Embed Size (px)
Citation preview

16.
17.
18.
19.
20.
LaSalle JM, Lalande M. Homologous association of oppositely imprinted chromosomal domains. Science I996;272:725-728 Holt IJ, Miller D H , Harding AE. Genetic heterogeneity and mitochondrial DNA heteroplasmy in Leber’s hereditary optic neuropathy. J Med Genet 1989;26:739-743 Ikebe S, Tanaka M, Ozawa T. Point mutations of mitochon- drial genome in Parkinson’s disease. Mol Brain Res 1395;28:
Bolhuis PA, Rleeker-Wagemakers NJ, Ponne NJ, et al. Rapid shift in genotype of human mitochondrial DNA in a family with Ixber’s hereditary optic neuropathy. Biochein Biophys Res Commun 1990;170:994-997 Howell N , Kabacka I, Smith R, et al. Association of the mito- chondrial 8344 MERKF mutation with maternally inherited spinocerebellar degeneration and Leigh disease. Neurology
28 1-295
1996;46:219-222
Molecular Analysis of Cytochrome c Oxidase Deficiency in Leigh’s Syndrome Paula L. Adams, BSc, Kobert N. Lightowlers, PhD, and Douglass M. Turnbull, MD
Cytochrome c oxidase deficiency is the most common bio- chemical defect associated with Leigh‘s syndrome. The genetic defect responsible for this deficiency has not been identified in any patient with Leigh’s syndrome. Given that this disorder appears to be inherited as an autosomal recessive trait, this would suggest prima facie that one of the nuclear DNA-encoded cytochrome c oxidase subunits is affected. We report the first detailed sequence analysis of all 10 cytochrome c oxidase nuclear complementary DNAs and the cytochrome c oxidase mitochondrial genes in a Leigh’s syndrome patient with cytochrome c oxidase deficiency. No pathological mutations were identified in any of the cytochrome c oxidase structural genes.
Adams PL, Lightowlers RN, Turnbull DM. Molecular analysis of cytochrome c oxidase
deficiency in Leigh’s syndrome. Ann Neurol 1997;41:268-270
From the Department of Neurology, University of Newcastle upon Tyne, Newcastle upon Tyne, United Kingdom.
Received May 9, 1936, and in revised form JuI 26. Accepted for publication Aug 12, 1996. Address correspondence to Dr. Turnbull, Department of Neurol- ogy, The Medical School, University of Newcastle upon Tyne, Fratnlington Place, Newcastle upon Tyne, NE2 4HH United Kingdom.
Cytochrome c oxidase (COX) deficiency is the most common biochemical defect associated with Leigh‘s syndrome [l]. This multisubunit complex is the termi- nal electron acceptor of the mitochondrial respiratory chain. It is composed of 13 subunits, 3 of which are encoded by the mitochondrial genome (1-111) and form the catalytic core of the enzyme. The remaining 10 subunits are encoded by the nuclear genome, syn- thesized in the cytoplasm and transported into the mi- tochondria (IV-VIII). The dual genetic control of this enzyme suggests that a genetic defect of COX could be due to a mutation in the nuclear or mitochondrial genome. COX deficiency associated with Leigh’s syn- drome is thought to be inherited as an autosomal reces- sive trait. Previous cell fusion experiments demon- strated the nuclear origin of the COX defect in fibroblasts from a patient with Leigh’s syndrome [2]. The most obvious site of the genetic defect would be in one of the COX nuclear genes, or perhaps in a nuclear regulatory gene involved in assembly or stability of the COX holoenzyme. To date, however, no nuclear gene mutations have been identified. We describe the bio- chemical and molecular investigations of a woman with COX deficiency, who presents with the clinical and neuroradiological features of Leigh’s syndrome.
Materials and Methods Patient Details A 32-year-old woman who is the third child of healthy, unre- lated parents had no family history of neurological disease. She first presented at the age of 3 and an eye movement disorder (nystagmus and bilateral sixth nerve palsies) and py- ramidal and extrapyramidal features progressively developed. At the age of 14, a computed tomography scan showed sym- metrical low densities in the putamen, head of the caudate, and corona radiata. She had mild lactic acidosis (blood lac- tate concentration, 2.5 mM; normal, < 2.0 mM).
Spectrophotometric and Immunoblot Analysis of the Mitochondria1 Fractions Mitochondrial fractions were prepared from skin fibroblasts and immortalized B lymphocytes from the patient and con- trol subjects [3]. Individual respiratory chain complexes I, 11, and IV, citrate synthase, and protein were measured as described elsewhere [3] . Reduced-minus-oxidized spectra of cytochromes were recorded at room temperature and cyto- chrome concentrations were determined, essentially as de- scribed previously [4] . Mitochondrial protein was separated by sodium dodecyl sulfate-polyacrylamide gel electrophore- sis a n d immunoblotted with antisera to the COX human heart holoenzyme [5].
