Embed Size (px)
Citation preview

MOD II 2016 ECRN CEBehavioral Emergencies,
Bariatric Patients, VAD’s, and
Life VestPrepared by:Deborah Semenek RN, EMT-P
Mark Dzwonkiewicz FP-C, LI
Elizabeth Peaslee RN
IDPH Site Code: 107200E-1216
1
Objectives Upon successful completion of this module, the ECRN will be able to:
1. Examine the differences in behavioral health diagnoses.
2. Review how to interact, de-escalate and treat patients with psychiatric disease.
3. Examine differences in patient care approaches when caring for the bariatric patient.
4. Review the patient population utilizing a VAD to support heart function.
5. Review care and transportation issues related to the patient with a VAD.
6. Review and discuss the use and care of a patient with a Life Vest.
7. Actively participate in review of selected Region X SOP’s related to the topic presented.
8. Successfully complete the post quiz with a score of 80% or better.2
Behavioral Emergencies
• Behavior- a persons observable conduct and activity
• Behavioral Emergency- A situation in which the patient’s
behavior becomes unusual, bizarre, threatening and/or
dangerous that another person takes notice.
• Factors that may indicate behavioral emergency….
• Core life function disruption
• Eating, sleeping, etc.
• Threat to oneself or others
• Deviation from societal expectations or norms3

Pathophysiology
• Up to 20% of the population has a form of mental health problem
• Most are cared for in outpatient centers
• Common reason for EMS involvement is due to medication non-compliance
4
Causes of Behavioral
Emergencies
• Biological
• Results from disease process
• Tumors or infections
• Structural changes
• Abuse of drugs and alcohol
• Never assume a patient with AMS has a
psychological condition until all possible medical
conditions or substance abuses are ruled out. 5

Psychosocial
• Related to personality style, unresolved
conflicts, or crisis management methods
• Examples….
• Traumatic childhood event
• Development of peer pressure
• Dysfunctional family
• Lack of parental support
• Abusive parent(s) 6

Sociocultural
• Related to patients actions and interactions with
society
• Effect patient social space, social isolation or
otherwise impact patient socialization
• Relationships, support system, social habits,
social skills and values
• Caused by profound events
• Rape, assault, witness to victimization of
others, death of a loved one, acts of violence7
AMS SOP
Consider Etiology
(Diabetes, drug overdose,
Poisoning, stroke,
Alcohol related)
Adult Routine Medical Care
Immobilize C-spine as indicated
Obtain blood glucose and record
If <60 administer Dextrose 50% 50 mL IVP/IO
-or-
Glucagon 1 mg IM/IN8

AMS SOP cont.If patient no alert, decreased respiration or
suspected narcotic overdose
Narcan 2mg IN/IVP/IO every 5 minutes as needed to
max dose of 10mg
• Attempt to ID substance involved
• Bring any containers found to hospital, so long as
they aren’t a safety risk
• Consider restraints prior to administration of
Narcan9
Remember Etiology
A- Acidosis,
Alcohol
E- Epilepsey
I- Infection
O- Overdose
U- Uremia
T- Trauma,
Tumor
I- Insulin
P- Psychosis
S- Stroke
10

At The Scene
• Scene safety and BSI
• Call law enforcement, if necessary
• Begin to establish rapport
• Determine and document if patient is a threat to
themselves or others
• Examine the environment for potential threats
• If suicidal, patient can not be left alone. At
least one EMS provider must remain with the
patient 11

Verbal De-escalation
• Attempt with all patients
• Should be first method to attempt to calm aggressive
patient
• Safest because it requires no physical contact
• Be honest and straight forward with a friendly tone
• Avoid direct eye contact or invading patient’s personal
space which may increase stress and anxiety
• Can diffuse a situation and prevent further escalation and
eliminate the need for physical restraints
12

Restraints• Last resort
• Two types- hard and soft
• Suggested to have 5 people for safe application
• Make every attempt to avoid injury to patient
• Never transport patient in prone position
• Document:
• Reason for restraint, type and location of
restraint, time of restraints
• Assess distal SMV’s 13
Condiser Medical
Etiology
• Hypoxia
• Substance Abuse/Overdose
• Excited Delirium/Hyperthermia
• Neurologic Disease (CVA, Intracerebral Bleed, etc.)
• Metabolic Problems (Hypoglycemia)
• Continue routine medical care for adult or pediatric patient
14

