Embed Size (px)
Citation preview
The Journal of Implant & Advanced Clinical Dentistry
Volume 8, No. 1 march 2016
Treatment of the Atrophic Maxilla with Autogenous Blocks
Modified Mandibular Implant Bar Overdenture

Get Social with
@JIACD on twitter
“JIACD dental journal” on LinkedIn
JIACD on FB
The Journal of Implant & Advanced Clinical Dentistry • 3
The Journal of Implant & Advanced Clinical DentistryVolume 8, No. 1 • march 2016
Table of Contents
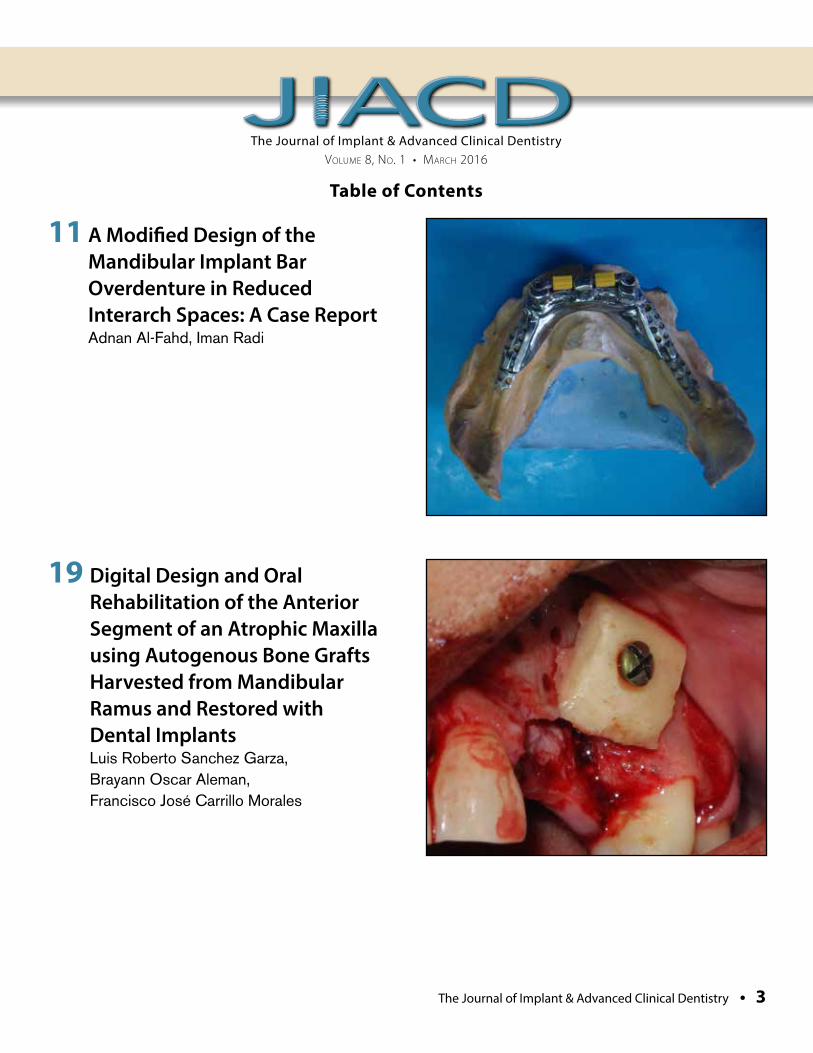
11 A Modified Design of the Mandibular Implant Bar Overdenture in Reduced Interarch Spaces: A Case Report Adnan Al-Fahd, Iman Radi
19 Digital Design and Oral Rehabilitation of the Anterior Segment of an Atrophic Maxilla using Autogenous Bone Grafts Harvested from Mandibular Ramus and Restored with Dental Implants Luis Roberto Sanchez Garza, Brayann Oscar Aleman, Francisco José Carrillo Morales

Autoclavable LED's Progressive Pedal Controlled Power
- Three times more power than PIEZOTOME1! (60 watts vs 18 watts of output power in the handpiece) Procedures are faster than ever, giving you a clean and effortless cut- NEWTRON LED and PIEZOTOME2 LED Handpieces output 100,000 LUX!- Extremely precise irrigation flow to avoid any risk of bone necrosis- Selective cut: respect of soft tissue (nerves, membranes, arteries) - Less traumatic treatment: reduces bone loss and less bleeding- 1st EVER Autoclavable LED Surgical Ultrasonic Handpieces - Giant user-friendly 5.7" color touch-control screen - Ultra-sharp, robust and resistant tips (30+ Surgical & 80+ Conventional)
PIEZOTOME2 and IMPLANT CENTER2
- I-Surge Implant Motor (Contra-Angles not included)- Compatible with all electric contra-angles (any ratio)- Highest torque of any micro-motor on the market- Widest speed range on the market
All the benefits of the PIEZOTOME2...PLUS...
ACTEON North America 124 Gaither Drive, Suite 140 Mount Laurel, NJ 08054Tel - (800) 289 6367 Fax - (856) 222 4726
www.us.acteongroup.com E-mail: [email protected]
..
.
The Journal of Implant & Advanced Clinical Dentistry • 5
The Journal of Implant & Advanced Clinical DentistryVolume 8, No. 1 • march 2016
Table of Contents
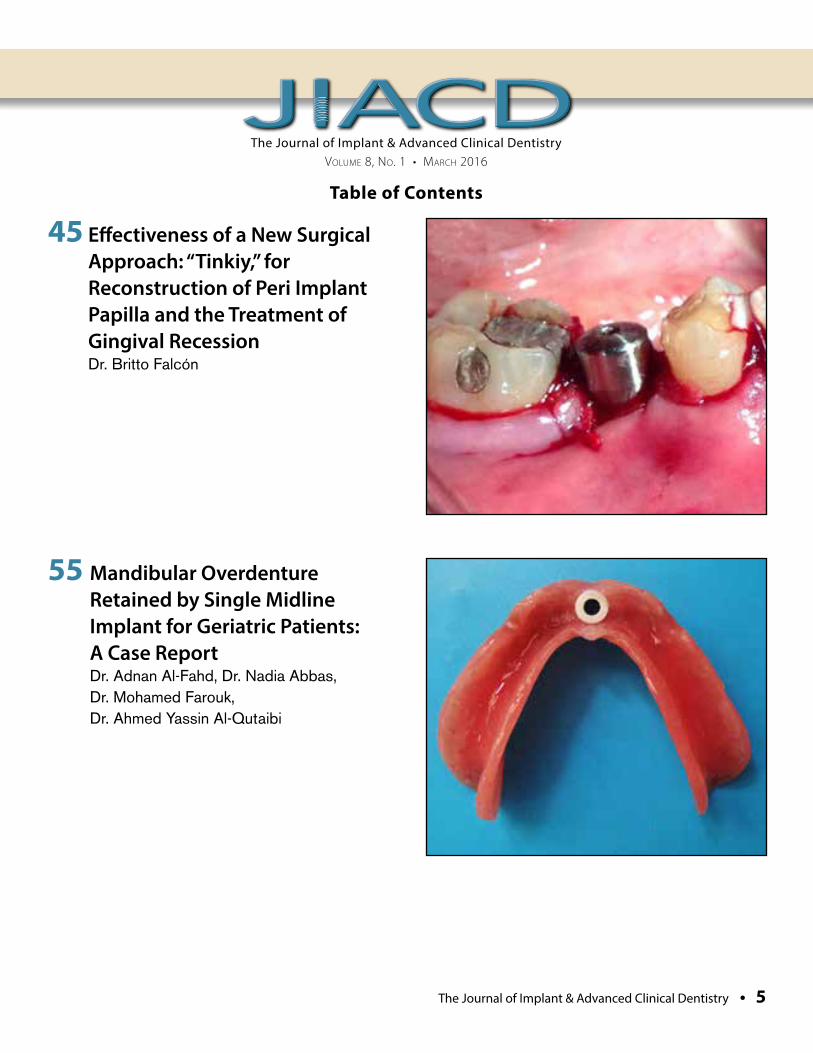
45 Effectiveness of a New Surgical Approach: “Tinkiy,” for Reconstruction of Peri Implant Papilla and the Treatment of Gingival Recession Dr. Britto Falcón
55 Mandibular Overdenture Retained by Single Midline Implant for Geriatric Patients: A Case Report Dr. Adnan Al-Fahd, Dr. Nadia Abbas, Dr. Mohamed Farouk, Dr. Ahmed Yassin Al-Qutaibi

Scan With YourSmartphone!
In order to scan QR codes,your mobile device
must have a QR codereader installed.
Wan
t Reg
ener
ative
Trea
tmen
t Sol
utio
ns?
Try A
n Oss
eoGua
rd® M
embr
ane
And
Endo
bon
® Xeno
graf
t
Granu
les!
OsseoGuard® Membranes And Endobon® Xenograft Granules Provide Clinicians One Solution At A Time
Protect Sites For Consistent Results During
Grafting Procedures
Choose Between Two Levels Of Drapability For Ease Of Use In
Various Clinical Scenarios
Slow Resorption ForBone Volume Retention
Conveniently PackagedIn NEW Value Packs
For More InformationAbout BIOMET 3iRegenerative Treatment Solutions, Contact YourLocal Sales Representative Today! In the USA: 1-888-800-8045, Outside The USA: +1-561-776-6700 Or Visit Us Online At www.biomet3i.com
Endobon, OsseoGuard and RegenerOss are registered trademarks of BIOMET 3i LLC.OsseoGuard Flex and Providing Solutions - One Patient At A Time are trademarks ofBIOMET 3i LLC. ©2011 BIOMET 3i LLC.
ClinicallyManageable
Value Packs
Bone Volume
MaintenancePredictable
INTRODUCING
Join Us
Follow Us
Watch Us
DownloadIt
Regenerative Treatment Solutions
NEWPACKAGING
NEWOsseoGuard Flex™
Membrane
OsseoGuard® Membrane And The NEW OsseoGuard Flex™ Membrane
Endobon® Xenograft GranulesWith NEW Packaging
JIACD_Jan2012_BIOMET 3i 12/16/11 5:10 PM Page 1

The Journal of Implant & Advanced Clinical Dentistry • 7
The Journal of Implant & Advanced Clinical DentistryVolume 8, No. 1 • march 2016
PublisherLC Publications
DesignJimmydog Design Group www.jimmydog.com
Production ManagerStephanie Belcher 336-201-7475 • [email protected]
Copy EditorJIACD staff
Digital ConversionJIACD staff
Internet ManagementInfoSwell Media
Subscription Information: Annual rates as follows: Non-qualified individual: $99(USD) Institutional: $99(USD). For more information regarding subscriptions, contact [email protected] or 1-888-923-0002.
Advertising Policy: All advertisements appearing in the Journal of Implant and Advanced Clinical Dentistry (JIACD) must be approved by the editorial staff which has the right to reject or request changes to submitted advertisements. The publication of an advertisement in JIACD does not constitute an endorsement by the publisher. Additionally, the publisher does not guarantee or warrant any claims made by JIACD advertisers.
For advertising information, please contact:[email protected] or 1-888-923-0002
Manuscript Submission: JIACD publishing guidelines can be found at http://www.jiacd.com/author-guidelines or by calling 1-888-923-0002.
Copyright © 2016 by LC Publications. All rights reserved under United States and International Copyright Conventions. No part of this journal may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying or any other information retrieval system, without prior written permission from the publisher.
Disclaimer: Reading an article in JIACD does not qualify the reader to incorporate new techniques or procedures discussed in JIACD into their scope of practice. JIACD readers should exercise judgment according to their educational training, clinical experience, and professional expertise when attempting new procedures. JIACD, its staff, and parent company LC Publications (hereinafter referred to as JIACD-SOM) assume no responsibility or liability for the actions of its readers.
Opinions expressed in JIACD articles and communications are those of the authors and not necessarily those of JIACD-SOM. JIACD-SOM disclaims any responsibility or liability for such material and does not guarantee, warrant, nor endorse any product, procedure, or technique discussed in JIACD, its affiliated websites, or affiliated communications. Additionally, JIACD-SOM does not guarantee any claims made by manufact-urers of products advertised in JIACD, its affiliated websites, or affiliated communications.
Conflicts of Interest: Authors submitting articles to JIACD must declare, in writing, any potential conflicts of interest, monetary or otherwise, that may exist with the article. Failure to submit a conflict of interest declaration will result in suspension of manuscript peer review.
Erratum: Please notify JIACD of article discrepancies or errors by contacting [email protected]
JIACD (ISSN 1947-5284) is published on a monthly basis by LC Publications, Las Vegas, Nevada, USA.
The Journal of Implant & Advanced Clinical Dentistry • 9
Tara Aghaloo, DDS, MDFaizan Alawi, DDSMichael Apa, DDSAlan M. Atlas, DMDCharles Babbush, DMD, MSThomas Balshi, DDSBarry Bartee, DDS, MDLorin Berland, DDSPeter Bertrand, DDSMichael Block, DMDChris Bonacci, DDS, MDHugo Bonilla, DDS, MSGary F. Bouloux, MD, DDSRonald Brown, DDS, MSBobby Butler, DDSNicholas Caplanis, DMD, MSDaniele Cardaropoli, DDSGiuseppe Cardaropoli DDS, PhDJohn Cavallaro, DDSJennifer Cha, DMD, MSLeon Chen, DMD, MSStepehn Chu, DMD, MSD David Clark, DDSCharles Cobb, DDS, PhDSpyridon Condos, DDSSally Cram, DDSTomell DeBose, DDSMassimo Del Fabbro, PhDDouglas Deporter, DDS, PhDAlex Ehrlich, DDS, MSNicolas Elian, DDSPaul Fugazzotto, DDSDavid Garber, DMDArun K. Garg, DMDRonald Goldstein, DDSDavid Guichet, DDSKenneth Hamlett, DDSIstvan Hargitai, DDS, MS
Michael Herndon, DDSRobert Horowitz, DDSMichael Huber, DDSRichard Hughes, DDSMiguel Angel Iglesia, DDSMian Iqbal, DMD, MSJames Jacobs, DMDZiad N. Jalbout, DDSJohn Johnson, DDS, MSSascha Jovanovic, DDS, MSJohn Kois, DMD, MSDJack T Krauser, DMDGregori Kurtzman, DDSBurton Langer, DMDAldo Leopardi, DDS, MSEdward Lowe, DMDMiles Madison, DDSLanka Mahesh, BDSCarlo Maiorana, MD, DDSJay Malmquist, DMDLouis Mandel, DDSMichael Martin, DDS, PhDZiv Mazor, DMDDale Miles, DDS, MSRobert Miller, DDSJohn Minichetti, DMDUwe Mohr, MDTDwight Moss, DMD, MSPeter K. Moy, DMDMel Mupparapu, DMDRoss Nash, DDSGregory Naylor, DDSMarcel Noujeim, DDS, MSSammy Noumbissi, DDS, MSCharles Orth, DDSAdriano Piattelli, MD, DDSMichael Pikos, DDSGeorge Priest, DMDGiulio Rasperini, DDS
Michele Ravenel, DMD, MSTerry Rees, DDSLaurence Rifkin, DDSGeorgios E. Romanos, DDS, PhDPaul Rosen, DMD, MSJoel Rosenlicht, DMDLarry Rosenthal, DDSSteven Roser, DMD, MDSalvatore Ruggiero, DMD, MDHenry Salama, DMDMaurice Salama, DMDAnthony Sclar, DMDFrank Setzer, DDSMaurizio Silvestri, DDS, MDDennis Smiler, DDS, MScDDong-Seok Sohn, DDS, PhDMuna Soltan, DDSMichael Sonick, DMDAhmad Soolari, DMDNeil L. Starr, DDSEric Stoopler, DMDScott Synnott, DMDHaim Tal, DMD, PhDGregory Tarantola, DDSDennis Tarnow, DDSGeza Terezhalmy, DDS, MATiziano Testori, MD, DDSMichael Tischler, DDSTolga Tozum, DDS, PhDLeonardo Trombelli, DDS, PhDIlser Turkyilmaz, DDS, PhDDean Vafiadis, DDSEmil Verban, DDSHom-Lay Wang, DDS, PhDBenjamin O. Watkins, III, DDSAlan Winter, DDSGlenn Wolfinger, DDSRichard K. Yoon, DDS
Editorial Advisory Board
Founder, Co-Editor in ChiefDan Holtzclaw, DDS, MS
Co-Editor in ChiefLeon Chen, DMD, MS, DICOI, DADIA
The Journal of Implant & Advanced Clinical Dentistry

