Embed Size (px)
Citation preview
0
Modern University for Technology & Information
Professor Dr Amani Nabil Shafik
Professor of Medical Pharmacology
Faculty of Medicine- Cairo University
2021-2022
1
Content
Subject Page
1- Routes of drug administration & Dosage forms
2
2- Actions of Drugs on Isolated Rabbit’s Intestine
13
3- Action of drugs on isolated toad’s heart
16
4- Locally acting drugs
18
5- Drugs and some related problems in dentistry
26
6- Treatment of common oral conditions
30
7- Emergency in dental practice
38
8- EBM
41
9- Prescription Writing
45
2
Routes of drug Administration
and dosage forms
Drug is given to a patient either to produce local actions or systemic effects.
Drugs are given either through:
I-Gastrointestinal tract (Enteral route):
Oral
Sublingual
Rectal
II-Parenteral: Injection
III. Inhalation
IV. Topical e.g. to skin, eye, ears, joint, vagina, etc.
I- Enteral routes
1.Oral administration
Advantages: Easy administration, economic & safe.
Disadvantages:
- Not suitable for Unconscious patients.
- Not convenient for emergency cases.
- Not convenient for drugs that are irritant to GIT.
- Drug can be lost by vomiting or diarrhea.
- Drug can be destroyed by digestive enzymes (e.g. insulin) or by gastric acidity
(e.g. benzylpenicillin).
- Drugs can be affected by diet (through combination with food items affect
absorption).
- Drugs can be destroyed through first - pass metabolism (e.g. lidocaine)
- Some drugs are not absorbed from GIT if systemic action in intended (e.g.
streptomycin).
Factors affecting oral absorption:
* Factors related to the drug formulation: disintegration and rate of dissolution,
excipients «additives», molecular weight, lipid solubility, stability in gut contents and
pka of the drug.
* Factors related to the patient:
1-State of absorbing surface, specific factor…
3
2-Surface area: Rate of absorption from intestine is greater than from stomach.
3-pH within the gut: Where absorption of weak acidic drugs starts in stomach while
weak base drugs are absorbed from intestine. Drugs which are destroyed by gastric
juice or those irritant on stomach are administered in enteric coated form e.g.
sodium salicylate.
4-Rate of dissolution and gut motility: Absorption of solid form of a drug is dependent
on its rate of dissolution, so drugs may be given in sustained release form to prolong
their duration. Decreased gastric emptying will increase the rate of absorption of
slowly dissoluted drug (digoxin) and decrease that of rapidly dissolute one
(paracetamol). Metoclopramide increases gastric emptying so decreases digoxin
absorption and increase absorption of paraceramol.
5-Presence of other substance within the lumen: e.g. food, calcium and iron decrease
tetracycline absorption. Fatty meals can enhance griseofulvin absorption.
6-First pass effect (pre-systemic metabolism): where drugs must pass through gut
mucosa and liver before reaching systemic circulation.
a- Gut first pass effect : e.g. benzyl penicillin is destroyed by gastric acidity,
insulin by digestive enzymes and tyramine by mucosal enzymes.
b- Hepatic first pass effect: e.g lidocaine (complete destruction so not effective
orally) and propranolol (extensive destruction) so oral dose must be higher
than parenteral route.
To overcome hepatic first pass metabolism increase the oral dose or use other
routes e.g. sublingual nitroglycerin and IV lidocaine.
Oral dosage forms
4
A) Solid Forms :
1)Tablets: tablet is a solid dosage form of varying weight, size and shape in which the
drug is compressed with pharmacologically inert substances (excipients).
Types of tablets:
- Simple
- Sugar coated
- Enteric coated in which tablets coated with substances which resist dissolution in the
acid juice of the stomach but dissolve in the alkaline juices of the intestine. Such
coating serves to protect the gastric mucosa against the action of irritant
e.g. sodium salicylate.
- Sustained – release (SR), controlled-release (CR), timed-release, or retard: These are
tablets that are designed to provide a prolonged action their advantage is reduction
in the frequency of administration of the drug with improved compliance by the
patient. These long acting preparations are formed of groups of drug particles
enclosed in coats with different dissolution rates in the GIT fluids. They are
designed to produce slow uniform absorption of the drug.
2) Capsules: These are gelatin shell containing individual doses of drugs; their purpose is to
provide accurate medication of drugs in a tasteless form. Capsules may be:
- Hard gelatin capsules packed with powdered drugs
- Soft gelatin capsules packed with “liquid” drugs
- Enteric coated capsules (see above)
5
3) Powders: In packets or in bulk.
4) Effervescent granules:
These are prepared by adding sodium bicarbonate + tartaric or citric acid. When added to
water CO2 is liberated → improved palatability
B) Liquid forms include:
Aqueous Preparations
Mixture: Mixtures are preparations in which drugs are simply dissolved or suspended in
water.
Emulsion: An emulsion consists of a fixed oil dispersed as small globules in water by
means of an emulsifying agent e.g. gums.
Suspension: A suspension is a preparation of insoluble finely divided drugs suspended in an
aqueous vehicle.
Syrup: Syrups are concentrated aqueous solutions of sugar containing flavoring, coloring or
therapeutically active substances e.g. syrup tolu.
Decoction: These are obtained by boiling in water dried plants. They should be prepared
fresh.
Infusion: These are obtained by soaking dried plants in cold or boiling water. Like
decoctions, they spoil quickly and so must be prepared fresh.
Alcoholic preparations:
a. Elixir: Elixirs are sweetened, flavored hydroalcoholic solutions that contain 25% alcohol.
They may be:
- Non- medicated elixirs used only as vehicles.
- Medicated elixirs that contain in addition a specific drug.
b.Tinctures: Tinctures are alcoholic preparations of vegetable drugs e.g. tincture
belladonna.
6
2- Sublingual administration Drug is absorbed through mucosa under the tongue to reach directly to systemic circulation.
Sublingual tablets should be palatable & effective in small dose.
Advantages:
Rapid onset of action
Bypass first passes effects in liver or intestine.
Avoids GIT enzymes and pH
The effect can be terminated by spitting out the tablet.
Sublingual dosage forms Sublingual tablets (linguets): These are small tablets to be placed under the tongue (e.g.
nitroglycerin sublingual tablets used in treatment of acute attacks of angina pectoris)
3- Rectal administration Drugs are absorbed through rectal mucosa to reach systemic circulation.
Advantages:
Drugs absorbed from the rectum mostly bypass the liver & avoids digestive enzymes.
This route of drug administration is suitable for:
o Patient suffering from vomiting.
o Drugs with unpleasant taste.
o Uncooperative children.
o Unconscious patients.
o Giving large volume of fluids.
Rectal dosage forms
1- Rectal Suppositories:
These are solid preparations at room temperature that melt at body temperature. The base
usually employed for preparation of rectal suppositories is “Oil of Theobroma”
(cocoa butter).
7
2- Enema:
These are fluid preparations for administration into the rectum.
Types of enemas:
a- Retention: These are given in order to be retained within the bowel, usually as a means
of giving a drug e.g. magnesium sulfate enema to reduce intracranial pressure and
prednisolone enema in ulcerative colitis.
b- Evacuant: These are given to evacuate feces from the bowel. They may act either
physically on account of their bulk causing bowel distension which promotes reflex
evacuation or by virtue a mild irritant associated with the enema, e.g. soap
NB: Vaginal suppositories (Pessaries): Special type of suppositories applied in vagina
either to produce local action or to be absorbed to produce systemic effect.
II- Parenteral routes 1- Injection
They should be sterile and pyrogen free.
Drugs for injection are either:
Solution.
Suspension.
Powder to be dissolved before use.
They are dispensed in the form of : ampoules or vials or bottles
Methods of Injection: Intravenous (I.V.), Intramuscular (I.M.), subcutaneous (S.C.),….
8
A. Intravenous (I.V.) either in a bolus form or infusion (drip).
Advantages:
It has the most rapid onset of action.
It is suitable for administration of large volumes
It is suitable for irritating drugs.
Disadvantages
Undesirable reactions are likely to occur as anaphylactic reaction or pyrogenic
reaction.
Local reaction can occur as abscess, necrosis or local venous thrombosis especially
with prolonged infusion and with bolus doses of irritant formulations.
Velocity reaction can occur.
Once the drug is injected, it can not be withdrawn.
Not suitable for drugs in an oily vehicle or suspensions.
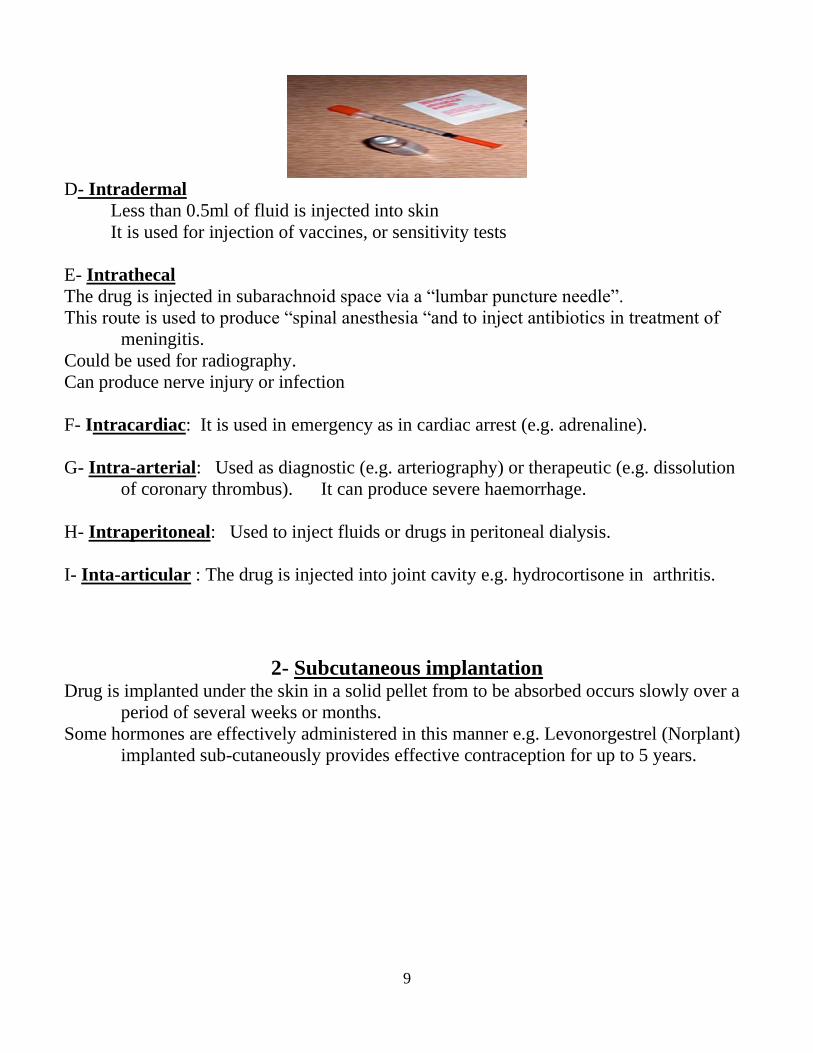
B. Intramuscular
It is suitable for aqueous or oily solutions and suspensions.
