Embed Size (px)
Citation preview

Models for the Study of Whole Systems
Models for Whole Systems Research
Iris R. Bell, MD, PhD, and Mary Koithan, RN, PhD
cally well-established approaches to care across a spec-trum of acute and chronic diseases and complete diag-nostic and therapeutic systems derived fromcomprehensive worldviews of nature that are holisticand vitalistic. The major theme of the present article isthat nonlinear dynamical complex systems and net-work theory provide a coherent conceptual basis andscientific approach that matches the holistic aspect ofwhole systems of CAM. Consequently, complex systemstheory facilitates an understanding of and ability tomove beyond the perplexing difficulties in repro-ducibility of randomized controlled trials (RCTs) onhomeopathy and other whole systems of CAM.
The global and multidimensional worldviews ofwhole systems of CAM differ from the implicitlyreductionistic and materialistic worldview of much ofmainstream medicine as currently practiced, in whichdiagnosis and treatment focus on (a) local body partsin isolation from one another and (b) the molecularmechanisms of local symptom expression (Table 1).As discussed elsewhere in detail,1-4 attempts to per-form reductionistic research, applying the main-stream pharmaceutical model for RCTs (testing thequestion of specific efficacy) to whole systems of CAM(where overall effectiveness is the most appropriatequestion), often produce conflicting and controver-sial results. The mismatch between the simplifieddirect causal model inherent in reductionism5 thatunderlies RCTs and the indirect multifactorial causalmodels inherent in holistic complex systems and net-works6 helps account for the discrepancies (Table 2).
This article summarizes a network and complex systemsscience model for research on whole systems of comple-mentary and alternative medicine (CAM) such as homeopa-thy and traditional Chinese medicine. The holistic conceptsof networks and nonlinear dynamical complex systems arewell matched to the global and interactive perspectives ofwhole systems of CAM, whereas the reductionistic sciencemodel is well matched to the isolated local organ, cell, andmolecular mechanistic perspectives of pharmaceuticallybased biomedicine. Whole systems of CAM are not drugswith specific actions. The diagnostic and therapeuticapproaches of whole systems of CAM produce effects thatinvolve global and patterned shifts across multiple subsys-tems of the person as a whole. For homeopathy, several char-acteristics of complex systems, including the probabilisticnature of attractor patterns, variable sensitivity of complexsystems to initial conditions, and emergent behaviors in theevolution of a system in its full environmental context overtime, could help account for the mixed basic science andcontrolled clinical trial research findings, in contrast with theconsistently positive outcomes of observational studies inthe literature. Application of theories and methods fromcomplex systems and network science can open a new era ofadvances in understanding factors that lead to good versuspoor individual global outcome patterns and to rationaltriage of patients to one type of care over another. The grow-ing reliance on complex systems thinking and systemsbiology for cancer research affords a unique opportunity tobridge between the CAM and conventional medical worldswith some common language and conceptual models.
Keywords: whole systems research; complementary and alter-native medicine; complex systems; global and localpatterns; chaos theory; network science; homeopa-thy; systems biology
Overview: Reductionism Versus Holism in Theory, Practice, and ResearchThe purpose of this article is to provide an introduc-tion to models of complex systems/network theory-driven clinical research in cancer, involving whole sys-tems of complementary and alternative medicine (CAM)such as homeopathy, traditional Chinese medicine(TCM), Ayurveda, and naturopathy. Distinguishingfeatures of whole systems of CAM include their histori-
Networks and Whole Systems Research ModelsNetwork research is a growing area within complexsystems science relevant to the whole systems of CAMview of the whole person as an emergent organism,
DOI: 10.1177/1534735406295293
INTEGRATIVE CANCER THERAPIES 5(4); 2006 pp. 293-307
IRB and MK are in the Departments of Family and CommunityMedicine and Medicine (Program in Integrative Medicine),University of Arizona College of Medicine, Tucson.
Financial disclosure: Dr. Bell acts as a consultant to StandardHomeopathic Co. and Hyland’s, Inc.
Correspondence: Iris R. Bell, MD, PhD, Department of Family andCommunity Medicine, University of Arizona College of Medicine,1450 N. Cherry Ave, PO Box 245052, Tucson, AZ 85719. E-mail:[email protected].
293

arising from interrelationships and interactions amongthe parts. In turn, the person is part of and in ongoinginteraction with the larger environmental context inwhich he or she exists. Network science focuses on thepatterns and strengths of interrelationships and inter-actions between the component parts of a system thathas self-organized into a whole.7,8 Thus, the behaviorsof a given system or network receive greater emphasisin complexity research than do the static structures ofthe parts themselves.7-9 Precisely because of the indivis-ibility of a network (complex system) into its compo-nent parts, the focus of study differs from the focus ofstudy from a reductionistic perspective.
By analogy, researchers cannot understand theorganization of or interactions within the Internet by
studying how a silicon chip is manufactured. Rather,they study the Internet as a whole network.10 In a sys-tems model, networks occur at every level of scalefrom ecological to social and economic to biologicaland biochemical. At the person level, the acupunc-ture meridian and acupoint system from CAM is oneexample of a network. However, this may not beunique to whole systems of CAM. In the conventionalmedical arena, network scientists have uncovered andbegun to map networks of biochemical interactionswithin single cells8 and genetic regulation across thegenome.11
Network models for research highlight patternsof outcomes, with emphasis on interrelationshipsbetween the parts of the whole. For homeopathic
Bell, Koithan
294 INTEGRATIVE CANCER THERAPIES 5(4); 2006
Underlying Worldview
Considerations in the evolving life courseof disease expression
Diagnostic approach to symptoms
Focus of treatment Nature of intervention
Usual outcomes expected
Whole Systems of CAM
Holism, Vitalism
Yes – “diagnoses” related to one anotherin a coherent pattern (stemming froma core or essential endogenousdisturbance that leads to multiplemanifestations, depending on hostsusceptibilities in environmentalcontext)
Symptom patterns are local expressionsof global disturbances in the organism
PatientPackages of care used to address the
individualized imbalances within theperson (organism) level of scale
Improvements in global well-being, energy,and a pattern of multiple biopsycho-social symptoms reflective of the initialimbalance within the organism
Conventional Medicine
Reductionism, Materialism
No – each diagnosis is unrelated to andindependent of other diagnoses(problem list of separate conditionswhose separate treatments mightinteract adversely)
Symptoms are local expressions of localdisturbances in the organ
Disease mechanism in the organSingle purified drug or other modality used
to target the presumed local disturbanceat the organ level of scale
Elimination of chief complaint andassociated symptoms at the local organ,with “side-effects” at other organs distalto the target organ
Table 1. Clinical Differences Between Whole Systems of CAM and Conventional Medicine (Usual Reductionism, NotSystems Biology)
Complex systems/Network theory andresearch models: Evaluate whole system
Reductionistic theory and researchmodels: Evaluate local organ or cell
Whole Systems of CAM Diagnoses andTreatments: Target Is the Person as aWhole Indivisible Organism in His or
Her Environmental Context
Good match
Poor match
Conventional Medicine Diagnoses andDrug Treatments: Target Is the Local
Organ or Cell in Isolation From orControlled for Other Environmental
Factors
Poor match
Good match
Table 2. Matching Clinical Models to Theory and Research Models
CAM = complementary and alternative medicine.
CAM = complementary and alternative medicine.

research, network science is far more likely thanreductionism to match the multidimensional patternsof outcomes described by clinicians.12-15 In homeopa-thy, for example, healing from chronic disease is nota random process. Rather, it is reported to follow ahierarchically self-organized pattern of gradual changeover time in accord with Hering’s Law of Cure. Hering’sLaw states that healing shifts from above downward(head to toes), from inside out (more important toless important organs), and in reverse order of timeof original appearance of a condition or symptom.The homeopathic clinical construct of suppressionassumes but does not articulate a network perspective.That is, homeopaths believe that treatment focusedon preventing expression of local disease in a bodypart, whether a conventional drug or an alternativemedicine treatment, only forces the organismic-leveldisturbances out of one body part and into another,without true cure.
Thus, for a whole system of CAM such as homeopa-thy, if the therapy itself addresses the whole system of theperson, then systems-relevant questions include these:Does the intervention affect network function? If so,how does it differ in pattern of effects from other inter-ventions (perturbations) of the overall system? Thesequeries differ from reductionistic questions such as this:Does the intervention have a specific active ingredientwith a biological mechanism beyond that of placebo?
