Embed Size (px)
Citation preview

1
Lithuanian University of Health Sciences Faculty of Medicine
Second year Spring semester
MODULE NUTRIENT UPTAKE
Part Biochemistry
Practicals
Kaunas Year 2014- 2015 February-March

2
ESSENTIAL INFORMATION
All laboratory works of Biochemistry will take place in Veterinary academu, Tilzes str. 18, Laboratory Building N 4, Biochemistry lab-rooms 307 (3rd floor)
Course organizer prof.L.Ivanoviene room 318 Coordinator prof. R.Morkūniene room 301

3
SAFETY NOTES OF WORK IN BIOCHEMISTRY LABORATORY
This document must be read before your first practical.
1.Department policy 1.1 It is overriding policy of the University and Department of biochemistry that experimental
work, whether associated with teaching or research, be done efficiently and safely. Safety begins with the individual’s personal responsibility. However, in addition, each member of the academic staff and each technician have a statutory duty to take reasonable care for persons under his/her supervision.
1.2 Students have a statutory obligation to protect themselves and others from hazards resulting from their acts or omissions in the laboratory.
1.3 Only the students of groups scheduled are permitted to be in the laboratory. Visitors or intruders should be asked to leave.
2. General
2.1. Smoking, eating and drinking are not permitted on the laboratory. 2.2. Outdoor clothing must be left in a cloakroom. Bags must be placed on side podia provided for
the purpose and not allowed to obstruct gangways or bench tops. 2.3. Suitable laboratory coats must be worn in the laboratory and removed after leaving. Safety
spectacles must be worn when carrying out any procedure where may be slightest risk of eye injury; gloves of the appropriate type must be worn when necessary. Long hair must be restrained e.g. by means of a cap, ribbon or headband.
2.4. The notes for each practical should be read before coming to the practical and note taken of any safety matters. Students are NOT permitted to do any experimental work unless a supervisor (demonstrator or a member of staff) is present.
2.5. The use of unfamiliar equipment and the handling of potentially hazardous materials will be explained to students. If a student, for some reason, misses the appropriate explanation, then it is the student’s responsibility to bring the lack of knowledge to the attention of the Chief Technician, so that appropriate arrangements can be made to remedy the situation.
2.6. Glassware and plastic ware that is being used should be labeled with felt-tip pen; this avoids confusion and will help the laboratory staff.
3. Substances and procedures hazardous to health 3.1. Where a potential hazard exists in a particular practical, this will be discussed in the talk before
the practical and details of safe working methods will be highlighted in the practical notes. 3.2. Students must NOT use unfamiliar equipment or procedures without them having been given
instruction. All safety instructions given in the preliminary talk and practical notes must be adhered to.
3.3. Mouth pipetting is forbidden for acids, bases and hazardous fluids. 3.4. All hazardous materials are deposited in a fume cupboard. 3.5. Never use toxic substances without taking the proper precautions and making arrangements for
safe working. Use volatile solvents in a fume cupboard. 3.6. Broken glassware must be placed in one of the special bins provided in the laboratory. 3.7. Used plastic pipette tips must be placed in the appropriate labeled container on the bench.
4. Waste
4.1. Bench should be left waste-free and tidy at the end of each practical – this reduces potential for accidents and spillages and is of considerable help to the laboratory staff.

