-
7/31/2019 mjms-18-2-040
1/7
www.mjms.usm.my Penerbit Universiti Sains Malaysia, 2011For
permission, please email:[email protected]
Abstract
Background:Knee proprioception is compromised in knee
osteoarthritis. There are severalways of measuring proprioceptive
acuity, but there is lack of consensus over the ideal
testingposition. The study aimed to evaluate the inuence of 2
testing positions (sitting versus prone lying)on proprioceptive
knee assessment score in patients with early knee
osteoarthritis.
Methods:The study included 70 subjects who came to the
Out-Patient Department with adiagnosis of early knee
osteoarthritis. The subjects were assessed for their proprioceptive
acuityscores in both the test positions at 30 and 60 of knee exion
using proprioceptive knee assessmentdevice. They were asked to
perform 5 trials in both testing positions with appropriate rest
intervals.After initial assessment, the subjects were randomly
allocated among group 1 and group 2. Treatmentimplementation was
done for 8 weeks followed by re-evaluation: group 1 received
context-specicproprioceptive retraining along with multijoint
coupling strategies and group 2, conventionaltreatment.
Results: The subjects were compared using difference of pre- and
post-treatmentproprioceptive acuity scores. The difference of
proprioceptive acuity impairment scores of the leftknee at 30 and
60, and the right knee at 60 in prone lying position were
statistically signicant,withPvalue ranging from less than 0.001 to
0.028.
Conclusion: It was found that the prone lying testing position
was more sensitive than sittingposition for assessing
proprioceptive acuity for knee osteoarthritis.
Keywords:adaptive behavior, knee, patient positioning,
proprioception, osteoarthritis
Original Article Inuence of Sitting and Prone Lying Positionson
Proprioceptive Knee Assessment Score inEarly Knee
Osteoarthritis
VijayBatra1
, Vijai Prakash Sharma1
, Meenakshi Batra1
,Girdhar Gopal agarwal2, Vineet Sharma3
1 Department of Physical Medicine and Rehabilitation,
Rehabilitation andArticial Limb Centre, Chhatrapati Shahuji Maharaj
Medical University(Formerly King George Medical University), Dali
Ganj Bridge, Nabiullah Road,
Lucknow: 226018, Uttar Pradesh, India
2 Department of Statistics, Lucknow University, Lucknow:226 007,
India
3 Department of Orthopaedics, Chhatrapati Shahuji Maharaj
MedicalUniversity (Formerly King George Medical University), Dali
Ganj Bridge,
Nabiullah Road, Lucknow: 226018, Uttar Pradesh, India
Submitted:9 Mar 2010Accepted:28 Aug 2010
IntroductionProprioception is the sense of position and
movement of the limbs, and it is the result ofsensory inputs
arising from muscle, skin, andjoint structures (1). It can also be
dened as theconscious and unconscious awareness of bodyposition,
movement, and forces acting on thebody, for which accurate sensory
input and centralintegration from peripheral proprioceptors area
must (2). Proprioception contributes to thedevelopment of the motor
control and plays amajor role in the reex protection of joints
againstpotentially harmful forces (1). The proprioceptiveacuity
impairment signicantly affects
neuromusculoskeletal integrity, contributingto pain and
functional disability (24). Kneeproprioception has consistently
been reportedto be compromised in individuals with
kneeosteoarthritis (3,511). This neuromuscular decithas been
suggested as the major contributingfactor to the disease process
(7,1013). However,studies have shown that the impairment
ofproprioceptive acuity is not exclusively a localresult of the
disease, and there is a need to study itsimportance in the
development and progressionof knee osteoarthritis (10,11).
