Embed Size (px)
DESCRIPTION
MR TR
Citation preview

Mitral valve disease
The mitral valve separates the left atrium and the left ventricle of the heart and is a fibrous structure lined by endocardium. It consists of
1. The mitral annulus, 2. The leaflets of which comprise a large anterior and a small posterior leaflet. 3. The chordae tendineae and the papillary muscles.
• Abnormalities in any of these structures can cause mitral valve dysfunction. • The leaflets are tethered to the left ventricle by the chordae tendineae. Chordae
tendineae are attached to papillary muscles and prevent prolapse of the mitral valve leaflet to prevent reflux of blood into the left atrium.
Mitral Stenosis Etiology
1. Rheumatic fever is the main cause of mitral stenosis (See figure 1) 2. Less common causes of mitral stenosis include:
o Severe calcification of the mitral annulus o Bacterial endocarditis o Congenital heart disease (parachute mitral valve) o Rarely, systemic lupus erythematosis and rheumatoid arthritis
Figure 1. Rheumatic mitral stenosis
Pathophysiology 1.The normal area of the mitral valve orifice is about 4 to 6 cm2. Under normal conditions, a normal mitral valve will not impede the flow of blood from the left atrium to the left ventricle during (ventricular) diastole, and the pressures in the left atrium and the left ventricle during diastole will be equal. The result is that the left ventricle gets filled with blood during early diastole, with only a small portion of extra blood contributed by contraction of the left atrium (the "atrial kick") during late ventricular diastole. 2.When the mitral valve area goes below 2 cm2, the valve causes an impediment to the flow of blood into the left ventricle, creating a pressure gradient across the mitral valve. This gradient may be increased by increases in the heart rate or cardiac output. 3.As the gradient across the mitral valve increases, the amount of time necessary to fill the left ventricle with blood increases. Eventually, the left ventricle requires the atrial kick to fill with blood. As the heart
rate increases, the amount of time that the ventricle is in diastole and can fill up with blood (called the diastolic filling period) decreases. 4.When the heart rate goes above a certain point, the diastolic filling period is insufficient to fill the ventricle with blood and pressure builds up in the left atrium, leading to pulmonary congestion. 5.When the mitral valve area goes less than 1 cm2, there will be an increase in the left atrial pressures (required to push blood through the stenotic valve). 6. Since the normal left ventricular diastolic pressures is about 5 mmHg, a pressure gradient across the mitral valve of 20 mmHg due to severe mitral stenosis will cause a left atrial pressure of about 25 mmHg. This left atrial pressure is transmitted to the pulmonary vasculature and causes pulmonary hypertension. 7. Pulmonary capillary pressures in this level cause an imbalance between the hydrostatic pressure and the oncotic pressure, leading to extravasation of fluid from the vascular tree and pooling of fluid in the lungs (congestive heart failure causing pulmonary edema). 8.The constant pressure overload of the left atrium will cause the left atrium to increase in size. As the left atrium increases in size, it becomes more prone to develop atrial fibrillation. When atrial fibrillation develops, the atrial kick is lost (since it is due to the normal atrial contraction). 9.In individuals with severe mitral stenosis, the left ventricular filling is dependent on the atrial kick. The loss of the atrial kick due to atrial fibrillation can cause a precipitous decrease in cardiac output and sudden congestive heart failure. Symptoms Patients with mitral stenosis may present with exertional dyspnea, paroxysmal nocturnal dyspnea, fatigue, atrial arrhythmias, embolic events, anginalike chest pain, hemoptysis, or even rightsided heart failure. Previously asymptomatic or stable patients may decompensate acutely during exercise, emotional stress, pregnancy, infection, or with uncontrolled atrial fibrillation. Physical examination
The patient with mitral stenosis may have malar flush. There may be ankle or sacral edema. Jugular venous pressure may be elevated. Prominent “a” waves may be due to pulmonary hypertension. Systolic venous pulsations may be present with severe tricuspid regurgitation. In case of atrial fibrillation, loss of “a’ waves in jugular venous pulse is evident.
On palpation, the apex of the heart is right ventricular and tapping. A diastolic thrill is usually palpable. A left parasternal heave may be palpable due to right ventricular hypertrophy. A diastolic shock is felt over second left intercostals space if there is severe pulmonary hypertension.
The characteristic findings of MS on auscultation include (see figure 2) o First heart sound is unusually loud and may be palpable (tapping apex beat) because of
increased force in closing the mitral valve. o If pulmonary hypertension secondary to mitral stenosis is severe, the P2 (pulmonic)
component of the second heart sound (S2) will become loud. o An opening snap which is a high pitched additional sound may be heard, which correlates
to the forceful opening of the mitral valve. o A mid‐diastolic rumbling murmur will be heard after the opening snap. The murmur is
best heard at the apical region and is not radiated. Since it is low‐pitched it should be picked up by the bell of the stethoscope. Rolling the patient towards left, as well as isometric exercise will accentuate the murmur.