4
4.1.Laboratory equipment must be left clean after the practical. The supervisor of the chief technician instructs about the place of test-tube or flask washing.
5. Accidents 5.1. All accidents and spillages, including any personal injuries and damage caused to equipment,
must be reported as soon as practicable to the supervisor, the chief technician or other technicians.
5.2. Concentrated acid or alkali on the skin: a) flood the splashed surface thoroughly with water and continue until satisfied that no chemical remains in contact with the skin. Soap will help to remove chemical which are insoluble in water; b) remove all contaminated clothing take care not to contaminate yourself in the process.
5.3. Splashes in the eye. Eye protection should be worn for any work where there is a potential hazard but if accident occurs: a) flood the eye thoroughly but gently with water; b) seek medical advice for all eye injuries from chemicals.
5.4. Burns and scalds. Cool affected area by immersing in cold water. Seed is essential. Continue for at least 5 minutes or until pain is relieved.
5.5. Spillages must be cleared up immediately and the area decontaminated; they must NOT be left as a hazard to others.
5.6. A first aid box is located in the preparatory room. Consult a demonstrator or technicians if you need items from the first aid box.
INSTRUCTION ABOUT YOUR RESULTS RECORDING AND PRESENTATION
Students should bring their own notebook or loose-leaf book along to the practical. The description of each practical should be organized in the following order: 1. Title of the practical. 2. Objectives of a practical. 3. Principles of the procedure. 4. Data of measurement and calculations. Graphs are often an essential part of data analysis. They are best plotted as you go along wherever possible. Remember to label axes clearly. 5. Interpretation and conclusions. Conclusions have to correspond to the objectives of practical. Problem solving exercises should be presented in paper-sheets. The first sheet includes: 1. The title of a topic to which the exercises are addressed. 2. Student’s name, surname and the group.3. The date of presentation.

