Embed Size (px)
Citation preview

Newborn baby boy with hypoglycemia and idiopathic
neonatal hepatitisMoina
Uddin, D.O
Endorama
12/5/13
Chief Complaint
• 11 day old male neonate with persistent hypoglycemia
HPI
• Born FT, AGA, via c‐section • Pregnancy complicated by maternal diabetes,
asthma and HTN, GBS + status
• Meconium‐stained amniotic fluid perinatal stress
• APGARS = 91, 95
• Initially to General Nursery

HPI
• POC glucose = 20 at 1 hour of life (26 on repeat)
• POC glucose = 41 s/p feed• Needed continuous IVF until DOL 5, with
highest GIR of 9.6 ml/kg/min to maintain POC glucose 60s‐70s.

HPI
• Repeated episodes of hypoglycemia after GIR was weaned ENDOCRINE CONSULT
Additional History
• Family Hx– Mother with GDM– Father with seizure disorder from birth until 7 yo,
some staring spells– Paternal great aunt with seizure disorder– Half‐brother died at age 3 yo from esophageal
rupture
• Social Hx– Will live at home with both parents and 2 siblings
Review of Systems
• Constitutional: Negative for fever. + appropriate
weight
• Endocrine: Hypoglycemia
• HENT: Negative• Respiratory: Negative• Cardiovascular: Negative• Gastrointestinal:
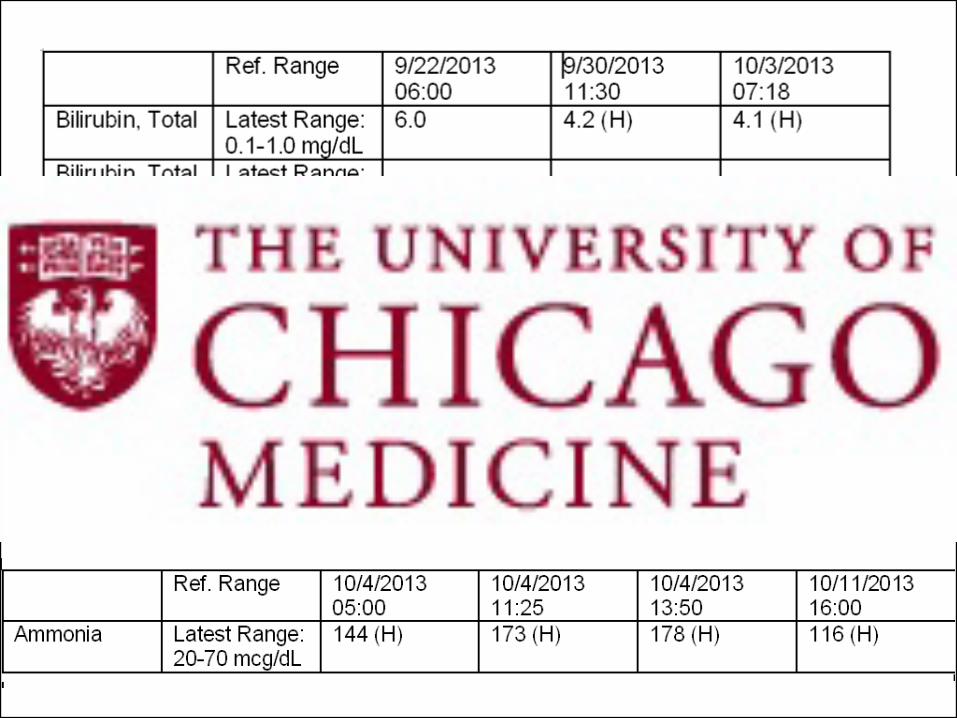
Hyperbilirubinemia
• Genitourinary: Negative• Skin: Negative• Neurological: Negative
for seizures
• Hematological: Polycythemia, now
resolved
• Psychiatry: No agitation or increased somnolence
Physical Examination
• Vitals: Wt: 3.425 (~40%ile),
Lt: 52 cm (~55%ile)Temp: 36.6‐36.8 C, HR: 140‐
181, RR: 32‐51, BP: 68‐
75/42‐44• General: Well appearing,
good grimace• HEENT: No facial
deformities, no cleft
palate, no nystagmus• Skin: Plethoric, sloughing
skin all over, non‐icteric
• CV: RRR, no murmurs, CR <
3 secs, 2+ femoral pulses• Pulmonary: CTAB, good
aeration bilaterally,
intermittent tachypnea, no
nasal flaring• Abdomen: Soft, ND, NT, No
HSM, +BS• GU: Normal phallus length
(3.5 cm), testes descended
bilaterally, • Neuro: Normal tone, Equal
DTRs, Nonfocal exam

