Embed Size (px)
Citation preview

Original article
Model for end-stage liver disease combined with serumprealbumin to predict the prognosis of patients with
decompensated liver cirrhosis
Fei LIU,* Ling Yan CAI,* Lan ZHONG,* Chi CHEN,* Fei XU,*Zhong Xin ZHAO† & Xi Mei CHEN‡
*Departments of Gastroenterology and †General Surgery, Shanghai East Hospital, Tongji University, and‡Department of Gastroenterology, Tongji Hospital, Tongji University, Shanghai, China
OBJECTIVE: To evaluate the prognostic value ofmodel for end-stage liver disease (MELD) combinedwith serum prealbumin (PA) in patients with decom-pensated liver cirrhosis.
METHODS: A total of 252 patients were enrolled inthe study and followed 1 year. PA was measured andMELD score was calculated on the first day of admis-sion. Analysis of variance (ANOVA) was used to assesscorrelation between PA level and MELD score. Multi-variable Cox proportional hazards model was used toscreen the prognosis related factors. Kaplan–Meiersurvival curves were drawn.
RESULTS: Of the 252 patients, 28 died within 3months, 58 within 6 months and 91 within 1 year.
Serum PA level in dead patients was significantlylower than that in survival patients (P < 0.005) anddecreasing with increasing of MELD score. Cox analy-sis showed that MELD score > 18 (RR = 2.749) andPA < 70 mg/L (RR = 2.412) were independent prog-nosis risk factors. The risk ratio of MELD score com-bined with PA level (1.854, P < 0.01) was higher thanthat of MELD score alone (1.054, P < 0.05). Kaplan–Meier survival curve analysis showed that MELDscore � 18 combined with PA � 70 mg/L couldclearly discriminate patients who would survive or diewithin 6 month and 1 year follow up.
CONCLUSION: MELD score � 18 combined withPA � 70 mg/L could predict the 6-month and 1-yearprognosis of patients with decompensated liver cir-rhosis, and was superior to that of MELD score alone.
KEY WORDS: model for end-stage liver disease, prealbumin, prognosis.
INTRODUCTION
Liver cirrhosis is one of the most serious diseasesthreatening human health. To seek an evaluation
system to estimate liver reserve function and progno-sis of patients with chronic liver disease for selectingthe most appropriate therapeutic measure such asmedical treatment, surgery, supportive measures andliver transplantation is clinically very important. Allsuch systems from the Child–Turcotte–Pugh (CTP)classification system to the model for end-stage liverdisease (MELD) have been designed for grading theseverity of liver disease. Despite the widespread recog-nition and application of MELD, some defects remainin it because only a limited liver function indices and
Correspondence to: Fei LIU, Department of Gastroenterology, ShanghaiEast Hospital, Tongji University, Shanghai 200120, China. Email:[email protected]© 2010 Chinese Medical Association Shanghai Branch, ChineseSociety of Gastroenterology, Renji Hospital Affiliated to ShanghaiJiaotong University School of Medicine and Blackwell PublishingAsia Pty Ltd.
Journal of Digestive Diseases 2010; 11; 352–357 doi: 10.1111/j.1751-2980.2010.00465.x
352

renal function are included in this model. Many clini-cians thus seek the combination of MELD with otherpredicting criteria for improving the predictability ofMELD. Prealbumin (PA), which is synthesized in theliver, serves as a transport protein in the body and is amarker of visceral protein status. Because of its shorthalf-life and high predictive sensitivity, PA is a sensi-tive indicator of the liver synthetic function.1,2 In thisstudy, using a retrospective analysis of 252 patientswith decompensated liver cirrhosis, we investigatedthe prognosis predictive value of PA for patients withdecompensated cirrhosis and we also investigatedwhether PA, when combined with MELD, improvedthe value of using MELD alone in predicting the prog-nosis of decompensated cirrhosis patients.
