Embed Size (px)
Citation preview

ARTICLE OPEN ACCESS CLASS OF EVIDENCE
Mitigating alemtuzumab-associatedautoimmunity in MSA ldquowhack-a-molerdquo B-cell depletion strategy
Ethan Meltzer MD Sarah Campbell RN Benjamin Ehrenfeld MSW Roberto A Cruz MD
Lawrence SteinmanMD Matthew S Parsons PhD Scott S Zamvil MD PhD Elliot M Frohman MD PhD and
Teresa C Frohman MPAS MSCS PA-C FANA
Neurol Neuroimmunol Neuroinflamm 20207e868 doi101212NXI0000000000000868
Correspondence
Dr EM Frohman
Elliotfrohmanaustinutexasedu
AbstractObjectiveTo determine whether the punctuated administration of low-dose rituximab temporally linkedto B-cell hyperrepopulation (defined when the return of CD19+ B cells approximates 40ndash50of baseline levels as measured before alemtuzumab treatment inception) can mitigatealemtuzumab-associated secondary autoimmunity
MethodsIn this hypothesis-driven pilot study 10 patients received low-dose rituximab (50ndash150 mgm2) a chimeric anti-CD20 monoclonal antibody after either their first or second cycles ofalemtuzumab These patients were then routinely assessed for the development of autoimmunedisorders and safety signals related to the use of dual monoclonal antibody therapy
ResultsFive patients received at least 1 IV infusion of low-dose rituximab following alemtuzumabtherapy with a mean follow-up of 41 months None of the 5 patients developed secondaryautoimmune disorders An additional 5 patients with follow-up over less than 24 monthsreceived at least 1 infusion of low-dose rituximab treatment following alemtuzumab treatmentNo secondary autoimmune diseases were observed
ConclusionsAn anti-CD20 ldquowhack-a-molerdquo B-cell depletion strategy may serve to mitigate alemtuzumab-associated secondary autoimmunity in MS by reducing the imbalance in B- and T-cell regu-latory networks during immune reconstitution We believe that these observations warrantfurther investigation
Classification of evidenceThis study provides Class IV evidence that for people with MS low-dose rituximab followingalemtuzumab treatment decreases the risk of alemtuzumab-associated secondary autoimmunediseases
MORE ONLINE
Class of EvidenceCriteria for ratingtherapeutic and diagnosticstudies
NPuborgcoe
From the Department of Neurology (EM SC BE RAC) Dell Medical School University of Texas at Austin Department of Neurology (LS) Stanford University School ofMedicine Palo Alto CA Division of Microbiology and Immunology (MSP) Yerkes National Primate Research Center and Department of Pathology and Laboratory Medicine EmoryUniversity Atlanta GA Department of Neurology and Program in Immunology (SSZ) University of California San Francisco and Departments of Neurology (EMF TCF)Ophthalmology amp Neurosurgery Dell Medical School at the University of Texas at Austin
Go to NeurologyorgNN for full disclosures Funding information is provided at the end of the article
The Article Processing Charge was funded by the National Multiple Sclerosis Society
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License 40 (CC BY-NC-ND) which permits downloadingand sharing the work provided it is properly cited The work cannot be changed in any way or used commercially without permission from the journal
Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the American Academy of Neurology 1
Alemtuzumab a humanized anti-CD52 monoclonal antibodythat depletes circulating B and T lymphocytes is approved inthe United States and Europe for the treatment of MS12
Patients who receive alemtuzumab have an estimated 60rate of attaining No Evidence of Disease Activity status whichis defined by no new clinical relapses disease progression ornew MRI activity in a 5-year follow-up period34 Antibody-mediated secondary autoimmune disease in patients with MStreated with alemtuzumab approaches an incidence of40ndash50 in prolonged follow-up with a peak incidence bythe third year following treatment initiation and waning in-cidence thereafter5ndash16
Themain adverse effect of alemtuzumab is the development ofpredominantly antibody-mediated secondary autoimmunedisorders The most common secondary autoimmune disor-der is antibody-mediated thyroid disease with autoimmunehyperthyroidism being the most common and exceeding thosedeveloping hypothyroidism56 Other antibody-mediated au-toimmune diseases have been reported including idiopathicthrombocytopenic purpura antindashglomerular basement mem-brane (GBM) disease neutropenia hemolytic anemia andvitiligo among others T cellndashmediated autoimmunity andgranulomatous inflammatory diseases (principally sarcoidosis)occur at a considerably lower incidence1ndash16 An increased riskof opportunistic infections continues to be an important andpotentially serious complication of all cell-depleting disease-modifying treatment strategies although there are a number ofsystematic risk-mitigating strategies
