-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
1/27
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
2/27
Introduction The primary goal is to determine the optimal bed
allocation and decrease
the number of refused admissions.
The major problem in planning the day to day operations in a
hospital is thevariable length of stay of a patient.
If this variability is disregarded a unrealistic picture of the
reality will
emerge.
A model just based on the average numbers is not capable of
describing thecomplexity of the patient flow at the hospital. This
is also known as the flawof averages.
This case is about the inflow of cardiac patients into a
hospital.
This particular patient inflow goes through 3 stages :
1) FCA (first cardiac aid)
2) CCU (coronary care unit)
3) NC (normal care unit)
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
3/27
What is the problem?
In most of the hospitals the CCU works at a 95% capacity, as a
result it
frequently occurs that the CCU has insufficient capacity, as the
unit is full.
Consequently the number of refused admissions is significant and
numerouspatients are turned away to other hospitals.
An admission guarantee to all the patients getting into the
emergency
department is one of their main goal, so they cant keep on
refusing patients.
In case of a heart attack, the sooner someone gets into the
emergency room thebetter the chance of his survival. This period is
referred to as the GOLDENHOUR
This study applies a queuing model to analyze congestion in the
emergencycare unit.
With this model the number of beds and equipment is determined
at differentservice levels.
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
4/27
Structural model
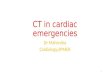
The first phase of this study is about constructing a flowchart
of the patientflow.
The primary flow of a heart patient is :
The different departments are defined as followed:
FCA (first cardiac aid) a hospital unit intended to provide
quick diagnosis andinitiation of treatment.
CCU (coronary care unit) a hospital unit specially equipped to
provideintensive care to heart patients with severe or chronic
heart disease.
NC (normal care) hospital unit equipped to give non-intensive
care to theheart patients.
Enters at
FCA
Stays at
CCU
Goes out
to NC
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
5/27
The secondary flow accounts for the direct entrance into the
CCU,and returns back after treatment bypassing the NC.
Here the patients are admitted for immediate intensive care.
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
6/27
Data Analysis
Arrivals Total number of arrivals in 2003 2838
The average number of patients arriving per day 7.78
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
7/27
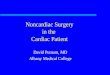
The FCA is characterized by time-varying arrivals during the
day
with arrival pattern over 24-hour period. 14%, 55% and 31% of
all patients arrive in the intervals 00.00-
08.00, 08.00-16.00 and 16.00-24.00.
The secondary patient flow is also unscheduled and modeled as
a
Poisson process with parameter
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
8/27
Routings
There is an alarming
amount of refusedadmissions.
Its not uncommon and soorganization of emergencycare is a hot
topic for
hospital professionals
Length of Stay (LOS) distributions
The real LOS is generally not equal to the LOS indicated by
hospital professionals the difference of which is caused
bycongestion or chain effects.
A certain part of the total LOS consists of additional time
which is around 20-30% of total LOS.
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
9/27
First Cardiac Aid (FCA) For 2401 (85%) of all arrivals the LOS
was registered. The
ALOS at the FCA is 6.4 hours and patients never stay longerthan
24 hours. The median is 5 hours and the CV equals 0.7.
Coronary Care Unit (CCU)
For primary patient flow ALOS is 67 hours, median 48hours and CV
0.99.
For secondary patient flow ALOS is 18 hours, median 5 and
CV 2.6.
About 80% of all patients leave within 12 hours and 80%have
prolonged stay. Paretos 80/20 principle applicable
here emphasizing on 20% that matters.
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
10/27
Normal Clinical Ward (NC)
ALOS at the ward is 164
hours, median 113 hours, andCV is 1.07.
Group with LOS smaller than10 days has 81% of thepatients and
consumes 47%of resources while group with
remaining 19% consumes53% of resources.
These numbers cannot be seen as constants as the processes have
largely variable LOS.
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
11/27
Impact of variation on capacity requirements
To demonstrate the effects we assume Poisson arrivals,
exponentialservice times and an infinite number of beds.
The queuing system under investigation is referred to as M\M\
in
Kendalls notation.
The following parameters describe the queuing system:
= average arrival rate
= average length of stay
B(t) = number of patients in the system at time t or number of
beds
occupied at time t
Following shows the relation between the expected number of
patients in the system, EB(t), and the average length of stay
()
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
12/27
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
13/27
Multiple State Analysis
The probability distribution of the number of beds occupied
at
the FCA is calculated with the use of a M\M\-model.