40Malaysian J Med Sci. Apr-Jun 2011; 18(2): 40-46
mailto:%20vijaybatra%40yahoo.com?subject=mailto:%20vijaybatra%40yahoo.com?subject=mailto:%20vijaybatra%40yahoo.com?subject=mailto:%20vijaybatra%40yahoo.com?subject=mailto:%20vijaybatra%40yahoo.com?subject=
-
7/31/2019 mjms-18-2-040
2/7
Original Article | Proprioceptive assessment in Knee
Osteoarthritis
www.mjms.usm.my 41
There are several ways of measuringproprioceptive acuity; one of
them is the thresholddetection of passive movement. However,
passivemovements do not reect real life movement orfunction;
proprioceptive functions in healthyand pathological joints are
quite variable andthere is a lack of correlation between
differentmeasurements of proprioception in the knee(1417). Active
assessments by asking the patientto replicate limb position, using
active movement,with vision occluded (16) or by reproducinglower
limb static loads (15) have been suggested.Generally,
proprioceptive assessment of the kneeis done in sitting position
(16). However, the idealtesting position for proprioceptive
assessmentof the knee is still debatable. One of the reasonscould
be that, during assessment, the subject
may exhibit an adaptive behaviour to compensatefor the loss of
proprioceptive acuity by usingvision or not relaxing the muscles
completelybefore attempting to replicate limb position. Thepurpose
of the present study was to evaluate theinuence of 2 testing
positions (sitting and pronelying) on proprioceptive acuity scores
(17) in theassessment of early knee osteoarthritis.
Subjects and Methods
The study involved 70 subjects (22 males
and 48 females) with history of knee pain andclinical diagnosis
of early knee osteoarthritis,with radiological ndings of grade I
(33 subjects)and grade II (37 subjects) according to theKellgren
and Lawrence Classication System(18). All patients were between 40
and 60 yearsof age. Subjects with traumatic knee injury,inammatory
arthritis, metabolic disorder, aswell as cardiovascular and
psychiatric illnesseswere excluded from the study.
The ethical approval was obtained from TheHuman Ethical
Committee of Chhatrapati ShahujiMaharaj Medical University
(formerly KingGeorge Medical College), Lucknow. Informedconsent was
obtained from the patient or theaccompanying family member.
The baseline evaluation of all the subjectswas done in 2 testing
positions (sitting and pronelying) for proprioceptive acuity score
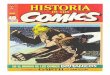
(17) usingproprioceptive knee assessment device. Thedevice
comprises a goniometer attached witha static bar and a movable set
of 5 bars that arexed, with respect to each other, at 10
interval.The central bar of the movable set of 5 bars islonger than
the other 4 bars (2 on each side).
The central mechanical axis of the goniometercoincides with the
anatomical axis of knee joint.
The static bar corresponds to the 90 of kneeexion, perpendicular
to the ground. The centralbar was positioned at the desired angles,
i.e., 30and 60 of knee exion (Figure 1). Any deviationfrom the
central bar was treated as an error.
With vision occluded, each subject was asked
to perform 30 and 60 exion of each knee for 5times, with
intermittent rest intervals of at least1015 seconds. Proprioceptive
impairment wascalculated by adding the proprioceptive acuityscores
of all the 5 attempts for each knee (Table 1).
Our main objective is to compare the2 test positions; thus, to
rule out the possibilityof results being inuenced by certain
treatments,the subjects were randomly allocated among 2intervention
groups (group 1 and group 2) with35 subjects in each arm. The mean
age was notsignicantly different between the 2 groups; themean age
for group 1 was 50.14 years (SD 5.49),
while for group 2, it was 51.15 years (SD 5.9). Ingroup 1,
context-specic proprioceptive retrainingalong with multijoint
coupling strategies (17) wasused, while for group 2, conventional
treatmentwas used. Test position 1 (sitting) was consideredas
control while test position 2 (prone lying) wasconsidered as
experimental.
The context-specic proprioceptive retrainingtechnique
incorporated both neurophysiologicaland biomechanical procedures
and techniques toinuence neuromusculoskeletal integrity (12,1821)
within functional context using facilitatory and
inhibitory procedures, sensorimotor experiences,procedures to
enhance dynamic adjustment
Figure 1: Proprioceptive assessment device.
-
7/31/2019 mjms-18-2-040
3/7
42 www.mjms.usm.my
Malaysian J Med Sci. Apr-Jun 2011; 18(2): 40-46
range, coupled motions of knee, hip, and anklejoints, and
multijoint coupling strategies (17).The conventional treatment
incorporated jointreproducibility with and without vision
occluded,quadriceps strengthening using isometric andisotonic
exercises, physical agent modalities,manual therapy, mobilization,
and manipulation.