Cooperation between B cells and T cells is required for B-celldifferentiation and mature antibody formation and yet it isnow well established that following alemtuzumab disease-modifying therapy for MS that there is a marked discordancein B vs T lymphocyte reconstitution kinetics with the formerbeing detected earlier and in considerably greater proportionusing objective methods for characterizing peripheral bloodmononuclear cells
Some evidence suggests that lymphocyte repopulation pat-terns in patients treated with alemtuzumab are not neces-sarily associated with the risk of developing secondaryautoimmune diseases1617 Instead a compromise in the in-tegrity of cellular regulatory networks corroborated sto-chastically by diminution in the regulatory signature ratios(eg the clonal frequency of regulatory T cells (Tregs) toTH-17 proinflammatory cells) could influence the functionalthresholds that determine the ignition of dynamic immuneresponse oscillations and their disposition toward activationvs anergy11 Furthermore reduced thymopoiesis can result in
the restricted heterogeneity in the T-cell receptor repertoirecreating conditions that can predispose to a heightened risk ofsecondary autoimmunity18 Therefore the discrepancy be-tween humoral and cellular immune networks appears to bebeyond the simplistic stochastic considerations
The kinetic disparities in the development release andrecirculation of B and T lymphocytes may have implicationsfor the coordinate-regulatory mechanisms which representthe immune basis for self-tolerance and the correspondingmolecular check-point verification strategies which are im-perative for ensuring the perpetual fidelity to discriminatebetween self and non-self (ie tolerance and its durability inresponse to challenges fundamental to its integrity and withtime especially with advancing age and the emergence of theincreasingly recognized property of immune senescence)
We hypothesize that anti-CD20 B-cell depletion punctuallyadministered and temporally coinciding with the precociousB-cell hyperrepopulation may represent a viable strategy formitigating the risk of alemtuzumab-associated secondaryautoimmunity
Here we report a strategic approach along with pilot observa-tions suggesting that the risk of secondary autoimmunity canpotentially be mitigated when low-dose anti-CD20 therapy isadministered during B-cell repopulation (ie what is referred to asa ldquowhack-a-molerdquo strategy19ndash23) following alemtuzumab therapy
MethodsThe study was approved by the Investigational Review Boardof the Dell Medical School at the University of Texas atAustin All patients consented for the off-label use ofrituximab
Our primary research question was to ascertain whether thepunctuated administration of low-dose rituximab temporallylinked with the discordant B-cell hyperrepopulation (whenthe return of the CD19+ cells approximated 40ndash50 ofbaseline measures examined before alemtuzumab therapyintervention) represents an effective strategy for mitigatingalemtuzumab-associated secondary autoimmunity (Class IVevidence)
We examined 2 small cohorts of 5 patients each The firstcohort (see table 1 for demographics) which was originallytreated with alemtuzumab received at least 1 infusion of low-dose rituximab (range 1 to gt3 doses 50ndash150 mgm2) afterB-cell reconstitution began Follow-up of these individuals
GlossaryANC = absolute neutrophil count EAE = experimental autoimmune encephalitis GBM = glomerular basement membraneNMOSD = neuromyelitis optica spectrum disorder Tregs = regulatory T cells
2 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
occurred for more than 24 months All patients who receivedalemtuzumab for treatment of MS were eligible Patients werenot selected on the basis of prior immunotherapy Rituximabis an anti-CD20 monoclonal antibody therapeutic In additionto CD20 CD19 is also a pan B-cell marker Anti-CD20therapeutic monoclonal antibody interferes with the recog-nition of the CD20 antigen As such the CD19+ B-cell levelas measured by flow cytometry was used as a proxy to mea-sure extent of B-cell depletion following anti-CD20 therapy24
Alemtuzumab-treated patients were scheduled to receiverituximab when CD19+ B cells repopulated to 40ndash50 oftheir baseline levels Baseline B-cell frequency was de-termined before initiation of alemtuzumab treatments byperforming lymphocyte subset analysis on 3ndash4 weekly blooddraws Rituximab dosing was predicated on insurance cov-erage Some dosages were delayed due to difficultiesobtaining insurance approval
