Embed Size (px)
Citation preview

Module.05
ClinicalNutrition This module is designed especially for veterinary nurses and covers the therapeutic role of diet in a variety of clinical disorders and during periods of stress or injury. It is assumed that you have already completed the course of study contained in modules 1 to 4.
Now that you have learned about the fundamentals of feeding healthy dogs and cats, the clinical nutrition module is designed to explore some of the more complex issues which arise in cat and dog nutrition. In this course we take a look at the major clinical conditions of dogs and cats in which diet, and the use of special veterinary diets, is an important part of the management of the condition.
Module.05

Module.05
Module.05Table of Contents
p01 - Conditions Affecting the Digestive System
p02 - Dietary Management of chronic Diarrhoea in Dogs
p12 - Dietary Sensitivity
p20 - Gastric Dilatation-Volvulus
p26 - Other Clinical Nutrition Topics
p27 - Dietary Management of Chronic Renal Failure
p33 - Critical Care Nutrition
p40 - Dietary Management of Obesity
p48 - Dietary Management of FLUTD

Module.05
In this module you will learn about dietary management of diseases which affect the digestive system of dogs and cats. The first topic we cover is the management of chronic diarrhoea. Dogs can suffer from chronic diarrhoea due to a range of causes, but the dietary management of these conditions often has a common basis. The use of low fat diets is examined in detail in this section.
The second area of interest is food allergy in cats and dogs. Wide-ranging research into this topic has been conducted at the WALTHAM Centre for Pet Nutrition, and many of their findings are presented here.
The final topic is canine gastric dilatation/torsion. There has been great interest in this condition from veterinarians and dog breeders, and the role that diet plays will be explained. At the end of this section there is another self test on digestive disorders to test your understanding of topics in this module.
01
Conditions Affecting the Digestive System

Module.05 02
Dietary Management of Chronic Diarrhoea in Dogs
Diarrhoea is one of the most commonly seen ailments in small animal practice. It may be defined as an increase in frequency, volume or fluidity of faeces, but these characteristics can also be affected by dietary changes. Diet plays an important role in the management of chronic diarrhoea, generally in conjunction with appropriate pharmacological therapy.
Diarrhoea may be classified as 'chronic' if it persists for longer than 3-4 weeks. Unlike many acute diarrhoeas, which are either self-limiting or respond to symptomatic therapy, the successful management of chronic diarrhoea is based on establishing a definitive diagnosis and implementing specific therapy.
Causes of Diarrhoea
03Module.05
Large quantities of water enter the gastrointestinal tract, through a combination of oral intake and endogenous secretions. Approximately 95% of this water is reabsorbed from the colon, so a relatively small decrease in absorption (or increase in secretion) can result in increased colonic water content and diarrhoea. A small change in faecal water content from about 70% (normal faeces) to 80% (very loose faeces) can result in a very marked change in faecal character.
Diarrhoea occurs as the result of one or more mechanisms:
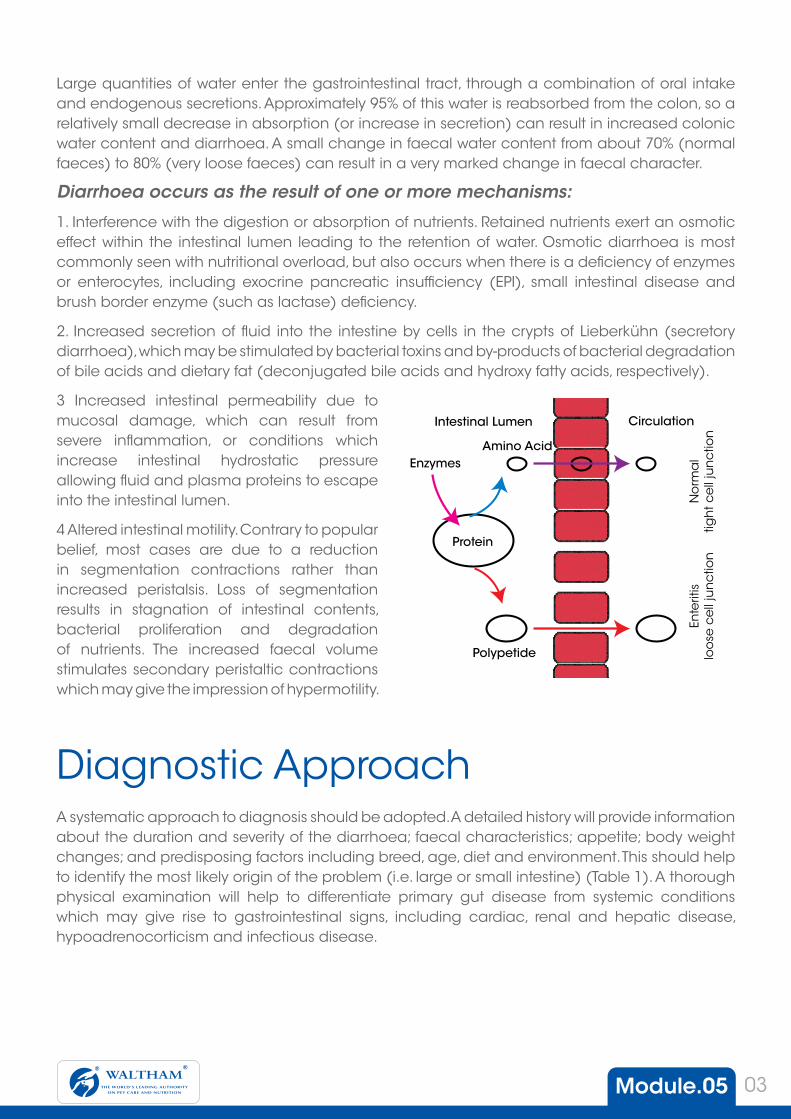
1. Interference with the digestion or absorption of nutrients. Retained nutrients exert an osmotic effect within the intestinal lumen leading to the retention of water. Osmotic diarrhoea is most commonly seen with nutritional overload, but also occurs when there is a deficiency of enzymes or enterocytes, including exocrine pancreatic insufficiency (EPI), small intestinal disease and brush border enzyme (such as lactase) deficiency.
2. Increased secretion of fluid into the intestine by cells in the crypts of Lieberkühn (secretory diarrhoea), which may be stimulated by bacterial toxins and by-products of bacterial degradation of bile acids and dietary fat (deconjugated bile acids and hydroxy fatty acids, respectively).
3 Increased intestinal permeability due to mucosal damage, which can result from severe inflammation, or conditions which increase intestinal hydrostatic pressure allowing fluid and plasma proteins to escape into the intestinal lumen.
4 Altered intestinal motility. Contrary to popular belief, most cases are due to a reduction in segmentation contractions rather than increased peristalsis. Loss of segmentation results in stagnation of intestinal contents, bacterial proliferation and degradation of nutrients. The increased faecal volume stimulates secondary peristaltic contractions which may give the impression of hypermotility.
Intestinal Lumen Circulation
Amino AcidEnzymes
Protein
Polypetide
Ente
ritis
loo
se c
ell
jun
ctio
nN
orm
al
tigh
t ce
ll ju
nc
tion
A systematic approach to diagnosis should be adopted. A detailed history will provide information about the duration and severity of the diarrhoea; faecal characteristics; appetite; body weight changes; and predisposing factors including breed, age, diet and environment. This should help to identify the most likely origin of the problem (i.e. large or small intestine) (Table 1). A thorough physical examination will help to differentiate primary gut disease from systemic conditions which may give rise to gastrointestinal signs, including cardiac, renal and hepatic disease, hypoadrenocorticism and infectious disease.
Diagnostic Approach

Module.05 04
For small intestinal diarrhoeas, further evaluations may include faecal examination; imaging; serum chemistry tests; sugar absorption tests to evaluate enterocyte function and intestinal permeability; breath hydrogen testing; and endoscopy.
For large intestinal diarrhoeas, techniques of particular diagnostic value include faecal examination for parasites and bacteria; endoscopy and histological examination of biopsy samples; radiography and ultrasonography.
Specific causes of small intestinal diarrhoea include: • Exocrine pancreatic insufficiency (EPI)
• Dietary sensitivity
• Neoplasia
• Bile acid deficiency
• Short bowel syndrome
• Small intestinal bacterial overgrowth (SIBO).
• Inflammatory bowel disease (IBD).
• Lymphangiectasia
Diet plays an important role in the management of small intestinal diseases. Although no single diet is appropriate for every condition, diets for the management of conditions involving the small intestine should be highly digestible since many diseases are likely to interfere with digestive and absorptive function.
Fat
Fat is the most complex of the macronutrients to digest and absorb. Hydrolysis of fat depends on the activity of pancreatic lipase and is facilitated by pancreatic co-lipase and bile salts. Bile salts also interact with the products of fat digestion to form mixed micelles, which is the form in which fat is most efficiently absorbed across the intestinal cell wall.
Restriction of dietary fat is recommended in a range of small intestinal diseases:
Exocrine pancreatic insufficiency
Exocrine pancreatic secretions are reduced or absent in EPI, leading to impaired digestion and absorption of fat and, to a lesser extent, carbohydrate and protein.
Small Intestinal Disease
Table 1: Differences between small intestinal and large intestinal diarrhoeaClinical Finding Small intestine Large intestineFrequency of defaecation Normal or slightly increased IncreasedFaecal volume Increased Small amountsUrgency or tenesmus Absent Usually present Blood in faeces Dark blood (digested) Red blood (fresh)Mucus in faeces Usually absent AbundantSteatorrhoea May be present AbsentAppetite Normal or increased Normal or reducedWeight loss May be present Rare but may occur if long term problem

Module.05 05
This results in weight loss, despite a ravenous appetite, and diarrhoea with steatorrhoea (fat in faeces). Bacterial overgrowth is also a common complication of EPI. Management of the condition involves the provision of a low fat, highly digestible diet along with the appropriate amount of pancreatic enzyme replacer.
Small intestinal bacterial overgrowth, because of deconjugation of bile salts, which interfere with micelle formation and fat absorption. In addition, by-products of microbial metabolism of undigested fat may promote a secretory diarrhoea.
Lymphangiectasia, because obstruction of lymphatic vessels hinders fat absorption.
Some inflammatory conditions (eg inflammatory bowel disease), can result in fat malabsorption due to a reduction in surface area of functional enterocytes.
Protein
Moderate to high quantities of good quality protein are recommended since protein malabsorption or protein-losing enteropathy may be a feature of chronic small intestinal diarrhoea. Protein deficiency can further comprimise a diseased intestinal tract by impairing immune function and the luminal barrier, and decreasing formation of brush border enzymes.
Protein is also important in cases of dietary sensitivity since most 'allergens' are proteins. Dietary sensitivity usually presents as skin disease, but gastrointestinal signs may also be present. Sensitivity to dietary protein may also play a part in some cases of inflammatory bowel disease (IBD). In cases of dietary sensitivity, only one or two sources of dietary protein should be used, which are not normally associated with sensitivity reactions.
Carbohydrate
Carbohydrate digestion and absorption can be impaired in conditions that reduce villus height or result in enterocyte damage, including IBD and lymphosarcoma. Damage to brush border enzymes may occur with SIBO. Nevertheless, starch presents a relatively low digestive challenge and is useful for increasing the energy content of low fat diets. Highly digestible sources of carbohydrate, such as rice, are recommended.
Mono- and disaccharides, particularly lactose, should be avoided because they increase the osmotic load in the gut. In addition, lactase and other disaccharidases are brush border enzymes that may be lost.
Dietary fibre
Although dietary fibre such as pectin is commonly used in the non-specific therapy of acute diarrhoeas, it is generally contraindicated in chronic small intestine diseases. Dietary fibre may interfere with digestion and absorption, further compromising an impaired gut.

Module.05 06
Specifically, soluble fibre is contraindicated in EPI since it may reduce the efficiency of pancreatic enzymes by up to 60%. In patients with EPI, even a small reduction in pancreatic enzyme activity can result in a marked decrease in fat absorption.
Vitamins and minerals
Small intestinal diseases may cause deficiencies of B-complex vitamins. EPI increases the risk of cobalamin (vitamin B12) deficiency due to binding of the vitamin by bacteria; decreased pancreatic intrinsic factor, and decreased production of pancreatic proteases. Cobalamin deficiency can also occur with other causes of bacterial overgrowth or malabsorption affecting the distal small intestine.
In contrast, folate deficiency may be induced by conditions affecting the proximal small intestine, including inflammatory bowel disease. Diets for small intestinal disease are, therefore, supplemented with B-complex vitamins. The bioavailability of cobalamin is poor following oral ingestion, so parenteral therapy may be required to correct deficiency states.
Large Intestinal Disease
Dietary fibre
Dietary fibre is of particular interest in large intestinal diarrhoea. Bacterial fermentation of fibres (particularly soluble fibres) within the large intestine yields short chain fatty acids. Of these, acetate and propionate may be absorbed and contribute to the energy balance of the host, whereas butyrate forms the major energy source for colonocytes and is important for colonocyte health and function. In addition, fermentation of fibre increases bacterial numbers which add to faecal bulk. Short chain fatty acids also acidify the colonic environment.
Insoluble fibre tends to be non-fermentable and primarily increases faecal bulk. This may help to stretch colonic smooth muscle and improve contractility and, in addition, may bind faecal water to produce better formed faeces. Diets containing a mixture of both soluble and insoluble fibres tend to normalise transit time and faecal water content, and can therefore be valuable in a number of large intestinal diseases.
Specific causes of large intestinal diarrhoea include parasitism, neoplasia and Clostridium perfringens. In other cases, biopsies will reveal inflammatory changes seen as infiltrations of lymphocytes and plasmacytes, or eosinophils. Some idiopathic cases of large intestinal diarrhoea respond to dietary fibre supplements and are termed 'fibre-responsive' whereas others are classified as functional diarrhoea, also known as 'irritable bowel syndrome'.