Moderately irritating drugs can be given by this route.
Drugs in aqueous solution are absorbed quite rapidly after I.M. injection, while
solution in oil or suspended in water oil (depot preparations) the rate of absorption
is very slow and constant.
The rate of absorption from muscles is greater than that from subcutaneous tissues.
C. Subcutaneous
Non irritant aqueous solution or suspension can be injected in subcutaneous tissue
(hypodermis)
Absorption from S.C. sites is more rapid and complete than after oral administration.
The rate of absorption of a suspension is slow compared with that of a soluble preparation.
The incorporation of a vasoconstrictor agent in a solution of a drug to be injected S.C.
retards absorption.
Absorption from S.C. sites of injection is poor in peripheral circulatory failure.
9
D- Intradermal
Less than 0.5ml of fluid is injected into skin
It is used for injection of vaccines, or sensitivity tests
E- Intrathecal
The drug is injected in subarachnoid space via a “lumbar puncture needle”.
This route is used to produce “spinal anesthesia “and to inject antibiotics in treatment of
meningitis.
Could be used for radiography.
Can produce nerve injury or infection
F- Intracardiac: It is used in emergency as in cardiac arrest (e.g. adrenaline).
G- Intra-arterial: Used as diagnostic (e.g. arteriography) or therapeutic (e.g. dissolution
of coronary thrombus). It can produce severe haemorrhage.
H- Intraperitoneal: Used to inject fluids or drugs in peritoneal dialysis.
I- Inta-articular : The drug is injected into joint cavity e.g. hydrocortisone in arthritis.
2- Subcutaneous implantation Drug is implanted under the skin in a solid pellet from to be absorbed occurs slowly over a
period of several weeks or months.
Some hormones are effectively administered in this manner e.g. Levonorgestrel (Norplant)
implanted sub-cutaneously provides effective contraception for up to 5 years.
10
III- Inhalation Drugs given by inhalation are absorbed through the thin alveolar epithelium to reach to
pulmonary circulation.
Advantages:
Drugs given by inhalation are rapidly absorbed from the lungs due to the large surface area
and rich blood supply of the alveoli.
Disadvantages:
Inaccurate dosing.
Drug may irritate pulmonary epithelium.
Dosage Forms of drugs given by inhalation
• Gas: as oxygen, and nitrous oxide (general anesthetic)
• Volatile liquid (vapor) e.g. halothane (general anesthetic).
• Solution administered as aerosol by means of a nebulizer or atomizer e.g. salbutamol
(bronchodilator). Aerosols provide high local concentration for action on bronchi,
minimizing systemic effects.
• Finely micronized powder e.g. disodium cromoglycate (Intal) used in prophylaxis of
bronchial asthma given by a special inhaling device called spinhaler.
IV- Topical administration Dosage Forms of drugs used for topical application
o Eye:
• Eye drops
• Eye Ointment
• Eye lotion
Preparation for eye should be sterile.
Topically applied ophthalmic drugs are used primarily for their local effects on the eye.
Some systemic absorption occurs when eye drops are given and can result in side effects
(e.g. bronchospasm in asthmatic patients using timolol eye drops for glaucoma).
o Ear drops
11
o Vagina:
• Vaginal tablet
• Vaginal ovule or pessary
• Vaginal douche
• Vaginal cream
o Nose:
• Nasal drops
• Nasal spray
• Nasal inhaler
o Mouth:
• Mouth wash
• Gargle
• Lozenge
• Paint
o Skin:
• Ointment: A fatty base in which one or more active drugs may be
incorporated. It is used for external application to the skin or mucous
membranes. Some ointment bases allow for some drug absorption to take
place so that systemic effects result e.g. adrenal steroids.
• Cream: This is prepared from a base which is miscible with water. Cream is
less greasy than ointment.
• Lotion: These are aqueous preparations that are applied to the skin without
rubbing e.g. calamine lotion.
• Dusting powder: This is a powder applied to the skin for protective purposes
e.g. talc powder.
• Liniment: This is a preparation of an irritant e.g. camphor in an oily, soapy or
alcoholic vehicle intended to be applied to the skin by rubbing. Liniment are
usually used for their counter-irritant effects e.g. camphor liniment.
• Collodion: This is a solution of nitrated cellulose and colophony resin in a
mixture of ether and alcohol. After evaporation of ether and alcohol a thin
flexible layer remains on skin. It is used for protection of wounds.
12
Transdermal Delivery System (TDS):
This is application of drugs to the skin for systemic effects e.g., Nitroglycerin
ointment or adhesive discs (patches)
Advantages of TDS: Prolonged blood levels with minimal fluctuations. Avoidance of
hepatic first – pass elimination.
13
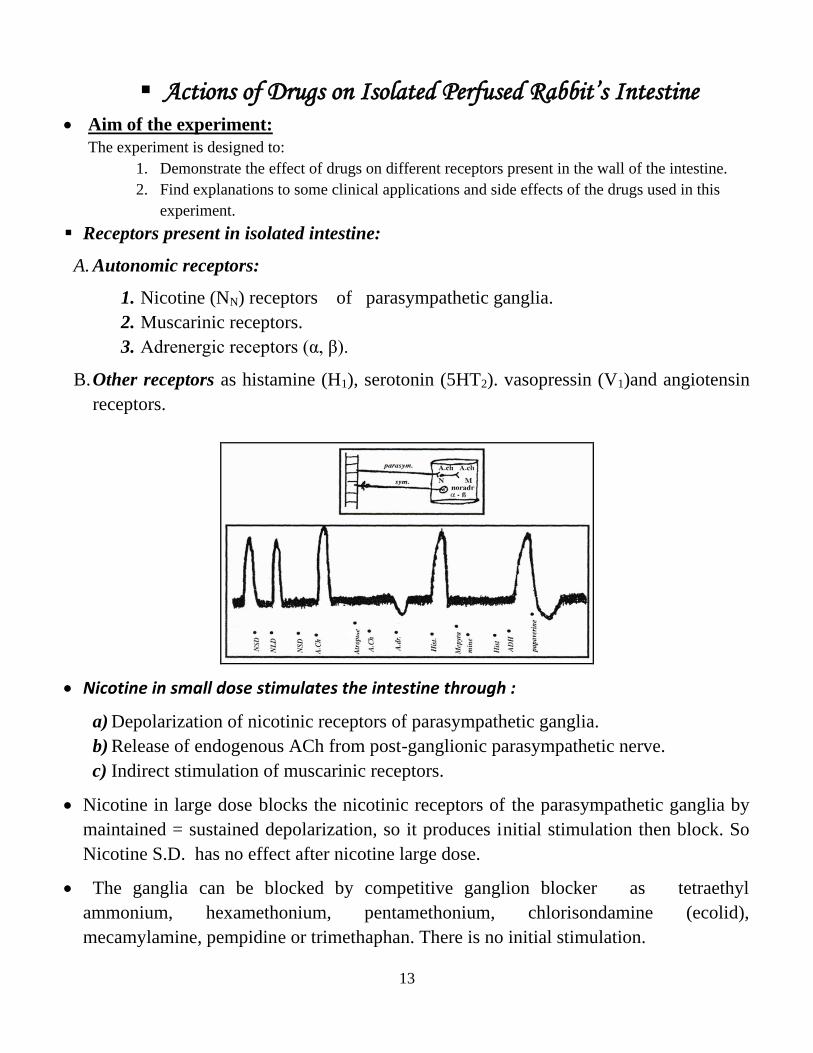
▪ Actions of Drugs on Isolated Perfused Rabbit’s Intestine • Aim of the experiment:
The experiment is designed to:
1. Demonstrate the effect of drugs on different receptors present in the wall of the intestine.
2. Find explanations to some clinical applications and side effects of the drugs used in this
experiment.
▪ Receptors present in isolated intestine:
A. Autonomic receptors:
1. Nicotine (NN) receptors of parasympathetic ganglia.
2. Muscarinic receptors.
3. Adrenergic receptors (α, β).
B. Other receptors as histamine (H1), serotonin (5HT2). vasopressin (V1)and angiotensin
receptors.
• Nicotine in small dose stimulates the intestine through :
a) Depolarization of nicotinic receptors of parasympathetic ganglia.
b) Release of endogenous ACh from post-ganglionic parasympathetic nerve.
c) Indirect stimulation of muscarinic receptors.
• Nicotine in large dose blocks the nicotinic receptors of the parasympathetic ganglia by
maintained = sustained depolarization, so it produces initial stimulation then block. So
Nicotine S.D. has no effect after nicotine large dose.
• The ganglia can be blocked by competitive ganglion blocker as tetraethyl
ammonium, hexamethonium, pentamethonium, chlorisondamine (ecolid),
mecamylamine, pempidine or trimethaphan. There is no initial stimulation.
14
• ACh stimulates the intestine by acting on muscarinic receptors.
• Atropine blocks muscarinic receptors by competition, so Ach has no effect after
atropine.
• Histamine stimulates intestine by acting on H1 receptors and its action can be blocked
by H1 blocker as mepyramine, promethazine, chlorpheneramine, terfenadine, antazoline,
diphenhydramine....
• Adrenaline relaxes the intestine by acting on adrenergic receptors (α , β).
• Vasopressin stimulates the intestine ( spasmogenic through V1receptors).
• Papaverine relaxes the intestine (direct spasmolytic).
Uses of parasympathomimetics:
Non-obstructive urine retention, post-operative abdominal distension- paroxysmal
atrial tachycardia- glaucoma.
Physostigmine is the antidote to atropine and neostigmine is the antidote to curare
and is used in myasthenia gravis.
• ACh, carbachol and anticholinesterases have muscarinic and nicotinic actions, so they
produce hypotension which is reversed by atropine.
• Choline esters are not given I.V. or I.M.
Direct Spasmolytics include:
Papaverine. Volatile oils & khellin.
Nitrites and organic nitrates. Aminophylline.

15
Intestinal Stimulants
1- Ganglion stimulant e.g.:- Nicotine small dose (NSD).
2- Muscarinic receptor stimulant = parasympathomimetic
e.g.:- 1- Choline esters (acetyl choline, methacholine, and carbachol).
2- Natural parasympathomimetic alkaloids e.g. pilocarpine and
muscarine.
3- Reversible anticholinestrases (Neostigmine, physostigmine,etc..).
4- Irreversible anticholinestrases (organophosphorous compounds).
3- Histamine
4- Serotonin
5- Vasopressin
6- Angiotensin II
Intestinal Inhibitors
1- Adrenergic α-receptor stimulants e,g. phenylephrine
2- Adrenergic β-receptor stimulants e.g. isoprenaline
3- Adrenergic α- & β receptor stimulants e,g. adrenaline & noradrenaline
4- Direct
e.g. 1- Papaverine
2- Volatile oils e,g, peppermint
3- Nitrites & Nitrates
4- Aminophylline

16
Actions of drugs on isolated perfused toad’s heart
Types of receptors present:
1. Nicotinic receptors of parasympathetic ganglia.
2. Muscarinic receptors (M2).
3. Adrenergic receptors (B1).
4. Histamine receptors (H2).
• Nicotine S.D. inhibits heart by stimulating nicotinic receptors of parasympathetic
ganglia. It acts by releasing ACh from post-ganglionic parasympathetic nerve ending, so
its action can be prevented by ganglion blocker or by atropine.