In addition to monthly monitoring of T- and B-cell(ie CD3+ and CD19+) lymphocyte subsets we also mea-sured thyroid function urinalysis and complete blood countsat baseline and monthly thereafter This was performed inaccordance with the Risk Evaluation andMitigation Strategies
program for alemtuzumab to identify evidence of autoim-mune thyroiditis anti-GBM antibody disease or immunethrombocytopenic purpura
The second cohort of 5 patients (demographics are shown intable 2) whichwas originally treatedwith alemtuzumab receivedat least 1 infusion of low-dose rituximab after B-cell re-constitution to 40ndash50 of baseline Follow-up of these indi-viduals occurred for less than 24 months Lymphocyte subsetsthyroid function urinalysis and complete blood counts weremeasured at baseline andmonthly thereafter as described above
Given the low number of patients in this retrospective caseseries and variations in protocol we did not have adequatepower to perform statistical tests to determine the efficacy ofanti-CD20 therapy in preventing alemtuzumab-mediatedsecondary autoimmunity
Data availabilityDeidentified data will be shared with other investigators fol-lowing requests made to the corresponding author
ResultsOf the 5 patients with follow-up greater than 24 months(table 1) who received low-dose rituximab infusions followingalemtuzumab 1 patient received 2 rituximab infusions and 1patient received greater than 3 rituximab infusions due toprolonged T-cell suppression Two of the patients receivedrituximab after a single cycle of alemtuzumab and 3 of thepatients received rituximab after 2 cycles of alemtuzumabNone of the patients received 3 cycles of alemtuzumab givenevidence of clinical remission and radiographic stabilizationas confirmed on follow-up MRI investigations
Table 1 Clinical characteristics and results of patientswith long-term follow-up
Characteristic Value
No of patients 5
Age mean (SD) y 47 (11)
Sex female 60
Cycles of alemtuzumab
1a 20
2 80
Follow-up mean (SD) mo 41 (5)
Rituximab doses individuals
1 3
2 1
3+ 1
Rituximab timing individuals
1st cycle 2
2nd cycle 3
Both 0
Secondary autoimmune disease 0
Shown are clinical characteristics of patients who received low-dose ritux-imab with follow-up duration greater than 24 months characterized by agesex cycles of alemtuzumab follow-up duration doses of rituximab timingof doses and development of secondary autoimmune diseasea One patient received only a single cycle of alemtuzumab at the patientrsquosrequest due to disease stability
Table 2 Clinical characteristics and results of patientswith short-term follow-up
Characteristic Value
No of patients 5
Age mean (SD) y 44 (13)
Sex female 80
Follow-up mean (SD) mo 14 (2)
Rituximab doses individuals
1 2
2 3
Median time to CD19 50 baseline mo 2
Median time to first rituximab dose mo 3
Shown are clinical characteristics of patients who received low-dose ritux-imabwith follow-up duration less than 24months characterized by age sexfollow-up duration doses of rituximab time to rise in CD19 count and timeto first rituximab dose
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 3
For all 5 patients the mean follow-up duration from the initialdose of alemtuzumab was 41 months (range 34ndash48 months)None of the patients developed secondary autoimmunecomplications as defined by the Comparison of Alemtuzumaband Rebif Efficacy in Multiple Sclerosis (CARE-MS) I and IItrials34 Based on the results of CARE-MS I we anticipatedthat 30ndash40 of patients with long-term follow-up wouldhave developed autoimmune thyroid disease34
Of the 5 additional patients with a follow-up duration of less than24 months (table 2) who received low-dose rituximab treatmentfollowing alemtuzumab 2 patients received 1 infusion of ritux-imab and 3 patients received 2 infusions of rituximab Themedian time to 40ndash50 recovery of the CD19+ cell count was2 months post-alemtuzumab and the median time to the firstrituximab dose administration was 3 months post-alemtuzumab
In this second cohort 1 patient developed transient neu-tropenia with an absolute neutrophil count (ANC) lt500μL2 months after the second dose of 100 mg of rituximab Thispatient was treated with granulocyte colony-stimulating factorand reconstituted the ANC within 1 month Another patientdeveloped a urinary tract infection and an additional patientdeveloped an upper respiratory tract infection after receivinglow-dose rituximab while both B- and T-cell lymphocyteswere suppressed
