Embed Size (px)
Citation preview
Modernizing Emergency
medical care in Libyan hospitals
Emergency medical care in Libyan hospitals is outdated‘Reception’ / Outpatient Department provide a disjointed serviceAn alternative model is proposedAs we all know, the emergency medical care in Libyan hospitals is far from optimum. The serviceprovided is disjointed and fragmented, and a complete overhaul is needed to modernise the service.
Introduction

• Each speciality has its own independent Emergency Department• SOPD, MOPD , POPD, GOPD• Difficulty for patients• Difficulty for Staff• Poor outcome of careAt present, each Speciality has its own ‘Reception’ and Emergency Department. This arrangementleads to significant problems.For example, patients would not necessarily have the ability to determine which OPD they shouldattend, and valuable time is lost. Patients attending the wrong Department will be seen by staff whoare not trained to deal with their conditions. All that leads to poor outcome, unnecessary suffering,and wasted resources.
Current Situations

• 24-hour access to high-quality emergency care• Easy access to diagnostic facilities• Immediate access to Critical Care / Intensive Care• Immediate access to emergency treatment including resuscitation,stabilization and surgeryThe Emergency Department should provide 24-hour high-quality care to all those who need it. It should allow easy access to diagnostic facilities, such as radiology, pathology, haematology, and biochemistry, to help in diagnosing conditions in a timely manner. It is also essential that such departments work closely with Intensive Care facilities, to provide the continuity of care that some critically ill or seriously injured patients might need. Emergency Departments should be backed up by facilities to enable the resuscitation, stabilization, and treatment of patients, including specialist surgeries
Optimum Emergency Care
The Emergency DepartmentModern Emergency Departments
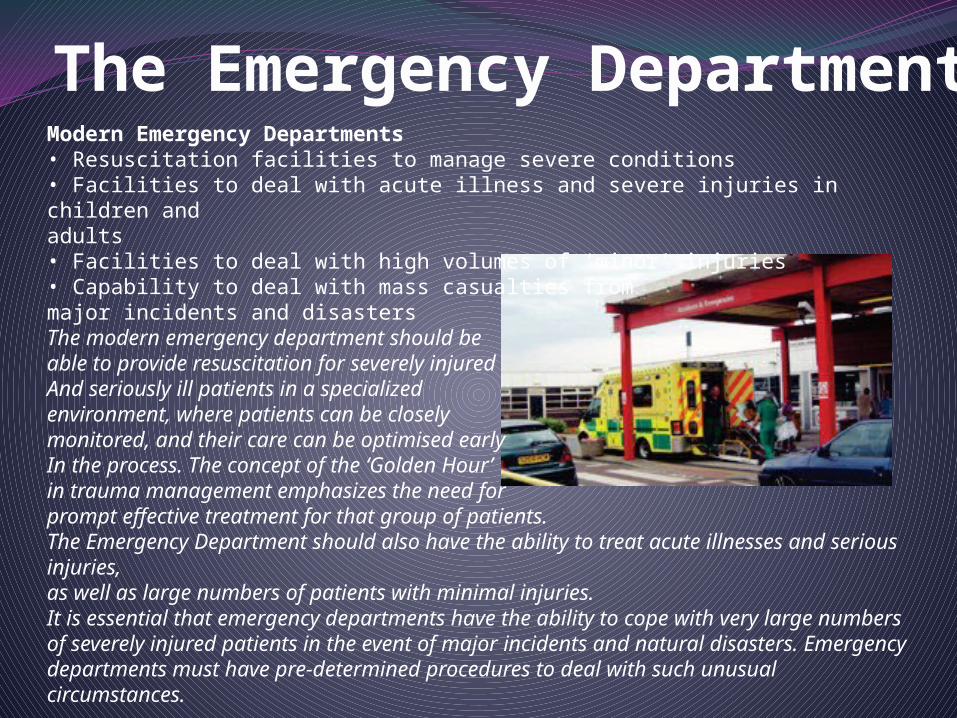
• Resuscitation facilities to manage severe conditions• Facilities to deal with acute illness and severe injuries in children andadults• Facilities to deal with high volumes of ‘minor’ injuries• Capability to deal with mass casualties from major incidents and disastersThe modern emergency department should be able to provide resuscitation for severely injured And seriously ill patients in a specialized environment, where patients can be closely monitored, and their care can be optimised early In the process. The concept of the ‘Golden Hour’ in trauma management emphasizes the need for prompt effective treatment for that group of patients.The Emergency Department should also have the ability to treat acute illnesses and serious injuries,as well as large numbers of patients with minimal injuries.It is essential that emergency departments have the ability to cope with very large numbersof severely injured patients in the event of major incidents and natural disasters. Emergencydepartments must have pre-determined procedures to deal with such unusual circumstances.

