Embed Size (px)
Citation preview

MOLAR DISTALIZATION – MOLAR DISTALIZATION – CURRRENT TRENDSCURRRENT TRENDS
INDIAN DENTAL ACADEMY
Leader in continuing dental education www.indiandentalacademy.com
www.indiandentalacademy.com

The appliances used for molar The appliances used for molar distalization can be divided into distalization can be divided into
Removable appliances andRemovable appliances and Fixed appliances.Fixed appliances.
Removable appliances are:Removable appliances are: Extra oral tractionExtra oral traction Removable appliances with finger Removable appliances with finger
springs springs Sliding jigs with intermaxillary Sliding jigs with intermaxillary
elastics.elastics.www.indiandentalacademy.com

The fixed appliances areThe fixed appliances areA. Intramaxillary applianceA. Intramaxillary appliance1. Wislons 3D appliance1. Wislons 3D appliance2. Repelling Magnets2. Repelling Magnets3.The pendulum appliance3.The pendulum appliance4. Niti based appliances : archwires – single 4. Niti based appliances : archwires – single
loop, double loop; Compressed coil springsloop, double loop; Compressed coil springs5. Jones jig5. Jones jig6. Distal Jet6. Distal Jet7. Fixed piston appliances7. Fixed piston appliances8. IBMD8. IBMD9. K-loop9. K-loop10.Franzulum appliance10.Franzulum appliance11. First class appliance11. First class appliance
www.indiandentalacademy.com

B. B. Intermaxillary appliance:Intermaxillary appliance:1. Herbst appliance1. Herbst appliance2. Jasper Jumper2. Jasper Jumper3. Eureka Spring3. Eureka Spring4. Klapper superspring4. Klapper superspring
C. SAS supported distalization:C. SAS supported distalization:
www.indiandentalacademy.com

INDICATIONS & CONTRAINDICATIONSINDICATIONS & CONTRAINDICATIONS THE INDICATIONS FOR MOLAR DISTALIZATIONTHE INDICATIONS FOR MOLAR DISTALIZATION 1. In non-extraction treatment of Class II 1. In non-extraction treatment of Class II
malocclusion cases.malocclusion cases. 2. In low & average mandibular plane angle cases.2. In low & average mandibular plane angle cases. 3. In class I skeletal pattern cases.3. In class I skeletal pattern cases. 4. In patients with mild arch length discrepancy.4. In patients with mild arch length discrepancy. 5. In cases where the upper permanent molars have 5. In cases where the upper permanent molars have
moved mesially due to early loss of deciduous moved mesially due to early loss of deciduous molars.molars.
6. In patients where the second molars extractions 6. In patients where the second molars extractions are planned or where it has not yet erupted.are planned or where it has not yet erupted.
7. In second molar extraction cases where the third 7. In second molar extraction cases where the third molars are well formed and erupting properly.molars are well formed and erupting properly.
www.indiandentalacademy.com

CONTRAINDICATIONS FOR MOLAR CONTRAINDICATIONS FOR MOLAR DISTALIZATIONDISTALIZATION
In high mandibular plane angle In high mandibular plane angle cases.cases.
Skeletal and Dental open biteSkeletal and Dental open bite Class II & III skeletal patternClass II & III skeletal pattern Severe arch length discrepancy Severe arch length discrepancy
patients.patients.
www.indiandentalacademy.com

INFLUENCE OF 2INFLUENCE OF 2NDND MOLAR ON DISTALIZATION OF MOLAR ON DISTALIZATION OF 11STST MOLAR MOLAR
A controversy exists concerning the influence of second A controversy exists concerning the influence of second molars on the distal movement of the first molars. molars on the distal movement of the first molars.
Graber noted that extraoral traction on the first molars, Graber noted that extraoral traction on the first molars, when the second molars have not totally erupted, led to when the second molars have not totally erupted, led to distal tipping only and not to bodily distal movement. distal tipping only and not to bodily distal movement. Bondemark et al (AO 94 Magnets vs NiTi coils) stated Bondemark et al (AO 94 Magnets vs NiTi coils) stated that the presence of second molars did influence tipping that the presence of second molars did influence tipping and distal movement of the first molars.and distal movement of the first molars.
Gianelly (AJO 91 NiTi coils) also found that treatment Gianelly (AJO 91 NiTi coils) also found that treatment time was increased with the presence of second molars.time was increased with the presence of second molars.
Muse et al (AJO 93 Wilsons BDA) found that the Muse et al (AJO 93 Wilsons BDA) found that the presence of maxillary second molars did not correlate presence of maxillary second molars did not correlate with the rate of maxillary first molar movement or with with the rate of maxillary first molar movement or with the amount of tipping that occurred. the amount of tipping that occurred.
www.indiandentalacademy.com

Studies on Pendulum ApplianceStudies on Pendulum Appliance The findings of the Byloff’s study (AO The findings of the Byloff’s study (AO
1997) were similar to those of Muse et al 1997) were similar to those of Muse et al i.e. no statistically significant differences i.e. no statistically significant differences in linear or angular changes were found in linear or angular changes were found among three groups of eruption stages of among three groups of eruption stages of second molars.second molars.
According to studies by Bussick and According to studies by Bussick and McNamara (AJO 2000March); Ghosh and McNamara (AJO 2000March); Ghosh and Nanda (AJO 96); and Joseph and Butchart Nanda (AJO 96); and Joseph and Butchart (Seminars in Orthod 2000) the position of (Seminars in Orthod 2000) the position of the 2the 2ndnd molar when distalizing the first molar when distalizing the first molar with a pendulum appliance is of molar with a pendulum appliance is of little if any importancelittle if any importance
www.indiandentalacademy.com

Kinzinger et al (AJO 2004 Jan) used modified pendulum Kinzinger et al (AJO 2004 Jan) used modified pendulum appliance for bilateral maxillary molar distalization in 36 appliance for bilateral maxillary molar distalization in 36 adolescent patients in various stages of the molar dentition.adolescent patients in various stages of the molar dentition.
In PG 1, eruption of the second molars had either not yet In PG 1, eruption of the second molars had either not yet taken place or was not complete.taken place or was not complete.
In PG 2, the second molars had already developed as far as In PG 2, the second molars had already developed as far as the occlusal plane, with the third molars at the budding stage.the occlusal plane, with the third molars at the budding stage.
In PG 3, germectomy of the wisdom teeth had been carried In PG 3, germectomy of the wisdom teeth had been carried out and the first and second molars on both sides had out and the first and second molars on both sides had completely erupted.completely erupted.
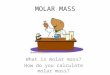
Analysis of cephalograms to identify any changes in the Analysis of cephalograms to identify any changes in the sagittal plane showed that, in the direction of distalization, sagittal plane showed that, in the direction of distalization, a a tooth bud acts on the mesial neighboring tooth like a fulcrum.tooth bud acts on the mesial neighboring tooth like a fulcrum.
PG1 PG2 PG3
www.indiandentalacademy.com

The degree of distal tipping of first molars was less in The degree of distal tipping of first molars was less in patients with erupted second molars (PG 2 and PG 3) patients with erupted second molars (PG 2 and PG 3) than in those whose second molars were not yet than in those whose second molars were not yet erupted (PG 1). erupted (PG 1).
Tipping of erupted second molars was much more Tipping of erupted second molars was much more marked in PG 2 but much less pronounced in PG 3 marked in PG 2 but much less pronounced in PG 3 than the corresponding movement of the second than the corresponding movement of the second budding-stage molars in PG 1. budding-stage molars in PG 1.
In PG3 almost exclusively bodily distalization of both In PG3 almost exclusively bodily distalization of both molars is possible, even without bands being applied molars is possible, even without bands being applied to the second molars.to the second molars.
However, if the first and second molars are distalized However, if the first and second molars are distalized simultaneously with a pendulum appliance, the simultaneously with a pendulum appliance, the duration of therapy will be longer, greater forces will duration of therapy will be longer, greater forces will have to be applied, and more anchorage will be lost. have to be applied, and more anchorage will be lost.
www.indiandentalacademy.com

REMOVABLE APPLIANCES AREREMOVABLE APPLIANCES ARE : : EXTRA ORAL FORCESEXTRA ORAL FORCES REMOVABLE APPLIANCESREMOVABLE APPLIANCES THE CETLIN APPLIANCETHE CETLIN APPLIANCE EXTRA ORAL FORCESEXTRA ORAL FORCES One of the earliest methods of molar One of the earliest methods of molar
distalization introduced and proved to be distalization introduced and proved to be effective was by extra oral forces effective was by extra oral forces employing use of the employing use of the head gear.head gear.Components of Head Gear:Components of Head Gear:
Force delivering Unit: Force delivering Unit: Force Generating Unit. Force Generating Unit. The Anchor Unit: The Anchor Unit:
www.indiandentalacademy.com

SELECTION OF HEADGEAR:SELECTION OF HEADGEAR: 11. . Headgear anchorage locationHeadgear anchorage location:: location of the location of the
anchorage unit determines the type of force that will anchorage unit determines the type of force that will be applied to the unit. The relation of the force to the be applied to the unit. The relation of the force to the Cres of the unit to which it is applied determines the Cres of the unit to which it is applied determines the effects that will be produced by the orthopedic force. effects that will be produced by the orthopedic force. High pull headgearHigh pull headgear:: this applies a superior this applies a superior
(intrusive) and distal force to the maxilla and the (intrusive) and distal force to the maxilla and the maxillary dentition.maxillary dentition.
Cervical pull:Cervical pull: this produces an inferior (extrusive) this produces an inferior (extrusive) and distalising force on the maxilla. and distalising force on the maxilla.
Combination headgearCombination headgear:: no moment is produced no moment is produced and a distalising force is applied to the maxilla.and a distalising force is applied to the maxilla.
Since the Cres of the molar is located in the mid root Since the Cres of the molar is located in the mid root region, force vectors above this point will result in a region, force vectors above this point will result in a distal root movement. Forces below this point will distal root movement. Forces below this point will result in a distal crown movement. Similar result in a distal crown movement. Similar considerations apply to the maxilla. considerations apply to the maxilla.
www.indiandentalacademy.com

TYPES OF HEADGEARS:TYPES OF HEADGEARS:CERVICAL HEADGEAR:CERVICAL HEADGEAR: This was first introduced This was first introduced
by by SILAS KLOEHNSILAS KLOEHN in 1947. in 1947. It is the most commonly It is the most commonly used facebow in clinical used facebow in clinical practice. Typically it is practice. Typically it is used in growing patients used in growing patients with decreased vertical with decreased vertical dimension. The purpose of dimension. The purpose of the facebow is to restrict the facebow is to restrict the forward growth of the the forward growth of the maxilla. The vector of force maxilla. The vector of force is below the occlusal plane is below the occlusal plane producing both extrusive producing both extrusive and distalising effects. and distalising effects.
www.indiandentalacademy.com

Effects of cervical headgear:Effects of cervical headgear: to erupt the entire upper jawto erupt the entire upper jaw tends to move the upper jaw tends to move the upper jaw
distallydistally Steepen the occlusal plane. Steepen the occlusal plane. Expansion of the upper arch.Expansion of the upper arch.Effect of different positions of the outer bow:Effect of different positions of the outer bow:
when the outer bow is bent upwardswhen the outer bow is bent upwards::The forces that are produced are The forces that are produced are
A distalising force to the upper teeth, which is good A distalising force to the upper teeth, which is good for correction of class II relation.for correction of class II relation.When the outer bow is bent upwards, bringing it When the outer bow is bent upwards, bringing it down to the occlusal plane tends to produce a down to the occlusal plane tends to produce a negative moment that flattens the occlusal plane. negative moment that flattens the occlusal plane. Hence the steepening effect of the cervical Hence the steepening effect of the cervical headgear is nullified.headgear is nullified.Eruption of the entire upper arch tends to increase Eruption of the entire upper arch tends to increase the mandibular plane angle and tends to worsen the mandibular plane angle and tends to worsen the class II skeletal relationship.the class II skeletal relationship.this type is good for patients with forward growth this type is good for patients with forward growth rotationrotation
www.indiandentalacademy.com

when the outer bow is bent when the outer bow is bent downwardsdownwards::
Forces that are produced areForces that are produced are Positive moment on the occlusal Positive moment on the occlusal
plane is seen that tends to steepen plane is seen that tends to steepen the occlusal plane since the pull is the occlusal plane since the pull is below the Cres.below the Cres.
Extrusive force and a distalising Extrusive force and a distalising force.force.
When the outer bow and When the outer bow and inner bow are in the same inner bow are in the same levellevel,, no moment is produced no moment is produced and there is a net distalising and there is a net distalising and extrusive force.and extrusive force.
When the When the outer bow is shorterouter bow is shorter than the inner bow, than the inner bow, the headgear strap hook is placed too far anteriorly. the headgear strap hook is placed too far anteriorly. This results in a greater tendency to steepen the This results in a greater tendency to steepen the occlusal plane when the straps are engaged. The pull occlusal plane when the straps are engaged. The pull of the bow is further forward from the Cres and this of the bow is further forward from the Cres and this tends to steepen the occlusal plane. When the tends to steepen the occlusal plane. When the outer outer bow is longbow is long, there is a tendency to flatten the occlusal , there is a tendency to flatten the occlusal plane.plane.
www.indiandentalacademy.com

Advantages Advantages Direction of pull is advantageous in Direction of pull is advantageous in
treatment of short face class II maxillary treatment of short face class II maxillary protrusive cases with low MPA and deep protrusive cases with low MPA and deep bites. bites.
Disadvantages: Disadvantages: It normally causes extrusion of the upper It normally causes extrusion of the upper
molars. This movement is seldom desirable molars. This movement is seldom desirable except in patients with reduced lower except in patients with reduced lower anterior facial height. It is contraindicated anterior facial height. It is contraindicated in patients with steep mandibular planes in patients with steep mandibular planes and in open bite cases.and in open bite cases.
www.indiandentalacademy.com

Long term study on cervical headgear:Long term study on cervical headgear:
Melsen et al in AJO 2003Melsen et al in AJO 2003 studstudiedied the the intramaxillary molarintramaxillary molar displacement 7 years after displacement 7 years after treatment with Kloehn headgeartreatment with Kloehn headgear and cervical and cervical tractiontraction. Two groups of 10 patients were studied. . Two groups of 10 patients were studied. In one group, the outer bow was tilted upward by In one group, the outer bow was tilted upward by 202000 and in another group, it was tilted down by and in another group, it was tilted down by 202000. In the group that had the outer bow tilted . In the group that had the outer bow tilted downwards, molar correction was faster. In both downwards, molar correction was faster. In both the groups, the maxilla was moved backward and the groups, the maxilla was moved backward and downward. downward. A strongA strong tendency of the molars to tendency of the molars to return to the key return to the key ridge wasridge was demonstrated, and demonstrated, and there there waswas no evidence that no evidence that the Class Ithe Class I relationship obtained by extraoral traction relationship obtained by extraoral traction waswas moremore stable than that obtained by functional or stable than that obtained by functional or intramaxillaryintramaxillary appliances.appliances.
www.indiandentalacademy.com

OCCIPITAL HEADGEAR:OCCIPITAL HEADGEAR: The occipital headgear consists of a The occipital headgear consists of a
facebow which fits over the occiput of facebow which fits over the occiput of the head. The force generated by a the head. The force generated by a high pull (occipital) has both distalising high pull (occipital) has both distalising and intrusive forces since the force is and intrusive forces since the force is exerted above the occlusal plane. Such exerted above the occlusal plane. Such forces are used in conditions where forces are used in conditions where vertical control of the molars is vertical control of the molars is important. As growth guiding important. As growth guiding appliance, a high pull headgear can appliance, a high pull headgear can decrease the vertical development of decrease the vertical development of the maxilla, thereby allowing for the maxilla, thereby allowing for autorotation of the mandible and autorotation of the mandible and maximizing the horizontal expression maximizing the horizontal expression of mandibular growth.of mandibular growth.
Occipital pull with short outer bow (force Occipital pull with short outer bow (force anterior to Cres)anterior to Cres)This results in a force system at the unit’s Cres with a This results in a force system at the unit’s Cres with a moment that tends to flatten the occlusal plane and moment that tends to flatten the occlusal plane and creates distalising and intrusive components.creates distalising and intrusive components.www.indiandentalacademy.com

b. b. occipital pull with force occipital pull with force passing through Crespassing through Cres
There is no moment that is There is no moment that is created and hence there is created and hence there is no change in the cant of the no change in the cant of the occlusal plane. Intrusive occlusal plane. Intrusive and distal components of and distal components of force are produced.force are produced.
c. c. occipital pull with long occipital pull with long outer bow( force outer bow( force posterior to Cres)posterior to Cres)
The force system at the The force system at the unit’s Cres has a moment unit’s Cres has a moment that tends to steepen the that tends to steepen the occlusal plane. Intrusive occlusal plane. Intrusive and distalising forces are and distalising forces are produced. This system produced. This system might be required in class II might be required in class II open bite patients.open bite patients.
www.indiandentalacademy.com