Medications Needed• Contact medical control for pediatric
patients
• In patient with severe anxiety or agitation:
• Versed 2mg IN
• May repeat every 2 minutes until desired
results to max of 10mg
• If additional medication needed:
• Valium 5 mg IVP over 2 minutes, may
repeat up to 10mg or Valium 10mg IM15

Petition
• Legal documentation to transport patient to the hospital from the scene with or without patient consent
• Assist keeping patient in hospital throughout evaluation
• Family members, police, EMS or bystanders can complete petition
• Petition does not guarantee a patient to be committed
16

Behavioral Emergency
Notes
• All region X hospitals can accept any psych patient
• Transport all medication or substance bottles saftly with patient
• Remember mentally ill patients are more aware of their surroundings than they appear, so becarful what is said around them
17

Cognitive Disorders
• Organic causes such as brain injury or
disease
• Caused by physical or chemical injuries
• Delirium
• Dementia
18
Delirium
• Rapid onset of widespread disorganized thoughts
(hours or days)
• Symptoms:
• Inattention, memory impairment,
disorientation and general clouding of the mind
• Causes:
• Medical conditions, intoxication or withdrawal
• Confusion is a hallmark sign19

Dementia
• Develops over months and is usually irreversible
• Several possible medical etiology
• Alzheimer’s, vascular problems, AIDS, head
trauma, Parkinson’s and substance abuse
• Involves…
• Memory, cognitive, and pervasive impairments
• Be supportive
20

Schizophrenia
• Effects estimated 1% of the U.S. population
• Hallmark sign is a significant change in behavior
and loss of contact with reality
• Symptoms:
• Hallucinations, delusions and depression
• Symptoms will cause social or occupational
dysfunction
• Usually diagnosed in early adulthood 21
Anxiety Disorders
• Characterized by dominating apprehension and
fear
• Affects approximately 2-4% of the population
• Uneasiness, discomfort, apprehension and
restlessness
• Panic disorder, phobia, and post-traumatic
stress syndrome
22
Panic Attack• Recurrant, extreme periods of anxiety resulting in great
emotional distress
• Acute in nature and unprovoked
• Usually peaks in 10 minutes and dissipates in 1 hour
• May present cardiac or respiratory in nature, so EMS must rule
out both possibilities
• Symptoms:
• Palpitations, sweating, trembling, shortness of breath, chest
pain or discomfort, nausea, dizziness, loss of control, fear of
dying, numbness or tingling sensation and/or chills or hot
flashes
• Management:
• Supportive care
23

Phobias
• A fear that becomes excessive and interferes with
functioning
• The fear is considered intense and irrational
• Exposure to fear will induce anxiety or panic
attack
• Manage patients by being supportive
24
Post-Traumatic Stress• A reaction to an extreme, usually life-threatening
stressor
• Natural disaster, victimization (rape, etc.), and
emotionally taxing situations
• Will avoid similar situations
• Recurrent intrusive thoughts
• Depression
• Sleep disturbances
• Nightmares
• Manage patient with respect, empathy and support25
Mood Disorders
• Pervasive and sustained emotion that colors a
person’s perception of the world
• Depression
• Bipolar Disorder
26

Depression• Profound sadness or feeling of melancholy
• Most prevalent psychiatric condition
• Major depressive disorder
• Depression that is prolonged or severe
• Symptoms:
• Depressed most of the day
• Decreased interest in pleasure
• Weight loss
• Insomnia or hypersomnia
• Lack of concentration
• Thoughts of death27

Bipolar Disorders• One or more manic episodes with or without subsequent or
alternating periods of depression
• Begins suddenly and escalates rapidly over a few days
• Develops in adolescence or early adulthood
• Symptoms:
• Increased self-esteem
• Less need for sleep
• More talking or pressure to keep talking
• Flight of ideas
• Distractibility
• Increased goal-directed activity
• Delusional thoughts
28
Substance Disorders
• Substance abuse is a common disorder
• EMS should rule out as a possibility when a patient
is experiencing a psychiatric or behavioral
disorder
• May present as depressed, psychotic or delirious
• Serious condition
• Patients may present ill from addiction or
withdrawal from the substance
29
Withdrawal from Alcohol
• Happens from abrupt discontinuation or after
prolonged use or from rapid fall in blood alcohol
level
• Symptoms can occur several hours after last drink
and can last up to 5-7 days
• Seizures can occur within the first 24-36 hours
after last drink
30