Al-Fahd et al
DID YOU KNOW?Roxolid implants deliver more treatment options
Roxolid is optimal for treatment of narrow interdental spaces.
Case courtesy of Dr. Mariano Polack and Dr. Joseph Arzadon, Gainesville, VA
Contact Straumann Customer Service at 800/448 8168 to learn more about Roxolid or to locate a representative in your area.
www.straumann.us
Al-Fahd et al
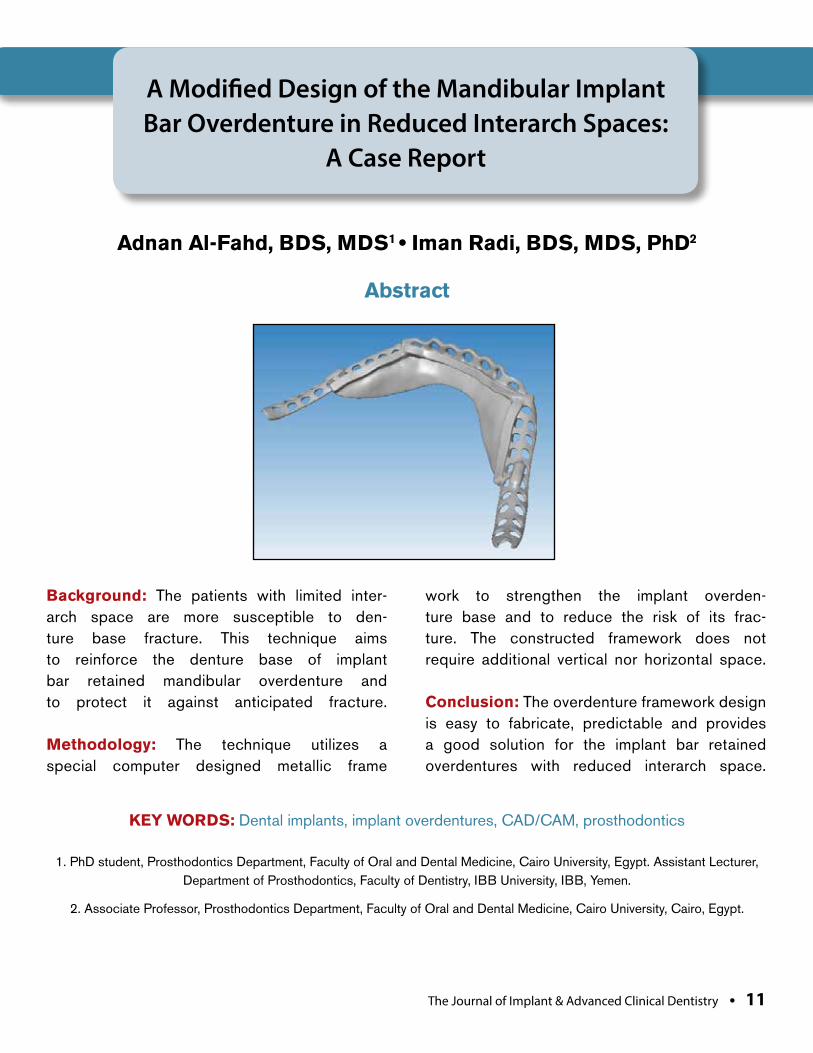
Background: The patients with limited inter-arch space are more susceptible to den-ture base fracture. This technique aims to reinforce the denture base of implant bar retained mandibular overdenture and to protect it against anticipated fracture.
Methodology: The technique utilizes a special computer designed metallic frame
work to strengthen the implant overden-ture base and to reduce the risk of its frac-ture. The constructed framework does not require additional vertical nor horizontal space.
Conclusion: The overdenture framework design is easy to fabricate, predictable and provides a good solution for the implant bar retained overdentures with reduced interarch space.
A Modified Design of the Mandibular Implant Bar Overdenture in Reduced Interarch Spaces:
A Case Report
Adnan Al-Fahd, BDS, MDS1 • Iman Radi, BDS, MDS, PhD2
1. PhD student, Prosthodontics Department, Faculty of Oral and Dental Medicine, Cairo University, Egypt. Assistant Lecturer, Department of Prosthodontics, Faculty of Dentistry, IBB University, IBB, Yemen.
2. Associate Professor, Prosthodontics Department, Faculty of Oral and Dental Medicine, Cairo University, Cairo, Egypt.
Abstract
KEY WORDS: Dental implants, implant overdentures, CAD/CAM, prosthodontics
The Journal of Implant & Advanced Clinical Dentistry • 11
12 • Vol. 8, No. 1 • March 2016
INTRODUCTION The value of implant overdentures in improv-ing denture retention, stability, masticatory performance, quality of life, and patient sat-isfaction has been extensively evaluated and well documented by many studies. Mandibu-lar overdentures retained by two implants
are considered as the first line of treatment for completely edentulous mandible.1–6 Frac-ture of the implant overdenture is not an uncommon problem which frustrates both cli-nicians and patients. It occurs mainly at the midline or at the implant abutments. Patients with limited interarch space show more
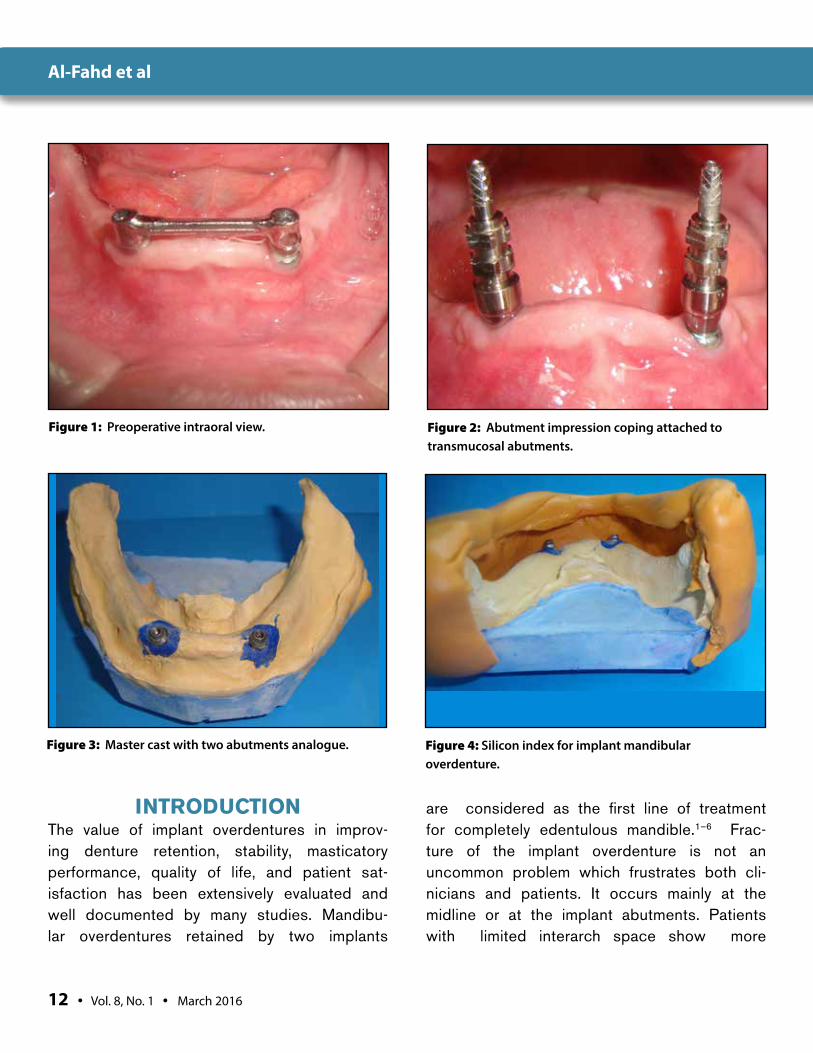
Figure 1: Preoperative intraoral view. Figure 2: Abutment impression coping attached to transmucosal abutments.
Figure 3: Master cast with two abutments analogue. Figure 4: Silicon index for implant mandibular overdenture.
Al-Fahd et al
The Journal of Implant & Advanced Clinical Dentistry • 13
liability to denture fracture due to limited amount of acrylic resin, especially over attach-ments areas.7–9 Enhancement of the denture base strength by incorporation metal or fiber reinforcements has been reported by many studies. But most of these techniques involve complete embedding of the metal reinforce-
ment inside the denture base and its exten-sion over the present the bar attachments, which requires additional vertical interarch space.10–12 Unlike the previous methods, the present technique provides sufficient reinforce-ment for the denture base without additional space requirements. The technique utilizes the
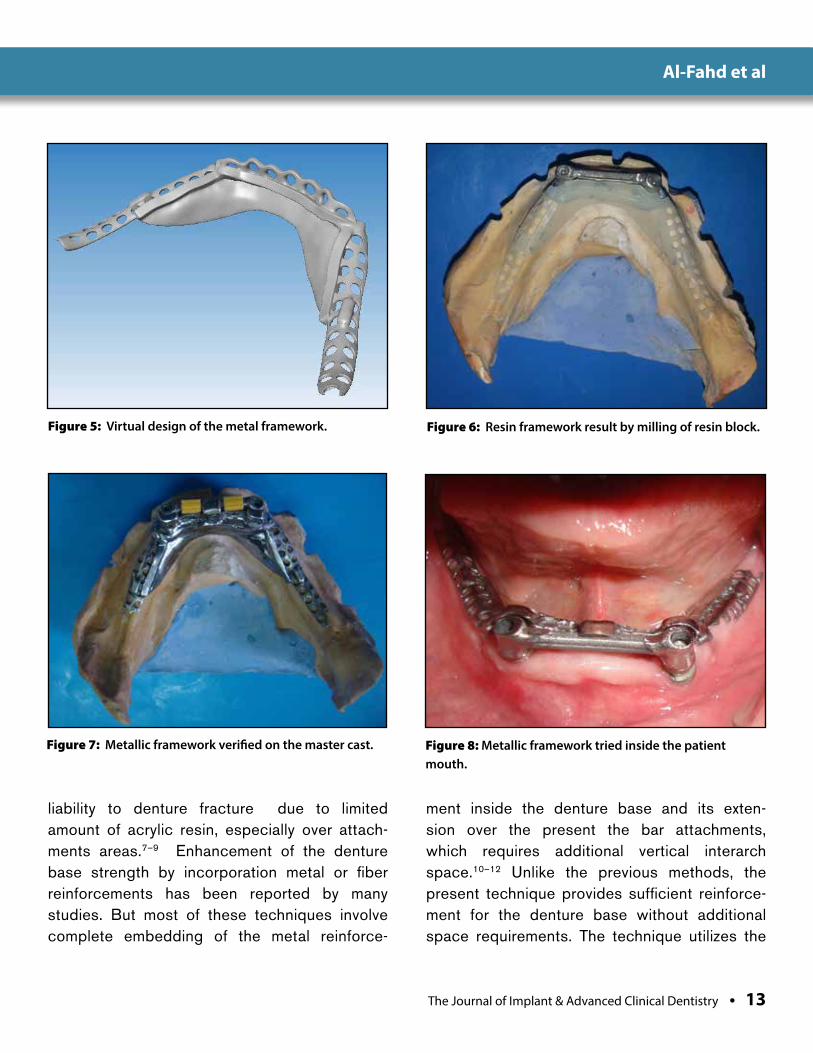
Figure 5: Virtual design of the metal framework. Figure 6: Resin framework result by milling of resin block.
Figure 7: Metallic framework verified on the master cast. Figure 8: Metallic framework tried inside the patient mouth.
Al-Fahd et al
14 • Vol. 8, No. 1 • March 2016
(CAD/CAM) technology with all of its advan-tages and is especially beneficial for patients with limited interarch space as in our case.
METHODOLOGY A 67 year old Egyptian male wearing a man-dibular bar-retained implant overdenture oppos-ing maxillary conventional complete denture presented to our outpatient clinic of Faculty of Oral and Dental Medicine-Cairo University with a complaint of repeated fractures and frequent repairs of his prosthesis (Fig.1). After examina-tion, the plan was to reinforce the denture base with a metal framework in the following steps:
1. After unscrewing the bar, impression cop-ings were connected to underlying Transmuco-sal abutments (Fig.2). Then, abutment level final impression was taken using open tray impres-sion technique using additional silicon impression material. Before pouring with extra hard stone, abutment analogues were fastened to the impres-sion copings to produce a master cast (Fig.3).
2. The jaw relation was recorded with the
maxillary denture in place to perform a diagnostic set up for the lower denture. A silicon index was then constructed to evaluate the space available for the bar attachment assembly, possible rein-forcement material, acrylic resin of denture base and the artificial teeth. This revealed an insuf-ficient space for the bar, clip, teeth and denture base which dictated the necessity for reinforc-ing the denture over the bar attachment with-out encroaching on the vertical space (Fig.4).
3. The cast with the bar was then scanned by a 3D scanner (SHERA eco-scan, Germany) to obtain the virtual model.
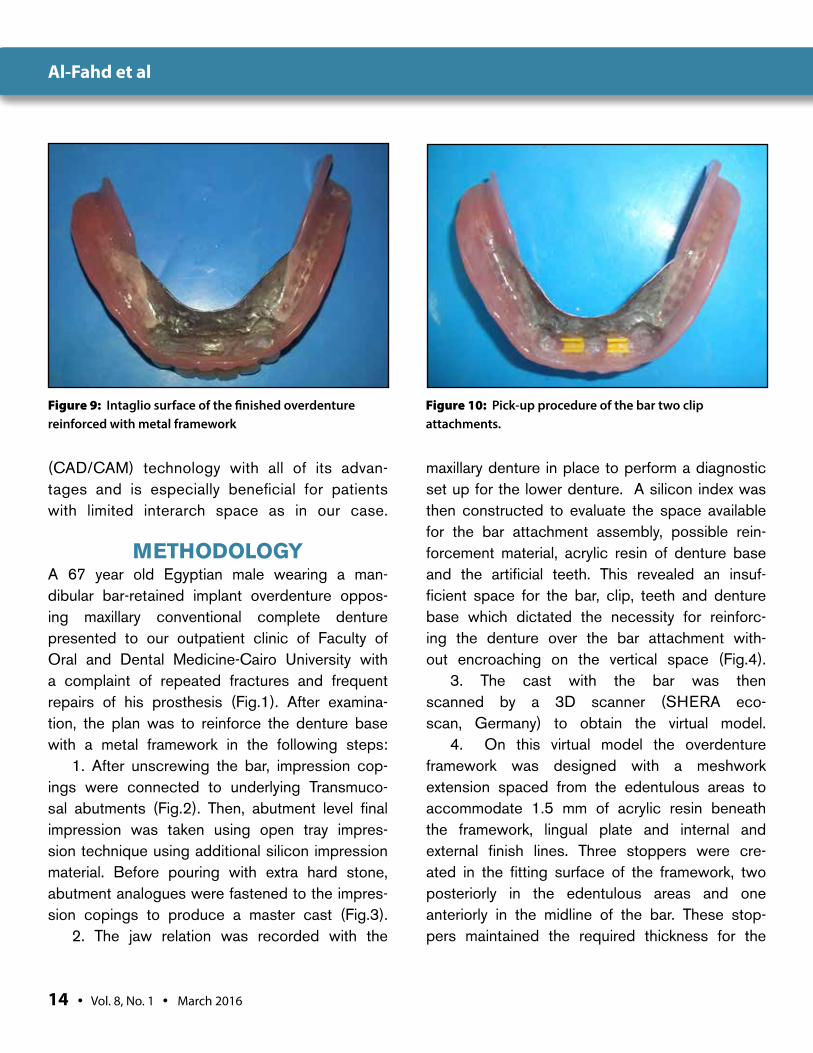
4. On this virtual model the overdenture framework was designed with a meshwork extension spaced from the edentulous areas to accommodate 1.5 mm of acrylic resin beneath the framework, lingual plate and internal and external finish lines. Three stoppers were cre-ated in the fitting surface of the framework, two posteriorly in the edentulous areas and one anteriorly in the midline of the bar. These stop-pers maintained the required thickness for the
Figure 9: Intaglio surface of the finished overdenture reinforced with metal framework
Figure 10: Pick-up procedure of the bar two clip attachments.
Al-Fahd et al

The Journal of Implant & Advanced Clinical Dentistry • 15
Figure 11: Intraoral anterior view of finished denture. Figure 12: Extraoral view with patient smiling.
acrylic resin of the denture base and for the clips of the bar attachments respectively (Fig.5).
5. The milling machine (SHERA eco-mil 5X, Germany) was used to convert the virtual frame-work into acrylic resin framework (Copra Plex PMMA milling blank, Germany) (Fig.6). A small horizontal extension was added manually by mill-ing wax because the version of milling machine was not capable of doing this particular func-tion. The framework was then converted into a metal framework (cobalt-chromium) using the conventional casting procedures (Fig.7).
6. The framework was then tried in intra-orally to verify its seating, stability and the designed space for bar clips (Fig.8).
7. The overdenture was then constructed in a conventional manner, where the mesh part of the framework was totally embedded in acrylic resin of the denture base, which terminated at the fin-ish lines of the metal framework (Fig.9). The bar clips were then picked up directly inside patient's mouth with cold cure acrylic resin (Fig.10)
8. The patient was satisfied with the
new denture and followed up for one year without complications (Figs.11&12).
DISCUSSION Denture base fracture is a common compli-cation encountered with implant-supported overdentures. The prevalence of the frac-ture rate was reported to be of 21.4% for the 1-implant-supported overdenture and 9.3% for the 2-implant-supported overden-ture designs.13 Fracture of the prosthesis is more likely to occur when there is sufficient space for the attachment system and denture teeth. This case presented with limited inter-arch space with complaint of repeated fracture that cannot be managed in conventional pro-cedure by covering the bar attachment with metal framework because the patient had lim-ited interarch space. Consequently, the novel approach in this technique was planned to provide a required metallic reinforcement for denture base without encouragement for the available vertical space. In addition, adequate
Al-Fahd et al

16 • Vol. 8, No. 1 • March 2016
space on the lingual side of bar was allowed at the anticipated bar clip positions to allow for subsequent pick-up procedure. The frame work was designed as a plate-form to provide the proper denture base strengthening with excellent retention to the acrylic resin and in the same time not restrict the tongue move-ment. We use computer in framework designing and then milling into hard milling resin because it is more accurate and to minimize process-ing errors that may happen with conventional waxing procedure. However, it is important to mention here why we don’t perform direct mill-ing into metal frame work because lack of such equipment in our country until now. Finally, this technique is simple, reliable, time saving, rela-tively low cost if compared with many conven-tional denture base replacements in cases that are more susceptible to frequent fracturing.
CONCLUSION This technique is used to reinforce overden-ture with metal framework to avoid anticipated fracture. It involves virtual planning for frame-work on especial software designing program then milling and casting in usual manner. This technique is beneficial for strengthening the implant overdenture base especially for those patients with limited interarch space as it did not require and additional vertical space. ●
Correspondence:Dr. Adnan Abdullah Al-FahdEmail: [email protected]: 2 Ali Attiya Hadayek Almaadi Cario, EgyptTel. No: 00201142228430
AcknowledgementSpecial thanks to Dr. Amr Hosni for his contribution to the laboratory part of this report.
Disclosure:The authors report no conflicts of interest with anything mentioned within this article.
References1. Burns DR, Unger JW, Coffey JP, Waldrop TC, Elswick RK. Randomized, pro-
spective, clinical evaluation of prosthodontic modalities for mandibular implant overdenture treatment. J Prosthet Dent [Internet]. The Editorial Council of the Journal of Prosthetic Dentistry; 2011 Jul [cited 2013 May 8];106(1):12–22.
2. Thomason JM, Feine J, Exley C, Moynihan P, Müller F, Naert I, et al. Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients--the York Consensus State-ment. Br Dent J. Nature Publishing Group; 2009;207(4):185–6.
3. Meijer HJA, Raghoebar GM, Van’t Hof MA, Visser A. A controlled clini-cal trial of implant-retained mandibular overdentures: 10 years’ results of clinical aspects and aftercare of IMZ implants and Branemark implants. Clin Oral Implants Res. Denmark; 2004 Aug;15(4):421–7.
4. Bergendal T, Engquist B. Implant-supported overdentures: a longitudinal pro-spective study. Int J Oral Maxillofac Implants [Internet]. 2000;13(2):253–62.
5. Brennan M, Houston F, O’Sullivan M, O’Connell B. Patient satisfac-tion and oral health-related quality of life outcomes of implant over-dentures and fixed complete dentures. Int J Oral Maxillofac Implants [Internet]. 2007 Jan [cited 2015 Sep 27];25(4):791–800.
6. Meijer HJ, Raghoebar GM, Van’t Hof M a, Geertman ME, Van Oort RP. Implant-retained mandibular overdentures compared with complete den-tures; a 5-years’ follow-up study of clinical aspects and patient satisfac-tion. [Internet]. Clinical oral implants research. 1999. p. 238–44.
7. Hemmings KW, Schmitt A, Zarb GA. Complications and mainte-nance requirements for fixed prostheses and overdentures in the edentulous mandible: a 5-year report. Int J Oral Maxillofac Implants [Internet]. 1994 Jan [cited 2014 Apr 24];9(2):191–6.
8. Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JYK. Clini-cal complications with implants and implant prostheses. J Prosthet Dent [Internet]. 2003 Aug [cited 2014 Mar 24];90(2):121–32.
9. Gonda T, Maeda Y, Walton JN, MacEntee MI. Fracture inci-dence in mandibular overdentures retained by one or two implants. J Prosthet Dent [Internet]. 2010;103(3):178–81.
10. Özçelik TB, Yılmaz B, Akçimen Y. Metal reinforcement for implant-supported mandibular overdentures. J Prosthet Dent [Inter-net]. 2013 May [cited 2015 Nov 7];109(5):338–40.
11. Rodrigues AH. Metal reinforcement for implant-sup-ported mandibular overdentures. J Prosthet Dent [Inter-net]. 2000 May [cited 2015 Nov 7];83(5):511–3.
12. Vallittu PK. A Review of Methods Used to Reinforce Poly-methyl Methacrylate Resin. J Prosthod. 1995;4:183–7.
13. Gonda T, Maeda Y, Walton JN, MacEntee MI. Fracture incidence in mandibular overdentures retained by one or two implants. J Pros-thet Dent [Internet]. The Editorial Council of the Journal of Pros-thetic Dentistry; 2010 Mar [cited 2013 Apr 27];103(3):178–81.
Al-Fahd et al
The Journal of Implant & Advanced Clinical Dentistry • XX
Al-Fahd et al
For more information, contact BioHorizonsCustomer Care: 1.888.246.8338 or shop online at www.biohorizons.com
SPMP12245 REV A SEP 2012
make the switch
The Tapered Plus implant system offers all the great benefits of BioHorizons highly successful Tapered Internal system PLUS it features a Laser-Lok treated beveled-collar for bone and soft tissue attachment and platform switching designed for increased soft tissue volume.
Laser-Lok® zoneCreates a connective tissue seal and maintains crestal bone
platform switchingDesigned to increase soft tissue volume around the implant connection
optimized threadformButtress thread for primary stability and maximum bone compression
prosthetic indexingConical connection with internal hex; color-coded for easy identification