Module.05 07
Protein
Since many cases of colitis in dogs are thought to be immune-mediated, hypoallergenic diets may be of benefit, at least in the initial stages of therapy.
Irritable bowel syndrome
Although the clinical signs of 'irritable bowel syndrome' are indistinguishable from colitis, no pathological changes are found on endoscopic examination or biopsy. The condition is associated with stressful situations that lead to altered intestinal motility. Treatment aims to remove the underlying stress factor, although therapy with motility modifiers, spasmolytics or sedatives may also be required. Dietary fibre supplementation may be beneficial in some cases due to its physical properties which help to normalise colonic contractility.
Colitis
Idiopathic (lymphocytic plasmacytic) colitis is the most common cause of chronic large intestinal diarrhoea in dogs which often requires long term management. Anti-inflammatory agents are usually required, at least in the initial stages of therapy, but appropriate dietary management provides an alternative to their long term use. Although the use of fibre-supplemented, meat-based diets has been advocated, attention has recently focused on the use of restricted antigen diets, based on the fact that the disease is immune-mediated.
Studies have shown that canine lymphocytic plasmacytic colitis can be successfully managed using a commercial low residue, 'hypoallergenic' diet, which contained only chicken and rice protein. Similar studies with veterinary low fat or high fibre diets were less successful in the management of chronic colitis in dogs. Using these diets, a greater dependence on anti-inflammatory drugs was required to maintain a clinical improvement that was less marked than with the selected protein diet.

Module.05 08
Clinical StudiesEvaluation of a restricted fat diet in the management of chronic diarrhoea in dogs
The value of a restricted fat diet (Canine Low Fat Diet) in the management of chronic diarrhoea of various aetiologies, was assessed in a study carried out in collaboration with the Department of Veterinary Clinical Studies, University of Edinburgh.
Forty eight dogs, presenting with chronic diarrhoea, were recruited from cases referred to the weekly gastrointestinal clinic within the department. The length of time for which diarrhoea had persisted, despite various attempts at drug and dietary management, varied from 1 month to five years with an average duration of 1.5 years. After a full history, physical examination and clinical work up (which included faecal analysis, blood biochemistry, assessment of digestion and absorption and, where appropriate, intestinal biopsy) had been obtained, the dogs were classified into five diagnostic groups:
(i) small intestinal bacterial overgrowth
(ii) colitis
(iii) exocrine pancreatic insufficiency (EPI)
(iv) idiopathic diarrhoea
(v) malabsorption syndrome
In addition to receiving specific medical therapy for each condition, the low fat diet was gradually introduced into the diets of all dogs over approximately five days until it constituted the entire daily ration. The daily maintenance energy requirement was calculated and offered as the appropriate amount of food in 2-4 equal portions. Each dog was assessed on the initial visit, and 14 selected parameters (which were likely to be adversely affected in dogs with chronic diarrhoea) were monitored on subsequent monthly visits, which continued for up to five months.
Change in Key Clinical Parameters DuringDietary Management of Canine Colitis
StrainingFaecal BloodFaecal mucusFaecal Consistency
100
80
60
40
20
00 1 2 3 4
Scor
e
Month
Parameter Average Change Parameter Average ChangeBodyweight Demeanour
Appetite
(change from 'ravenous'- 'good')
Drinking
Coat Condition Skin Condition
Straining Appearance of faeces
Consistency of faeces Frequency of defaecation
Flatulence no significant difference Copraphagia
Vomiting after meals no significant difference Vomiting (other times)
= significant increase or improvement (p<0.05) = significant decrease (p<0.05)

Module.05 09
Significant improvements were observed in virtually all signs related to chronic diarrhoea within the first month of management, these improvements persisting throughout the five months of the investigation.
Dogs with EPI exhibited the most consistent and marked improvements in response to the management programme; body weight gain and improvement in skin condition were significantly better than in dogs with chronic diarrhoea of other aetiologies (although this probably reflects the poorer condition of dogs with EPI at the initial visit). Faeces consistency in all diagnostic groups was dramatically improved; at initial presentation only 20% of faeces (over all dogs) were of normal consistency, this increased to 83% after one month and to 88% after five months.
The combination of the low fat diet and appropriate drug therapy provided a sound basis for the management of chronic diarrhoea in dogs. As would be expected from the underlying mechanisms, this strategy proved more effective for certain aetiologies; the beneficial effects were most pronounced in dogs with EPI.
Long term management of canine exocrine pancreatic insufficiency
Twenty dogs with confirmed EPI were managed for an initial four month period, allowing specific recommendations for short term management of the condition to be made. In addition,
contact was maintained with the owners of 17 of the dogs for a longer period (up to 39 months); this has permitted observations
of the long term outcome of cases to be monitored (Simpson et al, 1994b).
Initial management of the dogs included a commercial low fat diet (Canine Low Fat Diet) and an enzyme replacer.
The amount of low fat diet offered to the dogs was based on their present, not ideal, body weight, and the daily food
allowance was divided into two meals. The importance of preventing access to other sources of food was stressed to the owners. Using this regimen it was usually possible to restore normal faecal character within 48 hours. At this time daily food allowance and enzyme replacer were slowly increased until the level of diet for
the ideal body weight was reached, without recurrence of diarrhoea. Cimetidine (5 mg/kg 30 minutes before feeding) was provided only in those cases in which diet and enzyme replacer alone were unable to restore faecal character. If, following the restoration of normal faecal character, the amount of food fed was increased too rapidly or the dog managed to scavenge extra food, this resulted in an episode of diarrhoea. In these
situations starvation for 24 hours followed by a slow reintroduction of the regimen normally rectified the problem.
During the initial four month period the average body weight increase was 24% and
in all cases faecal character was restored to normal.

Module.05 10
As the patient’s body weight increased the ravenous appetite tended to decrease in conjunction with improvements in other clinical signs; coprophagia, scavenging, flatulence, poor coat and skin condition. Thus the low fat diet with appropriate enzyme supplementation proved highly effective in initial management of EPI in these dogs.
Long term follow-up also provided some interesting information. Of the 17 dogs with which contact was maintained, only three had been euthanased because of poor progress (another three had been euthanased for unrelated reasons). The remaining 11 dogs were progressing well, with no recurrence of diarrhoea. All had maintained their improved body weight whilst the level of enzyme replacer had been significantly reduced. Four dogs were still receiving Canine Low Fat Diet as their sole source of food and one was receiving it mixed with another commercial relatively low fat canned food. The remaining dogs were receiving a range of other foods, most of which were relatively low in fat. Perhaps the key observation was that the daily requirement for enzyme replacer was less than that required during initial stabilisation, with only approximately 24% (range 6-58%) of the original dose being used. This observation has important implications for the likely long term cost of maintaining dogs with EPI.
Clinical application of a hypoallergenic diet in the management of canine colitis
A study to evaluate a commercial diet in which protein sources were restricted to chicken and rice (Canine Selected Protein Diet) in the management of dogs with idiopathic chronic colitis (ICC) was carried out at the Royal (Dick) School of Veterinary Studies (Simpson et al, 1994a). Eleven cases were recruited from dogs with a history of chronic diarrhoea which were referred to the School’s small animal gastroenterology clinic. In each case, a diagnosis of ICC was made on the basis of clinical findings and endoscopic examination (including colonic biopsy). Any individuals with suspected small intestinal complications were excluded from the study.
Dogs with confirmed, uncomplicated ICC were switched gradually (over a period of several days) from their previous ration to the restricted antigen diet, which was subsequently fed as the sole source of nutrition. In addition, initial management also included the administration of sulphasalazine at a dose of 20-40 mg/kg/day, an anti-inflammatory drug with specific activity in the colon. With remission of clinical signs, drug therapy was phased out. Dogs were maintained on the diet and monitored for a four month period, returning to the clinic for evaluation at approximately monthly intervals. At both the initial and at each subsequent presentation, clinical status and progress were monitored through evaluation of ten different parameters.
Within one month, four key clinical signs associated with colitis (straining, faecal blood, faecal mucus and faecal consistency) were significantly (at least p <0.002) improved and remained so for
Module.05 11
Key Points
the subsequent three months. Furthermore, 60% of the dogs required less, or no, sulphasalazine within one month of commencing therapy, and 90% were stabilised with no drug therapy within two months.
Eight months after the end of the study, the owners reported that all the dogs were still in remission and none were employing any drug therapy at that time. Of the eleven dogs, eight were still being fed Canine Selected Protein Diet exclusively, while the remaining three were experimenting with other diets.
The significant and maintained improvements that were observed in the four primary presenting signs of colitis highlight the success that may be achieved through a combination of a ‘hypoallergenic’ dietary strategy and initial drug therapy. The prognosis for ICC is generally guarded and although clinical signs can often becontrolled with anti-inflammatory drugs, cessation of medication often leads to relapse. This was reflected by the dogs in this study, for which previous management strategies had not been effective. All of these dogs had a history of management involving both dietary change and various drugs over a period of up to 48 months prior to referral.
As with many clinical studies, differentiating between the dietary and drug-related effects of management is not easy when the two have been administered simultaneously. However, the findings indicate that whilst drugs are useful in combating the initial presenting signs, most cases could be stabilised without drug therapy within a relatively short space of time.
As a general approach in the management of canine colitis, it seems that the highly digestible, ‘hypoallergenic’ characteristics of Canine Selected Protein Diet are particularly appropriate. Successful management in terms of ceasing (or reducing) the requirement for drugs, and providing long term freedom from clinical signs appears a realistic goal in many cases, and indicates that at least a component of the underlying aetiology is being tackled.
• Accurate diagnosis is important for successful management of chronic diarrhoea
• Diets for small intestinal disease should be highly digestible and low in fibre
• Low fat diets are beneficial where there is malabsorption of fat
• Restricted antigen diets are useful for inflammatory and immune-mediated conditions
• Dietary fibre is beneficial for some large-intestinal disorders
• Soluble and insoluble dietary fibres help to normalise faecal consistency and transit time

Module.05 12
Dietary Sensitivity
Dietary sensitivity, or an adverse reaction to food, is a term used to describe a clinically abnormal response to the ingestion of a particular food item. True food allergy or hypersensitivity is an immunological phenomenon, mediated by an antibody, immune complex or cell-mediated response. Where an immunological mechanism cannot be demonstrated, the term food intolerance is more appropriate. Food intolerance may result from an inability to adequately digest the food (often because a specific enzyme is lacking) or from pharmacological, metabolic or toxic reactions. Reactions to ingested food components can affect many body systems.
In the dog and cat, adverse reactions to food usually manifest as skin or gastrointestinal disorders and a small proportion of cases will present with signs involving both systems. Respiratory and neurological signs are rare signs of dietary sensitivity in the dog. Neurological signs that have been attributed to dietary sensitivity in dogs include hyperaesthesia and hyperactivity, and epileptiform seizures. Signs that have been attributed to dietary sensitivity in cats include hyperaesthesia and hyperactivity, and feline asthma.

Module.05 13
In many cases, food intolerance is caused by a dietary idiosyncrasy, in which the animal is unable to digest or otherwise process a dietary component, but other mechanisms may be involved. For example, certain foods may contain a pharmacologically active chemical, or may cause the release of inflammatory mediators such as histamine. Some examples of histamine-releasing foods include fish, shellfish, chocolate and egg white.
Many cases of food intolerance present with clinical signs that are compatible with allergic disease and in practice, a distinction between the two is seldom made. Occasionally, the clinical picture may be confused by the presence of both immunological and metabolic reactions. Whatever the cause of the reaction, management protocols are similar for all cases of dietary sensitivity.
IncidenceThe reported incidence of dietary sensitivity varies considerably but most authors agree that it is a rare cause of skin disease in dogs and cats. It has been estimated that dietary sensitivity accounts for approximately 1% of all canine and feline skin conditions in general practice. In dogs it is involved in 10% of canine allergic skin disease, excluding flea allergic dermatitis, 10% of all non-seasonal dermatitis, and 10-20% of allergic dermatoses seen by referral dermatologists. In cats it accounts for 10% of all non-seasonal dermatitis, 10-20% of allergic dermatoses seen by referral dermatologists, and approximately 11% of feline miliary dermatitis cases.
Gastrointestinal signs of dietary sensitivity often go unreported because the owner may associate diet with disease and remove the offending food without seeking veterinary advice. A combination of gastrointestinal and dermatological signs is reported to occur in 10-15% of dogs with food hypersensitivity. In a recent study of 20 dogs with dermatological signs of food hypersensitivity, 60% had increased faecal frequency, commonly accompanied by faecal mucus and blood, that resolved on introduction of an elimination diet. Nevertheless only 20% of the dogs had gastrointestinal signs that had been considered severe enough to warrant previous veterinary consultation.
The true incidence of dietary sensitivity may be difficult to establish due to the problems in reaching a definitive diagnosis. In practice, the condition may be overdiagnosed because of an unwillingness to rechallenge with the original diet. Furthermore, skin disease frequently has a multifactorial cause and successful management of one aspect of disease may be sufficient to drop below the clinical threshold, causing an improvement in clinical signs. Investigation of other possible causes may then be discontinued at that point.