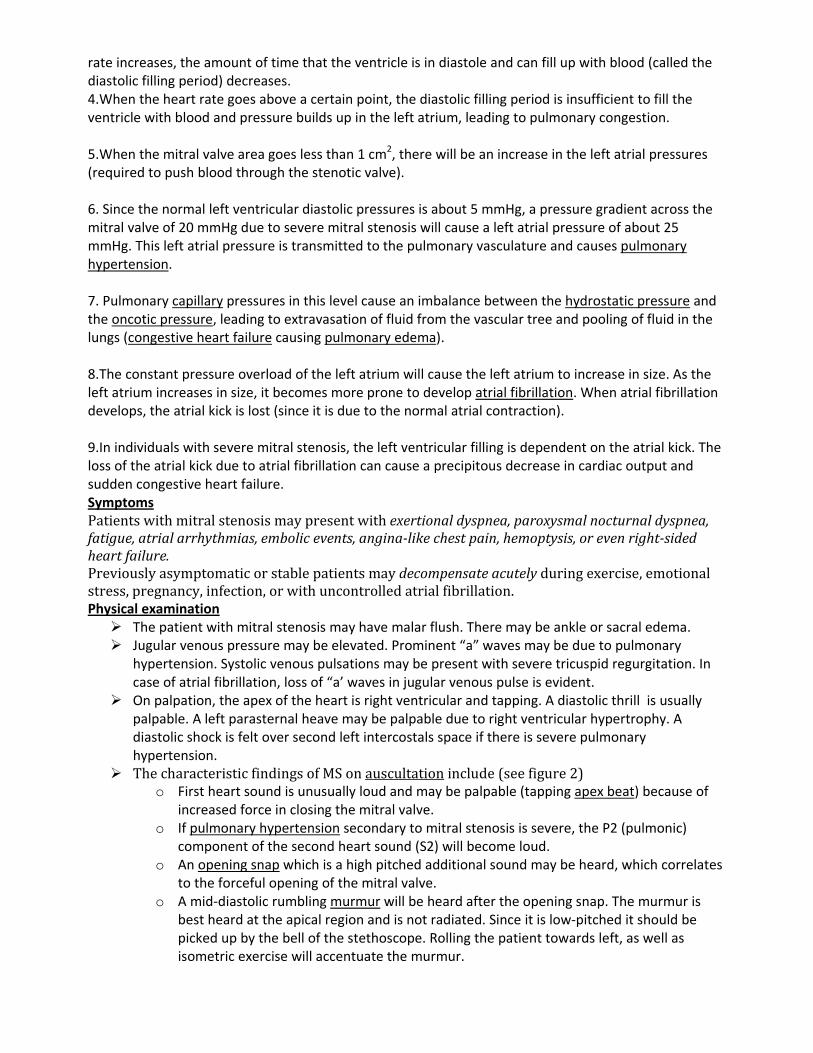
o The longer the duration of the diastolic murmur is, the more severe the stenosis is expected to be.
o The shorter the time interval from S2 to opening snap (S2‐OS interval) is, the more severe the stenosis will be.
Figure2 . Spectrum of Clinical Signs in Mitral Stenosis
Diagnosis ECG :
• In mild mitral stenosis : ECG may be normal .
• In the stage of pulmonary venous congestion, P wave is broad and notched: (P‐mitrale) .
• In stage of pulmonary arterial hypertension , signs of right ventricular enlargement are present .
• Atrial fibrillation may be seen as absent P waves which are replaced by fine or coarse fibrillatory waves.