5
Labwork 6.2.
Digestion of lipids. Effect of bile on efficiency of fat hydrolysis by pancreatic lipase Aim: To evaluate the effect of bile on digestion of dietary lipids Objectives:
1. To investigate digestion of lipids by pancreas enzymes 2. To evaluate the effect of bile acids on digestion of lipids by pancreas enzymes 3. To discuss the molecular mechanism of effect of bile acids on digestion of lipids
Pre-lab. Topics must be prepared before the labwork 1. Structure of fats, chemical name (Medical chemistry and Structures of biological
compounds courses) . 2. Hydrolysis of fats (Medical chemistry and Structures of biological compounds courses) . 3. Enzymes of fat hydrolysis. 4. Acid-base titration, role of indicators (Medical chemistry course).
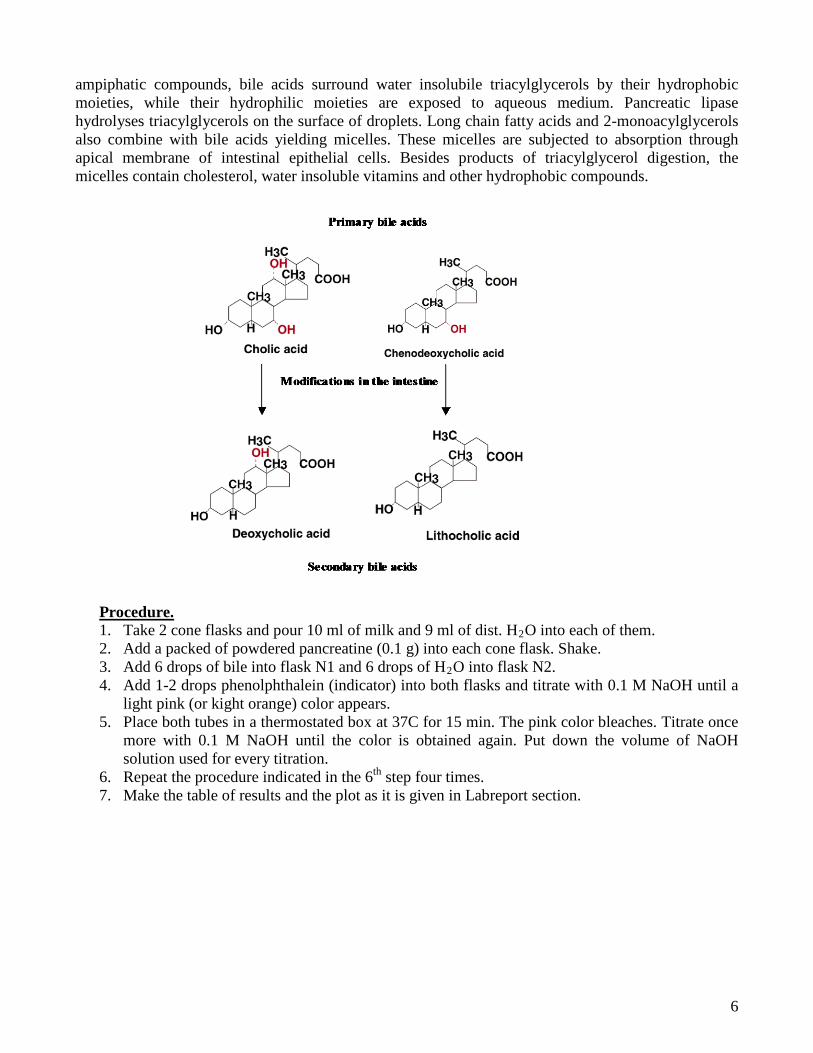
The term “lipid” is applied to fatty, oily and waxy substances of cell. Lipids are practically insoluble in water, but can be dissolved easily in non-polar solvents such as chloroform, ether or benzene. The main route for digestion of dietary triacylglycerols involves hydrolysis to fatty acids and 2-monoacylglycerols in the lumen of the intestine (see the reaction equation below). The major locus of triacylglycerol digestion is the duodenum. Alkaline pancreatic juice secreted into the duodenum raises the pH of the digestive mixture, allowing hydrolysis of the triacylglycerols by pancreatic lipase. Pancreatic lipase cleaves fatty acids from the C-1 and C-3 positions of triacylglycerol. As a result, 2-monoacylglycerol and free fatty acids are the products of hydrolysis. The insolubility of triacylglycerols in aqueous medium presents a problem related with digestion, since digestion can occur only on the surface of fat droplets. Consequently, the rate and efficiency of digestion depends upon the surface area of fat droplets. Emulsification of triacylglycerols by bile acids facilitates the digestion. Bile acids are ampiphatic (diphilic) molecules derived from cholesterol in the liver and secreted from the gall bladder. The bile acids are classified as primary and secondary ones. Bile acids act as detergents by binding to the globules of dietary triacylglycerols as they are broken up by peristaltic action. Being ampiphatic compounds bile acids are important for the emulsification of dietary fats, for the activation of pancreatic lipase and for the absorption of lipids through the intestinal mucose. Being
CH2-O-C-R1
CH2-O-C-R3
R2-C-O-CH
O
O
O + 2 H2O
HCH2-OH
CH2-OH
R2-C-O-CH
O
+ R1-COOH + R3-COOH
Triacylglycerol 2-Monoacylglycerol F tt id
6
ampiphatic compounds, bile acids surround water insolubile triacylglycerols by their hydrophobic moieties, while their hydrophilic moieties are exposed to aqueous medium. Pancreatic lipase hydrolyses triacylglycerols on the surface of droplets. Long chain fatty acids and 2-monoacylglycerols also combine with bile acids yielding micelles. These micelles are subjected to absorption through apical membrane of intestinal epithelial cells. Besides products of triacylglycerol digestion, the micelles contain cholesterol, water insoluble vitamins and other hydrophobic compounds.
Procedure. 1. Take 2 cone flasks and pour 10 ml of milk and 9 ml of dist. H2O into each of them. 2. Add a packed of powdered pancreatine (0.1 g) into each cone flask. Shake. 3. Add 6 drops of bile into flask N1 and 6 drops of H2O into flask N2. 4. Add 1-2 drops phenolphthalein (indicator) into both flasks and titrate with 0.1 M NaOH until a
light pink (or kight orange) color appears. 5. Place both tubes in a thermostated box at 37C for 15 min. The pink color bleaches. Titrate once
more with 0.1 M NaOH until the color is obtained again. Put down the volume of NaOH solution used for every titration.
6. Repeat the procedure indicated in the 6th step four times. 7. Make the table of results and the plot as it is given in Labreport section.