• Nicotine L.D. produces initial stimulation followed by block.
• ACh inhibits the heart and its action is blocked by atropine.
• Adrenaline stimulates the heart and its action is blocked by B-blocker.
• Caffeine is direct stimulant and quinidine is a direct myocardial depressant.
• direct depressant as:
1. General anaesthetic as halothane.
2. Antiarrhythmic drug as (quinidine, procainamide, disopyramide) or calcium blocker.
3. Emetine HCl (antiamoebic) or antihistaminic (H1 blocker).
• direct stimulant as cardiac glycosides, xanthines, amrinone,.....
17
Cardiac Stimulants
1- Adrenergic B1-receptor stimulants
e,g. 1- Adrenaline,
2- Noradrenaline,
3 Isoprenaline,
4- Dobutamine
2- H 2-receptor stimulant (histamine).
3- Direct myocardial stimulant e.g. caffeine, digitalis
Cardiac Depressants
1- Ganglion stimulant
e.g.:- 1- Nicotine small dose (NSD), present in cigarette smoke.
2- Muscarinic receptor stimulant = parasympathomimetic
e.g.:- 1- Choline esters ( acetyl choline , methacholine ,and carbachol)
2- Natural parasympathomimetic alkaloids e.g. pilocarpine and muscarine.
3- Reversible anticholinestrases (Neostigmine , physostigmine,etc..).
4- Irreversible anticholinestrases (organophosphorous compounds).
3- Direct myocardial depressant:e.g. Quinidine
18
Locally acting drugs
1. Antiseptics & Disinfectants -Antiseptic is an agent applied on a living tissue to inhibit the bacterial growth.
- Disinfectant is an agent used to inhibit or kill bacteria in inanimate objects (not on
living tissue)
A) Physical agents
1- Heat such as superheated steam
2- Irradiation such as ultraviolet rays, sunlight
3- Surface active agents: soaps and detergents
4- Substances exerting osmotic pressure: concentrated solution of sugar and salts
B) Chemical agents
I. Inorganic
1- Oxidizing agents: hydrogen peroxide, potassium permanganate.
2- Acids and alkalis: strong mineral acids, boric acid and caustic alkalis
3- Metallic salts: silver nitrate, mercurochrome, zinc sulphate.
II. Organic
1- Alcohols: ethanol and isopropanol
2- Aldehydes: formaldehyde
3- Phenols and simple aromatic compounds: phenol, cresol and chlorhexidine
4- Halogens: iodine, povidone iodine,
5- Dyes: gentian violet, brilliant green, acriflavine.
Uses:
1. Disinfectants of surgical instruments: - Formaldehyde for delicate electrical instruments
2. Antiseptic wash and dressings - Cetrimide, gentian violet, weak iodine solution
3. Cleansing agent for wound- Hydrogen peroxide (10-20%)
Important examples in dental practice include
Hydrogen peroxide:
▪ It is a colorless and odorless liquid. It produces thick froth in mouth. It should
be kept in dark bottles away from sunlight and in a cool place to prevent its
dissociation into water and oxygen
Uses:
(a) Antiseptic (specially anaerobic bacteria) to treat acute gingivitis, acute ulcerative
stomatitis (in tissues it liberates nascent oxygen)
(b) Bleaching agent: to remove superficial stains on the teeth
(c) Local hemostatic during cavity preparation
N.B. Long-use may cause hypertrophy of papillae of tongue
19
Potassium Permanganate (Condy's crystals) Antiseptic & deodorant: by liberation of nascent oxygen and by metallic action of
manganese. Its chief disadvantage is staining properties.
Uses: Mouth washes for stomatitis and Vincent's infection (it is replaced by hydrogen
peroxide).
2. Dental Caries Dental caries is a degenerative condition characterized by decay of the hard and soft
tissues of the teeth. It is mainly caused by infection and decaying food.
▪ To reduce the incidence of dental caries, ammonium ions are applied to the oral cavity
to decrease the number of acid producing pathogens, reduce the acidity of the mouth
and dissolve dental plaques.
Treatment of Dental Caries
1. Chlorophyll: a green coloring matter of plant present in many tooth pastes and tooth
powders to act as a protective agent 2. Antibiotics: They are present in dentifrices to reduce bacterial count of the mouth e.g.
penicillin,
3. Silver Nitrate applied on the deciduous teeth after cleaning debris and decaying
material
4. Fluorides
▪ Caries can be reduced by adding fluorides in water supply (one part of fluoride to
million part of water). Also dentifrices are convenient source of fluoride.
▪ Fluoride applied topically on enamel and plaque is more important than
systemically.
▪ Infants do not receive fluoride supplements until the age of 6 months.
Mechanism of action of fluoride in dental caries
1. Prevents acid decalcification of the tooth structure by inhibiting bacterial enzymes
which produce lactic acid
2. Increases tooth resistance to acid decalcification by changing the hydroxyl apatite of
enamel, dentine or bone into fluorapatite by which is more resistant to lactic acid
attack than the hydroxyl apatite.
Uses:
1- Prophylaxis of dental caries: sodium fluoride
▪ One part of sodium fluoride to million part of drinking water
▪ Tablets (1 mg): one tablet per day during the period of tooth development to
nursing mothers and to children up to the completion of calcification of third
molars.
2- Treatment of dental caries: application of 2% sodium fluoride solution every six
months to the teeth. This leads to the absorption of fluorine on the enamel surface
as calcium fluoride.
20
N.B.
➢ Sodium fluoride should be used carefully as it is poisonous substance. Acute toxicity (toxic dose 2.5-5 g fluoride found in 5-10 g Na fluoride) is manifested by
severe gut upset, acidosis, hypotension, arrhythmias and respiratory failure.
Treatment includes gastric lavage, administration of milk, alkalinization of urine
and supportive measures.
Chronic toxicity due to long-time intake of high doses of fluoride can result in dental
fluorosis (range from white flecks to extensive brown staining) and crippling
fluorosis (thickening of the cortex of long bones and exostosis especially in
vertebrae, and musculoskeletal changes involving calcification of ligaments,
kyphosis and limitation of motility.
brasivesDental a3. They are fine powder preparations which pass through a 60 mesh powder sieve.
Uses
1. Help the scouring action of tooth brush mechanically
2. Help cleaning, polishing and filling of teeth
Preparations: 1. Pumice: It is a light porous stone of volcanic origin.
2. Precipitated calcium carbonate: it is white finely ground chalk with mild abrasive
action.
Dentifrices4. They are therapeutic mechanical aids which are available as either tooth powder or tooth
paste. Many ingredients may be added to the dentifrices to acquire certain functions e.g.
1. Abrasives
2- Detergents to have cleaning actions
3. Antiseptics: menthol, cinnamon, boric acid
aterialsRoot canal filling m5. They are aseptic, insoluble, non-irritant materials used to seal the apex of the root, the
dentine foramina and tubules and make firm barrier against moisture and bacteria.
▪ Usually two or more are combined and used for filling purpose e.g. silver amalgam &
eucopercha.
ntsObtunda6. They are agents which are used to either diminish or eliminate the dentine sensitivity
in order to make the excavation painless.
• Obtundant use has declined due to the availability of local anesthetics e.g. xylocaine
for painless excavation.
21
• They may act through:
1. Paralyzing the sensory nerve endings e.g. phenol, camphor, menthol,
creosote, olive oil, ..
2. Precipitating proteins e.g. silver nitrate, zinc chloride,..
3. Destroying the nervous tissue e.g. absolute alcohol
7. Local Anesthetics Local Anesthetics (LA) are the drugs which upon topical application or local
injection cause reversible loss of sensory perception, especially of pain, in a
restricted area of the body.
• These drugs act by excessive stimulation followed by depression. To work
efficiently, the dental local anesthetics should have some requirements such as:
o High intrinsic activity, which ensures complete anesthesia for all dental
treatment
o Rapid onset
o Adequate duration of anesthesia (30 to 60 min for standard dental treatment)
o Low systemic toxicity
o High efficacy-toxicity ratio
o Low overall incidence of serious adverse effects
• The concentration of local anesthetics for dental use is higher from those for
nondental use, because the volume which can be injected into the oral mucosa is
limited.
• Local anesthetics cause some degree of vasodilation, therefore, vasoconstrictor
agents can be added to local anesthetic solutions to antagonize LA action, reduce
bleeding at surgical site, diminish toxicity and prolong the duration of anesthesia.
• Local anesthetics containing vasoconstrictor agents are to be used with caution in
patients with pheochromocytoma, uncontrolled or unstable angina, cardiac
arrhythmias, congestive heart failure, hyperthyroidism, or diabetes.
• An acidic carrier solution is added to the LA cartridge to maintain the pH of the
solution. Apart from this the dental cartridge also contains a reducing agent
Metabisulfite that prevents oxidation of the vasoconstrictor and Thymol that acts as a
fungicide.
8. Demulcents & Protective Demulcents are viscid inert agents used to protect and lubricate mucous
membranes. They sooth the inflamed and denuded mucosa by preventing contact
with air or irritants in the surrounding. They include:
• Acacia (Gum acacia): protect mucous membranes from irritation by coating its
surface with a gummy layer. So it is used to treat catarrhal infections of the mouth
• Glycerine : It is used as an emollient and protective to skin as a protective demulcent.
22
• Tragacanth (Gum tragacanth) is applied on mucous abrasions arising from friction to
form a gelatinous mass. It forms a valuable fixative for the denture when first worn
9. Astringents They are agents used to diminish the excretion or exudation of superficial cells. They act by
precipitating proteins in superficial cells, which are thus hardened.
The insoluble layer of precipitated proteins has the following actions:
a. Resists bacterial attack
b. Forms a protecting coating against irritants
c. Delays absorption from the surface e.g. toxins
d. They are also used in combination with antiseptics as mummifying agents
e. They help hemostasis by promoting clotting through precipitation of blood proteins
▪ They include
1. Vegetable astringents: tannic acid & catechu
2. Metallic astringents: zinc chloride and sulphate, alum, aluminum chloride, copper
sulphate, lead acetate.
➢ Aluminum chloride and Ferrous sulfate are preferred astringents amongst
prosthodontists because they cause minimum tissue damage.
10. Mummifying agents They are agents used to harden and dry tissues of the pulp and root canal so that the
tissues are resistant to infection (remain aseptic), more than one drug are used in the
form of paste.
▪ Clinically used important mummifying agents are paraform, iodoform, liquid
formaldehyde, tannic acid,
▪ Mummifying agents are particularly used when it is not possible to remove the pulp and
contents of root completely.
11. Bleaching agents
They are agents used to remove pigmentation of the teeth.