Chest radiography : • Signs of left atrial enlargement . • Signs of pulmonary congestion . • Signs of right ventricular hypertrophy
Severity of mitral stenosis
Degree of mitral stenosis Mean gradient Mitral valve area
Mild mitral stenosis <5 >1.5 cm2
Moderate mitral stenosis 5 ‐ 10 1.0 ‐ 1.5 cm2
Severe mitral stenosis > 10 < 1.0 cm2
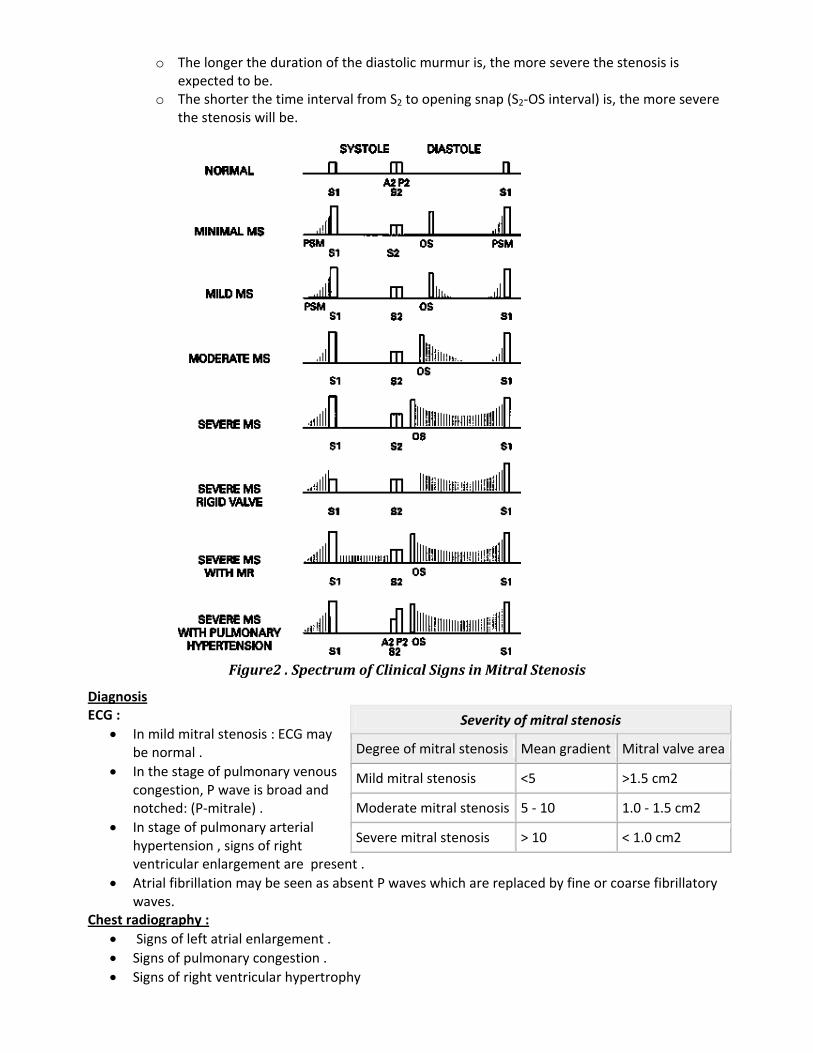
Echocardiography : See Figure 3 • Characteristic findings of MS include valve thickening, restricted valve opening, anterior
leaflet doming, and fusion of the leaflets at the commissures. • The trans‐mitral gradient as measured by Doppler echocardiography is the gold standard in the
evaluation of the severity of mitral stenosis. The mean pressure gradient across the mitral valve on Doppler echocardiography (echo) in MS is at least 5 mm Hg; in severe stenosis, it is usually higher than 10 mm Hg.
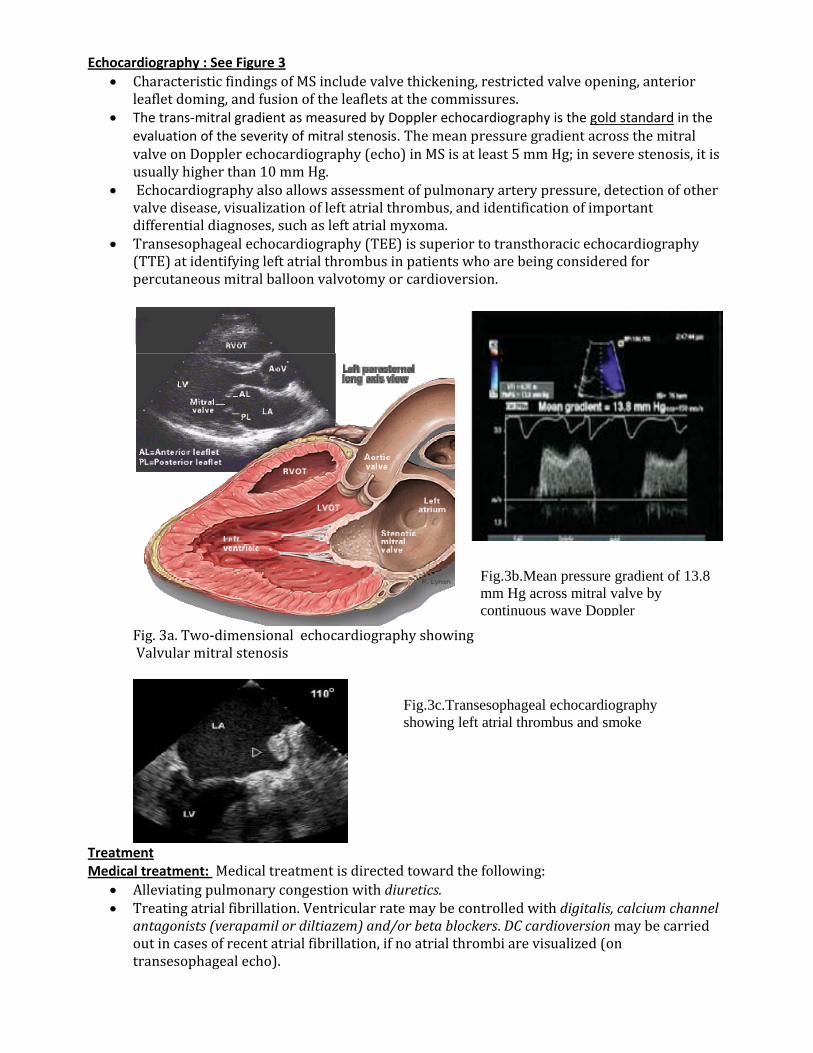
• Echocardiography also allows assessment of pulmonary artery pressure, detection of other valve disease, visualization of left atrial thrombus, and identification of important differential diagnoses, such as left atrial myxoma.
