Embed Size (px)
Citation preview

2016/10/13
1
Saibal Kar, MD, FACC, FAHA, FSCAI
Director of Interventional Cardiac Research
Heart Institute, Cedars-Sinai Medical Center,
Los Angeles, CA
Mitral Valvular Disease: An explosion ofmultiple new non-surgical options
Disclosure Statement of Financial InterestSaibal Kar, MD, FACC
• Grant/Research Support
• Consulting Fees/Honoraria
• Other Financial Benefit
• Abbott Vascular,Boston Scientific, StJude Medical, Gore Medical
• Abbott Vascular, Boston Scientific,St Jude Medical, Gore
Within the past 12 months, I or my spouse/partner have had a financialWithin the past 12 months, I or my spouse/partner have had a financialinterest/arrangement or affiliation with the organization(s) listed below.interest/arrangement or affiliation with the organization(s) listed below.
Affiliation/Financial Relationship Company
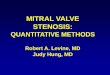
Mitral valve apparatus• Mitral valve is an apparatus rather than a single structure
and each of the components may cause MV malfunction.
Posterolateralcommissure
Posteriorannulus
Anterolateralpapillary
muscle
Anterior annulus Anterior leaflet Anteromedialcommissure
Posteriorleaflet
Chordaetendineae
Posteromedialpapillarymuscle
Left ventricularfree wall
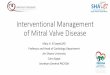
Functional Mitral Regurgitation
Otto N Engl J Med 2001:345:740-746
Mitral Regurgitation (MR)
Primary Disorder of the MitralValve Apparatus (annulus,
leaflets, chords, papillary muscle
Functional MR: Leafletsappear normal, MR due to
abnormal LV geometry
Valve makes the VentricleSick
Ventricle makes the ValveSick
Mechanical Solution: OpenSurgical /Transcatheter
repair/replacement
Medical treatment for LVdysfunction
Mechanical reduction ofMR ?
PercutaneousMitralApproaches
• Leaflet repair• MitraClip® ( Abbott Vascular )
• Leaflet folding( St Jude Medical)
• Coronary sinus annuloplasty• Cardiac Dimensions Carillon
• Direct annuloplasty• Mitralign Suture-Based Plication• Guided Delivery Anchor-Cinch Plication• Quantum Cor• Cardioband (Valtec Cardio, Or Yehuda, Israel)
• Chordal replacement• NeoChord, V-Chordal(Valtec)• MitraFlex
• Transcatheter Mitral ValveReplacement
Standard ofCare
Emergingoptions
PercutaneousMitralApproaches
• Leaflet repair• MitraClip® ( Abbott Vascular )
• Leaflet folding( St Jude Medical)
• Coronary sinus annuloplasty• Cardiac Dimensions Carillon
• Direct annuloplasty• Mitralign Suture-Based Plication• Guided Delivery Anchor-Cinch Plication• Quantum Cor• Cardioband (Valtec Cardio, Or Yehuda, Israel)
• Chordal replacement• NeoChord, V-Chordal(Valtec)• MitraFlex
• Transcatheter Mitral ValveReplacement
Standard ofCare

2016/10/13
2
MitraClip
• Concept
• Technical aspects
• Case selection
• Longterm data
Concept: Edge to Edge repair(Alfieri stitch)
•• Simple solution forSimple solution fora complex problema complex problem
•• Selected patientsSelected patientsof degenerativeof degenerativeand functional MRand functional MR
•• Not effective inNot effective inrheumatic MRrheumatic MR
MitraClip Creation of double orifice valve
MitraClip Concepts
• Coaptation of Leaflets• Reduces MR
• Creates tissue bridge• Limits dilatation of annulus• Septal-lateral (A-P) dimension• Supports durability of repair
• Restrains LV wall• Limits LV dilatation
MitraClip
• Concept
• Technical aspects
• Case selection
• Longterm data

2016/10/13
3
Case Selection: Suitable Anatomy
• Non rheumatic MR originatingfrom a localized area of thevalve
• Etiology: degenerative orfunctional
• Sufficient leaflet tissue formechanical coaptation
• Valve anatomic exclusions• Flail gap >10mm• Flail width >15mm• Calcified leaflet
• MVA ≥ 4 sq cm
Expanded indications of the MitraClip:Beyond the EVEREST criteria
• A1P1 or A3P3 flail or prolapse
• Failed surgical repair
– Ring annuloplasty, or snapping of artificialchord
• HOCM : Systolic anterior motion with MR
• End stage heart failure with MR
– Delay heart transplantation or VAD
Flail P2/P3segment
MitraClip for aFlail P2/P3
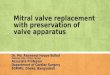
MitraClip Therapy Worldwide Experience(2003-2016)
> 35000 Cases
30| June | 2016
GLOBAL MITRACLIP EXPERIENCE
1. Includes clinical and commercial procedures as of 06/30/2016. Source: Data on file at Abbott Vascular
1200 cases in month of June

