Embed Size (px)
Citation preview

REVIEW ARTICLE
Mitral Arcade in Adults – A Systematic Overview
Fayaz A. Hakim, M.D., Chandrasekaran Krishnaswamy, M.D., and Farouk Mookadam, M.Sc., F.R.C.P.C.,F.A.C.C.
Department of Cardiovascular Diseases, Mayo Clinic, Scottsdale, Arizona
Mitral arcade (MA) is a rare congenital anomaly of the mitral valve and its tensor apparatus. This condi-tion has been reported primarily in children younger than 3 years of age. MA is characterized by elon-gated papillary muscles connected to each other and to the tip of anterior mitral leaflet by a bridge offibrous tissue. Because of progressive mitral regurgitation and/or mitral stenosis, survival into adulthoodis rare. Not much is known about MA in the adult population. In this review we address the demo-graphic features, clinical presentation, diagnosis, treatment, and outcome of this congenital anomaly inadult patients. (Echocardiography 2013;30:354-359)
Key words: mitral, arcade, mitral valve, adults
Mitral arcade (MA) is an infrequent congenitalmalformation of the mitral valve (MV) apparatus,first described by Layman and Edwards in 1967after 3 sudden and unexpected infant deathsoccurred.1 The anomaly is characterized by anarc like configuration of 2 papillary muscles (PM)due to an interconnecting band of fibrous tissuethat runs along the line of closure of the mitralleaflets (Fig. 1).1 We have previously reported onparachute MV in adults.2 In this systematicreview we report on an even less clinicallyencountered abnormality of the MV in adults. Areport of 15 cases encompasses predominantlyinfants and children3 but is less well describedamong adults. A clinical diagnosis of MA is diffi-cult to make and may only be made late in thedisease if sudden death does not supervene andsurvival into adulthood occurs. The presentationis usually that of severe congestive heart failure(CHF) related to progressive mitral regurgitation(MR) and/or mitral stenosis (MS). As MA is rare,the diagnosis is often not considered. Early mor-tality is high and survival into adulthood is extre-mely rare, which may be in part responsible for itgoing unrecognized in the echocardiographylaboratory. The aim of this review was to addressthe demographic features, clinical presentation,management, and outcome of MA in adult pop-ulation.
Findings of MA include the presence of afibrous band that extends between the superioraspects of elongated anterolateral and postero-medial PM that are in continuity with the freemargins of the anterior mitral leaflet (AML) orless frequently both the anterior and posteriormitral leaflets in an arcade like configuration.This also gives the MV a hammock appearancewhen viewed from atrial surface, accounting forits other name of “hammock” MV. The chordaetendineae tend to be short, thick, and fused ina manner that allows the PM to approximate ordirectly attach to the mitral leaflets. The valveleaflets itself may be thickened and fibrotic par-ticularly along the commissures. Layman andEdwards1 in their original report proposed thatMA results from an arrest in the developmentalstage in which the MV leaflets lose the directventricular muscular connections (chordaemuscularis) before attenuation and lengtheningof the collagenized chordae tendineae occur.Normal embryologic development of the chor-dae tendineae occurs between the 11th and13th week of gestation. During this embryonicphase the chordae tendineae begin differentiat-ing from the endocardial cushion at placeswhere the tips of the PM are attached to atrio-ventricular (AV) leaflets.4 An aberration in thisdevelopment results in the chordae tendineaebeing either short or near absent, so that thePM attach directly to the AV leaflets. The fibrousridge across the free margins of the mitral leaf-let is thought to be a vestigial remnant of adeveloping leaflet during early stages of devel-opment or may represent remodeling of
Address for correspondence and reprint requests: FaroukMookadam, MSc, FRCPC, FACC, Mayo Clinic College of Medi-cine, 13400 E Shea Blvd, Scottsdale, Arizona 85255.Fax: +480-301-8018;E-mail: [email protected]
354
© 2013, Wiley Periodicals, Inc.DOI: 10.1111/echo.12126 Echocardiography

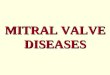
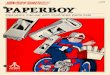
the valve complex due to turbulent bloodflow across the MV.5 The key pathologicalfeatures of MA are demonstrated in Figure 1and outlined in Table I.