Withdrawal Signs and
Symptoms• Tremors of the hands, tongue, and eyelids
• Nausea and vomiting
• General weakness
• Tachycardia
• Sweating
• Hypertension
• Orthostatic hypotension
• Anxiety, irritability or depressed mood
• Hallucinations
• Poor sleep31

Delirium Tremens
• Usually develop in second or third day of withdrawal
• Symptoms:
• Decreased level of consciousness
• Hallucinations
• Misinterpretation of events
• Seizures
• Significant mortality rates
• Treatment with benzodiazepines can help prevent against
seizures32

Excited Delirium• Can be caused by drug intoxication, psychotic illness or both
• Signs/Symptoms:
• Abnormal pain tolerance, tachycardia, sweating, agitation,
skin that feels hot, lack of tiring, unusual strength,
inappropriate clothing
• Difficult to diagnose
• Be aware of the patient who becomes suddenly tranquil after
frenzied activity because this is usually followed by cardiac
collapse and/or death
• Always evaluate if a patient must be restrained
• Allowing a patient to struggle against restraints increases risk of
death 33

Bariatric
Patient
• Most common reason
EMS is toned out is
for undifferentiated
abdominal pain
• Always assure scene
safety and BSI
34

Assess Patient Airway• Assess for patency
• Morbidly obese patients have excessive skin and adipose tissue around their cheeks, lower jaw and thorax which can place extra pressure on the tongue and airway
• Increased oxygen consumption
• Increased carbon dioxide production
• Excess metabolic activity35
Assessing Breathing• Decreased lung capacity from decreased chest
wall compliance and increased abdominal cavity contents
• Makes bariatric patients at risk for hypoxemia and hypercarbia
• Gives patients less respiratory reserve
• Prepare for rapid decline
• Breath sounds may be difficult to hear due to increased amount of adipose tissue
36

Ventilation Complications• If patient has no c-spine injury, place the patient supine and use
blankets to place under head, neck and shoulders to place in a “ramp
position”
• Utilize oral and nasal airways
• Don’t overestimate lung volume due to patient size
• When possible use two person technique with a jaw thrust for BVM
ventilation
• If intubation needed….
• Prepare for difficult attempt in patients with sleep apnea
• Sedatives given can completely occlude airway with tongue
• Use capnography for tube confirmation due to difficulty with
auscultation r/t to increased adipose tissue37
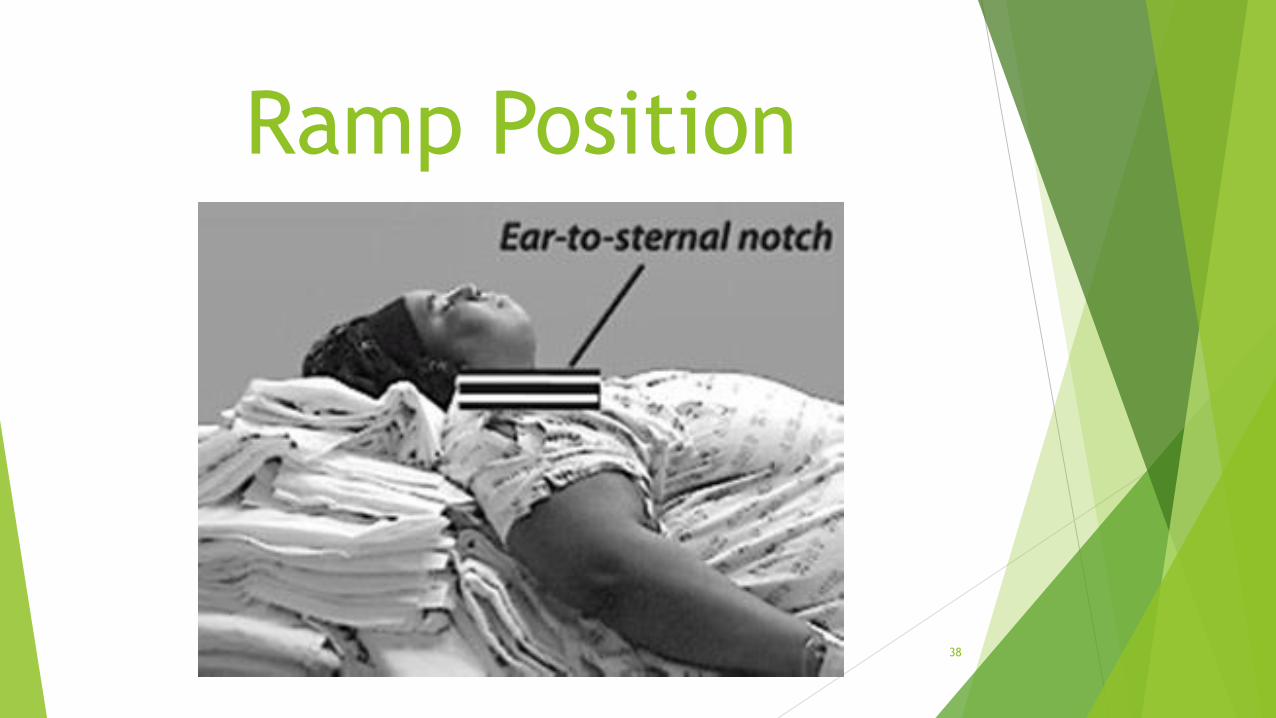
Ramp Position
38

