Embed Size (px)
Citation preview

Module 3: Management of Patients on Antiretroviral Therapy
Unit 2: Initiation and Monitoring of ART in Adults
and Adolescents
Objectives
Explain the principles of successful antiretroviral therapy (ART)
Explain ART combinations that are used and the rationale for use of national standardized ART regimens
Explain drug and non-drug related considerations prior to initiating ART
Objectives Explain when ART should be initiated
and who should be started on ART Describe when to change or stop
ART Describe type of monitoring
employed in ART management
Goals of ART 1. Maximal suppression of HIV
replication 2. Restoration and preservation
of immune function 3. Improved Quality of Life 4. Reduction of HIV related
Morbidity and Mortality
1. Suppression of HIV Replication
ARVs must be taken in combination of at least 3 drugs
Strict adherence to treatment is of the upmost importance <95% adherence allows the rapid
development of viral resistance Poor adherers do badly
Fail treatment much earlier
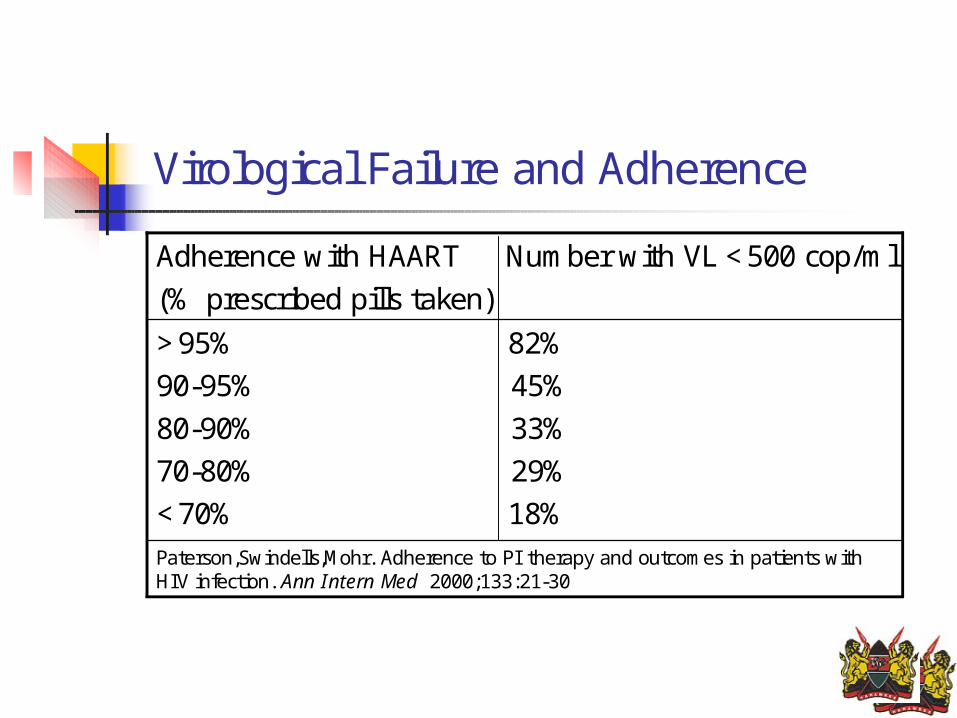
Virological Failure and Adherence
Paterson,Swindells,Mohr. Adherence to PI therapy and outcomes in patients with HIV infection. Ann Intern Med 2000;133:21-30
>95% 82%90-95% 45%80-90% 33%70-80% 29%<70% 18%
Adherence with HAART Number with VL <500 cop/ml(% prescribed pills taken)
2. Immune Reconstitution
ART prevents CD4 destruction by HIV CD4 cell count can recover Improved function of CD4 cells CD4 cells are central to the immune
system So there is improved overall function of the
immune system It takes from 6 to 8 weeks for this to become
evident clinically

3. Improvement of QOL
Decreased hospitalizations Decreased risk of illnesses Increased general well-being Reversal of weight loss Ability to return to work
Take-home Messages about ART
Not an emergency treatment Benefits take 6 to 8 weeks Should not be initiated while an inpatient
Treat opportunistic infections first OI’s cause >90% of morbidity in HIV >90% of OI’s are simple to treat
ART is only one part of HIV Care All who require ART should first be on CPT
first Optimize nutrition
Take-home Messages about ART
Adherence counselling essential Patients should be able to demonstrate an
understanding of: Importance of strict adherence Their ability to afford drugs long term Life-long treatment, monthly follow-up
The Kenyan National Guidelines should be followed “If you don’t agree with them, campaign for a change rather than ignoring them!”
Rationale Behind Standardized ARV Therapy
Success of TB treatment program Simplicity of prescribing Preservation of certain ARV’s on a
population level Simple sequencing of 1st to 2nd line Increased efficiency in drug
procurement Cost and availability of FDC’s
Standard 1st Line Regime for Adults and Adolescents
Lamivudine+
Stavudine+
Nevirapine
Lamivudine+
Stavudine+
Efavirenz
or
Standard 2nd Line Regime
for Adults and Adolescents
Zidovudine+
Didanosine+
Lopinavir/Ritonavir
Zidovudine+
Didanosine+
Nelfinavir
or
For Patients on Non-standard 1st line Regimes…
1st LineD4T+ddI+NNRTI
AZT+3TC+ABC
AZT+3TC+PI
2nd LineAZT+3TC+LPV/r
NNRTI+LPV/r+d4T
NNRTI+ABC+ddI
A note on Fixed Dose Combinations (FDC’s)
WHO Approved FDC’s are available for: d4T/3TC/NVP D4T/3TC AZT/3TC
Advantages Decreased pill burden Increased adherence Mono or duo-therapy not possible Lower cost Simplify stock control and forcasting
GoK has chosen these for the National roll-out