Module.05 14
Allergenic SourcesMost basic food ingredients have the potential to induce an allergic response, including proteins, lipoproteins, glycoproteins, lipopolysaccharides and carbohydrates. Nevertheless, proteins are the most commonly reported allergens, whereas food intolerance may be associated with any dietary ingredient.
In dogs, cow’s milk, beef and cereal (either alone or in combination) account for more than half of the reported cases. In cats, cow's milk and beef are the most commonly reported allergens. It is noteworthy that the majority of animals with dietary sensitivity react to major components of the diet. The frequency with which ingredients have been implicated may simply reflect their common use in traditional commercial and home-prepared canine diets.
Dermatological SignsDogs
The major presenting sign of food sensitivity in dogs is a pruritic skin disorder. This results in a gradation of signs ranging from saliva staining of the hair to severe self-trauma and a variety of secondary skin lesions.
Unilateral or bilateral otitis externa may be a feature and may occur in the absence of other signs of skin disease. The presence of urticaria is highly suggestive of food hypersensitivity. Occasionally, dogs will be non-pruritic and exhibit only seborrhoea.
Cats
There is no classic set of skin lesions for food sensitivity in cats. However, pruritus with excessive licking and scratching may be evident in over 90% of cases. Skin lesions commonly associated with food sensitivity in cats include
• Facial and neck pruritus, which is the most common presenting sign, leading to excoriation of the face
• Local or generalised scales or crusts, particularly around the neck
• Miliary dermatitis, with lesions particularly affecting the ears, head and neck
• Symmetrical or localised areas of alopecia
• Eosinophilic granuloma complex, particularly eosinophilic plaques
• Otitis externa
In one study, three of 14 cats with food allergy had concurrent flea bite hypersensitivity, flea collar hypersensitivity or atopy, which all contributed to the pruritus and skin lesions.

Module.05 15
The condition may mimic other skin disorders including atopy, allergic contact dermatitis and flea allergy. Furthermore, skin disease is often multifactorial and clinical signs are usually a sign of more than one underlying mechanism. Removal of one of these contributory factors may be sufficient to eliminate the symptoms.
Gastrointestinal SignsGastrointestinal signs, including vomiting and diarrhoea, may occur in dogs and cats with dietary hypersensitivity, either concurrently with skin lesions or as a separate entity.
Certain forms of food intolerance, notably lactose intolerance and gluten-sensitive enteropathy, usually manifest as diarrhoea. In addition, a number of chronic conditions of the gastrointestinal tract have been reported in which dietary hypersensitivity may play a role. These include:
• canine idiopathic chronic colitis
• canine eosinophilic gastroenteritis
• canine lymphocytic-plasmacytic enteritis
Gluten enteropathy of Irish Setters is a malabsorption syndrome that responds to removal of wheat (and hence gluten) from the diet. An impairment of the mucosal barrier has been demonstrated in affected animals, but it is not yet clear whether this condition has an immunological basis or if it is attributable primarily to other mechanisms of food intolerance.
Gastrointestinal manifestations of dietary sensitivity in cats include
• vomiting
• profuse watery diarrhoea
• inflammatory bowel disease, including lymphocytic-plasmacytic colitis
DiagnosisThe primary goal in the treatment of dietary hypersensitivity and intolerance is to provide a diet which is balanced and on which the patient is asymptomatic. This involves identification of the offending allergen and its removal from the diet.
Specific tests for diagnosing food hypersensitivity using immunological techniques are available, but they are unreliable in companion animals. Intradermal testing with food extracts, radioallergosorbent testing (RAST), enzyme-linked immunosorbent assay (ELISA) and gastroscopic food sensitivity testing have all been used but although they may help to rule out a specific diagnosis, their positive predictive value is still relatively low.

Module.05 16
Although it does not identify the underlying mechanism of disease, the most useful and reliable method of diagnosing dietary sensitivity is to feed an elimination diet followed by dietary challenge with a test meal. A detailed list of the animal’s diet should be compiled, which should aim to include everything that the animal has eaten in the preceding four weeks and should outline what it has eaten during its lifetime. By studying the list, it may be possible to identify foods which have not previously been fed and which may form the basis of an elimination diet that is ‘hypoallergenic’ for the individual.
The elimination diet should, ideally, contain no ingredients that have previously been consumed by the animal (certainly none that have been eaten in the preceding month) and should be formulated using single sources of protein and carbohydrate. The diet must be nutritionally complete and balanced, since prolonged feeding may be necessary and this should be achieved using a minimum number of ingredients, which may also provoke sensitivity reactions.
Elimination diets that have been successfully used for dogs include lamb, chicken, rabbit and fish as sources of protein and these are typically fed with rice or potatoes as a source of carbohydrates. In cats, elimination diets that have been successfully used include lamb, chicken, rabbit, venison and fish as sources of protein, which are typically fed with rice. There is no single diet that will be ‘hypoallergenic’ in every case. A small number of animals will react to commercially prepared elimination diets but not to home prepared diets using the same ingredients and it may be preferable to use a home prepared diet in the initial diagnostic stages. Cats have an additional specific dietary need for taurine. To ensure this need is met with home prepared diets, all cooking juices from the meat component of the diet should be fed or the diet should be otherwise supplemented.
During the diagnostic period, there should be no access to any other source of nutrients including treats or chews. Ideally, cats should be confined indoors to prevent them from supplementing their diet from other sources. In those parts of the world where heartworm is endemic in dogs, consideration should be given to using an alternative preventative medication for the duration of the trial. Distilled or bottled drinking water is preferable to tap water in this diagnostic phase, as fungal contaminants and chemicals in tap water are potential allergens.
Historically, it has been recommended to feed the elimination diet for a minimum of three weeks. Most dogs and cats with dietary sensitivity will respond within that time, but a trial period of up to 10 weeks may be necessary in some animals, and it is

Module.05 17
advisable to feed the elimination diet for a period of 10 to 12 weeks. Failure to respond within this time suggests that either:
• dietary sensitivity is not involved
• other factors may be contributing to the clinical disease
• the animal is sensitive to the protein in the elimination diet
• there may be poor owner compliance
If clinical improvement occurs, a diagnosis of dietary sensitivity may be confirmed by challenging with the original diet and demonstrating a worsening of clinical signs (particularly pruritus) within 1—14 days. This procedure also helps to establish the time interval between challenge and relapse. However, many owners are unwilling to rechallenge with the original diet since they are reluctant to re-subject the animal to the clinical signs.
Reintroduction of the elimination diet should result in an improvement in signs. At this stage, it may be possible to introduce a commercially prepared diet with the same ingredients, which is more suitable for long-term feeding. The elimination diet will form the basal diet for subsequent test meals. Individual protein sources can then be introduced at weekly intervals (or longer, depending on the previously determined challenge to relapse interval) to identify specific dietary allergens that should be avoided.
Dietary ManagementOnce a diagnosis has been established, it is usually possible to manage cases of dietary sensitivity using commercial diets with novel, restricted protein sources. Alternatively, it may be possible to identify a range of standard products that the animal is able to tolerate. Rarely, formulation of a suitable diet may be difficult because the animal develops multiple sensitivities to proteins as they are sequentially introduced into the diet.
The small number of cases that cannot tolerate any commercial diet must be maintained indefinitely on a home-prepared diet on which they are asymptomatic, but care must be taken to ensure that the diet is nutritionally balanced and complete.
Anti-inflammatory agents, such as corticosteroids or antihistamines, may be necessary in the diagnostic phase if the pruritus is severe in order to break the initial ‘itch-scratch-lick’ cycle. Once the appropriate dietary modifications have been made, there are few indications for the continued use of these drugs. However, they may be required in the following situations:
• poor owner compliance
Before Dietary Management
With Dietary Management

Module.05 18
• development of multiple food sensitivities
• concurrent atopy or other allergic disease
Dietary sensitivity should be regarded as a dynamic and fluctuating condition. Some patients may subsequently develop additional sensitivities necessitating a further change of diet and in others, it is possible for the sensitivity to diminish or disappear.
Clinical StudiesFood allergy and intolerance in dogs
In a study involving dogs attending a dermatology referral clinic, the value of Canine Selected Protein Diet (equivalent to WALTHAM Canine Sensitivity Control) in the management of clinical cases of dietary sensitivity was assessed. For each case, a home prepared ‘hypoallergenic diet’ of either chicken and rice or turkey and rice was introduced following a full clinical examination to eliminate other causes of skin disease. In all dogs, an improvement in clinical signs occurred within three weeks and the diagnosis was confirmed after challenge with the original diet. Subsequently, the dog’s response to the commercial diet was assessed and further provocative challenge studies were performed to identify the offending food ingredient. Twelve out of sixteen (75%) clinical cases of dietary sensitivity were successfully managed with Canine Selected Protein Diet.
Use of a limited protein source diet in the management of dogs with atopy
Twelve perennially affected atopic dogs maintained in clinical remission on oral, alternate day, low dose, prednisolone therapy were entered into a six month, open, crossover study. The dose of prednisolone had been kept largely stable and the dogs had been maintained on a variety of commercial diets for the two months prior to the study period. None of the dogs had improved after a three week trial with a home prepared, restricted diet of chicken, rice and water. Dogs were randomly assigned to one of two groups, and fed either a commercial diet in which protein sources were limited to chicken and rice (Canine Selected Protein Diet), or a control diet which was a canned food based mainly on fish, maize and wheat. Each diet was fed for three months before crossover, when the diets were reversed. Dogs were evaluated every four weeks for the dose of prednisolone required to control their clinical signs and for clinical score of pruritus, erythema, interdigital oedema, alopecia, self trauma and coat condition. Prednisolone dose and total clinical score were significantly (p<0.05) reduced in the dogs when Canine Selected Protein Diet was fed, compared with when the control diet was fed. In addition, prednisolone dose and total clinical score were significantly lower (p<0.05) at the mid point of the study, compared with the beginning, in the group of dogs receiving Canine Selected Protein Diet.
These data indicate that Canine Selected Protein Diet can provide significant benefits in the management of canine atopy, as measured by changes in the dose of anti-inflammatory drugs required to maintain remission of clinical signs.
Prevalence and causes of food sensitivity in cats with chronic pruritus, vomiting or diarrhoea
A study was conducted at the Massey University Small Animal Clinic, New Zealand to determine the prevalence of dietary sensitivity in cats with pruritic skin disease and/or gastrointestinal signs, and to identify the dietary components responsible for these sensitivities. A total of 128 cats were

Module.05 19
presented with the primary complaints of pruritus (n = 61), chronic vomiting (n = 29), diarrhoea (n = 26) or concurrent pruritus and vomiting or diarrhoea (n = 12) and underwent a standardised diagnostic protocol.
Dermatological cases were first screened for other causes and if no diagnosis was reached, then placed on an elimination diet for a minimum of four weeks, using a commercial diet in which protein sources were limited to chicken and rice or venison and rice. If signs recurred following rechallenge with the original diet, the elimination diet was reintroduced for 2-4 weeks until signs resolved. At this stage, a diagnosis of dietary sensitivity could be made and oral challenge tests were conducted to identify the food item responsible. Gastrointestinal cases were screened using a range of procedures to eliminate other possible causes and if no diagnosis was made, elimination diet trials were conducted as for the dermatological cases.
Twenty two of the 128 cats (17%) were confirmed as food sensitive. Within each category of presenting signs, food sensitivity was diagnosed in ten cats with pruritus (16%), three cats with vomiting (10%), four cats with diarrhoea (15%), and five cats with concurrent pruritus and gastrointestinal signs (42%). A variety of foods were found to be responsible for the sensitivity, including dry foods (6), canned foods (4), beef (5), lamb (3), chicken (1), milk (1), fish (1), viscera (1), gluten (1) and food additives (1).
The prevalence of food sensitivity in this study is relatively high compared with some, but not all, previous reports and may reflect a regional variation in the prevalence of food sensitivity or a more rigorous diagnostic effort from referring veterinary surgeons. Cats with concurrent dermatological and gastrointestinal signs had the highest prevalence of food sensitivity. A number of cases resolved with the elimination diet but signs did not recur following rechallenge with the original diet. These cats were not diagnosed as food sensitive and this highlights the need for rechallenge in confirming a diagnosis.
Key Points• Adverse reactions to foods may result from an inability to adequately digest the food or from
allergic, pharmacological, metabolic or toxic reactions
• Dietary sensitivity is relatively rare, accounting for approximately 1% of all canine and feline dermatoses in general practice
• Cow’s milk, beef and cereal (either alone or in combination) are the most commonly reported allergens in dogs
• In dogs, pruritic skin lesions and otitis externa are common signs of dietary sensitivity
• Cats with dietary sensitivity often develop pruritis and lesions around the head, neck and ears
• The most useful and reliable method of diagnosing dietary sensitivity is to feed an elimination diet for up to 10 weeks, followed by dietary challenge with a test meal
• Once a diagnosis has been established, it is usually possible to manage cases of dietary sensitivity using commercial diets with restricted protein sources
Module.05
Gastric dilation-volvulus (GDV) is an life-threatening condition in dogs, in which the stomach fills with gas, stretches and may become twisted or displaced. The displacement often involves the spleen, mesentery and blood vessels adjacent to the stomach.
Gastric Dilatation-Volvulus
20

