl ymphnodesampl esobtai nedby
endobronchialultrasound-guidedtransbronchialneedleaspiration.Clin
Cancer Res 2010;16:4938-45.90.Shaw AT, Yeap BY, Mino-Kenudson M, et
al. Clinical features and outcome of patients with non-small-cell
lung cancer who harbor EML4-ALK. J Clin Oncol
2009;27:4247-53.91.Wong DW, Leung EL, So KK, et al. Te EML4-ALK
fusion gene is involved in various histologic types of lung cancers
from nonsmokers with wild-type EGFR and KRS. Cancer
2009;115:1723-33.92.InamuraK,TakeuchiK,TogashiY,etal.EML4-ALKlungcancersare
characterizedbyrareothermutations,aTTF-1celllineage,anacinar
histology, and young onset. Mod Pathol 2009;22:508-15.93.Sasaki T,
Koivunen J, Ogino A, et al. A novel ALK secondary mutation and
EGFRsignallingcauseresistancetoALKkinaseinhibitors.CancerRes
2011;71:6051-60.94.Shol
lLM,WeremowiczS,GraySW,etal.CombineduseofALK
immunohistochemistryandFISHforoptimaletectionofALK-rearranged lung
adenocarcinomas. J Torac Oncol
2013;8:322-8.95.TiseoM,GelsominoF,BoggianiD,etal.EGFRandEML4-ALKgene
mutations in NSCLC: A case report of erlotinib-resistant patient
with both concomitant mutations. Lung cancer
2011;71:241-3.96.ChinLP,SooRA,SoongR,etal.TargetingROS1withanaplastic
lymphomakinaseinhibitors:apromisingtherapeuticstrategyforanewly
definedmolecularsubsetofnonsmall-celllungcancer.JThoracOncol
2012;7:1625-30.97.Bergethon K, Shaw AT, Ou SH, et al. ROS1
rearrangements defne a unique molecular class of lung cancers. J
Clin Oncol 2012;30:863-70.98.Takeuchi K, Soda M, Togashi Y, et al.
RET, ROS1 and ALK fusions in lung cancer. Nature Med
2012;18:378-81.99.Wells SA Jr, Santoro M. Targeting the RET pathway
in thyroid cancer. Clin Cancer Res 2009;15:7119-23.100.Tran TN,
Selinger CI, Kohonen-Corish MR, et al. Fibroblast Growth Factor
Receptor1(FGFR1)copynumberisanindependentprognosticfactorin
non-small cell lung cancer. Lung Cancer 2013. [Epub ahead of
print].101.Turner N, Grose R. Fibroblast growth factor signalling:
from development to cancer. Nat Rev Cancer
2010;10:116-29.102.DuttA, RamosAH, HammermanPS, etal . Inhi bi tor-
sensi ti ve
FGFR1amplificationinhumannon-smallcelllungcancer.PLoSOne
2011;6:e20351.103.IkedaK,WangL,TorresR,etal.Discoidindomainreceptor2interacts
withSrcandShcfollowingitsactivationbytypeIcollagen.JBiolChem
2002;277:19206-12.104.KnudsonAG.Antioncogenesandhumancancer.ProcNatlAcadSciUSA
1993;90:10914-21.105.Raso MG, Wistuba II. Molecular pathogenesis of
early-stage non-small cell
lungcancerandaproposalfortissuebankingtofacilitateidentifcationof
new biomarkers. J Torac Oncol
2007;2:S128-35.106.MogiA,KuwanoH.TP53mutationsinnonsmallcelllungcancer.J
Biomed Biotech
2011;2011:583929.107.WistubaII,BerryJ,BehrensC,etal.Molecularchangesinthebronchial
epitheliumofpatientswithsmallcelllungcancer.ClinCancerRes
2000;6:2604-10.108.DAmico D, Carbone D, Mitsudomi T, et al. High
frequency of somatically
aquiredp53mutatinosinsmall-celllungcancercelllinesandtumors.