MATERIALS AND METHODS
Patients
A total of 252 patients with decompensated cirrhosistreated in the Department of Gastroenterology ofShanghai East Hospital from September 2005 toAugust 2008 were enrolled. There were 161 men and91 women ranging in age from 29 to 89 (61.8 � 12.4)years. The diagnosis of cirrhosis was based on anunequivocal clinical picture and imaging result or aliver biopsy. Evidence of decompensated cirrhosis wasdefined as the presence of complications such asesophageal variceal bleeding, hepatic encephalopathyand ascites in liver cirrhosis patients.3 Patients withhepatocellular carcinoma and tumors of other organs,who had repeatedly been admitted to hospital, whosecase record was incomplete or who were lost to followup, or who were undergoing surgical proceduresdirectly involving the liver, such as a hepatectomy anda transjugular intrahepatic portosystemic shunt wereexcluded from the study. Of the 252 patients, 205 hadhepatitis B, one had hepatitis C, 30 had a mixed eti-ology (26 patients with hepatitis B and alcoholic liverdisease, three with hepatitis B and schistosomiasis,one with hepatitis B and hepatitis E), 11 had alcoholicliver disease, two had primary cholestatic liver diseaseand three had cryptogenic cirrhosis.
Clinical data
Laboratory results: serum bilirubin, serum creatinine,international normalized ratio (INR), and serum PAwere obtained on admission day. All the patients werefollowed up for 1 year, and survivals at 3 months, 6months and 1 year of follow up were observed.
Calculation of MELD score
The MELD score was calculated according to themethod described by Kamath et al.
MELD score = 3.8 ¥ loge[bilirubin (mg/dL)] + 11.2 ¥loge(INR) + 9.6 ¥ loge[serum creatinine (mg/dL)] +6.43 ¥ loge (etiology: cholestatic or alcoholic is 0,others are 1).4
Statistical analysis
All statistical analyses were conducted using SPSS forWindows 13.0 (SPSS, Chicago, IL, USA). Paired datawere compared using Student’s t-tests. ANOVA was usedfor comparing data between multiple groups. Multi-variate Cox proportional hazards model was used toscreen the factors affecting the prognosis. Kaplan–Meier survival curves were drawn, and areas underreceived operating characteristics curves (ROC) werecompared. P < 0.05 was considered statisticallysignificant.
RESULTS
MELD score and PA level in groups of patientswho died and those who survived
Of the 252 patients with decompensated liver cirrho-sis, 28 (11.1%) died within 3 months, 58 (23.0%)died within 6 months and 91 (36.1%) died within 1year of follow up. The MELD score was significantlyhigher (P < 0.005) and the PA level was significantlylower (P < 0.005) in the group that died than in groupthat survived. The MELD score (24.40 � 7.56)was significantly higher and PA level (47.86 �28.06 mg/L) was significantly lower in the group thatdied than in the survival group (15.18 � 5.33 and84.47 � 57.79 mg/L, respectively) (P < 0.005) at the3-month follow up. The MELD score (21.40 � 7.02)and PA level (54.82 � 30.90 mg/L) in the group thatdied were also significantly higher and lower, respec-tively, than those in the survival group (14.64 � 5.17and 88.05 � 60.04 mg/L, respectively) (P < 0.005)at 6-month follow up. At 1-year follow up, theMELD score (19.50 � 6.69) and PA level (57.67 �37.61 mg/L) in the group that died also were signifi-cantly higher and lower, respectively, than thosein the survival group (14.34 � 5.26 and 93.25 �62.45 mg/L, respectively) (P < 0.005) (Table 1).
Relationship between the MELD score and serumPA level
The 252 patients with decompensated cirrhosis weredivided into three groups according to their MELD
Journal of Digestive Diseases 2010; 11; 352–357 MELD and prealbumin in liver cirrhosis 353
© 2010 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated to Shanghai Jiaotong University Schoolof Medicine and Blackwell Publishing Asia Pty Ltd.

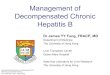
score: < 11 (group 1); 11 � MELD score < 20 (group2) and MELD score � 20 (group 3). The level of PAdecreased with the increase of the MELD score(P < 0.05) (Table 2). By correlation analysis, a moder-ate negative correlation existed between the MELDscore and serum PA level (r = -0.355, P < 0.01)(Fig. 1).