Late-onset neutropenia is a well-described phenomenon afterrituximab infusion which has been considered to be relatedto transient autoimmunity25 Alternately neutropenia hasalso been documented in postmarketing surveillance ofalemtuzumab-treated patients albeit at a much lower in-cident rate when compared with the frequency of the mostcommon alemtuzumab-induced secondary autoimmuneconditions particularly thyroiditis (eg Graves disease andHashimoto thyroiditis)34
All patients treated in both patient cohorts were on pro-phylactic valacyclovir or acyclovir for 24 consecutive monthsincluding during treatment with low-dose rituximab givenhigh rates of herpes reactivation in the clinical trials
DiscussionAlemtuzumab treatment in MS is associated with an earlyhyperrepopulation of B cells that emerge between 3 and 6months following treatment which precedes the repopulationof T cells that occurs between 12 and 24 months followingtreatment A fundamental discordance in the return of humoraland cellular networks is likely to play a role at least in part in theincidence of the adverse event most strikingly associated withalemtuzumab treatment secondary autoimmunity26ndash29
T-cell help is required for B-cell differentiation isotypeswitching and antibody secretion The interaction betweenB cells and T cells is bidirectional As such anti-CD20 B-cell
depletion in MS and experimental autoimmune encephalitis(EAE) promotes T-cell immune modulation characterizedby a significant reduction in proinflammatory Th1 and Th17cells which likely reflects a decrease in B-cell antigen-presenting cell function26 In this context selective de-ficiency of major histocompatibility complex (MHC) ClassII expression by B cells in mice eliminates both susceptibilityto EAE and the expansion of Th1 and Th17 cells29
In the absence of T-cell help B cells are rendered unable todifferentiate between the antigen presentation of self- vsnonndashself-epitopes at least in part secondary to a considerablylower threshold for presentation of low-magnitude antigenswhen compared with macrophages or dendritic cells Fur-thermore anti-CD20 treatment of MS and EAE promotesT-cell immune modulation characterized by a significant re-duction in the proinflammatory network at least in partmediated by Th1726ndash29 Conspicuously B cellndashspecific MHCClass IIndashdeficient mice are rendered resistant to the de-velopment of EAE28
Secondary humoral autoimmunity resulting in hyper- or hy-pothyroidism thrombocytopenia or renal disease are wellknown risks following alemtuzumab treatment of MS56 Wehypothesize that anti-CD20 B-cell depletion after alemtuzu-mab administration may mitigate the risk of secondary auto-immunity and have investigated this possibility Our initialresults suggest that anti-CD20 B-cell depletion is safe andpotentially efficacious However given the small sample sizeand unrandomized and unblinded cohort more rigorousstudies need to be pursued before making any declarationregarding efficacy
Several hypotheses attempt to delineate the cause of sec-ondary autoimmune disease associated with alemtuzumabMSdisease-modifying therapy Unlike traditional B-cell returnafter anti-CD20 therapies B-cell repopulation occurs rapidlyfollowing alemtuzumab treatment and is associated withhyperrepopulation of immature and mature B cells abovebaseline levels30 Following alemtuzumab treatment B-cellrepopulation occurs well in advance of T-cell repopulation(3ndash6 months compared with 12ndash24 months re-spectively) which may compromise the counterbalancing ofhumoral and cellular mechanisms that serve to maintain im-mune regulation
Notwithstanding these findings secondary autoimmune dis-ease after alemtuzumab treatment exhibits a long latencybefore presentation that is well beyond the observed B-cellhyperrepopulation and in fact coincides more closely withT-cell repopulation as autoantibody production is likely CD4T-cell dependent31
T-cell regeneration after depletion in adults is predominantlyachieved by thymic-independent homeostatic peripheral ex-pansion This process unlike T-cell regeneration in childrenwhich occurs primarily in the thymus is associated with
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
decreased self-tolerance a potential molecular scaffolding onwhich autoimmunity can result31
The goal of the temporally associated administration of low-doserituximab is not exclusively restricted to delaying the return ofthe CD19+ B-cell population or an attempt to solely synchronizethe reconstitution of B- and T-cell subsets Data from clinicaltrials that have analyzed the kinetics of humoral and cellularsubsets reveal no evidence of correlation that dichotomizes therisk predilection for alemtuzumab-mediated secondary autoim-munity16 Future work should also characterize the effect ofrituximab on a unique and proinflammatory mononuclear cellwhich coexpresses both CD20 andCD3 (ie CD20+ T cells andchimeric or C cells) which may serve to promote secondaryautoimmunity and would be expected to be deleted along withCD20+ B cells during our administration of low-dose rituximab