▪ They include reducing agents as sodium thiosulphate (hyposulphate), oxidizing agents as
perhydrol (30% hydrogen peroxide) and chlorinated lime powder (liberates chlorine).
N.B.
o Ultraviolet rays from a carbon or mercury arc lamp can be used to bleach the dentine
o Iron and silver stains on the teeth can be removed by hypochlorites
12. Mouth washes
They are solutions used to rinse the mouth.
23
▪ Superficial infections of the mouth are often helped by warm mouthwashes which have a
mechanical cleansing effect and cause some local hyperemia. However, to be effective,
they must be used frequently and vigorously.
o A warm saline mouthwash is ideal and can be prepared either by dissolving half a
teaspoonful of salt in a glassful of warm water or by diluting compound sodium
chloride mouthwash with an equal volume of warm water.
▪ Therapeutic mouth washes are prepared to reduce plaques, gingivitis, dental caries and
stomatitis
▪ Cosmetic mouth washes are formulated to reduce bad breath
▪ Recently mouth washes are being used as a dosage form for a number of specific
problems in the oral cavity. For this purpose certain medications are added to these
mouth washes e.g. antihistamine, hydrocortisone, nystatin, ..
▪ Mouth washes generally contain 4 groups of excipients:
a. Alcohol is used as solubilizing agent for some flavoring agents as well as a preservative
b. Surfactanst are nonspecific substances which are used to help in the solubilization of
flavors and in the removal of debris by providing foaming action
c. Flavors are used to overcome disagreeable taste
d. Coloring agents are used to give a pleasing color to mouth wash.
13. Antiplaque/Antigingivitis
▪ Dental plaque is the soft, nonmineralized bacterial deposit that forms on teeth that are
not adequately cleaned. There are different types of plaques leading to different types of
periodontal diseases.
▪ The microflora of the plaque is the source of numerous noxious products that are
deleterious to the teeth (such as organic acids) or to the periodontium (such as
ammonia, hydrogen sulfide, methyl mercaptan, toxic amines, and many enzymes). In
addition plaque bacteria produce inflammation-inducing substances and release
endotoxin and bacterial antigens, which indirectly cause damage. So, the dental plaque
is the common denominator in caries and periodontal diseases.
Control of plaque :
I. Agents acting against the microflora per se
1. Antibiotics:
▪ Systemic penicillins and erythromycin have resulted in emergence of resistant
bacteria.
▪ Topical non-absorbable antibiotics such as vancomycin, bacitracin, and kanamycin
are used in mouth washes.
▪ Topical tetracycline rinses can reduce the amount of plaque formed during a
nonbrushing period and can inhibit the development of ginigivitis.
24
▪ However the greatest promise of this antibiotic is in its use in controlled delivery
systems (in which the drug is embedded in a polymer matrix or in a biodegradable
carrier) suitable for intra-pocket insertion to suppress or eliminate periodontal
pathogens of the sub-gingival plaque microflora (this ensure highly sufficient
concentration of the antibiotic at action site).
2. Oxygenating Agents:
▪ Hydrogen peroxide mouth rinses have been reported to reduce plaque formation and
gingivitis and arrest ulcerative gingivitis.
3. Halogens:
▪ Oxychlorosene and chlorine dioxide are used in mouthwashes and chloramine (1%)
is used as a subgingival irrigant for office use.
▪ Povidone-iodine which affects gram-positive and gram negative bacteria, fungi,
mycobacteria, viruses and protozoa. It has been used in many mouthwashes, but has
a disagreeable taste and may stain teeth and tongue which interfere with compliance.
It can cause idiosyncratic mucosal irritation and hypersensitivity reactions and may
interfere with thyroid function tests.
4. Fluorides
▪ At sufficiently high concentrations, fluorides act as antibacterial agent. Stannous
fluoride in mouth rinse or in toothpaste diminishes the plaque.
5. Quaternary ammonium compounds:
▪ Several mouthwashes contain these agents such as benzethonium chloride. They are
more active against gram-positive than gram-negative bacteria.
6. Phenolic compounds:
▪ Phenol and its derivatives, thymol, chlorothymol and hexylresorcinol have weak
antiplaque activity and many limitations in use including bad taste, poor water
solubility, rapid discoloration, toxicity and allergy.
Thymol is available as mouthwash solution. It can reduce bacterial resistance to
common drugs such as penicillin through a synergistic effect, and thymol has been
shown to be an effective fungicide, particularly against fluconazole-resistant strains.
When used to reduce plaque and gingivitis, thymol has been found to be more effective
when used in combination with chlorhexidine than when used purely by itself.
7. Chlorhexidine:
▪ Chlorhexidine is an effective antiseptic which has the advantage of inhibiting plaque
formation on the teeth.
▪ It does not, however, completely control plaque deposition and is not a substitute for
effective tooth brushing as it poorly penetrates into the stagnant areas once pocketing
has developed.
▪ Chlohexidine can be used as a mouthwash, spray or gel for secondary infection in
mucosal ulceration and for controlling gingivitis, as an adjunct to other oral hygiene
measures.
25
▪ These preparations may also be used instead of tooth brushing where there is a painful
periodontal condition or if the patient has a hemorrhagic disorder or is disabled.
Side effects include mucosal irritation, taste disturbance, reversible brown staining of
teeth and tongue, and parotid gland swelling.
II. Agents interfering with bacterial attachment
They act either by attacking plaque matrix components or altering the tooth surface.
III. Mechanical removal of plaque.
14. Dental protective and dressings
They are used as:
a. Protective linings for cavities to prevent staining or chemical irritation of the dentine
b.Varnishes over synthetic fillings to protect them from secretions until setting is
complete and
c. To help in pulp healing.
1. Zinc Oxide: a weak antiseptic and used as basis for ointment and cements.
2. Resin: is a fine crystalline powder which is obtained as residue left after distilling oil
of turpentine.
3. Calcium hydroxide It is used as bland pulp-capping paste to help complete pulp
healing.
4. Gutta percha coagulated milky juice obtained from certain rubber trees that hardens
on cooling.
26
Drugs and some related problems in dental practice
Saliva is important for the protection of teeth against tooth decay, regulating the mouth's
pH value and diluting the acids produced by the dental plaque bacteria so decrease
risk of tooth decay.
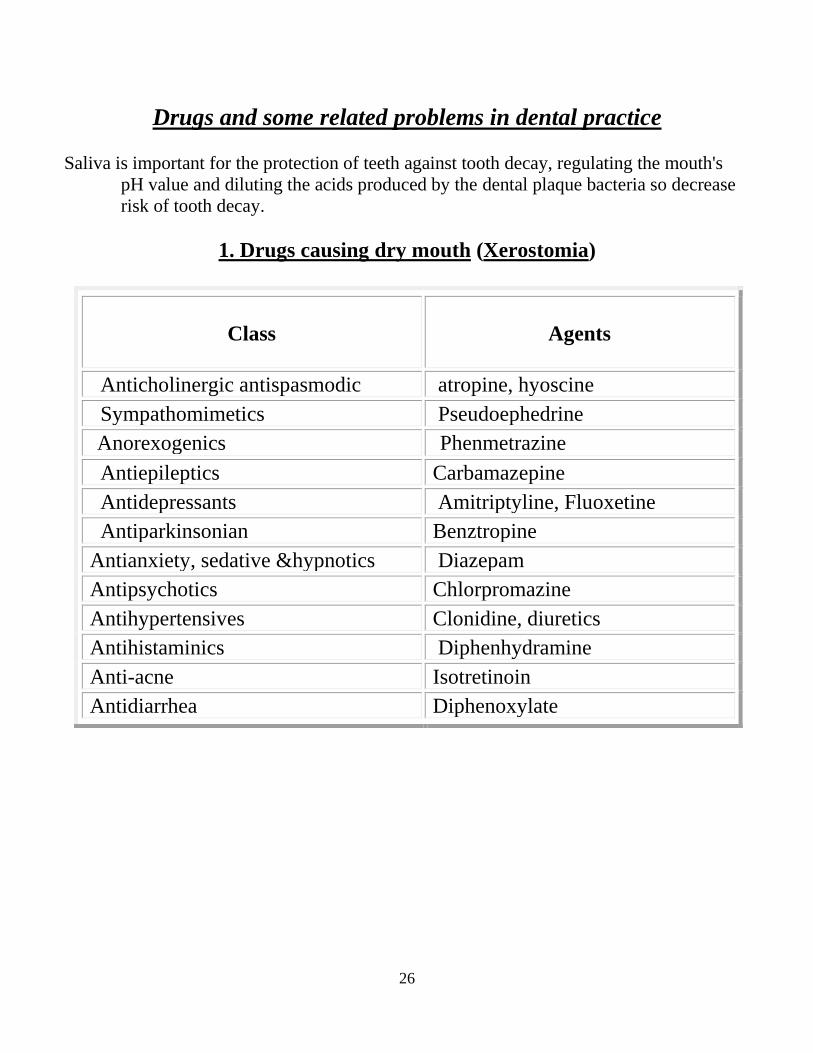
1. Drugs causing dry mouth (Xerostomia)
Class Agents
Anticholinergic antispasmodic atropine, hyoscine
Sympathomimetics Pseudoephedrine
Anorexogenics
Phenmetrazine
Antiepileptics Carbamazepine
Antidepressants Amitriptyline, Fluoxetine
Antiparkinsonian Benztropine
Antianxiety, sedative &hypnotics Diazepam
Antipsychotics Chlorpromazine
Antihypertensives Clonidine, diuretics
Antihistaminics Diphenhydramine
Anti-acne Isotretinoin
Antidiarrhea Diphenoxylate
27
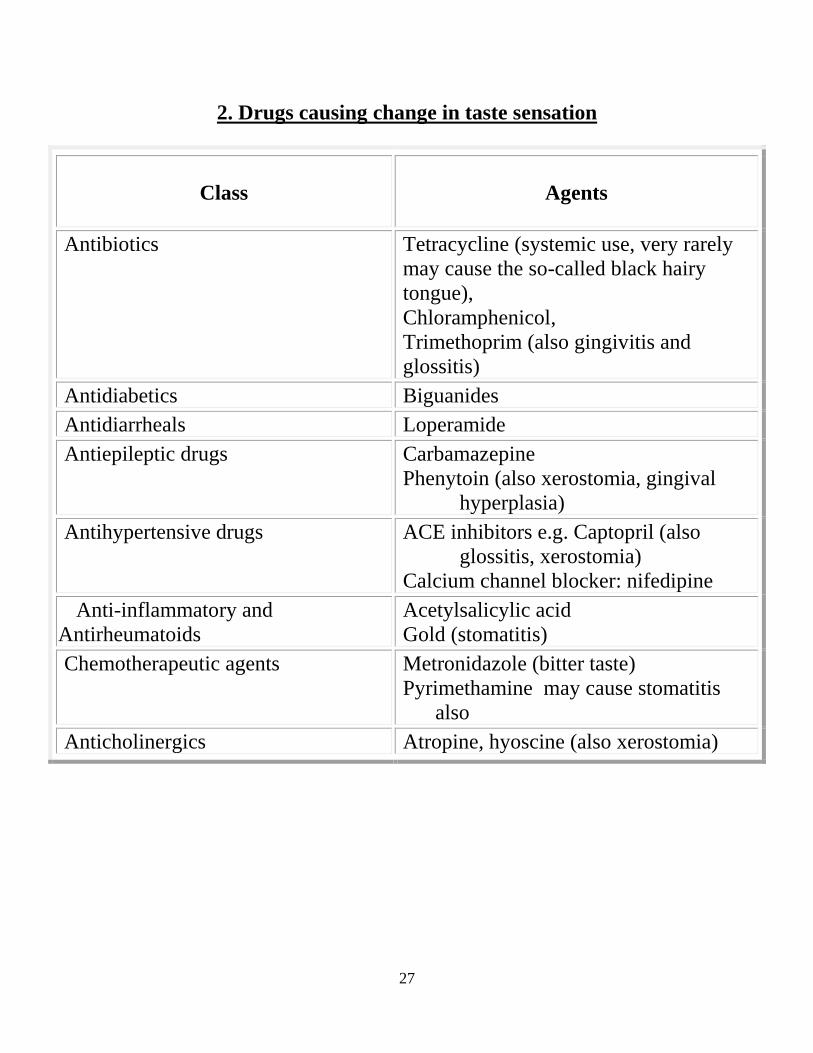
2. Drugs causing change in taste sensation
Class Agents
Antibiotics Tetracycline (systemic use, very rarely
may cause the so-called black hairy
tongue),
Chloramphenicol,
Trimethoprim (also gingivitis and
glossitis)
Antidiabetics Biguanides
Antidiarrheals Loperamide
Antiepileptic drugs Carbamazepine
Phenytoin (also xerostomia, gingival
hyperplasia)
Antihypertensive drugs ACE inhibitors e.g. Captopril (also
glossitis, xerostomia)
Calcium channel blocker: nifedipine
Anti-inflammatory and
Antirheumatoids
Acetylsalicylic acid
Gold (stomatitis)
Chemotherapeutic agents Metronidazole (bitter taste)
Pyrimethamine may cause stomatitis
also
Anticholinergics Atropine, hyoscine (also xerostomia)
28
Prophylaxis against bacterial endocarditis
prior to dental procedure
Antibiotic prophylaxis is recommended for the following conditions:
o Prosthetic cardiac valve
o Congenital cardiac malformations
o Valvular heart diseases
o Previous bacterial endocarditis
o Hypertrophic cardiomyopathy
Principle treatment
1. Oral amoxicillin taken or cephalexin or cephadroxil taken 1 hour before the
procedure.