Advantages:Advantages: These headgears can be used in These headgears can be used in
patients with steep mandibular patients with steep mandibular planes and in cases wherein planes and in cases wherein mandibular growth is more vertical mandibular growth is more vertical than horizontal. They can also be than horizontal. They can also be used in certain open bite cases used in certain open bite cases caused due to excessive eruption of caused due to excessive eruption of buccal teeth. buccal teeth.
www.indiandentalacademy.com

Combination headgears have both Combination headgears have both occipital and cervical traction springs. occipital and cervical traction springs. This is perhaps the most versatile type This is perhaps the most versatile type because the pull can be readily because the pull can be readily controlled by selecting the force level controlled by selecting the force level of the springs and by controlling the of the springs and by controlling the length of the outer bow. For distal length of the outer bow. For distal translation of the upper posteriors, a translation of the upper posteriors, a distal traction is needed that passes distal traction is needed that passes through the Cres, neither above nor through the Cres, neither above nor below. The combination type headgear below. The combination type headgear will allow a distal force straight will allow a distal force straight through Cres by having equal occipital through Cres by having equal occipital and cervical components on the outer and cervical components on the outer bow, which is angled upwards to allow bow, which is angled upwards to allow the force to pass through the Cres. the force to pass through the Cres.
COMBINATION HEADGEAR.COMBINATION HEADGEAR.
www.indiandentalacademy.com

Based on occlusal plane requirements:Based on occlusal plane requirements:Action desiredAction desired Outer bow Outer bow angulationangulation
distal force and flattening - outer distal force and flattening - outer bow above bow above Cres Cres
distal force and steepeningdistal force and steepening - - outer bow below outer bow below CresCres
distal force and no moment-- outer distal force and no moment-- outer bow at Cresbow at Cres
www.indiandentalacademy.com

Alain (JCO 1972) explained the use of a removable Alain (JCO 1972) explained the use of a removable appliance for distalizing the molars. The appliance was appliance for distalizing the molars. The appliance was originally devised by G.Vienne and later produced by originally devised by G.Vienne and later produced by A.Lorette.A.Lorette.
The appliances were introduced as the appliances with The appliances were introduced as the appliances with wires sliding in tubes.wires sliding in tubes.THE PRINCIPLETHE PRINCIPLE
The appliance consists of a stationary part and a movable The appliance consists of a stationary part and a movable part. Both these parts are held together by a long, part. Both these parts are held together by a long, horseshoe shaped wire which moves the movable part by horseshoe shaped wire which moves the movable part by virtue of the elasticity of the wire. Each end of the wire is virtue of the elasticity of the wire. Each end of the wire is inserted into a tube, one in the fixed part of the appliance inserted into a tube, one in the fixed part of the appliance and the other inthe removable part. and the other inthe removable part.
REMOVABLEREMOVABLE APPLIANCESAPPLIANCES
www.indiandentalacademy.com

THE APPLIANCETHE APPLIANCE The movable part has an adams clasp and two The movable part has an adams clasp and two
parallel tubes embedded for the molars to be parallel tubes embedded for the molars to be moved distally. moved distally.
The stationary part contains the other clasps for The stationary part contains the other clasps for the retention of the plate and one tube which the retention of the plate and one tube which contains the other end of the horse shoe shaped contains the other end of the horse shoe shaped active wire.active wire.ACTIVATIONACTIVATION
Using the 139 plier, the wire coming out of the Using the 139 plier, the wire coming out of the tube embedded in the stationary part is bent, tube embedded in the stationary part is bent, which makes the movable part slide distally. which makes the movable part slide distally. DISADVANTAGEDISADVANTAGE
A delicate appliance, since the two wires holding A delicate appliance, since the two wires holding the movablethe movable part should do so without binding.part should do so without binding.
www.indiandentalacademy.com

3. THE CETLIN APPLIANCE3. THE CETLIN APPLIANCE
JCO 1983 Cetlin and TenhoeJCO 1983 Cetlin and Tenhoe The appliance involves a combination of extra oral force The appliance involves a combination of extra oral force
in the form of head gear and an intraoral force in the in the form of head gear and an intraoral force in the form of a removable appliance.form of a removable appliance.
The Cetlin appliance utilises a removable appliance The Cetlin appliance utilises a removable appliance intraorally to tip the crowns distally and then an intraorally to tip the crowns distally and then an extraoral force to upright the roots. So the intra oral extraoral force to upright the roots. So the intra oral removable appliance can be called the crown mover removable appliance can be called the crown mover while the extra oral force, the root mover.while the extra oral force, the root mover.ANCHORAGEANCHORAGE
The anchorage for the removable appliance is by proper The anchorage for the removable appliance is by proper adaptation to the palate, an acrylic shield around the four adaptation to the palate, an acrylic shield around the four maxillary incisors and a modified adams clasp on the first maxillary incisors and a modified adams clasp on the first premolars.premolars. www.indiandentalacademy.com

THE EXTRA ORAL FORCETHE EXTRA ORAL FORCE The extra Oral appliance is a headgear which is The extra Oral appliance is a headgear which is
inserted into molar tube. The headgear used is inserted into molar tube. The headgear used is generally cervical or a high pull, depending on the generally cervical or a high pull, depending on the usual consideration of the skeletal pattern.usual consideration of the skeletal pattern.THE APPLIANCETHE APPLIANCE
The removable appliance is worn 24 hours a day. The The removable appliance is worn 24 hours a day. The appliance also contains a bite plane to disengage the appliance also contains a bite plane to disengage the molars (to aid in rapid molar movement).molars (to aid in rapid molar movement).THE FORCE APPLIEDTHE FORCE APPLIED
In the removable appliance, the spring is activated only In the removable appliance, the spring is activated only 1 to 1.5 mm, measured along the occlusal of the molar 1 to 1.5 mm, measured along the occlusal of the molar and it supplies force on the molars of only 30 gms. The and it supplies force on the molars of only 30 gms. The springs are placed as far gingivally as possible to springs are placed as far gingivally as possible to minimize crown tipping and to cause molar movement minimize crown tipping and to cause molar movement without irritation.without irritation.
The extra oral head gear on the other hand exerts a The extra oral head gear on the other hand exerts a 150 gm force per tooth and is used to control root 150 gm force per tooth and is used to control root position. The headgear is adviced to be worn for 12-14 position. The headgear is adviced to be worn for 12-14 hours/day.hours/day.
www.indiandentalacademy.com

INTRAMAXILLRY APPLIANCESINTRAMAXILLRY APPLIANCESWILSONS' RAPID MOLAR WILSONS' RAPID MOLAR
DISTALIZATIONDISTALIZATIONAdvocated by William L. Wilson & Robert C.Wilson Advocated by William L. Wilson & Robert C.Wilson
(1984 JCO)(1984 JCO)under modular orthodontics. under modular orthodontics. the pre-treatment antero-posterior positions. The the pre-treatment antero-posterior positions. The
Wilson treatment achieves molar distalization Wilson treatment achieves molar distalization without extra oral forces.without extra oral forces.
THE CONCEPTTHE CONCEPT Newton’s' 3rd law of motion states that 'for every Newton’s' 3rd law of motion states that 'for every
force, there is an equal and opposite force', (i.e.) for force, there is an equal and opposite force', (i.e.) for every moment, there is a counter moment.every moment, there is a counter moment.
Implicit in Newton’s' law is the concept that control Implicit in Newton’s' law is the concept that control of counter moments increases the efficiency of the of counter moments increases the efficiency of the moment of force. Modular orthodontic units have moment of force. Modular orthodontic units have been designed to control countermoments, been designed to control countermoments, eliminate 'round trips', and reduce headgear use.eliminate 'round trips', and reduce headgear use.
www.indiandentalacademy.com

DESIGN OF APPLIANCEDESIGN OF APPLIANCE Wilson advocates maxillary Wilson advocates maxillary
bimetric distalizing arches bimetric distalizing arches (BDA) and a mandibular (BDA) and a mandibular three dimensional lingual three dimensional lingual arch. The bimetric arch arch. The bimetric arch produces a coil spring action produces a coil spring action against the molars and against the molars and producing an anterior producing an anterior counter moment against the counter moment against the incisors, which is controlled incisors, which is controlled by the wearing of class II by the wearing of class II elastics.elastics.
These, in turn, react with a These, in turn, react with a lower molar mesial force lower molar mesial force vector which is controlled by vector which is controlled by the 3D lingual arch with a the 3D lingual arch with a design for anchorage design for anchorage resistance. This is resistance. This is supplemented by molar supplemented by molar buccal root torque and buccal root torque and cortical resistance to satisfy cortical resistance to satisfy increased anchorage needs.increased anchorage needs.
www.indiandentalacademy.com

The vertical component of elastic force is controlled The vertical component of elastic force is controlled by using the elastic load reduction principle, in by using the elastic load reduction principle, in which the elastic force is reduced to physiologically which the elastic force is reduced to physiologically acceptable levels. Mandibular anchorage and acceptable levels. Mandibular anchorage and elastic load reduction control the reactive elastic load reduction control the reactive countermoments and produce a relatively friction countermoments and produce a relatively friction free, rapid distalizing of molars; without headgear free, rapid distalizing of molars; without headgear and with preservation of mandibular arch integrity.and with preservation of mandibular arch integrity.Wilson's Schedule for Maximum Mandibular Wilson's Schedule for Maximum Mandibular AnchorageAnchorage
6 ounce elastics for 5 days.6 ounce elastics for 5 days. 4 ounce elastics for 5 days and4 ounce elastics for 5 days and 2 ounce elastics for 11 days.2 ounce elastics for 11 days.
For minimal mandibular anchorageFor minimal mandibular anchorage:: 6 ounce for 10 days6 ounce for 10 days 3 ounce for 11 days.3 ounce for 11 days.
www.indiandentalacademy.com

Anthony A. Gianelly (AJO 1989)Anthony A. Gianelly (AJO 1989)Design: Design:
Nance appliance extends anteriorly to the incisor segment by Nance appliance extends anteriorly to the incisor segment by means of an 0.045-inch wire soldered to the lingual aspect of means of an 0.045-inch wire soldered to the lingual aspect of the premolars. The acrylic component is placed against both the the premolars. The acrylic component is placed against both the palatal vault and the incisors.palatal vault and the incisors.
Bilateral distal extensions (0.045-inch wire) with loops at the Bilateral distal extensions (0.045-inch wire) with loops at the end are soldered to the labial aspect of the premolar bands so end are soldered to the labial aspect of the premolar bands so that the loops approximate the molar tubes. that the loops approximate the molar tubes.
Anchoring the modified Nance appliance to the first premolar Anchoring the modified Nance appliance to the first premolar encourages the distal drift of the second premolars that encourages the distal drift of the second premolars that normally occurs as first molars are moved posteriorly.normally occurs as first molars are moved posteriorly.
REPELLING MAGNETSREPELLING MAGNETS
www.indiandentalacademy.com

The modified Nance appliance serves two The modified Nance appliance serves two functions:functions:
Activation of the magnetsActivation of the magnets Contains the reaction force arising from the action Contains the reaction force arising from the action
of the magnets.of the magnets.
Molars were moved distally 2.0 mm while the Molars were moved distally 2.0 mm while the premolars moved anteriorly 2.1 mm.premolars moved anteriorly 2.1 mm.
When 2When 2ndnd molars were not present, the fastest molars were not present, the fastest molar movement was observed and Class I molar molar movement was observed and Class I molar relationships were attained within 2 to 5 months. relationships were attained within 2 to 5 months. Disadvantages :Disadvantages :
Magnets tend to be expensive and bulky.Magnets tend to be expensive and bulky. Magnetic force dissipates rapidly with increasing Magnetic force dissipates rapidly with increasing
intermagnet distance.intermagnet distance. Requires frequent recall reactivation appointment.Requires frequent recall reactivation appointment. Because of these drawbacks, Darendeliler has Because of these drawbacks, Darendeliler has
concluded that magnets concluded that magnets offer no advantage over offer no advantage over conventionalconventional systems in molar distalization. systems in molar distalization.
www.indiandentalacademy.com

PENDULUM APPLIANCEPENDULUM APPLIANCEJAMES J. HILGERS, JCO 1992JAMES J. HILGERS, JCO 1992
The Pendulum Appliance is a The Pendulum Appliance is a hybrid that uses a large Nance hybrid that uses a large Nance acrylic button in the palate for acrylic button in the palate for anchorage, along with .032" anchorage, along with .032" TMA springs that deliver a light, TMA springs that deliver a light, continuous force to the upper continuous force to the upper first molars without affecting first molars without affecting the palatal button. Thus, the the palatal button. Thus, the appliance produces a broad, appliance produces a broad, swinging arc— or pendulum— swinging arc— or pendulum— of force from the midline of the of force from the midline of the palate to the upper molars.palate to the upper molars.
www.indiandentalacademy.com

FabricationFabrication The right and left Pendulum The right and left Pendulum
springs, formed from .032" springs, formed from .032" TMA wire, consist of a TMA wire, consist of a recurved molar insertion wire, recurved molar insertion wire, a small horizontal adjustment a small horizontal adjustment loop, a closed helix, and a loop loop, a closed helix, and a loop for retention in the acrylic for retention in the acrylic button.button.
The springs are extended as The springs are extended as close to the center of the close to the center of the palatal button as possible to palatal button as possible to maximize their range of maximize their range of motion, to allow for easier motion, to allow for easier insertion into the lingual insertion into the lingual sheaths, and to reduce forces sheaths, and to reduce forces to an acceptable range. to an acceptable range.
www.indiandentalacademy.com

The anterior portion of the appliance can be retained The anterior portion of the appliance can be retained in place with occlusally bonded rests or soldered to in place with occlusally bonded rests or soldered to bands on either the deciduous molars or the first and bands on either the deciduous molars or the first and second bicuspids.second bicuspids.
The Nance button should be made as large as possible The Nance button should be made as large as possible
to prevent any tissue impingement. It should extend to to prevent any tissue impingement. It should extend to about 5mm from the teeth, to avoid the highly vascular about 5mm from the teeth, to avoid the highly vascular cuff of tissue near the teeth and to allow adequate cuff of tissue near the teeth and to allow adequate hygiene.hygiene.
If expansion of the upper arch is needed, a midpalatal If expansion of the upper arch is needed, a midpalatal jackscrew can be incorporated into the center of the jackscrew can be incorporated into the center of the Nance button . The screw is activated one-quarter turn Nance button . The screw is activated one-quarter turn every three days, after a week or so for patient every three days, after a week or so for patient adjustment, to produce a slow, stable expansion.adjustment, to produce a slow, stable expansion.
This version of the appliance is called a "This version of the appliance is called a "Pend-X".Pend-X".www.indiandentalacademy.com

Preactivation and PlacementPreactivation and Placement The springs should be bent The springs should be bent parallelparallel to the midline of the to the midline of the
palate. About one-third of this overactivation is lost in palate. About one-third of this overactivation is lost in placement, and the remaining pressure is tolerated easily placement, and the remaining pressure is tolerated easily by the patient.by the patient.
Once the appliance is cemented in place, each Pendulum Once the appliance is cemented in place, each Pendulum spring is brought forward with finger pressure, the mesial spring is brought forward with finger pressure, the mesial end of the recurved loop is grasped with a Weingart plier end of the recurved loop is grasped with a Weingart plier and the spring is seated in the lingual sheath. . Distal and the spring is seated in the lingual sheath. . Distal pressure holds the spring in the sheath quite effectively, pressure holds the spring in the sheath quite effectively, but an elastic "O" ring can be used to secure it.but an elastic "O" ring can be used to secure it.
www.indiandentalacademy.com

A. As the molar is driven distally, it moves on an arc toward A. As the molar is driven distally, it moves on an arc toward the midline of the appliance— in other words, toward the midline of the appliance— in other words, toward crossbite. crossbite.
B. This tendency can be counteracted by opening the B. This tendency can be counteracted by opening the adjustment loop slightly to increase the expansion and molar adjustment loop slightly to increase the expansion and molar rotation.rotation.
Distal root tip can also be produced by adjusting this Distal root tip can also be produced by adjusting this horizontal loop on the Pendulum spring. Tipping back the horizontal loop on the Pendulum spring. Tipping back the recurved portion of the spring at the loop causes a more direct recurved portion of the spring at the loop causes a more direct distal movement of the molars.distal movement of the molars.
www.indiandentalacademy.com

