Embed Size (px)
Citation preview

MMV Tenth Anniversary: A Decade of Discovery
Thursday, 12 November 2009Red Cross Museum Geneva
Getting drugs to patients: The challenges of
access and delivery
George Jagoe, MMV Global Access

Is Access really the Final Frontier?
CONFIDENTIAL – MMV internal use only
What’s our greatestchallenge Captain?
It’s Access Mr. Spock – it’s as difficult and
expensive as R&D
Availability
Affordability
Acceptability
Quality
Delivery
Quality
Affordability
Availability
Acceptability

Quality

Quality?
MMV portfolio 3Q’09
Pivotal StudyPreclinicalResearch Translational Development
MK 4815(Merck)
Novartisminiportfolio
GSKminiportfolio
Other Projects13 Projects
DHODHUTSW/UW/Monash
PyridoneGSK
iv artesunateQuilin
ArtemisoneUHKST
GSK 932121GSK
Pyramax®Shin Poong/University
of Iowa
AminoindoleBroad/ Genzyme
PfizerWhole cell screen
OzonideMonash/UNMC/STI
KAE 609Novartis
Lead Opt Phase IIPhase ILead Gen
Whole Cell LeadNovartis
sanofi aventisOrthologue screen
Natural Products5 Projects
P218 DHFR(BIOTEC/Monash/
LSHTM)
TafenoquineGSK
OZ 439(Monash/UNMC/STI)
(+) MefloquineTreague
Coarsucam®sanofi aventis/DNDi
KinasesMonash
QuinolineMethanols
WRAIR
DHODHBroad/Genzyme
Whole Cell Hits St Jude/Rutgers
Broad/ Genzymeminiportfolio
Coartem®-DNovartis
Registration
Eurartesim™sigma-tau
Quality – We Get It

Quality – A universal acceptance?
Health Impact
Supporting adoption
Expanding reach Shaping R&D
Health Impact
ACCEPTANCE EXPANSIONMeasure /Evaluate /Feedback
MMV’s Strategic Columns of Access & Delivery

Affordability

Affordability?
Guarantee It….
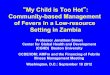
• August 2009 -- Novartis announces third price reduction for public sector buyers of Coartem since 2006
• Coartem is now 50% lower in price than it was in 2006
• Guarantee of 100 million treatment annual mfg capacity
• Coartem Dispersible - Youngest patients – $0.36 / treatment
• A Promise, a Guarantee

CSR Matters – and so does economics
Coartem Price-Volume, 2004-2009
0
10
20
30
40
50
60
70
80
90
2004 2005 2006 2007 2008 2009 (?)
mill
ion
tx
-
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
1.80
usd
pric
e / t
x
treatmentsprice
?

Affordability?
Study It….
Product PriceACTs 3.00 - 9.00Artemisinin mono 3.00 - 24.00Amodiaquine 0.24 - 0.48Chloroquine 0.12 - 0.30SP 0.30 - 0.60Quinine 2.50

Affordability?
Hypothesize an Answer
Masindi
Nakasongola
Kasese
Hoima
Kibaale
Kiboga
Luwero
Apac
MukonoKAMPA
LA
Mubende
Kabarole
Nebbi
Arua
Gulu
Adjumani
Kabale
Mbarara
Rakai
Sembabule Mas
aka
Kalangala
Iganga
Busia
Mle
Tororo
Kapc
hor
wa
Pallisa
Kumi
Katakwi
Moroto
Kotido
Kitgum
Soroti
Lira
Mpigi
Bushenyi
Rukungiri
Kamuli
Ntungamo
Moyo
SUDAN
KENYA
TANZANIARWANDA
Kamwenge
Kyenjojo
Knga
Kanungu
Yumbe
Pader
Sironko
NakapiripiritKma
ido
BugiriMay
uge
DEMOCRATIC REPUBLIC
CONGO
Kisoro
Wakiso
Jinja
Fort Portal
Bukedea
Kiru
hur
aIban
da
Isingiro
Bud
aka
Butaleja
Nak
ase
ke Kaliro
= 6 Interventiondistricts**
= 2 Controldistricts***
Study areas: Total population 3 million

Affordability?
Document ItIs the solution suggested by the AMFmworkable and relevant? …Is this a good use of resources? … Where is the evidence?...
Evidence is available from two pilot studies in Tanzania and Uganda in 2007–08 and 2008–09, respectively. Both studies have informed the design of the AMFm.
Let us take the example of Uganda.