Module.05 21
A tense, distended abdomen is usually the first sign of GDV, but it is not obvious in every case. The dog with GDV is visibly distressed and may try to vomit or retch. GDV can develop very fast, in just 15 minutes, and progress rapidly into a state of shock, characterised by pale gums, weakness and collapse.
PathogenesisThe gas which accumulates in the stomach of dogs with GDV is mainly swallowed air, combined with a small amount of gas from the stomach. Dogs with GDV seem unable to release these gases from the stomach by the normal means.
If the increased pressure in the stomach is not relieved, poor perfusion rapidly results in gastric necrosis.GDV increases the pressure on the diaphragm and chest cavity, and dramatically reduces the flow of blood back to the heart. This cuts down the output of the heart and reduces vital blood flow to the heart, lungs and the rest of the body, resulting in generalised anoxia. If the stomach also rotates, the tissues of the stomach and nearby abdominal organs may be crushed or seriously damaged by lack of circulation.
Shock develops rapidly, as chemicals are released by the damaged tissues into the circulation. Blood clotting mechanisms may also be disturbed, causing widespread bleeding. Further complications can set in up to a week after the GDV is relieved. The tissues which have been starved of oxygen release toxic substances into the bloodstream which together with reperfusion injury to the myocardium can cause arrhythmias of the heart and injure the tissues of the stomach, intestines and pancreas. Cardiac arrhythmias are observed in up to 40% of dogs with GDV possibly associated with rapid gastric decompression and fluid therapy.
Treatment After diagnosing, the usual treatment procedures are:
1. Emergency decompression and stabilisation
The usual procedure is to put the patient on an intravenous drip to help support blood pressure and intravenous antibiotics. A small trochar may then be use to puncture the stomach through the side of the abdomen to release some of the gas and relieve the pressure. An attempt can then be made to pass a stomach tube, usually under a light general anaesthetic. X-rays may also be taken at this stage to determine whether the patient needs immediate surgery.
2. Surgery to correct twisting and prevent recurrence
In severe cases where the stomach has already twisted, emergency abdominal surgery is required. At surgery, the trapped gases are released, and the stomach may be opened to remove food
Clinical Signs
Fig
ure
1. C
he
st a
nd
ab
do
me
n o
f a d
og
with
GD
V

Module.05 22
material. The stomach is then returned to its normal position, and anchored to the body wall in a gastropexy procedure to prevent the problem recurring. The patient is often in a critical condition, so emergency surgery carries a substantial risk of death from shock, bleeding or cardiac arrest.
Even in cases where the gas is released without surgery, and X-rays show that the stomach has not moved from its normal position, many authors stress the need for a gastropexy to stabilise the stomach and anchor it in position. Once a dog has had an episode of GDV, there is a very high probability of it happening again, sometimes within days, unless some form of gastric stabilising procedure is performed. It is often recommended that this is done within one week of the initial problem.
3. Post-operative treatment
Recovery from surgery for GDV is slow, and intensive hospital care is required for at least 3 days post-operatively. Prolonged intravenous infusions, antibiotic treatment and blood transfusions may be necessary to treat complications, which can set in several days after surgery.
The recovering patient is fed a bland, easily digested diet for at least a week after surgery, then gradually reintroduced to its normal diet during the following week. To minimise stretching of the stomach, food is usually divided into 3 to 4 small meals per day and dogs which tend to bolt down their food may be given a semi-liquid slurry. Exercise is also restricted during the recovery period.
Prognosis The consequences of canine GDV are severe, and it has been estimated that only about 50 per cent of cases of canine GDV make a full recovery. Delays in the diagnosis and treatment of GDV can be critical to the dog's chances of survival
The age of the dog is an important prognostic factor. Although GDV is rare in dogs less than two years of age, dogs that survive an episode of GDV tend to be younger. Their clinical condition at the time of treatment, as judged by their presenting signs and general responsiveness to external stimuli is also critical. The survival rate is also related to the condition of the stomach at the time of treatment; dogs with extensive gastric necrosis generally have a very poor outcome. This indicates that many lives could be saved if dog owners are educated to recognise the early signs of GDV and have access to high quality veterinary emergency treatment.
Some dogs will survive an initial bout of GDV, and then represent within days or weeks. The survival rate from subsequent episodes of GDV is poor. In a study of 103 dogs with GDV treated conservatively, e.g. without surgery, 71% had a recurrence between 5-760 days after initial treatment (3). In another study of 72 dogs with GDV that had a gastropexy performed, only 4 (5.6%) had a recurrence and 3 (75%) of these dogs died. These statistics highlight the role of gastropexy in reducing recurrence and postoperative mortality. Prophylactic gastropexy may be indicated in healthy dogs that are at high risk for GDV based on their large size and a family history of GDV (8).
Module.05 23
Little is known about the causes of GDV. There are probably a number of dietary, genetic and environmental risk factors which all contribute to the development this disease, but no single cause.
Breed
GDV can occur in any breed of dog. Clinical records show that large and giant breeds such as German Shepherds, Great Danes, Dobermanns, Weimaraners and Boxers are more predisposed to GDV than other breeds. However some small breeds with deep, narrow chests such as Dachshunds, also have an increased tendency to develop GDV.
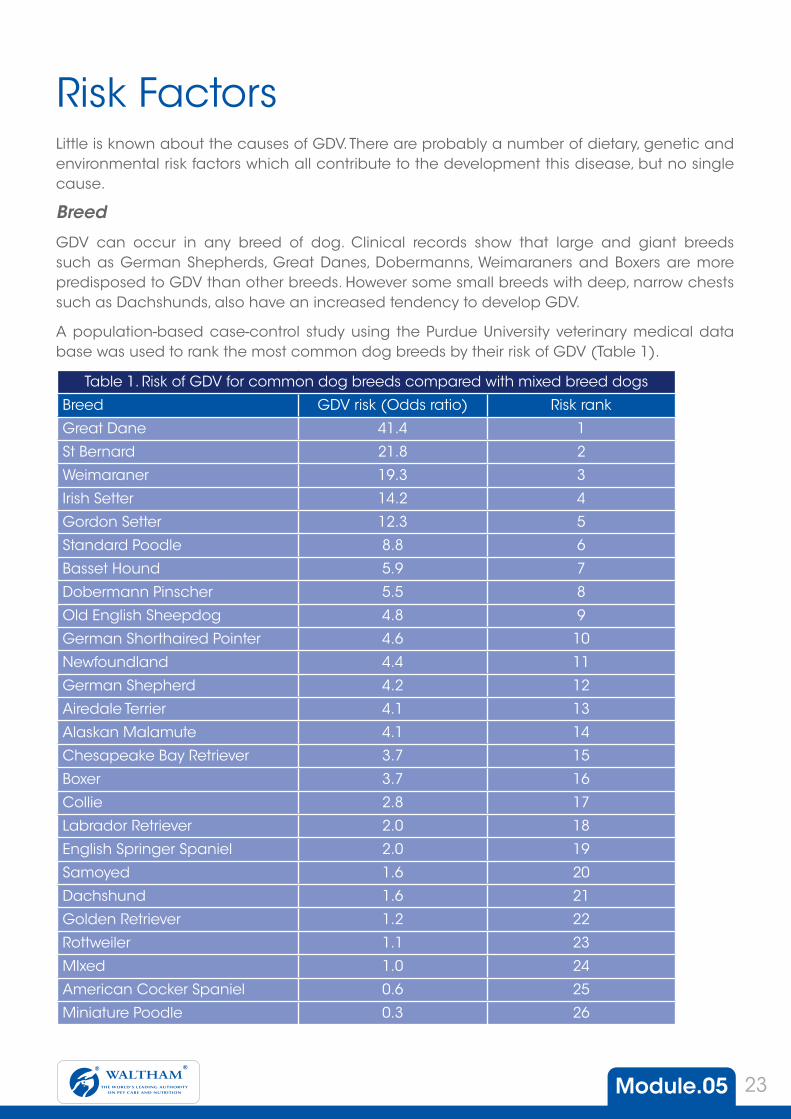
A population-based case-control study using the Purdue University veterinary medical data base was used to rank the most common dog breeds by their risk of GDV (Table 1).
Risk Factors
Table 1. Risk of GDV for common dog breeds compared with mixed breed dogs
Breed GDV risk (Odds ratio) Risk rank
Great Dane 41.4 1
St Bernard 21.8 2
Weimaraner 19.3 3
Irish Setter 14.2 4
Gordon Setter 12.3 5
Standard Poodle 8.8 6
Basset Hound 5.9 7
Dobermann Pinscher 5.5 8
Old English Sheepdog 4.8 9
German Shorthaired Pointer 4.6 10
Newfoundland 4.4 11
German Shepherd 4.2 12
Airedale Terrier 4.1 13
Alaskan Malamute 4.1 14
Chesapeake Bay Retriever 3.7 15
Boxer 3.7 16
Collie 2.8 17
Labrador Retriever 2.0 18
English Springer Spaniel 2.0 19
Samoyed 1.6 20
Dachshund 1.6 21
Golden Retriever 1.2 22
Rottweiler 1.1 23
MIxed 1.0 24
American Cocker Spaniel 0.6 25
Miniature Poodle 0.3 26

Module.05 24
The order confirms that body size is the most important determinant of GDV, but also indicates that among dogs of similar adult body size, great differences in risk may exist. For example, the Irish Setter and Gordon Setter are at a high risk similar to that of the giant breeds, whereas the Labrador Retriever and Golden Retriever are at much lower risk, similar to that of the much smaller breeds. This suggests that body conformation is also important.
Conformation
Anecdotal evidence indicates that a deep, narrow chest conformation can predispose dogs to GDV, possibly by making the normal movement of gases from the stomach more difficult. The subsequent accumulation of gas stretches the stomach wall, making the stomach round and unstable, so it is easy for the stomach to rotate along its axis, particularly in dogs with deep, narrow chests.
To test this hypothesis, chest conformation has been evaluated as a risk factor for GDV. Objective measurements of the average depth:width ratio of the chest for different breeds, were determined radiographically. The findings (Figure 2) indicate that 70% of the variability in breed risk of GDV can be explained by chest conformation plus large adult body size. Furthermore, in the Irish Setter breed, a greater chest depth: width ratio has been associated with a greater likelihood of GDV in individually measured dogs (Figure 2).
Figure 2 Predicted risk of GDV based on average chest depth:width ratio and adult body weight for individual dog breeds.
For example, when 155 Irish Setters were measured at the 1994 National Show, compared with dogs with chest depth:width ratios of 1.2-1.50, dogs with chest depth-width ratios of 1.51-1.60 and 1.61-1.85 had a 2.2 and 8.45-times greater likelihood, respectively, of having a history of GDV.
For other breeds such as the Great Dane however, it is an increased abdominal depth:width ratio that correlates best with the risk of GDV. The basis for these observations in high risk breeds might be that chest conformations which predispose to GDV are inherited through multiple genes. This is supported by the fact that analysis of five-generation pedigrees in Irish Setter dogs yield a higher average coefficient of relationship for dogs with a history of GDV compared with dogs without a history of GDV.
Other factors
An extensive epidemiological study of 101 pet dogs which had a first episode of GDV were compared with 101 dogs with medical conditions other than GDV (controls) that had been individually matched to the cases by age and breed if purebred, or size if of mixed breed. The results of this study indicate that other predisposing factors that significantly increased a dog's risk of GDV were male gender, being underweight, eating only one meal per day, a faster rate of eating, and a fearful or nervous temperament.
Weight: 10kg7
6
5
4
3
2
1
00.6 0.7
Average chest depth:width ratio
Pre
dic
ate
d r
isk
of G
DV
(kg
/od
ds)
0.8 0.9 1.0 1.1
Weight: 20kg
Weight: 30kg
Weight: 40kg

Module.05 25
The only factor that appeared to precipitate GDV, i.e. one which occurred more frequently in the eight hour period before the episode of GDV, was an event that the owner perceived as 'stressful' to their dog.
This epidemiologic study suggests that gastrointestinal function, especially in dogs of nervous or fearful temperament, is affected by stress, causing alterations in motility that may predispose to GDV. Faster eating may result in increased air intake during eating which causes the stomach to dilate. A deep and narrow chest or abdomen may provide a more conducive physical space in which a dilated stomach can rotate. Such events may be more likely to occur in dogs fed once daily, because this promotes maximum distention of the stomach on a regular basis. This suggested chain of events is not yet sufficient to explain all of the reported clinical and physiological findings in dogs with GDV. Some researchers have proposed that gastrin promotes GDV by causing delayed gastric emptying through its action on gastro-oesophageal sphincter pressure while others have suggested that GDV results from altered myoelectrical activity of the stomach.
PreventionOnly some of the known risk factors for GDV are amenable to manipulation (for example diet, stress, feeding patterns) while some are beyond our control (sex, age, breed, temperament). In the past, owners of dogs at risk of GDV have been advised to avoid exercising their dogs just before or after meals, to elevate feed bowls off the ground and feed frequent small meals, however none of these strategies have been proven to reduce the incidence of GDV. Population-based studies of pet dogs with GDV have now begun to explore other host and environmental factors that contribute to GDV risk. Once these factors are better understood we should be able to give accurate advice to dog owners about how to prevent this life-threatening condition
Key Points• GDV is a complex condition that involves physical and biochemical
injury to many organs
• Recurrence of volvulus is less likely if a gastric anchoring procedure is performed (N.B. this will stop volvulus but gastric anchoring will not affect bloat)
• The survival rate is related to the clinical condition of the dog at the time of surgery
• Breed, size and conformation are the major risk factors for GDV
• Temperament, feeding regimes and stress have also been implicated as risk factors