Reactivation Reactivation The spring is reactivated The spring is reactivated
by pushing the centre of by pushing the centre of helix distally toward the helix distally toward the midline with a bird beak midline with a bird beak plier. plier. StabilizationStabilization
Molars must be stabilized Molars must be stabilized in their new distalized in their new distalized positions or they will positions or they will rapidly drift back mesially. rapidly drift back mesially. It is also important to It is also important to move the buccal segments move the buccal segments into a Class I relationship into a Class I relationship to harness the full to harness the full advantages of the advantages of the appliance.appliance.
www.indiandentalacademy.com

The molars can be The molars can be stabilized stabilized in any of four ways:in any of four ways: The Nance portion is removed and a full upper The Nance portion is removed and a full upper
fixed appliance is bonded. An upper utility arch fixed appliance is bonded. An upper utility arch holds the molars back with the incisors as holds the molars back with the incisors as anchorage. anchorage.
After removal of the Pendulum Appliance, a After removal of the Pendulum Appliance, a smaller, easier-to-clean Nance button ("Insta-smaller, easier-to-clean Nance button ("Insta-Nance”) is placed.Nance”) is placed.
The entire upper arch is bonded and a continuous The entire upper arch is bonded and a continuous archwire with omega loops mesial to the upper first archwire with omega loops mesial to the upper first molar tubes is placed. molar tubes is placed.
A headgear is worn.A headgear is worn.Drawbacks of PADrawbacks of PA
The pendulum appliance not only drives the molars The pendulum appliance not only drives the molars distally, there is also a slight lingual tipping.distally, there is also a slight lingual tipping.
Causes the anterior bite to openCauses the anterior bite to open Not very easy to fabricate.Not very easy to fabricate.
www.indiandentalacademy.com

MODIFICATIONS IN PAMODIFICATIONS IN PASCUZZO JCO 1999 NovSCUZZO JCO 1999 Nov
The Modified PendulumThe Modified Pendulum:: M-M-PendulumPendulum
In the original design by In the original design by Hillgers, adjustable loop was Hillgers, adjustable loop was distally oriented to compensate distally oriented to compensate for the tendency toward for the tendency toward crossbite during distalization.crossbite during distalization.
M-Pendulum was designed by M-Pendulum was designed by reversing the loop to the reversing the loop to the mesial to provide bodily mesial to provide bodily movement of both the roots movement of both the roots and crowns of the maxillary and crowns of the maxillary molars, rather than tipping or molars, rather than tipping or rotation. After some rotation. After some distalization has occurred, the distalization has occurred, the loop is reactivated simply by loop is reactivated simply by opening it.opening it.
Hillgers design
M Pendulumwww.indiandentalacademy.com

If the horizontal Pendulum loop is inverted, it If the horizontal Pendulum loop is inverted, it will allow bodily movement of both the roots will allow bodily movement of both the roots and crowns of the maxillary molars. Once distal and crowns of the maxillary molars. Once distal molar movement has occurred, the loop can be molar movement has occurred, the loop can be activated simply by opening it. The activation activated simply by opening it. The activation produces buccal and/or distal uprighting of the produces buccal and/or distal uprighting of the molar roots and thus a true bodily movement molar roots and thus a true bodily movement rather than a simple tipping or rotation.rather than a simple tipping or rotation.
www.indiandentalacademy.com

Before intraoral placement of the appliance,the Before intraoral placement of the appliance,the Pendulum springs are activated to about 40-45° with Pendulum springs are activated to about 40-45° with a Weingart plier, resulting in about 125g of force on a Weingart plier, resulting in about 125g of force on each side. This activation is repeated until the each side. This activation is repeated until the desired distalization of the molars is obtained. desired distalization of the molars is obtained.
The inverted loop should not be adjusted until the The inverted loop should not be adjusted until the spring has deactivated following each phase of spring has deactivated following each phase of distalization. A passive fit of the distal ends of the distalization. A passive fit of the distal ends of the Pendulum springs in the lingual sheaths, with no Pendulum springs in the lingual sheaths, with no distal force applied to the molar crowns, will allow distal force applied to the molar crowns, will allow backward tipping of the molar roots. The terminal backward tipping of the molar roots. The terminal ends of the M-Pendulum springs are straight, rather ends of the M-Pendulum springs are straight, rather than looped as in the original appliance.than looped as in the original appliance.
The Pendulum springs should be activated primarily The Pendulum springs should be activated primarily by a derotational bending of the distal ends, as with by a derotational bending of the distal ends, as with a conventional palatal bar. After distalization is a conventional palatal bar. After distalization is complete, the terminal ends of the springs should be complete, the terminal ends of the springs should be deactivated to allow a passive fit in the lingual molar deactivated to allow a passive fit in the lingual molar sheaths.sheaths.
www.indiandentalacademy.com

SCUZZO JCO 2000 April SCUZZO JCO 2000 April A further modification of the M- A further modification of the M-
Pendulum appliance was made by Pendulum appliance was made by using removable TMA arms that using removable TMA arms that can be reactivated outside the can be reactivated outside the mouth.mouth.Fabrication and ActivationFabrication and ActivationThe modified appliance is The modified appliance is fabricated as follows:fabricated as follows:
Double over two 7-9mm lengths Double over two 7-9mm lengths of .032" TMA wire to form of .032" TMA wire to form bayonets. Attach each bayonet to bayonets. Attach each bayonet to an M-Pendulum arm, either by an M-Pendulum arm, either by using a laser welder or by wrapping using a laser welder or by wrapping .010" ligature wire around the arm .010" ligature wire around the arm and soldering the unit together and soldering the unit together with silver wire and a miniflame. with silver wire and a miniflame.
www.indiandentalacademy.com

Embed each bayonet Embed each bayonet in the soft acrylic in the soft acrylic that will be used to that will be used to form the Nance form the Nance button, producing button, producing sheaths in which to sheaths in which to insert the removable insert the removable armsarms
Activate the arms as Activate the arms as desired on the desired on the working cast working cast
www.indiandentalacademy.com

Place the appliance in the mouth, Place the appliance in the mouth, inserting the terminal ends of the inserting the terminal ends of the arms into the lingual molar band arms into the lingual molar band sheaths sheaths
The removable arms can be The removable arms can be reactivated during treatment reactivated during treatment without debonding and rebonding without debonding and rebonding the occlusal rests of the Nance the occlusal rests of the Nance button. Distal molar movement button. Distal molar movement can then be more precisely can then be more precisely controlled than by opening the controlled than by opening the horizontal loops in the mouth. The horizontal loops in the mouth. The conventional Pendulum or M-conventional Pendulum or M-Pendulum produces about 5mm of Pendulum produces about 5mm of distalization in three to four distalization in three to four months. With the removable months. With the removable arms, distal movement can be arms, distal movement can be continued at a rate of about continued at a rate of about 1.5mm per month for as long as 1.5mm per month for as long as necessary necessary www.indiandentalacademy.com

AdvantagesAdvantages Dramatic reduction in chair time.Dramatic reduction in chair time. Sound biomechanical principles, producing Sound biomechanical principles, producing
more precise and predictable results.more precise and predictable results. Less chance of unwanted side effects.Less chance of unwanted side effects. Easy replacement of Pendulum springs Easy replacement of Pendulum springs
without refabrication of the entire without refabrication of the entire appliance.appliance.
Ability to replace the active arms with Ability to replace the active arms with passive stainless steel auxiliaries after passive stainless steel auxiliaries after distal movement, thus producing a “quick” distal movement, thus producing a “quick” Nance appliance for stabilization.Nance appliance for stabilization.
www.indiandentalacademy.com

STUDIES EVALUATING STUDIES EVALUATING PAPA
Ghosh and. Nanda. (AJO 1996)Ghosh and. Nanda. (AJO 1996)
Friedrich K. Byloff (1997 AO) part 1 Friedrich K. Byloff (1997 AO) part 1 & Part 2& Part 2
Bussick & McNamara, AJO Bussick & McNamara, AJO 2000March2000March
www.indiandentalacademy.com

Ghosh and. NandaGhosh and. Nanda. (AJO 1996) evaluated the effect of . (AJO 1996) evaluated the effect of Hilgers PA on 41 patients , mean age 12 years and 5 Hilgers PA on 41 patients , mean age 12 years and 5 months.months.
After molar distalization was completed and the pendulum After molar distalization was completed and the pendulum appliance removed, a utility arch was placed to prevent appliance removed, a utility arch was placed to prevent relapse.relapse.DENTAL EFFECTDENTAL EFFECTSagittal PlaneSagittal Plane
The correction of the Class II relationship was achieved by The correction of the Class II relationship was achieved by a mean maxillary first molar distalization of 3.37 mm. a mean maxillary first molar distalization of 3.37 mm. Average distal tipping of 8.36°occurred in 1st molar.Average distal tipping of 8.36°occurred in 1st molar.
The second molar teeth were distalized to a mean of 2.27 The second molar teeth were distalized to a mean of 2.27 mm,and tipped distally 11.99°. mm,and tipped distally 11.99°.
There was a statistically significant correlation between the There was a statistically significant correlation between the amount of distalization and the amount of first molar amount of distalization and the amount of first molar tipping.tipping.Vertical planeVertical plane
The vertical change in molar position was insignificant. The vertical change in molar position was insignificant. There was a mean intrusion of 0.47 mm in second molar There was a mean intrusion of 0.47 mm in second molar positionposition
www.indiandentalacademy.com

Transverse planeTransverse plane The transverse width at the maxillary second premolars The transverse width at the maxillary second premolars
increased by 1.95 mm as they drifted distally into a wider increased by 1.95 mm as they drifted distally into a wider part of the arch. part of the arch.
The arc described by the spring during its distal The arc described by the spring during its distal movement causes a mesiobuccal rotation instead of movement causes a mesiobuccal rotation instead of distobuccal rotation. The width between the mesiobuccal distobuccal rotation. The width between the mesiobuccal cusps of the right and left first molar teeth increased by cusps of the right and left first molar teeth increased by 1.40 mm, whereas that between the distobuccal cusps 1.40 mm, whereas that between the distobuccal cusps showed no increase. The second molar teeth also showed showed no increase. The second molar teeth also showed an expansion of 2.33 mm between the mesiobuccal cusps. an expansion of 2.33 mm between the mesiobuccal cusps.
Distalization of the maxillary first molars with this Distalization of the maxillary first molars with this appliance therefore causes appliance therefore causes both distal as well as buccal both distal as well as buccal tippingtipping of the second molars. of the second molars.
The effect of distalization on the maxillary third molars The effect of distalization on the maxillary third molars was extremely variable. No patient showed more than was extremely variable. No patient showed more than half of root formation on the third molar teeth, and only half of root formation on the third molar teeth, and only the crowns were visible in most radiographs. The third the crowns were visible in most radiographs. The third molars showed a net distal tipping of 2.49°, but an molars showed a net distal tipping of 2.49°, but an insignificant amount of horizontal or vertical change in insignificant amount of horizontal or vertical change in position 0.19 mm distalization and 0.22 mm intrusion position 0.19 mm distalization and 0.22 mm intrusion
www.indiandentalacademy.com

Anchorage loss & effect on anterior segmentsAnchorage loss & effect on anterior segments Loss of anchorage was measured at the first Loss of anchorage was measured at the first
premolar teeth. For every millimeter of distal molar premolar teeth. For every millimeter of distal molar movement, the premolar moved mesially 0.75 mm. movement, the premolar moved mesially 0.75 mm.
The overjet increased by 1.30 mm and the overbite The overjet increased by 1.30 mm and the overbite decreased by 1.39 mm as a result of treatment. The decreased by 1.39 mm as a result of treatment. The maxillary central incisor was proclined an average of maxillary central incisor was proclined an average of 2.40° relative to the SN line.2.40° relative to the SN line.
The upper lip protruded 0.31 mm and the lower lip The upper lip protruded 0.31 mm and the lower lip protruded 0.95 mm relative to the E plane. protruded 0.95 mm relative to the E plane. Effect of eruption of the maxillary second molarEffect of eruption of the maxillary second molar
There were no statistically significant differences in There were no statistically significant differences in maxillary first molar movement, as well as anchorage maxillary first molar movement, as well as anchorage loss between the group of 18 patients who had loss between the group of 18 patients who had erupted maxillary second molars and the 23 who did erupted maxillary second molars and the 23 who did not, indicating that the eruption of maxillary second not, indicating that the eruption of maxillary second molars had molars had minimal effectminimal effect on first molar on first molar distalization.distalization.
www.indiandentalacademy.com

Skeletal effects with the pendulum appliance :Skeletal effects with the pendulum appliance : The pendulum appliance caused insignificant The pendulum appliance caused insignificant
changes in the cant of the palatal and occlusal changes in the cant of the palatal and occlusal planes. The mandibular plane, on the other planes. The mandibular plane, on the other hand, showed a small backward rotation of hand, showed a small backward rotation of 1.09° with treatment, which caused a 1.09° with treatment, which caused a decrease in the overbite by 1.39 mm. decrease in the overbite by 1.39 mm.
Because there was no vertical change in the Because there was no vertical change in the maxillary molar position and only an extrusion maxillary molar position and only an extrusion of 0.5 mm in mandibular first molar position, of 0.5 mm in mandibular first molar position, most of the backward mandibular rotation most of the backward mandibular rotation was caused by distalizing the maxillary molar was caused by distalizing the maxillary molar "into the wedge." The lower anterior face "into the wedge." The lower anterior face height, as a result, increased by 2.79 mm.height, as a result, increased by 2.79 mm.
www.indiandentalacademy.com

Effect based on MPAEffect based on MPA The patients in the sample were arbitrarily The patients in the sample were arbitrarily
divided into three groups, based on their initial divided into three groups, based on their initial Frankfort horizontal to mandibular plane angle Frankfort horizontal to mandibular plane angle (FMA) measurements.(FMA) measurements.
There was a trend for greater increase in FMA There was a trend for greater increase in FMA in group with FMA greater than 25°.in group with FMA greater than 25°.
Patients with high mandibular plane angles Patients with high mandibular plane angles showed posterior mandibular rotation and showed posterior mandibular rotation and increase in lower face height, 4.13 mm as increase in lower face height, 4.13 mm as compared to 1.97 mm in average MPA group. compared to 1.97 mm in average MPA group.
The increase in the lower face height as a The increase in the lower face height as a result of molar distalization, was more than result of molar distalization, was more than double in high angle group (4.13 mm) than in double in high angle group (4.13 mm) than in average group (1.97 mm).average group (1.97 mm).
www.indiandentalacademy.com

Friedrich K. Byloff (1997 AO) part 1Friedrich K. Byloff (1997 AO) part 1 studied, the dental and skeletal effects studied, the dental and skeletal effects of the pendulum appliance, applying of the pendulum appliance, applying 200 to 250 g of force to the molars in 200 to 250 g of force to the molars in 13 patients (age range 8 years to 13 13 patients (age range 8 years to 13 years 5 months) by means of years 5 months) by means of cephalometric radiographs. cephalometric radiographs.
This study suggest that the pendulum This study suggest that the pendulum appliance is effective in moving the appliance is effective in moving the maxillary first molars distally at a mean maxillary first molars distally at a mean monthly rate of 1.02 mm using an monthly rate of 1.02 mm using an initial force of 200 to 250 g in a mean initial force of 200 to 250 g in a mean period of 4 months. period of 4 months.
www.indiandentalacademy.com

Distal molar movement, molar and incisor tipping:Distal molar movement, molar and incisor tipping: The pendulum appliance produces 3.39 mm ±1.25 The pendulum appliance produces 3.39 mm ±1.25
mm distal molar movement with a mean bimolar mm distal molar movement with a mean bimolar intrusion of 1.17 mm ± 1.29 mm. This positive finding intrusion of 1.17 mm ± 1.29 mm. This positive finding can be related to prevention of dentoalveolar vertical can be related to prevention of dentoalveolar vertical growth by the rigid bonded appliance.growth by the rigid bonded appliance.
Molar distal tipping of 14.5° ± 8.33° occurred. The Molar distal tipping of 14.5° ± 8.33° occurred. The trajectory of the TMA springs may account for the trajectory of the TMA springs may account for the excessive tipping found in this study. excessive tipping found in this study.
Maxillary expansion is possible for transverse Maxillary expansion is possible for transverse deficiencies in combination with distal molar deficiencies in combination with distal molar movement.movement.
The pendulum appliance does not create dental or The pendulum appliance does not create dental or skeletal bite opening. skeletal bite opening.
Anchorage loss:Anchorage loss: Second premolar anchorage loss Second premolar anchorage loss found in this study was 1.63 mm (±1.37 mm) i.e. found in this study was 1.63 mm (±1.37 mm) i.e. 29 29 %.%. Distal molar movement represented 71% of the Distal molar movement represented 71% of the space opened between molars and premolars. Incisor space opened between molars and premolars. Incisor anchorage loss was minimalanchorage loss was minimal
www.indiandentalacademy.com