• Transesophageal echocardiography (TEE) is superior to transthoracic echocardiography (TTE) at identifying left atrial thrombus in patients who are being considered for percutaneous mitral balloon valvotomy or cardioversion.
Fig. 3a. Two‐dimensional echocardiography showing Valvular mitral stenosis
Treatment Medical treatment: Medical treatment is directed toward the following:
• Alleviating pulmonary congestion with diuretics. • Treating atrial fibrillation. Ventricular rate may be controlled with digitalis, calcium channel
antagonists (verapamil or diltiazem) and/or beta blockers. DC cardioversion may be carried out in cases of recent atrial fibrillation, if no atrial thrombi are visualized (on transesophageal echo).
Fig.3b.Mean pressure gradient of 13.8 mm Hg across mitral valve by continuous wave Doppler
Fig.3c.Transesophageal echocardiography showing left atrial thrombus and smoke
• Anticoagulation in patients who are at increased risk of arterial embolic events. Anticoagulation may be started with unfractionated heparin and continued with oral warfarin.
• Antibiotic therapy is important for the secondary prevention of rheumatic carditis. Patients with a history of rheumatic fever are at high risk of recurrence. Long‐term secondary prophylaxis, preferentially with penicillin, is therefore recommended for all patients with a history of rheumatic fever.
Surgery & invasive intervention Three invasive options are available for patients with MS:
o Percutaneous mitral balloon valvotomy (PMBV) o Surgical mitral commissurotomy o Mitral valve replacement (MVR)
Percutaneous mitral balloon valvotomy In experienced centers, PMBV is the initial procedure of choice and should be considered for (1) symptomatic patients (NYHA functional Classes II to IV) with moderate or severe MS and (2) asymptomatic patients with moderate or severe MS and pulmonary hypertension.
PMBV is a catheter‐based technique in which a balloon is inflated across the stenotic valve to split the fused commissures and increase the valve area. The MVA typically doubles in size, and hemodynamic as well as clinical improvements are seen immediately. The results are comparable with those achieved with open mitral commissurotomy, but it is less invasive and less costly.
The mitral valve morphology is an important predictor of successful balloon valvotomy. The following factors adversely affect the results of PMBV:
o Severe valve calcification o Severe valve thickening and fibrosis o Marked subvalvular affection o Presence of more than mild mitral regurgitation o Presence of left atrial thrombi
Open mitral commissurotomy It involves the use of cardiopulmonary bypass and the surgical repair of a diseased mitral valve by direct visualization. Open mitral commissurotomy may be considered in the following cases:
o Presence of a left atrial thrombus o Significant mitral regurgitation if the valve anatomy is suitable. o Patients who have other concomitant valvular disease o Patients with coronary artery disease that requires surgery
Mitral valve replacement (figure 4): indicated for patients with: i. Calcified valves that cannot be treated by valvotomy or commissurotomy
ii.Those with significant mitral regurgitation that is not suitable for repair Surgery for moderate to severe mitral stenosis is indicated for symptomatic patients (NYHA functional Class III or IV) where PMBV is unavailable or contraindicated.
Fig.4. Prosthetic bileaflet mitral valve prosthesis
Mitral Regurgitation
Causes : 1. Rheumatic fever . 2. Ischemic heart disease 3. Papillary muscle rupture or dysfunction . 4. Mitral vlave prolapse . 5. Infective endocarditis . 6. Calcification of mitral annulus . 7. Congenital as cleft mitral valve . 8. Cardiomyopathy
Pathophysiology : Significant MR leads to volume overload of the left ventricle, because it has to accommodate both the stroke volume and regurgitant volume with each heartbeat. During systole , blood regurgitates from left ventricle to left atrium leading to :
o Decreased effective left ventricular stroke volume . o Increased left atrial pressure and size . o Pulmonary congestion and later on pulmonary hypertension .
Progression of mitral regurgitation leads to left ventricular dilatation and aggravates mitral regurgitation. Left atrial enlargement predisposes the patient to atrial fibrillation and arterial thromboembolism. In long‐standing MR, patients may develop pulmonary hypertension and congestive heart failure. Clinical picture :
• Patients with chronic, severe mitral regurgitation may remain asymptomatic for years because the regurgitant volume load is well tolerated as a result of compensatory ventricular and atrial dilation. When symptoms do develop, the most common are dyspnea, fatigue, orthopnea, paroxysmal nocturnal dyspnea, and palpitations caused by atrial fibrillation.