The average arrival rate ( = 7.78) is assumed to be constant
overthe day. The ALOS () equals 6.4/24 = 0.27 days. Thus,
theexpected number of beds occupied is 2.1.
The 24-hour period is divided in three intervals of each
eighthours.
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
14/27
The expected number of beds occupied increases from 2.1 to
3.4
(+ 62%). Flexible staffing levels are a possible answer to
this
strong variation in workload.
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
15/27
Modeling the Emergency Cardiac Care Chain
In the previous section we assumed an infinite number ofbeds. In
this section capacity is limited.
Phenomena of blocking and economies of scale are
introduced. Both blocking (e.g. refused admissions) andeconomies
of scale are important features of health care
processes.
An important model from queuing theory is the Erlang Lossmodel
or M\M\c\c in Kendalls notation.
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
16/27
In this model customers.
Patients arrive according to a Poisson process with
intensity (including refused)= lambda The LOS of arriving
patients (independent and
exponentially distributed ) =.
The number of beds = c.
The fraction of patients which is blocked and sent away to other
hospitalsin the long run (Pc) can be calculated with the Erlang
Loss
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
17/27
The occupancy rate is related to the real demand and LOS ()
and
can be defined as,
the product is known as the workload of the system.
In general the unit size varies between 6 and approximately
60
beds. The target occupancy rate 85%.
In order to demonstrate the relation between the size of a
hospital unit, the feasibility of the 85% target and the
fraction of
refused admissions two calculations have been made.
1. The percentage of refused admissions (Pc) given an
occupancyrate of 85% (2
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
18/27
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
19/27
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
20/27
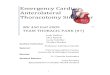
Larger hospital units can operate at higher occupancy rates
than
smaller ones while attaining the same percentage of refused
admissions.
The 85% target is only attainable for units with more than 5
If we hold the 85% target for a small unit such as the CCU
(6
beds) nearly half of all arriving patients is blocked, assuming
Pc =
0.05 is acceptable.
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
21/27
Results of the case study
The primary goal is to determine the optimal bed
allocation over the emergency cardiac care chain, given a
required service level.
The service level requirement is set at a maximum of 2%
refused admissions at the FCA.
In our model the service level requirement is rewritten
into a maximum of 5% blocking at the CCU.
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
22/27
We varied the number of CCU beds from 5 to 15 and the
number of NC beds from 12 to 19.
The LOS at the CCU is corrected for the additional waiting
time (based on measurements).The additional waiting time
was 27% of the original length of stay.
The ALOS at the CCU now equals 44 0.27 * 44 = 44 -12 = 32hours
(1.3 days).
The LOS at the NC is corrected for the additional time at
the
CCU. Furthermore a LOS-reductionof 20% is assumed.
The ALOS at the NC now equals 0.80 * (164 + 12) = 141 hours
(5.9 days).
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
23/27
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
24/27
In order to determine personnel costs for each bed
combination the following conversion rates are used:
2.2 fte (full time equivalent) per CCU bed 0.95 fte per NC
bed
The cheapest combination within the solution
area is 8 CCU beds and 16 NC beds (32.8 fte).
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
25/27
General results
A calculation based on average data, regarding the number
of arrivals and LOS, does not meet the actual
capacityrequirements and will most certainly result in frequent
operational difficulties.
The length of stay (LOS) of patients in hospital is highly
variable (Cv>= 1) and congestion or chain effects
influence
the average length of stay (ALOS).
The characteristics of arrival patterns and LOS
distributions
result in large workload variations at nursing units.
The 85% target is only attainable for units with a minimum
of approximately 50 beds
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
26/27
The variation in arrival rate at the FCA increases the
workload during office hours with 62%.
For a maximum of 2% refused admissions at the FCA a greatamount
of reserve capacity is required at the CCU and NC.
The number of beds required at the NC and CCU is
respectively and 16. The occupancy rate for this optimal
situation is respectively 55% and 78%. For the CCU this
means 2 extra beds are required, a capacity expansion of2/6 =
33%.
-
7/31/2019 Modeling the Emergency Cardiac in-patient Flow
27/27