When to Start ART in Adults and Adolescents
Where CD4 testing available
WHO II & III when CD4 < 200/mm3
WHO stage IV irrespective of CD4 level
When to Start ART in Adults and Adolescents
Where CD4 Testing Unavailable
WHO II when total lymphocyte count <1200/mm3
WHO III & IV regardless of total Lymphocyte count
Guidance on Clinical Criteria
CD4 levels are not “hard and fast” rules
A sick, deteriorating patient with a CD4 of 210 should not be excluded from ART if otherwise able and keen to begin
A very well, stable patient with a CD4 of 180 could reasonably opt for close follow up and deferral of ART to a later date
Pregnancy and ART Not a contraindication ART In general, best to defer to after the
first trimester (after organogenesis) EFV contraindicated ART greatly decreases vertical
transmission Also allows mother to remain well to
care for her child
Monitoring of ART (1)
ART is monitored using: Clinical information
Body Weight Signs and symptoms Past and present medical history Physical examination

End Points in Clinical Monitoring
Look for: Decrease or disappearance of
symptoms Increase in body weight Decrease in frequency and
severity of OIs
Monitoring of ART (2)
ART is monitored using: Laboratory Parameters
Minimum - HIV Test, Hb, pregnancy testStandard - FBC, SGPT/ALT, CreatinineDesirable - CD4Optional/Ideal - Viral Load
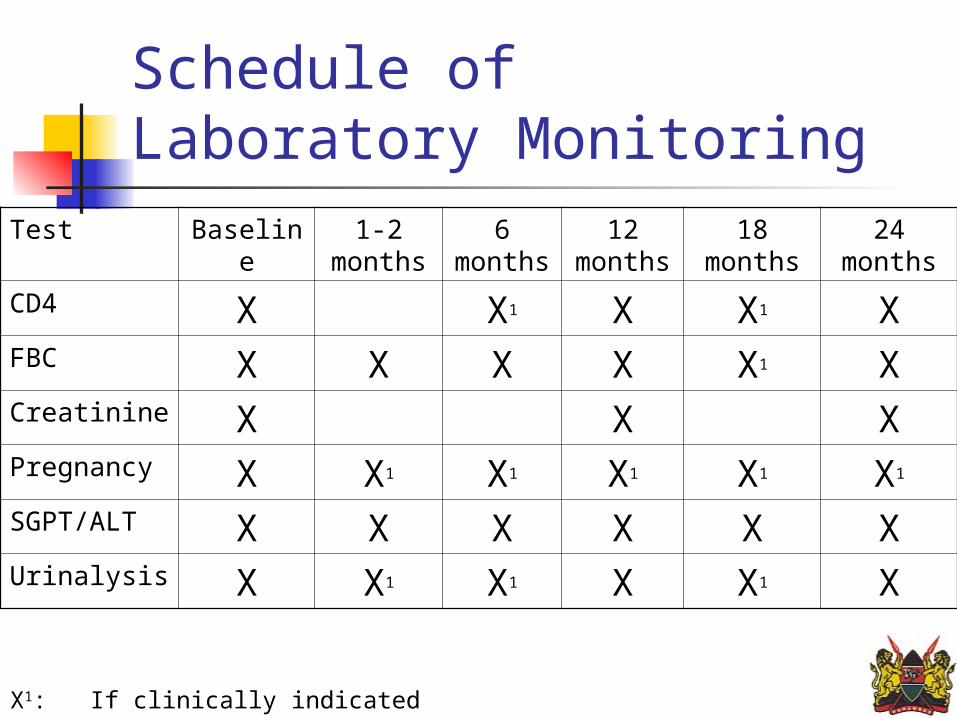
Schedule of Laboratory Monitoring
Test Baseline 1-2 months
6 month
s
12 months
18 months
24 months
CD4 X X1 X X1 XFBC X X X X X1 XCreatinine X X XPregnancy X X1 X1 X1 X1 X1
SGPT/ALT X X X X X XUrinalysis X X1 X1 X X1 X
X1: If clinically indicated












![Rapid advice - WHO · WHO Library Cataloguing-in-Publication Data Rapid advice: antiretroviral therapy for HIV infection in adults and adolescents -November 2009 [electronic version]](https://img.pdfslide.us/doc/110x75/5b378c9d7f8b9a5a518c7e30/rapid-advice-who-library-cataloguing-in-publication-data-rapid-advice-antiretroviral.jpg)