Module.05 26
In this module you will learn about dietary management of diseases which affect the digestive system of dogs and cats. The first topic we cover is the dietary management of chronic renal failure. Dogs and cats develop chronic renal failure due to a range of causes, but the dietary management of this condition has a common basis. The use of restricted protein, low phosphorus diets is examined in detail in this section.
The second area of interest is critical care nutrition in cats and dogs. Wide-ranging research into this topic has been conducted at the WALTHAM Centre for Pet Nutrition, and many of their findings are presented here.
The third topic is the dietary management of obesity in dogs and cats. This is the most common nutritional problem seen in small animal practice, but it can usually be managed by a combination of exercise, dietary calorie restriction and behaviour modification.
The final topic is dietary management of FLUTD. This group of diseases of cats often respond to appropriate dietary modifications.
At the end of this section there is another self test on clinical nutrition topics to test your understanding of topics in this module.
Other Clinical Nutrition Topics

Module.05 27
Chronic renal failure (CRF) is the most common renal condition in the dog and cat. It is mainly a disease of older animals and tends to be progressive in nature, leading to uraemia and other complications.
The kidney performs many vital functions, all of which are affected in CRF. Clinical and laboratory signs show a progressive decrease in these functions, but it is not until at least 65-75% of renal tissue is destroyed that clinical signs may become apparent. For this reason, early cases of CRF are likely to go undetected. Therefore, early diagnosis of CRF is desirable, via routine blood and urine analyses in the older animal.
Dietary Management of Chronic Renal Failure

Module.05 28
Dietary ManagementWhile there is no cure for CRF, appropriate medical management and diet can influence the progression and effects of CRF, resulting in good quality of life for the patient for months to years.
The goals of dietary management can be summarised as follows:
• to meet the animal’s nutrient and energy requirements
• to lessen clinical signs of uraemia by reducing protein breakdown
• to minimise electrolyte, vitamin and mineral disturbances
• to try to slow progression of renal failure
Since many of the clinical signs related to CRF are due to the accumulation of toxic protein breakdown products, and failure to excrete phosphorus, the emphasis in dietary therapy is on control of phosphorus and protein in the diet. However, other dietary components to be considered include calcium, sodium, potassium and water-soluble vitamins, together with the dietary energy content and fat.
Phosphorus
Dietary phosphorus restriction has been shown to slow the progression of renal failure in dogs. In cats with CRF, dietary phosphorus and protein restriction can increase survival time and slow progression of clinical disease.
High serum phosphorus concentrations are common in patients with CRF. When kidney function falls to approximately 20% of normal, excretion of phosphorus by the kidneys is impaired. Raised serum phosphorus can result in soft tissue mineralisation, increased parathyroid hormone (PTH) synthesis and release and potentially, to the progression of renal damage.
Dietary phosphorus restriction is an important part of management of CRF, which may slow the progression of the condition. Phosphorus restriction should, therefore, be initiated early in the course of CRF and should be considered for any dog or cat with impaired renal function resulting from primary renal failure.
Dietary therapy aims to normalise serum phosphorus concentration and control secondary hyperparathyroidism. The effect of phosphorus restriction should be monitored by measurement of serum phosphorus or PTH concentrations. If dietary phosphorus restriction does not correct hyperphosphataemia or hyperparathyroidism, further control of hyperphosphataemia may obtained with the use of oral medication to bind phosphorus.
Effect of Dietary Phosphorus (P)Restriction in Dogs with Renal Failure
Plasma Parathyroid HormoneConcentrations in Cats with CRF
Plasma Phosphate Concentrationsin Cats with CRF
Time (months)
From Brown et al. (1991)
0 4
0 28-48
p=0.083
p=0.040
p=0.009p=0.031
108-147
8 12 16 20 24
0.44% Phosphorus1.50% Phosphorus
Time (days)
Time (days)
Surv
ival
(%)
Plas
ma
para
thyr
oid
horm
one
conc
entra
tion
(pg/
ml)
Plas
ma
phos
phat
e co
ncen
tratio
n m
mol
/l)
Phosophate restricted groupNon-phosphate restricted group
Phosophate restricted groupNon-phosphate restricted group
0
20
40
60
80
100
120
0
50
100
150
200
250
300
350
0 28-48
p=0.087
p=0.206
p=0.007p=0.003
108-1470.50
1.00
1.50
2.00
2.50
3.00

Module.05 29
Protein
The reduced ability of the kidney to excrete protein breakdown products is one of the major causes of both uraemic signs and laboratory abnormalities in dogs and cats with renal failure. Several studies have shown that reducing dietary protein intake can reduce both urea and creatinine concentrations in blood. Dietary protein restriction may also help by (a) reducing the intake of dietary phosphorus, (b) decreasing the protein-related solute load, thereby lessening the severity of polydipsia and polyuria and (c) decreasing the acid load which may help to alleviate metabolic acidosis.
There are, however, potential problems with excessive protein restriction, which can result in protein malnutrition. The protein requirements of dogs and cats with CRF have not been established but it is likely that they may be quite similar or even higher than those of the healthy animal. In addition, renal failure may lead to increased urinary losses of protein or specific amino acids. It is important, therefore, that high quality protein sources are used in the formulation of restricted protein diets to minimise the risks of essential amino acid deficiency.
Because of their unique metabolism of protein, cats are at greater risk of protein malnutrition than dogs when protein intake is restricted. Also, low protein diets tend to be unpalatable to cats, which may reduce intake and further increase the risk of protein malnutrition. Diets for all cats with CRF should, therefore, be palatable and contain sufficient protein to meet the cat’s nutritional requirements.
Current recommendations are that all cats with azotaemia and moderate hyperphosphataemia (that persist following rehydration) should be fed diets which are restricted in phosphorus and moderately restricted in protein, even when they are not showing signs of uraemia. All cats receiving reduced protein diets should be carefully monitored for signs of protein malnutrition.
For dogs with CRF, a staged approach to management is recommended and early cases may benefit from phosphorus restriction whilst maintaining a protein intake that adequately meets adult maintenance requirements. More advanced cases which are showing clinical signs of uraemia should be fed diets which are restricted in both phosphorus and protein. Where possible, the degree of protein restriction should be adapted according to the dog’s clinical and biochemical state.
Potassium
Low potassium is the most common electrolyte abnormality in cats with CRF (30% of cases), which contributes significantly to muscle weakness and may further reduce renal function. and in these cats, supplementation is beneficial. However, for a small number of cases (13% in one study), high potassium levels may be a complication and may reflect the severity of renal failure.
This emphasises the need for regular monitoring of potassium status in cats with CRF, and the possible requirement for supplementation or adjustment of intake on an individual basis.
Calcium
Calcium concentrations in the blood of CRF patients may be low, normal or high. It has been recommended that calcium intake should be normal or supplemented in patients with CRF. Conversely, if the concentrations of calcium and phosphorus in blood is excessive, soft tissue calcification may occur leading to the progression of renal damage.

Module.05 30
Sodium
In the diseased kidney, surviving nephrons increase their excretion of sodium to cope with the increased load delivered to each one. In general, this response is adequate to maintain sodium balance until the condition is very advanced. However, the ability of the kidney to adapt to changes in sodium intake becomes progressively limited.
In dogs with chronic renal disease, some reports suggest that it is between 58 to 93% have hypertension (high blood pressure), whereas others suggest a much lower figure.
Hypertension may be important for two reasons:
• it can result in a variety of pathophysiological consequences, including heart failure, neurological abnormalities and ocular lesions.
• it may contribute to the progression of renal damage.
Reduction of blood pressure in dogs with proven hypertension is a desirable goal of therapy, so supplementation with sodium is not appropriate for most cases of CRF. Conversely, severe sodium restriction should probably also be avoided.
Hypertension has also been reported in cats in with CFR. In a recent study, systemic hypertension was present in 29% of cats with stable chronic renal failure, with a tendency to occur in older cats (>12 years).
Diets designed for the management of CRF are likely to be lower in sodium than in the normal foods that a patient may previously have been fed. This difference is one important reason for recommending a gradual introduction of dietary therapy (over one to two weeks), because the capacity to adjust sodium excretion is impaired in animals with CRF.
B-Complex Vitamins
Cats and dogs with CRF are at risk of water soluble vitamin deficiency because of
• reduced intake (inappetence)
• increased urinary losses in polyuric cases
• higher demands during the recovery processes
If present, water soluble vitamin deficiency may further contribute to anorexia. Supplementation with B-complex vitamins is, therefore, likely to be beneficial and at least twice the maintenance level is recommended.
Energy and Fat
The metabolism of protein (either from the diet or the body) to provide energy is undesirable in patients with CRF, since this increases the amount of nitrogenous waste products for excretion via the failing kidneys. An adequate energy supply in the diet is important, therefore, to prevent further tissue breakdown and this should be derived from non-protein sources.

Module.05 31
DOGS
Effects of low phosphorus, medium protein diets in dogs with chronic renal failure
From the results of a study conducted at the University of Veterinary Medicine, Vienna, of 60 dogs over a 28 week period with blood parameters suggestive of CRF, it can be concluded that many dogs with slight to moderate CRF can benefit from early diagnosis of the condition and dietary management using a medium protein diet with a low phosphorus content, such as Canine Early Renal Support. The reduction in serum creatinine levels that was observed suggested that renal function could be improved in dogs with early CRF whose kidneys were still capable of compensatory mechanisms. Many patients at this stage of the disease remain undiagnosed because of the absence or mildness of clinical signs, and it is recommended that elderly dogs should undergo routine blood and urine analyses to facilitate an early diagnosis.
CATS
Evaluation of a restricted phosphorus, restricted protein diet in the management of chronic renal failure in cats.
A clinical study using a restricted phosphorus, restricted protein diet (Feline Low Phosphorus, Low Protein Diet - equivalent to Feline Renal Support Diet) in the management of naturally occurring renal failure in cats.
Assessments of body weight, haematology, serum biochemistry and urinalysis were made weekly until the animal had completed four weeks of the trial. Further assessments were made at 8, 12 and 24 weeks.
The results demonstrated that the phosphorus and protein restricted diet was successful in reducing clinical and laboratory signs of uraemia, while maintaining adequate dietary protein intake to meet the special protein requirements of cats. This was evident in that both serum albumin and total protein levels remained normal in the test group. It also appeared that this diet was more effective than the control diet in slowing the rate of clinical deterioration of cats with renal failure, as perceived by both the clinician and the owner.
Clinical Studies
Effect of Dietary Phosphorus (P)Restriction in Dogs with Renal Failure
Plasma Parathyroid HormoneConcentrations in Cats with CRF
Plasma Phosphate Concentrationsin Cats with CRF
Time (months)
From Brown et al. (1991)
0 4
0 28-48
p=0.083
p=0.040
p=0.009p=0.031
108-147
8 12 16 20 24
0.44% Phosphorus1.50% Phosphorus
Time (days)
Time (days)
Surv
ival
(%)
Plas
ma
para
thyr
oid
horm
one
conc
entra
tion
(pg/
ml)
Plas
ma
phos
phat
e co
ncen
tratio
n m
mol
/l)
Phosophate restricted groupNon-phosphate restricted group
Phosophate restricted groupNon-phosphate restricted group
0
20
40
60
80
100
120
0
50
100
150
200
250
300
350
0 28-48
p=0.087
p=0.206
p=0.007p=0.003
108-1470.50
1.00
1.50
2.00
2.50
3.00
Appetite is often poor in affected animals, so the energy density of the diet should be high to enable the animal to obtain its nutritional requirements from a relatively small volume of food. In this respect, fat offers advantages over carbohydrate as a non-protein source of energy: it provides approximately twice the energy per gram and improves palatability. For this reason, canned diets designed for dogs and cats with CRF tend to be high in fat.

Module.05 32
Key PointsDiet is one of the key elements in the management of dogs and cats with chronic renal failure
Dietary phosphorus restriction has been shown to reduce high serum phosphate levels and slow the progression of renal failure
Protein restriction can lessen clinical signs of uraemia by reducing protein breakdown
Due to the high incidence of hypertension in dogs with CRF, supplementation with sodium is not appropriate for most cases
Cats and dogs with CRF are at risk of water soluble vitamin deficiency
An increased fat content in the diet is recommended to increase the energy density and improve palatability

Module.05 33
The value of nutritional support has been widely recognised in human medicine for many years, but until relatively recently, its importance in the veterinary field has been largely overlooked. However, failure to understand the altered nutritional needs of the critical care patient and how this may impact on the healing process can result in malnutrition and will deprive the animal of important supportive care.
Critical Care Nutrition

Module.05 34
Therapeutic benefits of nutritional support for the stressed or traumatised patient are well established and include:
• increased survival rate
• improved tolerance to invasive procedures
• shorter hospitalisation
• decreased incidence of complications
• earlier ambulation
• more rapid wound healing
The Healthy, Starved StateIn the healthy animal, food deprivation results in a series of metabolic adaptations which are designed to maintain blood glucose concentrations, preserve lean body tissue and promote survival. Metabolic rate, and hence energy expenditure, is decreased, glucose utilisation decreases and ketone body production rises. Tissue reserves of glycogen and fatty acids are mobilised to provide energy and amino acids are mobilised, initially from metabolically labile proteins in the liver, kidneys and gastrointestinal tract, to replace losses due to the normal daily turnover of protein.
Within a few days of initiating a fast, glycogen stores are depleted and fat becomes the primary fuel source. Protein utilisation increases as amino acids are used preferentially for gluconeogenesis to maintain circulating levels of glucose for cells (such as those of the nervous system, renal medulla, bone marrow and circulating blood) which are obligate users of glucose as an energy source. Fasting in the healthy animal will, therefore, result in a loss of some lean body tissue as well as fat. During starvation in the healthy dog or cat, fatty acid utilisation accounts for 70-85% of energy expenditure (including ketones up to 15%), proteins up to 25% and carbohydrates less than 10%. When feeding starts, amino acid mobilisation decreases and metabolism returns to normal within 24 hours.
Metabolic Response to Stress and TraumaMetabolic stress is characterised by an initial hypometabolic phase which lasts for 24-48 hours. During this 'ebb' or shock phase, metabolic rate is decreased as the body attempts to prevent further damage and maintain body fluids and tissue perfusion. Treatment during this phase is primarily aimed at life-saving procedures.
Subsequently, this nutrient-sparing phase is followed by the 'flow' phase of hypermetabolism which can last from days to several weeks, depending on the severity of the injury. Hypermetabolism in the short term, is intended to support the healing of wounds and resistance to infection. Energy requirements increase in accordance with the severity of the injury and can be particularly high in cases of head trauma (because the brain has a particularly high energy requirement), septicaemia, extensive burns, massive trauma or following radical surgery. Even healthy animals