The arc-like configuration of the PM with theinterconnecting fibrous band, together with theshort or absent chordae tendineae results inrestricted systolic mitral leaflet motion andincomplete mitral leaflet coaptation leading toMR. Elongated (and sometimes enlarged) PMwith the interconnecting fibrous band and com-missural fusion may also cause subvalvularcrowding resulting in mitral inflow stenosis.
Search Strategy:We performed an electronic literature search ofMedline, Ovid, and PubMed published in Englishlanguage papers over a 51-year period, fromJanuary 1, 1960 to December 31, 2011 using thesearch terms: “arcade,” “hammock,” “mitral,”“valve,” “adults,” and “anomalous.” An indepen-dent search was conducted by a qualified librar-ian and one of the authors (FH) using similarsearch terms and search engines. Bibliographiesof the retrieved articles were scanned to identifyfurther reported cases and were included in thestudy. Care was taken to avoid duplication of thecases. We reviewed and analyzed the demo-graphic profile, clinical features, diagnosticmodalities, treatment, and outcome of all adultpatients with MA.
Findings:We identified 7 cases of adult MA through thisbroad literature search spanning half a century.There were 4 (57%) female and 3 (43%) malepatients with mean age of 33 � 15 years (range18–65). The demographic data, clinical charac-teristics, management, and outcome of eachpatient is summarized in Tables II and III.
Clinical Presentation:Shortness of breath was the most commonsymptom (5/7), followed by fatigue (2/7), andCHF (2/7). One patient presented with a strokeand another atrial fibrillation (AF). One patientpresented with CHF in infancy, but a diagnosis ofMA was only established in adulthood. Anisolated systolic murmur was reported in 5/7,isolated apical mid-diastolic murmur in 1/7, andboth apical systolic and diastolic murmurs in 1/7patients. In 1 patient no murmur was mentioned.In 2/7 patients an apical systolic murmur washeard incidentally at age 12 and 16, respectively,but a diagnosis of MA was only established inadulthood when they presented with symptomsof heart failure.
Diagnosis:Transthoracic echocardiography (TTE) was per-formed in 6/7 and the diagnosis of MA estab-lished in 3, missed in 2, and mistaken for
Figure 1. Illustrates the cardinal morphological features ofmitral arcade; absent or short chordae tendineae, intercon-necting band of fibrous tissue between 2 papillary muscles(PM), elongated PM. Direct attachment of PM to mitral leaflet(arrow) and view from left atrium (inset) are also shown.
TABLE I
Pathological and Echocardiographic Diagnostic Characteris-tics of Mitral Arcade
Pathology Short, thick, and fused or absent mitralchordae tendineae
Elongated papillary musclesBand of fibrous tissues connecting apicesof 2 PMs and free margin of AML andPML in an arc like configuration(hammock appearance)
Normal or mild thickening of mitral valveEchocardiography LV parasternal long-axis view:
Elongated PMs directly attached tomitral leaflet/s due to short and thickor absent chordae tendineae.
LV parasternal short-axis view just belowmitral annulus:Hyperechoic mass between 2 PMsrepresenting interconnecting fibrousband (hammock mitral valve)
Restricted systolic and/or diastolicmovements of mitral leaflet (usuallyAML)
At mitral level:Thickened mitral leaflets (usually AML)
Apical two-chamber view with superiortilt:Arc like configuration of the PMsconstrained by interconnectingfibrous band
MA = mitral arcade; LV = left ventricular; AML = anteriormitral leaflet; PM = papillary muscles; PML = posterior mitralleaflet.