A uniquemember of the immune systemrsquosmononuclear cell poolis the CD20+ T cell (ie a chimeric lymphocyte or C cell figure1) which includes both CD4+ and CD8+ cells with the latterbeing the predominant of this cell type Its T-cell origin has beenconfirmed via the detection of CD3 encoded mRNA via reversetranscriptase-polymerase chain reaction (RT-PCR)3233 Thedistribution of these cells is broad and includes the primary andsecondary lymphoid tissue thymus bone marrow lymph nodeadenoids liver and cerebrospinal fluid (CSF) Conspicuously atresting conditions CD20+ T cells exhibit augmented release ofcytokines vs CD20minusT cells Specifically they release interferon γinterleukin (IL) 1 β IL-2 IL-4 IL-8 IL-10 transforming growthfactor β tumor necrosis factor α and c-c chemokine34
Under conditions of immune stimulation there is an escala-tion in cytokine production in CD20+ T cells32 Furthermoreenhanced expression of IL-17 is also characteristic of thissmall population of lymphocytes33 In patients with relapsing-remitting and primary progressive MS vs healthy controlsthere is an increased frequency of CD20+T cells in peripheralblood35
In those with MS there is an increased clonal frequency ofsuch cells in CSF when compared with the analysis of pe-ripheral blood mononuclear cells and the magnitude of thatclonal frequency is correlated with clinical disability in pa-tients with MS as measured by the long-validated ExpandedDisability Status Scale score36 Also CD20+ T cells areidentified within chronic white matter plaque lesions derivedfrom the MS brain36 In drastic contrast to the small pro-portion of such cells from the peripheral blood of controls theCD20+ T-cell fraction in patients with MS represents astriking 184 of all CD20+ cells including those mono-nuclear cells that are CD19+ B cells37
B-cell hyperrepopulation accompanied by a reduction ofT-cell help establishes circumstances whereby antigen pre-sentation coordinated by B cells renders them unable todifferentiate between self (whereby antigen presentation ofautoantigens stereotypically produces immune anergy) and
foreign epitopes (which appropriately culminates in immuneactivation) Alternately the B-cell depletion also comes withthe downregulation of inflammatory cytokines secondary toB-cell induction of T-cell activity and the eventual cytokinerelease syndrome
A detailed figure (figure 1) delineates our hypothetical con-stellation of features proposed as the basis for a low-dose anti-CD20 whack-a-mole strategy aimed at mitigating secondaryautoimmunity
If our proposed risk mitigation strategy were to be used morebroadly for feasibility there would need to be a straightfor-ward way of timing rituximab infusions As such figure 2illustrates a schematic for a potential protocol using a low-dose anti-CD20 (rituximab) whack-a-mole secondary auto-immunity mitigation strategy post-alemtuzumab treatmentand its effect on B-cell repopulation Specifically we timedlow-dose rituximab infusion with a CD19+ B-cell recovery of50 of normal baseline We chose this as a relatively easymarker to measure and to ensure that patients would receiverituximab synchronous to the B-cell hyperrepopulation phaseof postndashalemtuzumab-induced bone marrow mononuclearcell mobilization
Alternatively rituximab could be given at a fixed interval suchas 3 or 4 months after alemtuzumab infusion a commonalbeit not consistent duration for the bone marrow mobili-zation and peripheral repopulation of B cells However ifB-cell hyperrepopulation is delayed (eg until 4ndash6 months) afixed timing for whack-a-mole administration of low-doseanti-CD20 therapy could predispose a significant proportionof patients to harbor a temporal discordance between suchtreatment and its intended targets consequently producing anineffective depletion of both CD20+ B cells and CD20+CD3+ T cells (likely resulting in a potential type II error inefficacy analyses)
Given the heterogeneity in the kinetics of B-cell repopu-lation following alemtuzumab therapy coupled with theknown median half-life of rituximab at 22 days (with a rangeof 61ndash52 days as per package insert) we strongly advise formonthly lymphocyte subset analysis to precisely synchro-nize administration of a rituximab low-dose anti-CD20whack-a-mole therapy strategy to buffer against the dis-cordant B-cell hyperrepopulation in the absence of ade-quate T-cell help In addition this strategy will attenuatethe reemergence of the proinflammatory CD20+ T cellsIt remains to be seen if a single dose of rituximab willbe sufficient or whether multiple whack-a-mole cycleswill be required for a therapeutic effect of preventingalemtuzumab-associated secondary autoimmunity