Multivariate Cox proportional hazards modelanalysis
The multivariate Cox proportional hazards modelanalysis showed that a MELD score > 18 and aPA < 70 mg/L were independent risk factors for pre-dicting the prognosis of decompensated cirrhosis. Therisk ratios (RR) were 2.749 and 2.412, respectively(P < 0.005, Table 3). The higher the MELD score atadmission, the higher was the risk of death. The lowerthe PA level, the higher was the risk of death. Thedecrease of one mg/L of PA level, increased the risk ofdeath approximately 2.412-fold. With a MELD score
of 18 and PA 70 mg/L as the cut-off value, it was foundthat the risk ratio of the MELD score combined withthe PA level (1.854) was significantly higher than thatof MELD score alone (1.045) (P < 0.05, Table 4).When these patients were divided into group A(MELD score � 18 and a PA � 70 mg/L), groupB (MELD score � 18 and PA < 70 mg/L), group C(MELD score > 18 and PA � 70 mg/L), and group D(MELD score > 18 and PA < 70 mg/L), the RR ofgroups A, B and C were 0.071-fold, 0.246-fold and0.448-fold that of group D, respectively (P < 0.05,Table 5). The survival prospect was the best in groupA, then in group B, then group C, and the worst was ingroup D.
Kaplan–Meier survival curves of MELD combinedwith PA
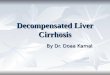
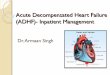
Based on the results of multivariate Cox proportionalhazards model analysis, with MELD = 18 andPA = 70 mg/L as cut-off values, 252 decompensatedcirrhosis patients were divided accordingly into fourgroups and drawing 3-month, 6-month and 1-yearKaplan–Meier survival curves (Figs 2–4). It was shownthat MELD score � 18 combined with PA � 70 mg/Lcould effectively discriminate patients who wouldsurvive or be dead at the 6-month and 1-year followup (P < 0.005) although the discrimination rate wasnot high at the 3-month follow up.
DISCUSSION
In 2001, by revising statistically the model previouslycreated for estimating the survival of patients under-
Table 1. Clinical outcome 252 patients with cirrhosis at 3-months, 6-months and 1-year follow up; data expressed asmean � SD
3-months follow up 6-months follow up 1-year follow up
Clinical outcome Survival group Group that died Survival group Group that died Survival group Group that diedMELD 15.18 � 5.33 24.40 � 7.56* 14.64 � 5.17 21.40 � 7.02* 14.34 � 5.26 19.50 � 6.69*PA (mg/L) 84.47 � 57.79 47.86 � 28.06* 88.05 � 60.04 54.82 � 30.90* 93.25 � 62.45 57.67 � 37.61*
*P < 0.05 versus the survival group.MELD, the model for end-stage liver disease; PA, prealbumin.
Table 2. Relationship between prealbumin (PA) level and model for end-stage liver disease model for end-stage liver disease(MELD) score in 252 patients with cirrhosis; data expressed as mean � data
Group1(MELD < 11)
Group2(11 � MELD < 20)
Group3(MELD � 20)
PA (mg/L) 119.26 � 71.55* 76.49 � 48.68* 50.02 � 31.87*
*pairwise comparisons P < 0.05.
Figure 1. Correlation between model for end-stage liverdisease (MELD) and prealbumin (PA).
Journal of Digestive Diseases 2010; 11; 352–357354 F Liu et al.
© 2010 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated to Shanghai Jiaotong University Schoolof Medicine and Blackwell Publishing Asia Pty Ltd.

going a transjugular intrahepatic portosystemic shuntprocedure, Kamath4 et al. of Mayo Clinic established aMELD for predicting the prognosis of decompensatedliver cirrhosis patients. The MELD could predict accu-rately the 1-week, 3-month and 1-year death risk ofdecompensated cirrhosis patients and was superior tothe CTP score system.5 Since the issue of MELD, manyverifying clinical studies have been performed.6 As anovel prognosis predicting system MELD has obviousmerits: it is objective, it uses continuous variables andhas no upper and lower limits, it is incorporated withrenal function and can predict the prognosis of cirrho-sis patients associated with complications and the riskof developing complications, as well as being used forestimating the RR of non-transplantation therapy andthose waiting for a liver transplant.7 Since 2002 theUnited Network for Organ Sharing used MELD toreplace the former grading system based on CTP forassessing priority in allocating an organ for a livertransplant.8 Although MELD has been applied widely,
some defects remain. Currently, clinicians9 try toincorporate other predictors to improve the prognosispredictive value of MELD in end-stage liver diseasepatients, such as kinetic MELD, MELD combined withserum sodium level,10,11 MELD combined with bloodlipid level,12 MELD combined with hepatic venouspressure gradients13 and so on.