Differential diagnosis and assessment for this 11 day‐old with persistent
hypoglycemia?
Differential Diagnosis of Hypoglycemia
• Hyperinsulinism• Hormonal deficiency
• Defects in hepatic glycogen
storage/release
• Defects of fatty acid oxidation and carnitine
metabolism
• Defects in ketone body synthesis/utilization
• Metabolic conditions
• Drug induced• Other‐
sepsis
Assessment and Plan
• Hyperinsulinism• Treat with Diazoxide• Send HI genetic testing panel

Additional history

Further testing
• CMV and Toxoplasma titers negative• Enterovirus culture negative• Liver biopsy: consistent with idiopathic
neonatal hepatitis.– Giant cell hepatitis, few acidophil bodies sign of
resolved viral infection– Dx: Idiopathic Neonatal Hepatitis
Assessment and Plan
• 1. Hyperinsulinism‐ Unknown etiology
• 2. Low GH?• 3. Idiopathic neonatal
hepatitis
• Diazoxide, Endo F/u
• Observation• Actigall, GI F/u

Follow‐up History
• Seen in GI clinic with improving labs and Actigall stopped
• Repeated episodes of hypoglycemia
on Diaxozide 15 mg/kg/day and q3 hr feeds
READMISSION
Hospital Course
• Diazoxide increased to 20 mg/kg/day
• Diuril began empirically
• Feeds spaced and BG monitored qac
q3 q4 q6 q6‐8
• 10 hour safety fast (BG checked at +6 hr, +8 hr, +9 hr and +10 hr)
– Lowest POC BG: 78– Serum BG: 91, insulin <2, ketones 1.17, FFA 1.18
Hospital Course
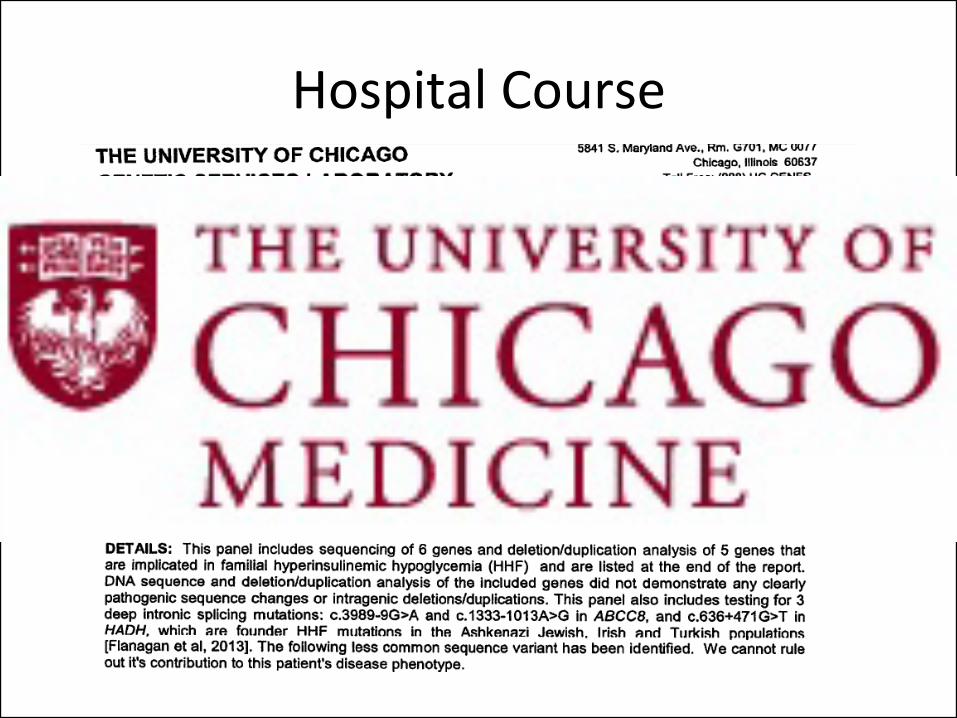
Hospital Course
Clinical Questions
• Is there a single mechanism to explain hyperinsulinemia and cholestasis in our patient?
• What is the clinical course of neonatal cholestasis due to growth hormone deficiency?
• What is the expected GH level following hypoglycemia in a neonate?
Clinical Questions
• Is there a single mechanism to explain hyperinsulinemia and cholestasis in our patient?
NO.
Clinical Questions
• What is the clinical course of neonatal cholestasis due to growth hormone deficiency?
Spray CH, McKiernan P, Waldron KE, Shaw N, Kierk J, Kelly DA. Investigation and outcome of neonatal
hepatitis in infants with hypopituitarism. Acta Paediatr 2000 89: 951‐4
Spray CH, McKiernan P, Waldron KE, Shaw N, Kierk J, Kelly DA. Investigation and outcome of neonatal