Clearer directions for research can emerge fromthese considerations. For example, can clinical net-work scientists document evidence for Hering’s Lawof Cure over the person as a whole during homeo-pathic treatment? Do conventional drug and placeboresponses follow Hering’s Law or not? The patterningof changes over the person could provide a theory-driven outcome for controlled research on whole sys-tems of CAM, instead of isolated measurements atsingle points in time.16 The nature of the relevant ques-tions depends on the worldview and theory underlyingthe research.
Nonlinear Dynamical Characteristics of Complex SystemsA complex system is a set of multiple component partsself-organized into an interactive, indivisible whole.17-
19 Within complexity, in addition to network interac-tions, investigators evaluate the nonlinear dynamicsof a system and focus on patterns of change or move-ment of a system over time, for example, attractors.Dynamics introduce time and patterns as major fac-tors in understanding the behavior of a system. Anattractor is a recurrent overall pattern within multi-dimensional phase space toward which the trajectoryof a given system will evolve, without necessarily passingthrough exactly the same place twice (Figure 1).
Models for Whole Systems Research
INTEGRATIVE CANCER THERAPIES 5(4); 2006 295
Figure 1 Attractor patterns, respectively, of low-performing (a) and high-performing (b) business teams, graphed in phase space forinteractional behaviors of inquiry-advocacy versus emotional space.28 Note that each pattern, low-productive (limited ellipse)or high-productive (butterfly), is circumscribed overall, but each system moves continuously, passing through trajectoriescovering similar but not identical specific locations in phase space over time. Reprinted with permission from Elsevier. 28

Leading complexity researchers hypothesize thatcomplex living systems function at the edge of chaos,where the system can exhibit marked sensitivity to ini-tial conditions (the “butterfly effect”).20,21 Small per-turbations in the system can lead to large changes if they occur at critical points in the dynamics of the sys-tem (nonlinearity). Furthermore, small differences inthe state of a given system at the start of a study canlead to progressively more divergent outcomes as acomplex system evolves within its environment overtime (Figure 2).
Thus, the very nature of complex systems is suchthat replicability or reproducibility of patterns is likely,but precise repetition of any specific outcome at anisolated point in time or space is unlikely. It is extremelydifficult to do reproducible reductionistic research ona whole system. A whole system is nonreductionistic(cannot meaningfully study the parts in isolation fromtheir interactions with one another and with theirenvironment) and nonlinear (with outcomes that couldmanifest as either increases or decreases in a givenvariable at a given point in time, depending on multiplefactors)22,23 by nature.
In complexity, the whole is greater than the sum ofthe parts in that the behaviors of the whole are emer-gent, that is, not predicted by understanding thebehaviors of the parts. With emergence, the system’sbehaviors and outcomes evolve over time throughinteractions between the parts and between the overallsystem and its total environment, such that the systemis never in exactly the same place from one moment to
the next. In general, concepts such as self-organization,emergence, self-similarity (fractality) at different levelsof scale (from global to local), nonlinearity (output dis-proportionate to input), and dynamics (processes ofchange) are characteristics of complex systems thatunderlie the empirical and computer simulation meth-ods of complex systems science.
As a result, because of (a) the imprecision of attrac-tor patterns to predict reliably a specific measured out-come, (b) sensitivity of a system’s dynamical evolutionto small differences in initial conditions, and (c) emer-gent behaviors over time, any intervention that targetsand acts at the level of the whole system will not pro-duce predictably repeatable isolated specific effects atan isolated local level. The outcomes in complex sys-tems are probabilistic, not certain. Sometimes, at acurrent moment of observation, the system (or one ofits parts) may be close in trajectory to the point it wasin the previous moment of observation; sometimes, itwill be elsewhere. In short, whole systems of CAM donot act—or even claim to act—with local specificitylike pharmaceutical drugs. Predictably, studies focusedon testing the specific but not the global effects ofwhole systems of CAM reflect theory-mismatcheddesigns.
Thus, the “results,” especially in terms of staticisolated endpoints typical of conventional medicalresearch, sampled at an arbitrary time point in anRCT such as 12 weeks after the start of treatment andat an arbitrary part of the system (one organ or typeof cell), could easily happen to be anywhere along the
Bell, Koithan
296 INTEGRATIVE CANCER THERAPIES 5(4); 2006
Figure 2 Divergence of 2 trajectories of temperature curves over time during meteorologist Edward Lorenz’s computer simulationsbecause of sensitivity to small differences in initial conditions in weather patterns (eg, a chaotic system in which the differ-ence at the start of the 2 curves [time=0] is 0.000127 degrees).121 Reprinted with permission from Blackwell Publishing. 121
trajectory, from very close by to polar opposite pointsin phase space from study to study, even within thesame patient. The point is to zoom out by enough lev-els of scale to be able to assess the big picture, that is,the global or holistic, pattern rather than zoom in tooclose onto one transient point along a moving target.Therefore, if a therapy such as a pharmaceutical drugor even a particular CAM modality (eg, an herb) isintended to target a specific local body part or mech-anism, then it is a reasonable match to employ reduc-tionistic study designs and methods to evaluate theresults. However, if a therapy such as a whole systemof CAM (homeopathy, TCM [acupuncture], Ayurveda,or naturopathy) is used clinically to target the personlevel of scale as a whole system (Figure 3),24 it is a far more rational match to use holistic study designs
including (but not limited to) complex systems modelsand methods (Table 2).
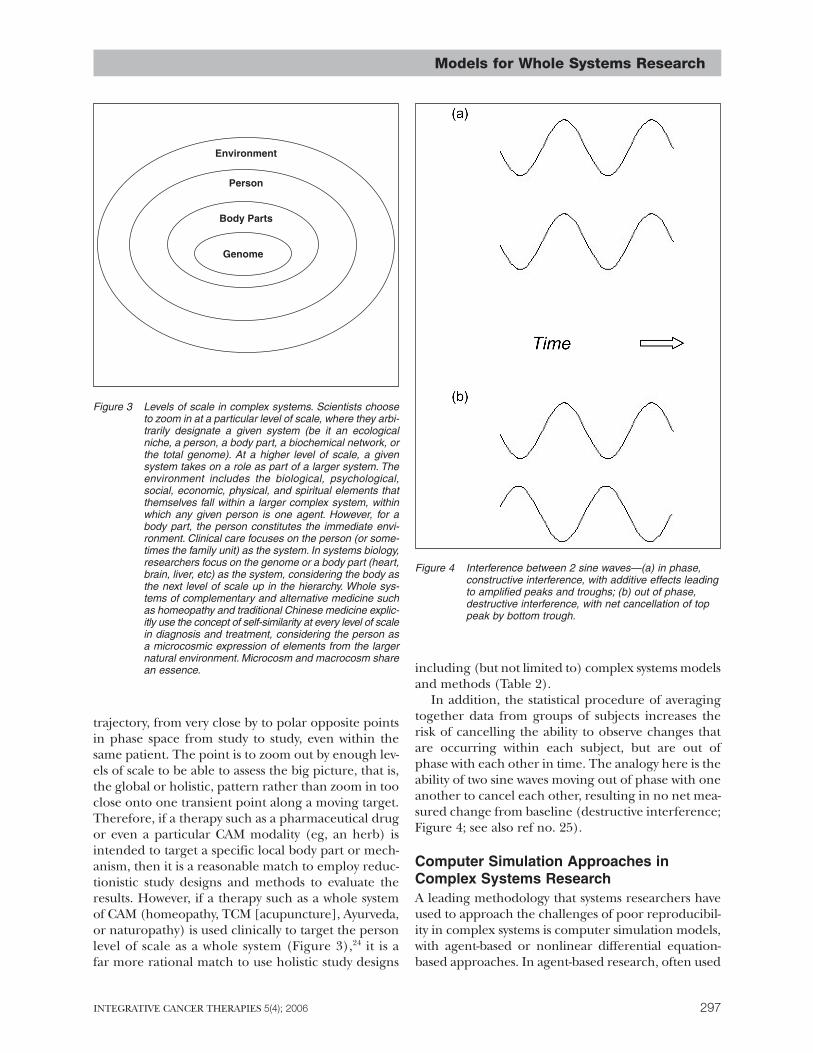
In addition, the statistical procedure of averagingtogether data from groups of subjects increases therisk of cancelling the ability to observe changes thatare occurring within each subject, but are out ofphase with each other in time. The analogy here is theability of two sine waves moving out of phase with oneanother to cancel each other, resulting in no net mea-sured change from baseline (destructive interference;Figure 4; see also ref no. 25).