Friedrich K. Byloff (1997 AO) part IIFriedrich K. Byloff (1997 AO) part II In this study, the appliance was modified by In this study, the appliance was modified by
incorporating an uprighting bend into the incorporating an uprighting bend into the distalizing spring during the second phase of distalizing spring during the second phase of treatment to avoid excessive distal tipping of treatment to avoid excessive distal tipping of the maxillary molars. the maxillary molars.
Treatment changes were analyzed and Treatment changes were analyzed and compared with the previous study. compared with the previous study.
Due to the initial moderate dental transverse Due to the initial moderate dental transverse deficiency, 8 of the patients required maxillary deficiency, 8 of the patients required maxillary expansion of 2 to 4 mm.expansion of 2 to 4 mm.Appliance design and activation:Appliance design and activation:
The major difference was the incorporation of The major difference was the incorporation of the molar uprighting bends. An expansion screw the molar uprighting bends. An expansion screw was added to the PA in 8 of the subjects who was added to the PA in 8 of the subjects who required 2 to 4 mm of transverse development; required 2 to 4 mm of transverse development; the appliance was activated every seventh day the appliance was activated every seventh day to achieve a slow rate of expansion. to achieve a slow rate of expansion.
www.indiandentalacademy.com

Active treatment in this study, contrary to the previous Active treatment in this study, contrary to the previous one, consisted of one, consisted of two phases.two phases.
1. Distal molar 1. Distal molar crown movementcrown movement: Molar distalization was : Molar distalization was done until an overcorrected Class I relationship was done until an overcorrected Class I relationship was obtained. obtained.
2. Molar 2. Molar root up rightingroot up righting: The appliance was modified by : The appliance was modified by adding a bend to the spring design to upright the molars adding a bend to the spring design to upright the molars by moving the roots distally. In order to make the by moving the roots distally. In order to make the uprighting bends, the angle between the recurved end of uprighting bends, the angle between the recurved end of the spring, which is engaged into the palatal molar the spring, which is engaged into the palatal molar sheaths, and the long arm of the spring was increased sheaths, and the long arm of the spring was increased intraorally in the sagittal plane intraorally in the sagittal plane 10° to 15°,10° to 15°, using a using a Weingart plier. The moment created was expected to Weingart plier. The moment created was expected to upright the molars. The springs were left slightly active in upright the molars. The springs were left slightly active in the sagittal plane to maintain the position of the molar the sagittal plane to maintain the position of the molar crowns. The appliance was left in place until the molar crowns. The appliance was left in place until the molar crown seemed to be sufficiently uprighted.crown seemed to be sufficiently uprighted.www.indiandentalacademy.com

Treatment timeTreatment time Mean total experimental time using the PA was 27.25 ± Mean total experimental time using the PA was 27.25 ±
7.12 weeks (6 months 3 weeks ± 7 weeks). 7.12 weeks (6 months 3 weeks ± 7 weeks). 1st phase of treatment, ( obtaining a super Class I 1st phase of treatment, ( obtaining a super Class I
relationship) the distal movement phase, took 16.45 ± relationship) the distal movement phase, took 16.45 ± 6.67 weeks.6.67 weeks.
2nd phase -- to upright the maxillary molars required 2nd phase -- to upright the maxillary molars required another 10.9 weeks. another 10.9 weeks.
Thus the total treatment time was increased by 64.1%. Thus the total treatment time was increased by 64.1%. Distal molar movement & molar tipping:Distal molar movement & molar tipping:
The percentage of molar movement compared with total The percentage of molar movement compared with total space opening decreased from 70.92 % to 64.16. space opening decreased from 70.92 % to 64.16.
Rate of movement was between 0.69 mm ± 0.29 mm Rate of movement was between 0.69 mm ± 0.29 mm and 1.20 mm ± 0.74 mm per month, depending on the and 1.20 mm ± 0.74 mm per month, depending on the rate of uprighting. rate of uprighting.
For 6.07° ± 5.15° of final molar tipping, rate of For 6.07° ± 5.15° of final molar tipping, rate of movement was 0.69 mm ± 0.29 mm per month.movement was 0.69 mm ± 0.29 mm per month.
During the uprighting phase, the average monthly distal During the uprighting phase, the average monthly distal movement of the apex was 1.01 mm ± 0.57 mm.movement of the apex was 1.01 mm ± 0.57 mm.www.indiandentalacademy.com

Second molar eruption stagesSecond molar eruption stages In both study the position of the second molars In both study the position of the second molars
didn’t influence the amount of distal molar didn’t influence the amount of distal molar movement or premolar or incisor anchorage loss. movement or premolar or incisor anchorage loss. Intrusion—extrusionIntrusion—extrusion
Increases in the premolar and incisor extrusion and Increases in the premolar and incisor extrusion and decrease in molar intrusion when compared with decrease in molar intrusion when compared with the first study might be a result of the vertical the first study might be a result of the vertical reactive component of the uprighting bend.reactive component of the uprighting bend.Anchorage lossAnchorage loss
The price for more space opening and distal molar The price for more space opening and distal molar crown movement, and especially for more root crown movement, and especially for more root movement and reduced final tipping of the molars, movement and reduced final tipping of the molars, was increased total treatment time and 0.61 mm was increased total treatment time and 0.61 mm more anchorage loss at the premolars and 0.62 mm more anchorage loss at the premolars and 0.62 mm at the incisor edge level.at the incisor edge level.
The effects of the original pendulum appliance were The effects of the original pendulum appliance were not significantly changednot significantly changed by the incorporation of the by the incorporation of the uprighting bends, although slightly more anchorage uprighting bends, although slightly more anchorage loss was noted on the maxillary incisal edge.loss was noted on the maxillary incisal edge.
www.indiandentalacademy.com

Bussick & McNamara, AJO 2000MarchBussick & McNamara, AJO 2000March Subjects were: Varying facial patterns (high, Subjects were: Varying facial patterns (high,
neutral, and low mandibular plane angles).neutral, and low mandibular plane angles).
Cephalometric radiographs obtained from 13 Cephalometric radiographs obtained from 13 practitioners were used to document the practitioners were used to document the treatment of 101 patients (45 boys and 56 treatment of 101 patients (45 boys and 56 girls).girls).
The relative effect of erupted maxillary The relative effect of erupted maxillary second molars on distalization of the first second molars on distalization of the first molar and the effects, if any, of permanent molar and the effects, if any, of permanent versus deciduous dentition based anchorage versus deciduous dentition based anchorage on distalization of maxillary molars were also on distalization of maxillary molars were also evaluated.evaluated.
Treatment with a pendulum/pendex Treatment with a pendulum/pendex appliance, similar to the type described by appliance, similar to the type described by Hilgers,was initiated in all patients Hilgers,was initiated in all patients
www.indiandentalacademy.com

Treatment effectsTreatment effects::1. An increase in overjet was shown.1. An increase in overjet was shown.2. The average maxillary first molar distalization was 5.7 mm, 2. The average maxillary first molar distalization was 5.7 mm, with a distal tipping of 10.6°. with a distal tipping of 10.6°. The maxillary first molars intruded 0.7 mm, and the first The maxillary first molars intruded 0.7 mm, and the first premolars extruded 1.0 mm. premolars extruded 1.0 mm.
The maxillary molar distalization contributed to 76% of the total The maxillary molar distalization contributed to 76% of the total space opening anterior to the maxillary first molar, whereas 24% space opening anterior to the maxillary first molar, whereas 24% was due to reciprocal anchorage loss of the maxillary premolars.was due to reciprocal anchorage loss of the maxillary premolars. 3. 3. Anchor teethAnchor teeth
Second premolar moved mesially by the 1.8-mm with a mesial Second premolar moved mesially by the 1.8-mm with a mesial tipping of 1.5°.tipping of 1.5°.
The maxillary central incisors proclined slightly during treatment.The maxillary central incisors proclined slightly during treatment.
4. 4. Second deciduous molars vs second premolar anchorageSecond deciduous molars vs second premolar anchorage :: A. The reduction in overbite was significantly greater in the A. The reduction in overbite was significantly greater in the
second premolar group (average –1.5mm) than in the second second premolar group (average –1.5mm) than in the second deciduous molar group (average –0.3mm).deciduous molar group (average –0.3mm).
B. Patients with erupted second premolars demonstrated B. Patients with erupted second premolars demonstrated significantly greater increases in lower anterior facial height (2.4 significantly greater increases in lower anterior facial height (2.4 ± 1.3 mm) than did second deciduous molars (1.6 ± 1.5 mm).± 1.3 mm) than did second deciduous molars (1.6 ± 1.5 mm).
These changes are related to a downward and backward rotation These changes are related to a downward and backward rotation of the mandible.of the mandible. www.indiandentalacademy.com

5. Presence or Absence of Erupted 5. Presence or Absence of Erupted Permanent Maxillary Second MolarsPermanent Maxillary Second Molars
1. No significant differences were noted in 1. No significant differences were noted in the anteroposterior movement of the the anteroposterior movement of the maxillary first molar and sagittal anchorage maxillary first molar and sagittal anchorage loss between the 57 patients who had loss between the 57 patients who had erupted maxillary second molars and the erupted maxillary second molars and the 44who had not. 44who had not.
2. In patients with erupted maxillary second 2. In patients with erupted maxillary second molars, there was a slightly greater molars, there was a slightly greater increase in lower anterior face height and increase in lower anterior face height and in the mandibular plane angle and a slightly in the mandibular plane angle and a slightly greater decrease in overbite in comparison greater decrease in overbite in comparison to patients with unerupted second molars.to patients with unerupted second molars.
www.indiandentalacademy.com

6. Variation in Facial Patterns6. Variation in Facial Patterns:: Lower anterior facial height increased 2.2 mm; Lower anterior facial height increased 2.2 mm;
there was there was no significant differenceno significant difference in lower in lower anterior facial height increase between anterior facial height increase between patients of high, neutral, or low mandibular patients of high, neutral, or low mandibular plane angles.plane angles.
For maximum maxillary first molar distalization For maximum maxillary first molar distalization with minimal increase in lower anterior facial with minimal increase in lower anterior facial height, this appliance appears to be height, this appliance appears to be best used best used on patients with maxillary second deciduous on patients with maxillary second deciduous molars for anchorage and the absence of molars for anchorage and the absence of erupted permanent maxillary second molarserupted permanent maxillary second molars, , although significant bite opening was not of although significant bite opening was not of major concern in any patient in the study.major concern in any patient in the study.
www.indiandentalacademy.com

Distalization appliances based on Distalization appliances based on NiTi wires and coilsNiTi wires and coils
Superelastic coilsSuperelastic coils
Superelastic archwire: single Superelastic archwire: single looped,looped,
double loopeddouble looped
www.indiandentalacademy.com

1. SUPER ELASTIC NiTi COILS1. SUPER ELASTIC NiTi COILS Anthony A. Gianelly (AJO 1991) used Japanese Anthony A. Gianelly (AJO 1991) used Japanese
NiTi super elastic coils, exerting 100 gm of NiTi super elastic coils, exerting 100 gm of force, compressed against the maxillary first force, compressed against the maxillary first molars and moved the molars distally 1 to 1.5 molars and moved the molars distally 1 to 1.5 mm/month.mm/month.
Coils are used in conjunction with a vertically Coils are used in conjunction with a vertically slotted (0.020-inch) fixed appliance.slotted (0.020-inch) fixed appliance.
A passive 0.016 ´ 0.22-inch wire with stops A passive 0.016 ´ 0.22-inch wire with stops that abut the distal wings of the premolar that abut the distal wings of the premolar brackets is inserted to ensure that the wire brackets is inserted to ensure that the wire cannot move past the first premolars, thus cannot move past the first premolars, thus placing the reaction force on the Nance placing the reaction force on the Nance appliance. Coils are placed on the wire appliance. Coils are placed on the wire between the first premolars and the molars.between the first premolars and the molars.
The coils are activated 8 to 10 mm by The coils are activated 8 to 10 mm by compressing and maintaining them against the compressing and maintaining them against the molars by crimpable hooks or Gurin locks.molars by crimpable hooks or Gurin locks.
www.indiandentalacademy.com

AnchorageAnchorage A Nance-type appliance was cemented onto the first A Nance-type appliance was cemented onto the first
premolars. The appliance extends from the incisors to premolars. The appliance extends from the incisors to the molar area and a bite plate is added to the incisal the molar area and a bite plate is added to the incisal portion to disclude the posterior teeth slightlyportion to disclude the posterior teeth slightlyAnchorage enhancement:Anchorage enhancement:
To enhance anchorage further, a 0.018-inch To enhance anchorage further, a 0.018-inch uprighting spring is placed in the vertical slot of the uprighting spring is placed in the vertical slot of the premolar brackets, directing the crowns distally.premolar brackets, directing the crowns distally.
Class II mechanics are used only when anchorage loss Class II mechanics are used only when anchorage loss is at least 1 mm. is at least 1 mm.
When Class II elastics are attached, a rectangular wire When Class II elastics are attached, a rectangular wire with 10° of incisor lingual root torque is inserted in with 10° of incisor lingual root torque is inserted in the mandibular arch to maintain lower incisor position. the mandibular arch to maintain lower incisor position.
100 gm superelastic coils can be used successfully in 100 gm superelastic coils can be used successfully in patients with Class II malocclusions to move molars patients with Class II malocclusions to move molars posteriorly at the rate of 1 to 1.5 mm/month with little posteriorly at the rate of 1 to 1.5 mm/month with little or no cooperation from the patient.or no cooperation from the patient.
www.indiandentalacademy.com

SUPER ELASTIC NiTi WIRESSUPER ELASTIC NiTi WIRES The use of shape memory, superelastic Nickel The use of shape memory, superelastic Nickel
Titanium wires inTitanium wires in distalizing the molars have been discussed by Ranieri distalizing the molars have been discussed by Ranieri
& Antony A.Gianelly in 1992.JCO& Antony A.Gianelly in 1992.JCOFABRICATION FABRICATION
Gianelly used a superelastic NiTi arch wire here.Gianelly used a superelastic NiTi arch wire here. 1. A 100 gm Neosentalloy wire with regular arch form 1. A 100 gm Neosentalloy wire with regular arch form
is placed over the maxillary arch. The superelastic is placed over the maxillary arch. The superelastic NiTi wire is an 0.018 X 0.025 inch wire that also NiTi wire is an 0.018 X 0.025 inch wire that also applies 100 gm of force.applies 100 gm of force.
The wire is then marked in three places on each side.The wire is then marked in three places on each side. A. At the distal wing of the first premolar bracket.A. At the distal wing of the first premolar bracket. B. 5-7 mm distal to the anterior opening of the buccal B. 5-7 mm distal to the anterior opening of the buccal
tubetube C. Between the lateral incisors and canines C. Between the lateral incisors and canines
www.indiandentalacademy.com

A stop is then crimped on the arch wire at each of the A stop is then crimped on the arch wire at each of the posterior marks and a hook is then added for inter-posterior marks and a hook is then added for inter-maxillary elastics between the lateral incisors and canines.maxillary elastics between the lateral incisors and canines.3. The wire is then inserted into the molar tube until the 3. The wire is then inserted into the molar tube until the posterior stop abuts the tube.posterior stop abuts the tube.
To place the wire through the first premolar bracket, the To place the wire through the first premolar bracket, the anterior stop is grasped and the wire gently forced distally anterior stop is grasped and the wire gently forced distally so that the stop abuts the distal wing of the first premolar so that the stop abuts the distal wing of the first premolar bracket, when ligated.bracket, when ligated.
Since the wire is 5-7 mm longer than the available space, Since the wire is 5-7 mm longer than the available space, the excess will be deflected gingivally into the buccal fold. the excess will be deflected gingivally into the buccal fold.
www.indiandentalacademy.com

ACTION OF THE WIRE/APPLIANCEACTION OF THE WIRE/APPLIANCE The distalization of the molars occur as the wire returns to its The distalization of the molars occur as the wire returns to its
original shape, exerting a distal force of 100 gms against the original shape, exerting a distal force of 100 gms against the molars and a reactionary mesial force on the first premolars, molars and a reactionary mesial force on the first premolars, canines and incisors.canines and incisors.
There is also a tendency for the premolars to move buccally.There is also a tendency for the premolars to move buccally.THE ANCHORAGETHE ANCHORAGEThe anchorage can be controlled byThe anchorage can be controlled by
a. Placing a 100-150 gm class II elastics against the first a. Placing a 100-150 gm class II elastics against the first premolars. (or)premolars. (or)
b. Placement of hooks between the lateral incisors and b. Placement of hooks between the lateral incisors and canines (or)canines (or)
c. A Nance appliance cemented to the first premolars.c. A Nance appliance cemented to the first premolars.www.indiandentalacademy.com