Assessing Circulation• Increased stress on the heart
• Increased cardiac output even at rest due to the need for
extra tissue profusion
• Increased basal heart rate
• ECG may be less reliable due to the distance of the
electrodes to the heart
• Increased prevalence of heart disease in a younger
demographic
• If the need for immobilization arises, use caution so the
collar is not so tight it restricts blood flow to the major
vessels in the neck 39
Obtaining History• Per normal protocol, as with any patient
• Signs and symptoms of complaint
• Allergies
• Medications
• Past medical history
• Prepare for increased number of medical
conditions
• DM, HTN, hyperlipidemia, increased vascular
disease, stroke, cardiac disease, CHF,
peripheral edema, and ulcerations of the skin 40

Bariatric Surgery• To include gastric bypass, Lap-Band and gastric
sleeve can result in early and late complications
• Early- within the first month s/p surgery
• Think DVT, PE, wound infection, sepsis or GI
bleed
• Late- after the first month s/p surgery
• Think strictures, hernia or hardware
complications
• Gastric bypass has increased incident of ulcers
• Lap-Band has increased hardware malfunctions41

Bariatric Surgery
Gastric Bypass Lap-Band
42

Abdominal Assessment
• Exam will be complicated by loss of
anatomical landmarks
• Palpation of deep structures will be
limited due to amount of adipose
tissue
• Increased adipose tissue also limits
Cullen’s and Grey Turnner’s signs43
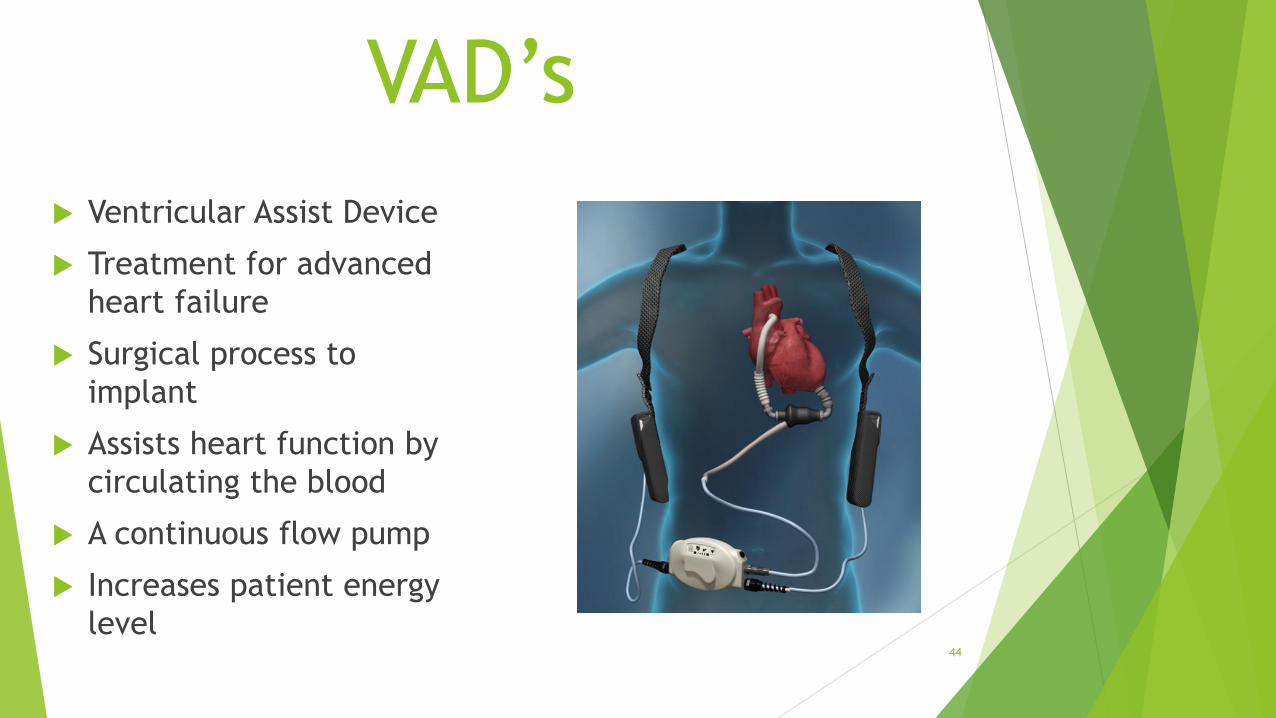
VAD’s
Ventricular Assist Device
Treatment for advanced
heart failure
Surgical process to
implant
Assists heart function by
circulating the blood
A continuous flow pump
Increases patient energy