PA is an acute-phase reactive protein with a relativemolecular mass in 55 kDa. In the physiological con-dition, PA presents mainly in blood and cerebrospinalfluid, and PA in plasma is solely synthesized by theliver and has a short half-life (1.9 day). Albumin isalso synthesized in the liver, so when the liver synthe-sis function is damaged, there are qualitative andquantitative changes of albumin. Previously, serumalbumin has been frequently used as an importantindicator of liver function and has been included inthe CTP score system. However, because of its longhalf-life (17–21 days) and because an exogenous
Table 3. Result of multivariate COX regression of 252 decompensated cirrhosis patients
B SE Wald d.f. P RR
95.0% CI
Lower Upper
MELD 0.050 0.021 5.725 1 0.017 1.051 1.009 1.095MELD > 18 1.011 0.307 10.884 1 0.001 2.749 1.508 5.012PA < 70 mg/L 0.881 0.264 11.164 1 0.001 2.412 1.439 4.044
B, beta coefficient; d.f., degree of freedom; MELD, model for end-stage liver disease; PA, prealbumin; RR, risk ratio; SE: standard error;Wald, c2 value.
Table 4. Multivariable Cox proportional hazards model analysis of model for end-stage liver disease (MELD) combinedwith prealbumin (PA) and MELD alone
B SE Wald d.f. P RR
95.% CI
Lower Upper
MELD alone 0.044 0.021 4.441 1 0.035 1.045 1.003 1.088MELD combined with PA 0.617 0.131 22.105 1 0.000 1.854 1.433 2.398
B, beta coefficient; d.f., degree of freedom; RR, risk ratio; SE: standard error; Wald, c2 value; co: combine.
Table 5. Multivariable Cox proportional hazards model analysis of model for end-stage liver disease (MELD) combinedwith prealbumin (PA)
B SE Wald d.f. P RR
95.0% CI
Lower Upper
MELD > 18, PA < 70 68.998 3 0.000MELD � 18, PA � 70 -2.647 0.356 55.372 1 0.000 0.071 0.035 0.142MELD � 18, PA < 70 -1.401 0.242 33.550 1 0.000 0.246 0.153 0.396MELD > 18, PA � 70 -0.804 0.369 4.744 1 0.029 0.448 0.217 0.923
B, beta coefficient; d.f., degree of freedom; RR, risk ratio; SE: standard error; Wald, c2 value.
Journal of Digestive Diseases 2010; 11; 352–357 MELD and prealbumin in liver cirrhosis 355
© 2010 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated to Shanghai Jiaotong University Schoolof Medicine and Blackwell Publishing Asia Pty Ltd.

albumin supplement is frequently used in clinicalpractice, serum albumin cannot truly reflect liverdamage at an early stage and with sensitivity anddynamically. Compared with albumin, because of itsshort half-life PA can show up rapidly in the serum
when the synthetic function of the liver is damagedand is a sensitive indicator of damage in the liversynthetic function.14
By studying the serum PA level in patients with livercirrhosis associated with hepatic cancer, chronic activehepatitis, alcoholic hepatitis, cryptogenic cirrhosis,obstructive jaundice, inflammatory bowel disease andmyocardial infarction, Hutchinson15 et al. found thatPA level was significantly decreased when the liverfunction was impaired and was within normal rangewhen there was no impairment of liver function.Therefore, PA has an important role in the evaluationof liver disease. Yan et al.16 reported that the PA level ofvarious types of chronic liver disease was significantlylower than that of controls (P < 0.05 or P < 0.01).Serum PA abnormality rates of mild, moderatechronic hepatitis B patients were significantly higherthan albumin and bilirubin abnormality rates(P < 0.01); the PA level could reflect liver syntheticfunction impairment earlier than serum albumin, andthe level of PA decreased with the increase in severityof liver disease. The decrease in PA level correlatedwith the severity of liver cell damage. The PA levelcould decreased to zero in fulminant hepatitis and inthe severe form of hepatitis, bilirubin was markedlyelevated and an ominous prognosis was suggested.Pang et al.17 studied the correlation between the PAlevel and CTP classification in 162 liver cirrhosis
Figure 2. Comparison of 3-month survival between dec-ompensated cirrhosis patients with model for end-stage liverdisease (MELD) showing group A (MELD score � 18 andprealbumin [PA] � 70 mg/L), group B (MELD score � 18and PA < 70 mg/L), group C (MELD score > 18 andPA � 70 mg/L), and group D (MELD score > 18 andPA < 70 mg/L).