THE ADVANTAGE OF THE THE ADVANTAGE OF THE APPLIANCEAPPLIANCE
1. The appliance distalizes the molar 1. The appliance distalizes the molar at the rate of 1-2 mm per month with at the rate of 1-2 mm per month with little loss of anchorage.little loss of anchorage.
2. The Neosentalloy wire is easy to 2. The Neosentalloy wire is easy to insert even after all teeth have been insert even after all teeth have been bracketed or banded.bracketed or banded.
www.indiandentalacademy.com

Giancotti, & Cozza (JCO 1998 April) used Giancotti, & Cozza (JCO 1998 April) used double double looploop for simultaneous distalization of both molarsfor simultaneous distalization of both molars
Superelastic nickel titanium wires have been found Superelastic nickel titanium wires have been found as effective as other means in producing distal as effective as other means in producing distal movement of the maxillary first molars. When the movement of the maxillary first molars. When the distalization is carried out before the second molars distalization is carried out before the second molars have erupted, it can reliably produce 1-2mm of have erupted, it can reliably produce 1-2mm of space. Once the second molars have erupted, space. Once the second molars have erupted, however, the distal movement can be more difficult however, the distal movement can be more difficult and time-consuming, and loss of anchorage is likely. and time-consuming, and loss of anchorage is likely.
Author used Nickel Titanium Double-Loop System Author used Nickel Titanium Double-Loop System for Simultaneous distalization of First and Second for Simultaneous distalization of First and Second Molars.Molars.
Appliance DesignAppliance Design The mandibular first and second molars and second The mandibular first and second molars and second
bicuspids are banded, and the remaining mandibular bicuspids are banded, and the remaining mandibular teeth are bonded. A lip bumper is placed to prevent teeth are bonded. A lip bumper is placed to prevent any extrusion from the use of Class II elastics.any extrusion from the use of Class II elastics.
The maxillary molars and bicuspids are banded, and The maxillary molars and bicuspids are banded, and the anterior teeth are bonded the anterior teeth are bonded
www.indiandentalacademy.com

An 80g NeoSentalloy An 80g NeoSentalloy archwire (regular archwire (regular mandibularmandibular archform) is archform) is placed on the maxillary arch placed on the maxillary arch and marked distal to the first and marked distal to the first bicuspid bracket and about bicuspid bracket and about 5mm distal to the first molar 5mm distal to the first molar tube . Stops are then tube . Stops are then crimped in the archwire at crimped in the archwire at each mark (distal to 4 and 6)each mark (distal to 4 and 6)
Two sectional nickel Two sectional nickel titanium archwires (one for titanium archwires (one for each side) are prepared by each side) are prepared by crimping stops distal and crimping stops distal and mesial to the second mesial to the second bicuspids and about 5mm bicuspids and about 5mm distal to each second molar distal to each second molar tube.tube.
Uprighting springs are Uprighting springs are inserted into the vertical inserted into the vertical slots of the first bicuspid and slots of the first bicuspid and Class II elastics are placedClass II elastics are placed
www.indiandentalacademy.com

JONES JIG APPLINCEJONES JIG APPLINCE Introduced by Jones & White in 1992.Introduced by Jones & White in 1992. Jones Jig uses an open-coil nickel titanium spring to Jones Jig uses an open-coil nickel titanium spring to
deliver 70-75g of force, over a compression range of 1-deliver 70-75g of force, over a compression range of 1-5mm, to the molars.5mm, to the molars.Appliance FabricationAppliance Fabrication
A modified Nance appliance provides anchorage for the A modified Nance appliance provides anchorage for the use of the Jones Jig. use of the Jones Jig. Modification in Nance:Modification in Nance:
It can be attached to the first bicuspids, second bicuspids, It can be attached to the first bicuspids, second bicuspids, or deciduous second molars. or deciduous second molars. The appointment sequence is as follows:The appointment sequence is as follows:
Appointment 1 : Separators are placed between the first Appointment 1 : Separators are placed between the first molars and the anchor teeth.molars and the anchor teeth.
Appointment 2 :Impression is made with bands. Pour the Appointment 2 :Impression is made with bands. Pour the impression with the bands in stone.impression with the bands in stone.A .036" stainless steel wire is adapted to the palate on the A .036" stainless steel wire is adapted to the palate on the cast, extending it as far as the canines, and soldered to cast, extending it as far as the canines, and soldered to the anchor bands.the anchor bands. www.indiandentalacademy.com

The Jones Jig assembly consists of a mainframe of two The Jones Jig assembly consists of a mainframe of two prescriptions (0.018 & 0.22 inches respectively), which can prescriptions (0.018 & 0.22 inches respectively), which can be contoured in the anterior one third. It also consists of a be contoured in the anterior one third. It also consists of a mainframe hook which is tied to the hook of the molar tube. mainframe hook which is tied to the hook of the molar tube. The force is delivered by a Nickel Titanium coil spring, The force is delivered by a Nickel Titanium coil spring, which acts along the mainframe wire, when activated using which acts along the mainframe wire, when activated using a ligature. A 0.014 inch ligature wire is generally used to a ligature. A 0.014 inch ligature wire is generally used to fasten the eyelet tube to the premolar bracket, which fasten the eyelet tube to the premolar bracket, which compresses the NiTi coil springs. The distal end of the compresses the NiTi coil springs. The distal end of the mainframe consists of a keeper wire (0.018 inch) which mainframe consists of a keeper wire (0.018 inch) which goes into the archwire slot and a mainframe wire which goes into the archwire slot and a mainframe wire which enters the head gear slot of the molar tube. The extreme enters the head gear slot of the molar tube. The extreme mesial end of the completed assembly should rest no mesial end of the completed assembly should rest no further than the distal 1/3rd of the bicuspid. further than the distal 1/3rd of the bicuspid.
www.indiandentalacademy.com

ACTIVATIONACTIVATION A 0.014 inch ligature wire is wound around the buccal A 0.014 inch ligature wire is wound around the buccal
tube and the mainframe hook very lightly. Then a 0.012 tube and the mainframe hook very lightly. Then a 0.012 inch-ligature wire is wound twice around the premolar inch-ligature wire is wound twice around the premolar bracket and the mesial end passed through the eyelet bracket and the mesial end passed through the eyelet tube. The ligature wire is then tightened until 'light' tube. The ligature wire is then tightened until 'light' through the middle of the open coil is barely seen.through the middle of the open coil is barely seen.
Bunching or over activation of the coil spring should Bunching or over activation of the coil spring should the avoided as it can lead to unwanted tipping and the avoided as it can lead to unwanted tipping and palatal irritation along the palatal button.palatal irritation along the palatal button.
Although the force of the Jones Jig is applied in a Class Although the force of the Jones Jig is applied in a Class I direction, the appliance may be contraindicated in I direction, the appliance may be contraindicated in cases of extreme vertical growth patterns, because cases of extreme vertical growth patterns, because extrusion of the molars is not restricted.extrusion of the molars is not restricted.REACTIVATIONREACTIVATION
Reactivation takes very little chair time and is due over Reactivation takes very little chair time and is due over a period or four to five week intervals.a period or four to five week intervals.
www.indiandentalacademy.com

TREATMENT TIMETREATMENT TIME In Pseudo class II where it is the rotated class In Pseudo class II where it is the rotated class
I which needs to be corrected, the treatment I which needs to be corrected, the treatment time is 90-120 days.time is 90-120 days.
In true class II molar relationships, the In true class II molar relationships, the corrected class I relationship can be achieved corrected class I relationship can be achieved in 120-180 days. However the treatment time in 120-180 days. However the treatment time is slightly increased in brachyfacial patterns.is slightly increased in brachyfacial patterns.Drawback:Drawback:
The use of the Nance appliance causes The use of the Nance appliance causes palatal tissue impingement.palatal tissue impingement.
Laboratory expense Laboratory expense Extra appointment needed to fit the Nance Extra appointment needed to fit the Nance
appliance.appliance. Coils demand extra diligence in cleaningCoils demand extra diligence in cleaning
www.indiandentalacademy.com

Comparison of Jones jig molar distalization appliance Comparison of Jones jig molar distalization appliance with extraoral tractionwith extraoral tractionSeda Haydar (AJO 2000 Jan)Seda Haydar (AJO 2000 Jan)
20 patients in late mixed dentition period with skeletal 20 patients in late mixed dentition period with skeletal Class I or slight Class II malocclusions, with dental Class I or slight Class II malocclusions, with dental Class II relationship were treated with Jones jig and Class II relationship were treated with Jones jig and headgear.headgear.
Ten cases were treated with the Jones jig appliance for Ten cases were treated with the Jones jig appliance for upper molar distalization, and 10 patients used cervical upper molar distalization, and 10 patients used cervical headgear for correction of dental Class II relationship.headgear for correction of dental Class II relationship.
The mean age was 10.6 and 10.7 years, respectively, The mean age was 10.6 and 10.7 years, respectively, for headgear and Jones jig group.for headgear and Jones jig group.
Long cervical face bows were used, and the outer bows Long cervical face bows were used, and the outer bows were parallel to the occlusal plane exerting 600 g of were parallel to the occlusal plane exerting 600 g of force with an average use of 16 hours per day until a force with an average use of 16 hours per day until a Class I molar relationship was reached. Average Class I molar relationship was reached. Average treatment time for distalization with headgear was 10.7 treatment time for distalization with headgear was 10.7 months followed by a fixed appliance phase of 11 months followed by a fixed appliance phase of 11 months.months.
www.indiandentalacademy.com

In the Jones jig group, the spring was activated at 4 In the Jones jig group, the spring was activated at 4 week intervals and 75 g of force was applied because week intervals and 75 g of force was applied because 5 mm of activation was made at each visit. A 5 mm of activation was made at each visit. A modified Nance appliance was used as an anchorage modified Nance appliance was used as an anchorage unit. The average treatment time to move molars unit. The average treatment time to move molars distally was 2.5 months. After distalization of molars, distally was 2.5 months. After distalization of molars, fixed appliance therapy was applied to each patient fixed appliance therapy was applied to each patient and total treatment time was 15.1 months.and total treatment time was 15.1 months.Skeletal change:Skeletal change:
In the In the headgear groupheadgear group the decrease in SNA angle the decrease in SNA angle was found statistically significant, downward tipping was found statistically significant, downward tipping of palatal plane was also found statistically of palatal plane was also found statistically significant.significant.
On the other hand, none of these effects occurred in On the other hand, none of these effects occurred in the the Jones jigJones jig treatment treatment group. group.
In this study, In this study, no increaseno increase was observed in GoGnSN was observed in GoGnSN angle in both groups.angle in both groups.
www.indiandentalacademy.com

Effect on molars and premolarsEffect on molars and premolars In theIn the headgear headgear group, the distalization of maxillary first group, the distalization of maxillary first
molars and maxillary second premolars was a consistent molars and maxillary second premolars was a consistent findingfinding
In the In the Jones jigJones jig group, the distalization and distal tipping group, the distalization and distal tipping of maxillary first molars and mesial movement of of maxillary first molars and mesial movement of premolar occurred.premolar occurred.
Extrusion of maxillary first molars was observed in Extrusion of maxillary first molars was observed in bothboth groups, but it was found statistically significant only in groups, but it was found statistically significant only in Jones jig group.Jones jig group.
Jones jig group, showed mesial tipping of the anchorage Jones jig group, showed mesial tipping of the anchorage unit, this is contrary to the finding in the headgear group unit, this is contrary to the finding in the headgear group in which spontaneous distalization of premolars was in which spontaneous distalization of premolars was observed as a result of the distalization of molar teeth. observed as a result of the distalization of molar teeth. Effect on IncisorsEffect on Incisors
HeadgearHeadgear group, showed the extrusion and retrusion of group, showed the extrusion and retrusion of incisors that might occur as a result of the retraction incisors that might occur as a result of the retraction effect of headgear on anterior teeth.effect of headgear on anterior teeth.
Jones jigJones jig group showed protrusion of the incisors group showed protrusion of the incisors because the incisors were part of the anchorage unitbecause the incisors were part of the anchorage unit
www.indiandentalacademy.com

Average treatment time Average treatment time The average treatment time for molar The average treatment time for molar
correction with headgear and Jones jig was correction with headgear and Jones jig was 10.7 10.7 and 2.5 monthsand 2.5 months, respectively. Because intraoral , respectively. Because intraoral distalization moves molars distally in a very distalization moves molars distally in a very short time, total treatment time is reduced by at short time, total treatment time is reduced by at least 6 to 8 months despite the fact that the least 6 to 8 months despite the fact that the anterior teeth move or tip mesially during molar anterior teeth move or tip mesially during molar correction. Although a distal drift of premolars correction. Although a distal drift of premolars take place during distalization, this does not take place during distalization, this does not reduce the total treatment time because reduce the total treatment time because treatment may cease at times when headgear treatment may cease at times when headgear cooperation is poor.cooperation is poor.
Intraoral distalization seems more appropriate Intraoral distalization seems more appropriate for regaining space for cases in which no for regaining space for cases in which no orthopedic effect is desired on the maxilla as orthopedic effect is desired on the maxilla as with skeletal Class I or borderline Class II with skeletal Class I or borderline Class II patients. patients.
www.indiandentalacademy.com

Brickman, & Nanda ( AJO 2000 NOVBrickman, & Nanda ( AJO 2000 NOV) ) evaluatedevaluated the the effects of the Jones jig appliance on distal movement of effects of the Jones jig appliance on distal movement of maxillary molars and reciprocal effects on premolars maxillary molars and reciprocal effects on premolars and maxillary incisors. and maxillary incisors.
Measurements were made on a matched sample of 35 Measurements were made on a matched sample of 35 patients treated with cervical headgear and compared patients treated with cervical headgear and compared with result of 72 patients treated with Jones jig.with result of 72 patients treated with Jones jig.
Both series of patients were treated to correct an Both series of patients were treated to correct an Angle Class II molar relationship. Angle Class II molar relationship. The results from the Jones jig sample showedThe results from the Jones jig sample showed
Mean maxillary first molar distal movement was 2.51 Mean maxillary first molar distal movement was 2.51 mm & distal tipping of 7.53°. mm & distal tipping of 7.53°.
The mean reciprocal mesial movement of the maxillary The mean reciprocal mesial movement of the maxillary premolar was 2.0 mm and mesial tipping of 4.76°. premolar was 2.0 mm and mesial tipping of 4.76°.
The maxillary first molar extruded 0.14 mm & the The maxillary first molar extruded 0.14 mm & the maxillary premolar extruded 1.88 mmmaxillary premolar extruded 1.88 mm
The maxillary second molars were also moved distally The maxillary second molars were also moved distally 2.02 mm and tipped distally 7.89°.2.02 mm and tipped distally 7.89°.
www.indiandentalacademy.com

The Jones jig sample demonstrated effective The Jones jig sample demonstrated effective distal molar movement and maintenance of distal molar movement and maintenance of the Class I molar relationship. Cervical the Class I molar relationship. Cervical headgear sample showed treatment headgear sample showed treatment results results comparablecomparable with Jones Jig. with Jones Jig.
The longitudinal assessment showed The longitudinal assessment showed significant significant differences differences between the Jones jig between the Jones jig sample and the cervical headgear sample for sample and the cervical headgear sample for lower lip to E-line and SNA. lower lip to E-line and SNA.
1. The Jones jig sample showed a mean 1. The Jones jig sample showed a mean decrease in lower lip to E-line of 0.25 mm decrease in lower lip to E-line of 0.25 mm versus 1.20 mm for the headgear sample. versus 1.20 mm for the headgear sample.
2. SNA decreased 0.40° for the Jones jig 2. SNA decreased 0.40° for the Jones jig sample versus 1.20° for the headgear sample.sample versus 1.20° for the headgear sample.
www.indiandentalacademy.com

DISTAL JET DISTAL JET Distal jet was designed by Aldo Distal jet was designed by Aldo
Carano & Mauro in 1996.Carano & Mauro in 1996.Appliance DesignAppliance Design
Bilateral tubes of .036" internal Bilateral tubes of .036" internal diameter which is attached to diameter which is attached to an acrylic Nance button. an acrylic Nance button.
A NiTi coil spring and a screw-A NiTi coil spring and a screw-clamp are slid over each tube. clamp are slid over each tube.
The wire extending from the The wire extending from the acrylic through each tube ends acrylic through each tube ends in a bayonet bend that is in a bayonet bend that is inserted into the lingual sheath inserted into the lingual sheath of the first molar band. An of the first molar band. An anchor wire from the Nance anchor wire from the Nance button is soldered to bands on button is soldered to bands on the second premolars the second premolars
www.indiandentalacademy.com