2. If the patient can not take the drug orally or there is no time:
IM or IV ampicillin or IM or IV Cefazolin within 30 minutes of starting the
procedure.
3. If the patient is allergic to penicillin:
Oral clindamycin or azithromycin or clarithromycin taken 1 hour before the
procedure .
4. If the patient is allergic to penicillin and unable to take the drug orally:
IV Clindamycin within 30 minutes of starting the procedure.
Drugs and pregnancy Categories of drugs according to relative risk and benefits during pregnancy by FDA.
Pregnancy Categories according to FDA
A- Studies on humans; no risk (safest)
B- Animal studies- no risk; No human studies
C- Either animal studies show adverse effect and no human studies OR no animal or human
studies (benefit should outweigh risk)
D- Positive evidence of human risk; but benefits may outweigh risks
X- Positive evidence of human risk; risk outweighs benefit and drug is contraindicated
(known danger--do not use!)
N.B. Regardless of the pregnancy category or the presumed safety of the drug, no drug
should be administered during pregnancy unless it is clearly needed and the
potential benefits outweigh potential harm to the fetus.
29
Examples of drugs contraindicated in pregnancy:
Fluoroquinolones (e.g. ciprofloxacin, ofloxacin): Possibility of joint abnormalities (seen
only in animals).
Sulfonamides (e.g. trimethoprim- sulfamethoxazole): if taken late in pregnancy they may
produce jaundice and possibly brain damage in the newborn.
Tetracycline: Slowed bone growth, permanent yellowing of the teeth, and increased
susceptibility to cavities in the baby and occasionally liver failure in the pregnant
woman.
Angiotensin-converting enzyme (ACE) inhibitors: all through pregnancy may produce
kidney damage in the fetus, decrease amniotic fluid and defects of the face, limbs,
and lungs.
Beta-blockers: bradycardia and low blood sugar level in the fetus and possibly slowed
growth.
Thiazide diuretics: decrease in Na+ & K+ and in the number of platelets in the fetus's
blood & affect growth.
Salicylates, ibuprofen & naproxen: if taken in large doses may produce jaundice, and
occasionally brain damage in the fetus and bleeding problems in the woman during
and after delivery and in the newborn.
If taken late in pregnancy, premature closure of ductus arteriosus, decreased
amniotic fluid & delayed labor may occur.

30
Treatment of common oral conditions
Supportive care:
Management of oral mucosal conditions may require topical and systemic
interventions. Therapy should address patient nutrition and hydration, oral
discomfort, oral hygiene, management of secondary infection, and local control of
the disease process.
I. Herpes Simplex
Clinical description:
Clear, then yellowish, vesicles develop intraorally and extraorally. These vesicles
rupture within hours and form shallow, painful ulcers.
A. Primary Herpetic Gingivostomatitis:
Etiology: A transmissible infection with herpes simplex virus, usually type I or, less
commonly type II. Usually it is self-limiting, with healing in 7 to 10 days.
Rationale for treatment:
-Relieve symptoms, prevent secondary infection, and support general health. Supportive
therapy includes forced fluids, protein, vitamin and mineral food supplements, and
rest.
-Topical steroids should be avoided because they tend to permit spread of the viral infection
o mucous membranes, particularly ocular.
1. Topical antihistaminic
• Diphenhydramine elixir.
2. Systemic antiviral therapy:
• Acyclovir oral capsules may relieve and decrease the duration of symptoms.
3. Systemic antibiotics:
• Penicillin V tablets 500 mg Or Erythromycin tables 250 mg.
They can be used for secondary bacterial infection in susceptible individuals. Do not
use routinely.
4. Analgesic: paracetamol tablets
B. Recurrent (Orofacial) Herpes Simplex:
Etiology: Reactivation of latent virus that resides in the sensory ganglion of the trigeminal
nerve. Precipitating factors include fever, stress, and exposure to sunlight, trauma,
and hormonal alterations.

31
Rationale for treatment:
Treatment should be initiated as early as possible.
1. Sunscreen lotion and gel (OTC)
2. Constant or intermittent application of ice to the area for 90 minutes during the
prodromal phase may result in abortion the lesion.
3. Cocoa butter ointment.
4. Antiviral creams and ointments but are of minimal efficacy.
2. Varicella Zoster (Shingles)
Etiology: Reactivation of latent herpes varicella virus present since an original varicella
infection through chickenpox. Precipitating factors include thermal, inflammatory,
radiologic, or mechanical trauma.
Clinical description:
Usually painful segmental eruption of small vesicles that later rupture to form
punctuate or confluent ulcers.
Rationale for treatment:
1. Acyclovir capsules 200 mg.
2. Valacyclovir HCI caplets 500 mg.
3. Patients older than 60 years are particularly prone to postherpetic neuralgia. In the
absence of specific contraindications, short-term, high-dose corticosteroid may be
given in conjunction with oral acyclovir.
3. Recurrent Aphthous Stomatitis
Etiology:
- An altered local immune response is the predisposing factor. Patients with frequent
recurrences should be screened for diseases as anemia, diabetes mellitus, vitamin
deficiency, inflammatory bowel disease and immunosuppression.
- Precipitating factors include stress, trauma, allergies and endocrine alterations,
dietary components, such as acidic foods and juices, and foods that contain gluten.
Clinical description:
Minor aphthae (canker sore), less than 0.6 cm, small, shallow, painful ulceration
covered by a gray membrane and surrounded by a narrow erythematous halo. They
usually occur on nonkeratinized (moveable) oral mucosa.
Rational for treatment:
Treatment should be initiated as early as possible in the course of lesions.
32
1. Topical steroids:
- Triamcinolone acetonide (Kenalog) in Orabase 0.1%
- Hydrocortisone 1% (Mixing onitments with equal parts of Orabase B paste promotes
adhesion).
N.B.: prolonged use of topical steroids (>2 weeks of continuous use) may result in
mucosal atrophy or secondary candidiasis and may increase the potential for
systemic absorption. It may be necessary to prescribe antifungal therapy with
steroids.
2. System steroids and immunosuppressants:
- Prednisone tablets 5 or 10 mg depending on severity (4 tablets in the morning for 5
days, then decrease by 1 tablet on each successive day).
- Medications such as azathioprine, pentoxifylline, levamisole, colchicine and
dapsone are used in severe, persistent, recurrent aphthous stomatitis, but should not
be routinely used because of the potential for side effects.
4. Candidiasis
Etiology:
- Candida albicans, a yeast like fungus. Candida is an opportunistic organism that
tends to proliferate with the use of broad-spectrum antibiotics, corticosteroids
medicines that reduce salivary output, and cytotoxic agents.
- Conditions that contribute to candidiasis include xerostomia, diabetes mellitus, poor
oral hygiene prosthetic appliances, and suppression of the immune system.
Clinical description:
The disease is characterized by soft, white slightly elevated plaques that usually can
be wiped away, leaving an erythematous area.
Rationale for treatment: To reestablish a normal balance of oral flora and improve oral
hygiene. Medication should be continued for 48 hours after disappearance of
clinical signs to prevent immediate recurrence.
a. Topical antifungal agents:
• Nystatin oral suspension. Or: Nystatin ointment. Or: Nystatin topical powder.
• Or Ketoconazole cream 2%.
b. Systemic antifungal agents: When topical therapy is not practical or is ineffective.
• Antifungal Azoles as Ketoconazole (Nizoral) tablets.
• Or Amphotericin B.
33
5. Cheilitis & Cheilosis
Etiology:
- Fissured lesions in the coroners of the mouth are caused by a mixed infection of the
microorganisms C. albicans, Staphylococcus, and Streptococcus.
- Predisposing factors include local habits, drooling, a decrease in intermaxillary
space, anemia, immunosuppression, and an extension of oral infection.
Clinical description:
The commissures may appear wrinkled, red, fissured, cracked or crusted.
Rationale for treatment: Identification and predisposing factors and elimination of the
secondary infection and inflammation.
1. Nystatin plus traimcinolone acetonide (Mycolog II) ointment.
2. Ketoconazole (Nizoral) cream 2%.
6. Xerostomia
Etiology:
- Acute or chronic reduced salivary flow may result from drug therapy, mechanical
blockage, dehydration, and emotional stress, infection of the salivary glands, local
surgery, avitaminosis, diabetes, anemia, connective tissue diseases, Sjogren's
syndrome, radiation, therapy, and congenital factors (e.g., ectodermal dysplasia).
Clinical description:
The tissues may be dry, pale, or red and atrophic. The tongue may be devoid of
papillae, atrophic, fissured, and inflamed. Multiple carious lesions may be present,
especially at the gingival margin and on exposed root surfaces.