Garza et al
Click For Our Quantity
Discount Options
www.exac.com/QuantityDiscountOptions
© 2
012
Exac
tech
, Inc
.
Oralife is a single donor grafting product processed in accordance with AATB standards as well as state and federal regulations (FDA and the states of Florida, California, Maryland and New York). Oralife allografts are processed by LifeLink Tissue Bank and distributed by Exactech Inc.1. Data on file at Exactech. 2. McAllister BS, Hagnignat K. Bone augmentation techniques. J Periodontal. 2007 Mar; 78(3):377-96. 3. Blum B, Moseley J, Miller L, Richelsoph K, Haggard W. Measurement of bone morphogenetic proteins and
other growth factors in demineralized bone matrix. Orthopedics. 2004 Jan;27(1 Suppl):s161-5.
What’s Your Sign?
www.exac.com/dental1-866-284-9690
• Cost-effectivegraftingmaterial
• Validatedtomaintainosteoinductivityand biomechanical integrity1
• MixtureofDBMwithmineral-retained cortical and cancellous chips, processed in a manner to retainthenaturally-occuringgrowthfactors(BMP)andbeaconductivelattice – all in one product1,2,3
NEW Oralife Plus Combination Allograft available now!
MEET OUR
PlusA QUALITY COMBINATION
Garza et al
Background: The surgical procedures involved in the restoration of the tissue architecture of the dental arches have been studied, developed, and modified throughout the years, and have reported great success. However, in some cases it’s diffi-cult to restore the complete anatomy of the den-tal arches even when multiple interventions of the soft and hard tissue have been performed.
Methods: A 54 years old female patient feel-ing social discomfort due to the absence of a superior tooth of the anterior segment of the maxilla which was removed by a den-tist about 10 years ago due to an apical rhi-zolysis caused by an included canine with an extensive resorption of the alveolar ridge
Results: Through the therapy applied, we were able to establish the functional parameters of chewing, swallowing, pho-netics, smile symmetry, harmony and dental shade and shape match resulting in phys-ical and psychological comfort of our patient.
Conclusions: The key facts to success in any treatment are, always keeping in mind the concern and desires of the patient, full under-standing and analysis of the case, a care-ful planning by the multidisciplinary team and always communicate to the patient what treat-ment options they have, what they consist and the expectations of the final result as well.
Digital Design and Oral Rehabilitation of the Anterior Segment of an Atrophic Maxilla using
Autogenous Bone Grafts Harvested from Mandibular Ramus and Restored with Dental Implants
Luis Roberto Sanchez Garza, DDS1 Brayann Oscar Aleman, DDS2 • Francisco José Carrillo Morales, DDS3
1.Oral and Maxillofacial Surgeon, Department of Oral and Maxillofacial Surgery ISSSTE Monterrey, Nuevo León, México; Private Practice Monterrey, Nuevo León, Mexico
2. Private Practice, Monterrey, Mexico
3. Private Practice Monterrey, Mexico
Abstract
KEY WORDS: Dental implants, digital design, atrophic maxilla, bone graft, rehabilitation
The Journal of Implant & Advanced Clinical Dentistry • 19
20 • Vol. 8, No. 1 • March 2016
INTRODUCTIONThe surgical procedures involved in the restora-tion of tissue architecture of the dental arches have been studied, developed, and modified throughout the years and have reported great success rates. Kois et al1 stated that the predict-ability of the final aesthetic result depends on the anatomy presented by the patient and the capac-ity of the dental surgeon to perform the required procedures. However, in some cases it’s difficult to restore the complete anatomy of the dental arches even when multiple interventions of the soft and hard tissue have been performed. It’s important to state that if the dental arches cannot be restored completely by the dental surgeon, the
clinician may support on the laboratory technician by sending dental models of the patient as the last attempt of “saving” the case by compensat-ing the not fully recovered anatomy of the dental arch on the prosthesis.1 The resultant prosthesis often meets the functional requirements but some-times it’s considered as a failure in the aesthetic point, and can cause frustration to the patient and the interdisciplinary team, as it differs from the aesthetic goals that initially where settled. That’s why it is imperative to make a good diagnosis, treatment plan, with the interdisciplinary team and inform the patient about the expected outcome and the possibilities of the different outcomes. Alternatives for prosthetic restoration for the gin-gival tissue should be presented to the patient.
ADVANTAGES ● Improve the white (teeth) and pink (gingiva)
appearance.● Reduce the necessity of complex additional
surgical interventions.● Improve the intraoral commodity to establish
a soft and uniform interphase between the gingival tissue, prosthesis and remanecents.
● Simplify the treatment, which reduce time and costs.
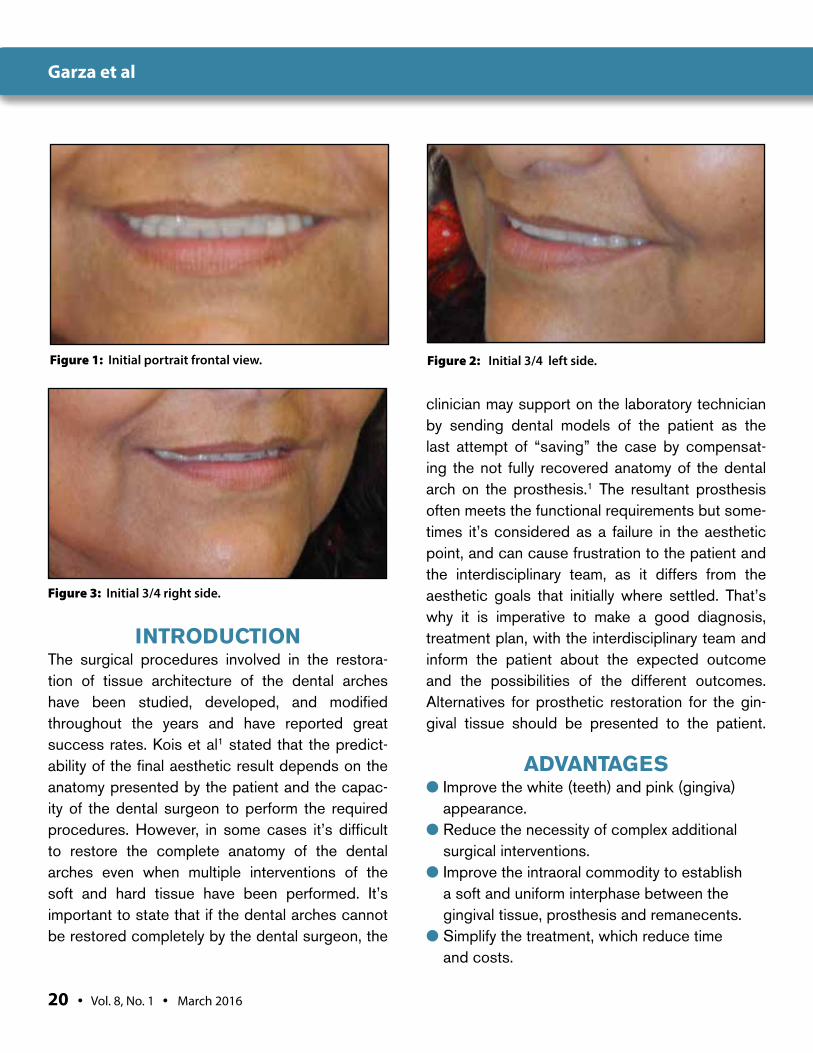
Figure 1: Initial portrait frontal view. Figure 2: Initial 3/4 left side.
Figure 3: Initial 3/4 right side.
Garza et al
The Journal of Implant & Advanced Clinical Dentistry • 21
● It corrects different maxillofacial defects, compensating the inadequate maxilla-mandibular relationship promoting the necessary seal for correct phonetics.
DISADVANTAGES● Requires additional motivation and discipline to
perform rigorous maintenance procedures that are critical for the proper periodontal and peri-implant health.
● The patient expectations can be a problem if this procedure is not explained in the initial planification.2
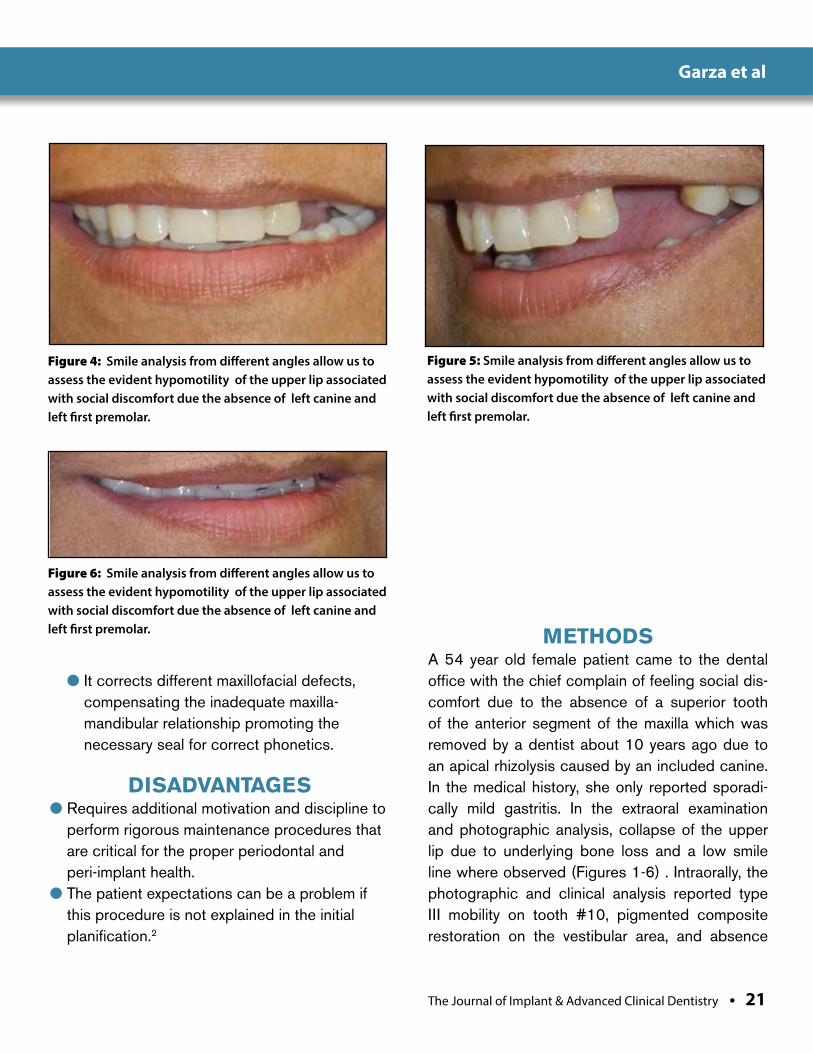
METHODSA 54 year old female patient came to the dental office with the chief complain of feeling social dis-comfort due to the absence of a superior tooth of the anterior segment of the maxilla which was removed by a dentist about 10 years ago due to an apical rhizolysis caused by an included canine. In the medical history, she only reported sporadi-cally mild gastritis. In the extraoral examination and photographic analysis, collapse of the upper lip due to underlying bone loss and a low smile line where observed (Figures 1-6) . Intraorally, the photographic and clinical analysis reported type III mobility on tooth #10, pigmented composite restoration on the vestibular area, and absence
Figure 4: Smile analysis from different angles allow us to assess the evident hypomotility of the upper lip associated with social discomfort due the absence of left canine and left first premolar.
Figure 5: Smile analysis from different angles allow us to assess the evident hypomotility of the upper lip associated with social discomfort due the absence of left canine and left first premolar.
Figure 6: Smile analysis from different angles allow us to assess the evident hypomotility of the upper lip associated with social discomfort due the absence of left canine and left first premolar.
Garza et al
22 • Vol. 8, No. 1 • March 2016
Garza et al
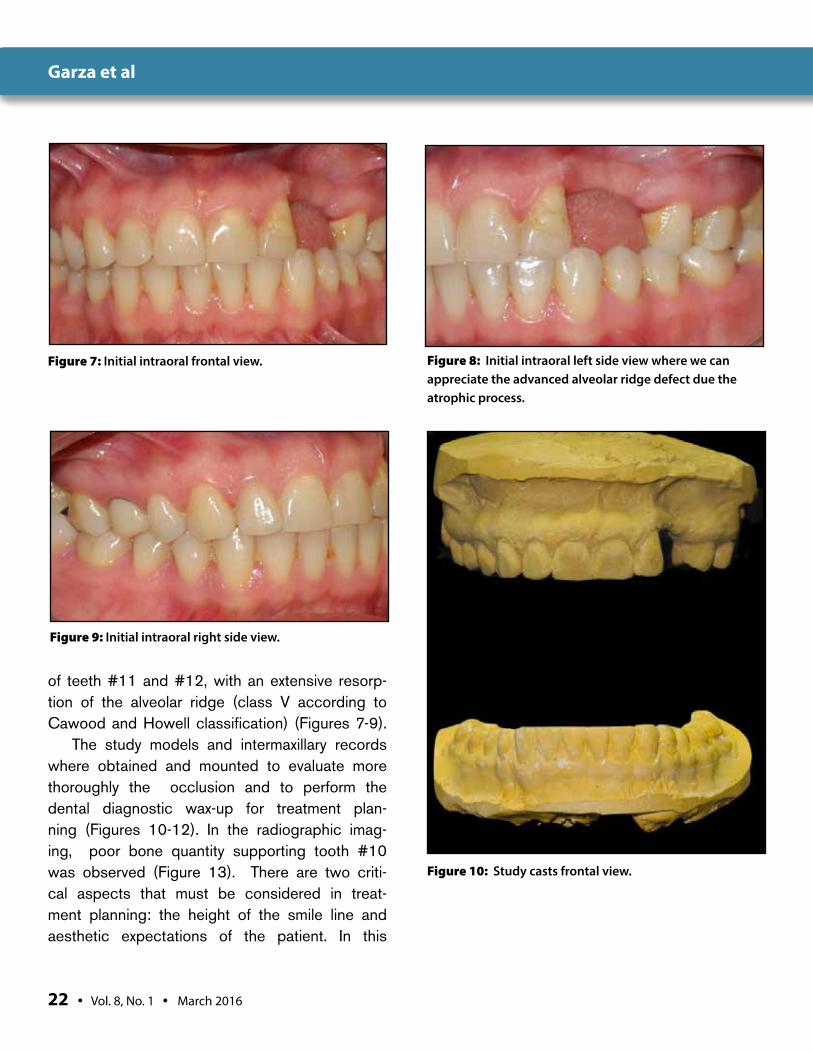
Figure 7: Initial intraoral frontal view. Figure 8: Initial intraoral left side view where we can appreciate the advanced alveolar ridge defect due the atrophic process.
Figure 9: Initial intraoral right side view.
Figure 10: Study casts frontal view.
of teeth #11 and #12, with an extensive resorp-tion of the alveolar ridge (class V according to Cawood and Howell classification) (Figures 7-9).
The study models and intermaxillary records where obtained and mounted to evaluate more thoroughly the occlusion and to perform the dental diagnostic wax-up for treatment plan-ning (Figures 10-12). In the radiographic imag-ing, poor bone quantity supporting tooth #10 was observed (Figure 13). There are two criti-cal aspects that must be considered in treat-ment planning: the height of the smile line and aesthetic expectations of the patient. In this
The Journal of Implant & Advanced Clinical Dentistry • 23
Garza et al
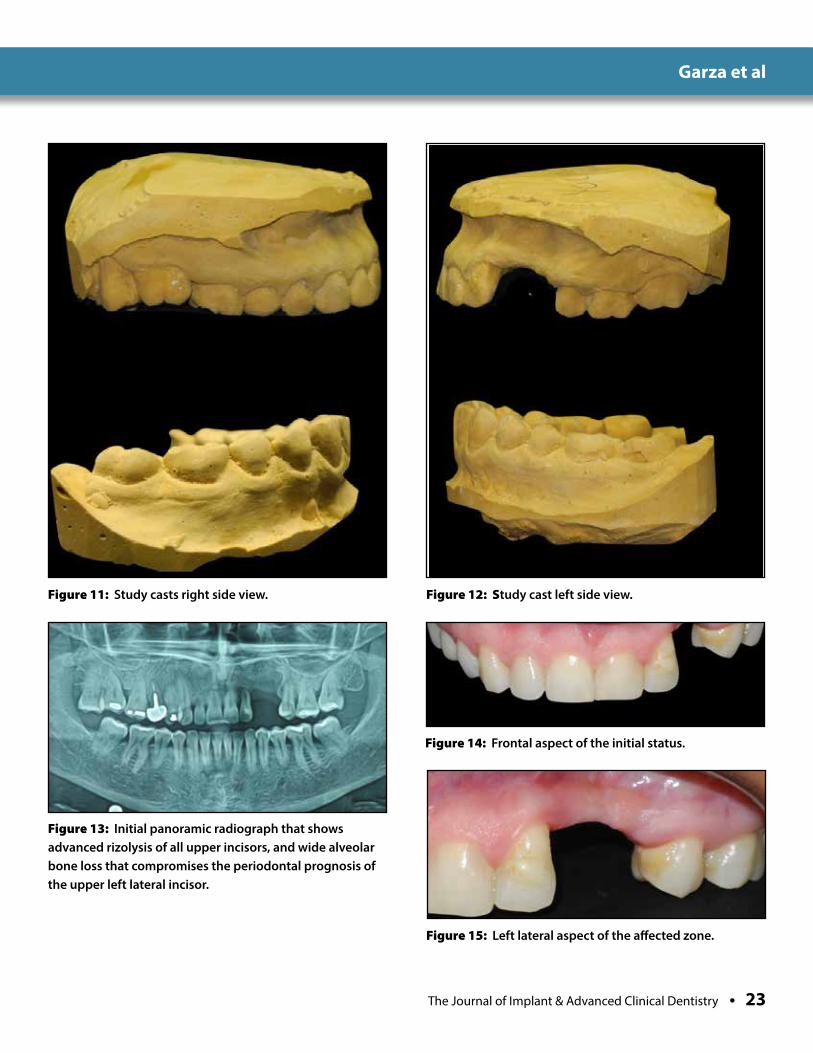
Figure 11: Study casts right side view. Figure 12: Study cast left side view.
Figure 13: Initial panoramic radiograph that shows advanced rizolysis of all upper incisors, and wide alveolar bone loss that compromises the periodontal prognosis of the upper left lateral incisor.
Figure 14: Frontal aspect of the initial status.
Figure 15: Left lateral aspect of the affected zone.

24 • Vol. 8, No. 1 • March 2016
Garza et al
Figure 16: Smile line draw in order to assess the correct position of the final oral rehabilitation.
Figure 17: Design and draw of the teeth number 11 and 12.
Figure 18: Shape, angulation and proportions of the virtual rehabilitation corrected.
Figure 19: Even with the correct position and proportions of the virtual rehabilitation we can appreciate an unaesthetic gap between the alveolar ridge and the crowns.
Figure 29: After the assessment of the edentulous zone in the aesthetic zone we decided to manufacture an implant retained dentogingival prothesis in order to provide the best outcome.
case, the patient had a low smile line and she expressed to us the desire of a fixed rehabili-tation with minimal surgical intervention. It’s imperative, for physicians and specialists, to get a good diagnosis and know the limitations of how much of the tissue can be restored by surgical intervention, and know when the tissue defects need to be compensated by a dento-gingival prosthesis. In an ideal case, the diag-nosis, planning and treatment is approached by a multidisciplinary team, i.e., the surgeon, prosthodontist, dental technician and other pro-fessionals that could be involved in the case.
Garza et al
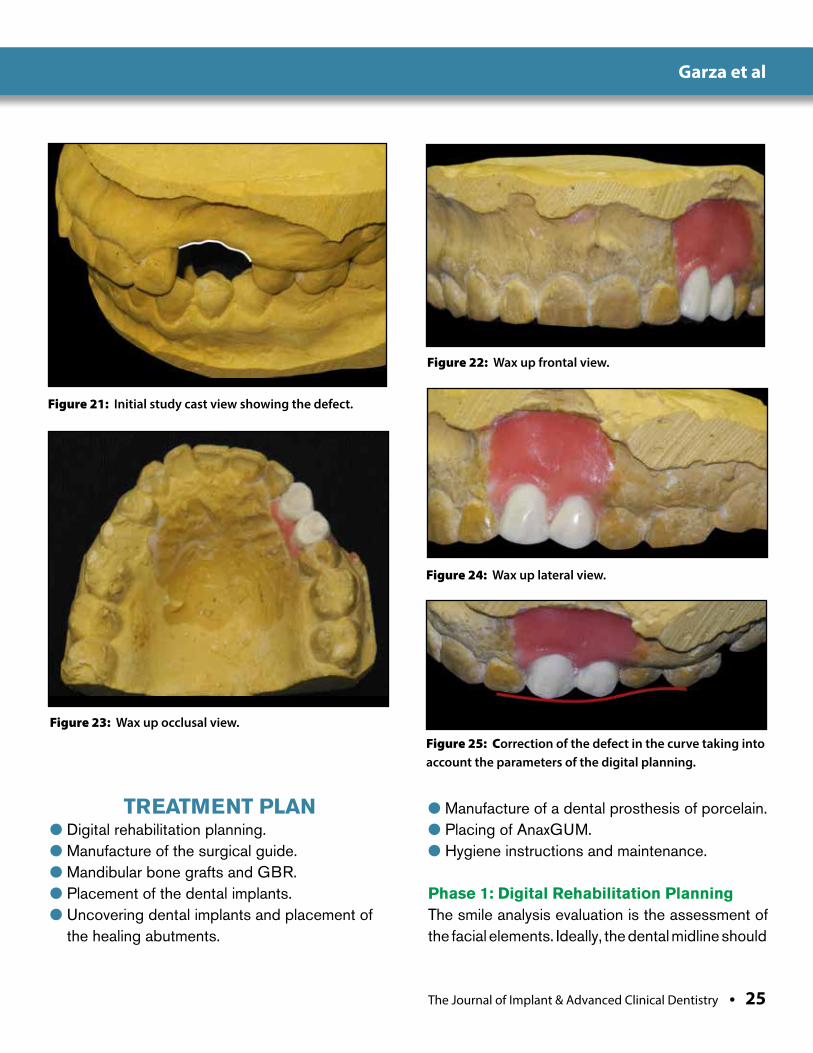
Figure 21: Initial study cast view showing the defect.
Figure 22: Wax up frontal view.
Figure 23: Wax up occlusal view.
Figure 24: Wax up lateral view.
Figure 25: Correction of the defect in the curve taking into account the parameters of the digital planning.
TREATMENT PLAN● Digital rehabilitation planning.● Manufacture of the surgical guide.● Mandibular bone grafts and GBR.● Placement of the dental implants.● Uncovering dental implants and placement of
the healing abutments.
● Manufacture of a dental prosthesis of porcelain.● Placing of AnaxGUM.● Hygiene instructions and maintenance.
Phase 1: Digital Rehabilitation Planning The smile analysis evaluation is the assessment of the facial elements. Ideally, the dental midline should
The Journal of Implant & Advanced Clinical Dentistry • 25

26 • Vol. 8, No. 1 • March 2016
Garza et al
Figure 26: Wax up duplicate occlusal view. This duplicate allow us to manufacture a surgical splint that will provide critical information (graft dimensions and optimal position, implant position and angulation, etc.).
Figure 27: Cast frontal view.
Figure 28: Cast right lateral view.
Figure 29: Cast left lateral view.
match the facial midline, but usually this doesn’t happen. Midline discrepancies of up to 4 mm will generally not be perceived as unaesthetic.
The evaluation of the relationship of the lips and the teeth, i.e., tooth display and lip posi-tion in smiling and speech. In this case, the patient shows a low smile and hypomotility of the upper lip.1 In the dentogingival analy-sis, the ratio of the tooth structure, gingival tis-sue and lips must be harmonized to prevent an over-dominance of any given element.1 The fourth and last step is the dental analysis, in which the intra-tooth and inter-tooth relation-ships are assessed. In the intra-tooth rela-tionship, the width and height of each tooth is evaluated, while the size and position of each tooth in the arcade is assessed in the inter-tooth relationship.1 During this system-
atic evaluation the digital rehabilitation exhibit deficiency of bone and soft tissue to create only a dental prothesis (Figures 14-20). This kind of approach gives us the opportunity to anticipate undesired outcomes and provide an extraordinary way of communication between the interdisciplinary team and patient as well.
The Journal of Implant & Advanced Clinical Dentistry • 27
Garza et al
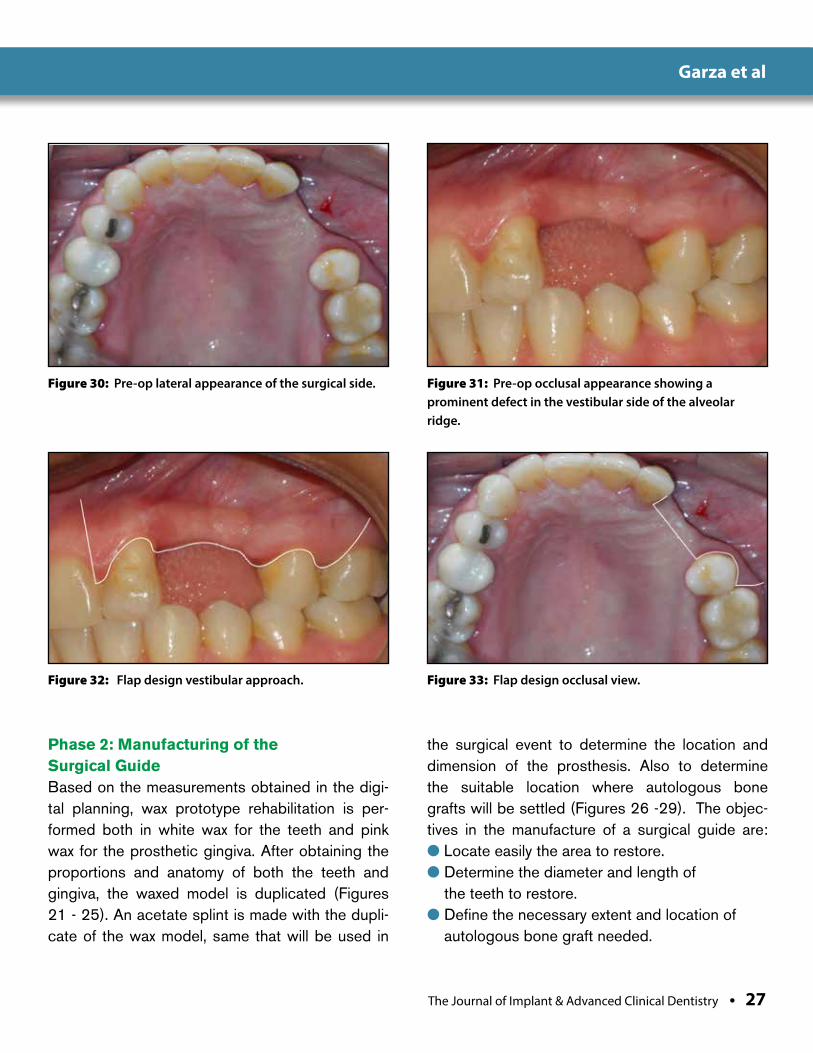
Figure 30: Pre-op lateral appearance of the surgical side. Figure 31: Pre-op occlusal appearance showing a prominent defect in the vestibular side of the alveolar ridge.
Figure 32: Flap design vestibular approach. Figure 33: Flap design occlusal view.
Phase 2: Manufacturing of the Surgical GuideBased on the measurements obtained in the digi-tal planning, wax prototype rehabilitation is per-formed both in white wax for the teeth and pink wax for the prosthetic gingiva. After obtaining the proportions and anatomy of both the teeth and gingiva, the waxed model is duplicated (Figures 21 - 25). An acetate splint is made with the dupli-cate of the wax model, same that will be used in
the surgical event to determine the location and dimension of the prosthesis. Also to determine the suitable location where autologous bone grafts will be settled (Figures 26 -29). The objec-tives in the manufacture of a surgical guide are:● Locate easily the area to restore.● Determine the diameter and length of
the teeth to restore.● Define the necessary extent and location of
autologous bone graft needed.