Computer Simulation Approaches inComplex Systems ResearchA leading methodology that systems researchers haveused to approach the challenges of poor reproducibil-ity in complex systems is computer simulation models,with agent-based or nonlinear differential equation-based approaches. In agent-based research, often used
Models for Whole Systems Research
INTEGRATIVE CANCER THERAPIES 5(4); 2006 297
Person
Environment
Body Parts
Genome
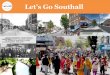
Figure 3 Levels of scale in complex systems. Scientists chooseto zoom in at a particular level of scale, where they arbi-trarily designate a given system (be it an ecologicalniche, a person, a body part, a biochemical network, orthe total genome). At a higher level of scale, a givensystem takes on a role as part of a larger system. Theenvironment includes the biological, psychological,social, economic, physical, and spiritual elements thatthemselves fall within a larger complex system, withinwhich any given person is one agent. However, for abody part, the person constitutes the immediate envi-ronment. Clinical care focuses on the person (or some-times the family unit) as the system. In systems biology,researchers focus on the genome or a body part (heart,brain, liver, etc) as the system, considering the body asthe next level of scale up in the hierarchy. Whole sys-tems of complementary and alternative medicine suchas homeopathy and traditional Chinese medicine explic-itly use the concept of self-similarity at every level of scalein diagnosis and treatment, considering the person asa microcosmic expression of elements from the largernatural environment. Microcosm and macrocosm sharean essence.
Figure 4 Interference between 2 sine waves—(a) in phase,constructive interference, with additive effects leadingto amplified peaks and troughs; (b) out of phase,destructive interference, with net cancellation of toppeak by bottom trough.

in the social sciences, investigators systematically mod-ify the rules by which the local parts (agents) interactwith one another. They then observe and documentglobal outcome scenarios as the whole system evolvesover time.26,27 At the level of scale of the person, agent-based research might be a useful match for studies ofacupuncture, to model differential global outcomesbased on varying the pattern of acupuncture pointschosen and people in the patient’s social environment(both the points and the people—acupuncturist, fam-ily, friends, other health care providers, etc, are poten-tially agents, albeit at different levels of scale), relativedegrees of stimulation or sedation for the points andtypes of interactional patterns with the people (rules),and the presumptive meridian pathways for interactionsbetween them across the person as a whole (network).
In addition to agent-based research, Figures 1a (low-functioning team dynamics) and 1b (high-functioningteam dynamics) give an example of nonlinear differ-ential equation-based modeling of human interactionsin the context of business teams, based on models fromthe field of fluid dynamics28,29 (see further descriptionin the section below on translating phenotypes withinwhole systems of CAM). Low-functioning teams appearstuck in adverse dynamical attractor patterns of repeti-tive, restrictive trajectories called limit cycles and pointattractors (Figure 1a). However, several complexity andchaos science researchers have noticed a generalizabil-ity and even “archetypal” quality across many differentdisciplines for what are termed the Lorenz equa-tions28,30 (see Figure 1b—leading dynamically to abutterfly-appearing attractor pattern, named after themeteorologist who developed them to model changesin weather). Lorenz equations appear to characterizesystems with healthier dynamics, including flexibility inthe face of environmental challenges, creativity, capac-ity to innovate, positivity, and balanced interactionsbetween self and others.28,29,31 Small changes in initialconditions within the Lorenz equations can lead tovariations of the essential pattern but, nonetheless, arecognizable “essence.”29,32
The relevance of the Lorenz equations33 at differ-ent levels of scale, that is, both human interactions (liv-ing systems) and fluid dynamics, may be especiallyrelevant for improving understanding of the interac-tion between the person and homeopathy. In home-opathy, at the person level, clinicians strive to perceivethe essence or global pattern of the person, as expressedoverall and, concomitantly, in his or her body parts.For treatment, the homeopath then chooses the singleremedy with an essence most closely matched (simi-lar) to the patient’s own core pattern. At the remedylevel of scale (a remedy derives from an animal, min-eral, or plant environmental source), preparation ofhomeopathic remedies involves serial dilution and
succussion of liquids. Succussion is vigorous shaking,with induced turbulence of water solvent in which theoriginal source material has been dissolved, leading tomeasurable and evolving changes in the physicalchemistry properties of the solvent molecule network.34-36
Notably, water is also a hub molecule in the network ofbodily biochemistry8,37 and therefore a potential media-tor of the dynamical interactions between patient andremedy as a system.38 As in any whole system of CAM,of course, the practitioner and the rest of the person’ssocial network also are part of the complex systemscontext for the treatment. Milgrom has developed thenotion of a complex system in homeopathy to encom-pass the patient, the practitioner (a component of thesocial environment), and the remedy (a component ofthe natural environment).39,40
More than 25 years ago, Vithoulkas41 defined healthin homeopathy in terms of behaviors that researcherstoday might view as consistent with a Lorenz attractorpattern,28,29,31 that is, freedom from physical and emo-tional pain, freedom from selfishness, increased adapt-ability, and creativity. Synthesizing contemporarysystems science approaches such as Lorenz modelswith homeopathic theories of health could enableresearchers to model and test for the evolution of heal-ing during successful homeopathic care. Ultimately,improved predictions of which individuals will and willnot benefit globally (though not necessarily in specificlocal outcomes) from homeopathic treatment underparticular contextual conditions could result.
Systems Biology in Medicine and CancerResearch: A Bridge to Complexity Modelsfor Whole Systems of CAMThe concepts of complex systems are familiar in cancerresearch.42-45 Mainstream researchers already use com-plex systems approaches to improve delivery of cancercare and refine prognostic predictions for individualpatients, as well as to understand the basic biology of thedisease. Systems biology is the integrative interdiscipli-nary academic field that studies the relationships andinteractions between gene and protein networks in a liv-ing organism toward understanding the behavior of theorganism itself as a whole. Systems biology researchersrely on both multivariate empirical investigations andmathematical computer simulation modeling studies toadvance their field. Genes and proteins interact in com-plex ways, and it is not useful to attempt reductionisticstudy of a single gene in isolation from its context, forthe study of how, when, and why a patient expresses thephenotype of a particular cancer or other disease.46,47
Systems-oriented researchers seek therapies that arehighly individualized and capable of addressing themultifactorial processes, including polygenic influences
Bell, Koithan
298 INTEGRATIVE CANCER THERAPIES 5(4); 2006

that result in disease development and progression suchas specific cancers.47-49
At the same time, complex systems concepts arebeginning to lead to empirical studies revealing genome-wide gene regulatory networks that control the dynam-ical patterns of cell differentiation. That is, systemsresearch is beginning to show evidence for integratedcontrollers of the body’s complex networks with thou-sands of “separate” parts.11 Other network researchershave shown interactive influences as well betweenglobal and local levels of organization.9 Self-similarityover different levels of scale, that is, fractality, is a fea-ture of complex systems.
Notably, homeopathy researchers such as Hylandand Lewith50 have previously postulated that the abilityof a single homeopathic constitutional remedy to mod-ulate global and multiple outcomes derives from itstherapeutic influence on function of the controllerhubs for the person as a whole. If so, then the “mecha-nism” by which homeopathic remedies act would holdparticular relevance to systems biology research andcould provide empirical probes for studying genome-wide gene regulatory networks. Some homeopathsreport significant clinical remissions and cures of theprimary cancer disease process,51 in addition to pallia-tion of adjunctive symptoms from the disease and con-ventional cancer treatments such as radiotherapy andchemotherapy.52-54
Mainstream researchers at the cutting edge of con-ventional medicine have explicitly recognized thatcancer biology is complex and multifactorial. Systemsbiologists are grappling with the reality that differentpeople can exhibit the same phenotype but arrive atthe same “destination” via multiple different, multifac-torial pathways. In turn, when trying to use drugs asthe interventional tool in cancer, systems biologistsknow that people differ in their ability to benefit fromand metabolize any given agent. The goal of moderngenomics/proteomics research is individualized treat-ment. To determine the most effective and best toler-ated drug for a specific patient, they first need to knowthe many variants of the phenotype and the multipledifferent pathways to the same apparent end-result.
Dynamical Translation of PhenotypesWithin Whole Systems of CAMSimilarly, for whole systems of CAM, the phenotype isthe nonlinear dynamical global pattern or essence ofthe system as a whole,29 labeled, for example, in home-opathy as the constitutional remedy type (eg, Sulphur,Stramonium, Lachesis, etc) or in Chinese medicine, asthe root diagnosis (eg, Liver Qi Rising or Kidney YangDeficiency). At the same time, people can be healthyor unhealthy variants of their essential constitutions.
Individual persons differ in their phenotypic expres-sion of the essential pattern at any given time becauseof small differences in initial conditions and interac-tions between the person and a multitude of endoge-nous and exogenous factors. Disease represents aconvergence of the person as a system into an unhealthyattractor pattern23,28,55 (see Figure 1a). The homeo-pathic and TCM interventions then serve as smallcourse corrections at critical points in the trajectoriesof the person as a network-system, shifting the systemback into an optimal dynamical expression of the person’sessential and unique nature, that is, a healthy variantof the self (see Figure 1b).