Direct Sequencing of Complementary DNAs Encoding ALL of the COX Nuclear and Mitochondria1 Subunits COX nuclear transcripts (IV-VIII) were reverse transcribed (RT) and amplified by polymerase chain reaction (PCR)
268 Copyright 0 1997 by the American Neurological Association

from total cytosolic RNA [GI. Mitochondrial COX genes (I- 111) were amplified by PCR from mitochondrial DNA using standard techniques. Single-strand sequencing of the ampli- fied products was performed using Sequenase either manually or by automated sequencing (ABI model 373A DNA se- quencer). Positions of the RT-PCR, PCR, and sequencing primers are available from the authors.
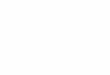
Results The activities of COX (complex IV) in patient fibro- blasts and B lymphoblasts were 12% and 13% of con- trol values, respectively. The decrease in activity was related to a decreased amount of all immunologically reactive subunits of COX and a low cytochrome ad, concentration (Fig). This decrease in protein was pro- portional to the loss in COX activity. Northern blot analysis failed to reveal any abnormality in size or abundance of all the COX nuclear transcripts studied (data not shown). Direct sequencing of RT-PCR and PCR-generated complementary DNA (cDNA) encod- ing all the COX nuclear (IV-VIII) and mitochondrial (1-111) subunits identified no pathological mutations. Comparison of our sequences with the original human cDNA sequences and the Cambridge mitochondrial DNA sequence [7], however, revealed several base sub- stitutions and insertions, some of which were predicted to alter amino acids. These nucleotides were subse- quently sequenced in six different controls and the same base substitutions and insertions were identified in all control samples (Table). These changes have now been submitted to Genebank and EMBL.
Discussion We describe the biochemical and molecular investiga- tions of a woman with COX deficiency, who presented with the clinical and neuroradiological features consis- tent with Leigh’s syndrome. A strong link between COX deficiency and Leigh’s syndrome has already been well documented in a number of biochemical studies performed in various tissues [I , 81. This is the first detailed report, however, of a Leigh’s syndrome patient with COX deficiency whose sequences of all the COX nuclear and mitochondrial genes have been identified and analyzed (excluding muscle isoforms).
The report demonstrates a systemic defect of COX. The activity and amount of the enzyme were low, but the estimated turnover number was normal (patient, 21.3 sec-’; mean for 7 controls, 21.0 _+ 2.1 sec-’). A number of groups [ 1, 81 reported a generalized decrease in all immunoreactive COX subunits, including a de- creased steady-state level of COX subunit IV in COX- deficient Leigh’s syndrome patients. Several groups, however, reported the relative sparing of COX subunit IV in COX-negative fibers of skeletal muscle from pa- tients with large deletions of mitochondrial DNA [9], a microdeletion of COX I11 gene [lo], or mutations
A
400 500 600 $00
Wavelength (nm)
B
(A) Immunoblot analysis o f holocomplex IV in mitochondrial fiactions. Lane I , purified bovine cytochrome c oxidase (COX) (5 pd; lanes 2 and 3, patient jbroblast mitochon- dFial protein (50 and 80 pd; lanes 4 and 5, control jbro- blast mitochondria1 protein (50 and 80 jig); lanes 6 and 7, patient lymphoblast mitochondrial protein (50 and 80 pd; and lanes 8 and 9, control lymphoblast rnitochondrial protein (50 and 80 pd . Mitochondrial proteins were separated by sodium dodecyl sulfate-polyacrylamide gel electrophoresis and immunoblotted using human heart antiserum to the COX boloenzyme. A generalized reduction o f COX subunits II, I K Va, and Vb in the mitochondria o f both patient cell lines is apparent. (B) Cytochrome spectra of lymphoblast mitochon- drial fiactions. One milligram of mitochondrial protein iso- lated fiom patient and control lymphoblasts were subjected to spectrophotornetric analysis as described in Materials and Methods. A marked loss o f cytochrome aa3 in the patient (upper trace) compared with a control subject (lower trace) is apparent.
Brief Communication: Adams et al: COX Deficiency in Leigh‘s Syndrome 269

References Base Substitutionsllnsertions Identijed in Cytocbrome c Oxidase (COX) Mitochondria1 Genes (COX I-Ill) and Nuclear cDNA Transcr$ts (COX JV- VIII)‘
Gene/ cDNA Differences
Accession Numbers
COX 1 cox I11
COX 1v COX Va COX Vb COX
V1a.L COX Vlc cox VITI
T,,,,C silenr C,,IIT silent Co365T silent T,,,,C silent [ l5] GgIj,C Arg,,, + Pro” [I61 G jj l.cj4GG 3’UTR M2 1575 C,;,A:T,,,C Leu6, + Thr A,,,,T silent M22760 G,,;C silenr C& Gln-, + Glu” MI9961 C?,,--,, CC 5’UTR XI5341
CLL r 5er,) 4 Phch X13238 GI , T 3’UYR (6 nt from stop codon) J04823
”The riucleotide positions in the mitochondria1 COX genes refer tu the L-strand of the published mitochondrial DNA sequence [7]. Nucleotide positions in the nuclear COX cDNAs refer to the pub- lished human COX cDNA sequences (LV-VIII). ”Refers to an amino acid change that is homologous to the pub- lished bovine COX amino acid sequence.