28 • Vol. 8, No. 1 • March 2016
Garza et al
Figure 34: Full thickness flap elevation. Figure 35: Alveolar bone defect.
Figure 36: Measurement of the donor area of the mandible.
● Establish the site in which the implants will be placed.
● Reduce surgical time.● Systematize the success and longevity of
the treatment.
Phase 3: Mandibular Bone Grafts and GBRAfter a tooth is extracted the alveolar ridge decreases in width and height very rapidly, with as much as 50% loss in width during the first year and two-thirds of which occurs in the initial 3 months.3,4 The use of the intraorally harvested bone blocks from the mandible for augmentation of edentulous ridges are frequently used, some of their advantages include:
● Increased in horizontal alveolar bone volume up to 7.5mm, compared to 4.5mm increase docu-mented with particulate GBR techniques.4, 6, 7
● Rapid reentry for implant placement, often in 3-4 months compared to the 6-9 months required for particulate GBR techniques.6, 7, 8, 9
● Excellent implant stability due to the cortical nature of the graft and optimal bone density.
● Reliable space maintenance during heal-ing ensures the shape and stability of the bone block is retained without collapse.4, 9
● Locally available donor sites avoid the need for extraoral autogenous bone sources, diminish-ing the possibility of contamination of the graft, patient discomfort, and diminishing recovery time.10
Although these events are considered rare, some of the possible complications and disad-vantages of harvesting bone blocks from the mandible include: mandibular fracture, lingual or inferior alveolar nerve neurosensory distur-bance, bleeding, infections and incision dehis-cence. The mandibular ramus buccal shelf block graft can provide adequate bone for aug-mentations involving a span of 2-3 teeth. Hori-
The Journal of Implant & Advanced Clinical Dentistry • 29
Garza et al
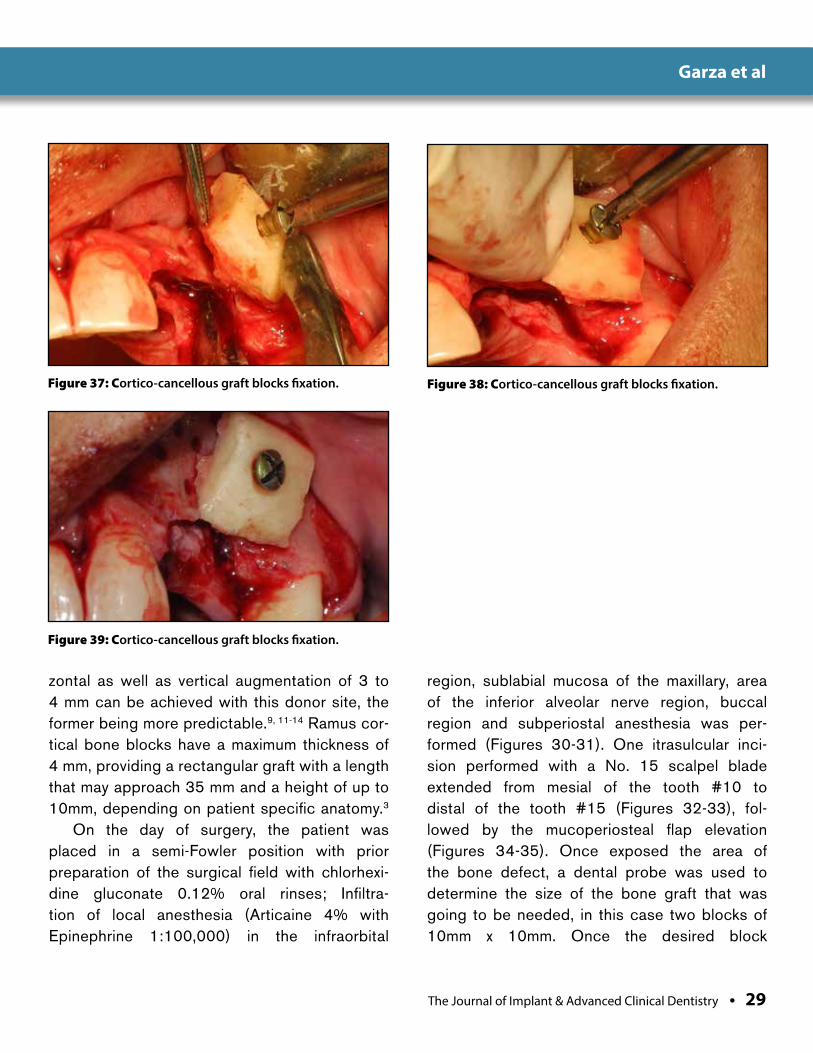
Figure 37: Cortico-cancellous graft blocks fixation. Figure 38: Cortico-cancellous graft blocks fixation.
Figure 39: Cortico-cancellous graft blocks fixation.
zontal as well as vertical augmentation of 3 to 4 mm can be achieved with this donor site, the former being more predictable.9, 11-14 Ramus cor-tical bone blocks have a maximum thickness of 4 mm, providing a rectangular graft with a length that may approach 35 mm and a height of up to 10mm, depending on patient specific anatomy.3
On the day of surgery, the patient was placed in a semi-Fowler position with prior preparation of the surgical field with chlorhexi-dine gluconate 0.12% oral rinses; Infiltra-tion of local anesthesia (Articaine 4% with Epinephrine 1:100,000) in the infraorbital
region, sublabial mucosa of the maxillary, area of the inferior alveolar nerve region, buccal region and subperiostal anesthesia was per-formed (Figures 30-31). One itrasulcular inci-sion performed with a No. 15 scalpel blade extended from mesial of the tooth #10 to distal of the tooth #15 (Figures 32-33), fol-lowed by the mucoperiosteal flap elevation (Figures 34-35). Once exposed the area of the bone defect, a dental probe was used to determine the size of the bone graft that was going to be needed, in this case two blocks of 10mm x 10mm. Once the desired block
30 • Vol. 8, No. 1 • March 2016
Garza et al
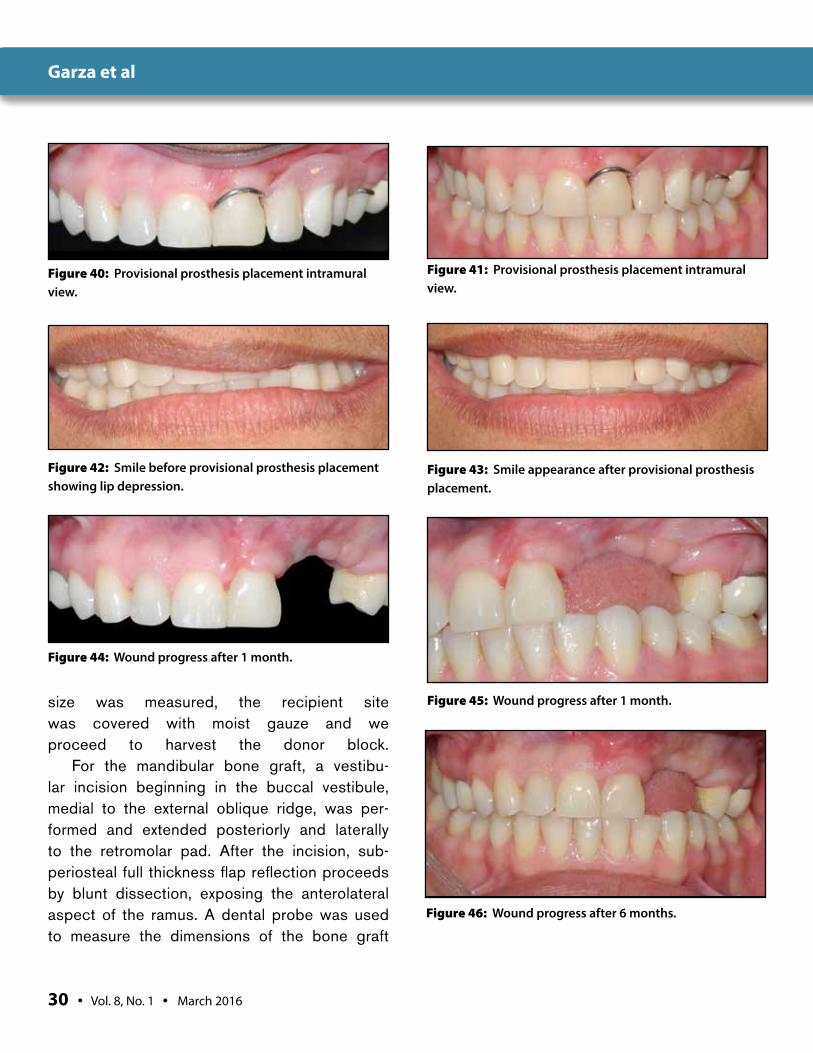
Figure 40: Provisional prosthesis placement intramural view.
Figure 42: Smile before provisional prosthesis placement showing lip depression.
Figure 43: Smile appearance after provisional prosthesis placement.
Figure 44: Wound progress after 1 month.
Figure 45: Wound progress after 1 month.
Figure 46: Wound progress after 6 months.
size was measured, the recipient site was covered with moist gauze and we proceed to harvest the donor block.
For the mandibular bone graft, a vestibu-lar incision beginning in the buccal vestibule, medial to the external oblique ridge, was per-formed and extended posteriorly and laterally to the retromolar pad. After the incision, sub-periosteal full thickness flap reflection proceeds by blunt dissection, exposing the anterolateral aspect of the ramus. A dental probe was used to measure the dimensions of the bone graft
Figure 41: Provisional prosthesis placement intramural view.
The Journal of Implant & Advanced Clinical Dentistry • 31
Garza et al
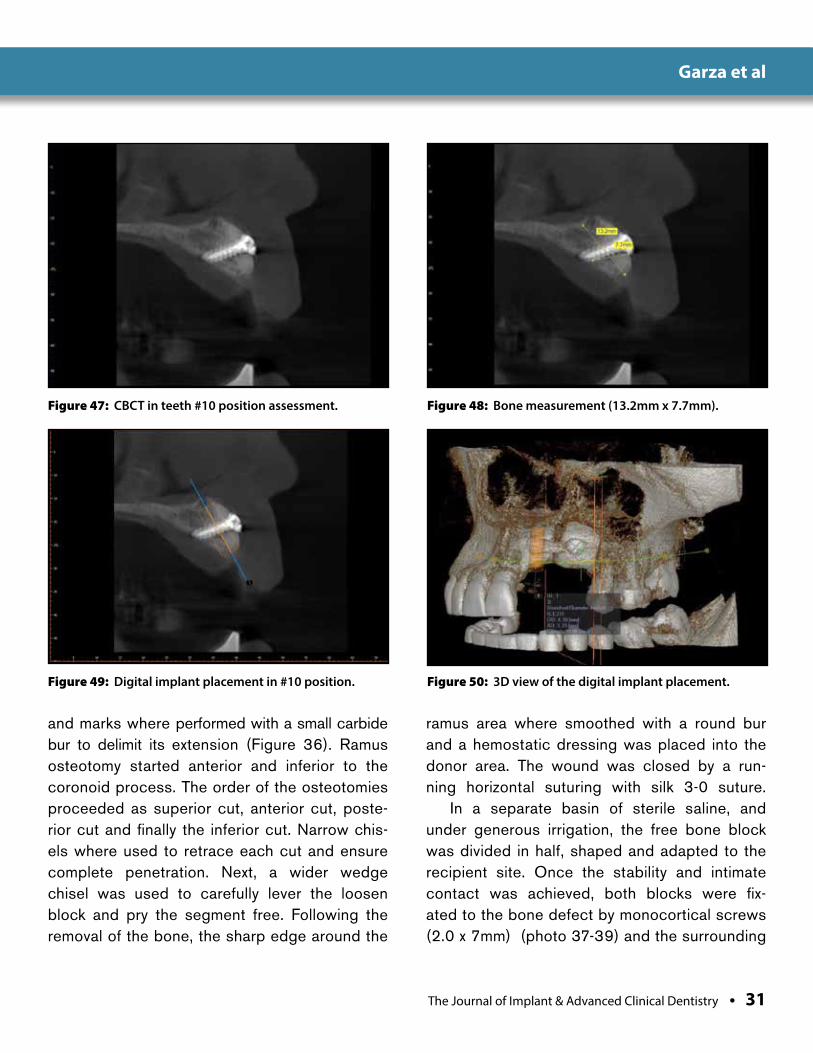
Figure 47: CBCT in teeth #10 position assessment. Figure 48: Bone measurement (13.2mm x 7.7mm).
Figure 49: Digital implant placement in #10 position. Figure 50: 3D view of the digital implant placement.
and marks where performed with a small carbide bur to delimit its extension (Figure 36). Ramus osteotomy started anterior and inferior to the coronoid process. The order of the osteotomies proceeded as superior cut, anterior cut, poste-rior cut and finally the inferior cut. Narrow chis-els where used to retrace each cut and ensure complete penetration. Next, a wider wedge chisel was used to carefully lever the loosen block and pry the segment free. Following the removal of the bone, the sharp edge around the
ramus area where smoothed with a round bur and a hemostatic dressing was placed into the donor area. The wound was closed by a run-ning horizontal suturing with silk 3-0 suture.
In a separate basin of sterile saline, and under generous irrigation, the free bone block was divided in half, shaped and adapted to the recipient site. Once the stability and intimate contact was achieved, both blocks were fix-ated to the bone defect by monocortical screws (2.0 x 7mm) (photo 37-39) and the surrounding
32 • Vol. 8, No. 1 • March 2016
Garza et al
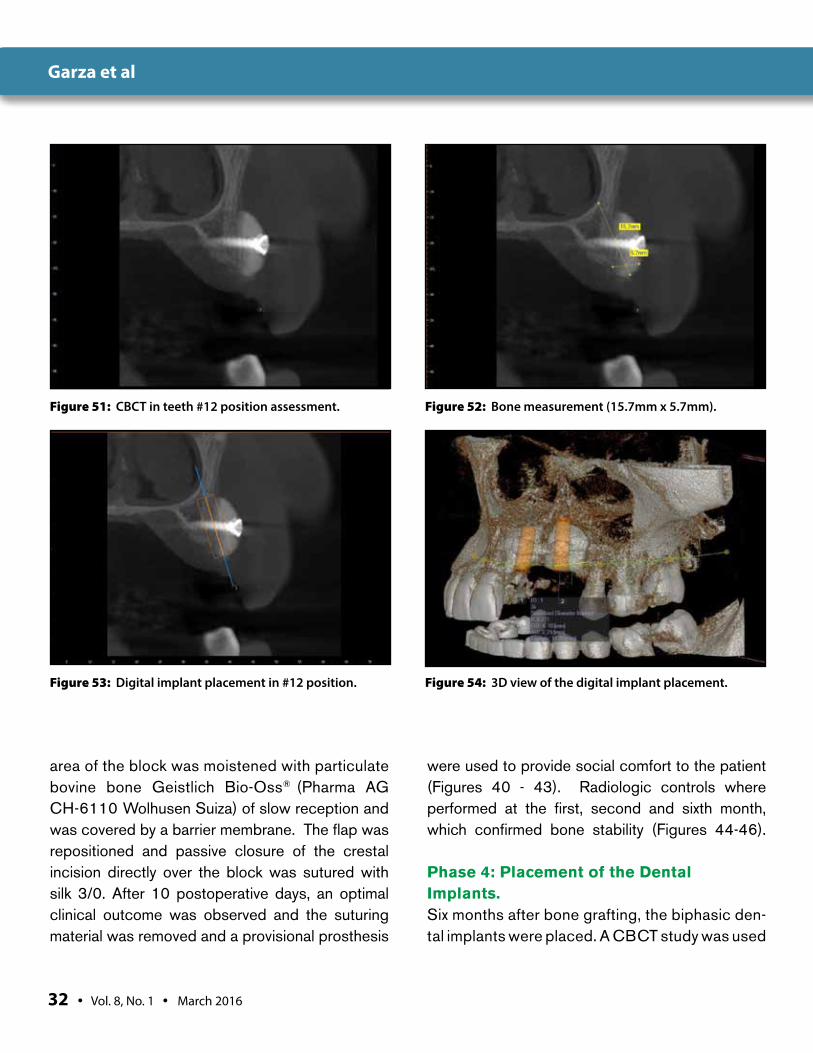
Figure 51: CBCT in teeth #12 position assessment. Figure 52: Bone measurement (15.7mm x 5.7mm).
Figure 53: Digital implant placement in #12 position. Figure 54: 3D view of the digital implant placement.
area of the block was moistened with particulate bovine bone Geistlich Bio-Oss® (Pharma AG CH-6110 Wolhusen Suiza) of slow reception and was covered by a barrier membrane. The flap was repositioned and passive closure of the crestal incision directly over the block was sutured with silk 3/0. After 10 postoperative days, an optimal clinical outcome was observed and the suturing material was removed and a provisional prosthesis
were used to provide social comfort to the patient (Figures 40 - 43). Radiologic controls where performed at the first, second and sixth month, which confirmed bone stability (Figures 44-46).
Phase 4: Placement of the Dental Implants.Six months after bone grafting, the biphasic den-tal implants were placed. A CBCT study was used
The Journal of Implant & Advanced Clinical Dentistry • 33
Garza et al
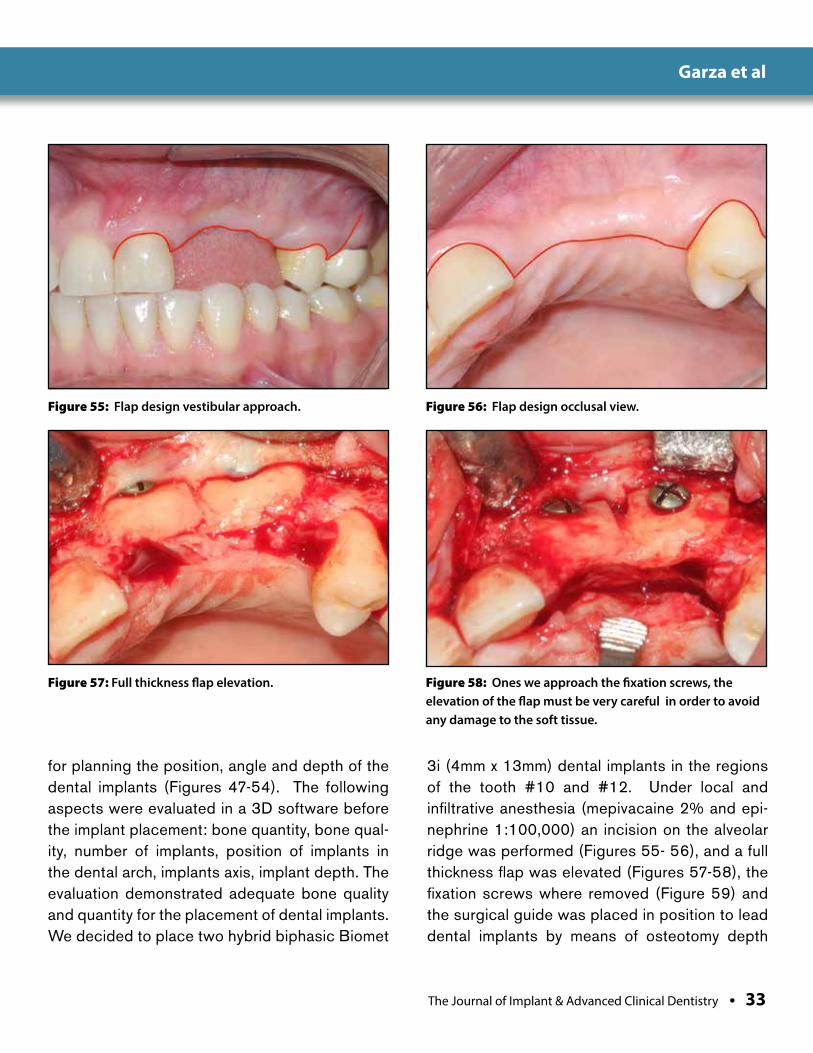
Figure 55: Flap design vestibular approach. Figure 56: Flap design occlusal view.
Figure 57: Full thickness flap elevation. Figure 58: Ones we approach the fixation screws, the elevation of the flap must be very careful in order to avoid any damage to the soft tissue.
for planning the position, angle and depth of the dental implants (Figures 47-54). The following aspects were evaluated in a 3D software before the implant placement: bone quantity, bone qual-ity, number of implants, position of implants in the dental arch, implants axis, implant depth. The evaluation demonstrated adequate bone quality and quantity for the placement of dental implants. We decided to place two hybrid biphasic Biomet
3i (4mm x 13mm) dental implants in the regions of the tooth #10 and #12. Under local and infiltrative anesthesia (mepivacaine 2% and epi-nephrine 1:100,000) an incision on the alveolar ridge was performed (Figures 55- 56), and a full thickness flap was elevated (Figures 57-58), the fixation screws where removed (Figure 59) and the surgical guide was placed in position to lead dental implants by means of osteotomy depth
34 • Vol. 8, No. 1 • March 2016
Garza et al
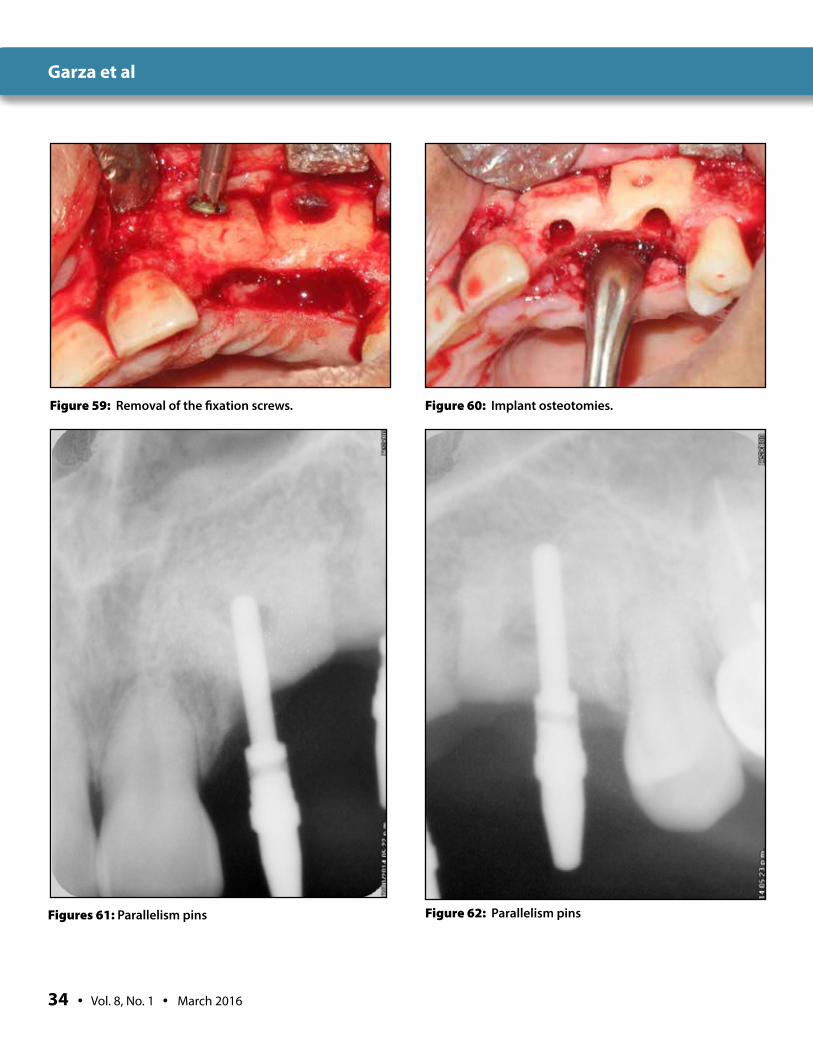
Figure 59: Removal of the fixation screws. Figure 60: Implant osteotomies.
Figures 61: Parallelism pins Figure 62: Parallelism pins