In complex systems research, Dabby32 with musicalcomposers and Losada28,29 with business teams havesuccessfully shown precedents for defining the dynam-ical global essence of a given system and demonstratingdivergent trajectories (outcomes) based on varying ini-tial starting conditions and/or interactional patterns.Frederickson and Losada31 have further outlined adynamical systems model for healthy individual humanflourishing, which might apply to the system-wide, bio-psycho-social-spiritual transformation that a subset ofpatients treated with homeopathy and acupuncturereport. In a conceptual sense, when coordinated mod-ulation of global network processes is the goal, wholesystems of CAM may be better suited than pharmaceu-tical drugs to serve as potential therapies in complexsystemic diseases.
Evidence in Homeopathy and AcupunctureConsistent With the Nonlinear DynamicalComplex Systems ModelThe findings from a large British study of homeo-pathically prepared dust mite, prescribed isopathi-cally in asthmatics (all patients received the sameremedy in 30 c potencies) provide evidence for the large-scale effects of homeopathically prepared remedieson nonlinear dynamics. That is, as seen in Figure 5 forthe 3 main outcome measures, lung function, globalasthma ratings, and mood ratings, the verum groupfluctuated in an oscillatory pattern over time, endingup in the same place as the placebo group at the endof the 16-week study. However, the placebo groupshowed a flatter set of curves, without the same kindof oscillatory change during the study. The data leadto seemingly paradoxical conclusions, from a reduc-tionistic perspective, that homeopathically prepareddust mite is therapeutically not different fromplacebo, but that the homeopathically prepared dustmite is not a placebo (ie, it is biologically active, notinert). From a complex systems perspective, however,the verum remedy was actively altering the trajectoryof the system as a whole. The data showed that the
Models for Whole Systems Research
INTEGRATIVE CANCER THERAPIES 5(4); 2006 299

verum had destabilized the disease dynamics of thesubjects in the active treatment group from theirusual attractor patterns, whereas placebo had not.
What occurs over time with homeopathy in the pat-tern of large-scale outcomes if the verum treatment is therapeutically helpful? Bell et al have such anexample with an objective electrophysiological bio-marker assessed at initial remedy exposure and after 3months and 6 months of individualized classical home-opathic treatment in patients with fibromyalgia. Aspublished previously, only patients who subsequentlyhad both an exceptionally good global health changeand local tender point pain lessening to treatment hadshown an initial difference from placebo in prefrontalelectroencephalographic cordance patterns for thealpha frequency (8-12 Hz), averaged over 16 acute snifftest exposures/sessions to their remedy under double-blind conditions.56 Cordance is an algorithmically
derived measure of the ratio between relative andabsolute alpha power.
However, the direction of the cordance findingchanged over the course of time. Unpublished follow-up analyses revealed a shifting of cordance findingsover the 6-month study, consistent with the evolutionof divergent nonlinear electrophysiological changes inthe therapeutically responsive patients as nonlineardynamical complex systems. That is, Figure 6 showsthat the exceptional responders diverged for cordancedifference scores (mean treatment solution minusmean remedy-free solvent control sniff effects) fromverum clinical nonresponders and placebo patients atall 3 time points. However, the direction of the differ-ence scores in the verum responders transitioned overthe 6 months of the study, from strongly negative tostrongly positive.
Again, the data are suggestive of a biphasic patternin which true verum differed from placebo effectsover time. As in many other homeopathic studies, thedirection of the initial finding did not replicate 3 or 6months later. However, verum acting therapeutically
Bell, Koithan
300 INTEGRATIVE CANCER THERAPIES 5(4); 2006
Figure 5 Oscillatory response of outcome measures in asth-matics (mean of individual patient means during morn-ing [am] assessments) to therapeutically ineffective,homeopathically prepared dust mite remedy.50,122 PEF =Peak Expiratory Flow; VAS = Visual Analogue ScaleScore. Reprinted with Permission from BMJ PublishingGroup, Ltd. 122
Intermediate Excellent
Clinical Responder Group
−1.20
−0.80
−0.40
0.00
0.40
0.80
Poor
Initial Session 3-Month Session6-Month Session
Mea
n D
iff. S
core
for
Sni
ff C
orda
nce
(Tx-
Con
trol
Sol
utio
ns)
Figure 6 Divergence and shifts in quantitative electroencephalo-graphic cordance magnitude and direction over time intreatment for excellent verum responders versus allothers in study (on verum or placebo without excellentclinical response). Subjects were designated as excel-lent, intermediate, or poor responders as follows: excel-lent = top 1/3 of the sample (n = 62) for both changesin global health and reduction in tender point pain onexamination; intermediate = top 1/3 for either globalhealth OR pain, but not both; poor = bottom 2/3 of thesample for both global health and pain.123

altered the overall dynamics of the response patternover time at the level of the central nervous system ina way that therapeutically ineffective remedy andplacebo did not. This study demonstrates an impor-tant methodological consideration based on systemsbiology and complex systems empirical research.11
That is, it is necessary to identify the real-world phe-notype of interest (exceptionally good clinical respon-ders to verum remedy, as defined by both global andlocal improvements in this case), and then look formultifactorial mediators and the evolution of emer-gent patterns of change over time that contribute tothe eventual phenotypic expression.
The animal and other research literature onhomeopathy contains additional evidence in supportof a nonlinear complex systems interpretation. Forexample, as a crude example of sensitivity to initialconditions, Bertani et al57 used the same mixture ofhomeopathically prepared minerals at the same potencyin a rodent model of carageenan-induced paw edema.In the latter study, they varied only the time of admin-istration of the remedy in 3 different groups of rats:60 minutes before, during, or 30 minutes after theinduction of the injury. The direction of the resultsdepended on the timing of administration of the rem-edy. In fact, the results ended up completely oppositein the before-injury (increased approximately 15%over controls) and after-injury (decreased approxi-mately 14% over controls) groups. The simultaneousinjury/remedy timing led to only a small increase inedema over control (approximately 4%). The implica-tions of the findings are that the responses to homeo-pathic remedies are nonlinear. The direction ofresponses to homeopathic remedies is dependent uponthe state of the host as a system at the time of inter-vention and time point of observation.
As the interventions of homeopathy, TCM, andAyurveda target the person level of organization, com-plex systems theory predicts that outcomes will not beconsistently reproducible between studies with thesame designs and similar procedures (procedures cannever be absolutely identical because of variations inmultiple interactive factors, including participants,their social contacts [family, friends, business associ-ates], research personnel, time of year, environmentalfluctuations, ambient laboratory conditions). Clinically,homeopaths themselves often report that the sameremedy at the same potency in the same individualpatient at 2 different points in time has vastly differenteffects (eg, ranging from none to major improvementsto minor improvements or even worsening).
In summary, nonlinear dynamical complex systemtheory predicts the situation documented through-out the homeopathic research and clinical literatureas well as in acupuncture. In view of the fact that
effectiveness studies capture the more holistic, real-world contextual conditions of treatment far betterthan RCTs, observational trials, especially well-designedobservational trials,58,59 would merit greater weightthan RCTs as evidence of presence or absence of ther-apeutic benefit for a given whole system of CAM.Observational data overwhelmingly demonstrate favor-able outcomes for homeopathic treatment,60-63 in con-trast with the much more mixed results for RCTs andcontrolled basic science studies that focus on parts ofthe whole system. Cohort- or case-controlled observa-tional studies that document both global and local out-comes and include assessments of dynamics are mostlikely to provide optimal tests of homeopathy.
Furthermore, acupuncture researchers using mixedqualitative and quantitative methods have demon-strated the phenomenon of emergence. That is,patients report both global and multidimensionalchanges over the course of treatment.64-69 They caneven forget to mention the original chief complaintbecause of their enthusiastic description of multipleother changes that they had not originally anticipated.Attempts at individualization of symptoms for prospec-tive designs have been unable to capture emergenceduring treatment. For example, Paterson’s group in the United Kingdom developed and validated apatient-centered outcome scale, the MYMOP.70 Thisscale asks patients to name and rate their respectiveleading symptoms in their own words. Although theMYMOP is sensitive to change in the original chiefcomplaint compared with baseline, open-ended inter-views with patients revealed that the MYMOP com-pletely missed a wide range of additional global andlocal changes, that is, emergents, that the patientsexperienced in the course of the acupuncture treat-ment. Efforts to modify the MYMOP to capture emer-gent changes are under way.65,67,71
Skeptics will undoubtedly assert that the aboveargument is only an excuse for the failures of repli-cation in homeopathic or acupuncture clinical RCTand basic science research. Perhaps it is. On theother hand, within Jonas’s evidence house construct,72,73
the complex systems argument opens the door to amore inclusive perspective in which both holisticand reductionistic models can belong. That is, for agiven therapy, depending on its clinical target interms of level of scale (person or part), theory-dri-ven testable hypotheses and research using the best-matched methods for the intervention are appropriateand feasible.