It has the following requirements:• Area to fit t a specialised resuscitation bed.space to ensure 360° access to all parts of the patient for uninterrupted procedures• Circulation space to allow movement of staff and equipment around the work area.• Space for equipment, monitors, storage, wash up and disposal facilities.• Appropriate lighting, equipment to hang IV fluids etc.• Maximum possible visual and auditory privacy for the occupants of the room and other patients and relatives.• Minimum size for a single bed resuscitation room is 35m2 or 25m2 for each bed space if in amultimedia room (not including storage area).• The following should be immediately accessible:Intravenous access trolleys• Peritoneal lavage tray, Thoracotomy tray, Intercostals tray , USSG, Urinary catheterisation tray,Airway management tray (including surgical airway equipment), Invasive vascular access insertiontray, Paediatric resuscitation equipment, and Refrigerator.
The Resuscitation Room
This room is used for the resuscitation and treatment ofcritically ill or injured patients.
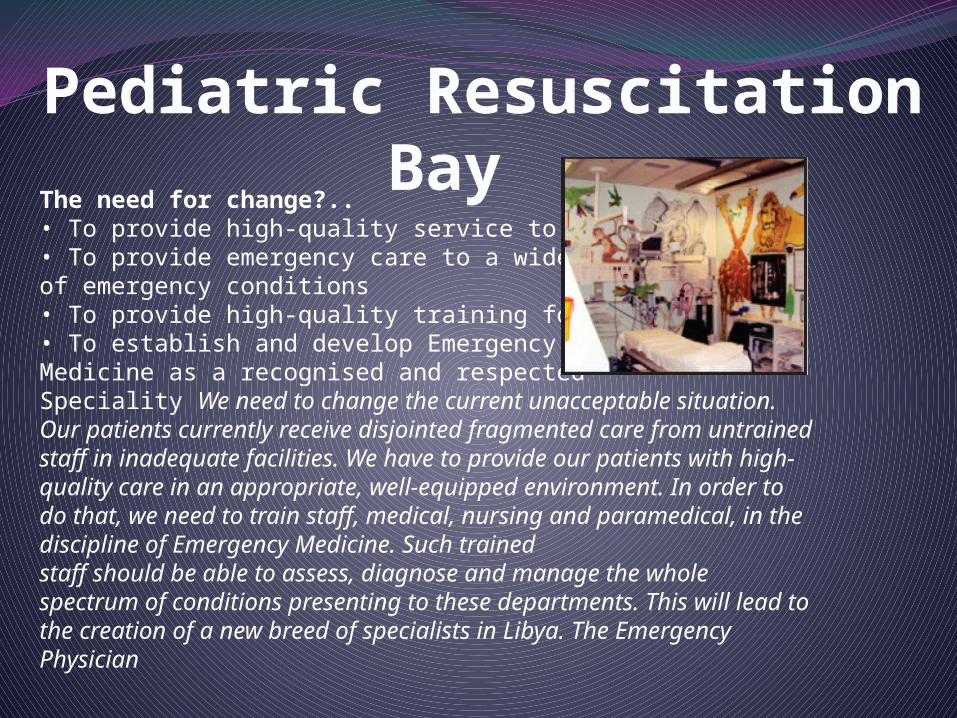
The need for change?..• To provide high-quality service to patients• To provide emergency care to a wide spectrum of emergency conditions• To provide high-quality training for staff• To establish and develop EmergencyMedicine as a recognised and respectedSpeciality We need to change the current unacceptable situation. Our patients currently receive disjointed fragmented care from untrained staff in inadequate facilities. We have to provide our patients with high-quality care in an appropriate, well-equipped environment. In order to do that, we need to train staff, medical, nursing and paramedical, in the discipline of Emergency Medicine. Such trainedstaff should be able to assess, diagnose and manage the whole spectrum of conditions presenting to these departments. This will lead to the creation of a new breed of specialists in Libya. The Emergency Physician
Pediatric Resuscitation Bay