The Journal of Implant & Advanced Clinical Dentistry • 35
Garza et al
Figure 63: Clinical view of implants in position.
Figure 65: Radiographic assessment of implants position.
Figures 64: Clinical view of implants in position.
Figure 66: Radiographic assessment of implants position.
36 • Vol. 8, No. 1 • March 2016
Garza et al
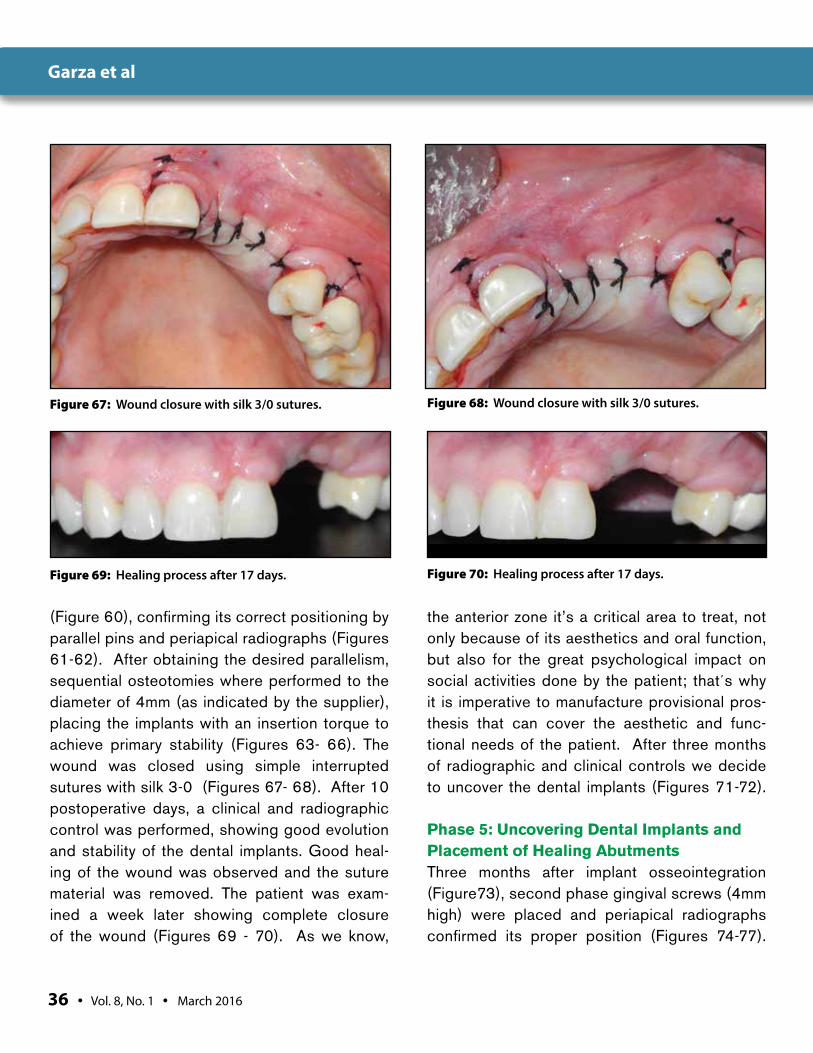
Figure 67: Wound closure with silk 3/0 sutures.
Figure 69: Healing process after 17 days.
(Figure 60), confirming its correct positioning by parallel pins and periapical radiographs (Figures 61-62). After obtaining the desired parallelism, sequential osteotomies where performed to the diameter of 4mm (as indicated by the supplier), placing the implants with an insertion torque to achieve primary stability (Figures 63- 66). The wound was closed using simple interrupted sutures with silk 3-0 (Figures 67- 68). After 10 postoperative days, a clinical and radiographic control was performed, showing good evolution and stability of the dental implants. Good heal-ing of the wound was observed and the suture material was removed. The patient was exam-ined a week later showing complete closure of the wound (Figures 69 - 70). As we know,
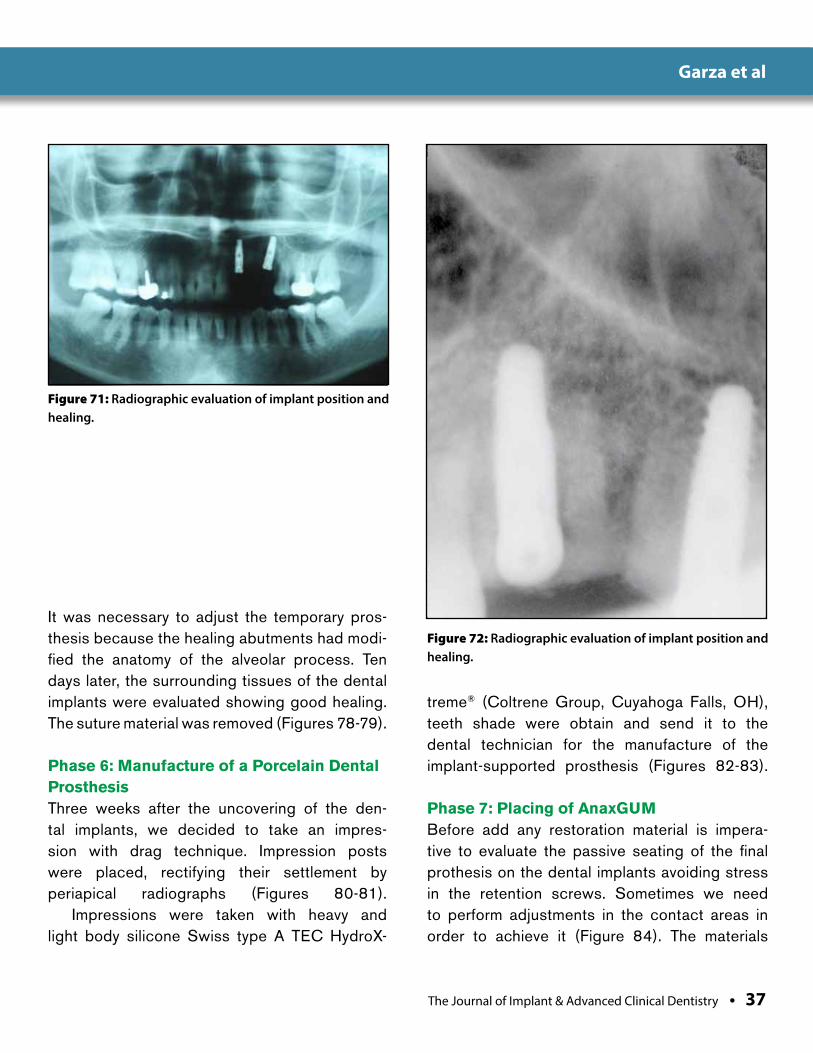
the anterior zone it’s a critical area to treat, not only because of its aesthetics and oral function, but also for the great psychological impact on social activities done by the patient; that´s why it is imperative to manufacture provisional pros-thesis that can cover the aesthetic and func-tional needs of the patient. After three months of radiographic and clinical controls we decide to uncover the dental implants (Figures 71-72).
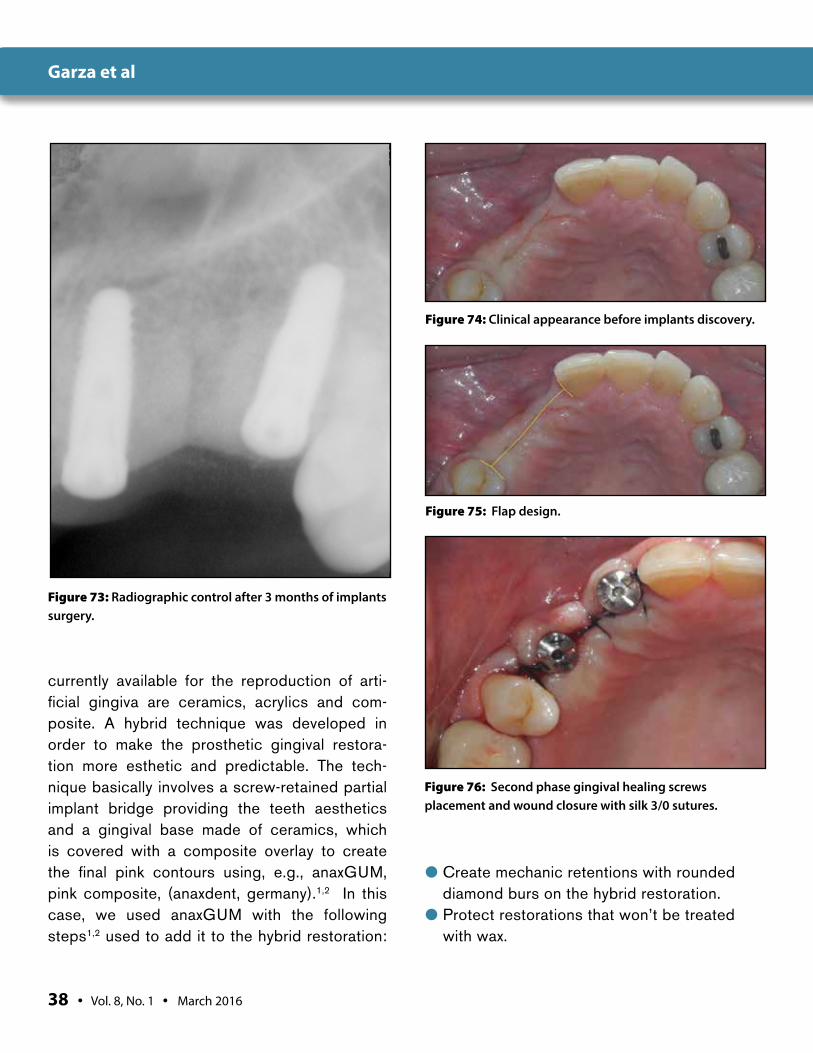
Phase 5: Uncovering Dental Implants and Placement of Healing AbutmentsThree months after implant osseointegration (Figure73), second phase gingival screws (4mm high) were placed and periapical radiographs confirmed its proper position (Figures 74-77).
Figure 68: Wound closure with silk 3/0 sutures.
Figure 70: Healing process after 17 days.
The Journal of Implant & Advanced Clinical Dentistry • 37
Garza et al
Figure 71: Radiographic evaluation of implant position and healing.
Figure 72: Radiographic evaluation of implant position and healing.
It was necessary to adjust the temporary pros-thesis because the healing abutments had modi-fied the anatomy of the alveolar process. Ten days later, the surrounding tissues of the dental implants were evaluated showing good healing. The suture material was removed (Figures 78-79).
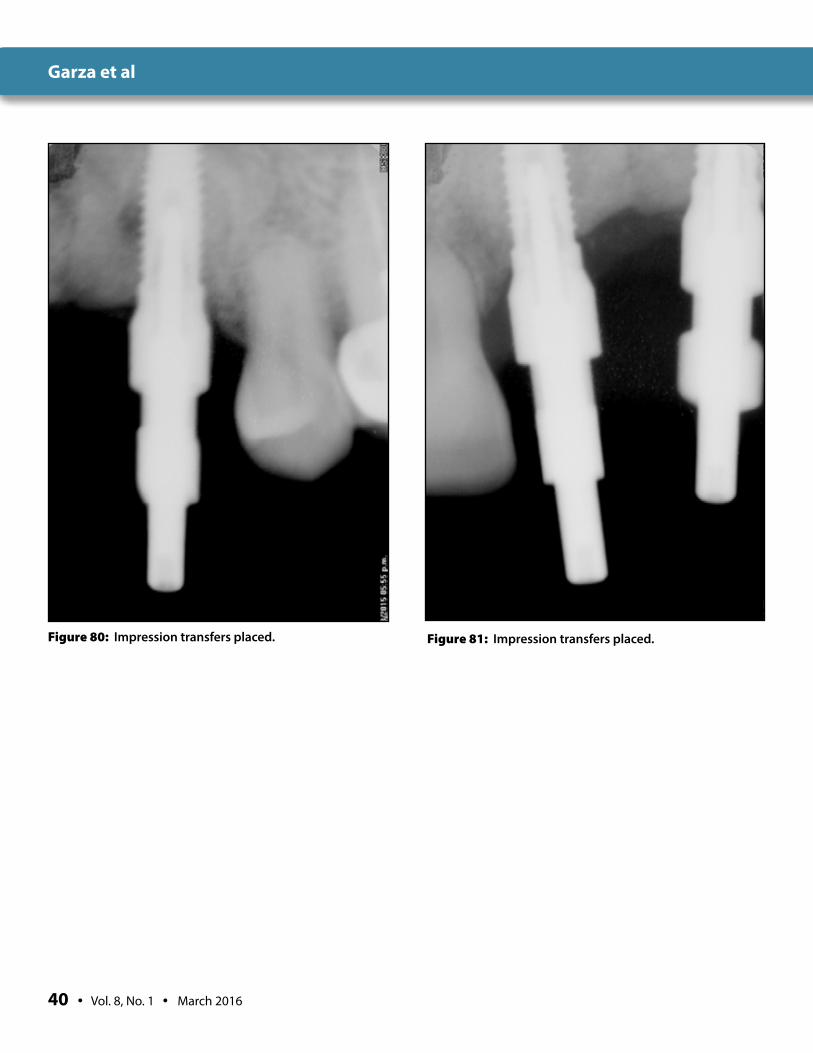
Phase 6: Manufacture of a Porcelain Dental Prosthesis Three weeks after the uncovering of the den-tal implants, we decided to take an impres-sion with drag technique. Impression posts were placed, rectifying their settlement by periapical radiographs (Figures 80-81).
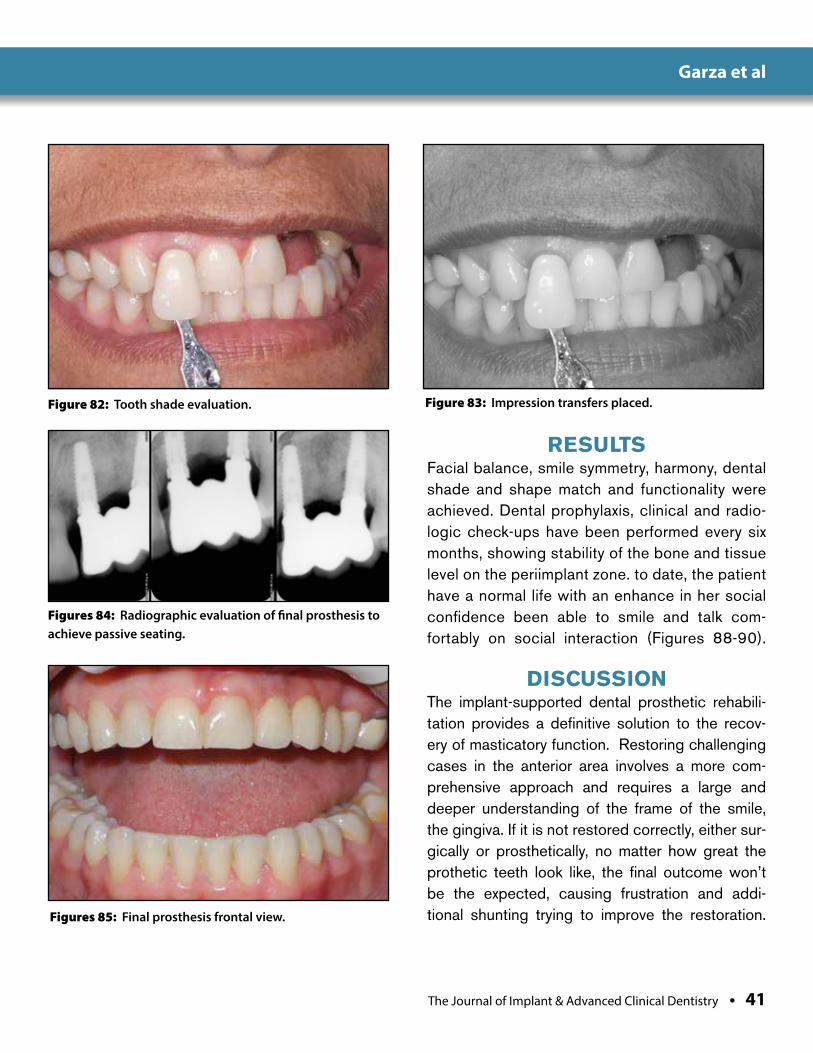
Impressions were taken with heavy and light body silicone Swiss type A TEC HydroX-
treme® (Coltrene Group, Cuyahoga Falls, OH), teeth shade were obtain and send it to the dental technician for the manufacture of the implant-supported prosthesis (Figures 82-83).
Phase 7: Placing of AnaxGUMBefore add any restoration material is impera-tive to evaluate the passive seating of the final prothesis on the dental implants avoiding stress in the retention screws. Sometimes we need to perform adjustments in the contact areas in order to achieve it (Figure 84). The materials
38 • Vol. 8, No. 1 • March 2016
Garza et al
Figure 73: Radiographic control after 3 months of implants surgery.
Figure 74: Clinical appearance before implants discovery.
Figure 75: Flap design.
Figure 76: Second phase gingival healing screws placement and wound closure with silk 3/0 sutures.
currently available for the reproduction of arti-ficial gingiva are ceramics, acrylics and com-posite. A hybrid technique was developed in order to make the prosthetic gingival restora-tion more esthetic and predictable. The tech-nique basically involves a screw-retained partial implant bridge providing the teeth aesthetics and a gingival base made of ceramics, which is covered with a composite overlay to create the final pink contours using, e.g., anaxGUM, pink composite, (anaxdent, germany).1,2 In this case, we used anaxGUM with the following steps1,2 used to add it to the hybrid restoration:
● Create mechanic retentions with rounded diamond burs on the hybrid restoration.
● Protect restorations that won’t be treated with wax.