Figure 3. Comparison of 6-month survival between dec-ompensated cirrhosis patients with model for end-stage liverdisease showing ( ) group A (MELD score � 18 and pre-albumin [PA] � 70 mg/L), ( ) group B (MELD score � 18and PA < 70 mg/L), ( ) group C (MELD score > 18 andPA � 70 mg/L), and ( ) group D (MELD score > 18 andPA < 70 mg/L).
Figure 4. Comparison of 1-year survival between decom-pensated cirrhosis patients with model for end-stage liverdisease ( ) group A (MELD score � 18 and a prealbumin[PA] � 70 mg/L), ( ) group B (MELD score � 18 andPA < 70 mg/L), ( ) group C (MELD score > 18and PA � 70 mg/L), and ( ) group D (MELD score > 18and PA < 70 mg/L).
Journal of Digestive Diseases 2010; 11; 352–357356 F Liu et al.
© 2010 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated to Shanghai Jiaotong University Schoolof Medicine and Blackwell Publishing Asia Pty Ltd.

patients and found that the PA level decreased signifi-cantly with the elevation of CTP grade (P < 0.01).
In this study, the MELD score was combined with PAlevel to predicting the prognosis of decompensatedcirrhosis patients. Taking MELD score 11 and 20 ascut-off values, 252 decompensated cirrhosis patientswere divided into three groups, namely, one with aMELD score � 11, one with a MELD score between 11and 20, and one with a MELD score � 20. The PA leveldiffered significantly between these three groups step-wise. Our study also found that with the increasingMELD score, serum PA level decreased.
Multivariate Cox proportional hazards model analy-sis showed that a MELD score > 18 and a PAlevel < 70 mg/L were two independent risk factors ofthe prognosis of decompensated cirrhosis. The riskratios were 2.749 and 2.413, respectively (P < 0.05).The higher the MELD score and the lower the PA levelat admission, the higher was the risk of death. Using aMELD score > 18 and a PA level < 70 mg/L as cut-offvalues, it was found that the risk of death of a MELDscore > 18 combined with a PA < 70 mg/L was higherthan that of a MELD score > 18 alone (P < 0.05), andwas also higher than the other three MELD withPA groups, namely, a MELD score > 18 and a PAlevel > 70 mg/L, a MELD score < 18 and a PAlevel < 70 mg/L, and a MELD score < 18 and aPA level > 70 mg/L groups (P < 0.05). This showedthat MELD combined with PA could increase the capa-bility of MELD to predict the prognosis of decom-pensated cirrhosis patients. Kaplan–Meier survivalcurves demonstrated that a MELD score � 18 anda PA level � 70 mg/L could effectively discriminatepatients who will survive or die at a 6-month or 1-yearfollow-up. Correlation analysis showed that there wasa moderate negative correlation between the MELDscore and PA level (r = -0.355, P < 0.01). Because ofthe difference in numeric data types and MELD com-bined with the fact that PA is non-continuous vari-able, it could not be compared with MELD combinedwith serum sodium, which is a continuous variable.For MELD combined with PA, a further study with alarge sample size is needed to confirm its benefit andan optimal calculation formula deduced by statisti-cians is needed.