The subjects in each group receivedintervention 3 times per week
for 30 minutes persession. At the end of 8 weeks of intervention,
eachsubjects proprioceptive acuity was reassessed
in both knees at each angle in both testingpositions (17).
Test position 1 (sitting)Each subject was asked to sit over the
plinth
with hip at 90 of exion and knee relaxed andsuspended off the
plinth in gravity-dependentposition. Both knees were assessed
separately.Initially, the subject was asked to relax for 5minutes.
Then, the knee was passively positionedby a therapist using
proprioceptive assessmentdevice in 30 of exion, and the subject
wasinstructed to replicate the same knee position.The subject was
asked to perform 5 trials withintermittent rest intervals of 10 to
15 secondseach. The other knee was also assessed by usingthe same
procedure. The similar sequence wasfollowed, for each knee
separately, at 60 ofexion.
Test position 2 (prone lying)The subject was asked to lie in
prone position
while keeping both the hip and knees neutral (i.e.,hip in 0 of
exion or extension, 0 of abduction oradduction, and 0 of internal
or external rotation;
knee in full extension). The testing procedure wassame as the
procedure for position 1 (sitting).
Statistical analysisIn order to adjust for the discrepancies
in
baseline characteristics, the differences of pre-and
post-proprioceptive acuity scores were usedfor analysis. Some of
these differences werenegative and skewed. Therefore, a
logarithmictransformation of the form ln (x + c) was used,where c
is a suitably chosen positive constant.Students ttest was performed
on the transformeddata. For asymmetrically distributed
variables,non-parametric MannWhitney U test was
used.Pvalue of less than 0.05 was considered asstatistically
signicant.
Results
All 70 subjects, irrespective of the treatment,were analyzed for
their various acuity scores inthe 2 testing positions.
Between-group analysisStudents t test was used for the
analysis
of proprioceptive acuity scores of the left kneeat 30 and 60,
and the right knee at 60;MannWhitney U test was used for the right
kneeat 30. The mean for sitting position for the left kneeat 30 and
60, and the right knee at 60 were 1.498(SD 0.062), 1.515 (SD
0.075), and 1.509 (SD0.072), respectively. The mean for prone
lyingposition for the left knee at 30 and 60, and theright knee at
60 were 1.534 (SD 0.059), 1.549 (SD0.069), and 1.55 (SD 0.066),
respectively. Themedian and interquartile range in sitting
positionfor the right knee at 30 was 1.491 and 0.063,and for prone
lying position, 1.505 and 0.071,respectively. The P values at 95 %
condence
interval for the change in proprioceptive acuityscores of the
left knee at 30 (P < 0.001), the
Table 1: Proprioceptive knee assessment scoring system
Score Description
1 Normal
2 Patient overshoots or undershoots the target by more than 10
but canacquire the target position
3 Patient overshoots or undershoots the target by more than 30
but can
acquire the target position
4 Patient overshoots or undershoots the target by more than 10
and
cannot acquire the target position
5 Patient overshoots or undershoots the target by more than 30
and
cannot acquire the target position
6 Impaired
-
7/31/2019 mjms-18-2-040
4/7
Original Article | Proprioceptive assessment in Knee
Osteoarthritis
www.mjms.usm.my 43
left knee at 60 (P = 0.007), and the right kneeat 60 (P<
0.001) were found to be statisticallysignicant (Table 2).
Between-group analysisThe subgroup analyses were also done to
ruleout the treatment effect. Students ttest was usedfor the
analysis of proprioceptive acuity scores ofthe left knee at 30 and
60, and the right knee at60; MannWhitney U test was used for the
rightknee at 30.