Rational for treatment: Salivary stimulation or replacement therapy to keep mouth moist,
prevention of caries and candidal infection, and palliative relief.
1. Saliva substitutes: Sodium carboxymethyl cellulose 0.5% aqueous solution (OTC).
2. Saliva stimulants:
a. Chewing sugarless gum and sucking sugarless mints are conservative methods to
temporarily stimulate salivary flow in patients.
b. Pilocarpine HCI solution Or tablets (Salagen).
c. Bethanechol (Urecholine).
3. Caries prevention: Stannous fluoride gel 0.4% (Apply to teeth daily for 5 minutes; 5-10
drops in a custom tray. Do not swallow the gel).
4. Treatment for candidiasis may be required along with treatment for dry mouth as
xerostomia provides an excellent environment for overgrowth of C. albicans.
34
7. Oral Erythema Multiforme
Etiology:
- Oral erythema multiforme is believed to be an autoimmune condition. It can occur at
any age.
- Drug reactions to medications such as penicillin and sulfonamides may play a role in
some cases.
- In a few patients who developed oral erythema multiforme, a herpetic infection
occurred immediately before the onset of clinical signs.
Clinical description:
Signs of oral erythema multiforme include "blood-crusted" lips, "targetoid" or
"bull's-eye" skin lesions, and a nonspecific mucosal slough.
Rationale for treatment:
1. Suppressive antiviral therapy may be necessary before initiation of steroid therapy.
- Patients should be questioned carefully about a previous history of recurrent herpetic
infections because of the possible relationship or oral erythema multiforme with
herpes simplex virus.
- Suppressive antiviral therapy:
Acyclovir (Zovirax) capsules. Or Valacyclovir (Valtrex) capsules.
2. Steroid therapy: systemic and local.
8. Teeth Discoloration
Etiology:
- Foods/drinks: Coffee, tea, colas, wines and certain fruits and vegetables (eg apples
and potatoes).
- Smoking or chewing tobacco
- Poor dental hygiene
- Medications:
• The antibiotics tetracycline and doxycycline are known to discolor teeth when
given to children whose teeth are still developing (before the age of 8).
• Mouth rinses and washes containing chlorhexidine .
• Antihistamines , antipsychotic drugs, and antihypertensive medications.
• Head and neck radiation and chemotherapy
• Dental materials: as silver sulfide-containing materials, can cast a gray-black
color to teeth.
35
- Advancing age: the outer layer of enamel gets worn away revealing the natural
yellow color of dentin
- Genetics: Some people have naturally brighter or thicker enamel than others.
- Environment. Excessive fluoride either from environmental sources (naturally high
fluoride levels in water) or from excessive use (fluoride applications, rinses,
toothpaste, and fluoride supplements taken by mouth).
- Trauma. For example, damage from a fall can disturb enamel formation in young
children whose teeth are still developing. Trauma can also cause discoloration to
adult teeth.
Management:
1. Prophylaxis
- Lifestyle changes, eg: quitting smoking & stopping drinking tea.
- Improve dental hygiene by brushing and flossing regularly and cleaning teeth by a
dental hygienist every 6 months.
2. Treatment Options to Whiten Teeth: vary depending on the cause of the
discoloration
- Using proper tooth brushing and flossing techniques
- Avoidance of the foods and beverages that cause stains
- Bondings.
- Veneers
- Using over-the-counter whitening agents
9. Gingival Enlargement
Etiology:
- Drugs as Phenytoin sodium, calcium channel-blocking agents (nifedipine) and
cyclosporine therapy
- Blood dyscrasias and hereditary fibromatosis
Clinical description:
The gingival tissues, especially in the anterior region, are dense, resilient,
insensitive, and enlarged but essentially of normal color.
Rational for treatment: Folic acid and drug serum levels should be determined every 6
months.
36
Treatment:
1. Meticulous plaque control
2. Gingivoplasty when indicated
3. Folic acid oral rinse
4. Chlorexidine gluconate
10. Dentine sensitivity
• Painful symptoms arising from exposed dentine which can arise as a result of
toothbrush trauma or periodontal disease.
Treatment:
1. Fluorides:
sodium fluoride, stannous fluoride and sodium monofluorphosphate. They induce
mineralization within the dental tubules, thus creating a calcific barrier on the dentine
surface.
2. Calcium hydroxide:
It occludes dentinal tubules however it poorly adhere to exposed dentine.
3. Strontium chloride:
It accelerates the rate of calcification thus obliterating dentinal tubules (Sensodyne
toothpaste contains 10% strontium chloride)
4. Formaldehyde:
It precipitates proteins in the dentinal tubules reducing sensitivity.
5. Resins and adhesives:
They seal off the tubules and hence act as a mechanical barrier to external stimuli.
11. Management of Patients Receiving
Antineoplastic Agents & Radiation Therapy
Etiology:
- Cancer chemotherapy and radiation to the head and neck tend to reduce the volume
and alter the character of the salvia.
- The balance of the oral flora is disrupted, allowing overgrowth of opportunistic
organisms (e.g., C. albincans).
- Anticancer therapy damages fast-growing tissues, especially the oral mucosa.
37
Clinical description:
The oral mucosa becomes red and inflamed. The saliva is viscous or absent.
Treatment
1. Alkaline saline (salt/bicarbonate) mouth rinse.
2. Chlorhexidine gluconate mothwash.
3. Caries control (See Xerostomia).
4. Topical antihistaminics: Diphenhydramine (Benadryl) elixir.
5. Nystatin pastilles 200.000 units.
38
Emergencies in dentistry
Although rare, medical emergencies can occur in the dental setting so prompt treatment is
essential.
1. Allergy/Anaphylactic Shock An allergic reaction is the result of an antigen antibody reaction to a substance to
which the patient has been previously sensitized. Histamine and other complex chemicals
are released from body cells causing symptoms in the patient. These symptoms may be
confined to a single organ system or become generalized (anaphylaxis).
• Treatment of acute anaphylactic reaction must be immediate.
• Placed horizontally by appropriate adjustments of dental chair or placing on the
floor.
• If respiratory depression is present, oxygen should be administered or mouth to
mouth respiration performed.
• Adrenaline 0.5 ml of 1:1000 (0.1 mg/ml) solution should be injected intramuscularly
often into the upper arm or thigh (never intravenously).
• Give hydrocortisone sodium succinate, 100mg I.V.
2. Fainting (vaso-vagal syncope) Fainting or syncope results from either the psychologic response to fear, anxiety, stress,
pain, or unpleasant situations or from poor autonomic adjustments to changes in the
patient’s posture. In some cases, syncope may be due to very rapid or slow cardiac
arrhythmias. Syncope accounts for over 50% of reported emergencies in the dental office.
The psychologic reaction causes an abrupt slowing of the heart rate and pooling of
blood in the extremities. Within seconds the patient may complain of a flushed sensation,
followed rapidly by loss of consciousness.
Management:
• Before the patient loses consciousness, the possibility of hypoglycemia should be
born in mind, and a glucose drink may be helpful
• Lay the patient flat with head down. Do not allow the patient to sit up, as they will
frequently faint again. Keep the patient supine for a few minutes.
• Loosen any tight clothing around the neck
➢ Recovery is usually rapid and occasionally the patient may jerk as they regain
consciousness in a manner resembling a fit.
➢ Prolonged unconsciousness should lead to consideration of other causes of collapse.
39
3. Bleeding Management:
1- Pressure using gauze pack Absorbable gelatin sponge (Gelfoam).
2- Dental packing blocks: can be cut to fit and applied to bleeding site.
3- Powder: Apply to bleeding site may be:
Gelfoam with thrombin.
Thrombin: Powder with isotonic saline .
4- Oxidized cellulose (Oxycel) Pad: Cut to appropriate size and apply dry.
5- Tranexamic acid Solution: 100 mg/ml in 10-ml vials; tablets: 500 mg, after surgery 25
mg/kg orally.
6- Oxidized regenerated cellulose (surgical absorbable hemostat): lay over extraction site to
control bleeding.
8- Microfibrillar collagen hemostat: apply topically, it adheres firmly to bleeding surfaces.
9- Collagen hemostat pads apply directly to bleeding surface with pressure.
4. Hypoglycemia The lack of glucose in the neurons of the central nervous system results in immediate
dysfunction, causing the patient to appear confused and restless. Patients may also
complain of a headache or exhibit bizarre behavior. Their skin becomes pale, cool and
clammy, and their heart rate increases. If a source of glucose is not administered
immediately, permanent damage may result.
• If the patient exhibits signs and symptoms of hypoglycemia and he is able to
swallow: give him sugar sweets.
• If the patient is unable to swallow: intravenous dextrose should be administered.
• If a vein cannot be found: give glucagon I.M.
5. Angina Pressure or squeezing in the chest. The pain also can occur in shoulders, arms, neck,
jaw, or back. Angina pain may even feel like indigestion.
Management
Sublingual Glyceryl Trinitrate spray or tablets.
6. Epileptic Seizure Patients may experience a seizure as a result of stopped taking or missed a dose of their
anti-seizure medication or exposure to a triggered or stressful situation. As a seizure
begins, the patient typically loses consciousness and then becomes tonic as the entire
skeletal muscles contract. The patient is apneic, becomes cyanotic, and may bite their
tongue. This is followed by the clonic phase in which muscles contract and relax in waves.
During this phase, these involuntary movements make the patient susceptible to injuries to
40
the head, arms, or legs, and they may become incontinent of urine and stool. A seizure is
followed by a period of drowsiness, confusion and extreme fatigue.
• If the patient is known to be an epileptic it is important for him to continue
medication.
• If the patient has an attack in the dental surgery:
-All appliances should be removed from the mouth as quickly as possible.
-Make no attempt to put anything in the mouth or between the teeth.
-Whether or not dental treatment is continued can only be decided by the operator.
-The drug of choice is the Benzodizaepines (diazepam).
-The ultra-short acting barbiturate, thiopentone, will also cut short an attack.
• Status epilepticus is a dangerous condition and the patient should be taken to
hospital as soon as possible.
7. Adrenal Crisis Patients with primary (Addison's disease) or secondary (exogenous corticosteroid
induced) adrenal insufficiency may be at risk for adrenal crisis during or following
surgical procedures performed in dentistry. Adrenal crisis is a medical emergency that
requires prompt intervention to save the patient's life. Adrenal crisis is a rare event in
dentistry. Four factors appear to be associated with the risk for adrenal crisis: (1)
magnitude of surgery, (2) general anesthesia, (3) health status and stability of the patient,
and (4) degree of pain control.
Manifestations of such crisis: Weakness, pallor, perspiration, tachycardia, weak pulse
&hypotension.
Management
- Nonsurgical dental procedures
- Regimen: No supplementation required.
- Minor oral surgery:
- Few simple extractions, biopsy Minor periodontal surgery.