355
Mitral Arcade in Adults

TABLE
II
Dem
ograph
icCha
racteristic
s,Clin
icalFeatures,D
iagn
ostic
Mod
alities,T
reatmen
t,an
dOutco
mein
Adu
ltPa
tientswith
MitralArcad
e
NAutho
r(Yea
r)Age
/ge
nder
Presen
ting
Com
plaints
Clin
ical
Find
ings
Clin
ical
Diagn
osis
Diagn
osisof
MA
Trea
tmen
ts
Outco
mes
Autop
syEcho
cardiograp
hyCardiac
catheterization
CT
scan
Med
ical
Surgical
1Pe
rezet
al.
(198
7)12
28/F
Prog
ressive
SOB
Holosytolic
murmur
MR,
CHF
TTE:
Non
specific
thickening
ofMV
Severe
MR
EF45
%NA
CHF med
ication
Normal
MVCRA
Dea
thdu
eto
CHF
MA
2Myerset
al.
(198
7)13
36/M
Fatig
ueExertio
nal
SOB
Apical
pansystolic
murmur
Mid-diastolic
murmur
MR,
MS
NA
MA,M
RNA
NA
MAan
dmod
erate
MS
MVR
(27mm
Bjork-Sh
iley)
Une
ventful
reco
very.
Long
-term
F/UNA
NA
3Espino
la-
Zavaleta
etal.
(200
2)11
28/F
Stroke
Diastolic
murmur
NA
TTE:
Severe
MS
andmild
MR
3D-TEE:M
A
NA
NA
NA
NA
NA
NA
4Kim
etal.
(200
5)10
65/M
Exertio
nal
SOB
Apical
pansystolic
murmur
MR
TTE:
Mod
erateMR
andMATE
E:MA
NA
MDCT:
MA
ACEI,
diuretics
Improv
edLo
ng-term
F/UNA
NA
5Collin
sII
etal.
(201
0)7
18/F
Fatig
ueExertio
nal
SOB
Ortho
pnea
Tach
ypne
aApical
systolic
murmur
MR
TTE:
Mod
erateMR
andMA
NA
NA
NA
MVR
(29mm
StJude
)Im
prov
edLo
ng-term
F/UNA
NA
6Fede
rici
etal.
(201
0)3
33/M
Exertio
nal
SOB,
AF
Apical
systolic
murmur
MR
TTE:
Severe
MR,
Mod
erateMS
andMA
NA
NA
Bisoprolol,
warfarin
MVrepa
irIm
prov
edLo
ng-term
F/UNA
NA
7Morris
etal.
(201
1)8
25/F
Prog
ressive
SOB
NA
CHF
TEE:
Severe
MR,
Intrao
perativ
e;-
TEE:
MA
NA
CCT: MA
NA
MAMecha
nical
MVR
(typ
eno
tmen
tione
d)
Improv
edLo
ng-term
F/UNA
NA
N=case
numbe
r;TT
E=tran
stho
racicecho
cardiograp
hy;TE
E=tran
sesoph
agealecho
cardiograp
hy;MR=mitral
regu
rgita
tion;
MS=mitral
sten
osis;MA=mitral
arcade
;CT=co
m-
putedtomog
ram;M
V=mitral
valve;
MVR
=mitral
valvereplacem
ent;PH
=pu
lmon
aryhy
perten
sion
;SOB=shortnessof
brea
th;C
HF=co
ngestiv
ehe
artfailu
re;A
F=atria
lfibrillation;
Postop
=po
stop
erative;
F/U
=follo
w-up;
CRA
=carpen
tierrin
gan
nuloplasty;C
CT=cardiacCTscan
;MDCT=multid
etectorCTscan
;NA=no
tavailable;
ACEI
=an
gioten
sinco
nvert-
ingen
zymeinhibitor.
356
Hakim, et al.

rheumatic MV disease in 1 patient. Transesopha-geal echocardiography (TEE) was performed in3/7 patients and a diagnosis of MA established orconfirmed in all the 3 patients. Three-dimen-sional (3D) reconstruction was performed in 2 ofthese patients for better anatomical delineationof the MV apparatus.