Module.05 35
undergoing minor elective surgical procedures may experience a transient increase in energy requirements of up to 10% above normal. Some therapeutic agents, such as high doses of steroids, can also exacerbate the patient's energy needs.
In stressed animals, glycogen reserves are rapidly depleted and fat becomes the major and preferred energy source. There is a marked increase in gluconeogenesis from amino acids to maintain blood glucose levels for cells that are obligate glucose users, including repairing tissues and some neoplasms. Protein catabolism is increased to meet this demand, resulting in a depletion of tissue protein and negative nitrogen balance. Hypermetabolic patients also exhibit a peripheral insulin resistance and, consequently, hyperglycaemia. Stressed and traumatised patients are unable to utilise glucose efficiently. High levels of dietary carbohydrate are, therefore, contraindicated during this period, and can result in respiratory acidosis and other complications.
Following stress or injury, the protein-sparing adaptations to food deprivation that occur in the healthy individual appear to be overridden, with the net loss of marked amounts of protein. The drain on tissues may continue for weeks and during this time, nutritional support becomes a crucial part of the treatment. Failure to address the nutritional needs of the patient most commonly results in protein-energy malnutrition. Unlike the fasting healthy animal, the metabolically stressed cat or dog can continue to exhibit negative nitrogen balance, accelerated gluconeogenesis and insulin resistance even when feeding is resumed.
Protein-Energy MalnutritionProtein-energy malnutrition can have a number of adverse effects which, in combination, can delay recovery and increase the patient's susceptibility to infection and shock. These include:
• Atrophy of skeletal and smooth muscle tissues,
• Reduced digestive and absorptive capacity due to atrophy of the gastrointestinal mucosa and decreased production of digestive enzymes.
• Increased gut permeability and an associated risk of bacterial translocation, resulting in systemic infections.
• Impaired cellular and humoral immune function.
• Delayed wound healing.
• Hypoalbuminaemia, which can lead to decreased plasma volume, a lowered resistance to fluid losses and an increased risk of wound dehiscence and local infection
• Ultimately, atrophy and reduced functional capacity of respiratory and cardiac muscles.
• In extreme cases, death can occur as a result of multiple organ failure which is often associated with sepsis.
Patient assessmentIdentification of patients in need of nutritional support, is somewhat subjective but consideration should be given to the animal's medical and dietary history, its current eating behaviour, physical examination and laboratory tests.

Module.05 36
Specific nutritional support is indicated if:
• oral intake is reduced for 3-5 days
• there is an acute weight loss of 5-10% of body weight (excluding fluid losses) •actual weight is 15% or more below ideal body weight
• body condition, on a scale of 1 (cachectic) to 5 (obese), is below the optimal score of 3
• physical changes are accompanied by hypoalbuminaemia
• recent trauma, surgery or sepsis is accompanied by anorexia
Once an initial assessment has been made, the degree and duration of nutritional support can be estimated and a nutritional plan formulated on an individual basis. For surgical patients, pre-operative assessment is particularly important so that any feeding tube placement can be performed at the time of surgery.
Techniques for Nutritional SupportNutritional support may be provided by either the enteral or the parenteral (intravenous) route. Total parenteral nutrition is expensive, and has inherent technical problems, and so is usually reserved for a small number of patients with gastrointestinal failure.
Where the gastrointestinal tract is functional, enteral nutrition is a more economical and physiologically sound option. Prolonged lack of enteral nutrition can result in intestinal mucosal atrophy, with an associated reduction in functional capacity and risk of intestinal bacterial translocation into the portal blood. A number of techniques are available for enteral feeding, the choice of which depends on various factors including type of injury, medical condition or surgical procedure and should be based on individual patient assessment.
If voluntary intake is still occurring, nutritional support may simply take the form of providing a more concentrated source of energy and nutrients. Other patients may be encouraged to eat by hand feeding, providing highly aromatic foods and heating the food offered to stimulate the appetite. Inappetent cats may respond to the administration of diazepam (0.1 mg/kg I/V) but this method of appetite stimulation should not be continued for longer than 3 days.
Where the patient's needs cannot be met through voluntary intake, some form of involuntary tube feeding must be considered. Force feeding by syringe, by daily oro-gastric intubation or by rolling the food into small balls and 'pilling' the animal are short-term options, but these methods can be stressful for the patient and may not satisfy the animal's nutritional needs.
Feeding tubes
1. Naso-oesophageal
Naso-oesophageal intubation requires no sedation and is well tolerated by most patients. The tube may be left in place for several weeks, but since the tube size is limited, this method is only suitable for a specially formulated concentrated diet. It can also be used for long term administration of fluids. Naso-oesophageal
Module.05 37
feeding is recommended as an adjunct to voluntary feeding or where sedation or anaesthesia of the patient poses too great a risk for surgical placement of a feeding tube.
2. Pharyngostomy
Surgical placement of a pharyngostomy tube has been used successfully for feeding patients with prolonged anorexia and an inability to prehend or masticate food. The popularity of this method of tube feeding has recently declined in favour of nasal feeding or gastrostomy tubes. If placed correctly however, this method of feeding can be very useful for medium term enteral support.
3. Oesophagostomy
In recent years, the technique of placing a feeding tube percutaneously into the oesophagus has become more popular. This technique, which is facilitated by using a purpose-designed applicator, maintains a feeding tube that is well tolerated and can be maintained for long-term feeding.
4. Gastrostomy
Gastrostomy tube feeding is indicated where long term involuntary nutritional support is anticipated and/or the presence of pharyngeal or oesophageal lesions precludes the use of pharyngostomy tubes. The use of gastrostomy tubes is increasing thanks to the development of a technique for percutaneous tube placement without the need for laparotomy. Percutaneous endoscopic gastrostomy (PEG) is a simple and well tolerated procedure, but requires the use of a flexible endoscope. Alternatively, a large bore Foley catheter can be placed into the stomach at laparotomy and secured to the abdominal musculature. Gastrostomy tubes are wide bore and so will accommodate most types of diet. The tube may be left in place for weeks to months and tube feeding by this method can be continued by most owners at home.
5. Enterotomy catheters
Feeding by enterotomy catheter may be required when serious conditions of the upper gastrointestinal tract, such as pancreatitis or major gastric or small bowel surgery, are present. Animals fed in this way should receive liquid elemental diets that require little digestion and are readily absorbed from the jejunum and ileum. Parenteral nutrition is an alternative if small bowel function is severely compromised.
Energy and Nutrient RequirementsDaily energy requirements of the hospitalised patient are based on cage-rest maintenance energy requirements (MER) multiplied by an arbitrary factor, the size of which varies according to the severity and nature of the illness. In some cases, energy requirements may be below normal

Module.05 38
because the animal is hypometabolic or because it is physically inactive as a result of the injury.
The volume of food required is calculated by dividing the total daily energy requirement (kcal) by the energy density of the diet (kcal/ml or kcal/100g) as recorded on the product label. The total volume required is divided into 4-6 feeds per day, depending on previous oral intake and individual animal tolerance. The calculated volume should be approached over a period of 48-72 hours to avoid vomiting, abdominal discomfort and diarrhoea (eg, 50% on the first day, 75% on the second day, 100% on the third day). For animals that have been inappetent for prolonged periods, slow rates of administration (>10 minutes) are recommended.
Weight and body condition score should be recorded on a daily basis to enable accurate calculation of the patient's energy requirements and to monitor its progress. Adjustments in food allowance can then be made according to changes in the animal's body weight and body condition. Frequent monitoring of haematological and biochemical profiles is recommended.
The increase in protein catabolism in response to stress and trauma indicates an increased need for dietary protein. Protein levels ranging from 25-48% of metabolisable energy requirements may be needed to maintain wound healing and immune function in some disease conditions. However, restriction of dietary protein may be indicated in specific conditions, such as portosystemic shunts, and chronic kidney or liver disease.
High fat diets are also recommended because triglycerides rather than glucose provide the principal fuel for the hypermetabolic, catabolic patient. In addition, high fat diets tend to be more palatable, digestible and calorie-dense, which are advantages for feeding potentially anorexic patients.
A number of specific nutrients may have properties which are beneficial in the nutritional management of critical care patients. In particular, the amino acid glutamine is important for maintaining the IgA-secreting cells of the gut mucosa and an adequate supply is required to ensure the integrity of the intestinal mucosal barrier. Supplementation with arginine has been shown to enhance cellular immunity and branched chain amino acids are thought to have a beneficial effect on nitrogen balance. The requirement for water-soluble B-complex vitamins may increase in the hypermetabolic patient due to fluid losses and increased energy expenditure. Zinc may be important by virtue of its role in wound healing and immune function and supplementation should be considered in anorexic patients with gastrointestinal disease.
Calculating Energy Requirements of PatientsMaintenance energy requirements (MER) (kcal/day)
= 95 BWT0.75 (dog)= 77.6 BWT0.711 (cat)
where BWT is the animal's body weight (kg) and 1 kcal = 4.184 kJAdjustments are made to give the illness energy requirement (IER) as follows:
Condition Factor X MER ExamplesHypometabolismPhysical inactivity, starvation 0.5 - 0.9 Hypermetabolism
Mild stress 1.0 - 1.2 SurgeryModerate stress 1.2 - 1.5 Sepsis, cancer, polytraumaSevere stress 1.5 - 2.0 Extensive burns, head injuries
Module.05 39
Diet SelectionIn selecting a diet for enteral administration, it is important to consider the dietary formulation, the caloric density of the diet and, where appropriate, the diameter of the feeding tube. Elemental diets containing amino acids or glucose may be useful if gastrointestinal function is compromised or to supplement other diets, however polymeric diets or blenderised canned diets may be used for most purposes. Ideally, diets for the critical patient should be highly palatable, highly digestible and nutrient dense to ensure an adequate intake of nutrients in a reduced volume of food. Commercial diets which are formulated to meet the specific needs of the stressed animal are particularly suitable.
Complications of Nutritional SupportFollowing a period of food deprivation, all dietary transitions should be made slowly to avoid complications. In the initial stages of feeding, vomiting may occur due to gastrointestinal hypomotility and diarrhoea may result from reduced intestinal surface area, decreased enzyme activity and hypoalbuminaemia. Normal digestive function is usually restored within a few days of gentle transition to an appropriate enteral feeding method.
Calorie intake has an important effect on convalescence. An insufficient intake can result in protein-energy malnutrition, but overfeeding can be equally detrimental, particularly when the carbohydrate intake is excessive. In starved, hypometabolic patients, excessive carbohydrate can lead to insulin-induced transport of phosphorus and potassium into cells and subsequently, hypophosphataemia and hypokalaemia. The resultant respiratory and cardiovascular failure could prove fatal in some cases.
Other complications of nutritional support include mechanical problems or infections related to the feeding tube. Tube obstructions can be minimised by using liquid diets, by sieving liquidised canned diets, and by flushing with water after each feed. Occasionally, naso-oesphageal tubes may be regurgitated and pharyngostomy tubes can cause gagging, airway obstruction and related problems. Endoscopically placed gastrostomy tubes should be left in situ for at least seven days (even if oral intake is resumed) to allow for adequate seal of stomach to body wall.
Key Points• Enteral nutritional support can significantly reduce morbidity and mortality in the critical care
patient
• Patient assessment and implementation of a nutritional plan at an early stage will contribute to a successful outcome
• Particular attention should be paid to the individual animal's energy requirements
• Diet formulation, route of administration and frequency of feeding should be carefully chosen for each patient

Module.05 40
Obesity is considered to be the most common form of malnutrition encountered in small animal practice. Studies in Europe have indicated that between 9 and 44% of dogs and between 6 and 40% of cats attending veterinary practices are overweight or obese.
Obesity is a consequence of energy intake exceeding requirement at some stage in the animal’s life. In a few cases obesity may be secondary to a number of other conditions, such as endocrine disorders and drug-induced polyphagia.
Current therapies available for the treatment of obesity include dietary management, exercise, psychological and behaviour modification, drug therapy and surgery. However, the cost and
Dietary Management of Obesity