7
Name Family name Group N Year Faculty
Labwork N 6.2.
Title …………………………………………………………………………………………… ………………………………………………………………………………………………… Aim…………………………………………………………………………………………… ………………………………………………………………………………………………… ………………………………………………………………………………………………….. …………………………………………………………………………………………………… Principle of the lab-work … ……………………………………………………………………………………………………………………………………………………………………………………………………………………. ………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………… Equipment and materials…………………………………………………………………………. ……………………………………………………………………………………………………… …………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………… Results and calculations.
Fill the table N.1. Results of titration of milk specimen in the presence of bile
Time of
incubation at
370C
Milk+H2O Milk+bile
Volume of 0,1 M NaOH Volume of 0,1 M NaOH
Added ml Total ml Added ml Total ml
0 min
15 min
30 min
45 min
60 min

8
Make a plot. Total volumes of 0,1M NaOH solution have to be used in Y axis.
Volume
of NaOH (ml)
time of incubation, (min) 0 15 30 45 60 Note. At each time-point of the graph, the volume of NaOH represents the sum of the volume of the last titration and those of former titrations.
Conclusion. References: L. Ivanovienė, R. Morkūnienė, R. Banienė, L. Ivanovas, V. Borutaitė. Laboratory manual on biochemistry, part II, KMU leidykla, Kaunas, 2005, p. 5 – 12. Control questions for practical work defense
1. Be able to draw a reaction of hydrolysis of triacylglycerol (in structural formulas) catalyzed by pancreatine. Characterize pancreatic lipase in terms of enzyme class, specificity and solubility in water.
2. Importance of bile in fat digestion: Active components of bile and their function. 3. Which method has been used for assessment of fat hydrolysis efficiency? How does the method
work? Give a reaction which demostrate principles of hydrolysis evaluation.

9
4. Why was phenolphthalein used as an indicator? 5. Which compouds are released from fats during digestion by pancreatic lipase. Draw their
structures. 6. Indicate main causes of positive effect of bile in fat digestion. 7. Consider absorbtion of fat digestion product in intestine. What compounds are essential of
endocytosis? What do they do? 8. Propose what can happen with fat digestion if bile does not enter into duodenuum.

10
Labwork 6.6.
Determination of creatinine in urine. Determination of carbamide (urea) in urine. Aims:
1. To quantify the daily amount of creatinine excreted with urine, to use data obtained to evaluate functional state of skeletal muscle and kidney.
2. To determine the amount of carbamide in urine. 3. To be able to interpret data obtained and to evaluate the efficiency of processes of ammonia
detoxification. Objectives:
1. To learn how to determine the amount of creatinine in urea and to calculate daily amount of excreted creatinine in urine.
2. To get knowledge on metabolism of creatine and creatinine and their biological significance. 3. To understand changes in creatine and creatinine concentrations and how they relate to
physiological and pathological processes. 4. To be able to evaluate changes in creatine and creatinine concentrations and in activity of
isoenzymes of creatine kinase in biological samples during pathological or physiological processes.
5. To get knowledge on metabolic production of ammonia, its toxicity and ways of detoxification in human organism.
6. To learn how to determine the main product of ammonia detoxification – carbamide in biological fluids.
7. To be able to evaluate changes in carbamide concentrations in biological fluids during various pathological processes.
Part1. Determination of creatinine in urine. Creatine is important in energy transport from mitochondria to myofibrils in muscles. In aged cell creatine is converted to creatinine:
Creatinine is excreted with urine. The level of creatinine in urine depends on body mass and intensity of nitrogen metabolism. The latter increases during active physical exercise, lung inflammation, etc. Creatine is absent in urine of healthy persons, but it can appear in the case of kidney disease or muscle atrophy. Procedure.
1. Transfer 2,7 ml of reagent (picric acid + NaOH ) and 0,3 ml of urine (dilution 1:50) to the test tube and shake the contents.
C = NH
NHC = O
CH3 - N
H2C
NH2
C = NHN - CH3
CH2
COOH