Components: Components: 1. The Transpalatal connector – rigidly immobilizes the premolars 1. The Transpalatal connector – rigidly immobilizes the premolars
and provides a support to the Nance button.and provides a support to the Nance button. 2. The bayonet director unit - Lumen of the tube portion supports 2. The bayonet director unit - Lumen of the tube portion supports
the molar bayonet, while its outside diameter supports the spring the molar bayonet, while its outside diameter supports the spring and the activation lock.and the activation lock.
3. The molar bayonet - It is drawn out of the bayonet director unit 3. The molar bayonet - It is drawn out of the bayonet director unit during distalization and inserts into the lingual sheath.during distalization and inserts into the lingual sheath.
4. The Distal stop - Prevents the spring from riding up on the 4. The Distal stop - Prevents the spring from riding up on the vertical arm of the molar bayonet while activation of the vertical arm of the molar bayonet while activation of the appliance.appliance.
5. Nickel titanium springs - Two force ranges - 180 gms and 240 5. Nickel titanium springs - Two force ranges - 180 gms and 240 gms.gms.
6. Activation locks - To compress and activate the springs.6. Activation locks - To compress and activate the springs. 7. Lock wrench - To engage and tighten the screw of the 7. Lock wrench - To engage and tighten the screw of the
activation lockactivation lock
1. TP connector
2. Bayonet director
3. Molar bayonet
6. Activation lock
7. C Res
www.indiandentalacademy.com

Activation:Activation: The Distal Jet is The Distal Jet is
reactivated by sliding the reactivated by sliding the clamp closer to the first clamp closer to the first molar once a month. molar once a month.
Once distalization is Once distalization is complete, the appliance complete, the appliance can be converted to a can be converted to a Nance retainer simply by Nance retainer simply by replacing the clamp-replacing the clamp-spring assemblies with spring assemblies with cold-cure acrylic and cold-cure acrylic and cutting off the arms to cutting off the arms to the premolars.the premolars.
www.indiandentalacademy.com

Advantage of distal jet :Advantage of distal jet : The appliance is relatively easy to fabricate, The appliance is relatively easy to fabricate,
easy to insert, is well tolerated and is easy to insert, is well tolerated and is esthetic.esthetic.
Easy activationEasy activation Ease of conversion to a Nance holding arch Ease of conversion to a Nance holding arch
to maintain the distalized molar positions.to maintain the distalized molar positions. The Distal Jet also permits the simultaneous The Distal Jet also permits the simultaneous
use of full bonded appliances, possibly use of full bonded appliances, possibly avoiding the need for two phases of avoiding the need for two phases of treatment treatment
www.indiandentalacademy.com

distaldistal
www.indiandentalacademy.com

MODIFICATIONS OF DISTAL JETMODIFICATIONS OF DISTAL JET
Bowman (1998 Sept JCO) described several Bowman (1998 Sept JCO) described several modifications to the original appliance. modifications to the original appliance.
Conversion to Nance Holding Arch:Conversion to Nance Holding Arch:Upon completion of molar distalization, the Upon completion of molar distalization, the Distal Jet is converted to a Nance holding arch to Distal Jet is converted to a Nance holding arch to prevent further distal movement and consequent prevent further distal movement and consequent anchorage loss. It can be done by these two anchorage loss. It can be done by these two methods:methods:
1. One way to stop movement of the bayonet 1. One way to stop movement of the bayonet wire through the tube is to flow a light-cured wire through the tube is to flow a light-cured acrylic around the coil spring, over the distal acrylic around the coil spring, over the distal bayonet bend, and over the activation collar to bayonet bend, and over the activation collar to produce a solid extension from the molar bands produce a solid extension from the molar bands to the acrylic button.to the acrylic button.
www.indiandentalacademy.com

2. Wrap an .014" stainless steel ligature wire 2. Wrap an .014" stainless steel ligature wire around the end of the doubled back wire around the end of the doubled back wire (extending distally from the lingual sheath on (extending distally from the lingual sheath on the first molar band) and tie it around the tube the first molar band) and tie it around the tube just mesial to the activation collar. The coil just mesial to the activation collar. The coil spring should be compressed completely and the spring should be compressed completely and the set screw tightened to prevent mesial movement set screw tightened to prevent mesial movement of the molars. of the molars.
www.indiandentalacademy.com

Double -Set -Screw Distal JetDouble -Set -Screw Distal Jet A modification of the Distal Jet A modification of the Distal Jet
incorporating two set screws incorporating two set screws into the activation collar into the activation collar permits an easier, cleaner, and permits an easier, cleaner, and more reliable conversion to a more reliable conversion to a molar Nance holding arch.molar Nance holding arch.
The mesial set screw is used The mesial set screw is used during active distalization .The during active distalization .The distal screw is set on the distal screw is set on the bayonet wire, locking the two bayonet wire, locking the two pieces together to prevent pieces together to prevent molar movement. molar movement.
The premolar supporting wires The premolar supporting wires are sectioned where they enter are sectioned where they enter the acrylic button, using a high-the acrylic button, using a high-speed handpiece and diamond speed handpiece and diamond bur. bur.
The bayonet wire or tube can be The bayonet wire or tube can be bent with a three-prong plier to bent with a three-prong plier to adjust the pressure of theacrylic adjust the pressure of theacrylic button against the palate button against the palate
www.indiandentalacademy.com

Conversion of double-set-screw Distal Jet to Nance holding Conversion of double-set-screw Distal Jet to Nance holding arch:arch: A. Upon completion ofmolar distalization, double-set-screw A. Upon completion ofmolar distalization, double-set-screw activation collar is slid mesially to gain access to coil spring.activation collar is slid mesially to gain access to coil spring.B.Free end of coil spring is grasped with plier. Coil spring is B.Free end of coil spring is grasped with plier. Coil spring is removed by peeling it away from bayonet wire.removed by peeling it away from bayonet wire.C. Distal end of tube, where bayonet wire enters, can now be C. Distal end of tube, where bayonet wire enters, can now be seen.seen.D. Double set-screw collar is slid back to this junction, mesial D. Double set-screw collar is slid back to this junction, mesial set screw is locked on tube, and distal screw is set on bayonet.set screw is locked on tube, and distal screw is set on bayonet.www.indiandentalacademy.com

Quick & Angela Harris (JCO 2000 July)Quick & Angela Harris (JCO 2000 July) The Distal Jet is a fixed palatal appliance that The Distal Jet is a fixed palatal appliance that
is most commonly used to distalize the is most commonly used to distalize the maxillary molars, either unilaterally or maxillary molars, either unilaterally or bilaterally. bilaterally.
DisadvantageDisadvantage of Distal jet: Lies in activation of Distal jet: Lies in activation The appliance is activated by sliding a collar The appliance is activated by sliding a collar
along the supporting tube to compress a coil along the supporting tube to compress a coil spring, then fixing the collar in place by spring, then fixing the collar in place by tightening a small set-screw. tightening a small set-screw.
This procedure is sometimes difficult because This procedure is sometimes difficult because of the small size of the screw, the moisture and of the small size of the screw, the moisture and confined space of the intraoral environment, confined space of the intraoral environment, and food impaction in the screw head. and food impaction in the screw head.
In addition, activation requires the use of a In addition, activation requires the use of a small small Allen wrenchAllen wrench, which has the risk of being , which has the risk of being swallowed or aspirated.swallowed or aspirated.
www.indiandentalacademy.com

Appliance DesignAppliance Design The basis of the modification is The basis of the modification is
the rear entry of the sliding the rear entry of the sliding section into the lingual molar section into the lingual molar sheath, so that the appliance pulls sheath, so that the appliance pulls rather than pushes the molars rather than pushes the molars distally. The doubled-backwire (or distally. The doubled-backwire (or “foot”) is inserted into the lingual “foot”) is inserted into the lingual sheath from the distal. The foot sheath from the distal. The foot should be a little longer than the should be a little longer than the sheath so it can be tied back to sheath so it can be tied back to the sliding section with an the sliding section with an elastomeric or metal ligature. elastomeric or metal ligature.
Either .030" or .032" wire is Either .030" or .032" wire is suitable for the sliding sections. suitable for the sliding sections. Support tubes of corresponding Support tubes of corresponding internal diameter are embedded internal diameter are embedded in the acrylic Nance button. The in the acrylic Nance button. The desired amount of activation is desired amount of activation is achieved by compressing the coil achieved by compressing the coil spring between the distal end of spring between the distal end of the support tube and a stop the support tube and a stop soldered to the sliding wire.soldered to the sliding wire.www.indiandentalacademy.com

To reactivate the appliance, the safety To reactivate the appliance, the safety ligature is cut, the sliding wire is pulled ligature is cut, the sliding wire is pulled out distally, and a new, longer section of out distally, and a new, longer section of coil is placed over the wire. coil is placed over the wire.
In addition, no set-screws or Allen In addition, no set-screws or Allen wrenches are used, simplifying the wrenches are used, simplifying the activation procedure. activation procedure.
After molar distalization is completed, After molar distalization is completed, the molar positions are held by replacing the molar positions are held by replacing the open coils with either closed coils or the open coils with either closed coils or solid tubing to prevent anterior relapse solid tubing to prevent anterior relapse or a new Nance button can be made.or a new Nance button can be made.
www.indiandentalacademy.com

The appliance was described by The appliance was described by Raphael U.Greenfield in 1997.Raphael U.Greenfield in 1997.
The appliance proposed to achieve The appliance proposed to achieve distal bodily movement of the molars distal bodily movement of the molars without tipping the crown with no without tipping the crown with no loss of posterior anchorage.loss of posterior anchorage.
THE APPLIANCETHE APPLIANCEThe components of the appliance The components of the appliance are:are:
a. Maxillary first molar and first a. Maxillary first molar and first bicuspid bands.bicuspid bands.
b. 0.036" stainless steel tubing b. 0.036" stainless steel tubing (soldered to the bicuspids).(soldered to the bicuspids).
c.0.030" stainless steel wires c.0.030" stainless steel wires (soldered to the first molar).(soldered to the first molar).
d. Enlarged Nance button reinforced d. Enlarged Nance button reinforced with an 0.040" stainless steel wire with an 0.040" stainless steel wire for control of anterior anchorage.for control of anterior anchorage.
e. 0.055" hyperplastic nickel e. 0.055" hyperplastic nickel titanium open-coil springs - to titanium open-coil springs - to provide a light but continuous force.provide a light but continuous force.
THE FIXED PISTON APPLIANCETHE FIXED PISTON APPLIANCE
www.indiandentalacademy.com

FabricationFabrication 1. The first molars are banded 1. The first molars are banded
with a double or triple tube.with a double or triple tube. 2. The first / second bicuspids are 2. The first / second bicuspids are
then banded. Normally the buccal then banded. Normally the buccal and lingual piston assemblies and lingual piston assemblies should extend to the embrasure of should extend to the embrasure of the cuspid and first bicuspid to be the cuspid and first bicuspid to be long enough for adequate long enough for adequate distalization.distalization.
In maximum molar distalization In maximum molar distalization however, the piston assembly may however, the piston assembly may be extended beyond the first be extended beyond the first bicuspids.bicuspids.
3. A full arch silicone/vinyl 3. A full arch silicone/vinyl impression is then taken such that impression is then taken such that the bands seat securely in the the bands seat securely in the impression.impression.
4. The bands are then waxed and 4. The bands are then waxed and a working cast in stone is made.a working cast in stone is made.
www.indiandentalacademy.com

5. A 0.040" stainless steel5. A 0.040" stainless steel wire is then adapted to the wire is then adapted to the palate and is brought posteriorly to the gingival third of palate and is brought posteriorly to the gingival third of the bicuspid for soldering.the bicuspid for soldering.
6. A 0.036" stainless steel tubing is then soldered to the 6. A 0.036" stainless steel tubing is then soldered to the buccal and lingual occlusal thirds of the bicuspid bands.buccal and lingual occlusal thirds of the bicuspid bands.
7. The 0.030" stainless steel wire is soldered to the 7. The 0.030" stainless steel wire is soldered to the buccal and lingual surfaces of the first molar bands. buccal and lingual surfaces of the first molar bands. 0.040" stainless steel Nance wire is then soldered to the 0.040" stainless steel Nance wire is then soldered to the bicuspid bands.bicuspid bands.
www.indiandentalacademy.com

The piston assemblies must be The piston assemblies must be parallel in both the occlusal parallel in both the occlusal and sagittal views. and sagittal views.
A slight palatal cant from A slight palatal cant from distal to mesial can however distal to mesial can however be given to prevent occlusal be given to prevent occlusal displacements of the palatal displacements of the palatal acrylic.acrylic.
A 2mm split ring stop is than A 2mm split ring stop is than added to the mesial of the added to the mesial of the buccal and lingual tube on buccal and lingual tube on each piston assembly every 6 each piston assembly every 6 to 8 weeks. This provides to 8 weeks. This provides around 25 gms of force to around 25 gms of force to each piston assembly which each piston assembly which works out to 50 gms per tooth.works out to 50 gms per tooth.
www.indiandentalacademy.com

THE ADVANTAGESTHE ADVANTAGESThe fixed piston appliance has been proved to be The fixed piston appliance has been proved to be effective in molar distalisation and is said to have the effective in molar distalisation and is said to have the following advantages:following advantages:
Bodily movement of maxillary first molars (with no Bodily movement of maxillary first molars (with no loss of posterior anchorage).loss of posterior anchorage).
Minimum patient compliance.Minimum patient compliance. Allows the use of head gear if needed.Allows the use of head gear if needed. In non-extraction cases, it is proved to reduce In non-extraction cases, it is proved to reduce
treatment time as it distalizes at the rate of 1mm per treatment time as it distalizes at the rate of 1mm per month. month.
Maintains the arch width after expansion with Haas or Maintains the arch width after expansion with Haas or Hyrax appliances.Hyrax appliances.
Uses a light, controlled force of only 1-2 ounce per Uses a light, controlled force of only 1-2 ounce per tooth. Because of this there is no loss of anterior tooth. Because of this there is no loss of anterior anchorage and no inflammation of the palatal mucosa anchorage and no inflammation of the palatal mucosa beneath and adjacent to the modified Nance button.beneath and adjacent to the modified Nance button.
Does not interfere with the occlusal plane, thus Does not interfere with the occlusal plane, thus maintaining effective control over the vertical maintaining effective control over the vertical dimensions.dimensions.
www.indiandentalacademy.com

IBMDIBMD Ahmet Keles¸AJO (Jan 2000)Ahmet Keles¸AJO (Jan 2000) 15 patients were treated with IBMD , their 15 patients were treated with IBMD , their
average age was 13.53 years old ranging from average age was 13.53 years old ranging from 11 to 16 Years old. Second molars were 11 to 16 Years old. Second molars were present in all the cases.present in all the cases.Appliance ConstructionAppliance Construction
The The intraoral bodily molar distalizerintraoral bodily molar distalizer (IBMD (IBMD was composed of 2 parts: the anchorage unit was composed of 2 parts: the anchorage unit and the distalizing unit.and the distalizing unit.
The anchorage unit was a wide Nance button, The anchorage unit was a wide Nance button, and the active unit consisted of distalizing and the active unit consisted of distalizing springssprings
The springs had 2 components: the distalizer The springs had 2 components: the distalizer section of the spring applied a crown tipping section of the spring applied a crown tipping force, while the uprighting section of the force, while the uprighting section of the spring applied a root uprighting force on the spring applied a root uprighting force on the first molars.first molars.
www.indiandentalacademy.com

Maxillary first molars and premolars were banded. On Maxillary first molars and premolars were banded. On the palatal side of the first molar bands, 0.032 × the palatal side of the first molar bands, 0.032 × 0.032 inch slot size hinge cap palatal attachments 0.032 inch slot size hinge cap palatal attachments were welded, and a maxillary impression was taken. were welded, and a maxillary impression was taken. On the model, a wide acrylic Nance button was On the model, a wide acrylic Nance button was constructed and attached to the first premolar bands constructed and attached to the first premolar bands with 0.045 inch in diameter stainless steel retaining with 0.045 inch in diameter stainless steel retaining wires.wires.
The acrylic button was constructed that functioned The acrylic button was constructed that functioned as an anterior bite plane to disclude the posterior as an anterior bite plane to disclude the posterior teeth and enhance molar distalization.teeth and enhance molar distalization.
For molar distalization 0.32 x 0.32 inch size TMA For molar distalization 0.32 x 0.32 inch size TMA springs were bent and oriented from the acrylic. The springs were bent and oriented from the acrylic. The springs had 2 components. The distalizer section of springs had 2 components. The distalizer section of the spring applied a crown tipping force, whereas the the spring applied a crown tipping force, whereas the uprighting section of the spring applied a root uprighting section of the spring applied a root uprighting force to the first molars uprighting force to the first molars
www.indiandentalacademy.com