The Journal of Implant & Advanced Clinical Dentistry • 39
Garza et al
Figure 77: Radiographic evaluation of second phase gingival healing screws.
Figure 78: Clinical control after four weeks.
Figure 79: Clinical control after four weeks.
● Aluminum oxide sandblasting on the surface of the hybrid restoration.
● Etch of the hybrid restoration with hydro-fluoric acid 10% for 90 seconds.
● Silane activation.● Flowable composite application.● Gingival shape and shade analysis● Direct application of composite with different
shades in order to create the most natural outcome.
● Light curing.After all adjustments are made and final
polishing is accomplished, the restora-tion is ready to be settled (Figures 85-87).
Phase 8: Hygiene Instructions and MaintenanceIt is vital to reinforce, step by step, the impor-tance of hygiene maintenance to the patient and schedule a check-up appointment in 1 month. Maintenance is crucial for the long-term success of such restorations. Implant-supported restora-tions are designed to enable patients to perform excellent maintenance; it is strongly recom-mended to have check-up appointments periodi-cally to unscrew the denture and verify the health of the tissues involved. Furthermore, this also enables the practitioner to repair, polish, reshape, or add to the artificial gingiva if necessary.1,2,15,
40 • Vol. 8, No. 1 • March 2016
Garza et al
Figure 80: Impression transfers placed. Figure 81: Impression transfers placed.
The Journal of Implant & Advanced Clinical Dentistry • 41
Garza et al
Figure 82: Tooth shade evaluation.
Figures 84: Radiographic evaluation of final prosthesis to achieve passive seating.
Figures 85: Final prosthesis frontal view.
RESULTSFacial balance, smile symmetry, harmony, dental shade and shape match and functionality were achieved. Dental prophylaxis, clinical and radio-logic check-ups have been performed every six months, showing stability of the bone and tissue level on the periimplant zone. to date, the patient have a normal life with an enhance in her social confidence been able to smile and talk com-fortably on social interaction (Figures 88-90).
DISCUSSIONThe implant-supported dental prosthetic rehabili-tation provides a definitive solution to the recov-ery of masticatory function. Restoring challenging cases in the anterior area involves a more com-prehensive approach and requires a large and deeper understanding of the frame of the smile, the gingiva. If it is not restored correctly, either sur-gically or prosthetically, no matter how great the prothetic teeth look like, the final outcome won’t be the expected, causing frustration and addi-tional shunting trying to improve the restoration.
Figure 83: Impression transfers placed.

42 • Vol. 8, No. 1 • March 2016
Garza et al
Figure 86: Final prosthesis lateral view. Figure 87: Smile analysis with the final restoration.
Figure 88: Final radiograph.
CONCLUSIONSSurgical techniques in order to restore and regenerate the lack of tissues by any pathology have been developed and enhanced through the years, achieving amazing results, however it is important for the clinician to understand that sometimes to achieve the desired the surgical cosmetic results its necessary that the patient undergo several surgical procedures with implies a longest treatment time, as well, a higher treat-ment cost. Creating a prosthetic gingiva can represent an aesthetic and functional alternative for the predictable reconstruction of ridge defor-mities in fixed partial implant restorations, partic-
ularly in patients who do not want to undergo any surgical procedure. The key facts have in mind to success in any treatment are, always have in mind the concern and desires of the patient, full understanding and analysis of the case, a care-ful planning by the multidisciplinary team and always communicate to the patient what treat-ment options they have and what they consist as well the expectations of the final result. ●
Correspondence:Dr. Luis Roberto Sanchez Garza,Gómez Morín 2003 L-9, Col. Carrizalejo, San Pedro Garza García, Zip Code: 66254, Phone: 044-818-280-8992, Office: 83461176 email: [email protected].

The Journal of Implant & Advanced Clinical Dentistry • 43
Garza et al
Figure 89: Initial smile photograph. Figure 90: Final smile photograph.
DisclosureThe authors report no conflicts of interest with anything mentioned in this article.
References1. Prosthetic Gingival Reconstruction in the Fixed Partial Restoration. Part 2: Diag-
nosis and Treatment Planning Christian Coachman, DDS, CDT, Maurice Salama, DMD ,David Garber, DMD ,Marcelo Calamita, DDS ,Henry Salama, DMD ,Guilherme Cabral, DDS, CDT, The International Journal of Peri-odontics & Restorative Dentistry, Volume 29, Number 6, 2009.
2. Minimally Invasive Reconstruction in Implant Therapy: The Pros-thetic Gingival Restoration. Christian Coachman, CCD, CDT, Eric Van Dooren, DDS, Galip Gurel, DDS, MS, Marcelo A. Calamita, DDS, MSc, PhD, Murilo Calgaro, CDT4 ,Juvenal de Souza Neto, CDT.
3. KoisJC.Predictablesingletoothperi-implantesthetics:fivediagnostickeys. Compend Contin Educ Dent 2001;22(3):199–206.
4. The Art of Block Grafting, A review of the Surgical protocol for Reconstruction of Alveolar Ridge Deficiency: Nicholas Toscano, DDS MS1 • Nicholas Shumaker, DDS MS2 Dan Holtzclaw, DDS MS3, JIACID Vol.2, No.2, March 2010 pg. 45-66.
5. Schropp L, et al. Bone healing and soft tissue contour changes follow-ing single-tooth extraction: a clinical and radiographic 12-month prospec-tive study. Int J Periodontics Restorative Dent. 2003 Aug;23(4):313-23.
6. Feuille F, Knapp CI, Brunsvold MA, Mellonig. Clinical and histo-logic evaluation of bone-replacement grafts in the treatment of local-ized alveolar ridge defects. Part 1: Mineralized freeze-dried bone allograft. Int J Periodontics Restorative Dent 2003;23(1):29-35.
7. Buser DA, Bragger U, Lang N, Nyman S. Regeneration and enlargement of jaw bone using guided tissue regenera-tion. Clin Oral Implants Res. 1990 Dec;1(1):22-32.
8. Pikos MA. Mandibular block autografts for alveolar ridge augmenta-tion. Atlas Oral Maxillofacial Surg Clin N Am. 2005; (13):91- 107.
9. Pikos MA. Block autografts for localized ridge augmentation: Part II. The posterior mandible. Implant Dent. 2000;9(1):67-75.
10. Linklow LI. Bone transplants using the symphysis, the iliac crest, and synthetic bone materials. J Oral Implantol. 1983;11:211-247.
11. Pikos MA. Facilitating implant placement with chin grafts as donor sites for max-illary bone augmentation--Part I. Dent Implantol Update. 1995 Dec;6(12):89-92.
12. Pikos MA. Facilitating implant placement with chin grafts as donor sites for maxillary bone augmentation-Part II. Dent Implantol 1996.
13. Pikos MA. Block autografts for localized ridge augmentation; Part I. The posterior maxilla. Implant Dent 1999; 8:279-284.
14. Prosthetic Gingival Reconstruction in Fixed Partial Restorations. Part 3: Laboratory Procedures and Maintenance,Christian Coachman, DDS, CDT, Maurice Salama, DMD, David Garber, DMD,Marcelo Calamita, DDS,Henry Salama, DMD,Guilherme Cabral, DDS, CDT, The International Journal of Periodontics & Restorative Dentistry,Volume 30, Number 1, 2010.
Falcón
Built-in platform shiftingDual-function prosthetic connection
Bone-condensing property
Adjustable implant orientation for optimal final placement
High initial stability, even in compromised
bone situations
NobelActive™
A new direction for implants.
Nobel Biocare USA, LLC. 22715 Savi Ranch Parkway, Yorba Linda, CA 92887; Phone 714 282 4800; Toll free 800 993 8100; Tech. services 888 725 7100; Fax 714 282 9023Nobel Biocare Canada, Inc. 9133 Leslie Street, Unit 100, Richmond Hill, ON L4B 4N1; Phone 905 762 3500; Toll free 800 939 9394; Fax 800 900 4243Disclaimer: Some products may not be regulatory cleared/released for sale in all markets. Please contact the local Nobel Biocare sales office for current product assortment and availability. Nobel Biocare, the Nobel Biocare logotype and all other trademarks are, if nothing else is stated or is evident from the context in a certain case, trademarks of Nobel Biocare.
NobelActive equally satisfies surgical and restorative clinical goals. NobelActive thread design progressively condenses bone with each turn during insertion, which is designed to enhance initial stability. The sharp apex and cutting blades allow surgical clinicians to adjust implant orientation for optimal positioning of the prosthetic
connection. Restorative clinicians benefit by a versatile and secure internal conical prosthetic connec-tion with built-in platform shifting upon which they can produce excellent esthetic results. Based on customer feedback and market demands for NobelActive, theproduct assortment has been expanded – dental professionals will
now enjoy even greater flexi bility in prosthetic and implant selection. Nobel Biocare is the world leader in innovative evidence-based dental solutions. For more information, con-tact a Nobel Biocare Representative at 800 322 5001 or visit our website.
www.nobelbiocare.com/nobelactive
© N
ob
el B
ioca
re S
ervi
ces
AG
, 2
01
1.
All
rig
hts
res
erve
d.
TIUNITE® SURFACE,
10-YEAR EXPERIENCE
New data confi rm
long-term stability.
NOW AVAILABLE
WITH NOBELGUIDE™
64_NA2010_8125x10875.indd 1 8/1/11 1:37:30 PM

Falcón
Background: The goal of this article to is present and evaluate the clinical effective-ness of a new surgical approach using a coronally advanced flap performed during second stage implant surgery for the recon-struction of peri implant papillae and treat-ment of gingival recession of adjacent teeth.
Methods: Patients requiring the second stage surgery for uncovering dental implants and presenting with concurrent gingival reces-sion (Miller I or II) in the adjacent teeth. A coronally advanced flap secured with a sus-pensory suture was utilized for the procedure.
Results: Six months after the second stage implant surgery, the reconstruction of the peri implant papillae and treatment of gin-gival recessions were evaluated. Resulted were of a stable and predictable form.
Conclusions: This preliminary study pres-ents a new surgical approach (technical tin-kiy), which can be used in the second surgical phase of dental implants. The results show that the alternative operative time is reduced since only one surgery is performed, obtain-ing stable and predictable papillae and root coverage with minimal postoperative dis-comfort and improving the aesthetic result.
Effectiveness of a New Surgical Approach: “Tinkiy,” for Reconstruction of Peri Implant Papilla and the
Treatment of Gingival Recession
Dr. Britto Falcón1
1. Magister in Odonto-Stomatology, Specialist in periodontics and Implantology, Coordinator APPO
(Asociación Peruana de Periodoncia y Oseointegración)-Tacna, Private Practice. Tacna- Perú.
Abstract
KEY WORDS: Dental implants, dental papilla, esthetics, coronally advanced flap, gingival recession
The Journal of Implant & Advanced Clinical Dentistry • 45
46 • Vol. 8, No. 1 • March 2016
INTRODUCTIONThe common esthetic factor in single tooth implant-supported restorations is the soft-tis-sue profile, which ideally should be identical to that of the natural tooth. Soft tissue man-agement has become an important topic in implant dentistry and gingival esthetics has become a critical factor in the overall success of an implant-supported restoration.1 Lack of papilla can lead to cosmetic deformities, pho-netic difficulty, and food impaction, especially during smiling or the speaking and the clini-cal dilemma is that the interdental papilla is invariably deficient in height when compared to the contralateral natural tooth, causing an unsightly space known as black hole disease.2-4
A tissue-punch or full thickness flap reflec-tion before abutment connection have been the traditional soft tissue techniques used at sec-ond stage uncovery surgery.5,6 Limited atten-tion was focused on increasing the height of the soft tissue in the interimplant region. Several approaches have been proposed to reconstruct inter-implant papillae with vari-ous surgical techniques and shown encour-aging, but often unpredictable results.4,5 In
surgical management the flap designs with papilla-sparing incisions protect the under-lying bone and in turn the interproximal papilla against the post-operative recession.7
With the years the reconstruction manage-ment deficient papilla has cast with the tradi-tional methods using the connective tissue graft increasing the tissue height in the edentulous site of traditional prostheses or alternatives as allograft material.3,5,8 Palacci6 reported a novel papilla regeneration technique in the time of the second-stage implant surgery with a semi-lunar beveled incision in relation to the elevated flap in relation to each implant to create a ped-icle that is rotated at 90 degrees to the mesial aspect of the abutment and stabilized with the interrupted mattress suture to form new interim-plant papilla. Grossberg2 used a modifica-tion of the flap technique described by Palacci with a horizontal incision creating a double-pedicle flap; Nemcosky1 performed U-shaped incision with divergent arms open toward the buccal aspect surrounding the implant site in the palatal aspect. The flap is split in the center through its whole thickness, separating it into mesial and distal parts. Each part of the buc-
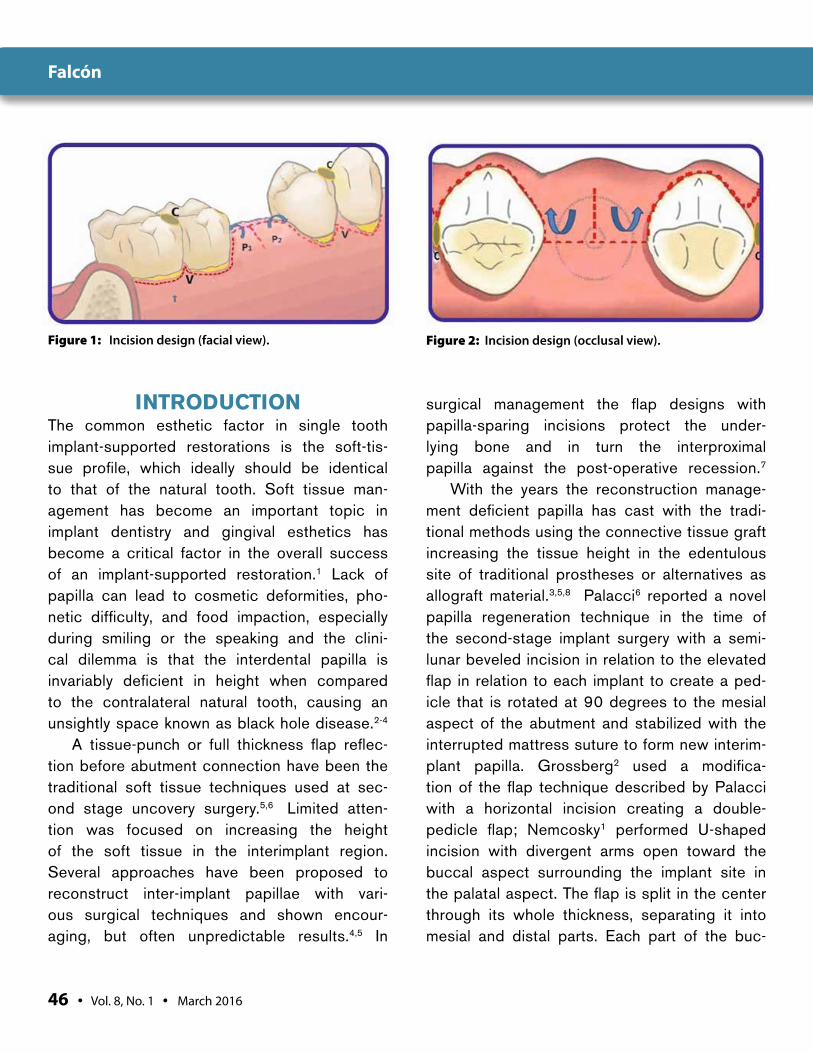
Figure 1: Incision design (facial view). Figure 2: Incision design (occlusal view).
Falcón