2016/10/13
4
Clinical summary using MitraClip
• > 35,000 cases performed worldwide
• Most patients are high surgical riskpatients
• In US
– Oct 2013: FDA approved the MitraClip forprohibitive risk primary MR (degenerative)
– Functional MR: Investigational
– Ongoing clinical trials for Functional MR .
Key MitraClip Data
• Safety
– Impeccably safe in experienced hands
– No early or late safety events
• Effective
– Selected patients with both degenerative orfunctional MR
• Durability
– New data supports durability .
Freedom From Mortality andMV Surgery/Re-operation
Kaplan-Meier Freedom FromMitral Valve Surgery/Re-operation
Kaplan-Meier Freedom FromMortality
EVEREST II RCT
Feldman et al ACC 2014
EVEREST II 5 year: Sustained reduction ofMR
N=149 N=106 N=66 N=41
p<0.005 p<0.00581% 82% 99% 98%
MitraClip (N=178)MR ≤ 2+ at 1 and 5 Years
Surgery (N=80)MR ≤ 2+ at 1 and 5 Years
4+
4+
4+
4+
3+
3+
3+
3+
2+
2+
2+
2+
1+ 1+
0+ 0+
0%
20%
40%
60%
80%
100%
BL 1 Year BL 5 Years
Pa
tie
nts
(%)
4+ 4+
3+
3+
3+
3+
2+
2+
2+
2+
1+1+
0+ 0+
0%
20%
40%
60%
80%
100%
BL 1 Year BL 5 Years
Pa
tie
nts
(%)
p<0.005 p<0.005
EVEREST II RCT
Feldman et al ACC 2014
MitraClip in High Risk patients
Final 5 Year Results of theEVEREST II High Risk Registry

2016/10/13
5
MR Grade and NYHA Functional Class
4+
4+
4+
3+
3+
3+
3+
2+
2+2+
1+1+
0%
20%
40%
60%
80%
100%
BL 1 Year BL 5Years
Pa
tie
nts
(%)
N=54 N=24
Mitral Regurgitation Grade NYHA Functional Class
p < 0.005 p = 0.01
IV
IV
IV
III
III
III
III
II
II
II
II
II
0%
20%
40%
60%
80%
100%
BL 1 Year BL 5 Years
Pa
tie
nts
(%)
N=54 N=24
p < 0.005 p = 0.00678% 75% 74% 83%
EVEREST II HRR
Kar et al ACC 2014
REALISM ( degenerative MR Cohort)
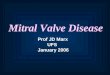
Freedom From MV Surgery in DMR:EVEREST II RCT, REALISM Non-High Risk and REALISM High Risk
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
30 Days98.9%95.6%90.0%
1 Year97.8%89.9%75.1%
REALISM High Risk DMR
EVEREST II RCT DMR MitraClip
REALISM Non-High Risk DMR
# At Risk Baseline 30 Days 6 Months 12 Months
High Risk DMR 189 176 159 121
Non-High Risk DMR 185 173 162 151
RCT DMR MitraClip 130 117 98 92
Eve
nt
Fre
eS
urv
ival
Kar et al ESC 2015
Learning Curve Experience inthe MitraClip REALISM Trial:
An Analysis of 899 High Risk andNon-High Risk Subjects
See Important Safety Information Referenced Within. Not to be reproduced, distributed or excerpted.
©2015 Abbott. All rights reserved. AP2941763-US Rev. A
Acute Procedural Success Rate
79% 81% 80%93%
0%
20%
40%
60%
80%
100%
Cohort A(n=354)
Cohort B(n=250)
Cohort C(n=115)
Cohort D(n=180)
AP
SR
ate
p=0.020
p=0.038
p=0.033
Kar et al TCT 2015 See Important Safety Information Referenced Within. Not to be reproduced, distributed or excerpted.
©2015Abbott. All rights reserved. AP2941763-US Rev. A
No of cases ( 0 - 10) (11 – 20) (21 – 30) ( > 31 )
Surgery following failed MitraClip
Repair can be done following failed MitraClipeven upto 5 years later
The surgical risk is not increased
Surgical options are preserved since there isno loss leaflet tissue