The mean proprioceptive acuity score forsitting position (group
1) for the left knee at 30and 60, and the right knee at 60 were
1.532 (SD0.049), 1.564 (SD 0.043), and 1.554 (SD
0.041),respectively. In prone lying position, the valueswere 1.568
(SD 0.051), 1.598 (SD 0.043), and
1.598 (SD 0.040), respectively. The median andinterquartile
range in sitting position for the rightknee at 30 was 1.519 and
0.039; for prone lyingposition, they were 1.531 and 0.051,
respectively(Table 3). The changes in proprioceptive acuityscores
of the left knee at 30 (P= 0.004), the leftknee at 60 (P= 0.002),
and the right knee at 60(P< 0.001) were statistically signicant,
whereasno signicant difference was observed for theright knee at 30
(P= 0.068) (Table 3).
The mean proprioceptive acuity score forsitting position (group
2) for the left knee at 30
and 60, and right knee at 60 were 1.464 (SD0.055), 1.467 (SD
0.069), and 1.464 (SD 0.068);for prone lying position, the mean
values were1.501 (SD 0.047), 1.500 (SD 0.052), and 1.502 (SD0.051),
respectively. The median and interquartilerange in sitting position
for the right knee at 30was 1.462 and 0.076; for prone lying
position, theywere 1.477 and 0.044, respectively.The changes
inproprioceptive acuity scores of the left knee at 30(P= 0.004),
the left knee at 60 (P= 0.028), andthe right knee at 60 (P= 0.009)
were statisticallysignicant, whereas no signicant difference
wasobserved for the right knee at 30 (P = 0.162)(Table 4).
Discussion
Based on the analyses, null hypothesisstating that both sitting
and prone lying positionsare equally effective for assessing
proprioceptiveacuity impairment in knee osteoarthritis can
berejected; the prone lying test position was found tobe more
sensitive than the sitting position in mostof the components. The
results can be explainedbased on the neurophysiological mechanism
of
neuromuscular control system.
In early knee osteoarthritis, the kneejoint complex is richly
innervated withmechanoreceptors, such as receptors in the
joint,skin, and muscle (22,23). The combination of
both muscle and joint receptors forms an integralcomponent of a
complex sensorimotor system thatplays a major role in the
proprioceptive mechanism(24,25). Mechanoreceptors can be
quick-adaptingand slow-adapting, and they have differentshapes,
threshold levels, locations, and adaptiveproperties based on their
response to stimuli(23,2527). Quick-adapting
mechanoreceptorsmediate the sensation of joint motion, whereasthe
slow-adapting mechanoreceptors mediate thesensation and change in
joint position (22,23). Theproprioceptive mechanism, which is
initiated byactivation of these mechanoreceptors, has direct
implication over proprioceptive acuity score ofthe knee. Since
proprioceptive acuity score of eachknee has a combined effect over
the functionalstatus, in the present study,
proprioceptiveimpairment of each knee was assessed separatelyto
identify the ideal test position.
Statistical analysis showed mixed results,but the prone lying
position was found to be moresensitive for assessing proprioceptive
acuity statusthan the sitting position. In prone lying, the kneearc
of motion starts from extension to exion, withboth knees and hip in
neutral; the direct inuence
of gravity and the effect of diarthodial muscles arenullied, and
the length feedback is controlled ina better manner. As a result,
mechanoreceptors(especially slow-adapting) do not get
stimulated,and the knees can be fully relaxed. On the otherhand, in
sitting position, the hip and the knees arein 90 of exion, and the
knee arc of motion startsfrom 90 knee exion to extension. In
addition,the muscles around knee, being diarthodial, areunder the
direct inuence of gravity, and themuscle stretch reex activity may
get stimulated.The proprioceptive acuity scores obtained insitting
position may not represent the actualproprioceptive acuity status
of each knee.
Motor control relies on inputs fromproprioceptors, visual
receptors (telereceptors),and vestibular receptors. When
kneeproprioceptive acuity gets impaired, the subjectmay exhibit
adaptive behaviours (23,25,26) toaccommodate proprioceptive decit
by relying onvision or not allowing the muscles to get
relaxedbefore attempting to replicate limb position. Inthe present,
study this adaptive behaviour wasdrastically minimized by occluding
the visionand incorporating intermittent rest intervals.