It is of interest that anti-CD20 therapy achieves about a 99loss of peripheral blood B lymphocytes without affectingplasma cells or plasmablasts the principal antibody-secretingcells which are devoid of cell surface CD20 expression In
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 5
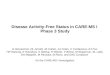
Figure 1 A model for the mitigation of secondary autoimmunity in patients with MS post-alemtuzumab
In the upper portion of the figure we illustrate alemtuzumab treatment and its effect on elimination of antindashself-lymphocytes by 2 principal mechanismsclearance through the reticular endothelial system (RES on the left) and assembly of themembrane attack complex (MAC) facilitating the passage of C9 whichcompromises cell membrane integrity thereby culminating in cytotoxicity and cell death The lower middle illustration emphasizes post-alemtuzumabtreatment-inducedmobilization of bonemarrow stem cells reconstituting the immune system B cells undergo a discordant hyperrepopulation approachingpretreatment baseline numbers 3ndash6 months following alemtuzumab treatment whereas T-cell reconstitution is considerably delayed (12ndash24 months)Hypothetically the highly discordant hyperrepopulation of B cells plays a role in the development of secondary autoimmunity Post-alemtuzumab treatmentcirculatingmononuclear cells are principally CD3+-naive T cells CD19+ CD20+-naive B cells as well as a unique population of cells that express both the B-cellantigen CD20 and the T-cell antigen CD3 These latter cells we refer to as Chimeric lymphocytes (C cells) and they are known to express proinflammatorycytokines which in the absence of adequate T-cell help can foment the production of antindashself-antibodies This can initiate corresponding autoantibody-mediated disorders such as those designated by green labels in the figure as well as to T cells capable of orchestrating cellularmechanisms of autoimmunity(designated by purple labels) To the lower left of the lower diagram one can see an enrichment in the CD3+ CD20+ C cells simultaneouswith the discordant B-cell hyperrepopulation (generally emerging approximately 3ndash6 months following alemtuzumab treatment) in the context of a deficiency in the clonalfrequency of regulatory T cells (Tregs) (ie identified as CD4+CD25hiFoxP3+) In the absence of T-cell help such B cells are rendered incapable of discriminatingbetween self and foreign epitopes to both other B cells thereby coordinating the development of antibodies as well as to T cells leading to T-cell receptormaturation with elaboration of cytokine and chemokine expression profiles commensurate to foment cellular autoimmunemechanisms The central portionof the diagram serves to illustrate the potential diversity of antibody-mediated secondary autoimmune states (green line paths) We also see activation ofT cells which can mediate secondary autoimmunity (purple line paths) and granulomatous inflammatory disease most specifically sarcoidosis Monitoringmonthly lymphocyte subsets facilitates detection of the discordant B-cell hyperrepopulation phase of bone marrow mononuclear cell mobilization afteralemtuzumab therapy and thereby provides for the discrete and temporally punctuated administration of an anti-CD20 ldquowhack-a-molerdquo strategy formitigating secondary autoimmunity Specifically we administered low-dose rituximab to orchestrate the deletionof bothCD20+B cells in conjunctionwith theCD20+CD3+ C cells along with their B-cell activation capabilities via the elaboration of proinflammatory cytokine and chemokine cascades The net effect isseen approximately 4months later (in the upper circle on the right lower side of the diagram) when there is amarked diminution of both effectormemory Bcells and autoimmunity-inducing C cells with a corresponding expansion in the clonal frequency of Tregs
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
keeping with this observation anti-CD20 therapy appears toexert no impact on CSF antibody indices such as oligoclonalbanding increased immuno gamma globulin (IgG) indexandor an elevation in IgG synthesis rates characteristic ab-normalities identified in approximately 90 of patients withMS when using isoelectric focusing techniques Alternatelythe peripheral loss of B cells does correspond to a markedreduction in the development of both T1 gadolinium-enhancing and combined unique MS plaque lesions3839