level44

Indications
• Patient in class 3 or 4 heart failure while at rest or in
cardiogenic shock
• Short term
• Patient on transplant list but very sick
• Long term
• Not a transplant candidate
• Bridge to Recovery
• Treating cardiogenic shock
• Unable to come off heart-lung machine s/p surgery45

Usual Demographics
35-65 years old
Multiple medical
problems
Death is primarily
from non-VAD related
causes
Without transplant
survival rate is about
4-5 years46

Living with the VAD
• May return to daily activities with few limitations
• Patients look normal and healthy
• They have increased energy
• No travel restrictions
• Must avoid contact sports and water activities
47

Risks To Patient
• Bleeding
• All VAD patients are on prophylactic anticoagulants
which increase a patients risk for bleeding
• Infection
• Direct access portal-of-entry to heart
• Stroke
• Device malfunction
• Death
48

VAD Function
Inflow portion
surgically connected
to apex of left
ventricle
Outflow portion
surgically connected
to ascending aorta
Right side of heart can
still function normally
49

Components of VAD Surgically implanted in body
with communication to the outside of the body
Pump
Inside body and delivers blood to aorta
Take over the work of left ventricle
Driveline
Inside and outside of body
Communicates with the pump
Don’t cut or disconnect, pump will stop
50
Components (con’t)• System Controller
• Outside of the body
• Computer that controls all functions of the VAD
• “Brain”
• Batteries
• Outside the body
• External power source
• Last 4-12 hours
• Can press battery button to determine the charge level
• AC/wall power
• NEVER remove both power sources at the same time51