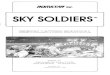
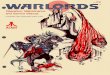
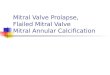
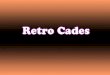
The classical echocardiographic findings ofMA (Table I) first described by Parr in the pedi-atric population6 were demonstrated on two-dimensional (2D) parasternal long (Fig. 2) andshort-axis (Fig. 3) views in 3 patients and onapical two and four-chamber views withsuperior tilting in 2 patients. Color Dopplerinterrogation of the MV inflow demonstratedmultiple jets of accelerated diastolic flowthrough multiple orifices between foreshortenedmitral chordae7 and a regurgitant jet (Fig. 4)across the MV.
The diagnosis of MA was incidentally madeon coronary computed tomography (CT) angio-gram and later confirmed at intraoperative TEE in1 patient and reconfirmed by multidetector CTscan in another after the diagnosis was initiallyestablished by echocardiography.
TABLE III
Frequency of Symptoms, Clinical Findings, Diagnostic Modali-ties, and Treatment in Adult Patients with Mitral Arcade
Symptoms n (%)SOB 5/7 (71)Fatigue 2/7 (28)Stroke 1/7 (14)CHF 2/7 (28)AF 1/7 (14)
Clinical findingsIsolated ASM 4/7 (57)Isolated ADM 1/7 (14)ASM + ADM 1/7 (14)
Hemodynamic DiagnosisIsolated MR 4/7 (57)Mixed MR/MS 3/7 (43)
Diagnosed testsTTE 6/7 (86)TEE 3/7 (43)MDCT 1/7 (14)LHC 1/7 (14)Autopsy 1/7 (14)
TreatmentMV Replacement 3/7 (43)MV repair 1/7 (14)CRA 1/7 (14)
N = number; TTE = transthoracic echocardiography; TEE =transesophageal echocardiography; MR = mitral regurgitation;MS = mitral stenosis; MV = mitral valve; SOB = shortness ofbreath; CHF = congestive heart failure; AF = atrial fibrillation;CRA = carpentier ring annuloplasty; MDCT = multidetector CTscan; LHC = left heart catheterization; ASM = apical systolicmurmur; ADM = apical diastolicmurmur.
Figure 2. Parasternal long-axis view showing very shortchordae tendineae (CT) attached to anterior mitral leaflet anddirect attachment of the papillary muscle (PM) to posteriormitral leaflet (PML) due to absent chordae tendineae (*).
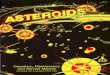
Figure 3. Parasternal short-axis view showing interconnect-ing band of tissue (*) between 2 papillary muscles (PM).
Figure 4. Color flow apical four-chamber view showingsevere mitral regurgitation due to poor coaptation of mitralleaflets.
357
Mitral Arcade in Adults

Left heart catheterization performed forhemodynamic assessment diagnosed MA in 1patient. The abnormality was described as a rect-angular radiolucent defect (fibrous band) extend-ing between the MV and PM. The abnormalchordae tendineae and restricted mitral leafletmotion were demonstrated as well.
The diagnosis of MA in 1 patient wasestablished at autopsy after the initial TTE andcardiac catheterization failed to diagnose theabnormality.
Hemodynamic Consequences of Adult MA:Four (57%) patients had isolated MR and 3(43%) patients had mixed MR/MS. MR wassevere in 3, moderate in 2, and mild in 1patient. Mitral stenosis was severe in 1 and mod-erate in 2 patients. Pulmonary hypertension wasreported in 3 and elevated pulmonary capillarywedge pressure in 2 patients. The hemodynamicabnormalities of adult MA are summarized inTable IV.