• Acute severe MR, as occurs with chordal rupture or papillary muscle rupture, is almost always symptomatic because the sudden regurgitant volume load in the nondilated left ventricle and atrium leads to pulmonary venous hypertension, congestion and acute pulmonary edema.
Signs : • Signs of left ventricular hypertrophy . • Systolic thrill over apex . • Muffled first heart sound . • Third heart sound S3 may be heard . • Harsh pan‐systolic murmur over apex propagated to axilla , incase of ruptured chordae tendinae
murmur may be cooing (seagull quality) ; in case of fail mitral cusps , murmur may be musical . • In case of severe mitral regurgitation , short mid‐diastolic rumbling murmur may be heard due to
augmented blood flow from left atrium to left ventricle . Investigations : ECG : Signs of left atrial and left ventricular enlargement . Chest radiography : Increase in left atrial size , left ventricular enlargement , signs of pulmonary congestion . Echocardiography (figure 5 ) : Visualization of mitral leaflets , papillary muscles and chordae tendinae . Left ventricular dimensions and functions Degree of mitral regurgitation .
Treatment Medical treatment :
• In patients with acute severe MR, afterload reduction with intravenous nitroprusside and nitroglycerin reduces the regurgitant fraction and pulmonary pressures.
• In patients with chronic asymptomatic mitral regurgitation caused by primary valve disease, there is no evidence for the routine use of medication in delaying the need for surgery or preventing left ventricular dysfunction. The management of these patients is focused on deciding on the appropriate timing of surgery, before the development of irreversible left ventricular dysfunction.
• Patients should be followed up every 6 to 12 months to assess for symptoms and to measure left ventricular size, function, and severity of MR by echocardiography.
Surgical treatment : Surgery is indicated for (1) symptomatic patients with severe primary MR (2) asymptomatic patients with severe primary MR and evidence of LV dysfunction. The standard indications for surgery in asymptomatic patients are an
o LV end‐systolic dimension of more than 4.0 cm o A resting LV ejection fraction of less than 60% o Pulmonary hypertension o Development of atrial fibrillation