In a recent study the third-generation glycoengineered chi-meric anti-CD20 therapy ublituximab was shown to reduceboth effector and memory CD8 T-cell populations while alsoaugmenting the clonal frequency of naive CD8+ T cells38 Oneof the most conspicuous observations was the identification ofa population of lymphocytes with cell surface expression ofboth CD20+ and CD3+ (those designated as chimeric or Ccells in our hypothetical model figure 1) with further char-acterization revealing that such cells exhibit features inkeeping with memory CD8+ T cells40
The functionally chimeric lymphocytes produce proin-flammatory mediators which may play a key role in thepromiscuous antigen presentation of self-motifs during thediscordant hyperrepopulation of B cells following alemtuzu-mab treatment (figure 1) Lovett-Racke et al categoricallycharacterized both the cellular identification and cytokinechemokine expression profiles using flow cytometric tech-niques from 47 patients withMS treated with ublituximab and
confirmed that such treatment resulted in significantly at-tenuated expression of proinflammatory cytokines reducedantigen presentation a shift from the effectormemory phe-notype to repopulation of naive lymphocytes and importantlyaugmentation in the clonal frequency of regulatory T cells(Tregs)33
A primary immune defect in patients with MS is a deficiencyin Tregs Efficacy in treating the disorder at least in partinvolves reconstitution of the immune networkrsquos regulatorycapabilities through the expansion of Tregs specificallyidentified as CD4+CD25hiFoxP3+2838 The observationsfrom this investigation suggest that anti-CD20 therapy is ca-pable of provoking a skewing or immune deviation that maybe secondary perhaps at least in part to the deletion ofCD20+CD3+ C cells thereby resulting in reduced B cellndashmediated degenerate antigen presentation of self-motifsalong with a broadening in the clonal frequency of Tregs all ofwhich may be germane to our understanding of how we canuse alemtuzumab while actively reducing (vis a vis with theapplication of a lsquowhack-a-molersquo cell depletion strategy) theincidence of secondary autoimmunity (figures 1 and 2)33
We successfully used low-dose rituximab 100 mg (50ndash75mgm2) for patients with neuromyelitis optica spectrumdisorder (NMOSD) who could not afford access to higherdoses of rituximab A 100-mg infusion depletes the CD19population of B cells to less than 2 for an average of 99 days(in essence B-cell suppression is highly titratable analogous
Figure 2 Low-dose anti-CD20 therapy post-alemtuzumab schematic illustrating a potential pilot protocol
This schematic depicts normal CD4+ and CD19+ cell reconstitution9 as well as the theoretical CD19+ reconstitution with our proposed low-dose rituximabprotocol Low-dose rituximab (eg 100 mg) is given subsequent to the detection of the precociously discordant B-cell hyperrepopulation phase of bonemarrow mononuclear cell mobilization following alemtuzumab treatment an intervention which attenuates promiscuous antigen presentation by B cellscapable of activating antindashself-humoral and cellular networks while also serving to promote a more synchronized repopulation across the bone marrowmobilization of mononuclear cell heterogeneity (ie achieving a more balanced return of B and T lymphocyte populations with the added dividend ofamplifying the clonal frequency of Tregs and observation akin to tolerance induction in patients with MS)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 7
to immunologic labetalol the latter commonly used as ahighly titratable agent for management of hypertensive crisessuch as hypertensive encephalopathy where loss of cerebro-vascular autoregulation precludes the employment of long-acting agents which could result in a protracted compromisein cerebral blood flow dynamics predisposing to a hypoxic-ischemic insult) in patients with NMOSD compared with 184days for a 1000 mg dose of rituximab41
Low-dose rituximab is a more attractive alternative to stan-dard doses of 1000 mg or 375 mgm2 First doses of ritux-imab as low as 1 mgm2 suppress B cells by 97 in healthycontrols and B cells remain suppressed to 75 of baselinelevels at 12 weeks after infusion4243
Second low-dose anti-CD20 therapy does not result in pro-longed B-cell depletion so as not to interfere with repeatcycles of alemtuzumab therapy41
Third low-dose rituximab may facilitate greater control ofB-cell repopulation and improved temporal synchronizationwith T-cell repopulation
Last reduced dosing magnitude reduces the duration of im-munosuppression compared with conventional doses of rit-uximab and may eventually be shown in evidence-basedstudies to demonstrate both safety and cost advantages if fewcomplications are identified with the low-dose regimen