2016/10/13
6
Robotic surgical repair;6 years following MitraClip What if a surgeon wants to replace
a valve following failed mitraclip
• Replace the surgeon, don’t replace thevalve
AHA/ACC Guideline 2014
Circulation. 2014 Mar 3]
ESC Guideline 2012
ESC/EACT S GUIDELIN ES
Guidelines on the management of valvular heartdisease (version 2012)
The Joint Task Force on the Managem ent of Valvular Hear t Diseaseof the European Society of Cardiology (ESC) and the EuropeanAssociation for Cardio-Thor acic Surgery (EACTS)
Authors/Task Force Member s: Alec Vahanian (Chairperson) (France) *, Ot tavio Alfier i
(Chairperson) * (Italy), Felicita Andreot t i (Italy), Manuel J. Antunes (Port ugal),Gonzalo Bar on-Esquivias (Spain), Helm ut Baum gartner (Germany),
Michael Andr ew Borger (Germany), Thierr y P. Carrel (Switzer land), Michele De Bonis
(Italy), A rtur o Evangelista (Spain), Volkmar Falk (Switzer land), Bernard Iung(France), Patr izio Lancellot t i (Belgium), Luc Pier ard (Belgium ), Susanna Pr ice (UK),
Hans-Joachim Schafers (Ger many), Gerhar d Schuler (Ger many), Janina Stepinska
(Poland), Kar l Swedber g (Sweden), Johanna Takkenberg (The N ether lands),Ulr ich Otto Von Oppell (UK), Stephan W indecker (Switzer land), Jose Luis Zam orano
(Spain), Mar ian Zembala (Poland)
ESC Commit tee for Pract ice Guidelines (CPG): Jeroen J. Bax (Chairperson) (T he N ether lands), Helmut Baumgartner
(Germany), Claudio Ceconi (Italy), Veronica Dean (France), Chr ist i Deaton (UK), Robert Fagard (Belgium),
Chr ist ian Funck-Brentano (France), David H asdai (Israel), Arno Hoes(The N ether lands), Paulus Kirchhof(United Kingdom), Juhani Knuut i (Finland), Phi lippe Kolh (Belgium), Theresa McDonagh (UK), Cyr il Moulin (France),
Bogdan A. Popescu (Romania), Zeljko Reiner (Croat ia), U do Sechtem (Germany), Per Anton Sirnes (Norway),Michal Tendera (Poland), Adam Torbicki (Poland), A lec Vahanian (France), Stephan W indecker (Switzer land)
Document Reviewers:: Bogdan A. Popescu (ESC CPG Review Coordinator ) (Romania), Ludwig Von Segesser (EACTSReview Coordinator ) (Switzerland), Luigi P. Badano (Italy), Mat jaz Bunc (Slovenia), Marc J. Claeys (Belgium),
N iksa Drinkovic (Croat ia), Gerasimos Filippatos (Greece) ,Gilbert H abib (France), A. Pieter Kappetein (The N ether lands),
Roland Kassab (Lebanon), Gregory Y.H. Lip (U K), N ei l Moat (U K), Georg Nickenig (Germany), Cather ine M. Ot to (USA),John Pepper, (UK), N icolo Piazza (Germany), Pet ronella G. Pieper (The Nether lands), Raphael Rosenhek (Aust r ia),
N alt in Shuka (Albania), Ehud Schwammenthal (Israel ), Juerg Schwit ter (Switzer land), Pilar Tornos Mas(Spain),Pedro T. Tr indade (Switzer land), Thomas W alther (Germany)
The disclosure forms of the authors and reviewers are avai lable on the ESC website www.escardio.org/guidelines
Online publish-ahead-of-print 24 August 2012
Ottavio Alfieri, S. Raffaele University Hospital, 20132 Milan, Italy. Tel: + 39 02 26437109; Fax: + 39 02 26437125. Email: [email protected]†Other ESC ent ities having participated in the development of this document :
Associations: European Association of Echocardiography (EAE), European Association of Percutaneous Cardiovascular Interventions (EAPCI), Heart Failure Association (HFA)
Working Groups: Acute Cardiac Care, Cardiovascular Surgery, Valvular Heart Disease, Thrombosis, Grown-up Congenital Heart Disease
Councils: Cardiology Practice, Cardiovascular ImagingThe content of these European Society of Cardiology (ESC) Guidelines hasbeen published for personal and educational use only. No commercial use isauthorized.No part of the
ESC Guidelines may be translated or reproduced in anyform without writ ten permission from the ESC. Permission can be obtained upon submission of awritten request to Oxford
University Press, the publisher of the European Heart Journal, and the party authorized to handle such permissions on behalf of the ESC.
* Correspondingauthors: Alec Vahanian, Service de Cardiologie, Hopital Bichat AP-HP,46 rue Henri Huchard, 75018 Paris,France. Tel: + 33 1 40 25 67 60;Fax:+ 33 1 40 25 67 32.
Email: [email protected]
Disclaimer . The ESC/EACTS Guidelines represent the views of the ESC and the EACTS and were arrived at after careful consideration of the available evidence at the time they
were written.Health professionals are encouraged to take them fully into account when exercising their clinical judgement. The guidelines do not, however, override the individual
responsibility of health professionals to make appropriate decisions in the circumstances of the individual pat ients, in consultation with that patient and, where appropriate and
necessary, the patient’s guardian or carer. It is also the health professional’s responsibility to verify the rules and regulations applicable to drugs and devices at the time ofprescription.
& The European Society of Cardiology 2012. All rights reserved. For permissions please email: [email protected]
European Heart Journal (2012) 33, 2451–2496doi:10.1093/eurheartj/ehs109
atC
edarsS
inai
Medical
Cen
terM
edicalL
ibraryo
nM
ay2
1,2
014
http
://eurhea
rtj.ox
fordjo
urnals.o
rg/
Dow
nload
edfro
m
“The guideline recommendsthe MitraClip therapy as classIIb indication for bothdegenerative and functionalMR”
What about Functional MR
Treatment of FMR
• Medical treatment is the mainstay
• The role of surgery is controversial
– Often high risk since patients have low EF
– Symptomatic improvement
– High recurrence
– No mortality benefit
– No census whether repair is better thanreplacement