The two available surgical options are mitral valve repair and mitral valve replacement. Mitral valve repair is the procedure of choice in the surgical management of MR caused by degenerative valve disease and in some cases of MR caused by infective endocarditis and ischemic heart disease. Mitral Valve Prolapse
o Mitral valve prolapse is a type of myxomatous valve disease. Mitral valve prolapse (MVP) is the systolic billowing of one or both mitral leaflets into the left atrium during systole. The tissue of the mitral valve leaflets and chordae are abnormally redundant, so that as the heart beats, the mitral valve bows or flops back into the left atrium ( See figure 6).
o Those with mitral valve prolapse may not have any regurgitation (leaky valve) or they may have a range of severity from a mild leak to a very floppy, leaky valve.
o The majority of people have no leak or a mild leak. In this case, MVP is not a cause for concern. A small percentage of people with mitral valve prolapse have severe MVP, requiring further treatment.
o Mitral valve prolapse is very common, affecting about three to five percent of the population. o Females are affected twice as often as males. o Mitral valve prolapse can be seen in children, teens, and adults.
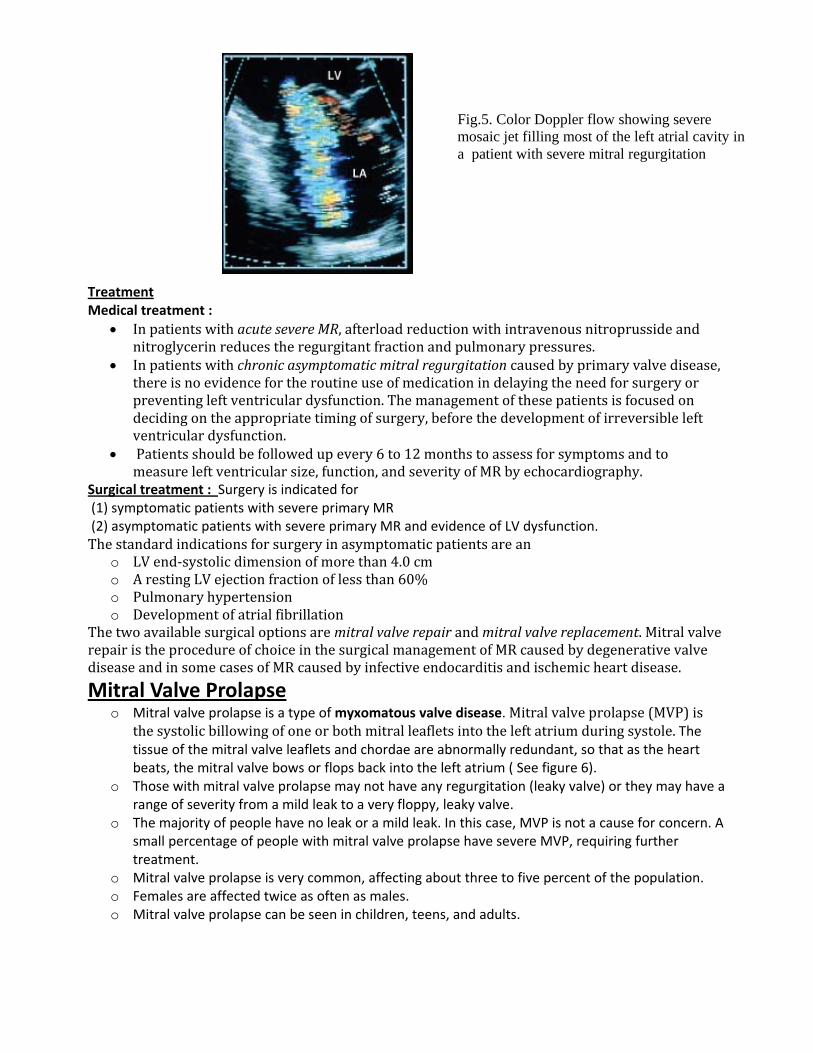
Fig.5. Color Doppler flow showing severe mosaic jet filling most of the left atrial cavity in a patient with severe mitral regurgitation
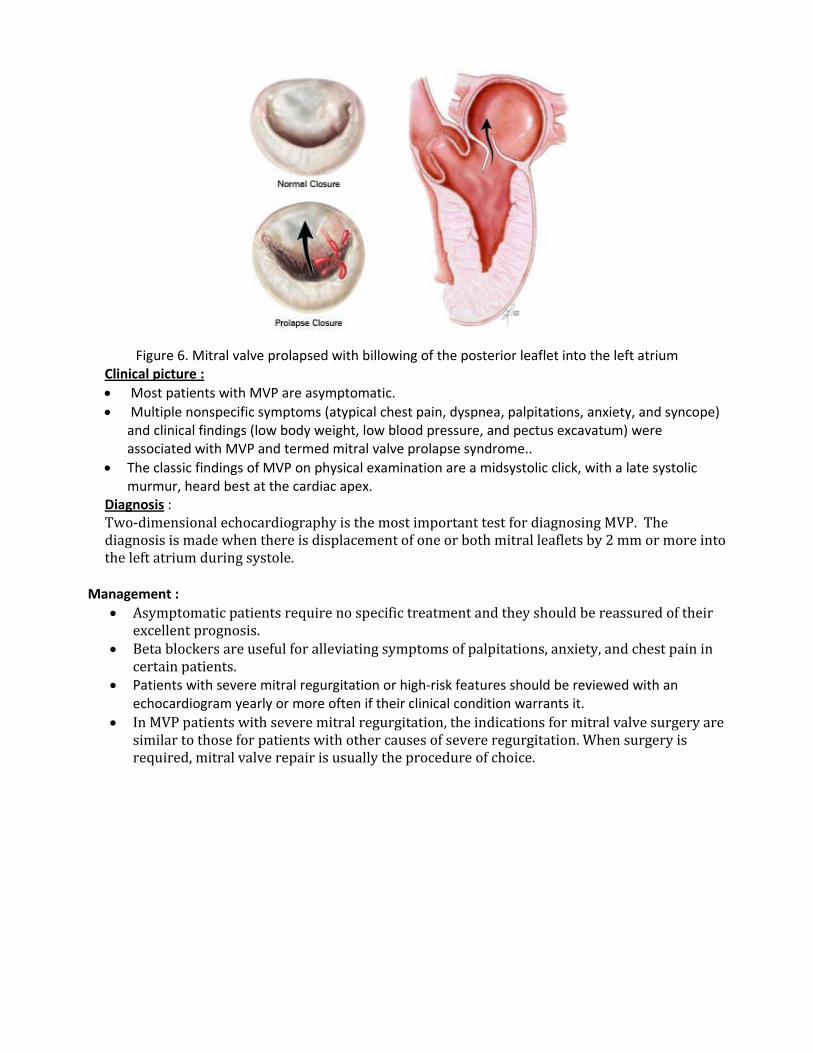
Figure 6. Mitral valve prolapsed with billowing of the posterior leaflet into the left atrium
Clinical picture : • Most patients with MVP are asymptomatic. • Multiple nonspecific symptoms (atypical chest pain, dyspnea, palpitations, anxiety, and syncope)
and clinical findings (low body weight, low blood pressure, and pectus excavatum) were associated with MVP and termed mitral valve prolapse syndrome..
• The classic findings of MVP on physical examination are a midsystolic click, with a late systolic murmur, heard best at the cardiac apex.
Diagnosis : Two‐dimensional echocardiography is the most important test for diagnosing MVP. The diagnosis is made when there is displacement of one or both mitral leaflets by 2 mm or more into the left atrium during systole.