With complex systems models, it is possible toexamine outcomes with far greater face and constructvalidity than otherwise possible from a reductionisticor even patient-centered/humanistic point of view. In other words, measuring endpoint change in a
Models for Whole Systems Research
INTEGRATIVE CANCER THERAPIES 5(4); 2006 301

bio-marker, a chief complaint rating, or even quality-of-life score in isolation cannot capture the holistic(global well-being, energy, organism-wide multiplesymptom pattern) and dynamical patterns of nonlin-ear changes that the interaction of a complex systemof CAM, the complex system of a person as a livingorganism, and the environmental context (the person’sbiological, chemical, physical, and social world) would beexpected to generate in the course of treatment.
Rather, evaluating patterns of systemwide changesover time series of repeated measure data (within bothmultiple variables by themselves, at various levels ofscale, and across the interrelationships between multi-ple variables within the person overall), assessing emer-gent changes not present at baseline, and studyingmultiple mediating factors contributing to markedlygood versus poor outcomes in individual patients inlarge observational studies have much greater poten-tial than reductionistic designs to advance whole sys-tems CAM research. Naturalistic studies based onwell-established qualitative methods also have thecapacity to provide fuller pictures of patient outcomesover time than do RCTs and related reductionisticapproaches.74
Theory-Driven Study Design Strategies in a Complex Systems ModelFinally, another strategy within the nonlinear dynam-ical complex systems model is to work out the multi-ple parameters of a given experimental protocol asa system, in advance of performing the actual con-trolled study. Some experimental systems will gener-ate more repeatable results than others. For instance,Frei et al published a series of studies on childrenwith attention deficit disorder treated with individu-alized homeopathic remedies in 1M(1 part per 1,000)potencies. First, they did open-label treatment todetermine the length of time needed for most of thechildren to show improvement on homeopathy, if itoccurred.75 They also defined “improvement” as atleast a 50% reduction in behavioral disturbance rat-ings by the parents. As is typical in clinical cases, thepoint in time at which this reduction occurred var-ied from patient to patient. Furthermore, they refinedthe clinical diagnostic procedures for determiningthe correct prescription,76 for example, from 21% to54% for the first remedy chosen and from 68% to84% for the fifth remedy chosen. Methodologically,this fundamental research is long overdue in theclinical field of homeopathy,77 as homeopaths oftenmiss the correct remedy initially, thereby renderingan unknown subset of the verum remedies in the“active” group therapeutically inactive within a typi-cal short-term double-blind RCT.
Notably, the study design assessed the amount of timefrom the start of treatment to threshold improvement,rather than averaging improvement scores at a fixedtime point. This tactic permitted the investigators to cap-ture the individualized time course of change (therebyavoiding the problems with patients being out of phasewith one another in their change patterns and can-celling the ability to document any net change—seeabove). The investigators also tested for the possibil-ity of a washout period that might enable a crossoverdesign for the LM potencies.
For their actual double-blind RCT, the Frei groupchose to enroll only patients who had already shownnot only good clinical responsivity to the remedy inLM potencies but also a susceptibility to relapse witha 3-week washout period off remedy. Their eventualmodified RCT study showed that homeopathy wassuperior to placebo.78 A separate study by anotherresearch group who launched immediately into a con-ventionally designed double-blind pilot RCT withoutpretesting the parameters of their experimental pro-tocol or the treatment responsivity of their subjectsfailed to show a difference between verum individual-ized treatment and placebo.79 Given the clinical reali-ties that homeopaths often do not find the “right” ormost appropriate remedy for the case in their firstchoice and that the time course of responses variesindividually, any RCT study that has not pretested thestudy subjects’ actual capacity for responsivity to the rem-edy and documented the individualized time courseof follow-up runs the risk of Type II error. The metho-dological strategy used by Frei avoided potential con-founds that homeopathic researchers otherwise haveencountered.80 In addition to disease-related staticendpoints, measurement of nonlinear dynamical pat-terns of behavior and physiology, such as documentedin previous human behavior studies,28,31,81 would alsolower the risk of Type II error. These ideas are not theonly possible approach but point the way toward ahybrid methodology in which valid RCT designs maybe possible for whole systems of CAM, but only whenthe systems issues have been accommodated (and viceversa).
To approach the issue of predefining the experi-mental system from a nonlinear dynamical perspec-tive, the systems model predicts that an experimentalprotocol (itself a system) whose dynamics are morestable (less chaotic) will generate results that aremore reproducible than will a less stable experimen-tal system. It is possible to characterize and quantifythe dynamics of some systems in terms of their sensi-tivity to small differences in initial conditions, using aparameter known as the largest Lyapunov exponent.A testable hypothesis is that an experimental systemwhose dynamics are less sensitive to initial conditions
Bell, Koithan
302 INTEGRATIVE CANCER THERAPIES 5(4); 2006

(eg, with a more negative Lyapunov exponent) shouldgenerate more repeatable results from trial to trial orstudy to study than a different experimental systemwhose dynamics are more sensitive to initial conditions(eg, with a more positive Lyapunov exponent).
Skeptics might argue that the need to define theexperimental system with so much pretesting pre-cludes the ability to answer the broad public healthquestion that a typical RCT answers—as to whether ornot homeopathy is a desirable treatment for a particu-lar conventional medical diagnosis in general. In thiscriticism, the skeptics would be correct. Awareness ofthese issues, however, could lead to asking the clini-cally relevant, patient-centered question of individual-ization—that is, how can researchers identify andtriage people for whom a given system of care willprobably be very helpful so that these individualsreceive the intervention sooner rather than later ornot at all?82 Conversely, how can people for whom theintervention will probably not be helpful be triagedelsewhere with less loss of time and money, as well aslower risk?
Summary and ImplicationsThe methodological implications of the complex sys-tems perspective are that well-designed observationaltrials, which permit assessment of the patient in hisor her full, real-world environmental context, are thetype of clinical research that better matches the holis-tic worldview of complex systems theory than doRCTs. In the conventional health field, it has beenbehavioral rather than biomedical scientists whohave already recognized the need for multilevel ormultiscale analysis of outcomes.81,83-86 Inclusion ofpatient-provider relationship measures, quality-of-lifemeasures, individualized symptom variables, or evenglobal outcomes, when used in isolation from theoverall systemic patterns of outcomes in time andspace, is part of patient-centered research. However,patient-centered selection of variables does not byitself move whole systems of CAM research studiesinto a complex systems and network theory–drivenmodel.
Appropriate outcome measures will be those cap-turing both global changes and patterns of multiplelocal changes across the person in terms of diseasedand healthy network interactions and system dynam-ics.23,28,29,31,55,87,88 Plotting changes in attractor patternsin phase space using sets of nonlinear differentialequations,28,29,31,32 computing descriptive measures ofshifts in systemic complexity,89-91 and adapting othertypes of pattern analysis from systems biology88,92,93
will provide a starting place for assessing quantitativeoutcomes within a complexity science research model.
It will also be important to compare the ability of
nonlinear methods with conventional multivariate sta-tistical techniques such as latent variable/path analysismodeling and cluster analysis94,95 to describe theprocesses and outcomes of whole systems of CAM.Moreover, as several leading CAM researchers havecommented, qualitative methods also provide essen-tial tools74,96 with which to characterize the scopeand nuances of changes at the whole person level oforganization.4,74,97-101
What whole systems of CAM add to the discussionconceptually is a focus on a higher order level of scalejust above that of biological systems, that is, theperson as an indivisible network-system, in the con-text of his or her biopsychosocial environment.50,102-107
The clinical interventions of CAM offer practical, cur-rently available tools for modulating the presumptiveintegrated controllers of the body’s complex net-works, long before conventional medicine will havethe personalized drugs that it now seeks to developthrough systems biology research. As such, the synthe-sis of whole systems of CAM and systems biology tech-nologies may be a bridge leading to truly integrativemedical research.
A skeptic of CAM could argue that invoking com-plexity theory is merely providing a sophisticated“excuse” for why CAM therapies sometimes do not per-form as well as drugs or better than placebo in ran-domized placebo-controlled double-blind efficacy trialswith targeted endpoints. On the contrary, the scientificevidence is that living organisms are complex nonlin-ear dynamical systems by nature.91 Consequently, it islogical to predict that conventional drugs, which aredeveloped to perform well in reductionistic causal sys-tems, might not perform as well as whole systems ofCAM in effectiveness trials.