Module.05 41
ethical issues surrounding pharmaceutical and surgical treatment of obesity render these approaches unacceptable for most patients. The success of exercise or behavioural modification is poor when these procedures are used in isolation, but when combined with dietary therapy, they have a synergistic effect. Current recommendations in man suggest that a combination of these procedures is the best approach for effective and sustained weight loss.
Similarly, a weight reduction programme based on a combination of decreased energy intake, increased physical exercise (where possible) and behavioural management is considered the most effective approach to reducing body weight in the companion animal.
Dietary TherapyDietary therapy focuses on restricting energy consumption. Dietary management options include starvation (total energy restriction) or controlled energy restriction.
Starvation to reduce weight has been shown to be safe in the dog, but has several disadvantages. Unlike moderate calorie restriction, it is associated with unacceptable losses in lean body tissue. Furthermore, starvation is normally expensive (because hospitalisation of subjects is required) and likely to be less effective in the long-term, since pet owners are not directly involved with the process. Starvation should not be considered an option in the cat because of the link between anorexia and the development of idiopathic hepatic lipidosis (IHL). For this and other reasons, the recommended dietary approach is one of controlled moderate energy restriction.
EnergyIn practice, it has been found that a maximum of 15% decrease in body weight is initially a reasonable goal. Once this 15% weight loss has been achieved, further reductions can then be planned.
Clinical studies have shown that in dogs, a weight loss of 12-14% over twelve weeks can be achieved by feeding 40-50% of the animal’s energy requirement for maintenance at its target weight. In cats, a weight loss of 14-18% over eighteen weeks can be achieved by feeding 60% of the animal’s energy requirement for maintenance at its target body weight. The rates of weight loss in these studies are comparable to current recommendations in man.
Although this is a guide to the approximate weight loss that can be expected, a certain amount of individual variation will occur. Feeding should be individualised to accommodate such differences in rate of weight loss.
There are two methods for reducing energy intake in the companion animal. One approach is to feed the normal diet, but in reduced quantities. When this technique is used, it rarely forms part of
Weight Reduction in Dogs
Canine Calorie Control Diet
080
85
90
95
100
105
2 4 6 8 10 12
Canine Low Calorie Diet

Module.05 42
a structured weight reduction programme and consequently, attrition rates tend to be high and success rates low. More importantly, most prepared pet foods are balanced to a normal energy intake and by restricting energy intake, essential nutrients are also restricted. This can produce deficiency states that may be dangerous.
The alternative is to feed a prepared, low calorie diet that has been specifically formulated to achieve weight loss, and ensures adequate intake of essential nutrients despite the restricted energy intake. This is particularly important where the diet is to be fed long term.
ProteinSome lean body mass in obese individuals is lost with effective dieting. However, excessive protein loss during weight reduction is not desirable, because functional tissue losses will need replacing. Some of the adverse effects of very low calorie diets in man may be related to inadequate protein intake and the subsequent loss of lean body mass.
A dose response curve between preservation of lean tissue mass and increasing protein content of very low calorie diet formulations has been demonstrated in man during weight loss. However, the protein requirement to maintain optimum well being and minimise tissue protein loss during weight reduction has not been determined.
It would appear prudent, therefore, to provide at least as much protein to the individual on a weight reduction programme as would normally be expected to maintain a non-dieting individual of comparable weight. For cats, in particular, excessive tissue protein loss should be avoided since protein or specific amino acid deficiencies may be causative factors for idiopathic hepatic lipidosis.
Vitamins, Minerals and Essential Fatty AcidsA number of adverse health problems during weight loss in man have been attributed to possible deficiencies in minerals and/or vitamins. There is no evidence to suggest that the mineral, vitamin or essential fatty acid (EFA) requirement of the dieting individual is reduced thus normal intake should be ensured.
FibreIn human and small animal medicine, dietary fibre has been included in foods as a bulking agent in an attempt to overcome hunger and increase compliance during weight reduction programmes. In man, some support for this view has been provided by a number of short term studies, which have demonstrated that dietary fibre reduces food intake and/or the perception of hunger. Other studies, however, have provided conflicting results.
In the past, few studies have been carried out to evaluate the satiating properties of dietary fibre during energy restriction but, despite the lack of evidence, there is a popular assumption that

Module.05 43
the addition of dietary fibre (particularly insoluble fibre), is a beneficial component of weight reduction programmes in small animals. In fact, one recent study found that the addition of moderate levels of insoluble fibre to a commercial low calorie diet had no apparent beneficial effects on satiety when fed to dogs on an energy intake compatible with weight reduction.
These studies have shown that increasing the soluble or insoluble fibre content to high levels had no beneficial effects on satiety in the dog.
Step by Step ApproachThe following procedure is recommended as a guide for managing obesity in dogs and cats, and can be used in combination with appropriate exercise and behavioural programmes.
1. Counsel the owner on the need to reduce the animal’s body weight, stressing the medical implications of obesity.
2. Weigh the animal and set a target weight. The planned reduction should represent no more than 15% of the animal’s current weight.
3. Indicate to the owner how long it is likely to take to reach the target weight safely. In dogs, the weight loss can usually be achieved in 10-15 weeks by feeding 40-50% of the maintenance energy requirements at target body weight. In cats, the weight loss can usually be achieved in 16-20 weeks by feeding 60% of the maintenance energy requirements at target body weight. Food intake should be monitored and extra treats or scraps should not be fed.
4. Cats should ideally be confined to the home for the period of weight reduction to prevent supplementation of its diet from other sources.
5. Advise weighing the animal carefully on the same scales at the same time every week or fortnight, and encourage the owner to record the weight on a chart. Small and steady weight losses are more evident from the weight chart than from simple observation of the animal.
6. If satisfactory weight loss is not occurring, then the daily food allowance may be reduced by 10%, whilst keeping a careful watch on the general health of the animal. If such a reduction is necessary, it should be maintained for the rest of the dieting period.
7. When a satisfactory weight loss has been achieved, the dog or cat should be changed to a normal high quality diet. It is important to calculate and regularly reassess the daily amount of food required to maintain the target weight.
8. Follow up after one month, three months and then at six monthly intervals. At all times, give the owner adequate encouragement.
Example of Step-by-Step Weight LossProgramme for a Labrador Retriever
Target weight: 43.8 kg-15% b.w.
Target weight: 37.2 kg-15% b.w.
Final weight: 36.2 kg-3% b.w.
Initial weight: 51.5 kg
3 weeks
14 weeks
10 weeks

Module.05 44
Physical ExerciseWhen used in combination with dietary therapy, exercise promotes fat loss and may assist in lean tissue preservation during weight loss. There is also some evidence that exercise may help to prevent the rapid weight regain that can occur following weight loss.
In formulating an exercise programme for dogs, co-existent health problems must be considered and it is important that grossly obese animals are not subjected to an immediate increase in activity levels. In general, an exercise programme for dogs can be relatively easily applied in the form of walking, but other types of exercise may be chosen to accommodate concurrent health problems. For example, swimming is a valuable option for dogs with arthritic or other locomotor complaints, and provides a range of muscular activity while avoiding the stress of weight bearing.
It is clearly difficult to apply a structured exercise programme to cats. However, physical activity may be encouraged by increasing outside access to those cats that are ‘house bound’ (as long as this does not allow access to additional food), or by initiating periods of play with interactive toys.
Behavioural ModificationIn man, behavioural modification and dietary therapy are used in combination to improve the outcome of weight reduction programmes and prevent rapid weight regain. Behavioural programmes focus on changing environmental factors that control behaviour, using a variety of techniques. The goal of such a programme is to produce lifelong habit changes and hence permanent weight loss.
Although many of the techniques employed in man are clearly impractical and inappropriate for the companion animal, some of them can be relatively easily applied and may improve the outcome and maintenance of weight loss. It is of fundamental importance that behavioural therapy in the companion animal should include the owner as well as the pet.
The OwnerThe most important factor in the treatment of companion animal obesity is good owner compliance in implementing and following a therapeutic plan. Owner recognition of obesity in their pet must be the first step in a weight reduction programme and their continued motivation and compliance is essential, since they control the food bowl. Regular counselling and support will help to instil these attributes.
An important lifestyle change to impress on clients is the abolition of edible ‘treats’. Many owners perceive the reward of ‘treats’ as a valuable component of the companion animal bond, and may be reluctant to heed this advice. However, by putting aside a portion of the normal daily ration, treats can be

Module.05 45
provided without increasing the daily energy intake. Negative behavioural traits such as begging should not be indulged or reinforced with treats, although persistent begging can be modified by implementing a reward system. In this, the pet receives a treat only after performing some positive task, such as sitting, lying, or fetching an object, rather than simply begging for food.
The Dog or CatIn the obese individual, there is a breakdown in the mechanisms which control food intake, leading to excess energy intake and subsequent obesity. Appetite in the dog may manifest in the form of begging, and this type of behaviour is well established in many obese dogs. Begging is a learned trait and may operate independently of the animal’s apparent hunger. Presumably in these animals, social or other factors have overcome normal satiety mechanisms, contributing to the development of begging behaviour and subsequently to obesity. It is unlikely that any diet would be satiating from the point of view of controlling this behavioural trait in these individuals. Behavioural modification of the dog and a change in habits of the owner are, therefore, essential to the success and long-term maintenance of weight loss.
Any diet that is used as part of a weight reduction programme must be palatable, since long-term acceptance will influence compliance and ultimately the success of the programme. This is particularly important in cats which are recognised as ‘finicky eaters’; poor acceptance of an unpalatable diet can lead to withdrawal from the weight reduction programme, or worse still, prolonged anorexia and the risk of idiopathic hepatic lipidosis.
Clinical StudiesWeight reduction using Canine Low Calorie Diet
In one study, 34 obese dogs were recruited from three private practices (UK, Netherlands and Denmark). The dogs were fed a commercial low calorie canned diet (Canine Low Calorie Diet - equivalent to Canine Calorie Control Diet) as the sole source of food for up to 12 weeks. The amount of food allocated was based on providing approximately 45% of the calculated maintenance energy requirement of the dog at its target weight. Where possible, the dogs were re-weighed at two-week intervals.
The results showed that substantial weight loss could be achieved using the low calorie diet as part of a programme of controlled calorie reduction. In the dogs that completed the trial, an average weight loss of 14% of the initial body weight was achieved after 12 weeks.
In a more recent study in Finland, 20 overweight or obese dogs were fed the same diet over a period of 12 weeks. Prior to inclusion in the trial, each dog was thoroughly evaluated clinically and blood and urine analyses were performed to exclude cases associated with hypothyroidism or diabetes mellitus. The dogs were weighed initially and checked regularly throughout the study period. A target weight was assigned and food was allocated to provide approximately 45% of the maintenance energy requirement at the target weight.
The diet was found to be very palatable and resulted in a significant (p<0.01) average weight loss (11.7 + 5.1%) over the 12 week study period, giving an average rate of weight loss of approximately 1% per week.

Module.05 46
The effects of feeding Canine Calorie Control Diet on weight loss and behaviour in obese dogs
In a study conducted at two clinical centres (UK and Switzerland), the effects of feeding a commercial low calorie dry diet (Canine Calorie Control Diet) on weight loss and behaviour were investigated in obese dogs. Sixteen dogs, identified as obese, were recruited as part of a 12-week weight reduction programme.
Initially, the dogs were weighed and a target weight was calculated for each. Food was allocated to provide approximately 55% of maintenance energy requirements at target body weight, and was divided into two separate meals. Throughout the 12-week period (or until target weight was reached, if shorter), the dogs were weighed at two-week intervals.
There was a significant (p<0.001) absolute (3.6 kg) and percentage (11.9%) weight loss of the dogs during the weight reduction programme, resulting in an average weekly weight loss of approximately 1%.
Owners assessed the palatability of the diet as very good and there were no problems in changing from a canned to dry diet. Approximately 69% of owners reported an increase in activity of their dog during the weight reduction programme.
Effect of level and source of dietary fibre on food intake in the dog
Studies have been carried out using a commercial low calorie canned diet (Canine Low Calorie Diet) to evaluate the effects of different levels and sources of dietary fibre on satiety and the perception of hunger in the dog.
These studies showed that the addition of moderate levels of various fibre sources to the commercial low calorie canned diet had no beneficial effect on satiety when fed to dogs on an energy intake compatible with weight reduction. Furthermore, there was no indication of residual long term or carry over effect of fibre intake on satiety, as no effect of diet on intake of the standard product was seen during the washout periods.
In a subsequent study, the effect of diets formulated with moderate and very high levels of either insoluble or soluble dietary fibre were evaluated in a similar protocol. Results of this study indicated that even high levels of insoluble or soluble fibre have no effect on satiety in dogs receiving an energy intake appropriate to weight reduction.
Clinical application of Feline Low Calorie Diet for weight reduction in obese cats
A study to evaluate the safety and efficacy of a weight reduction programme using a commercial low calorie diet (Feline Low Calorie Diet - equivalent to Feline Calorie Control Diet) for the management of obesity in cats was carried out at a small-animal clinic in Denmark. Twenty two obese, client-owned cats successfully completed the trial.
Challenge Meal Intakes FollowingTest Meals
Test meal (given 3 hours before challenge meal)
Chal
leng
e M
eal I
ntak
e(g)
Soluble �bre, high levelsSoluble �bre, intermediate levels
Insoluble �bre, high levelsInsoluble �bre, intermediate levels
Canine Low Calorie Diet
1000
800
600
400
200
0
1200