• Nov 10 2009 – Global Fund Board approves funding forPhase One AMFm country proposals
• A major public health experiment• Intensive country consultation from Nov 08 to Jul 09• 11 Countries submitted proposals.
MMV:
• Co-developed Uganda & Senegal proposals.
• Supported CHAI and AMFm secretariat in devisinginformation and comms outreach
• Advised GF in M&E design and final RFP reviews
• Extensive contributions to HWG
Affordability? We Hope We Get It
Don’t be afraid to try for BHAGs* (but be smart too)
* Big Hairy Audacious Goals – JCollins and JPorras in Built to Last

Availability

Availability in General?
Who got the drugs there, what incentivizes them?

In Public Sector….Availability?

In Public Sector….Availability? And…Correct Use / Good Case Management?

CQ pilots
ACT pilots
RDT pilots
Inclusion in ICCM
Evolution of HBMF Programs and Research Focus
• Goal:• Evaluate the process by
which HBMF can be effectively implemented in rural settings
• Goal:• Determine whether ACTs
can be appropriately distributed and used within existing HBMF structures
• Goal: • Assess RDT quality• Determine whether CHWs
can effectively utilize RDTs to distinguish cases requiring ACT treatment
• Challenges identified:• Lack of compelling product• Community acceptance
(esp. in absence of treatments for negative test results)
• Potential for many false positives in endemic areas
• Goal: • Integrate CHW-delivered
community health activities• Provide range of treatments
for all major childhood diseases
• Challenges identified:• Lack of plan for expanding
CHW training and managing drug supply
• Should CHWs be trusted to manage multiple resistance-prone therapies (including antibiotics)?
1998 - 2003Beginning in mid-2000’s
Beginning in 2007-2008
Gaining focus in 2009-2010
CQ = chloroquine; ACT = artemisinin-based combination therapy; RDT = rapid diagnostic test; ICCM = integrated community case management
• Challenges identified:• Need for community buy-in• Importance of prepacking• CHW incentive structures and
attrition rates• Need for simple training materials
and re-training on ACTs
Best-known: Burkina Faso, Ghana, Nigeria, Uganda E.g., Sudan, Zambia 17 countries (PSI/TDR, others)
Availability….Innovation to last mile?

As of 2009, most countries have included HBMF in their national malaria control strategic plans
Some HBMF efforts discussed or planned*
HBMF using ACTs – pilot stages
HMM using ACTs + RDTs – scaling up
Malawi
Some HBMF implementation
HBMF using ACTs – scaling up
Status of HBMF Program ImplementationNiger
Ghana
Ethiopia
KenyaUganda
Tanzania
ZambiaAngola
Namibia
South Africa
Mali
BurkinaFaso
Moz
ambi
que
Senegal
Zimbabwe
Botswana
DR Congo
Somalia
SudanChad
CAR
GabonCongo
Cameroon
Nigeria
BeninGuinea
SierraLeone
Liberia
Coted’Ivoire
TogoM
adag
asca
r
Zanzibar
Gambia
Rwanda
Mauritania
South Sudan
Eq. Guinea
Guinea Bissau
No known HBMF efforts or plans to date
* E.g., mention in NMCP plan, request for funds in recent round of Global Fund or PMI (but details of implementation not known)
Burundi
AL is current 1st line treatment in national guidelines
Comoros
HBMF using ACTs + RDTs – pilot stages
DjiboutiEritrea
Mauritius
Swaziland
Lesotho
Note: Refer to file “HBMF Countries database_Sept09.xls” for details and full citations.
However, the status of existing and planned HBMF initiatives is highly variable across countries, with few having achieved significant scale to date

Acceptability

Acceptability? Do we make it easy to understand…. For moms?

Acceptability? Do we make it easy to understand…. For health workers?

Acceptability? Do we listen to…
• The Voice of the Policy Makers globally and nationally?• Malariologists, Reseachers and other KOLs?• National Logisticians and Central Medical Stores?• Funding Partners?• Patients

Acceptability? And when they say…
• We Need Simpler Dosing?• Longer-lasting protection?• Specially suited for pregnant moms?• Severe malaria?• New tools for IPTx?

Access… the Final Frontier…? Tell Me What You See….

The Mission / Vision helps clear the fog
MMV A&D’s VisionA world where free or easily affordable quality medicines that MMV has helped develop are always available to treat and when appropriate prevent malaria, wherever it occurs.
MMV A&D’s MissionTo ensure that medicines which MMV has helped develop are available in key malaria-endemic countries to a sufficient extent that they deliver a major health impact.

And in the end… a picture is worth one thousandwords. Voilà – the simple access ambition