11
2. After 20 min. incubation (in room temperature) measure the level of light absorbance at 492 nm wavelength.
3. Calculate creatinine level (g) from the calibration curve. 4. Calculate amount of creatinine excreted per day (daily urination is 1500-2000 ml), express in
g/24 h. 5. Calculate creatinine amount in mmol/l (Mcreatinine= 113,12 g/mol). Normal values: women – 5,3-13,3 mmol/24 val., men – 8,8-17,7 mmol/24 val.
Part 2. Determination of carbamide (urea) in urine. Urea is synthesized in the liver as by-product of the determination of amino acids. It’s elimination in the urine represents the major route for nitrogen excretion. Elevated urea concentration in plasma is found as a result of a high-protein diet, increase protein catabolism, after a gastrointestinal hemorrhage, mild dehydration, shock and heart failure or treatment with glucocorticoids (pre-renal uremia). Post-renal uremia is caused by conditions that obstruct outflow; nephrolithiasis, tumor or prostatic hypertrophy. The usefulness of urea as an indicator of renal function is limited by the variability of its plasma concentration as a result of nonrenal factors. Clinical diagnosis should not be made on the findings of a single test result, but should integrate both clinical and laboratory data. Principle of the method:
Urea in the sample forms a coloured comlex (reactions below), that can be measured spectrophotometrically:
Urea + 2H2O →urease 2NH4+ + CO2
NH4+ + Salicylate + NaOCl → idenitropruss
Indophenol Reagents: A reagent: sodium salicylate 62 mmol/l, sodium nitroprusside 3,4 mmol/l, phosphate buffer 20 mmol/l, urease > 500 U/ml, pH 6,9. B reagent: sodium hypochlorite 7 mmol/l, sodium hydroxide 150 mmol/l. S Urea Standart solution Procedure:
1. Pippete into labelled test tubes:
Blank Standart Sample Urea Standart S Sample A Reagent
_ _
1,0 ml
10 µl _
1,0 ml
_ 10 µl
1,0 ml 2. Mix thoroughly and incubate the tubes for 10 min at romm temperature (16-25°C) or 5 min at
37°C temp. 3. Pipette:
B Reagent 1,0 ml 1,0 ml 1,0 ml

12
6. Mix thoroughly and incubate the tubes for 10 min at romm temperature (16-25°C) or 5 min at 37°C temp.
7. Read the light absorbance of Standart and the Sample at 600 nm light wave length against the blank.
8. Calculate urea concentration in the sample using the following formula:
×× tdarSdartS
Sample CAA
tantan
Sample dilution factor = Сsample
If the Urea Standart provided has been used to calibrate: Serum and plasma Urine
darts
sample
AA
tan
×50 = mg/dl urea ×23,3 = mg/dl BUN ×8,3 = mmol/l urea
×2500 = mg/dl urea ×1165 = mg/dl BUN ×415 = mmol/l urea
BUN (blood urea nitrogen) Reference values: Serum and plasma: 15-39 mg/dl urea = 7-18 mg/dl BUN = 2.5-6.5 mmol/l urea. Concentrations in the neonatal period are lower, and in adults over 60 years of age are higher. Concentration also tend to be slightly higher in males than in females. Urine: 26-43 g/24-h urea = 12-20 g/24 h BUN = 428-714 mmol/24 h urea.
13
Name Family name Group N Year Faculty
Labwork N 6.6.
Title …………………………………………………………………………………………… ………………………………………………………………………………………………… Aim…………………………………………………………………………………………… ………………………………………………………………………………………………… ………………………………………………………………………………………………….. …………………………………………………………………………………………………… Principle of the lab-work … 1. Determination of creatinine in urine. …………………………………………………………………………………………………………………………………………………………………………………………………………………… 2. Determination of carbamide (urea) in urine.…………………………………………………………… ……………………………………………………………………………………………………… ……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………… Equipment and materials…………………………………………………………………………. ……………………………………………………………………………………………………… ……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………… Results and calculations. 1. Determination of creatinine in urine.

14
Calibration curve for determination of creatinine
2. Determination of carbamide (urea) in urine.………………………………………… Conclusion.