BB. The intraoral bodily molar distalizer (IBMD) was . The intraoral bodily molar distalizer (IBMD) was cemented to the first premolars without the springs cemented to the first premolars without the springs engaged. engaged.
B.B. After the cementation, the hinge caps on the molar After the cementation, the hinge caps on the molar bands were opened.bands were opened.
CC. Activation of distalizing component. Activation of distalizing componentD.D. Activation of the springs was accomplished by pulling Activation of the springs was accomplished by pulling
from distal to mesial with the help of a Weingart plier from distal to mesial with the help of a Weingart plier and then seating into the slot of the palatal hinge cap and then seating into the slot of the palatal hinge cap attachments. It applied a total of 230 g of distal force. attachments. It applied a total of 230 g of distal force.
www.indiandentalacademy.com

www.indiandentalacademy.com

This study showed that maxillary 1st molars were This study showed that maxillary 1st molars were distalized bodilydistalized bodily 5.23mm on average. Maxillary 5.23mm on average. Maxillary molar extrusion was not observed after distalization. molar extrusion was not observed after distalization. Maxillary molars did not rotate and intermolar Maxillary molars did not rotate and intermolar distance did not change after distalization.distance did not change after distalization.
Class I molar relationship was achieved in an Class I molar relationship was achieved in an average period of 7.5 months. average period of 7.5 months.
Maxillary first premolars moved forward 4.33 mm, Maxillary first premolars moved forward 4.33 mm, were extruded 3.33 mm, and tipped 2.7° distally.were extruded 3.33 mm, and tipped 2.7° distally.
A 4.77 mm protrusion and 6.73° proclination of the A 4.77 mm protrusion and 6.73° proclination of the incisors were observed. incisors were observed.
The overjet was increased by 4.1 mm; whereas the The overjet was increased by 4.1 mm; whereas the overbite was reduced by 2.63 mm. Mandibular first overbite was reduced by 2.63 mm. Mandibular first molars were extruded by 1.53 mm. molars were extruded by 1.53 mm.
After the removal of IBMD, incisor protrusion and After the removal of IBMD, incisor protrusion and mesial migration of premolars spontaneously mesial migration of premolars spontaneously relapsed distallyrelapsed distally
www.indiandentalacademy.com

Skeletal change:Skeletal change: Mandibular plane angle Mandibular plane angle
increased by 1.26°.increased by 1.26°. Anterior lower face height to Anterior lower face height to
total face height ratio was total face height ratio was increased by 0.95 mm.increased by 0.95 mm.
SNA increased by 1.56°, SNA increased by 1.56°, whereas ANB angle increased whereas ANB angle increased by 1.66°.by 1.66°.
www.indiandentalacademy.com

K-LoopK-LoopPut forward by Valrun Kalra (JCO 1995)Put forward by Valrun Kalra (JCO 1995)The K-Loop molar distalizer consists ofThe K-Loop molar distalizer consists of
1. A K-Loop to provide the forces and 1. A K-Loop to provide the forces and moments.moments.
2. A Nance button - to resist anchorage.2. A Nance button - to resist anchorage. The k-Loop is made of 0.017’ x 0.025' The k-Loop is made of 0.017’ x 0.025'
TMA wire which can be activated twice TMA wire which can be activated twice as much as stainless steel, before it as much as stainless steel, before it undergoes permanent plastic undergoes permanent plastic deformation.deformation.
www.indiandentalacademy.com

A.A. The loop of the 'K' should be 8 mm long The loop of the 'K' should be 8 mm long and 1.5 mm wide. and 1.5 mm wide.
BB. The legs of the 'K' are to be bent down 20 . The legs of the 'K' are to be bent down 20 ° and inserted into the molar tube and the ° and inserted into the molar tube and the premolar bracket. premolar bracket.
CC. The wires are marked at the mesial of the . The wires are marked at the mesial of the molar tube and the distal of the premolar molar tube and the distal of the premolar bracket. bracket.
A B C
www.indiandentalacademy.com

DD. Stops are bent into the wire 1 mm distal . Stops are bent into the wire 1 mm distal to the distal mark and 1 mm mesial to the to the distal mark and 1 mm mesial to the mesial mark. Each stop are well defined mesial mark. Each stop are well defined and are about 1.5mm long. and are about 1.5mm long.
EE. These bends help keep the appliances . These bends help keep the appliances away from the mucobuccal fold, allowing a away from the mucobuccal fold, allowing a 2mm activation of the loop 2mm activation of the loop
D E
www.indiandentalacademy.com

The bends in the appliance legs produce The bends in the appliance legs produce moments that counteract the tipping moments that counteract the tipping moments created by the force of the moments created by the force of the appliance, and these moments are appliance, and these moments are reinforced by the moment of activation as reinforced by the moment of activation as the loop is squeezed into place. Thus, the the loop is squeezed into place. Thus, the molar undergoes a translatory movement molar undergoes a translatory movement instead of tipping. Root movements are said instead of tipping. Root movements are said to continue even after the forces dissipate.to continue even after the forces dissipate.
www.indiandentalacademy.com

For additional molar movement, the For additional molar movement, the reactivation is 2mm after 6 to 8 weeks.reactivation is 2mm after 6 to 8 weeks.
The premolars move forward by 1 mm during The premolars move forward by 1 mm during 4 mm of molar distalization (the anchorage 4 mm of molar distalization (the anchorage loss). To prevent anchorage loss a head gear loss). To prevent anchorage loss a head gear (straight pull or high pull) with forces of 150 g (straight pull or high pull) with forces of 150 g to the premolars can be used.to the premolars can be used.
AdvantagesAdvantages Simple & efficientSimple & efficient Controls moment to force ratio to produce Controls moment to force ratio to produce
bodily movementbodily movement Easy fabrication and placement Easy fabrication and placement Hygienic and comfortable to the patient Hygienic and comfortable to the patient Low cost.Low cost.
www.indiandentalacademy.com

First class appliance jco First class appliance jco 99 june99 june
Bands are placed on Bands are placed on the maxillary first the maxillary first molars and on either molars and on either the maxillary second the maxillary second premolars or the premolars or the second deciduous second deciduous molars.molars.
Impressions are taken Impressions are taken with these bands in with these bands in place, and a working place, and a working cast is poured.cast is poured.
www.indiandentalacademy.com

Vestibular componentsVestibular components:: Formative screws are soldered Formative screws are soldered on the buccal sides of the first on the buccal sides of the first molar bands, occlusal to molar bands, occlusal to the .022" × .028" single tubes, the .022" × .028" single tubes, so they will not interfere with so they will not interfere with subsequent insertion of the subsequent insertion of the archwire . archwire .
Split rings, welded to the Split rings, welded to the second premolar or second second premolar or second deciduous molar bands, deciduous molar bands, control the vestibular screws. control the vestibular screws.
Stop screws are used to Stop screws are used to maintain the distal positions of maintain the distal positions of the molars after active the molars after active movement has been movement has been completed.completed.
www.indiandentalacademy.com

2. 2. Palatal componentsPalatal components. . In the palatal aspect, the In the palatal aspect, the appliance is much like a modified Nance button, but is appliance is much like a modified Nance button, but is wider and has a butterfly shape for added stability and wider and has a butterfly shape for added stability and support during retention . The butterfly section is support during retention . The butterfly section is soldered to the second bicuspid or deciduous molar soldered to the second bicuspid or deciduous molar bands.bands.The embedded .045" wires should be in single sections, The embedded .045" wires should be in single sections, without welded joints, to prevent breakage. Sections without welded joints, to prevent breakage. Sections of .045" tube are soldered to the palatal sides of the first of .045" tube are soldered to the palatal sides of the first molar bands for insertion of the butterfly component of molar bands for insertion of the butterfly component of the appliance. These tubes allow the molars to be the appliance. These tubes allow the molars to be distalized without undesirable tipping. distalized without undesirable tipping. www.indiandentalacademy.com

Nickel titanium .010" × .045" coil springs, Nickel titanium .010" × .045" coil springs, approximately 10mm each in length, are fully approximately 10mm each in length, are fully compressed between the bicuspid solder compressed between the bicuspid solder joints and the tubes on the deciduous molar joints and the tubes on the deciduous molar or second bicuspid bands. These springs are or second bicuspid bands. These springs are designed to balance the action of the designed to balance the action of the vestibular screws, preventing molar rotations vestibular screws, preventing molar rotations and development of posterior crossbites.and development of posterior crossbites.
www.indiandentalacademy.com

Bodily distalization of first molars on Bodily distalization of first molars on both sides; detail of formative screw both sides; detail of formative screw at end of activationat end of activation
www.indiandentalacademy.com

BYLOFF et al (JCO 2000 sept) made a new device, BYLOFF et al (JCO 2000 sept) made a new device, based on the Pendulum that can based on the Pendulum that can distalize mandibulardistalize mandibular molars without the drawbacks of other appliances. molars without the drawbacks of other appliances. Appliance Design Appliance Design
The The Franzulum Franzulum Appliance’sAppliance’s anterior anchorage unit is anterior anchorage unit is an acrylic button, positioned lingually and inferiorly to an acrylic button, positioned lingually and inferiorly to the mandibular anterior teeth, and extending from the the mandibular anterior teeth, and extending from the mandibular left canine to the mandibular right canine.mandibular left canine to the mandibular right canine.
Rests on the canines and first premolars are made Rests on the canines and first premolars are made from .032" stainless steel wire. Tubes between the from .032" stainless steel wire. Tubes between the second premolars and first molars receive the active second premolars and first molars receive the active components. The posterior distalizing unit uses nickel components. The posterior distalizing unit uses nickel titanium coil springs, about 18mm in length, which titanium coil springs, about 18mm in length, which apply an initial force of 100-120g per sideapply an initial force of 100-120g per sidewww.indiandentalacademy.com

A J-shaped wire passing through each coil is inserted A J-shaped wire passing through each coil is inserted into the corresponding tube of the anchorage unit the into the corresponding tube of the anchorage unit the recurved posterior portion of the wire is engaged in recurved posterior portion of the wire is engaged in the lingual sheath of the mandibular first molar band. the lingual sheath of the mandibular first molar band.
The anchorage unit is bonded with composite resin to The anchorage unit is bonded with composite resin to the canines and first premolars. the canines and first premolars.
The J-shaped distalizing unit is then ligated to the The J-shaped distalizing unit is then ligated to the lingualsheaths of the molar bands, compressing the lingualsheaths of the molar bands, compressing the coil springs. Thus, the active part of the appliance coil springs. Thus, the active part of the appliance runs lingually at a level close to the center of runs lingually at a level close to the center of resistance of the molar, to produce an almost pure resistance of the molar, to produce an almost pure bodily movement bodily movement www.indiandentalacademy.com

During the distalization phase, the During the distalization phase, the mandibular molars moved 4.5-5mm mandibular molars moved 4.5-5mm distally while the incisors moved distally while the incisors moved 1mm anteriorly. The mandibular right 1mm anteriorly. The mandibular right molar crown tipped 4° distally, and molar crown tipped 4° distally, and the mandibular incisor crowns tipped the mandibular incisor crowns tipped 1° labially. Thus, the movement of the 1° labially. Thus, the movement of the incisor crown resulted in an incisor crown resulted in an anchorage loss of 1mm and 1°. anchorage loss of 1mm and 1°.
www.indiandentalacademy.com

Herbst ApplianceHerbst Appliance The Herbst appliance is completely tooth-borne The Herbst appliance is completely tooth-borne
and uses both the maxillary and mandibular and uses both the maxillary and mandibular dentition to transfer the force exerted from the dentition to transfer the force exerted from the telescopic arms of the Herbst bite jumping mech telescopic arms of the Herbst bite jumping mech anism to the bases of the maxilla and the anism to the bases of the maxilla and the mandible. The telescopic system produces a mandible. The telescopic system produces a posterosuperiorly directed force on the maxil lary posterosuperiorly directed force on the maxil lary posterior teeth and an anteriorly directed force on posterior teeth and an anteriorly directed force on the mandibular dentition. As a result, Class II the mandibular dentition. As a result, Class II molar correction generally is a combina tion of molar correction generally is a combina tion of skeletal and dentoalveolar changes irre spective of skeletal and dentoalveolar changes irre spective of facial morphology. facial morphology.
www.indiandentalacademy.com

The Herbst telescoping bitejumping mechanism The Herbst telescoping bitejumping mechanism places a distal and intrusive force on the maxillary places a distal and intrusive force on the maxillary molars and the force vector passes occ1usally to molars and the force vector passes occ1usally to the center of resistance. This force system the center of resistance. This force system produces backward and upward movements of produces backward and upward movements of maxillary molars in conjunction with distal crown maxillary molars in conjunction with distal crown tip ping. Because of the intrusive effect, distal tip ping. Because of the intrusive effect, distal movements of maxillary molars do not tend to open movements of maxillary molars do not tend to open the mandible. These effects are similar to those the mandible. These effects are similar to those produced by high-pull head gear. produced by high-pull head gear.
In general, maxillary molar distal ization has been In general, maxillary molar distal ization has been shown to comprise approxi mately 25% to 40% of shown to comprise approxi mately 25% to 40% of molar correction with the banded Herbst molar correction with the banded Herbst appliance, whereas in the acrylic design it appliance, whereas in the acrylic design it accounts for 20% to 25% of the correction. accounts for 20% to 25% of the correction.
www.indiandentalacademy.com

The distalizing effects are reported to range from an The distalizing effects are reported to range from an average of 1.8 mm in the study by Franchi et al (AJO average of 1.8 mm in the study by Franchi et al (AJO 1999) to 2.8 mm in the study by Pancherez (AJO 1982). 1999) to 2.8 mm in the study by Pancherez (AJO 1982). The intrusive effects are 1mm approximately. The The intrusive effects are 1mm approximately. The amount of distal and vertical movement of maxillary amount of distal and vertical movement of maxillary molars is found to be independent of the presence of molars is found to be independent of the presence of erupted 2erupted 2ndnd molar. molar.StabilityStability
In a long-term study on the results of Herbst treatment, In a long-term study on the results of Herbst treatment, Pancherz (AJO 1991) compared two groups of Herbst-Pancherz (AJO 1991) compared two groups of Herbst-treated patients with and without relapse in the treated patients with and without relapse in the occlusion. Skeletal and dentoalveolar changes in the occlusion. Skeletal and dentoalveolar changes in the mandibular arch were found to be similar in both groups mandibular arch were found to be similar in both groups 5 years after treatment. The reason for relapse was 5 years after treatment. The reason for relapse was thought to be the anterior movements of maxillary thought to be the anterior movements of maxillary dentition owing to muscular influence from the lips or dentition owing to muscular influence from the lips or tongue, or to an unstable occlusal condition after tongue, or to an unstable occlusal condition after treatment.treatment.
www.indiandentalacademy.com

The Klapper Superspring II:The Klapper Superspring II: In 1997 Lewis Klapper introduced In 1997 Lewis Klapper introduced
the Klapper Superspring for the the Klapper Superspring for the correction of Class II malocclusions. correction of Class II malocclusions. It resembles a Jasper Jumper with It resembles a Jasper Jumper with the substitution of a cable for the the substitution of a cable for the coil spring. In 1998 the cable was coil spring. In 1998 the cable was wrapped with a coil.wrapped with a coil.
The Klapper Superspring II inserts The Klapper Superspring II inserts from the mesial and is rigidly from the mesial and is rigidly secured to the molar by an oval secured to the molar by an oval attachment tube. The Klapper attachment tube. The Klapper Superspring creates a mo ment on Superspring creates a mo ment on the molar, which is expressed the molar, which is expressed clinically as distal root tip, but clinically as distal root tip, but extended wear of the appliance extended wear of the appliance results in excessive distal root results in excessive distal root tipping.tipping.
www.indiandentalacademy.com

Because the Klapper Superspring inserts gingivally Because the Klapper Superspring inserts gingivally on the molar and cannot roll to the buccal as on the molar and cannot roll to the buccal as readily as a Jasper Jumper, there may be a greater readily as a Jasper Jumper, there may be a greater vertical component to the force vector. If this were vertical component to the force vector. If this were of clinical significance, a patient with a pro nounced of clinical significance, a patient with a pro nounced curve of Spee would level more quickly with the curve of Spee would level more quickly with the Klapper Superspring. However, extended wear Klapper Superspring. However, extended wear should pro duce excessive intrusions and may should pro duce excessive intrusions and may require removal before sagittal corrections have require removal before sagittal corrections have been completed.been completed.
Disadvantages of the Klapper Superspring:Disadvantages of the Klapper Superspring: 1. Requirement of a special molar tube, 1. Requirement of a special molar tube, 2. Limitation to maximal opening, 2. Limitation to maximal opening, 3. Risk of injury to the patient if breakage oc curs 3. Risk of injury to the patient if breakage oc curs 4. Extended wear may cause excessive distal root 4. Extended wear may cause excessive distal root
tipping to the maxillary molar and more intrusion tipping to the maxillary molar and more intrusion to the molars and incisors than desiredto the molars and incisors than desired
www.indiandentalacademy.com