Effectiveness designs involve the real-world com-plexity of indirect causality and interactions betweenmultiple interventions, multiple providers, the patientand his or her biopsychosocial environment, especiallyin terms of the full patterns of multidimensional out-comes and nonlinear dynamical processes that occurin a person as a whole system over time. The clinicalliterature is already providing initial evidence in sup-port of the latter perspective. Data indicate greatersafety (“side effects” are part of the complete pictureof outcomes from a complex systems perspective) aswell as sometimes shorter acute illnesses and lowercosts for certain CAM therapies, including homeopa-thy, compared with conventional drugs in noncancerconditions.60,61,63,108-110
Finally, it is beyond the scope of this article to dis-cuss the macro-entanglement model for CAM clinicalresearch, which has received extensive coverage else-where103,111-117 Nonetheless, it is important to acknowl-edge that entanglement is an emergent phenomenon
Models for Whole Systems Research
INTEGRATIVE CANCER THERAPIES 5(4); 2006 303

in the behavior of closed systems in quantum mechan-ics. However, it is possible, but not essential, to invokemacro-entanglement concepts to apply the complexsystems thinking outlined in the present article. Thus,although entanglement may be a valid and at leastindirectly testable hypothesis to explain the findingsand methodological limitations of some RCT designs,the current argument can stand on its own as a direc-tion for new research programs more compatiblethan typical RCT designs with the theory and clinicalpractice of whole systems of CAM.
ConclusionsDespite the political pressures to evaluate CAMthrough mainstream reductionistic medical science,118-
120 complex systems/network theories offer a more rel-evant epistemological framework for scientificallybased research on whole systems of CAM than do main-stream reductionistic medical models (Table 2). At thesame time, complex systems and network science are apotential meeting place for CAM and conventionalmedicine researchers to find common ground. Cancerresearch is the mainstream field where the 2 worlds con-verge conceptually. Challenging and ground-breakingadvances in understanding the nature of disease anddeveloping expanded tools for health care in chronicillness such as cancer could result. In the least, complexsystems and network science offers the possibility ofevaluating whole systems of CAM where they claim tohave their strong suit, that is, improving the person’sfunction as a whole by optimizing the ability of theparts to play their healthiest roles possible in relation-ship to one another. Depending on the nature of thequestion that needs to be answered, one or the otheror both models for research (complexity or reduction-ism) may be appropriate.72,73
In conclusion, Bell et al previously proposed thathomeopathy is the therapeutics for the dynamics ofthe person as a whole complex system.16 Hyland et alfurther suggested that homeopathy changes pheno-typic expression by modulating the controller hubs ofthe body as a network.50,103 The complexity/networkmodel, taken together with the body of empirical lit-erature on whole systems of CAM, especially home-opathy and acupuncture, points the way to a potentialproductive resolution of the current impasse betweenCAM and conventional researchers on how to moveforward toward the “truth” about the nature of thebasic and preclinical effects and the clinical effective-ness of whole systems of CAM.
AcknowledgmentsThis study was supported in part by grants fromNIH/NCCAM (K24 AT000057, R21 AT000388-01A2,
T32 AT01287), Samueli Institute for InformationBiology, and the Lotte and John Hecht MemorialFoundation.
Bell, Koithan
304
References1. Walach H, Jonas WB. Homeopathy. In: Lewith G, Jonas WB,
Walach H, eds. Clinical Research in Complementary Therapies.Edinburgh: Churchill Livingstone; 2002:229-246.
2. Walach H. The efficacy paradox in randomized controlled tri-als of CAM and elsewhere: beware of the placebo trap. J AlternComplement Med. 2001;7(3):213-218.
3. Walach H. Entangled—and tied in knots! Practical conse-quences of an entanglement model for homeopathic researchand practice [Review]. Homeopathy: J Faculty Homeopathy.2005;94(2):96-99.
4. Verhoef MJ, Lewith G, Ritenbaugh C, Boon H, Fleishman S,Leis A. Complementary and alternative medicine whole sys-tems research: beyond identification of inadequacies of theRCT. Complement Ther Med. 2005;13(3):206-212.
5. Bar-Yam Y. Reductionism. Available at: http://necsi.org/guide/concepts/reductionism.html. Accessed August 31, 2006.
6. Bar-Yam Y. Emergence. Available at: http://necsi.org/guide/concepts/emergence.html. Accessed August 31, 2006.
7. Barabasi AL. Linked. How Everything Is Connected to EverythingElse and What It Means for Business, Science, and Everyday Life.Cambridge, MA: Plume; 2003.
8. Barabasi AL, Bonabeau E. Scale-free networks. Sci Am.2003;288(5):60-69.
9. Vasquez A, Dobrin R, Sergi D, Eckmann JP, Oltvai ZN,Barabasi AL. The topological relationship between the large-scale attributes and local interaction patterns of complex net-works. Proc Natl Acad Sci U S A. 2004;101(52):17940-17945.
10. The ICSI Center for Internet Research. Available at:http://www.icir.org/ In. Accessed September 2, 2006.
11. Huang S, Eichler G, Bar-Yam Y, Ingber EE. Cell fates as high-dimensional attractor states of a complex gene regulatorynetwork. Phys Rev Lett. 2005;94(12)128701.
12. Oberbaum M, Singer SR, Vithoulkas G. The colour of thehomeopathic improvement: the multidimensional nature ofthe response to homeopathic therapy. Homeopathy. 2005;94(3):196-199.
13. Bell IR, Koithan M, Gorman MM, Baldwin CM. Homeopathicpractitioner views of changes in patients undergoing consti-tutional treatment for chronic disease. J Altern ComplementMed. 2003;9(1):39-50.
14. Schulman D. The unexpected outcomes of acupuncture: casereports in support of refocusing research designs. J AlternComplement Med. 2004;10(5):785-789.
15. Gould A, MacPherson H. Patient perspectives on outcomesafter treatment with acupuncture. J Altern Complement Med.2001;7:261-268.
16. Bell IR, Baldwin CM, Schwartz GE. Translating a nonlinearsystems theory model for homeopathy into empirical tests.Altern Ther Health Med. 2002;8(3):58-66.
17. Bar-Yam Y. Dynamics of Complex Systems. Reading, MA: PerseusBooks; 1997.
18. Bar-Yam Y, Epstein IR. Response of complex networks to stim-uli. Proc Natl Acad Sci U S A. 2004;101(13):4341-4345.
19. Bar-Yam Y. Introducing Complex Systems. Cambridge, MA: NewEngland Complex Systems Institute; 2001.
20. Langton CG. Life at the edge of chaos. In: Langton CG,Taylor JD, Farmer D, Rasmussen S, eds. Artificial Life II. SantaFe Institute Studies in the Sciences of Complexity, vol. X. RedwoodCity, CA: Addison-Wesley; 1991:41-91.
INTEGRATIVE CANCER THERAPIES 5(4); 2006

Models for Whole Systems Research
21. Waldrop MM. Complexity. The Emerging Science at the Edge ofOrder and Chaos. New York: Touchstone; 1992.
22. Calabrese EJ. Toxicological awakenings: the rebirth of hormesisas a central pillar of toxicology [Review]. Toxicol Appl Pharmacol.2005;204(1):1-8.
23. Costa M, Goldberger AL, Peng CK. Multiscale entropy analy-sis of complex physiologic time series. Phys Rev Lett. 2002;89:068102:1-4.
24. Bar-Yam Y. Scale. Available at: http://necsi.org/guide/con-cepts/scale.html. Accessed August 31, 2006.
25. Russell DA. Superposition of waves in acoustics and vibrationanimations. Available at: http://www.kettering.edu/~dru-sell/Demos/superposition/superposition.html. Accessed August31, 2006.
26. Anon. Welcome to the Swarm Development Group Wiki.Available at: http://www.swarm.org/wiki/ Main_Page. AccessedSeptember 2, 2006.
27. Terano T, Kita H, Toshiyuki K, Arai K, Dequchi H. Agent-BasedSimulation: From Modeling Methodologies to Real-World Applications:Post Proceedings of the Third International Workshop on Agent-BasedApproaches. Series on Agent Based Social Systems. New York:Springer; 2005.
28. Losada M. The complex dynamics of high performanceteams. Math Comp Model. 1999;30:179-192.
29. Losada M, Heaphy E. The role of positivity and connectivityin the performance of business teams: a nonlinear dynamicsmodel. Am Behav Sci. 2004;47(6):740-765.
30. Thompson JMT, Stewart HH. A tutorial glossary of geometricdynamics. Int J Bifurcation Chaos. 1993;3(2):223-239.
31. Fredrickson BL, Losada MF. Positive affect and the complexdynamics of human flourishing. Am Psychol. 2005;60(7):678-686.