Treatment:Mitral valve replacement (MVR) was performedin 3 (43%) patients. Case #2 with mixed MVdisease (moderate MS and MR) underwent MVRwith 27 mm Bjork-Shiley prosthesis. Case #5with moderate MR had MVR with a 29 mm St.Jude prosthesis. Case #7 with severe MR under-went successful mechanical MVR (type notmentioned) by robot-assisted minimally invasivesurgery. MV repair was performed in 1 patient,which included splitting of the posteromedialPM, interposition of 2 artificial polytetrafluoro-
ethylene chordae (Gore-Tex; W.L. Gore andAssociates, Flagstaff, AZ, USA) at the P1 levelafter resection of the anterior PM head andremoval of fibrous tissue, and finally, applicationof a complete (Sovering No. 38 mm; Sorin Bio-medica, Milan, Italy) mitral annuloplasty ring.The surgical procedures were successful withimprovement in hemodynamic abnormalities ona postoperative echocardiogram. However,long-term follow-up on these patients is notavailable. One patient who presented with CHFdue to severe MR was treated with a Carpentierring annuloplasty after initial TTE, cardiac cathe-terization, and surgical examination of the MVfailed to diagnose MA. The patient died sud-denly 2 months later after initial improvementand MA was diagnosed at autopsy. Twopatients were treated medically for CHF and 1patient who had AF was treated with beta-blocker and long-term anticoagulation.
Discussion:From this 50 year look at the published literature,it appears that MA is extremely rare in the adultpopulation. The diagnosis is challenging to makebecause of failure to recognize the condition andhence treatment may be less than optimal. Themajority of patients present with worseningdyspnea due to progressive MR, MS, or both. Anincidental cardiac murmur may be auscultated inasymptomatic individuals years before clinicalpresentation. MR is by far the commonest lesionwith or without MS. Isolated MS does not appearto occur.
TABLE IV
Hemodynamics in Adult Patients with Mitral Arcade
N Author (Year) Valve LesionAssessingModality LVEF
PAP(Mean) PCWP RVP
CI (L/min/m2)
1 Perez et al.(1987)12
Severe MR Cardiaccatheterization
47% NA 16 (v wave 25) NA
2 Myers et al.(1987)13
MR (severity notmentioned) ModerateMS
Cardiaccatheterization
NA 65/35(45)
16 (a wave 16,v wave 24)
115/5
2.1
3 Espinola-Zavaletaet al. (2002)11
Mild MR Severe MS (MVA0.7 cm2)
Echocardiography NA (79) NA NA NA
4 Kim et al. (2005)10 Moderate MR (RV 45 mL) Echocardiography NA NA NA NA NA5 Collins et al. II
(2010)7Moderate MR Echocardiography Normal NA NA 70 NA
6 Federici et al.(2010)3
Severe MR Moderate MS Echocardiography NA NA NA NA NA
7 Morris et al.(2011)8
Severe MR Echocardiography NA NA NA NA NA
N = number; MR = mitral regurgitation; MS = mitral stenosis; LVEF = left ventricular ejection fraction; NA = not available;PAP = pulmonary artery pressure; PCWP = pulmonary capillary wedge pressure; RVP = right ventricular pressure; CI = cardiacindex; MVR = mitral valve replacement.
358
Hakim, et al.

Careful echocardiographic examination, spe-cifically looking for the characteristic features canclinch the diagnosis, especially in subjects whohave “atypical rheumatic thickening or inflowobstruction” of the MV or when the etiology forthe MR is not clearly attributable to the knowncommon causes. Multiplane TTE with color flowDoppler can provide valuable adjunctive informa-tion to precordial imaging for assessing anatomi-cal and functional status with increasingdiagnostic accuracy.8 TEE with 3D-reconstructiondemonstrates more precisely the anatomy of thearcade.9
Cardiac CT has a higher spatial resolutionthan echocardiography for assessing the anatom-ical details of the tensor apparatus but provideslittle information on the hemodynamic abnor-malities10 and may be used as an adjunctivediagnostic tool in patients with poor acousticwindows or when the diagnosis is still in doubt.
Although MA may be suspected or even diag-nosed during contrast left ventriculography,echocardiography is needed to confirm the diag-nosis and assess the hemodynamic abnormali-ties.