Module.05 47
This study demonstrated that obesity in the cat can be safely and successfully managed in a practical situation using Feline Low Calorie Diet as part of a programme of controlled calorie reduction.
In a study aimed at achieving more rapid rates of weight reduction in cats, target weights were individualised according to the degree of obesity and ranged from 60-80% of the starting body weight. By feeding of Feline Low Calorie Diet at 60% of maintenance energy requirements at these target weights, weight losses of 16-39% (average 20%) over 18 weeks could be attained. Furthermore, a 25% reduction in weight of obese cats was safely achieved by restricting energy intake to 45% of maintenance energy requirements at the target weight (85% of initial weight).
This trial used a degree of energy restriction that was more severe than is usually recommended for the management of obesity in cats, but no adverse health effects of this programme were noted. The palatability of the diet was seen as an important factor in determining that energy intake was not further compromised and the maintenance of serum albumin concentrations over the 18 week period suggested that protein intake was adequate. WALTHAM Veterinary Diet Feline Calorie Control is thus considered a safe product for rapid weight reduction in markedly obese cats under veterinary supervision.
Key Points• Weight reduction programmes for dogs and cats should be based on a combination of
decreased energy intake, increased physical exercise (where possible) and behavioural management
• Using controlled moderate energy restriction, a maximum of 15% decrease in body weight should be the initial goal
• In dogs, a weight loss of 12-14% over twelve weeks can be achieved by feeding 40-50% of the animal’s energy requirement for maintenance at its target weight
• In cats, a weight loss of 14-18% over eighteen weeks can be achieved by feeding 60% of the animal’s energy requirement for maintenance at its target body weight
• Feeding a prepared, low calorie diet that has been specifically formulated to achieve weight loss ensures adequate intake of essential nutrients
• For cats, in particular, excessive tissue protein loss should be avoided since protein or specific amino acid deficiencies may be causative factors for idiopathic hepatic lipidosis
• Increasing the soluble or insoluble fibre content to high levels had no beneficial effects on satiety in the dog
• The most important factor in the treatment of companion animal obesity is good owner compliance in implementing and following a therapeutic plan

Module.05
The term feline lower urinary tract diseases (FLUTD) covers a spectrum of clinical conditions in cats that give rise to a similar set of clinical signs. The clinical signs associated with FLUTD include:
• haematuria (blood in urine)
• pain on urinating
• frequent urination
• urination in inappropriate places
• urinary obstruction.
Where urinary obstruction occurs, potentially fatal, acute post-renal renal failure can follow within a relatively short period of time.
A number of causes of FLUTD (acting either singly or in combination) have been proposed or identified, including viruses,
Dietary Management of FLUTD
48

Module.05 49
bacteria, urethral plugs and urolithiasis, although in a substantial proportion of cases no cause can be identified, and these are classified as ‘idiopathic’. Both urolithiasis (urinary stones) and urethral plugs are considered to be of particular importance; in one clinical study, over 20% of cases had these symptoms.
Uroliths of a variety of mineral compositions have been found in cats, including struvite, calcium oxalate, calcium phosphate, uric acid and urates, cystine and silica. The most common mineral found in feline uroliths has been struvite, although there is evidence that calcium oxalate is now of at least equal importance in North America. Struvite remains by far the most common crystalline component of urethral plugs.
Struvite UrolithiasisThe formation, growth and dissolution of struvite crystals in urine depend on the concentration of solutes that are free to react with other solutes. Struvite crystallisation in urine may be considered as follows:
Oversaturation (concentration is above the formation product of struvite). Crystals form spontaneously and pre-formed crystals grow rapidly.
Supersaturation. In this zone crystals do not form spontaneously but pre-formed crystals do not dissolve and may grow.
Undersaturation (concentration is below the solubility product). Crystals do not form and pre-formed crystals dissolve.
The principle of management of struvite associated FLUTD is to create and maintain urinary undersaturation with struvite. Under these circumstances uroliths would be expected to dissolve and further struvite formation would be prevented. In addition to preventing the recurrence of uroliths, prevention of reformation of the mineral component of urethral plugs may reduce the risk of recurrence of obstruction.
Based on experimental and theoretical data the following factors are important in achieving urinary undersaturation with struvite:
• acidification of the urine
• enhancement of urine volume and reduction of specific gravity
• restriction of crystalloid intake
Oversaturation
IncreasingActivityProduct
Undersaturation
Metastable Supersaturation
> Spontaneous crystallisation> Rapid crystal growth
Formation Product
Soluble Product (saturation)
> No crystallisation> Dissolution of preformed crystals
> No dissolution> Possible growth of preformed crystals

Module.05 50
Urine pHUrinary pH is a key factor in controlling struvite formation. Changing urinary pH has a more important effect rather than other factors, such as reducing urinary magnesium concentration. The ideal urine pH for the dissolution of struvite has not been established in experimental studies. However, struvite crystals are rarely found at pH values of less than 6.5.
Urine pH values below 6.5 are, therefore, likely to be associated with undersaturation with struvite and in time, should bring about the dissolution of pre-formed crystalline material. Nevertheless, if a cat is maintained on a diet that consistently produces a urine pH below 6.0, the risk of it developing metabolic acidosis is increased. Urine pH should, therefore, be maintained between 6.0 and 6.5, on average.
Dietary acidification may affect potassium balance in cats, and low blood potassium has been reported in cats fed acidified diets marginal in potassium. Furthermore, WALTHAM studies have shown that increased levels of taurine may be required in acidified diets to maintain normal plasma taurine status in cats. Levels of potassium and taurine should, therefore, be enhanced in diets designed to promote the production of acidic urine.
Urine VolumeIncreasing the urine volume and decreasing the specific gravity are also desirable goals of therapy because of the diluting effects on the concentration of all crystalloids. In addition, it may help to increase the frequency of urination, allowing less opportunity for urine to ‘pool’ within the bladder and less time for crystals to form.
Mineral IntakeAlteration of urinary crystalloid levels is relatively less important than controlling urinary pH and volume. Nevertheless, studies have shown that increasing dietary mineral levels can bring about the formation of crystalline material and/or obstruction of the lower urinary tract in cats.
Phosphorus restriction is of theoretical value in diets for the management of struvite-associated FLUTD, as reduction of urinary phosphate will reduce the struvite activity product. However, acidified diets have been shown to decrease phosphorus balance in adult cats. For these reasons excessive phosphorus restriction should be avoided.
Despite these concerns, urinary magnesium and phosphorus concentrations can influence the struvite activity product, thus, dietary restriction of these minerals to try to reduce urinary excretion is reasonable for cats which are known to be susceptible to struvite formation.
Excessive restriction of dietary magnesium may, however, not be appropriate. In other species, magnesium has been reported to act as an inhibitor of calcium oxalate crystallisation.

Module.05 51
Calcium Oxalate UrolithiasisCalcium oxalate crystal formation also cannot occur in urine undersaturated with its component crystalloids, calcium and oxalate. However, it is not yet clear whether calcium oxalate uroliths will dissolve in vivo in undersaturated urine. Diets promoting the production of urine that is undersaturated with calcium oxalate should prevent the recurrence of calcium oxalate formation after the surgical removal of clinically active uroliths.
While the degree of urinary saturation provides the driving force for calcium oxalate crystallisation, promoters and inhibitors of this process appear of much greater importance than is the case with struvite. Inhibition of crystal growth and aggregation become important if crystal formation cannot be prevented.
Dietary factors that are important in controlling urinary saturation with calcium oxalate include:
• urine pH
• urine volume
• calcium and oxalate intake
Urine pHWALTHAM research suggests that moderately acidic urine is associated with the lowest urinary calcium oxalate saturation in cats. Studies have shown that saturation tended to increase as urine pH became very acidic or moved towards neutrality.
Urine VolumeEnhancement of urine volume and decrease of specific gravity are desirable since this has the effect of decreasing urinary concentrations of calcium and oxalate in a manner comparable to that seen with struvite.
Calcium and Oxalate IntakeIncreased urinary excretion of calcium or oxalate will increase urinary saturation. Dietary restriction of only one of these components may tend, however, to increase absorption of the other.
Effect of Urine pH on Calcium OxalteRelative Supersaturation
Mean urine pH
Undersaturation
5.8 6.1 6.4 6.7 7.0
Calc
ium
oxa
late
RSS
0
1
2
3
4

Module.05 52
Idiopathic FLUTDIn most cats with non-obstructive signs of FLUTD, a specific cause cannot be identified. Clinical signs of idiopathic FLUTD tend to resolve spontaneously within 5-7 days but may recur after a variable period and effective management remains a significant challenge. Idiopathic cystitis in cats has many features in common with interstitial cystitis in humans.
A recent WALTHAM study has demonstrated that dietary intervention can reduce the rate of recurrence of idiopathic cystitis in cats. Cats with idiopathic cystitis were fed either canned or dry formulations of a commercial diet designed to maintain production of an acidic urine. For 89% of cats fed the canned diet, there was no recurrence of signs of FLUTD. Of those fed the dry formulation, signs did not recur in 61% of cats, which is similar to the normal rate of recurrence, irrespective of diet type. Bacterial urinary tract infection was found to be the problem in only one of seven cats available for re-evaluation at recurrence.
Both diets resulted in the production of a moderately acidic urine with a pH that was unlikely to predispose to either struvite or calcium oxalate urolithiasis
Urine specific gravities were lower in cats fed the canned formulation than in those fed the dry diet and may have been a factor in reducing the recurrence of signs. It is possible that the lower urine specific gravities of cats fed the canned diet were related to increased urine volume, as this effect has been observed in clinically normal cats fed the canned diet.
These data suggest that feeding this canned diet may reduce the proportion of cats with idiopathic cystitis that show recurrence of FLUTD within a 12-month period. It is thought that this is the first form of dietary intervention shown to be effective in the management of this condition.
Clinical StudiesUse of Feline pH Control Diet in the management of FLUTD
Data from a series of clinical studies have demonstrated the effectiveness of Feline pH Control Diet in clinical situations and its ability to create and maintain the key parameters of a relatively dilute and acidic urine that are recommended for the management of struvite-associated FLUTD in cats.
(1) In a 48-week clinical study carried out at the University of Queensland, a commercial, acidified diet for the management of struvite urolithiasis (Feline pH Control Diet; canned) was fed to twenty one cats with naturally-occurring FLUTD. Eleven of the cats had a history of obstructive, and ten of non-obstructive FLUTD. The mean (± sd) urine pH values recorded whilst feeding the test diet were 6.15 ± 0.36.
Percentage of Cats with Idiopathic CystitisShowing No Recurrence of LUTD
Time (months)0 2 4 6 8 10 12
% o
f cat
s in
gro
up w
ithou
t rec
urre
nce
0
60
70
80
90
100
110
Canned DietDry Diet

Module.05 53
Eight of the cats had shown 2-4 bouts of disease within the previous 18 months. Once transferred to the test diet, no signs of recurrence were observed over the 48-week study period, although two cats continued to show stranguria up until week 4 and one had signs of postrenal renal failure until week 2.
Considering the previous history of the cats and the high probability of recurrence, this study provided evidence that dietary therapy with Feline pH Control Diet could play a beneficial role in the prevention of recurrence of many cases of obstructive FLUTD.
(2) The role of Feline pH Control Diet (canned) has also been studied in the management of another group of 17 cats with naturally-occurring signs of FLUTD. Dietary therapy resulted in a significant (p<0.05) decrease in both urine pH and specific gravity, and was associated with a reduction in haematuria and struvite crystalluria in most of the cats showing these signs.
No struvite crystals were observed in urine samples that were available for analysis from 16 of the cats during weeks 4 or 5 of the study, compared with 12 cats (of 16 sampled) which showed struvite crystalluria at the start of the study. The results of this study demonstrated the effectiveness of the diet in controlling struvite crystalluria.
Urinary struvite and calcium oxalate saturations in cats fed Feline pH Control Diet
Feline pH Control Diet (canned and dry) was fed in studies to measure urinary struvite saturation and calcium oxalate saturation. The canned diet was fed for 10 days; the dry diet was fed (divided into three meals a day) for a 21 day period. Urine pH was monitored continuously. For 48 hours in the second week of the study all urine voided by the cats was collected. The samples were then processed and the concentrations of appropriate minerals then entered in to a computer programme, which calculates the complex ion concentration and urolith relative supersaturation data.
It was concluded that Feline pH Control Diet produced urine undersaturated with struvite, necessary for urolith dissolution. In addition, Feline Low pH Control Diet (canned) produced urine undersaturated with calcium oxalate. Cats fed Feline Low pH Control Diet (dry) produced urine with a level of saturation well below the estimated formation product of calcium oxalate. Spontaneous homogeneous crystallization will only occur above the formation product.
Studies to evaluate the safety and performance of WALTHAM Veterinary Diet Feline Control pHormula
The key performance criteria for a diet designed for the prevention and management of struvite-associated lower urinary tract diseases are to produce a dilute acidic urine, with a target of maintaining a urine pH of 6.5 and below, whilst avoiding over-acidification, which would tend to promote metabolic acidosis. The diet should also contain restricted quantities of the minerals implicated in struvite formation (magnesium and phosphorus).
To meet AAFCO-accredited feeding requirements, adult maintenance trials have been completed with both canned and dry formulations of WALTHAM Veterinary Diet Feline Control pHormula. These studies were conducted in healthy adult cats over a period of 28 weeks. Parameters assessed included 24-hour urine pH profiles and acid base balance. Both diets achieved consistent urinary acidification with no indication of metabolic acidosis. Overall mean urine pH was 6.4 for the canned diet and 6.3 for the dry diet.

Module.05 54
Key Points• urolithiasis (urinary stones) or urethral plugs are found in around 20% of cases of FLUTD
• struvite is the most common crystalline component of urethral plugs
• calcium oxalate is an important cause of feline urolithiasis in North America
• urinary pH is a key factor in controlling struvite and calcium oxalate crystallisation
• increasing urine volume has diluting effect on the urinary concentration of crystalloids and may help to increase the frequency of urination
• moderate dietary restriction of magnesium and phosphorus may also inhibit struvite formation
• feeding a canned diet which maintains a mildly acidic urine pH can reduce the rate of recurrence of idiopathic cystitis in cats





