32. Dabby DS. Musical variations from a chaotic mapping. Chaos.1996;6:95-107.
33. Anon. The Lorenz Equations. Available at: http://www.geom.uiuc.edu/java/Lorenz/. Accessed September 6, 2006.
34. Roy R, Tiller W, Bell IR, Hoover MR. The structure of liquidwater: novel insights from materials research and potential rel-evance to homeopathy. Mat Res Innovat. 2005;9(4):557-608.
35. Elia V, Niccoli M. Thermodynamics of extremely dilutedaqueous solutions. Ann N Y Acad Sci. 1999;879:241-248.
36. Elia V, Niccoli M. New physico-chemical properties of extremelydiluted aqueous solutions. J Therm Anal Calorimetr. 2004;75:815-836.
37. Chaplin M. Water cluster structure. Available at: http://www.martin.chaplin.btinternet.co.uk/abstrct.html. AccessedSeptember 6, 2006.
38. Bell IR. The homeopathic universe: disease and healing asmanifestations of consciousness. Shift: At the Frontiers ofConsciousness. 2006;March-May(10):22-26.
39. Milgrom LR. patient-practitioner-remedy (PPR) entangle-ment Part 4. Toward classification and unification of the dif-ferent entanglement models for homeopathy. Homeopathy: J Faculty Homeopathy. 2004;93(1):34-42.
40. Milgrom LR. Patient-practitioner-remedy (PPR) entangle-ment. Part 5. Can homeopathic remedy reactions be out-comes of PPR entanglement? [Review]. Homeopathy: J FacultyHomeopathy. 2004;93(2):94-98.
41. Vithoulkas G. The Science of Homeopathy. New York: GroveWeidenfeld; 1980.
42. Waliszewski P, Molski M, Konarski J. On the holistic approachin cellular and cancer biology: nonlinearity, complexity, andquasi-determinism of the dynamic cellular network. J SurgOncol. 1998;68(2):70-78.
43. Sittig DF. Potential impact of advanced clinical informationtechnology on cancer care in 2015. Cancer Causes Control. 2006;17(6):813-820.
INTEGRATIVE CANCER THERAPIES 5(4); 2006
44. Jones AS, Taktak AG, Helliwell TR, et al. An artificial neuralnetwork improves prediction of observed survival in patientswith laryngeal squamous carcinoma. Eur Arch Otorhinolaryngol.2006;263(6):541-547.
45. Liu ET, Kuznetsov VA, Miller LD. In the pursuit of complex-ity: systems medicine in cancer biology. Cancer Cell. 2006;9(4):245-247.
46. Williams RW. Expression genetics and the phenotype revolution.Mamm Genome. 2006;17(6):496-502.
47. Hornberg JJ, Bruggeman FJ, Westerhoff HV, Lankelma J.Cancer: a systems biology disease. Biosystems. 2006;83(2-3):81-90.
48. Rew DA. Tumour biology, chaos, and non-linear dynamics.Eur J Surg Oncol. 1999;25:86-89.
49. Belair J, Glass L, an der Heiden U, Milton J. Dynamical disease:mathematical analysis of human illness. Chaos. 1995;5:1-215.
50. Hyland ME, Lewith GT. Oscillatory effects in a homeopathicclinical trial: an explanation using complexity theory, andimplications for clinical practice. Homeopathy. 2002;91(3):145-149.
51. Ramakrishnan AU, Coulter CR. A Homeopathic Approach toCancer. St. Louis, MO: Quality Medical; 2001.
52. Thompson EA, Reillly D. The homeopathic approach tosymptom control in the cancer patient: a prospective obser-vational study. Palliat Med. 2002;16(3):227-233.
53. Oberbaum M, Yaniv I, Ben-Gal Y, et al. A randomized, con-trolled clinical trial of the homeopathic medication TRAUMEELS in the treatment of chemotherapy-induced stomatitis inchildren undergoing stem cell transplantation. Cancer. 2001;92(3):684-690.
54. Jacobs J, Herman P, Heron K, Olsen S, Vaughters L.Homeopathy for menopausal symptoms in breast cancer sur-vivors: a preliminary randomized controlled trial. J AlternComplement Med. 2005;11(1):21-27.
55. Lipsitz LA, Goldberger AL. Loss of ‘complexity’ and aging.Potential applications of fractals and chaos theory to senes-cence. JAMA. 1992;267:1806-1809.
56. Bell IR, Lewis DAI, Schwartz GE, et al. Electroencephalographiccordance patterns distinguish exceptional clinical responderswith fibromyalgia to individualized homeopathic medicines. J Altern Complement Med. 2004;10(2):285-299.
57. Bertani S, Lussignoli S, Andrioli G, Bellavite P, Conforti A. Dualeffects of a homeopathic mineral complex on carrageenan-induced oedema in rats. Br Homoeopath J. 1999;88(3):101-105.
58. Concato J, Shah N, Horwitz RI. Randomized, controlled trials,observational studies, and the hierarchy of research designs. N Engl J Med. 2000;342(25):1887-1892.
59. Concato J. Observational versus experimental studies: what’sthe evidence for a hierarchy? NeuroRx. 2004;1(3):341-347.
60. Witt C, Keil T, Selim D, et al. Outcome and costs of homoeo-pathic and conventional treatment strategies: a comparativecohort study in patients with chronic disorders. ComplementTher Med. 2005;13(2):79-86.
61. van Wassenhoven M, Ives G. An observational study of patientsreceiving homeopathic treatment. Homeopathy. 2004;93(1):3-11.
62. Sevar R. Audit of outcome in 829 consecutive patients treatedwith homeopathic medicines. Br Homoeopath J. 2000;89(4):178-187.
63. Riley D, Fischer M, Singh B, Haidvogl M, Heger M.Homeopathy and conventional medicine: an outcomes studycomparing effectiveness in a primary care setting. J AlternComplement Med. 2001;7(2):149-159.
64. Goldstein MS, Glik D. Use of and satisfaction with homeopathyin a patient population. Altern Ther Health Med. 1998;4(2):60-65.
65. Paterson C, Britten N. Acupuncture for people with chronicillness: combining qualitative and quantitative outcome assess-ment. J Altern Complement Med. 2003;9(5):671-681.
305

Bell, Koithan
66. Paterson C, Britten N. Acupuncture as a complex intervention:a holistic model. J Altern Complement Med. 2004;10(5):791-801.
67. Paterson C, Dieppe P. Characteristic and incidental (placebo)effects in complex interventions such as acupuncture. BMJ.2005;330(7501):1202-1205.
68. Paterson C. Measuring changes in self-concept: a qualitative eval-uation of outcome questionnaires in people having acupuncturefor their chronic health problems. BMC Complement Altern Med.2006;6(1):7.
69. Paterson C, Ewings P, Brazier JE, Britten N. Treating dyspepsiawith acupuncture and homeopathy: reflections on a pilot studyby researchers, practitioners and participants. Complement TherMed. 2003;11(2):78-84.
70. Paterson C. Measuring outcome in primary care: a patient-generated measure, MYMOP, compared to the SF-36 healthsurvey. Br Med J. 1996;312:1016-1020.
71. Paterson C, Britten N. Acupuncture for people with chronicillness: combining qualitative and quantitative outcome assess-ment. J Altern Complement Med. 2003;9(5):671-681.
72. Jonas WB. The evidence house: how to build an inclusive basefor complementary medicine. West J Med. 2001;175(2):79-80.
73. Jonas WB. Building an evidence house: challenges and solu-tions to research in complementary and alternative medicine.Forsch Komplementarmed Klass Naturheilkd. 2005;12:159-167.
74. Lincoln YS, Guba EG. Naturalistic Inquiry. Beverly Hills, CA:Sage; 1985.
75. Frei H, Thurneysen A. Treatment for hyperactive children:homeopathy and methylphenidate compared in a family set-ting. Br Homoeopath J. 2001;90(4):183-188.
76. Frei H, von Ammon K, Thurneysen A. Treatment of hyperactivechildren: increased efficiency through modifications of homeo-pathic diagnostic procedure. Homeopathy. 2006;95(3):163-170.
77. Bell IR. Evidence-based homeopathy: empirical questionsand methodological considerations for homeopathic clinicalresearch. Am J Homeopath Med. 2003;96(1):17-31.
78. Frei H, Everts R, von Ammon K, et al. Homeopathic treat-ment of children with attention deficit hyperactivity disorder:a randomised, double blind, placebo controlled crossovertrial. Eur J Pediatr. 2005; [Epub ahead of print].