The Journal of Implant & Advanced Clinical Dentistry • 47
cal flap is positioned over deepithelized papil-lae and sutured to the palate mucosa. Azzi et al.5 released a buccal flap beyond the muco-gingival line; the papillae are undermined from their insertion to the bone and connective tis-sue graft is inserted in the pouch-like tunnel and completely submerged beneath the buccal flap and papillae8 and Misch et al. used the “split finger technique” to promote papilla formation.
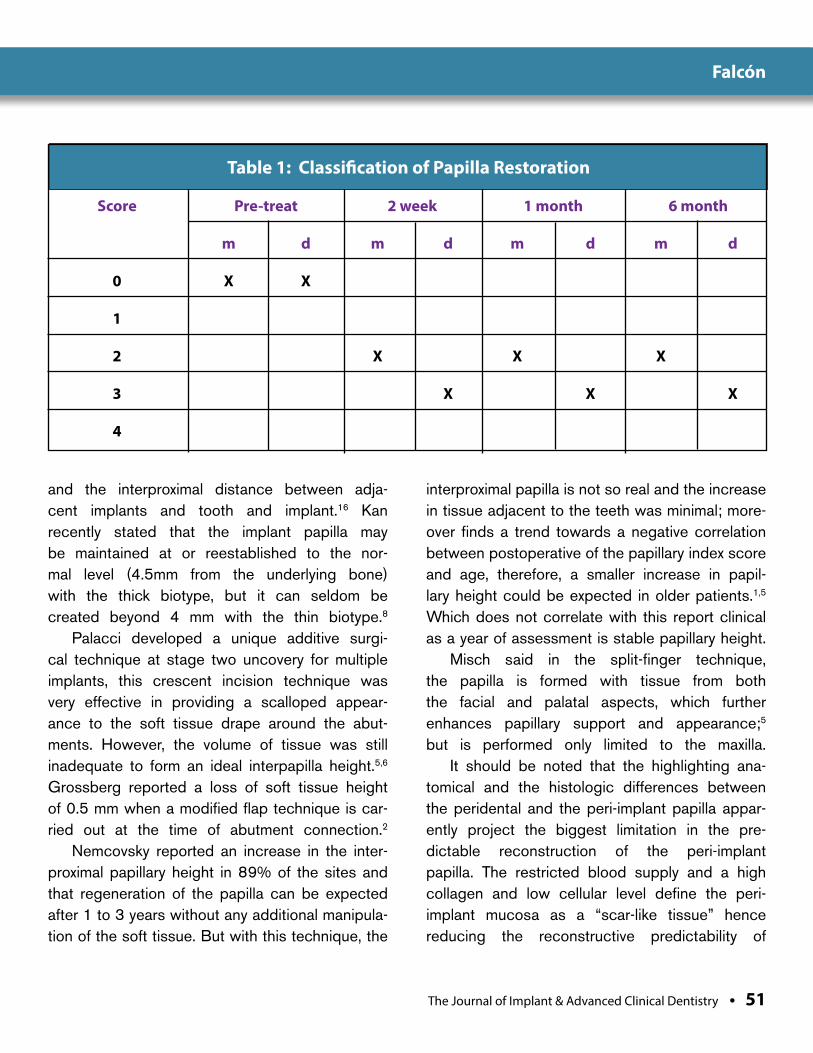
Jemt in 1997,9 proposed a classifica-tion of papilla restoration as score 0, no papilla is present; score 1, less than half of the papilla is present; score 2, at least half of the papilla is present, but not all the way up to the contact point between the teeth; score 3, the papilla fills up the entire proxi-mal space and is in good harmony with the adjacent papillae; score 4, the papilla is hyper-plasic and covers too much of the single-implant restoration and/or the adjacent tooth.
An important factor for the management of both the recession and the reconstruc-tion of peri-implant papillae is the periodon-tal biotype, thick or thin, affects the dimension of the periodontal tissue. A thick biotype is prone to pocket formation, whereas a thin
biotype is prone to gingival recession fol-lowing mechanical or surgical manipulation.8
With respect to the treatment of reces-sion type defects, Zucchelli reported in many studies that the reposition coronally flap pres-ent better result because of the amplied blood supply provided by the base of the flap ; in the treatment of multiple recession defects for root coverage (miller class I or II) with new surgi-cal approach to the coronally advanced flap procedure,10-14 but should try to identify critical elements in design and execution of coronally advanced flap influencing in the flap design and execution: the dimension and the thickness of tissue positioned over the denuded roots; the stability and suturing of the flap in a posi-tion coronal to the cement-enamel junction.15
The aim of this report is to present a new technique approach for papillae reconstruction and the treatment of gingival recession, surgi-cal performed in the second stage of an single or multiple dental implants where by coronally advanced flap, gets done both treatments.
Figure 3: Goals of incision design (facial view). Figure 4: Pre-operative view of implant requiring stage 2 surgery with concurrent teeth having gingival recession.
Falcón
48 • Vol. 8, No. 1 • March 2016
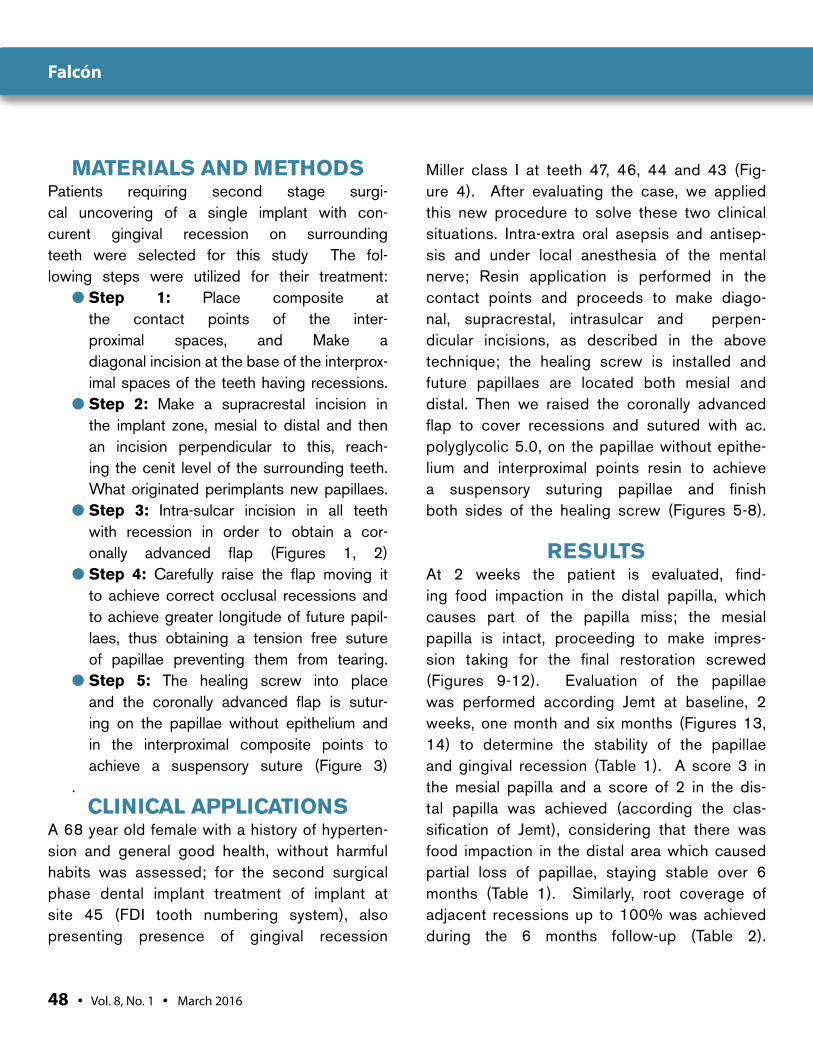
MATERIALS AND METHODSPatients requiring second stage surgi-cal uncovering of a single implant with con-curent gingival recession on surrounding teeth were selected for this study The fol-lowing steps were utilized for their treatment:
● Step 1: Place composite at the contact points of the inter-proximal spaces, and Make a diagonal incision at the base of the interprox-imal spaces of the teeth having recessions.
● Step 2: Make a supracrestal incision in the implant zone, mesial to distal and then an incision perpendicular to this, reach-ing the cenit level of the surrounding teeth. What originated perimplants new papillaes.
● Step 3: Intra-sulcar incision in all teeth with recession in order to obtain a cor-onally advanced flap (Figures 1, 2)
● Step 4: Carefully raise the flap moving it to achieve correct occlusal recessions and to achieve greater longitude of future papil-laes, thus obtaining a tension free suture of papillae preventing them from tearing.
● Step 5: The healing screw into place and the coronally advanced flap is sutur-ing on the papillae without epithelium and in the interproximal composite points to achieve a suspensory suture (Figure 3)
. CLINICAL APPLICATIONS
A 68 year old female with a history of hyperten-sion and general good health, without harmful habits was assessed; for the second surgical phase dental implant treatment of implant at site 45 (FDI tooth numbering system), also presenting presence of gingival recession
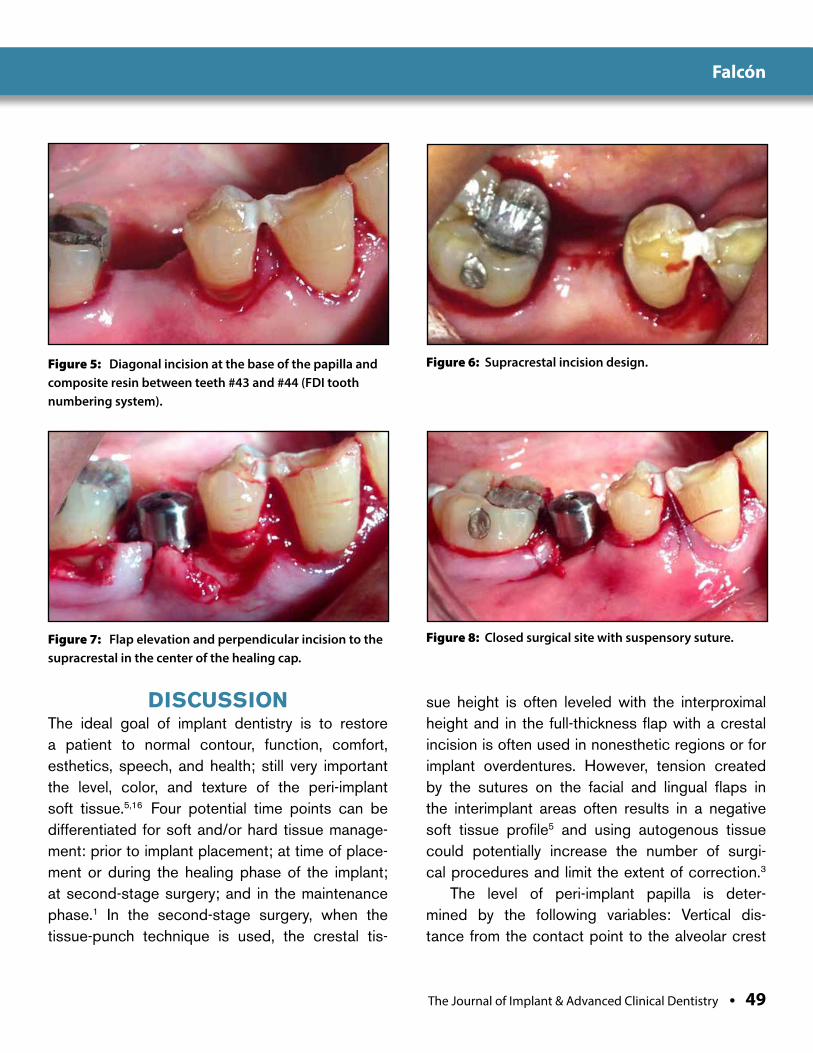
Miller class I at teeth 47, 46, 44 and 43 (Fig-ure 4). After evaluating the case, we applied this new procedure to solve these two clinical situations. Intra-extra oral asepsis and antisep-sis and under local anesthesia of the mental nerve; Resin application is performed in the contact points and proceeds to make diago-nal, supracrestal, intrasulcar and perpen-dicular incisions, as described in the above technique; the healing screw is installed and future papillaes are located both mesial and distal. Then we raised the coronally advanced flap to cover recessions and sutured with ac. polyglycolic 5.0, on the papillae without epithe-lium and interproximal points resin to achieve a suspensory suturing papillae and finish both sides of the healing screw (Figures 5-8).
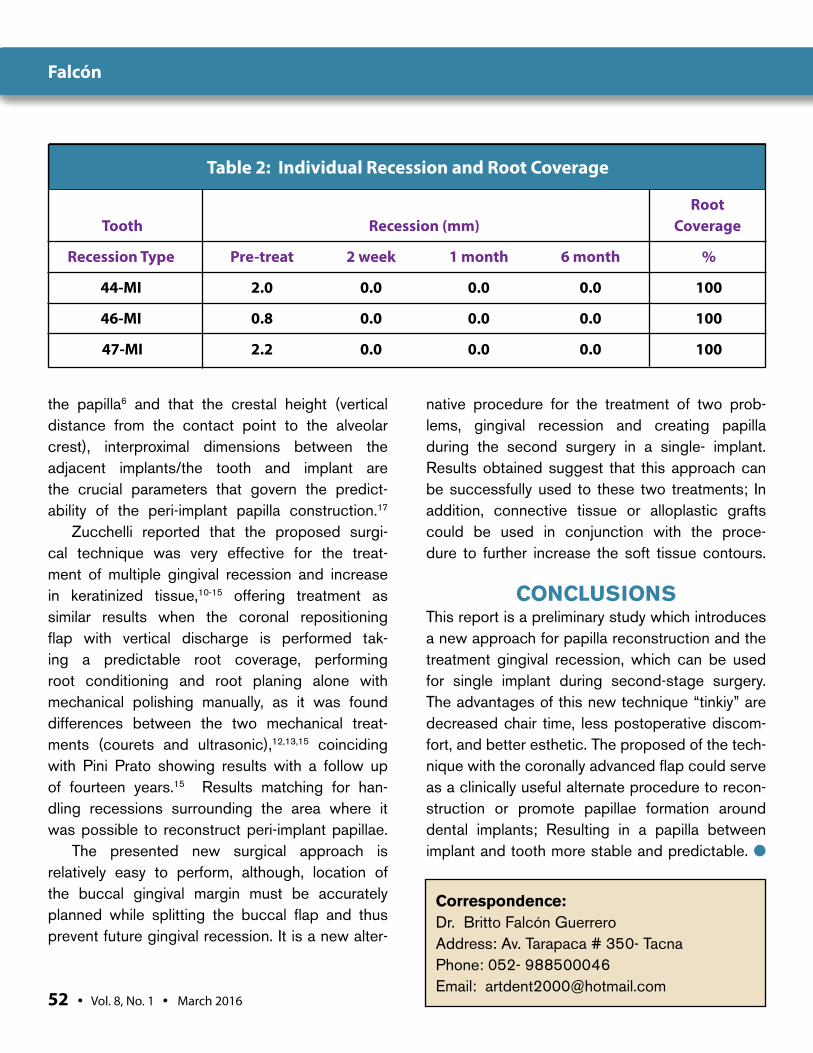
RESULTSAt 2 weeks the patient is evaluated, find-ing food impaction in the distal papilla, which causes part of the papilla miss; the mesial papilla is intact, proceeding to make impres-sion taking for the final restoration screwed (Figures 9-12). Evaluation of the papillae was performed according Jemt at baseline, 2 weeks, one month and six months (Figures 13, 14) to determine the stability of the papillae and gingival recession (Table 1). A score 3 in the mesial papilla and a score of 2 in the dis-tal papilla was achieved (according the clas-sification of Jemt), considering that there was food impaction in the distal area which caused partial loss of papillae, staying stable over 6 months (Table 1). Similarly, root coverage of adjacent recessions up to 100% was achieved during the 6 months follow-up (Table 2).
Falcón
The Journal of Implant & Advanced Clinical Dentistry • 49
Figure 5: Diagonal incision at the base of the papilla and composite resin between teeth #43 and #44 (FDI tooth numbering system).
Figure 6: Supracrestal incision design.
DISCUSSIONThe ideal goal of implant dentistry is to restore a patient to normal contour, function, comfort, esthetics, speech, and health; still very important the level, color, and texture of the peri-implant soft tissue.5,16 Four potential time points can be differentiated for soft and/or hard tissue manage-ment: prior to implant placement; at time of place-ment or during the healing phase of the implant; at second-stage surgery; and in the maintenance phase.1 In the second-stage surgery, when the tissue-punch technique is used, the crestal tis-
sue height is often leveled with the interproximal height and in the full-thickness flap with a crestal incision is often used in nonesthetic regions or for implant overdentures. However, tension created by the sutures on the facial and lingual flaps in the interimplant areas often results in a negative soft tissue profile5 and using autogenous tissue could potentially increase the number of surgi-cal procedures and limit the extent of correction.3
The level of peri-implant papilla is deter-mined by the following variables: Vertical dis-tance from the contact point to the alveolar crest
Figure 7: Flap elevation and perpendicular incision to the supracrestal in the center of the healing cap.
Figure 8: Closed surgical site with suspensory suture.
Falcón

50 • Vol. 8, No. 1 • March 2016
Figure 9: Two weeks after surgery. Note that food is impacted in the distal papilla.
Figure 10: Appropriate emergence profile and gingival architecture at 2 weeks.
Figure 11: Transmucosal impression coping. Figure 12: Final restoration.
Figure 13: Final restoration at 1 month. Figure 14: Final restoration at 6 months.
Falcón
The Journal of Implant & Advanced Clinical Dentistry • 51
and the interproximal distance between adja-cent implants and tooth and implant.16 Kan recently stated that the implant papilla may be maintained at or reestablished to the nor-mal level (4.5mm from the underlying bone) with the thick biotype, but it can seldom be created beyond 4 mm with the thin biotype.8
Palacci developed a unique additive surgi-cal technique at stage two uncovery for multiple implants, this crescent incision technique was very effective in providing a scalloped appear-ance to the soft tissue drape around the abut-ments. However, the volume of tissue was still inadequate to form an ideal interpapilla height.5,6 Grossberg reported a loss of soft tissue height of 0.5 mm when a modified flap technique is car-ried out at the time of abutment connection.2
Nemcovsky reported an increase in the inter-proximal papillary height in 89% of the sites and that regeneration of the papilla can be expected after 1 to 3 years without any additional manipula-tion of the soft tissue. But with this technique, the
interproximal papilla is not so real and the increase in tissue adjacent to the teeth was minimal; more-over finds a trend towards a negative correlation between postoperative of the papillary index score and age, therefore, a smaller increase in papil-lary height could be expected in older patients.1,5 Which does not correlate with this report clinical as a year of assessment is stable papillary height.
Misch said in the split-finger technique, the papilla is formed with tissue from both the facial and palatal aspects, which further enhances papillary support and appearance;5 but is performed only limited to the maxilla.
It should be noted that the highlighting ana-tomical and the histologic differences between the peridental and the peri-implant papilla appar-ently project the biggest limitation in the pre-dictable reconstruction of the peri-implant papilla. The restricted blood supply and a high collagen and low cellular level define the peri-implant mucosa as a “scar-like tissue” hence reducing the reconstructive predictability of
Score Pre-treat 2 week 1 month 6 month
m d m d m d m d
0 X X
1
2 X X X
3 X X X
4
Table 1: Classification of Papilla Restoration
Falcón
52 • Vol. 8, No. 1 • March 2016
the papilla6 and that the crestal height (vertical distance from the contact point to the alveolar crest), interproximal dimensions between the adjacent implants/the tooth and implant are the crucial parameters that govern the predict-ability of the peri-implant papilla construction.17
Zucchelli reported that the proposed surgi-cal technique was very effective for the treat-ment of multiple gingival recession and increase in keratinized tissue,10-15 offering treatment as similar results when the coronal repositioning flap with vertical discharge is performed tak-ing a predictable root coverage, performing root conditioning and root planing alone with mechanical polishing manually, as it was found differences between the two mechanical treat-ments (courets and ultrasonic),12,13,15 coinciding with Pini Prato showing results with a follow up of fourteen years.15 Results matching for han-dling recessions surrounding the area where it was possible to reconstruct peri-implant papillae.
The presented new surgical approach is relatively easy to perform, although, location of the buccal gingival margin must be accurately planned while splitting the buccal flap and thus prevent future gingival recession. It is a new alter-
native procedure for the treatment of two prob-lems, gingival recession and creating papilla during the second surgery in a single- implant. Results obtained suggest that this approach can be successfully used to these two treatments; In addition, connective tissue or alloplastic grafts could be used in conjunction with the proce-dure to further increase the soft tissue contours.
CONCLUSIONS This report is a preliminary study which introduces a new approach for papilla reconstruction and the treatment gingival recession, which can be used for single implant during second-stage surgery. The advantages of this new technique “tinkiy” are decreased chair time, less postoperative discom-fort, and better esthetic. The proposed of the tech-nique with the coronally advanced flap could serve as a clinically useful alternate procedure to recon-struction or promote papillae formation around dental implants; Resulting in a papilla between implant and tooth more stable and predictable. ●
Table 2: Individual Recession and Root Coverage
Root Tooth Recession (mm) Coverage
Recession Type Pre-treat 2 week 1 month 6 month %
44-MI 2.0 0.0 0.0 0.0 100
46-MI 0.8 0.0 0.0 0.0 100
47-MI 2.2 0.0 0.0 0.0 100
Correspondence:Dr. Britto Falcón GuerreroAddress: Av. Tarapaca # 350- TacnaPhone: 052- 988500046Email: [email protected]
Falcón
The Journal of Implant & Advanced Clinical Dentistry • 53
DisclosureThe author reports no conflicts of interest with anything mentioned in this article.
References1. Nemcovsky CE, Moses O, Artzi Z. Interproximal papillae reconstruction in
maxillary implants. J Periodontol 2000; 71:308-14.
2. Grossberg DE. Interimplant papilla reconstruction: assessment of soft tissue changes and results of 12 consecutive cases. J Periodontol 2001;72:958-62.
3. Tarnow DP , Chu SJ. Surgical and Prosthetic Correction of Two Adjacent Anterior Implants: A Clinical Case Report. Adv Periodontics 2011;1:174-181.
4. Pradeep AR, Karthikeyan BV. Peri-implant papilla reconstruction: realities and limitations. J Periodontol 2006;77: 534-44.
5. Misch CE, Al-Shammari KF, Wang HL. Creation of interimplant papilla through a split finger technique. Implant Dent 2004;13:20-7.
6. Palacci P, NOWZARI H. Soft tissue enhancement around dental implants. Periodontology 2000, Vol. 47, 2008, 113–132
7. Juodzbalys G, Wang HL. Soft and hard tissue assessment of immediate implant placement: A case series. Clin Oral Implant Res 2007;18:237-43.
8. Pradeep AR, Karthikeyan BV. Peri-implant papilla reconstruction: Realities and limitation. J Periodontol 2006;77:534-44
9. Jemt T. Regeneration of gingival papillae after single-implant treatment. Int J Periodontics Restorative Dent 1997; 17: 326-333.
10. Zucchelli G, De Sanctis M. Treatment of multiple recession-type defects in patients with esthetic demands. J Periodontol 2000; 71:1506-1514.
11. Zucchelli G, De Sanctis M. Long-term outcome following treatment of multiple Miller class I and II recession defects in esthetic areas of the mouth. J Periodontol 2005;76:2286-2292.
12. Zucchelli G, Mounssif I, Stefanini M, Mele M, Montebugnoli L, Sforza NM. Hand and Ultrasonic Instrumentation in Combination With Root-Coverage Surgery: A Comparative Controlled Randomized Clinical Trial. J Periodontol 2009;80: 577-585.
13. Zucchelli G, Mele M, Mazzotti C, Marzadori M, Montebugnoli L, De Sanctis M. Coronally advanced flap with and without vertical releasing incisions for the treatment of multiple gingival recessions: A comparative controlled randomized clinical trial. J Periodontol 2009;80:1083-1094.
14. Zucchelli G, Mele M, Stefanini M, Mazzotti C, Mounssif I, Marzadori M, Montebugnoli L. Predetermination of Root Coverage. J Periodontol 2010;81: 1019-1026.
15. De Sanctis M, Clementini M. Flap approaches in plastic periodontal and implant surgery: critical elements in design and execution. J Clin Periodontol 2014; 41 (Suppl. 15): S108–S122. doi: 10.1111/jcpe.12189.
16. Romeo E, Lops D, Rossi A, Storelli S, Rozza R, Chiapasco M.Surgical and Prosthetic Management of Interproximal Region With Single-Implant Restorations: 1-Year Prospective Study . J Periodontol 2008; 79:1048-1055.
17. Tarnow DP, Wallace SS. The effect of the interimplant distance on the height of the interimplant bone crest. J Periodontol 2000;71:546-9.
ATTENTION PROSPECTIVE
AUTHORSJIACD wants
to publish your article!
The Journal of Implant & Advanced Clinical Dentistry
For complete details regarding publication in
JIACD, please refer to our author guidelines at
the following link: http://www.jiacd.com/
authorinfo/ author-guidelines.pdf
or email us at: [email protected]
Falcón
Al-Fahd et al
IntroducIng
Less pain for your patients.1
Less chair side time for you.1
Mucograft® is a pure and highly biocompatible porcine collagen matrix. The spongious nature of Mucograft® favors early vascularization and integration of the soft tissues. It degrades naturally, without device related inflammation for optimal soft tissue regeneration. Mucograft® collagen matrix provides many clinical benefits:
For your patients...
Patients treated with Mucograft® require 5x less Ibuprofen than
those treated with a connective tissue graft1
Patients treated with Mucograft® are equally satisfied with esthetic outcomes when compared to connective tissue grafts2
For you...
Surgical procedures with Mucograft® are 16 minutes shorter in duration on average when compared to those involving connective tissue grafts1
Mucograft® is an effective alternative to autologous grafts3, is ready to use and does not require several minutes of washing prior to surgery
For full prescribing information, please visit us online at www.osteohealth.com or call 1-800-874-2334
References: 1Sanz M, et. al., J Clin Periodontol 2009; 36: 868-876. 2McGuire MK, Scheyer ET, J Periodontol 2010; 81: 1108-1117. 3Herford AS., et. al., J Oral Maxillofac Surg 2010; 68: 1463-1470. Mucograft® is a registered trademark of Ed. Geistlich Söhne Ag Fur Chemische Industrie and are marketed under license by Osteohealth, a Division of Luitpold Pharmaceuticals, Inc. ©2010 Luitpold Pharmaceuticals, Inc. OHD240 Iss. 10/2010
Mucograft® is indicated for guided tissue regeneration procedures in periodontal and recession defects, alveolar ridge reconstruction for prosthetic treatment, localized ridge augmentation for later implantation and covering of implants placed in immediate or delayed extraction sockets. For full prescribing information, visit www.osteohealth.com
Ask about our limited time, introductory special!
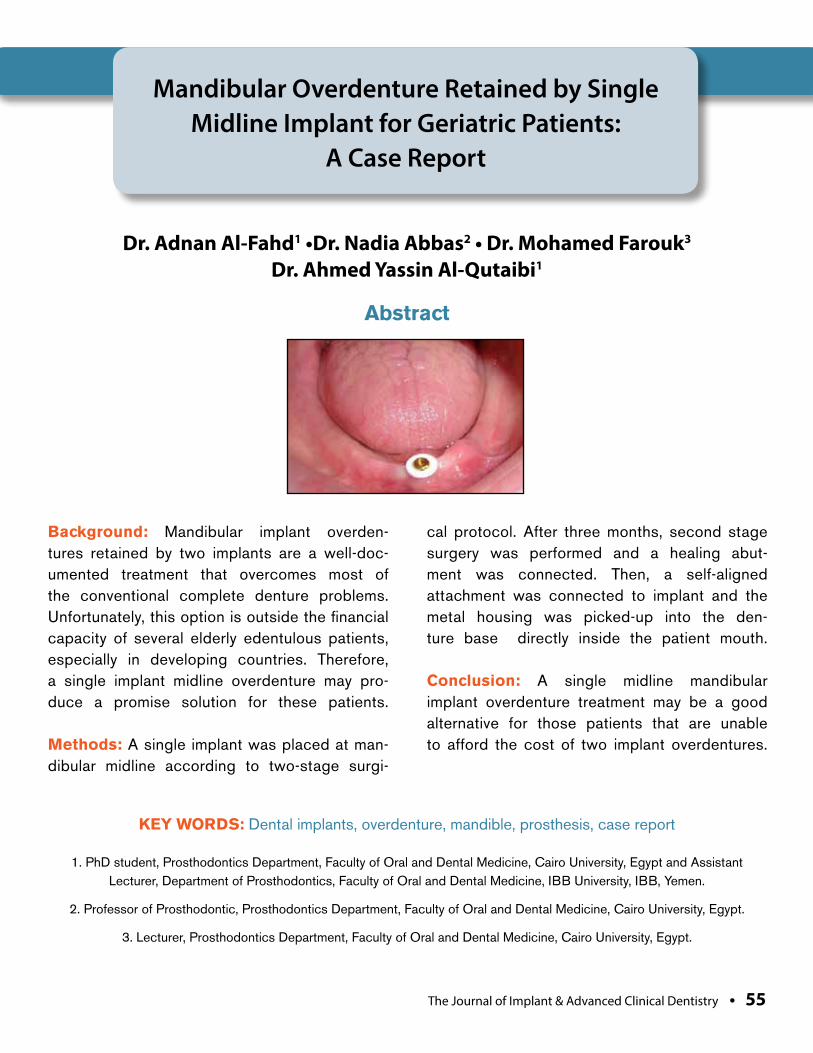
Al-Fahd et al
Background: Mandibular implant overden-tures retained by two implants are a well-doc-umented treatment that overcomes most of the conventional complete denture problems. Unfortunately, this option is outside the financial capacity of several elderly edentulous patients, especially in developing countries. Therefore, a single implant midline overdenture may pro-duce a promise solution for these patients.
Methods: A single implant was placed at man-dibular midline according to two-stage surgi-
cal protocol. After three months, second stage surgery was performed and a healing abut-ment was connected. Then, a self-aligned attachment was connected to implant and the metal housing was picked-up into the den-ture base directly inside the patient mouth.
Conclusion: A single midline mandibular implant overdenture treatment may be a good alternative for those patients that are unable to afford the cost of two implant overdentures.
Mandibular Overdenture Retained by Single Midline Implant for Geriatric Patients:
A Case Report
Dr. Adnan Al-Fahd1 •Dr. Nadia Abbas2 • Dr. Mohamed Farouk3 Dr. Ahmed Yassin Al-Qutaibi1
1. PhD student, Prosthodontics Department, Faculty of Oral and Dental Medicine, Cairo University, Egypt and Assistant Lecturer, Department of Prosthodontics, Faculty of Oral and Dental Medicine, IBB University, IBB, Yemen.
2. Professor of Prosthodontic, Prosthodontics Department, Faculty of Oral and Dental Medicine, Cairo University, Egypt.
3. Lecturer, Prosthodontics Department, Faculty of Oral and Dental Medicine, Cairo University, Egypt.
Abstract
KEY WORDS: Dental implants, overdenture, mandible, prosthesis, case report
The Journal of Implant & Advanced Clinical Dentistry • 55
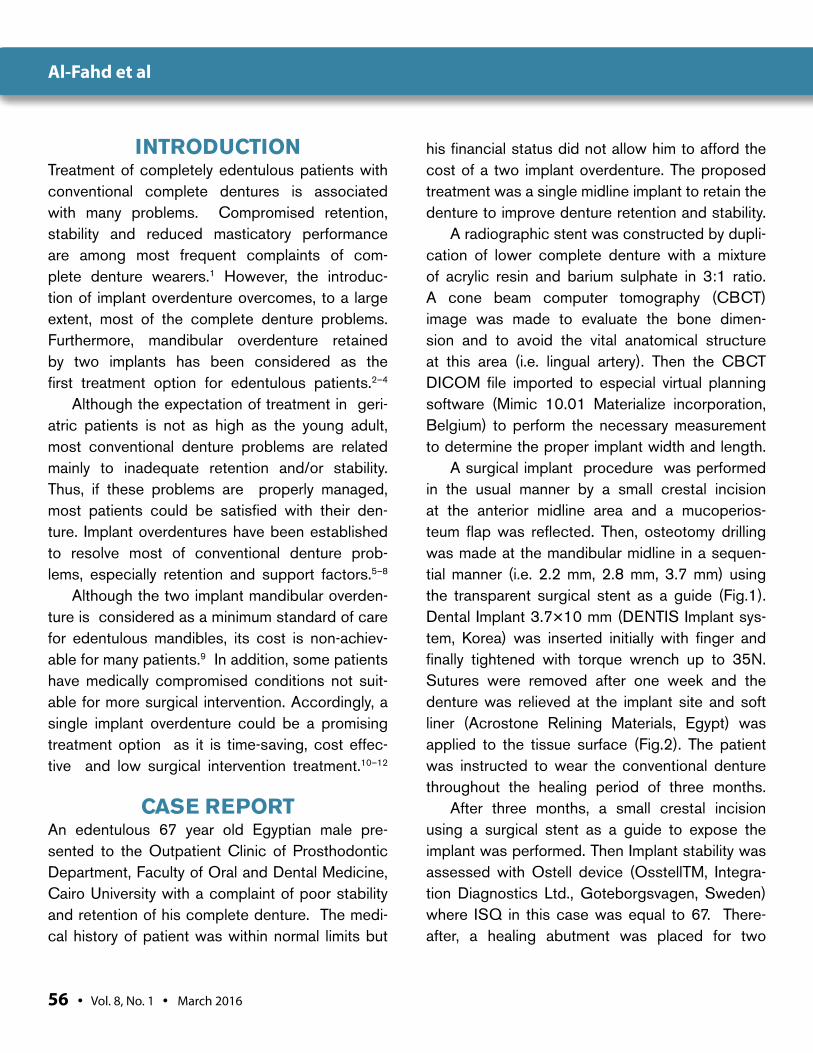
56 • Vol. 8, No. 1 • March 2016
INTRODUCTION Treatment of completely edentulous patients with conventional complete dentures is associated with many problems. Compromised retention, stability and reduced masticatory performance are among most frequent complaints of com-plete denture wearers.1 However, the introduc-tion of implant overdenture overcomes, to a large extent, most of the complete denture problems. Furthermore, mandibular overdenture retained by two implants has been considered as the first treatment option for edentulous patients.2–4
Although the expectation of treatment in geri-atric patients is not as high as the young adult, most conventional denture problems are related mainly to inadequate retention and/or stability. Thus, if these problems are properly managed, most patients could be satisfied with their den-ture. Implant overdentures have been established to resolve most of conventional denture prob-lems, especially retention and support factors.5–8
Although the two implant mandibular overden-ture is considered as a minimum standard of care for edentulous mandibles, its cost is non-achiev-able for many patients.9 In addition, some patients have medically compromised conditions not suit-able for more surgical intervention. Accordingly, a single implant overdenture could be a promising treatment option as it is time-saving, cost effec-tive and low surgical intervention treatment.10–12
CASE REPORTAn edentulous 67 year old Egyptian male pre-sented to the Outpatient Clinic of Prosthodontic Department, Faculty of Oral and Dental Medicine, Cairo University with a complaint of poor stability and retention of his complete denture. The medi-cal history of patient was within normal limits but
his financial status did not allow him to afford the cost of a two implant overdenture. The proposed treatment was a single midline implant to retain the denture to improve denture retention and stability.
A radiographic stent was constructed by dupli-cation of lower complete denture with a mixture of acrylic resin and barium sulphate in 3:1 ratio. A cone beam computer tomography (CBCT) image was made to evaluate the bone dimen-sion and to avoid the vital anatomical structure at this area (i.e. lingual artery). Then the CBCT DICOM file imported to especial virtual planning software (Mimic 10.01 Materialize incorporation, Belgium) to perform the necessary measurement to determine the proper implant width and length.
A surgical implant procedure was performed in the usual manner by a small crestal incision at the anterior midline area and a mucoperios-teum flap was reflected. Then, osteotomy drilling was made at the mandibular midline in a sequen-tial manner (i.e. 2.2 mm, 2.8 mm, 3.7 mm) using the transparent surgical stent as a guide (Fig.1). Dental Implant 3.7×10 mm (DENTIS Implant sys-tem, Korea) was inserted initially with finger and finally tightened with torque wrench up to 35N. Sutures were removed after one week and the denture was relieved at the implant site and soft liner (Acrostone Relining Materials, Egypt) was applied to the tissue surface (Fig.2). The patient was instructed to wear the conventional denture throughout the healing period of three months.
After three months, a small crestal incision using a surgical stent as a guide to expose the implant was performed. Then Implant stability was assessed with Ostell device (OsstellTM, Integra-tion Diagnostics Ltd., Goteborgsvagen, Sweden) where ISQ in this case was equal to 67. There-after, a healing abutment was placed for two
Al-Fahd et al