Oncogene
1992;7:339-46.109.TammemagiMC,McLaughlinJR,BullSB.Meta-analysesofp53tumor
suppressorgenealterationsandclinicopathologicalfeaturesinresected
!""#$% $' ()* +")$,-)(% ,.(/0$1 2/ )-/0 ,(/,$% S49Olung cancers.
Cancer Epidemiol Biomarkers Prev
1999;8:625-34.110.Husgafvel-PursiainenK,BoffettaP,KannioA,etal.p53mutationsand
exposure to environmental tobacco mmoke in a multicenter study on
lung Cancer. Cancer Res
2000;60:2906-11.111.TakagiY,OsadaH,KuroishiT,etal.p53mutationsinnon-small-celllung
cancers occurring in individuals without a past history of actve
smoking. Br J Cancer
1998;77:1568-72.112.SteelsE,PaesmansM,BerghmansT,etal.Roleofp53asaprognostic
factor for survival in lung cancer: a systematic review of the
literature with a meta-analysis. Eur Respir J
2001;18:705-19.113.Jin G, Kim MJ, Jeon HS, et al. PTEN mutations
and relationship to EGFR,
ERBB2,KRS,andTP53mutationsinnon-smallcelllungcancers.Lung cancer
2010;69:279-83.114.MarsitCJ,ZhengS,AldapeK,etal.PTENexpressioninnonsmall-cell
lung cancer: evaluating its relation to tumor characteristics,
allelic loss, and epigenetic alteration. Hum Pathol
2005;36:768-76.115.MarignaniPA.LKB1,themultitaskingtumoursuppressorkinase.JClin
Pathol
2005;58:15-9.116.ShawRJ,BardeesyN,ManningBD,etal.TheLKB1tumorsuppressor
negatively regulates mTOR signaling. Cancer Cell
2004;6:91-9.117.Koivunen JP, Kim J, Lee J, et al. Mutations in the
LKB1 tumour suppressor
arefrequentlydetectedintumoursfromCaucasionbutnotAsianlung cancer
patients. Br J Cancer
2008;99:245-52.118.MatsumotoS,IwakawaR,TakahashiK,etal.Prevalenceandspecifcityof
LKB1 genetic alterations in lung cancers. Oncogene
2007;26:5911-8.119.Sanchez-CespedesM,ParrellaP,EstellerM,etal.InactivationofLKB1/STK11isacommoneventinadenocarcinomasofthelung.CancerRes
2002;62:3659-62.120.OnozatoR,KosakaT,AchiwaH,etal.LKB1genemutationsinJapanese
lung cancer patients. Cancer Sci
2007;98:1747-51.121.HarbourJW,LaiSL,Whang-PengJ,etal.Abnormalitiesinstructure
andepxressionofthehumanretinoblastomageneinSCLC.Science
1988;241:353-7.122.Trimarchi JM, Lees JA. Sibling rivalry in the
E2F family. Nat Rev Mol Cell Biol
2002;3:11-20.123.BrambillaE,MoroD,GazzeriS,etal.AlterationsoftheexpressionofRb,
p16(INK4A)andcyclinD1innon-smallcelllungcarcinomaandtheir clinical
signifcance. J Pathol
1999;188:351-60.124.OttersonGA,KratzkeRA,CoxonA,etal.Absenceofp16INK4protein
isrestrictedtothesubsetoflungcancerlinesthatretainswildtypeRB.
Oncogene
1994;9:3375-8.125.PaoW,HutchinsonKE.Chippingawayatthelungcancergenome.Nat
Med
2012;18:349-51.126.PaoW,GirardN.Newdrivermutationsinnon-small-celllungcancer.