The Eureka SpringThe Eureka Spring The interarch Eureka Spring The interarch Eureka Spring
became available in 1996, has a became available in 1996, has a pure compression action, and pure compression action, and therefore delivers linear force therefore delivers linear force throughout its range. It permits throughout its range. It permits unlimited mandibular move ments unlimited mandibular move ments and has good patient acceptance. and has good patient acceptance. It can be used in Class II and It can be used in Class II and Class III malocclusions, does not Class III malocclusions, does not require molar tubes, and can be require molar tubes, and can be used in conjunction with used in conjunction with extraoral force. These springs extraoral force. These springs come in two sizes and are come in two sizes and are converted at the time of insertion converted at the time of insertion into left or right action; therefore into left or right action; therefore inventory is minimal. inventory is minimal.
www.indiandentalacademy.com

No auxiliary attachments are required. Because it No auxiliary attachments are required. Because it is truly a compression spring, it is less prone to is truly a compression spring, it is less prone to breakage than curvi linear than Jasper Jumper. A breakage than curvi linear than Jasper Jumper. A constant force of 16 grams per millimeter is constant force of 16 grams per millimeter is generated, which permits the clinician to visually generated, which permits the clinician to visually determine the force at any time and adjust the determine the force at any time and adjust the force as needed force as needed
A cephalometric evaluation of the first 50 A cephalometric evaluation of the first 50 consecutively treated bilateral Class II patients consecutively treated bilateral Class II patients indicated the following:indicated the following:
Average anteroposterior correction was at the rate Average anteroposterior correction was at the rate of 0.7mm per month.of 0.7mm per month.
For every 3 mm of anteroposterior correction, the For every 3 mm of anteroposterior correction, the maxil lary molars intruded 1 mm and the maxil lary molars intruded 1 mm and the mandibular incisors intruded 2 mm.mandibular incisors intruded 2 mm.
www.indiandentalacademy.com

The maxillary dentition moved distally 1.5 mm and The maxillary dentition moved distally 1.5 mm and the mandibular dentition moved mesially 1.5 mm.the mandibular dentition moved mesially 1.5 mm.
No increase occurred in anterior face height No increase occurred in anterior face height between the dolichocephalic and brachycephalic between the dolichocephalic and brachycephalic subgroups.subgroups.
As with the Jasper Jumper, intrusion of teeth As with the Jasper Jumper, intrusion of teeth occurs dur ing treatment. However, unlike the occurs dur ing treatment. However, unlike the Jasper Jumper the amount of intrusive force can be Jasper Jumper the amount of intrusive force can be altered by changing the force vector and altered by changing the force vector and magnitudemagnitude
www.indiandentalacademy.com

Karaman -Karaman - implant-supported implant-supported modified distal jet appliancemodified distal jet appliance
Graz implant supported pendulumGraz implant supported pendulum Sugawara & Umemori SAS Sugawara & Umemori SAS
supported mandibular distalizationsupported mandibular distalization
IMPLANT SUPPORTED IMPLANT SUPPORTED DISTALIZATIONDISTALIZATION
www.indiandentalacademy.com

Karaman (AO 2002 April ) A Karaman (AO 2002 April ) A case reportcase report
In this study, author used an In this study, author used an implant-supported modified implant-supported modified distal jet appliance that has the distal jet appliance that has the advantages of implants and advantages of implants and intraoral distalization appliances, intraoral distalization appliances, and assessed its effect on and assessed its effect on dentofacial structures.dentofacial structures.
Molar bands with palatal tubes Molar bands with palatal tubes were fitted to the upper first were fitted to the upper first molars. An anchorage screw molars. An anchorage screw three mm in diameter and 14 three mm in diameter and 14 mm in length was placed at the mm in length was placed at the anterior palatal suture, two–anterior palatal suture, two–three mm posterior to the canalis three mm posterior to the canalis incissivus under local incissivus under local anesthesia . anesthesia . www.indiandentalacademy.com

Anchor wires 0.8 mm in Anchor wires 0.8 mm in diameter were soldered to the diameter were soldered to the tubes for occlusal rests on the tubes for occlusal rests on the first premolars. The 0.9-mm first premolars. The 0.9-mm wire extended through each wire extended through each tube, ending in a bayonet tube, ending in a bayonet bend that was inserted into bend that was inserted into the palatal tube of the first the palatal tube of the first molar band.molar band.
For force application, Niti For force application, Niti open-coil springs were open-coil springs were adjusted.adjusted.
The implant-supported The implant-supported modified distal jet appliance modified distal jet appliance was attached to the anchor was attached to the anchor premolars and implant with premolars and implant with light-cured composite light-cured composite adhesive.adhesive.
www.indiandentalacademy.com

The screw was removed without anesthesia and with The screw was removed without anesthesia and with no discomfort for the patient during the removal.no discomfort for the patient during the removal.
Maxillary molar moved distally 5mm after 4 months Maxillary molar moved distally 5mm after 4 months of treatment and intruded by 2mm without of treatment and intruded by 2mm without movement of premolars.movement of premolars.
Upper incisor position, MPA, and LAFH remained Upper incisor position, MPA, and LAFH remained the same.the same.
The main advantages of the appliance are its The main advantages of the appliance are its stability against rotational movements. Adequate stability against rotational movements. Adequate distal movement of the molar tooth was achieved distal movement of the molar tooth was achieved without the loss of anchorage.without the loss of anchorage.
Irritation of the palatal mucosa and gingival Irritation of the palatal mucosa and gingival hyperplasia didn’t occur because the patient could hyperplasia didn’t occur because the patient could maintain optimum oral hygiene.maintain optimum oral hygiene.
www.indiandentalacademy.com

GRAZ IMPLANT SUPPORTED PENDULUMGRAZ IMPLANT SUPPORTED PENDULUM Byloff et al (Int J Adult Orthod. Orthognathic Byloff et al (Int J Adult Orthod. Orthognathic
Surg 2000)Surg 2000) To avoid mesial movement of anchor teeth, To avoid mesial movement of anchor teeth,
extraoral anchorage such as headgears and extraoral anchorage such as headgears and intraoral Nance holding arches are commonly intraoral Nance holding arches are commonly used.used.
Advances with implants have made it possible to Advances with implants have made it possible to use them as a means of anchorage in adult use them as a means of anchorage in adult orthodontic patients. orthodontic patients.
But with orthodontic patients, when only the But with orthodontic patients, when only the question of anchorage must be addressed, the question of anchorage must be addressed, the retro molar area or the palate as implant retro molar area or the palate as implant locations are preferred because they do not locations are preferred because they do not interfere with orthodontic tooth movement. interfere with orthodontic tooth movement.
www.indiandentalacademy.com

Site for Orthodontic Implants:Site for Orthodontic Implants: The histomorphology of the palatal bone The histomorphology of the palatal bone
shows that the median palatal region is the shows that the median palatal region is the best location for an endosseous implant. best location for an endosseous implant. Implant loading:Implant loading:
Implants are loaded after a period of Implants are loaded after a period of approximately 12 to 24 weeks to allow approximately 12 to 24 weeks to allow healing and osseointegration, which seems healing and osseointegration, which seems to be a general rule in the use of implants. to be a general rule in the use of implants.
Byloff described a newly designed palatal Byloff described a newly designed palatal anchoring system, the Graz implant-anchoring system, the Graz implant-supported pendulum (GISP) .This system can supported pendulum (GISP) .This system can be loaded within 2 weeks to distalize and be loaded within 2 weeks to distalize and anchor maxillary first and second molars.anchor maxillary first and second molars.
www.indiandentalacademy.com

The anchorage part of the GISP consists of a simple The anchorage part of the GISP consists of a simple surgical plate (15 X 10 mm) with 4 screw holes. surgical plate (15 X 10 mm) with 4 screw holes. Two cylinders (10 mm long and 3.5 mm in Two cylinders (10 mm long and 3.5 mm in diameter) are soldered at right angles to the diameter) are soldered at right angles to the center of the plate. center of the plate.
The plate is fixed to the palatal bone via four 5-mm-The plate is fixed to the palatal bone via four 5-mm-long titanium mini screws The 2 cylinders perforate long titanium mini screws The 2 cylinders perforate the palatal mucosa to enter the oral cavity .The the palatal mucosa to enter the oral cavity .The entire anchorage device is made of 100% Titanium.entire anchorage device is made of 100% Titanium.
www.indiandentalacademy.com

Implant is placed under GA.Implant is placed under GA. Maxillary impression is taken after 2 weeks Maxillary impression is taken after 2 weeks
of healing.of healing. Removable PA is fabricated.Removable PA is fabricated. TMA springs are activated extraorally to TMA springs are activated extraorally to
generate 250 g of forcegenerate 250 g of force www.indiandentalacademy.com

Because molars tend to tip back when Because molars tend to tip back when distalized with a PA,an uprighting bend ( distalized with a PA,an uprighting bend ( Byloff AO 1997) was introduced into the Byloff AO 1997) was introduced into the recurved end of the spring when recurved end of the spring when necessary.necessary.
After the 8 months of molar After the 8 months of molar distalization, the first and second distalization, the first and second premolars have drifted distally, premolars have drifted distally, presumably under the influence of the presumably under the influence of the elastic fibers in that area. The molars elastic fibers in that area. The molars were almost in a full Class II relationship were almost in a full Class II relationship at the beginning of treatment at the beginning of treatment
www.indiandentalacademy.com

Advantages:Advantages:1. Class II elastics to support anchorage are 1. Class II elastics to support anchorage are unnecessary, and side eff ects on the mandible are unnecessary, and side eff ects on the mandible are avoided. avoided. 2. This system can be loaded almost immediately, 2. This system can be loaded almost immediately, which is an advantage over implants requiring a which is an advantage over implants requiring a healing and osseointegration time of at least 3 – 4 healing and osseointegration time of at least 3 – 4 month.month.3. Unilateral distalization can be done without any 3. Unilateral distalization can be done without any effect of generated moment.effect of generated moment.4. Treat ment time is decreased because of the 4. Treat ment time is decreased because of the anchorage provided by the GISP. En masse retraction anchorage provided by the GISP. En masse retraction of anteriors can be done shortening the treatment of anteriors can be done shortening the treatment time considerably.time considerably.5. Stability against rotational movements5. Stability against rotational movements
Disadvantage: Disadvantage: Invasive surgical procedureInvasive surgical procedure for for insertion and removal of anchorage plates.insertion and removal of anchorage plates.
www.indiandentalacademy.com

Sugawara & Umemori, (Ajo 2004JanSugawara & Umemori, (Ajo 2004Jan) ) The skeletal anchorage system (SAS) consists of The skeletal anchorage system (SAS) consists of
titanium anchor plates and monocortical screws titanium anchor plates and monocortical screws that are temporarily placed in either the maxilla that are temporarily placed in either the maxilla or the mandible, or in both, as absolute or the mandible, or in both, as absolute orthodontic anchorage units, Distalization of the orthodontic anchorage units, Distalization of the molars has been one of the most difficult molars has been one of the most difficult biomechanical problems in traditional biomechanical problems in traditional orthodontics, particularly in adults and in the orthodontics, particularly in adults and in the mandible, However, it has now become possible mandible, However, it has now become possible to move molar's distally with the SAS to correct to move molar's distally with the SAS to correct anterior crossbites, maxillary dental protrusion, anterior crossbites, maxillary dental protrusion, crowding, dental asymmetries without having to crowding, dental asymmetries without having to extract premolars.extract premolars.
www.indiandentalacademy.com

Skeletal anchorage system (SAS) uses pure Skeletal anchorage system (SAS) uses pure titanium anchor plates and screws as absolute titanium anchor plates and screws as absolute orthodontic anchorage units. The anchor orthodontic anchorage units. The anchor plates are monocortically placed at the plates are monocortically placed at the piriform opening rim, the zygomatic piriform opening rim, the zygomatic buttresses, and any regions of the mandibular buttresses, and any regions of the mandibular cortical bone, Because the anchor plates work cortical bone, Because the anchor plates work as the onplant and the screws function as the as the onplant and the screws function as the implant, SAS enables the rigid anchorage that implant, SAS enables the rigid anchorage that results from the osseointegration effects in results from the osseointegration effects in both the anchor plates and screws. both the anchor plates and screws.
www.indiandentalacademy.com

SAS does not interfere with tooth SAS does not interfere with tooth movement. Therefore, it is possible to movement. Therefore, it is possible to distalize the mandibular molars with distalize the mandibular molars with anchor plates placed at the anterior border anchor plates placed at the anterior border of the mandibular ramus or mandibular of the mandibular ramus or mandibular bodybody
www.indiandentalacademy.com

Sugawara & Umemori evaluated the treatment Sugawara & Umemori evaluated the treatment
and posttreatment changes during and after and posttreatment changes during and after distalization of the mandibular molars, In 15 adult distalization of the mandibular molars, In 15 adult patients, a total of 29 mandibular molars were patients, a total of 29 mandibular molars were successfully distalized with SAS.successfully distalized with SAS.
The amount of posterior displacement at the The amount of posterior displacement at the crown and root levels was measured on the crown and root levels was measured on the occlusograms and the cephalometric tracings, occlusograms and the cephalometric tracings, respectively. The type of tooth movement was respectively. The type of tooth movement was evaluated by the crown and root movement ratio. evaluated by the crown and root movement ratio. When the percentage ratio of the root movement When the percentage ratio of the root movement to the crown movement (the to the crown movement (the tipping ratiotipping ratio) was ) was less than 25%, the type of tooth movement was less than 25%, the type of tooth movement was determined to be tipping. determined to be tipping.
www.indiandentalacademy.com

The average amount of distal move ment with SAS The average amount of distal move ment with SAS was 3.5 mm at the crown level and 1.8mm at root was 3.5 mm at the crown level and 1.8mm at root apex level. The maximum amount of distalization at apex level. The maximum amount of distalization at the crown level was 7.1 mm, and the minimum was the crown level was 7.1 mm, and the minimum was 1.0 mm at the first molar. The average tipping ratio 1.0 mm at the first molar. The average tipping ratio was 46.3%. Although most of the first molars showed was 46.3%. Although most of the first molars showed bodily movement, 9 of 29 molars showed tipping bodily movement, 9 of 29 molars showed tipping movement, in which the tipping ratios were less than movement, in which the tipping ratios were less than 25%.25%.
Maximum relapse was 0.8 mm. and the maxi mum Maximum relapse was 0.8 mm. and the maxi mum relapse rate was 40%. The average amount of relapse relapse rate was 40%. The average amount of relapse was 0.3 mm at both the crown and root apex levels. was 0.3 mm at both the crown and root apex levels. No significant correlation was found between the No significant correlation was found between the amount of relapse and the tipping ratio and the amount of relapse and the tipping ratio and the amount of tooth movement.amount of tooth movement.
www.indiandentalacademy.com

The SAS has The SAS has outstanding advantagesoutstanding advantages not provided by not provided by the other mechanisms for distalizing the mandibular the other mechanisms for distalizing the mandibular molars.molars.
1. It is possible to intrude the mandibular molars 1. It is possible to intrude the mandibular molars with the SAS. Therefore the extrusion of the with the SAS. Therefore the extrusion of the mandibular molars after the tipping of the molar mandibular molars after the tipping of the molar distalization can be corrected easily.distalization can be corrected easily.
2. En masse distalization of the mandibular buccal 2. En masse distalization of the mandibular buccal segments or the entire dentition is also possible if segments or the entire dentition is also possible if the mandibular dentition is aligned. the mandibular dentition is aligned.
3. With the SAS, it is not always neccssary to 3. With the SAS, it is not always neccssary to extract the mandibular first or second premolars extract the mandibular first or second premolars even in patients with moderate to severe crowding.even in patients with moderate to severe crowding.
4. Molar relationship in patients with symmetric or 4. Molar relationship in patients with symmetric or asymmetric Class III molar relationship can be asymmetric Class III molar relationship can be corrected without having to extract mandibular corrected without having to extract mandibular premolars.premolars.
www.indiandentalacademy.com

Conclusion Conclusion Traditionally, the arch length deficiency Traditionally, the arch length deficiency has been calculated anterior to the first has been calculated anterior to the first molars because molar distalization was molars because molar distalization was assumed to be nearly impossible. However assumed to be nearly impossible. However by using the space posterior to the second by using the space posterior to the second molars. 14 permanent teeth can be well molars. 14 permanent teeth can be well aligned in the alveolar bone as demon aligned in the alveolar bone as demon strated by the present study. Therefore it strated by the present study. Therefore it will now become necessary to find an will now become necessary to find an indicator to determine the posterior limits indicator to determine the posterior limits of the alveolar region from the standpoints of the alveolar region from the standpoints of orthodontics, anatomy, and periodon of orthodontics, anatomy, and periodon tology. E.g. Location of mandibular 3tology. E.g. Location of mandibular 3rdrd molar molar www.indiandentalacademy.com

Thank youThank you
For more details please visit For more details please visit www.indiandentalacademy.comwww.indiandentalacademy.com
www.indiandentalacademy.com