15
Control questions for practical work defense Part I. 1. What is creatinine? Where does it come from? 2. Which method is used to determine creatinine? 3. Which parameter has to be found for calculation of creatinine amount? 4. What is clinical significance of creatinine determination in urine? 5. What can you suppose if creatinine excretion is enormously high? 6. What can you suppose if creatinine excretion is enormously low? Part II.
1. In terms of human physiology, what is urea? Be able to draw the structural formula of urea. 2. What is normal concentration of urea in blood serum? 3. How is condition of high urea concentration reffered? 4. What is the principle of urea determination in laboratory? 5. Be able to draw the reactions implicated in spectrophotometric determination of urea? Why is
light absorbace changed? 6. Be able to explain meaning of presence of urase in reagents of urea determination?
References: L. Ivanoviene, R. Morkuniene, R. Baniene, L. Ivanov, V. Borutaite. Laboratory Manual on Biochemistry, part 2, Kaunas, 2005, p. 39-41

16
Labwork 6.9.
Determination of cholesterol concentration in blood serum. Determination of cholesterol, high density lipoproteins, low density lipoproteins and tiacylglycerols by
automatic analyzer Cardio-Check. Aim: To learn how to determine and to calculate cholesterol and its transferring lipoprotein concentrations in human blood serum as well as to interpret obtained results. Objectives:
1. To determine concentration of cholesterol in human blood plasma by Ilck. 2. To calculate concentration of cholesterol in both systemic and non-systemic units. 3. To determine concentrations of cholesterol, high density lipoproteins, low density lipoproteins
and triacelglycerols in blood serum by automatic analyzer. 4. To evaluate the results and to interpret them.
Cholesterol is cyclic compound whose structure is shown below:
OH
CH3
CH3
CH3
CH3
CH3
In spite of a very low solubility of cholesterol in water, it has high solubility in blood owing to the presence of lipoproteins (called plasma lipoproteins) with high affinity to cholesterol. 1. Determination of cholesterol concentration in blood serum by enzymatic method.
Principle of the method: Free and esterified cholesterol in the sample forms a coloured complex (reactions below), that can be measured spectrophotometrically:
Cholesterol + ½ O2 Cholestenone + H2O2
2 H2O2 + 4-aminoantipyrine + Phenol Peroxidase Quinoneimine + 4 H2O
Cholesterol esterase
+ Free fatty acid
Cholesterol ester (cholesterol stearate) Cholesterol Cholesterol oxidase
1.
2.
3.

17
Reagents: A reagent: PIPES (piperazin-N-N'-bis [2-etansulphonic acid]) 35 mmol/l, phenol 28 mmol/l, cholesterol esterase 0,2 U/ml, cholesterol oxidase 0,1 U/ml, peroxidase 0,8 U/ml, 4-aminoantipyrine 0,5 mm.l/l, pH 7.0 S Cholesterol Standart Darbo eiga:.
1. T ake 2 test tubes (standart and sample) and pipette 1 ml reagent A into both labelled tubes 2. Pipette 0,01 ml of Cholesterol standart (concentration 200 mg/dl, 5,18 mmol/l) into Standart
tube. 3. Pipette 0,01 ml of blood serum into Sample tube. 4. Mix thoroughly and incubate the tubes for 10 min at room temperature (16-25°C) or 5 min at
37°C temp. 5. Read the absorbance of Standart and the Sample at 500 ± 20 nm against the blank. 6. Calculate cholesterol concentration in the sample using the following formula:
ASample AStandart
Reference values: Desirable: up to 200 mg/dl (5.2 mmmol/l) High: >240 mg/dl (6.24 mmmol/l)
× CStandart = CSample

18
Name Family name Group N Year Faculty
Labwork N 6.1.
Title …………………………………………………………………………………………… ………………………………………………………………………………………………… Aim…………………………………………………………………………………………… ………………………………………………………………………………………………… ………………………………………………………………………………………………….. …………………………………………………………………………………………………… Principle of the lab-work … 1. Determination of cholesterol concentration in blood serum by enzymatic method. ……………………………………………………………………………………………………………………………………………………………………………………………………………………2. . …………………………………………………………………………………………………………………………………………………………………………………………………………………………22. Determination of cholesterol, high density lipoproteins, low density lipoproteins and tiacylglycerols by automatic analyzer Cardio-Check. ………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………… Equipment and materials…………………………………………………………………………. ……………………………………………………………………………………………………… ……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………… Results and calculations. 1. Determination of cholesterol concentration in blood serum by enzymatic method. 2. Determination of cholesterol, high density lipoproteins, low density lipoproteins and tiacylglycerols by automatic analyzer Cardio-Check.