In conclusion, the MELD score and PA level are twoimportant indexes for predicting the prognosis ofpatients with decompensated cirrhosis. A MELDscore � 18 combined with a PA level � 70 mg/L may
well predict the 6-month and 1-year prognosis ofpatients with decompensated liver cirrhosis.
REFERENCES
1 Geisler JP, Linnemeier GC, Thomas AJ, Manahan KJ et al.Nutritional assessment using prealbumin as an objectivecriterion to determine whom should not undergo primaryradical cytoreductive surgery for ovarian cancer. GynecolOncol 2007; 106: 128–31.
2 Hou M, Sun S, Jiang Z. A new and selective and sensitivenanogold-labeled immunoresoance scattering spectral assayfor trace prealbumin. Talanta 2007; 72: 463–7.
3 Franchis R de. Evolving Consensus in portal hypertensionreport of the Baveno IV Consensus Workshop onmethodology of diagnosis and therapy in portalhypertension. J Hepatol 2005; 43: 167–76.
4 Kamath PS, Wiesner RH, Malinchoc M et al. A model topredict survival in patients with end-stage liver disease.Hepatology 2001; 33: 464–70.
5 Farnsworth N, Fagan SP, Berger DH, Awad SS.Child–Turcotte–Pugh versus MELD score as a predictor ofoutcome after elective and emergent surgery in cirrhoticpatients. Am J Surg 2004; 188: 580–3.
6 Said A, Williams J, Holden J et al. Model for end stage liverdisease score predicts mortality across a broad spectrum ofliver disease. J Hepatol 2004; 40: 897–903.
7 Bambha K, Kim WR, Pedersen R, Bida JP, Kremers WK,Kamath PS et al. Predictors of re-bleeding and mortalityafter actue variceal haemorrhage in patients with cirrhosis.Gut 2008; 57: 814–20.
8 Martin AP, Bartels M, Hauss J, Fangmann J. Overview of theMELD score and the UNOS adult liver allocation system.Transplant Proc 2007; 39: 3169–74.
9 Liu F, Cai LY, Chen XI. The progress in evaluating of liverfunction model. Int J Dig Dis 2009; 29: 268–70 (in Chinese).
10 Wang YW, Huo TI, Yang YY et al. Correlation andcomparison of the model for end-stage liver disease, portalpressure, and serum sodium for outcome prediction inpatients with liver cirrhosis. J Clin Gastroenterol 2007; 41:706–12.
11 Jiang M, Liu F, Xiong WJ et al. Comparison of four modelsfor end-stage liver disease in evaluating the prognosis ofcirrhosis. World J Gastroenterol 2008; 14: 6546–50.
12 Jiang M, Liu F, Xiong, WJ et al. Combined MELD and bloodlipid level in evaluating the prognosis of decompensatedcirrhosis. World J Gastroenterol 2010; 16: 1397–401.
13 Ripoll C, Bañares R, Rincón D et al. Influence of hepaticvenous pressure gradient on the prediction of survival ofpatients with cirrhosis in the MELD era. Hepatology 2005;42: 793–801.
14 Zhang Y, Qi CY, Ying YA et al. Comparison clinicalsignificance of 12 kinds of plasma protein in hepatitis,liver cirrhosis. Anhui Medicine 1992; 13 (6): 6–8 (inChinese).
15 Hutchinson DR, Halliwell RP, Smith MG, Parke DV et al.Serum ‘prealbumin’ as an index of liver function in humanhepatobiliary disease. Clin Chim Acta 1981; 114: 69–74.
16 Yan MX, Wang WQ, Liu Q et al. Clinical value of serumprealbumin combination with total bile acids in chronicliver disease. Shandong Medicine 2000; 40: 3–4 (in Chinese).
17 Pang GJ, Liu HP, Sun JF. The relationship between detectionof serum prealbumin co-cholinesterase and classificationof cirrhosis. Harbin Pharmaceutical 2008; 28: 12–3 (inChinese).
Journal of Digestive Diseases 2010; 11; 352–357 MELD and prealbumin in liver cirrhosis 357
© 2010 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated to Shanghai Jiaotong University Schoolof Medicine and Blackwell Publishing Asia Pty Ltd.