The Journal of Implant & Advanced Clinical Dentistry • 57
weeks to allow for proper soft tissue healing around implant. After that, the healing abutment was removed and the self-aligned attachment (KeraTor overdenture attachment, Korea) was con-nected and torqued to 35N with a torque wrench.
The pick-up procedure was done directly inside patient mouth by relieving the denture base at the site of attachment metal housing. Dur-ing pick-up white spacer was placed to prevent acrylic resin ingress inside the underlining tis-sue and the metal housing with a black process-ing cap was placed overall as shown in (Fig.3). The pick-up cold cure acrylic resin was injected all around metal housing and the patient was instructed to close in centric position until com-plete setting of acrylic resin as shown in (Fig.4).
After finishing and polishing, the black pro-cessing cap was replaced with functional reten-tive orange cap before delivery to the patient (Fig. 5). Final occlusal adjustment was performed intraorally by articulating paper until harmoni-ous occlusal contacts in posterior teeth were
obtained. After one year follow-up the patient was satisfied with only complaint about decrease in retention after 5 months due to wearing of reten-tive cap that actually replaced by another cap.
DISCUSSION The single implant is relatively a new approach that reduces time and cost considerably. This treatment option produces a promising solu-tion for complete denture problems, especially in developing countries where the treatment cost is the main challenge for many patients.
In this case a CBCT was made to accurately measure the available bone and to determine proximity to lingual artery which is a vital struc-ture as damage to it may lead to severe complica-tion.13 Two surgical stage technique was selected to allow proper time for osseointegration.14
During healing period soft liner was applied to the denture base and change every month because it act as a shock absor-bent that reduce the force and trauma
Figure 1: Transparent surgical stent. Figure 2: Soft liner applied to the mandibular denture throughout the healing period.
Al-Fahd et al
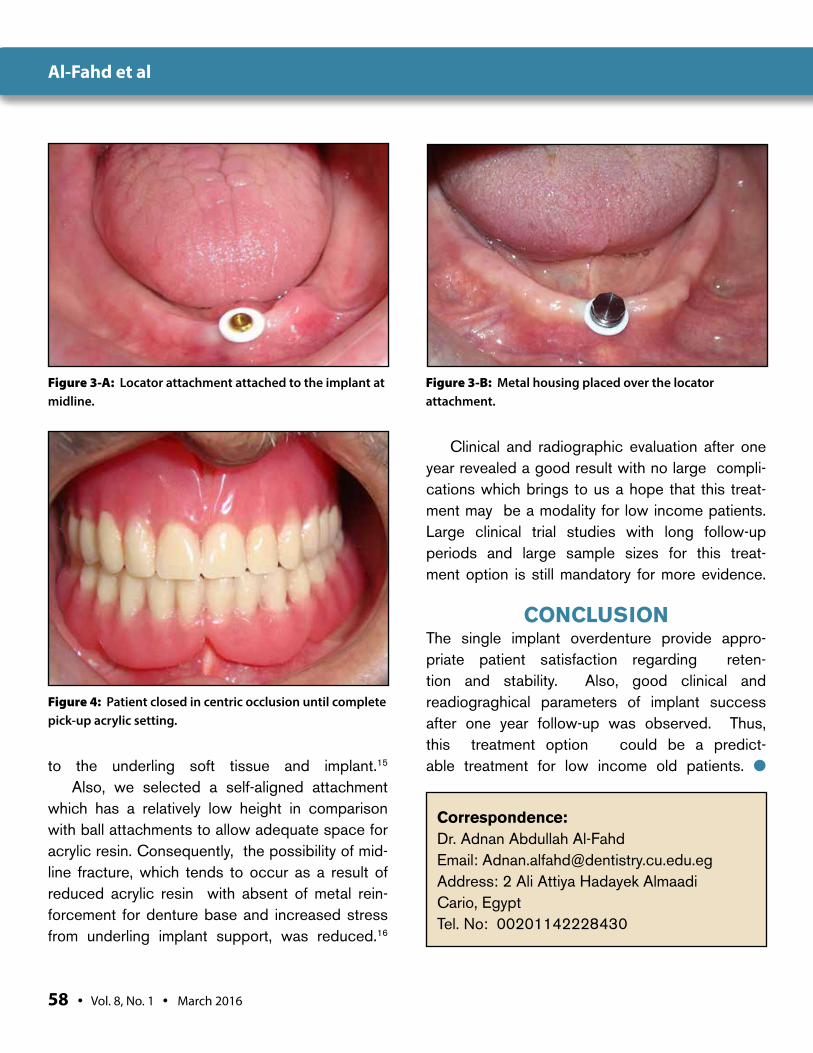
58 • Vol. 8, No. 1 • March 2016
to the underling soft tissue and implant.15 Also, we selected a self-aligned attachment
which has a relatively low height in comparison with ball attachments to allow adequate space for acrylic resin. Consequently, the possibility of mid-line fracture, which tends to occur as a result of reduced acrylic resin with absent of metal rein-forcement for denture base and increased stress from underling implant support, was reduced.16
Clinical and radiographic evaluation after one year revealed a good result with no large compli-cations which brings to us a hope that this treat-ment may be a modality for low income patients. Large clinical trial studies with long follow-up periods and large sample sizes for this treat-ment option is still mandatory for more evidence.
CONCLUSION The single implant overdenture provide appro-priate patient satisfaction regarding reten-tion and stability. Also, good clinical and readiograghical parameters of implant success after one year follow-up was observed. Thus, this treatment option could be a predict-able treatment for low income old patients. ●
Figure 3-A: Locator attachment attached to the implant at midline.
Figure 3-B: Metal housing placed over the locator attachment.
Figure 4: Patient closed in centric occlusion until complete pick-up acrylic setting.
Correspondence:Dr. Adnan Abdullah Al-FahdEmail: [email protected]: 2 Ali Attiya Hadayek Almaadi Cario, EgyptTel. No: 00201142228430
Al-Fahd et al
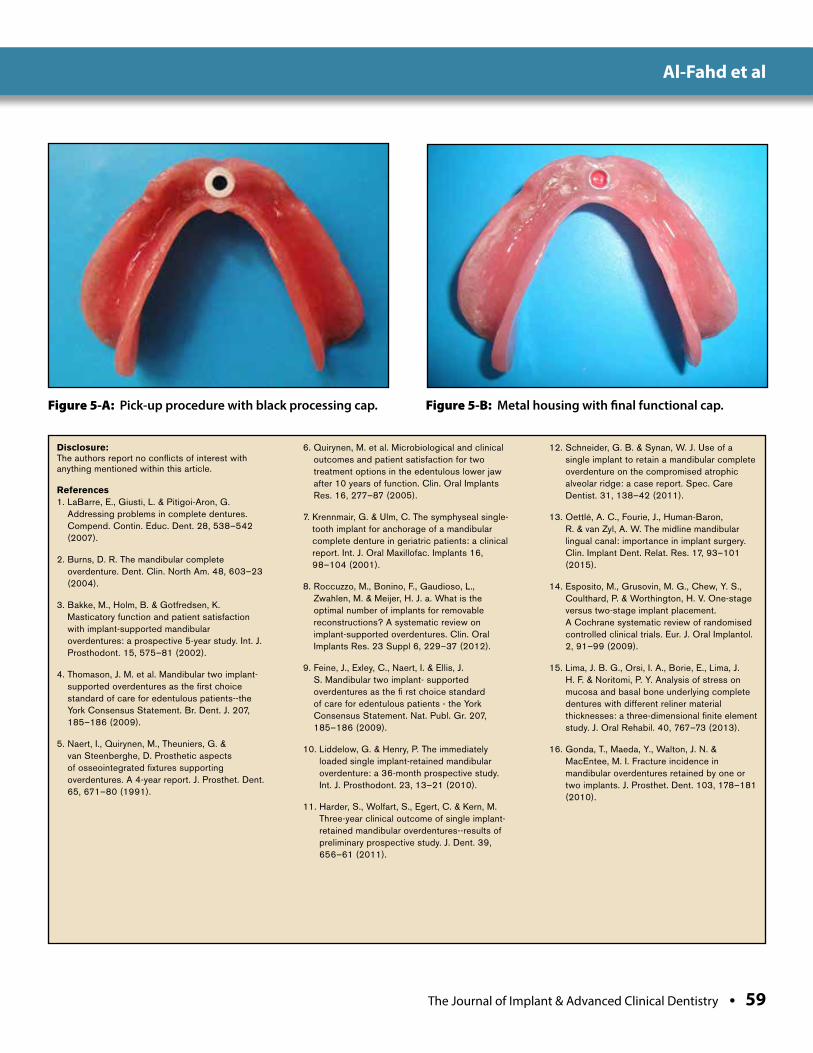
The Journal of Implant & Advanced Clinical Dentistry • 59
Figure 5-A: Pick-up procedure with black processing cap. Figure 5-B: Metal housing with final functional cap.
Disclosure:The authors report no conflicts of interest with anything mentioned within this article.
References1. LaBarre, E., Giusti, L. & Pitigoi-Aron, G.
Addressing problems in complete dentures. Compend. Contin. Educ. Dent. 28, 538–542 (2007).
2. Burns, D. R. The mandibular complete overdenture. Dent. Clin. North Am. 48, 603–23 (2004).
3. Bakke, M., Holm, B. & Gotfredsen, K. Masticatory function and patient satisfaction with implant-supported mandibular overdentures: a prospective 5-year study. Int. J. Prosthodont. 15, 575–81 (2002).
4. Thomason, J. M. et al. Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients--the York Consensus Statement. Br. Dent. J. 207, 185–186 (2009).
5. Naert, I., Quirynen, M., Theuniers, G. & van Steenberghe, D. Prosthetic aspects of osseointegrated fixtures supporting overdentures. A 4-year report. J. Prosthet. Dent. 65, 671–80 (1991).
6. Quirynen, M. et al. Microbiological and clinical outcomes and patient satisfaction for two treatment options in the edentulous lower jaw after 10 years of function. Clin. Oral Implants Res. 16, 277–87 (2005).
7. Krennmair, G. & Ulm, C. The symphyseal single-tooth implant for anchorage of a mandibular complete denture in geriatric patients: a clinical report. Int. J. Oral Maxillofac. Implants 16, 98–104 (2001).
8. Roccuzzo, M., Bonino, F., Gaudioso, L., Zwahlen, M. & Meijer, H. J. a. What is the optimal number of implants for removable reconstructions? A systematic review on implant-supported overdentures. Clin. Oral Implants Res. 23 Suppl 6, 229–37 (2012).
9. Feine, J., Exley, C., Naert, I. & Ellis, J. S. Mandibular two implant- supported overdentures as the fi rst choice standard of care for edentulous patients - the York Consensus Statement. Nat. Publ. Gr. 207, 185–186 (2009).
10. Liddelow, G. & Henry, P. The immediately loaded single implant-retained mandibular overdenture: a 36-month prospective study. Int. J. Prosthodont. 23, 13–21 (2010).
11. Harder, S., Wolfart, S., Egert, C. & Kern, M. Three-year clinical outcome of single implant-retained mandibular overdentures--results of preliminary prospective study. J. Dent. 39, 656–61 (2011).
12. Schneider, G. B. & Synan, W. J. Use of a single implant to retain a mandibular complete overdenture on the compromised atrophic alveolar ridge: a case report. Spec. Care Dentist. 31, 138–42 (2011).
13. Oettlé, A. C., Fourie, J., Human-Baron, R. & van Zyl, A. W. The midline mandibular lingual canal: importance in implant surgery. Clin. Implant Dent. Relat. Res. 17, 93–101 (2015).
14. Esposito, M., Grusovin, M. G., Chew, Y. S., Coulthard, P. & Worthington, H. V. One-stage versus two-stage implant placement. A Cochrane systematic review of randomised controlled clinical trials. Eur. J. Oral Implantol. 2, 91–99 (2009).
15. Lima, J. B. G., Orsi, I. A., Borie, E., Lima, J. H. F. & Noritomi, P. Y. Analysis of stress on mucosa and basal bone underlying complete dentures with different reliner material thicknesses: a three-dimensional finite element study. J. Oral Rehabil. 40, 767–73 (2013).
16. Gonda, T., Maeda, Y., Walton, J. N. & MacEntee, M. I. Fracture incidence in mandibular overdentures retained by one or two implants. J. Prosthet. Dent. 103, 178–181 (2010).
Al-Fahd et al

24 JIACDThe Journal of Implant & Advanced Clinical Dentistry
October 2008 Review | Oral Implications of Cancer Cheomotherapy October 2008October 2008
ADVERTISE WITHADVERTISEADVERTISE WITHADVERTISEADVERTISE WITH
TODAY!
WWW.JIACD.COM
Using revolutionary online technology, JIACD provides its
readers with an experience that is simply not available with traditional
hard copy paper journals.
Reach more customers with the dental profession’s fi rst truly interactive
paperless journal!
simply not available with traditional