19
What does the test result mean? In Adults: Total Cholesterol: Desirable: Less than 200 mg/dL (5.18 mmol/L) Borderline high: 200-239 mg/dL (5.18 to 6.18 mmol/L) High: 240 mg/dL (6.22 mmol/L) or higher LDL Cholesterol: Optimal: Less than 100 mg/dL (2.59 mmol/L) Near/above optimal: 100-129 mg/dL (2.59-3.34 mmol/L) Borderline high: 130-159 mg/dL (3.37-4.12 mmol/L) High: 160-189 mg/dL (4.15-4.90 mmol/L) Very high: Greater than 190 mg/dL (4.90 mmol/L) HDL Cholesterol: Low level, increased risk: Less than 40 mg/dL (1.0 mmol/L) for men and less than 50 mg/dL (1.3 mmol/L) for women Average level, average risk: 40-50 mg/dL (1.0-1.3 mmol/L) for men and between 50-59 mg/dl (1.3-1.5 mmol/L) for women High level, less than average risk: 60 mg/dL (1.55 mmol/L) or higher for both men and women Fasting Triglycerides: Desirable: Less than 150 mg/dL (1.70 mmol/L) Borderline high: 150-199 mg/dL(1.7-2.2 mmol/L) High: 200-499 mg/dL (2.3-5.6 mmol/L) Very high: Greater than 500 mg/dL (5.6 mmol/L) Conclusion. Control questions for practical work defense
1. Be able to draw structural formula of cholesterol. Characterize cholesterol in terms of solubility and stability.
2. What is origin of cholesterol in bood serum? 3. What method is used for determination of cholesterol amount in blood serum? 4. Be able to make the outline of cholesterol determination? 5. According to which compound amount can be the amount of choletrol determined? 6. What is physiological norm of cholesterol concentration in blood serum? 7. How is condition of high colestrol level called? 8. What is clinical significance of cholesterol amount determination?
References: L. Ivanovienė et al. Laboratory Manual on Biochemistry. KMU leidykla, Kaunas, 2005, p. 22-24.
20
Labwork 6.12. Protein digestion by pepsin.
Analysis of gastric juice. Aim: To identofy optimum conditions for action of gastric pepsin. To determine gastric juice acidity. Objectives:
1. Evaluate effect of hydrochloric acid on pepsin action. 2. Evaluate factors that can cause pepsin inactivation. 3. To know molecular mechanism of pepsin action. Perform quantitative analysis of gastric juice. 4. Calculate acidity of gastric juice. 5. Acquit with essential types of gastric juice and its clinical importance. Determine pathological
compounds of gastric juice. Part 1.
Protein digestion. Effect of pepsin. Proteins are broken down by hydrolases with specificity for the peptide bond - peptidases. The
process of protein digestion can be divided into a gastric, a pancreatic and an intestinal phase, depending on the source of peptidases. Proteolysis begins in the stomach, where gastric HCl acidifies the food to pH 2-3, the optimum pH for the proteolytic enzyme pepsin. The major gastric protease, pepsin A prefers peptide bonds formed by amino group of aromatic acids (Phe, Tyr). The products of pepsin action are large peptide fragments and some free amino acids. Pepsin is endopeptidase. After hydrolysis of fibrine by pepsin the mixture of different length peptides is formed. This can be determined by biuret reaction.
Procedure.
1. Take 5 test tubes and mark them. Pour the volumes of solutions into each tube as indicated in the table below. Add neutralized pepsin solution (~ pH 7) into the tube No.1. Use 1% NaHCO3 for this purpose and check pH by litmus as indicator. Add boiled pepsin into the tube No.4.
2. Add fibrine crumb into each of the tubes. Shake and put into a thermostated box (at 37oC) for 60 min.
3. Filtrate the reaction samples. Take about 1ml (10 drops) of each filtrated sample and perform biuret reaction.
4. Biuret reaction: add 5 drops of 10% NaOH and 1 drop of 1% CuSO4 into the test tube containing 10 drops of peptide solution. Shake. Violet-blue color appears in the presence of peptides.
5. Record the results of biuret reaction in the table (see below).
Part 2.
Analysis of gastric juice.
Determination of total acidity. Total acidity is expressed as a volume (ml) of 0.1 M NaOH used for the titration of 100 ml gastric juice. Normal level of gastric juice acidity is equal to 40-60.