In comparison with pediatric patients; most ofwhom died in infancy and a diagnosis of MAestablished at autopsy, adults with MA seem tohave milder MR/MS that escape detection in earlylife and present later, likely due to degenerativethickening of the mitral leaflets over time. Symp-tomatic adult MA patients with hemodynamicallysignificant MR or MS are best treated with MVR.However, the long-term outcome of this interven-tion is not known. Arcade repair has beendescribed, but scant supporting data are avail-able. Inadvertent repair is undertaken if the diag-nosis is not confirmed preoperatively. Experiencefrom the pediatric patients suggests that MArepair frequently results in failure necessitatingvalve replacement.13 Medical treatment is limitedto symptomatic relief of heart failure and AF.
Limitations:Being a systematic overview of literature asymp-tomatic adult MA cases are likely be under repre-sented. The rarity of adult MA lends itself nicelyto scrutiny with the research methodology of aqualitative systematic overview as we have per-formed. Furthermore, there is a need for anational or international registry to better under-stand the management of this uncommon condi-tion both in terms of diagnosis and optimalsurgical treatment.
Recommendation for Imaging:Multiplane 2D-TTE with Doppler color flow map-ping is an excellent initial method of detecting
the MA anomaly and assessing its hemodynamicconsequences.9 When clinically unexplained MRor MS is seen, consideration of MA should spurthe need to undertake the views described abovein an effort to clinch the diagnosis. TEE with3D-reconstruction can be helpful in more chal-lenging cases.11 Cardiac CT scan should beadjunctive to echocardiography when the diag-nosis is still in doubt.10
Conclusions:Mitral arcade in adults is a rare but importantcause of progressive MR or MS. This anomalyshould be considered in adult patients in whomthe mechanism of MR or MS is not clear. Echo-cardiography is an excellent imaging techniqueto establish the diagnosis and assess associatedhemodynamic abnormalities. Symptomaticpatients with hemodynamically significant MVdysfunction should be referred for surgical MVR.
References1. Layman TE, Edwards JE: Anomalous mitral arcade: A type
of congenital mitral insufficiency. Circulation 1967;35:389–395.
2. Hakim FA, Kendall CB, Al-Harthi M, et al: Parachutemitral valve in adults – An overview. Echocardiography2010;27:581–586.
3. Federici D, Palmerini E, Lisi M, et al: Congenital mitraldisease: Anomalous mitral arcade in a young man. AnnThorac Surg 2010;89:629–631.
4. Seguela PE, Houyel L, Acar P: Congenital malformation ofthe mitral valve. Arch Cardiovasc Dis 2011;104:465–479.
5. Mtasushima AY, Park J, Szulc M, et al: Anomalous atrio-ventricular valve arcade. Am Heart J 1991;121:1824–1826.
6. Parr GVS, Fripp RR, Whiteman V, et al: Anomalous mitralarcade: Echocardiographic and angiographic recogni-tion. Pediatr Cardiol 1983;4:163.
7. Collins RT II, Ryan M, Gleason MM, et al: A rare cause offatigue in an 18 years old female. Circulation 2010;121:379–383.
8. Morris MF, Williamson EE, Topilsky Y, et al: Multi-imag-ing assessment of the congenital mitral arcade. J Am CollCardiol 2011;57:1856.
9. Pacileo G, Russo MG, Calabro R: Anomalous mitralarcade: Echocardiographic and color flow findings. Echo-cardiography 1991;8:657–659.
10. Kim SJ, Shin ES, Park MK, et al: Congenital mitral insuffi-ciency caused by anomalous mitral arcade in an elderlypatient; use of echocardiography and multidetector com-puted tomography for diagnosis. Circ J 2005;69:1560–1563.
11. Espinola-Zavelta N, Vargas-Barron J, Keirns C, et al:Three-dimensional echocardiography in congenital mal-formations of mitral valve. J Am Soc Echocardiogr2002;15468–472.
12. Perez JA, Herzberg AJ, Reimer KA, et al: Congenital mitralinsufficiency secondary to anomalous mitral arcade in anadult. Am Heart J 1987;114:894–895.
13. Myers ML, Goldblach MM, Sears GA: Anomalous mitralarcade: A rare cause of mitral valve disease in an adult.Can J Cardiol 1987;3:60–62.
359
Mitral Arcade in Adults