However, in prone lying position, the reliance
-
7/31/2019 mjms-18-2-040
5/7
44 www.mjms.usm.my
Malaysian J Med Sci. Apr-Jun 2011; 18(2): 40-46
on vision and muscle tension as well as the effectof diarthodial
muscles on the proprioceptiveacuity could be ruled out. Both test
positionswere equally sensitive in the assessment ofproprioceptive
acuity for the right knee at 30.Therefore, each test position is
useful in differentmethods of assessment. Since onset of
kneeosteoarthritis is usually unilateral and may laterprogress
bilaterally, the proprioceptive acuityscores of each knee can guide
the treatment
process. Hence, the null hypothesis was rejected.
Conclusion
The prone lying position is more sensitive thanthe sitting
position in assessing proprioceptiveacuity of each knee and
identifying the actualproprioceptive impairment status. Prone
lyingposition could serve as an effective evaluation toolto guide
the treatment process in patients withearly knee
osteoarthritis.
Table 2: Comparison of the changes in proprioceptive acuity
scores (pre- and post-interventionbetween sitting and prone lying
positions
ProprioceptiveAcuity
Left Knee Right Knee
30a
60a
30b
60a
Sitting position 1.498 (0.062) 1.515 (0.043) 1.491 (0.063) 1.509
(0.072)
Prone lying position 1.534 (0.059) 1.549 (0.685) 1.505 (0.071)
1.550 (0.066)
Test statistics (df) -3.525 (138) -2.741 (138) -1.576 -3.532
(138)
Pvalue
-
7/31/2019 mjms-18-2-040
6/7
Original Article | Proprioceptive assessment in Knee
Osteoarthritis
www.mjms.usm.my 45
Acknowledgements
We are thankful to the Indian Council forMedical Research for
their nancial support.
Authors Contributions
Conception and design, collection and assemblyof the data: VB,
MBDrafting and nal approval of the article: VB,VPS, MB,
VSStatistical expertise: GGA
Correspondence
Dr Vijay Batra
PhD Occupational Therapy (Chhatrapati Shahuji
Maharaj Medical University)Department of Physical Medicine &
Rehabilitation
Rehabilitation and Articial Limb CentreChhatrapati Shahuji
Maharaj Medical University(Formerly King George Medical
University)
Dali Ganj Bridge, Nabiullah RoadLucknow: 226018Uttar Pradesh,
India
Tel: +91-9868019077, +91-9044467434Email:
[email protected],
[email protected]
References
1. Gandevia SC. Kinesthesia: Roles for afferent signalsand motor
commands. In: Rowell LB, ShepardJT, editors. Handbook on
integration of motor,circulatory, respiratory and metabolic control
duringexercise. Bethesda, MD: American PhysiologicalSociety; 1996.
p. 128172.
2. Riemann BL, Lephart SM. The sensorimotor system,part I: The
physiologic basis of functional jointstability.J Athl Train.
2002;37(1):7179.
3. Felson DT, Gross KD, Nevitt MC, Yang M, Lane NE,Torner JC, et
al. The effects of impaired joint positionsense on the development
and progression of pain andstructural damage in knee
osteoarthritis. Arthritis
Rheum. 2009;61(8):10701076.
4. Bennell KL, Hinman RS, Metcalf BR, CrossleyKM, Buchbinder R,
Smith M, et al. Relationship ofknee joint proprioception to pain
and disability inindividuals with knee osteoarthritis. J Orthop
Res.2003:21(5):792797.
5. Barrett DS, Cobb AG, Bently G. Joint proprioceptionin normal,
osteoarthritic and replaced knees. J Bone
Joint Surg. 1991;73(1):5356.
6. Garsden LR, Bullock-Saxton JE. Joint repositionsense in
subjects with unilateral osteoarthritis of theknee. Clin Rehabil.
1999;13(2):148155.
7. Hurley MV, Scott DL, Rees J, Newham DJ.Sensorimotor changes
and functional performancein patients with knee osteoarthritis.Ann
Rheum Dis.1997:56(11):641648.
8. Marks R. Further evidence of impaired position
sense in knee osteoarthritis. Physiother Res
Int.1996;1(2):127136.
9. Pai YC, Rymer WZ, Chang RW, Sharma L. Effectof age and
osteoarthritis on knee proprioception.