• All patients present to a single ‘Reception’ area.• Rapid assessment by trained nurses– ‘Triage’• Patients directed to the appropriate area– Resuscitation– ‘Major’ Area– ‘Minor’ AreaIn the model we propose, which is broadly based on the Emergency Departments in the UK, patients would present to a central reception area, regardless of their complaint or injury. The patient wouldthen be assessed by trained nurses, who, using protocols and guidelines, can determine the broad nature of the complaint, and direct the patient to the appropriate part of the Department. Theywould also be able to determine the seriousness of the problem by the process of ‘Triage’, therefore determining the priority at which patients would be seen.
The Proposed Model…
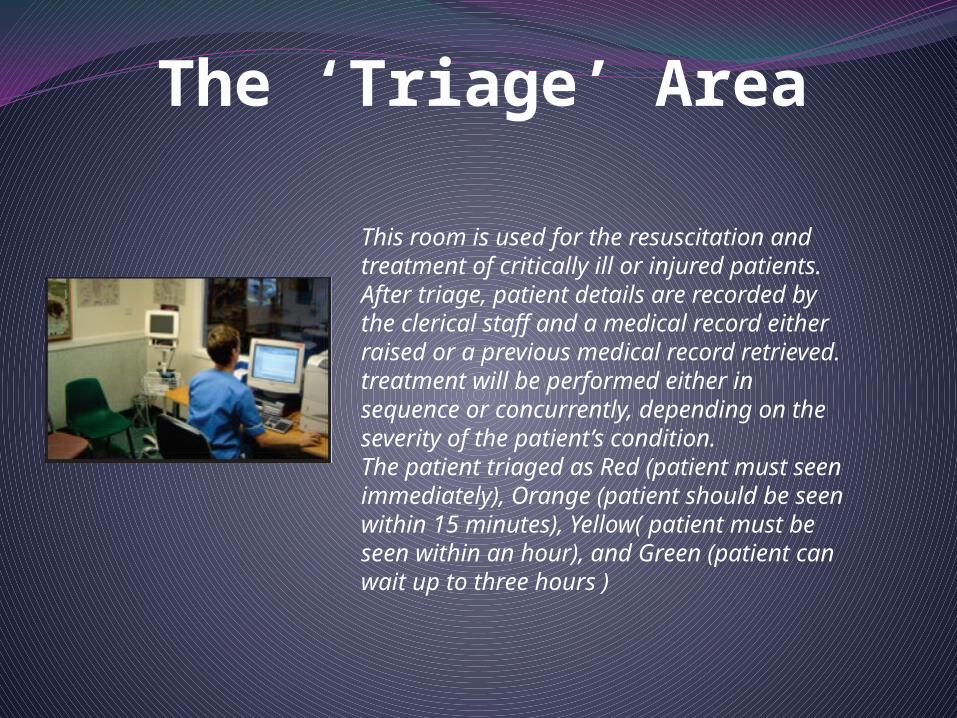
This room is used for the resuscitation and treatment of critically ill or injured patients. After triage, patient details are recorded by the clerical staff and a medical record either raised or a previous medical record retrieved. treatment will be performed either in sequence or concurrently, depending on theseverity of the patient’s condition.The patient triaged as Red (patient must seenimmediately), Orange (patient should be seen within 15 minutes), Yellow( patient must be seen within an hour), and Green (patient can wait up to three hours )
The ‘Triage’ Area