Management : • Asymptomatic patients require no specific treatment and they should be reassured of their
excellent prognosis. • Beta blockers are useful for alleviating symptoms of palpitations, anxiety, and chest pain in
certain patients. • Patients with severe mitral regurgitation or high‐risk features should be reviewed with an
echocardiogram yearly or more often if their clinical condition warrants it. • In MVP patients with severe mitral regurgitation, the indications for mitral valve surgery are
similar to those for patients with other causes of severe regurgitation. When surgery is required, mitral valve repair is usually the procedure of choice.
Tricuspid Valve Disease.
o The tricuspid valve apparatus includes leaflets or cusps, chordae and papillary muscles, and tricuspd annulus. In general, the tricuspid valve has three distinct leaflets described as septal, anterior, and posterior and three sets of papillary muscles.
o Tricuspid valve disease is generally classified as primary (i.e. intrinsic) valve pathology or secondary. The latter is secondary to left‐heart disease and resulting right ventricular hypertension, dilatation, and dysfunction. It is also described as functional TR.
o The common causes of right ventricular (RV) hypertension, dilatation and failure are from left‐heart disease in form of advanced mitral, aortic and left ventricular myocardial disorders. Thus, TR is most commonly secondary to conditions affecting the left heart, and is caused by annular dilatation and leaflet tethering.
o Etiology of Primary Tricuspid Valve Disease 1. Rheumatic valve disease, generally in association with rheumatic mitral disease 3. Infective endocarditis 4. Carcinoid heart disease 5. Congenital (Ebstein anomaly)
Etiology of Secondary or Functional Tricuspid Valve Disease 1. Right ventricular dilatation2. Right ventricular hypertension (i.e., pulmonary hypertension) 3. Right ventricular dysfunction with cardiomyopathy.
Clinical Presentations The functional derangement may be in form of (1) pure or predominant tricuspid stenosis, (2) pure or predominant tricuspid regurgitation, or (3) mixed. Symptoms
• Generally the symptoms of left heart disease predominate in those with secondary tricuspid valve disease.
• The symptoms specific to advanced tricuspid valve disease are related to (a) Decreased cardiac output, for example, fatigue; (b) Right atrial hypertension, for example, liver congestion resulting in right upper quadrant discomfort, or gut congestion with symptoms of dyspepsia, indigestion, or fluid retention with leg edema and ascites.
Physical Signs These include signs related to tricuspid valve disease and those secondary to chronic venous congestion, that is, leg edema, ascites. Tricuspid stenosis
• Slow V to Y descent and prominent "a" waves. • Liver is enlarged with a firm edge, and pulsatile in presystole. • Auscultation reveals a low‐to‐medium‐pitched diastolic rumble with inspiratory
accentuation. Tricuspid regurgitation
• Prominent C‐V wave or systolic wave in venous pulse. • Parasternal lift from right ventricular enlargement. • Liver shows systolic pulsations, is enlarged and often tender. • Cardiac auscultation reveals a holosystolic murmur which is augmented with inspiratory
effort (Carvallo sign).
Diagnosis Electrocardiogram There are no specific markers of tricuspid valve (TV) disease, although the following clues may be present: (1) right ventricular (RV) hypertrophy and "strain" with right axis duration and (2) right atrial enlargement with prominent P waves. Chest Radiograph Cardiomegaly associated with prominent right‐heart borders may be noted. There are no specific findings to suggest a diagnosis of tricuspid valve disease. Echocardiography Two‐dimensional echocardiogram with color‐flow Doppler evaluation provides the most accurate and comprehensive laboratory test in evaluation of TV disease. The TV morphology helps differentiate primary from secondary TR . Its severity may be semiquantitated based on extent of the regurgitation jet penetration into the right atrium and inferior vena cava. Common Primary Tricuspid Valve Diseases Rheumatic Tricuspid Valve Disease
o Rheumatic involvement of the tricuspid valve is far less common than the mitral and the aortic valves.
o Isolated rheumatic tricuspid valve disease is rare. However, clinically significant tricuspid valve disease, in association with mitral and/or aortic valve disease, is reported between 10 and 20 % of patients.
o The tricuspid valve is thickened and the leaflets are contracted with fibrosis. Commissural fusion is often present. The resulting clinical syndrome is one of mixed stenosis and regurgitation.
o Treatment of rheumatic TV disease consists of valve repair with annuloplasty when the valve dysfunction is not severe. However, in presence of severe disease, valve replacement with a low profile mechanical or a bioprosthetic valve is indicated.
Infective Endocarditis o Infective endocarditis of the tricuspid valve is not uncommon among drug addicts using
intravenous drugs. o It may also be observed in patients with long‐term intravenous lines. o The clinical presentation is one of general systematic symptoms such as fever, weight loss,
anemia, and fatigue, or of pulmonary embolism, or of right‐heart failure with hepatic congestion, peripheral edema and ascites.
o The diagnostic confirmation is made by echocardiographic lesions suggestive of vegetations and positive blood cultures.