hepatitis in infants with hypopituitarism. Acta Paediatr 2000 89: 951‐4
Clinical Questions
• What is the expected GH level following hypoglycemia in a neonate?
Poor Specificity of Low Growth Hormone and Cortisol Levels During Fasting Hypoglycemia for the Diagnoses of
Growth Hormone Deficiency and Adrenal Insufficiency Andrea Kelly, MDa,b, Randy Tang, RN, BSN, BSEa, Susan
Becker, BSN, RNa, Charles A. Stanley, MDa, Pediatrics 2008;122;e522
Poor Specificity of Low Growth Hormone and Cortisol Levels During Fasting Hypoglycemia for the Diagnoses of Growth Hormone Deficiency and Adrenal Insufficiency Andrea Kelly,
MDa,b, Randy Tang, RN, BSN, BSEa, Susan Becker, BSN, RNa, Charles A. Stanley, MDa, Pediatrics 2008;122;e522
Senniappan S, Hussain K. An Evaluation of Growth Hormone and IGF‐1 Responses in Neonates with
Hyperinsulinaemic Hypoglycaemia . Int J of Endocrinol 2013; Article ID 638257
Senniappan S, Hussain K. An Evaluation of Growth Hormone and IGF‐1 Responses in Neonates with
Hyperinsulinaemic Hypoglycaemia . Int J of Endocrinol 2013; Article ID 638257

References
• Choo
Kang LR, Sun CC, Counts DR. Cholestatsis
and hypoglycaemia:
manifestations of congenital anterior hypopituitarism.
J Clin Endocrinol
Metab 1996; 81: 2786–9
• Senniappan
S, Hussain
K. An Evaluation of Growth Hormone and IGF‐1
Responses in Neonates with Hyperinsulinaemic
Hypoglycaemia
. Int
J of
Endocrinol
2013; Article ID 638257
• Spray CH, McKiernan P, Waldron KE, Shaw N, Kierk
J, Kelly DA.
Investigation and outcome of neonatal hepatitis in infants with
hypopituitarism. Acta
Paediatr
2000 89: 951‐4
• Kelly A, Tang R, Becker S, Stanley CA Poor Specificity of Low Growth
Hormone and Cortisol
Levels During Fasting Hypoglycemia for the
Diagnoses of Growth Hormone Deficiency and Adrenal Insufficiency.
Pediatrics 2008;122;e522



![Managing obesity could be our biggest challenge · somnolence (sleepiness), hypoventilation (under-breathing) and plethoric (red) 1 face.] The health consequences of obesity are now](https://img.pdfslide.us/doc/110x75/5f556a80503e66714c33a843/managing-obesity-could-be-our-biggest-somnolence-sleepiness-hypoventilation-under-breathing.jpg)