Major Treatment Bay
Minor Treatment Area
• Specialists:– Consultants– Middle Grade DoctorsThe Emergency Department should be staffed by an adequate number of doctors, with varying degrees of skills and qualifications. The senior staff, or the Consultants, provide the supervision, guidance and training. They also oversee the management of patients, and get closely involved in the assessment and treatment of the more seriously-ill patients. In addition, Consultants have important management roles, which would allow the smooth running of this complex operation. The Middle Grade doctors provide the direct supervision of the junior staff, and offer support and help to trainees. They can also be involved in certain management issues, such as staff recruitment, education and manpower management. It would be expected that larger Emergency Departments would have two types of trainees:- basic trainees, who are junior doctors working in the Emergency Department to gain experience to help them develop their career in other disciplines (Orthopaedics, General Surgery, Anaesthetics, Medicine, General Practice, etc.), and specialist trainees, who are experienced doctors training in the speciality of Emergency Medicine. These doctors would have broad experiences in General Medicine, General Surgery, Orthopaedics, Critical Care and Paediatrics. They work under the supervision of Consultants to compliment their training to become Emergency Medicine Consultants in the future.
Medical Staffing
• Broad base of skills• Flexibility• More senior nurses have important management roles• Specialist skills and extended roles The Emergency Department nurses are highly-skilled nurses, with broad experiences. They must have the flexibility to work under unpredictable conditions. Senior nurses are heavily involved in the management of the Department, and support the senior medical staff in that task. Increasingly, Emergency Nurses are developing extended roles, and specialist skills, allowing them to see and manage a number of conditions independently.
Nursing Staffing

• Helicopter Landing Pad• Rapid Response Team• Decontamination Facilities• Major Incident and Disaster Management Plans• Observation Ward
Extra Facilities
Patients can be lifted byHelicopter
Helicopter Pad
Decontamination Facilities
A decontamination room should be available for patients who are contaminated with toxic substances. In addition to the requirements of an isolation room, this room must:• Be directly accessible from the ambulance bay without entering any other part of the department• Have a flexible water hose, floor drain and contaminated water trap

The Eye Room Theatre
How can we achieve this?...• A new concept
• Staff training• Modern environmentIn order to achieve this change, we must embrace the new model of delivery of emergency care. Then, it is equally important that staff training and good physical environments go hand in hand.
How can we achieve this?...• Experience of others
• Develop links with international centres• Exchange programmes and ‘twinning’ initiatives with recognisedteaching hospitals It would make perfect sense that we benefit t from the experiences of others who have established emergency care programmes. It would be advantageous to us to establish links with recognised training centres and organizations in countries like the UK.I have already established the feasibility of bringing over to the UK trainees from Libyan teaching hospitals, for training in Emergency Medicine in the UK. Early discussions are in place for twinninginitiatives, which would allow Libyan doctors to train in reputable UK centres providing high-quality training in Emergency Medicine. The success of such important and exciting initiatives dependsheavily on cooperation from the Libyan authorities.
In Summary…• Change is badly needed• Alternative models available• Methods of achieving change are being explored• Help and support from authorities is essentialIn summery, there is no doubt that the current situation is suboptimal and needs to be changed. There are a number of alternative models that can replace the existing system. I have described one that is well tried and tested in an established health care system. Ways in which we can achieve the transition smoothly have been proposed, but such change depends heavily on support from the Libyan authorities

ConclusionThe emergency department is an integral unit of a hospital and the experience of patients attending the emergency department significantly influences the public image of the hospital. Its function is to receive, stabilise and managepatients who present with a large variety of urgent and non urgent conditions whether self or otherwise referred. The emergency department also provides for the reception and management of disaster patients as part of its rolewithin the Disaster plan of each region. In addition to standard treatment areas, some departments may require additional specifically designed areasto fulfil special roles.