Care of the Driveline
• A wire that exits the body
• High risk for infection
• Always stays covered with a sterile dressing
• Direct portal to the heart
• DO NOT remove the dressing
• DO NOT pull or tug on the driveline
• DO NOT disconnect from battery pack
52
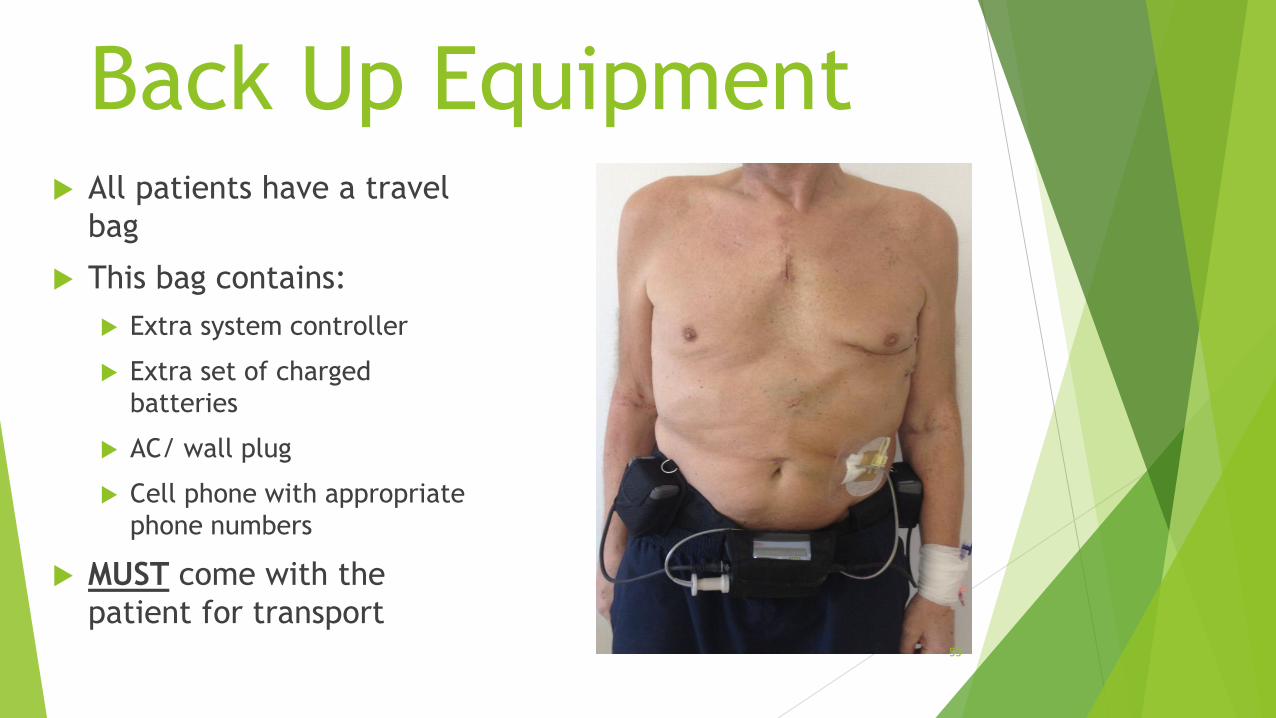
Back Up Equipment All patients have a travel
bag
This bag contains:
Extra system controller
Extra set of charged
batteries
AC/ wall plug
Cell phone with appropriate
phone numbers
MUST come with the
patient for transport53

VAD Readings• Flow
• Amount of blood flowing through the pump
• Measured in L/min
• AKA cardiac output
• Speed
• A set number
• Shows how fast the pump is running
• PI
• Volume in left ventricle
• Power
• Amount of energy in WATTS to maintain speed54
Patient Assessment• Pulses may or may not be present
• Differs from patient to patient
• Use a stethoscope over lower part of heart to
listen for the “hmmm” sound of the VAD
working
• May only obtain blood pressure if patient has
pulses
• If no pulses, a Doppler is needed to assess
pressure
• Pulse-ox may be unreliable 55
Patient Assessment• Neurologic
• Increased risk for stroke due to anti-
coagulation
• Glucose levels are unaffected
• Skin parameters stay the same
• VAD doesn’t affect ECG
• Electrical activity continues in the heart with
or without capture
• PEA56

VADs & Anticoagulation
All VAD patients are
anticoagulated
Increased risk for bleeding
Take all bleeding
precautions
Coumadin/warfarin are
the only medication
approved for all devices
57