- Regimen: Target 25 mg hydrocortisone equivalent (5 mg prednisone), day of
surgery
- Major oral surgery - Multiple extractions
- Quadrant periodontal surgery
- Extraction of bony impactions - Osseous surgery
- Osteomy - Bone resections - Cancer surgery
- Surgical procedures involving se of general anesthesia
- Procedures lasting more than 1 hour
- Procedures associated with significant blood loss
Regimen: glucocorticoid target is approximately 50-100 mg/day hydrocortisone equivalent,
day of surgery and at least 1 postoperative day.
41
Evidence Based Medicine (EBM)
It means integrating individual clinical expertise with the best available external clinical
evidence from systematic research.
EBM Combines:
1. your clinical knowledge with
2. your knowledge of your patient, with
3. evidence from the literature
Two types of evidence-based medicine
1. Evidence-based guidelines
The practice of EBM at the organizational or institutional level.
This includes the production of guidelines, policy, and regulations. This approach has also
been called evidence based healthcare.
2. Evidence-based individual decision making practiced by the individual health care
provider.
Why use EBM?
• Improves patient care.
• It helps to avoid legal pitfalls.
• Medical school knowledge quickly becomes dated and/or forgotten
The Five Step EBM Model:
The practice of EBM involves five essential steps:
1- Formulating answerable clinical questions.
2- Finding the best evidence to answer the question.
3- Appraising the evidence.
42
4- Applying the evidence results to the patient.
5- Evaluating performance
Step 1: Formulating answerable clinical questions:
Convert a clinical situation into a searchable, (and hopefully answerable) question.
Good clinical questions should be:
1- Clear
2- Directly focused on the problem
3- Answerable by searching the medical literature.
Build questions with Four Components: PICO (or three PIO):
P: Patient or Problem.
I: Intervention or Exposure of interest
C: Comparison Intervention
O: Specific Clinical Outcome
Example of clinical question:
In children with dental caries will fluoride varnish, as compared to no fluoride varnish,
result in a decreased incidence of caries?
Patient/population/problem children w/ dental caries
Intervention fluoride varnish
Comparison no varnish
Outcome decrease in incidence of caries
Step 2: Finding the best evidence to answer the question:
Effective searches aim to maximize the potential of retrieving relevant articles within the
shortest possible time.
Basic Search Principles:
1- Generate appropriate keywords:
A word list can be generated, based on keywords from the Clinical question. For example,
from the clinical question above, the following keywords could be used for the
search: viral bronchiolitis (patient or problem); corticosteroids: glucocorticoids,
steroids, prednisolone, dexamethasone (intervention); clinical score, hospital stay
(outcomes)
2- Choose an online bibliographic database:
Numerous online databases are available. These include:
- The Cochrane Library databases (www.thecochranelibrary.com),
- MEDLINE (Pubmed: www.pubmed.com; a version of MEDLINE
43
That is freely available on the internet, and is updated regularly)
- EMBASE, and CINAHL.
3- Run the search:
Once the key words and databases have been identified, the next thing is to run the search.
At the basic level, an efficient method is to combine individual words or terms
using ‘AND’ and ‘OR’ If you are combining two terms, AND allows only articles
containing both terms while OR allows articles containing either term.
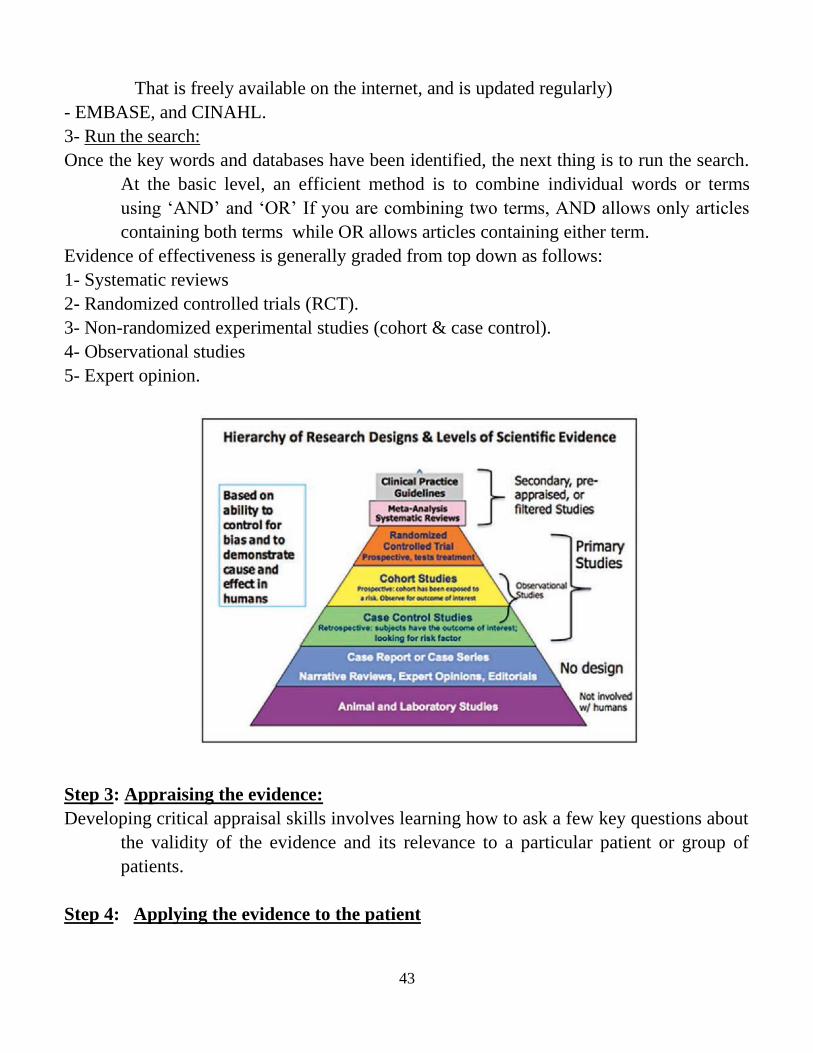
Evidence of effectiveness is generally graded from top down as follows:
1- Systematic reviews
2- Randomized controlled trials (RCT).
3- Non-randomized experimental studies (cohort & case control).
4- Observational studies
5- Expert opinion.
N
Step 3: Appraising the evidence:
Developing critical appraisal skills involves learning how to ask a few key questions about
the validity of the evidence and its relevance to a particular patient or group of
patients.
Step 4: Applying the evidence to the patient

44
After critical appraisal of the evidence, we then have to decide whether that evidence can
be applied to our individual patient or population.
In deciding this we have to take into account:
1- The patient’s own personal values and circumstances.
2- Costs and the availability of that particular treatment in your hospital or practice.
3- The evidence regarding both efficacy and risks should be fully discussed with the patient
or parents, or both, in order to allow them to make an informed decision.
Step 5: Evaluating performance
As we incorporate EBM into routine clinical practice, we need to evaluate our approach at
frequent intervals and to decide whether we need to improve on any of the four
steps discussed above. Also, we need to ask whether we integrate clinical expertise
and patient’s values with the evidence in a way that leads to a rational, acceptable
management strategy that improves the patient care.
45
Prescription Writing Definition:
A prescription is a written order of a physician to a pharmacist with names and doses of
drugs, instructions for preparation and dispensing for the pharmacist and mode of
administration for the patient. Because prescription orders are medico legal
documents, they should be written in ink. It is also an excellent custom, too
infrequently followed, for doctor to keep a copy for the files. This protects the
physician and serves to complete the record of treatment
Parts of a Prescription
a. Superscription
b. Inscription
c. Subscription
d. Signature
Superscription
1- Physician's name, qualification, address and telephone number
2- Patients' name, age and address
3- Date
The symbol R/ (not RX) is an abbreviation for recipe, the Latin for "taken thou". It is likely
to be originated from the symbol of the eye of Horus
Inscription
It is the body of the prescription order and contains the official English name and the
amount of each ingredient. Drugs can be prescribed by their non-proprietary
(generic) names or their proprietary (brand) names. Abbreviations should be
avoided since they are likely to result in errors. The name of each drug is placed on
a separate line directly under the preceding one. The weights and volumes of drugs
should be written in the "Metric System". If there is more than one ingredient, their
order should be ideally as follows:
Basis: is the principal active drug and gives the prescription its chief action
Adjuvant aids or increases the action of the basis.
Corrective modifies or corrects any undesirable effect of the basis or adjuvant. It may be
flavoring, coloring or a sweetening agent.
Vehicle is an inert agent used to distribute the above ingredients. It may serve either as a
solvent or to increase the bulk or both. In the case of a liquid, if it is intended
merely to dilute the active drug, it is called a diluent. In powders, an inert powder
may serve as diluent. The inert substance added to medicine to give it a proper
consistency, as in pills, is known as excipient. In ointments, the soft or greasy
substance in which a more active drug is incorporated is usually called the ointment
base
46
Subscription
It contains directions to the pharmacist. They are written in English but occasionally few
Latin abbreviations are used such as M., ft., etc. In prescription orders for a single
drug this consists of writing the total quantity or number to be dispensed e.g.
"Dispense (or send) 20 tablets". In case of presence of many ingredients, it is
usually either a short sentence such as make a solution or a word such as "Mix"
Transcription & Signature
It consists of directions to the patient written in Arabic regarding the use of the medicines.
The directions should be simple, complete and clear to the patient. They include
instructions as to the amount of the drug to be taken, frequency of the dose, route of
administration, duration of therapy and any special precautions. At the bottom of
the prescription the physician should sign with his registration number which is
especially necessary when any narcotic drug is prescribed.
Narcotic prescription:
Prescribing narcotic drugs e.g. morphine, meperidine, etc. requires a special form that could
be obtained from the Ministry of Health. This form should be filled by a licensed
physician. Narcotic prescription should include the physician's name, address, and
signature, the patient's name, age, address, diagnosis and date. The quantity should
be written in numbers and letters. Narcotic prescription should be written in ink. It
is kept by the pharmacist and is not returned to the patient.
Policy in prescription writing:
After the diagnosis has been made and the prescription ingredients have been decided upon,
the following points should be given consideration in writing a prescription:
Never give a ready-written prescription
Write deliberately and without hesitation
Avoid rewriting a prescription
Do not converse with the patient while writing
Write in clear handwriting
Avoid erasing, crossing out, and tearing up a prescription in the presence of the patient
For conditions that call for limited course of therapy (e.g. most infections) the duration of
therapy should be made clear so that the patient will not stop taking the drug
prematurely.