Carcinoid Heart Disease o Carcinoid tumors arising in the intestinal tract with secondary liver metastases are
commonly associated valvular pathology. o The most commonly affected valve is the tricuspid valve followed by the pulmonary valve.
The left‐sided cardiac valves are spared unless a right‐to‐left shunt through patent foramen ovale or atrial septal defect is present
o The pathology of the valve consists of thickening with fibrosis and markedly restricted motion. The valve leaflets are held partially open during systole and diastole. The opening results in obstructed inflow.
o Thus, there are signs of tricuspid stenosis and regurgitation, with the latter predominating. o The clinical features are those of the carcinoid tumor and right‐heart failure.
Ebstein Anomaly The Ebstein anomaly is a congenital lesion of tricuspid valve that is characterized by apical displacement of the septal leaflet of the tricuspid valve, a large, sail‐like anterior leaflet that results in atrialization of the RV inflow. Functionally, a variable degree of TR is observed. The right‐heart chambers are markedly dilated. A right‐to‐left shunt at atrial level may be present if atrial septal defect coexists.
MCQ 1. In pure mitral regurgitation S1 is
a. Normal
b. Accentuated
c. Decreased, soft
2. Features of left atrial enlargementin X‐Ray include
a. Double density
b. Elevation of left bronchus
c. Posterior displacement of the esophagus
d. All of the above
3. In middiastolic murmurs due to increased flow across atiroventricular valves, the common accompaniment is
a. Loud S1
b. Loud S2
c. S3
d. S4
4. Middiastolic murmurs due to increased flow across atiroventricular valves occur in
a. Mitral regurgitation
b. VSD
c. PDA
d. All of the above
5. Which of the following is not a middiastolic murmur
a. Carey Coomb murmur
b. Austin Flint murmur
c. Graham Steell murmur
d. Mitral stenosis
6.Holosystolic murmurs are usually caused by all except
a. Mitral regurgitation
b. Tricuspid regurgitation
c. VSD
d. Pulmonary stenosis
7.In a patient with mitral stenosis and mitral regurgitation, mitral regurgitation is said to be dominant in presence of all except
a. Soft S1
b. S3 c. Dominant V wave in jugular venous pulse
d. RV apex
8‐ Acute mitral regurgitation can occur due to
a. Infective endocarditis
b. Myocardial infarction
c. Cheat trauma
d. All of the above
9‐A middiastolic murmur may be heard in any of the following conditions
a. Mitral stenosis
b. Atrial myxoma
c. Mitral annular calcification
d. Parachute mitral valve
e. All of the above
10‐ Systemic embolization in patients with mitral stenosis most commonly occurs from
a. Left atrial mural thrombi
b. Left atrial appendage thrombi
c. Vegetations on the mitral valve
d. Left ventricular apical thrombi
11‐ A prominent “a” wave in jugular veins of patients with mitral stenosis indicates
a. Significant tricuspid regurgitation
b. Signficant mitral regurgitation
c. Pulmonary hypertension
d. Left atrial enlargement
12‐ The ventricular rate in patients with rapid atrial fibrillation can be controlled with
a. Beta blockers
b. Digoxin
c. Calcium channel blockers
d. Amiodarone
e. All of the above
13‐ The procedure of choice for patients with uncomplicated mitral stenosis with pliable, mobile, relatively thin, minimally calcified mitral leaflets with minimal or no subvalvular stenosis is
a. Mitral valve replacement
b. Percutaneous balloon mitral valvuloplasty
c. Surgical open mitral commissurotomy
d. All of the above
14‐ All these conditions can cause primary tricuspid disease EXCEPT:
a. Rheumatic heart disease
b. Infective endocarditis
c. Ebstein anomaly
d. Carcinoid heart disease
e. Left ventricular failure
15‐ All these are typical findings in severe tricuspid regurgitation EXCEPT:
a. The jugular venous pulse exhibiting prominent C‐V wave or systolic wave.
b. There is often a parasternal lift from right ventricular enlargement.
c. The liver shows systolic pulsations, is enlarged and often tender.
d. Ascitis and icterus in the sclera
e. Long middiastolic rumble with accentuation of first heart sound which is localized to the lower sternal border
16‐ Surgery is indicated in patients with mitral regurgitation, who are:
a. Symptomatic with severe mitral regurgitation
b. Asymptomatic with severe mitral regurgitation and LV dysfunction
c. Symptomatic patient with pulmonary hypertension
d. Severe mitral regurgitation complicated by atrial fibrillation
e. All of the above
17‐ All these findings may suggest severe mitral regurgitation except:
a. Fourth heart sound over the apex
b. Downward and outward displaced left ventricular apex
c. Third heart sound over the apex
d. Presence of pulmonary congestion in chest x ray film
e. All of the above