Arthritis Rheum. 1997;40(12):22602265.
10. Sharma L, Pai YC. Impaired proprioception andosteoarthritis.
Curr Opin Rheumatol. 1997;9(3):253258.
11. Sharma L, Pai YC, Holtkamp K, Rymer WZ. Is kneejoint
proprioception worse in the arthritic knee versusthe unaffected
knee in unilateral knee osteoarthritis?
Arthritis Rheum. 1997;40(8):15181525.
12. Hurley MV, Scott DL. Improvement in quadricepssensorimotor
function and disability of patients withknee osteoarthritis
following a clinically practicableexercise regime. Br J Rheumatol.
1998:37(11):11811187.
13. Salo P. The role of joint innervation in the pathogenesisof
arthritis. Can J Surg. 1999;42(2):91100.
14. Grob KR, Kuster MS, Higgins SA, Lloyed DG, Yata H.Lack of
correlation between different measurementsof proprioception in the
knee. J Bone Joint Surg Br.2002:84(4):614618.
15. Murtaugh K, Costigan PA, Evaluating theproprioception of
lower extremity loads. Winter.
2003:6(2):1519.
16. Olson L, Lund H, Henriksen M, Rogind H, BliddalH,
Danneskiold-Samsoe B. Testretest reliabilityof a knee joint
position sense measurement methodin sitting and prone position. Adv
Physiother.2004;6(1):3747.
17. Batra V, Sharma VP, Batra M, Agarwal GG, Sharma
V.Multi-joint coupling strategies to enhance functionalrecovery in
knee osteoarthritis.Ind J Phys Occ Ther.Forthcoming.
18. Hochberg MC, Altman RD, Brandt KD, Clark BM,Dieppe PA, Grifn
MR, et al. Guidelines for the medicalmanagement of osteoarthritis.
Part I. Osteoarthritis of
the hip. American College of Rheumatology.ArthritisRheum.
1995;38(11):15351540.
19. Hurley MV. Muscle dysfunction and effectiverehabilitation of
knee osteoarthritis: What we knowand what we need to nd out.
Arthritis Rheum.2003;49(3):444452.
20. Farina D, Arendt-Nielsen L, Graven-Nielsen T.Experimental
muscle pain reduces initial motorunit discharge rates during
sustained sub maximalcontractions.J Appl Physiol.
2005;98(3):9991005.
21. Smania N, Picelli A, Romano M, Negrini S.Neurophysiological
basis of rehabilitation ofadolescent idiopathic scoliosis. Disabil
Rehabil.
2008;30(10):763771.
-
7/31/2019 mjms-18-2-040
7/7
46 www.mjms.usm.my
Malaysian J Med Sci. Apr-Jun 2011; 18(2): 40-46
22. Sekir U, Gur H. A multi-station proprioceptiveexercise
program in patients with bilateral kneeosteoarthrosis: Functional
capacity, pain andsensorimotor function. A randomized controlled
trial.
J Sports Sci Med. 2005:4:590603.
23. Williams GN, Chmielewski T, Rudolph K, BuchananTS,
Snyder-Mackler L. Dynamic knee stability: Currenttheory and
implications for clinicians and scientists.JOrthop Sports Phys
Ther. 2001;31(10):546566.
24. Dixon J, Howe TE. Quadriceps force generationin patients
with osteoarthritis of the knee andasymptomatic participants during
patellar tendonreex reactions: An exploratory cross-sectional
study.
BMC Musculoskelet Disord. 2005:6:46.
25. Houk JC. Regulation of stiffness by skeletomotorreexes.Annu
Rev Physiol. 1979:41:99114.
26. Houk JC, Rymer WZ. Neural control of muscle lengthand
tension. In: Brooks VB, editor. Handbook of
physiology: Section I. The nervous system. Volume 2:
Motor control. Bethesda, MD: American PhysiologicalSociety;
1981. p. 257323.
27. Nichols TR, Cope TC, Abelew TA. Rapid spinalmechanisms of
motor coordination. Exerc Sport Sci
Rev. 1999:27:255284.