2016/10/13
7
MitraClip for Functional MR
• Majority of patients outside US are highrisk functional MR
• Evidence of safety and possible efficacy
• No randomized studies in this subgroup todemonstrate survival benefit
Ongoing Studies for MitraClip forFMR
• COAPT Trial ( US and Canada)• RESHAPE trial (Europe)
430 patients enrolled at up to 85 US sites
Randomize 1:1
Clinical and TTE follow-up:
1, 6, 12, 18, 24, 36, 48, 60 months
Control group
Standard of careN=215
Deemed not suitable for mitral valve surgery
Specific valve anatomic criteria
MitraClipN=215
Significant FMR (≥3+ by core lab) treated per standard of ccare
Trial design
Study has been extended468 patients have been randomized
COAPT : TOP ENROLLERS HIGHLIGHT!
Case summaryPatient: 45-year-old man
Clinical Presentation:Shortness of breath (NYHA functional class IV)Acute decompensated CHF (Dopamine; 3 mg/kg/min)
Past Medical History:Endstage non-ischemic cardiomyopathyHypertension
Past Surgical History:CRT-D implantation [2012]
45 year old male with non ischemic dilatedcardiomyopathy Class IV on inotropes Destination
IA for transplant/VAD“Parasternal short axis view” “4ch view” “3ch view”
Severe functional MR with LV dysfunction EROA = 0.46 cm2
LVEF = 23%, LVID d/s = 63/59 mm

2016/10/13
8
MitraClip procedure“Post 3rd clip deployment”
“Cardiac output increased from 2.9 to 3.7 L/min”
12 Month Follow-up : NYHA I off thetransplant list
“Parasternal long axis view” “4ch view” “3ch view”
Cedars Sinai Experience
Cedars Sinai Experience ( 2005 to 2016)
• Total number of patients treated: 502
– Clinical Trials: 198
– EVEREST II
– REALISM
– COAPT
– Comercial(since Oct 2013) 304
• Total number of procedures: 519
210
159
4333
20
33
154 5 6
11
71
109
86
0
20
40
60
80
100
120
05 06 07 08 09 10 11 12 13 14 15 16
Number of MitraClip Procedures in CSMC
MitraClip Trials commercial
Commercial approval Oct 2013
Cedars Sinai Experience(Results)
• Total No patients treated 502
• Primary success 96%
• In hospital mortality ( 2 case) 0.4%
• Partial clip detachment 1%
• Stroke 0.6%
• No case of urgent open heart surgery
• Surgery for failed clip procedure 4%
– 30 day and 1 year mortality for 0%

2016/10/13
9
Conclusion• Transacatheter MV repair is a safe and effective
treatment for selected patients with MR who are athigh risk for surgery.
• MitraClip is the leader in the field, though othertechnologies are in development
• Limitation of transcatheter repair include
– Adverse leaflet pathology
– Residual MR
Conclusion• Transcatheter MV repair using the MitraClip is a
safe and effective treatment for selected patientssignificant MR
• Evidence of safety, efficacy and durability
• In US the MitraClip is approved for treatment ofhigh risk primary (degenerative) MR
• The true role of MitraClip is being evaluated in theongoing COAPT trial.
62 yr old male with flail P2 treated withMitraClip in May 2006
9years later NYHA I
Low risk patients
• Is MitraClip and effective and durable treatmentoption for intermediate risk degenerative MRpatients
Probably yes
In the right patient
In the right hands
In the right time
Heart Team