47
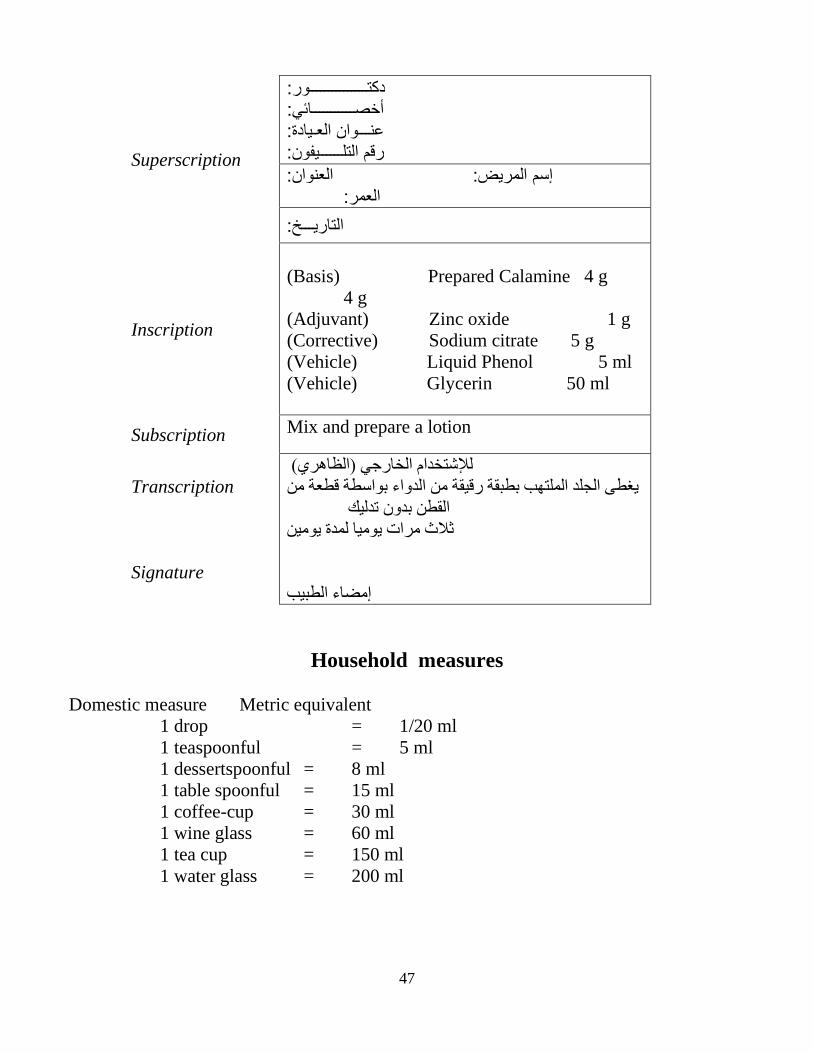
Superscription
دكتـــــــــــــــور: أخصـــــــــــائي: عنـــوان العـيادة: رقم التلــــــيفون:
المريض: العنوان: إسم العمر:
التاريـــخ:
Inscription
(Basis) Prepared Calamine 4 g
4 g
(Adjuvant) Zinc oxide 1 g
(Corrective) Sodium citrate 5 g
(Vehicle) Liquid Phenol 5 ml
(Vehicle) Glycerin 50 ml
Subscription Mix and prepare a lotion
Transcription
Signature
للإشتخدام الخارجي )الظاهري(
يغطى الجلد الملتهب بطبقة رقيقة من الدواء بواسطة قطعة من
القطن بدون تدليك
ثلاث مرات يوميا لمدة يومين
إمضاء الطبيب
Household measures
Domestic measure Metric equivalent
1 drop = 1/20 ml
1 teaspoonful = 5 ml
1 dessertspoonful = 8 ml
1 table spoonful = 15 ml
1 coffee-cup = 30 ml
1 wine glass = 60 ml
1 tea cup = 150 ml
1 water glass = 200 ml
48
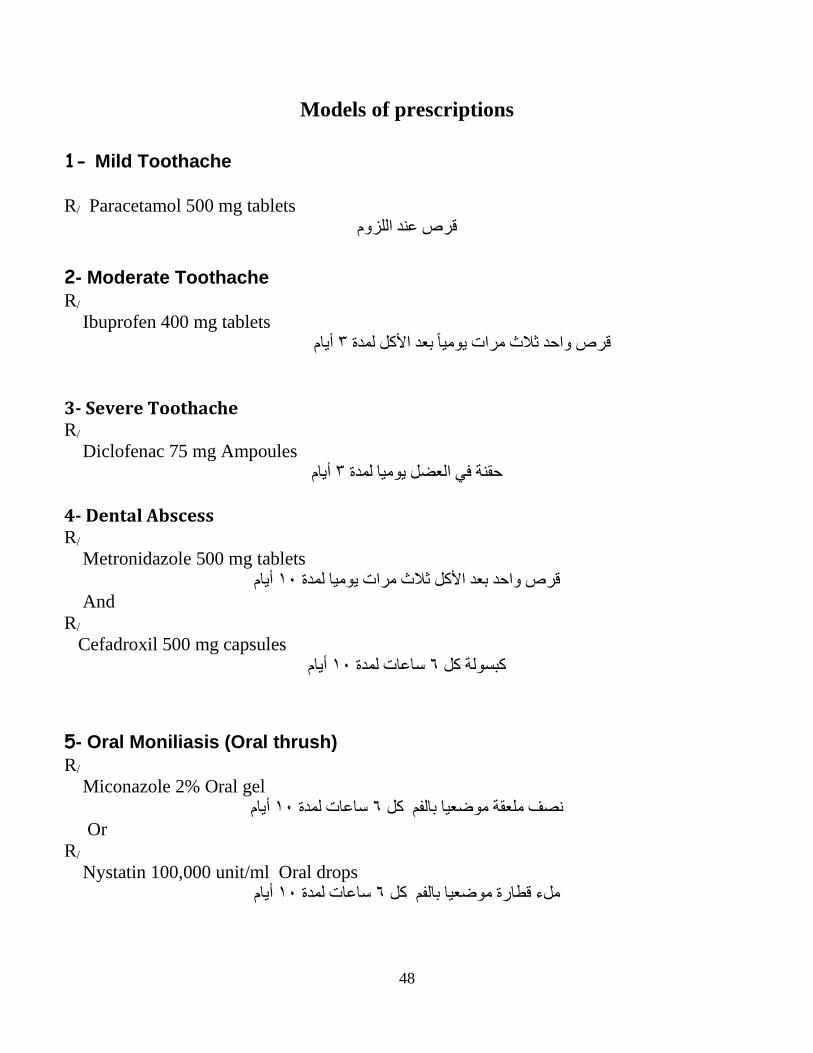
Models of prescriptions
1- Mild Toothache
R/ Paracetamol 500 mg tablets
قرص عند اللزوم
2- Moderate Toothache
R/
Ibuprofen 400 mg tablets
أيام ٣قرص واحد ثلاث مرات يومياً بعد الأكل لمدة
3- Severe Toothache R/
Diclofenac 75 mg Ampoules
أيام ٣حقنة في العضل يوميا لمدة
4- Dental Abscess R/
Metronidazole 500 mg tablets
أيام ١٠قرص واحد بعد الأكل ثلاث مرات يوميا لمدة
And
R/
Cefadroxil 500 mg capsules
أيام ١٠ساعات لمدة ٦كبسولة كل
5- Oral Moniliasis (Oral thrush)
R/
Miconazole 2% Oral gel
أيام ١٠ساعات لمدة ٦نصف ملعقة موضعيا بالفم كل
Or
R/
Nystatin 100,000 unit/ml Oral drops
أيام ١٠ساعات لمدة ٦ملء قطارة موضعيا بالفم كل
49
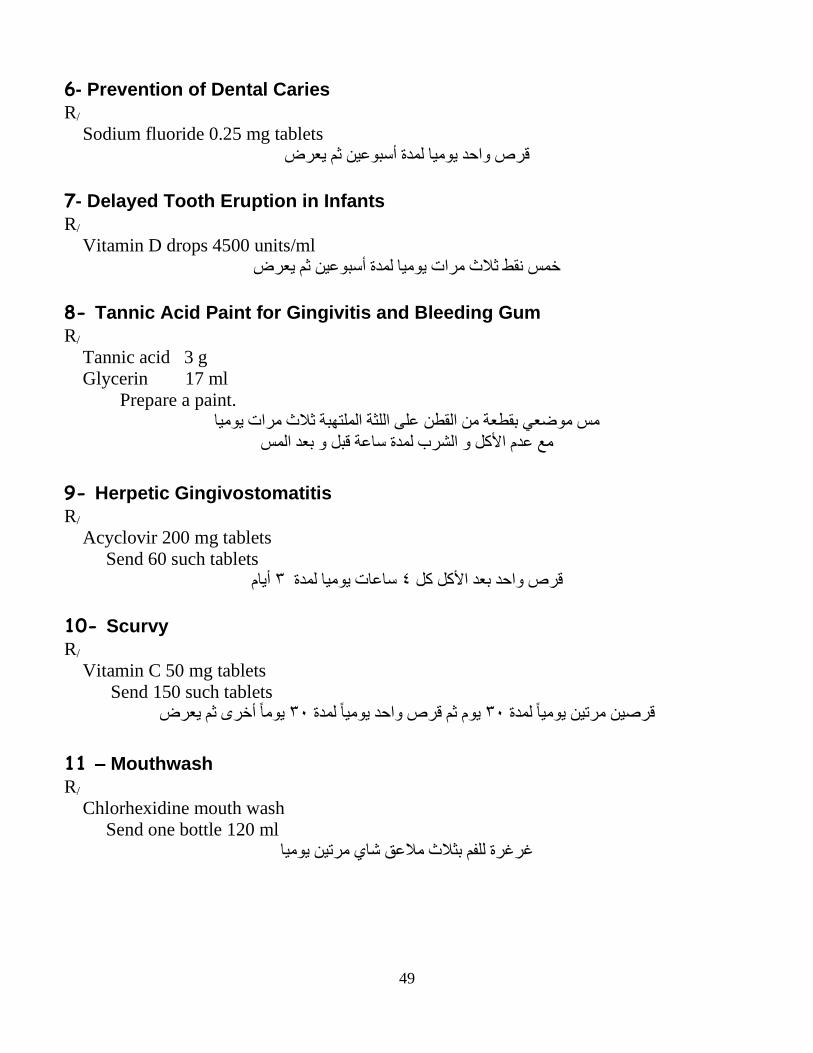
6- Prevention of Dental Caries
R/
Sodium fluoride 0.25 mg tablets
قرص واحد يوميا لمدة أسبوعين ثم يعرض
7- Delayed Tooth Eruption in Infants R/
Vitamin D drops 4500 units/ml
خمس نقط ثلاث مرات يوميا لمدة أسبوعين ثم يعرض
8- Tannic Acid Paint for Gingivitis and Bleeding Gum R/
Tannic acid 3 g
Glycerin 17 ml
Prepare a paint.
على اللثة الملتهبة ثلاث مرات يوميا مس موضعي بقطعة من القطن
مع عدم الأكل و الشرب لمدة ساعة قبل و بعد المس
9- Herpetic Gingivostomatitis
R/
Acyclovir 200 mg tablets
Send 60 such tablets
أيام ٣ساعات يوميا لمدة ٤قرص واحد بعد الأكل كل
10- Scurvy
R/
Vitamin C 50 mg tablets
Send 150 such tablets
يوماً أخرى ثم يعرض ٣٠يوم ثم قرص واحد يومياً لمدة ٣٠قرصين مرتين يومياً لمدة
11 – Mouthwash R/
Chlorhexidine mouth wash
Send one bottle 120 ml
غرغرة للفم بثلاث ملاعق شاي مرتين يوميا