79. Jacobs J, Williams AL, Girard C, Njike, VY, Katz D. Homeopathyfor attention-deficit/hyperactivity disorder: a pilot random-ized controlled trial. J Altern Complement Med. 2005;11(5):799-806.
80. Kron M, English JM, Gaus W. Guidelines on methodology ofclinical research in homeopathy. In: Ernst E, Hahn EG, eds.Homeopathy: A Critical Appraisal. Oxford, UK: Butterworth-Heinemann; 1998:9-47.
81. Mandell AJ, Selz KA. Nonlinear dynamical patterns as per-sonality theory for neurobiology and psychiatry. Psychiatry.1995;58:371-390.
82. Turk DC. The potential of treatment matching for subgroups ofpatients with chronic pain: lumping versus splitting [Review].Clin J Pain. 2005;21(1):44-55.
83. Anderson NB. Levels of analysis in health science. A frameworkfor integrating sociobehavioral and biomedical research. Ann NY Acad Sci. 1998;840:563-576.
84. Cacioppo JT, Berntson GG, Sheridan JF, McClintock MK.Multilevel integrative analysis of human behavior: social neu-roscience and the complementing nature of social and biolog-ical approaches. Psychol Bull. 2000;126(6):829-843.
85. Schwartz GE, Russek L. The challenge of one medicine: the-ories of health and eight world hypotheses. Advances: J Mind-Body Health. 1997;13(3):7-23.
86. Schwartz GE. A systems analysis of psychobiology and behaviortherapy. Implications for behavioral medicine. PsychotherPsychosom. 1981;36:159-184.
306
87. Goldberger AL. Non-linear dynamics for clinicians: chaos theory,fractals, and complexity at the bedside. Lancet. 1996;347:1312-1314.
88. Yang ACC, Hseu SS, Yien HW, Goldberger AL, Peng CK.Linguistic analysis of the human heartbeat using frequency andrank order statistics. Phys Rev Lett. 2003;90:108103.
89. Woyshville MJ, Lackamp JM, Eisengart JA, Gilliland JA. On themeaning and measurement of affective instability: clues fromchaos theory. [erratum appears in Biol Psychiatry. 1999 Apr15;45(8): following 1081]. Biol Psychiatry. 1999;45(3):261-269.
90. Woyshville MJ, Calabrese JR. Quantification of occipital EEGchanges in Alzheimer’s disease utilizing a new metric: thefractal dimension. Biol Psychiatry. 1994;35(6):381-387.
91. Coffey DS. Self-organization, complexity, and chaos: the newbiology for medicine. Nature Med. 1998;4(8):882-885.
92. Yang ACC, Peng C-K, Yien HW, Goldberger AL. Informationcategorization approach to literary authorship disputes. PhysicaA. 2003;329:473-483.
93. Peng CK, Henry IC, Mietus JE, et al. Heart rate dynamics dur-ing three forms of meditation. Int J Cardiol. 2004;95(1):19-27.
94. Tabachnick BG, Fidell LS. Using Multivariate Statistics. 4th ed.Boston: Allyn and Bacon; 2001.
95. Katz MH. Multivariable analysis: a primer for readers of med-ical research. Ann Intern Med. 2003;138:644-650.
96. Averill JB. Matrix analysis as a complementary analytic strategyin qualitative inquiry. Qual Health Res. 2002;12(6):855-866.
97. Ritenbaugh C, Verhoef M, Fleishman S, Boon H, Leis A. Wholesystems research: a discipline for studying complementary andalternative medicine. Altern Ther Health Med. 2003;9(4):32-36.
98. Verhoef M, Lewith G, Ritenbaugh C, Thomas K, Boon H,Fonnebo V. Whole systems research: moving forward. FocusAltern Complement Ther. 2004;9(2):87-90.
99. Verhoef MJ, Casebeer AL, Hilsden RJ. Assessing efficacy ofcomplementary medicine: adding qualitative research meth-ods to the “Gold Standard.” J Altern Complement Med. 2002;8(3):275-281.
100. Bell IR, Caspi O, Schwartz GE, et al. Integrative medicine andsystemic outcomes research: issues in the emergence of a newmodel for primary health care. Arch Intern Med. 2002;162(2):133-140.
101. Broom A. Using qualitative interviews in CAM research: a guideto study design, data collection and data analysis. ComplementTher Med. 2005;13(1):65-73.
102. Milgrom LR. The sound of two hands clapping: could home-opathy work locally and non-locally? [Review]. Homeopathy: J Faculty Homeopathy. 2005;94(2):100-104.
103. Hyland M. Extended network generalized entanglementtheory: therapeutic mechanisms, empirical predictions, andinvestigations. J Altern Complement Med. 2003;9(6):919-936.
104. Bellavite P, Signorini A. The Emerging Science of Homeopathy.Complexity, Biodynamics, and Nanopharmacology. 2nd ed. Berkeley,CA: North Atlantic Books; 2002.
105. Bellavite P. Complexity science and homeopathy: a syn-thetic overview. Homeopathy: J Faculty Homeopathy. 2003;92(4):203-212.
106. Milgrom LR. Vitalism, complexity, and the concept of spin.Homeopathy: J Faculty Homeopathy. 2002;91(1):26-31.
107. Walach H, Jonas WB, Ives J, Van Wijk R, Weingartner O.Research on homeopathy: state of the art. J Altern ComplementMed. 2005;11(5):813-829.
108. Frenkel M, Hermoni D. Effects of homeopathic interventionon medication consumption in atopic and allergic disorders.Altern Ther Health Med. 2002;8(1):76-79.
109. Witt CM, Luedtke R, Baur R, Willich SN. Homeopathic med-ical practice: long-term results of a cohort study with 3981patients. BMC Public Health. 2005;5(1):115 epub.
INTEGRATIVE CANCER THERAPIES 5(4); 2006

Models for Whole Systems Research
110. Maxion-Bergemann S, Wolf M, Bornhoft G, Matthiessen PF,Wolf U. Complementary and alternative medicine costs—asystematic literature review. Forsch Komplementarmed. 2006;13(Suppl 2):42-45.
111. Walach H. Entanglement model of homeopathy as an exampleof generalised entanglement predicted by weak quantumtheory. Forschende Komplementarmedizin/Res Complement Med. 2003;10(4):192-200.
112. Milgrom LR. Patient-practitioner-remedy (PPR) entangle-ment. Part 3. Refining the quantum metaphor for homeopa-thy. Homeopathy: J Faculty Homeopathy. 2003;92(3):152-160.
113. Milgrom LR. Patient-practitioner-remedy (PPR) entanglementPart 5. Can homeopathic remedy reactions be outcomes ofPPR entanglement? Homeopathy: J Faculty Homeopathy. 2004;93(2):94-98.
114. Hyland ME. Does a form of ‘entanglement’ between peopleexplain healing? An examination of hypotheses and method-ology. Complement Ther Med. 2004;12(4):198-208.
115. Walach H. Entangled—and tied in knots! Practical conse-quences of an entanglement model for homeopathic researchand practice homeopathy. J Faculty Homeopathy. 2005;94(2):96-99.
116. Lewith GT, Brien S, Hyland ME. Presentiment or entangle-ment? An alternative explanation for apparent entanglementin provings [Review]. Homeopathy: J Faculty Homeopathy. 2005;94(2):92-95.
INTEGRATIVE CANCER THERAPIES 5(4); 2006
117. Walach H. Generalized entanglement: a new theoreticalmodel for understanding the effects of complementary andalternative medicine. J Altern Complement Med. 2005;11(3):549-559.
118. National Center for Complementary and Alternative MedicineFive-Year Strategic Plan. Available at: http://nccam.nih.gov/about/plans/2005/index.htm. Accessed: September 5, 2006.
119. Angell M, Kassirer JP. Alternative medicine—the risks ofuntested and unregulated remedies. N Engl J Med. 1998;339(12):839-841.
120. Lewith G, Verhoef M, Koithan M, Zick SM. Developing CAMresearch capacity for complementary medicine. Evidence BasedComplement Altern Med. 2006;3(2):283-289.
121. Stewart I. Does God Play Dice? The Mathematics of Chaos. Oxford,UK: Blackwell; 1990.
122. Lewith GT, Watkins AD, Hyland ME, et al. Use of ultramolec-ular potencies of allergen to treat asthmatic people allergic tohouse dust mite: double blind randomised controlled clinicaltrial. BMJ. 2002;324(7336):520-523.
123. Bell IR, Lewis DAI, Brooks AJ, et al. Individual differences inresponse to randomly-assigned active individualized homeo-pathic and placebo treatment in fibromyalgia: implications ofa double-blind optional crossover design. J Altern ComplementMed. 2004;10(2):269-283.
307