EMS Arrest Interventions• Listen for the “hmmm” of the VAD, if you hear it, no need
for compressions. VAD is circulating the blood.
• If no “hmmm”, begin CPR
• Don’t worry about dislodging equipment because if
nothing is done patient has no survival chance
• Cardiac medications
• Can be given, but will have different levels of
effectiveness
• Discuss Dopamine with medical control prior to use
• 90-95% of patients have ICD’s, but if need arises EMS may
use their defibrillator
• Most arrests are not VAD failures, but rather some other
etiology
58
Emergency Action
• VAD stops functioning, must be restored or patient
will die
• Check driveline connection to controller
• Check power lead connection to controller
• Check power source
• Replace system controller
59
VAD Do’s and Don’tsDo
Follow CAB’s
Listen to family
Bring all VAD equipment
to the hospital
Keep patient on 2 good
power sources at all times
Do Not
Never disconnect
driveline from controller
Never disconnect both
power sources at the
same time
Never expose VAD to
water
Don’t open or view
sterile exit site
60
EMS Tips
• Follow BLS protocol
• Make sure all connections are properly connected
• Verify power
• Listen to patient’s family
• Bring all equipment to hospital in the ambulance
• A DNR is not required for a VAD patient
61

Zoll Life
Vest
• First wearable
defibrillator
• 98% first shock efficacy
rate
62

Zoll Life Vest
• Wearable defibrillator is a treatment option for sudden cardiac arrest
• Worn on the outside of the body
• Continuously monitors patient with dry non-adhesive electrodes
• If life-threatening rhythm is detected the device will alert patient prior to delivering shock to give the conscious patient a chance to turn the shock off
• If the patient is unconscious, the device will release a blue gel over the electrodes prior to delivering shock
63
Life Vest and EMS
• Standard evaluation and treatment
• Begin CPR if device is not saying
• “Press the response button”
• “Electric shock possible. Do not touch patient”
• “Bystanders do not interfere.”
• May replace with external defibrillator after removing Life Vest
• To remove
• First pull battery out
• Then remove vest
64

Zoll Life Vest
65

Case Scenario #1
A patient arrives via EMS with a chief complaint of feeling “under the weather”.
They are responsive, GCS 15, warm and dry, with a capillary refill less than 2
seconds. They have a VAD device.
How will the VAD influence the ability to complete the assessment of vital signs
and ECG for the patient?
Patient may or may not have pulses
No pulses means no blood pressure
The ECG will remain unaffected
66

Case Scenario #2
Your patient is suffering from severe anxiety.
What medications can be administered per CMC EMS Region X SOP’s?
Versed and Valium
What is the dosing parameters and route of administration of these medications?
Versed 2mg IN every 2 minutes, titrate to desired effect to a max dose of
10mg
Valium 5mg IVP over 2 minutes, repeat as needed to max dose of 10mg.
Valium 10mg IM
67

Case Scenario #3
EMS was toned out for a patient who, according to bystanders, “passed out”.
When they arrive they note a blue gel on the patient.
What does this indicate?
Patient is wearing a Life Vest
Your patient remains unconscious. What is the next step in assisting the patient?
If patient is safe to touch, take off Life Vest by removing battery first. Wipe
off blue gel from patient and apply EMS pads.
CPR and ACLS medications as needed.
68

Case Scenario #4
EMS arrives on scene for a morbidly obese patient complaining of difficulty
breathing.
How would their airway assessment change for this patient?
Breath sounds will be difficult to hear through extra adipose tissue
Excess tissue around cheeks, lower jaw and thorax decrease airway patency
Ventilation is more difficult
Intubation will be very difficult or impossible due to patient anatomy
69

Bibliography• Bledsoe, B., Porter, R., Cherry, R. Paramedic Care Principles & Practices, 4th
edition. Brady. 2013.
• Mistovich, J., Karren, K. Prehospital Emergency Care. 9th Edition. Brady. 2010.
• Page, B. Slap the Cap-The Role of Capnography in EMS. 2012.
• Region X SOP’s; IDPH Approved April 10, 2014.
• www.hearthope.com
• www.thoratec.com
• CMC EMS System CE Module August 2015
• Debbaudt, D. Autism Risk and Safety Management, 2011.
• Nixon, L. Universal Care of the Ventricular Assist Device (VAD) Patient,
powerpoint, 2015.
70



















![Patient care [autosaved]](https://img.pdfslide.us/doc/110x75/55d1f481bb61ebff468b4763/patient-care-autosaved.jpg)