21
Procedure. Pour 10 ml of gastric juice into the cone flask and add 1-2 drops of indicator phenolphthalein. Titrate with 0.1 M NaOH until a pink color appears. Put down the volume of NaOH used for titration and calculate this volume for 100 ml of gastric juice. Calculation. Let us assume that 5 ml of 0.1 M NaOH have been consumed to titrate 10 ml of gastric juice, then the total acidity is 5 × 100 / 10 = 50 units. Determination of free chloric acid. Hydrochloric acid is secreted by the parental cells at a concentration of approximately 0.07-0.17%. The concentration of free hydrochloric acid is determined by titration with 0.1 M NaOH. Free acidity is expressed as a volume of NaOH used for titration and calculated for 100 ml of gastric juice and in percentage. Procedure: Pour 10 ml of gastric juice into the flask and add 2-3 drops of 5% dimethylaminoazobenzene. Titrate with 0.1 M NaOH until constant yellow color is obtained. Express free acidity in the same way as total and in percentage. Combined acidity. The old term “combined acidity” stems from the fact that some amount of acid is bound to or reacted with other substances, especially proteins. Combined acidity is calculated as difference of total and free acidity.

22
Name Family name Group N Year Faculty
Labwork N 6.1.
Title …………………………………………………………………………………………… ………………………………………………………………………………………………… Aim…………………………………………………………………………………………… ………………………………………………………………………………………………… ………………………………………………………………………………………………….. …………………………………………………………………………………………………… Principle of the lab-work … 1. Protein digestion. Effect of pepsin. …………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………… 2. Analysis of gastric juice. ………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………… Equipment and materials…………………………………………………………………………. ……………………………………………………………………………………………………… …………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………… Results and calculations. Fill the data table
Protein digestion by pepsin. No of test tube
Volume of pepsin (ml)
Volume of 0.2% HCl (ml)
Volume of H2O (ml)
Protein Result of biuret reaction
1. 2. 3. 4. 5.
5.0 -
2.5 2.5 -
- 5.0 2.5 2.5 -
- - - -
5.0
fibrine fibrine fibrine fibrine fibrine

23
2. Analysis of gastric juice. Conclusion. References: Ivanovienė L, Morkūnienė R, Banienė R, Ivanovas L, Borutaitė V. Laboratory manual on biochemistry. Part 2, KMU leidykla, Kaunas, 2005, p. 27–33. Control questions for practical work defense Part I.
1. Be able to characterise pepsin in terms of enzyme classification, specificity and optimum conditions.
2. Why is fibrin used in this experiment? Can we use albumin insted? Explain wy yes or no. 3. What does pepsin do with fibrin? In general terms name the products of fibrin digestion. 4. What happened with pepsin when you boiled its solution? 5. Why is biuret test convienient for determination of pepsin action. 6. According to your results, in which condition pepsin action was most efficient? Explain why.
Part II. 1. What is origin of HCl in gastric juice? 2. What are function of HCl in stomach? 3. Which types of acidity of gastric juice you know? 4. Which one of acidity types is of greates clinical importance? 5. How did you determine acidity of gastric juice in laboratory? Be able to write equation used for
HCL determination. 6. Why were two kineds of indicators used? Explaine the reason of choise of those indicators.





