UTR = untranslated region; i i t = nucleotide.
of transfer RNA genes [ l I] . It is therefore tempting to speculate that such a decreased steady-state level of COX subunit IV may prove to be pathognomic for COX deficiency associated with defects of the nuclear rather than the mitochondrial genome. These findings are supported by other immunological studies that also showed near-normal steady-state levels of COX subunit IV in p” cells [12] and thiamphenicol (an inhibitor of mitochondrial protein synthesis)-treated HepG2 cells
We showed that the deficiency of Cox associated with Leigh’s syndrome in our patient is not caused by a mutation in one of the genes encoding a nuclear, or indeed a mitochondrial subunit of COX. Instead, the genetic defect must lie in a nuclear regulatory protein involved in the assembly or stability of the COX holo- enzyme itself. Only a limited number of nuclear regula- tory genes have been identified in humans [13, 141. During the preparation of this manuscript, RT-PCR of the nuclear transcript OXAl [13], a human gene known to be involved in COX assembly, was per- formed. Sequence analysis of our patient sample, how- ever, showed a normal sequence. We are currently us- ing an alternative approach to identify the genetic defect underlying COX deficiency, involving func- tional complementation.
151.
This work was funded by a Wellcome Trust Studentship.
We gratefully acknowledge Dr M. Hiratio and Dr E. A. Schon for assistance in suhmirting the nucleotide corrections to Genbank and EMBL.
1.
2.
3.
4.
5 .
6.
7.
8.
9.
10.
11.
12.
13.
14.
15
16
DiMauro S, Servidei S, Zeviani M, et al. Cytochrome c oxidase deficiency in Leigh syndrome. Ann Neurol 1987;22:498-506 Tiranto V, Minaro M, Sandona D, et al. Nuclear origin of cytochrome c oxidase deficiency in Leigh’s syndrome: genetic evidence based on patient’s-derived ? transformanrs. Hum Mol Genet 1995;4:20 17-2023 Lowerson SA, Taylor L, Briggs HL, Turnbull DM. Measure- ment of the activity of individual respirarory chain complexes in isolated fibroblast mitochondria. Anal Biochem 1992;205:
Bindoff LA, Birch-Machin MA, Cartlidge NEF, et al. Respira- tory chain abnormalities in skeletal muscle from patients with Parkinson’s disease. J Neurol Sci 1991;104:203-208 Clirzanowska-Ligl~towlers ZMA, Turnbull DM, Bindoff LA, Lightowlers RN. An antisense oligodeoxynucleotide approach to investigate the function of the nuclear-encoded subunits of human cytochrome c oxidase. Biochem Biophys Res Commun 1993; 196:328-335 Mallet F, Onol G, Mary C, et al. Continuous RT-PCR using AMV-RT and Taq polymerase: characterisation and compari- son to uncoupled procedures. Biorechniques 1995;18:678-687 Anderson S, Bankier AT, Barrel1 BG, et al. Sequence and orga- nization of the human mitochondrial genome. Nature 1981; 290:457-465 Lombes A, Naltase H, Tritschler HJ, et al. Biochemical and molecular analysis of cytochrome c oxidase deficiency in high‘s syndrome. Neurology 1991;41:491-498 Moraes CT, UiMauro S, Zeviani M, et al. Mitochondria1 DNA deletions in progressive external ophthalmoplegia and Keartis-Sayre syndrome. N EngI J Med 1989:320: 1293-1299 Keightley J, Hoffbuhr I<, Burton M, et al. A microdeletion in cytochrome c oxidase (COX) subunit 111 associated with COX deficiency and recurrent myoglobinuria. Nat Genet 1996;12: 4 10-4 16 Mira S, Schmidt B, Schon EA, et 31. Detection of “deleted” mitochondrial genomes in cytochrome-c.-oxidase deficient mus- cle fibers of a patient with Kearns-Sayre syndrome. Proc Natl Acad Sci USA 1989;86:9509-9513 Taanman I-W, Burton M, Marusich M , et al. Subunit specific monoclonal antibodies show different steady-stare levels of vari- ous cytochrome c oxidase subunits in chronic progressive exter- nal ophthalmoplegia Biochim Biophys Acta 1996;1315:193- 207 Bonnefoy N , Kermorganr M, Groudinsky 0, et al. Cloning of a human gene involved in cytochrome oxidase assembly by functional complementation of an oxal- muration in Sacrbum- myces cevevisiue. Proc Natl Acad Sci USA 1994;91:11978- 11982 Altamura N, Capitanio N, Bonnefoy N, et al. The SUCC~LZYO- myces rerevisiue OXAl gene is required for the correct assembly of cytochrome c oxidase and oligomycin-sensitive ATP syn- thase. FEBS Lett 1996:382: 1 1 1-1 15 Monnat R, Loeh L. Nucleoride sequence preservation of hu- man mtDNA. Proc Natl Acad Sci USA 1985;82:2895-2839 Marzuki S, Noer A, Lertrit P, et al. Normal variants of human mtDNA and translation products: the building of a reference data base. Hum Genet 1391;88:139-145
372-374
270 Annals of Neurology Vol 41 No 2 February 1997