Lancet Oncol
2011;12:175-80.127.SriramKB,LarsenJE,YangIA,etal.Genomicmedicineinnon-small
celllungcancer:pavingthepathtopersonalizedcare.Respirology
2011;16:257-63.128.PaikPK,JohnsonML,DAngeloSP,etal.Drivermutationsdetermine
sur vival insmokersandnever-smokerswithstageIIIB/IVl ung
adenocarcinomas. Cancer 2012;118:5840-7.129.Shaw AT, Solomon B.
Targeting anaplastic lymphoma kinase in lung cancer. Clin Cancer
Res
2011;17:2081-6.130.TravisWD,BrambillaE,RielyGJ.Newpathologicclassificationoflung
cancer:relevanceforclinicalpracticeandclinicaltrials.JClinOncol
2013;31:992-1001.131.MotoiN,SzokeJ,RielyGJ,etal.Lungadenocarcinoma:modifcationof
the2004WHOmixedsubtypetoincludethemajorhistologicsubtype suggests
correlations between papillary and micropapillary adenocarcinoma
subtypes, EGFR mutations and gene expression analysis. Am J Surg
Pathol 2008;32:810-27.132.ZakowskiMF, HussainS, PaoW, etal .
Morphologicfeaturesof adenocarcinoma of the lung predictive of
response to the epidermal growth
factorreceptorkinaseinhibitorserlotinibandgefitinib.ArchPatholLab
Med
2009;133:470-7.133.OhtsukaK,OhnishiH,FujiwaraM,etal.Abnormalitiesofepidermal
growth factor receptor in lung squamous-cell carcinomas,
adenosquamous
carcinomas,andlarge-cellcarcinomas:tyrosinekinasedomainmutations
arenotrareintumorswithanadenocarcinomacomponent.Cancer
2007;109:741-50.134.MokT,WuYL,ZhangL.Asmallsteptowardspersonalizedmedicinefor
non-small cell lung cancer. Discov Med 2009;8:227-31.135.Zhou C, Wu
YL, Chen G, et al. Erlotinib versus chemotherapy as frst-line
treatmentforpatientswithadvancedEGFRmutation-positivenon-small-celllungcancer(OPTIMAL,CTONG-0802):amulticentre,open-label,
randomised, phase 3 study. Lancet Oncol 2011;12:735-42.136.YangJC,
Shi hJY, SuWC, etal . Afati ni bforpati entswi thl ung
adenocarcinomaandepidermalgrowthfactorreceptormutations(LUX-Lung
2): a phase 2 trial. Lancet Oncol
2012;13:539-48.137.WuJY,YuCJ,ChangYC,etal.Efectivenessoftyrosinekinaseinhibitors
onuncommonepidermalgrowthfactorreceptormutationsofunknown
clinicalsignificanceinnon-smallcelllungcancer.ClinCancerRes
2011;17:3812-21.138.LeeW,JiangZ,LiuJ,etal.Themutationspectrumrevealedbypaired
genome sequences from a lung cancer patient. Nature
2010;465:473-7.139.PleasanceED,StephensPJ,O'MearaS,etal.Asmall-celllungcancer
genomewi thcompl exsi gnaturesof tobaccoexposure. Nature
2010;463:184-90.140.ImielinskiM,BergerAH,HammermanPS,etal.Mappingthehallmarks
oflungadenocarcinomawithmassivelyparallelsequencing.Cell2012;
150:1107-20.141.PeiferM,Fernndez-CuestaL,SosML,etal.Integrativegenomeanalyses
identifykeysomaticdrivermutationsofsmall-celllungcancer.NatGenet
2012;44:1104-10.142.Rudin CM, Durinck S, Stawiski EW, et al.
Comprehensive genomic analysis identifes SOX2 as a frequently
amplifed gene in small-cell lung cancer. Nat Genet 2012;
44:1111-6.Citethisarticleas:CooperWA,LamDCL,OToole
SA,MinnaJD.Molecularbiologyoflungcancer.J
ThoracDis2013;5(S5):S479-S490.doi:10.3978/j.issn.2072-1439.2013.08.03