A more robust clinical trial with a primary outcome of thedevelopment of secondary autoimmunity would not likelyrequire a large number of participants given the incidence rateof 40 of autoimmune thyroid disease in patients with MSwho have received alemtuzumab34 Hence we would esti-mate an incidence of 40 in the control group ofalemtuzumab-only treated patients and with an assumption ofan incidence of 10 in patients who would receive adjunctrituximab If we assign the probability of a type I error of 5and a power of 80 a trial would need approximately 80patients total (40 in each arm) accounting for drop-outs
In addition to our small sample size and an unrandomizedand unblended cohort many physicians prescribe steroidswith rituximab infusion (methylprednisolone 250 mg beforeeach and every alemtuzumab infusion in our center) to pre-vent infusion reactions It is possible that the potential positiveeffects of secondary autoimmunity prevention attributed torituximab are instead or at least in part due to steroid usageIn addition treatment may simply delay secondary autoim-munity rather than preventing it and longer periods of as-certainment will be required to assess for this prospect
An alternate explanation concerning the impact of rituximabon secondary autoimmunity is that some individuals mayrespond differently to low-dose anti-CD20 therapy due to theeffects of the FCGR3A polymorphism42 We do not know theeffect of the polymorphism on low-dose rituximab kinetics
however binding affinity may play a larger role in low-doserituximab compared with conventional doses given the lowerabsolute concentration of rituximab Such issues should becarefully considered in the design of a larger trial particularlygiven potential effects of such factors on response character-istics as well as on study cost
As the field of neurology shifts from amodel of step escalationto induction therapy for the treatment of MS strategies thatare aimed at mitigating the risks of potent disease modifyingtherapies are urgently needed43
Only through the scientific method of subjecting our hy-pothesis to the rigors of a controlled adequately blindedprospective and adequately powered clinical trial can weconfirm or refute the hypothesis-driven question can theapplication of low-dose anti-CD20 therapy temporally syn-chronized with objective confirmation of B-cell hyper-repopulation serve to adequately reduce or even preventalemtuzumab-associated secondary autoimmunity
Furthermore the addition of anti-CD20 therapy could po-tentially confer benefits on immune deviation that would exertadded efficacy in synergy with the alemtuzumab-mediatedmechanisms of action in the establishment of disease re-mission while constituting augmented and durable regulatoryproperties in keeping with those achieved during the criticalperiod that we now recognize collectively as self-tolerance
Buffeted by the broad dissemination of bone marrow mobili-zation of stem cells following alemtuzumab treatment maypromote the process of restoration and neurologic functionalreconstitution Recent evidence has demonstrated that anemerging biomarker for assessing tissue damage in the CNS ofpatients withMS the neurofilament light chain is reducedmostmarkedly following the administration of alemtuzumab whencompared with other disease-modifying therapies and that suchlevels remain reduced to the greatest magnitude over time44
It was once thought that a proposition such as repair andfunctional recovery from MS was wholly enigmatic and un-likely However we have arrived at a point in the history of ourunderstanding of the disorderrsquos pathobiology in concert withthe corresponding derangements in immune regulatory in-fluences and how to remediate them We believe our work torepresent but a single small step toward this constellation ofgoals that are so important to our deserving patients theirfamilies our community and those of us who serve on thoseteams who care for and about them
AcknowledgmentThe authors thank Mr Jason Ooi and Dr Matthew Parsonsfor their transformation and production of Elliot andTeresa Frohmanrsquos formulation of the figure 1 medicalillustration which showcases alemtuzumabrsquos mechanism ofaction the pathobiological underpinnings for treatment-associated secondary autoimmunity and the hypothetical
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
mechanisms germane to our ldquowhack-a-molerdquo B-cell de-letion strategy aimed at mitigating alemtuzumab-associatedautoimmunity in MS
Study fundingThe National Multiple Sclerosis Society 5-Year InstitutionalFellowship Training Grant Awarded to TC Frohman andEM Frohman Fellows funded E Meltzer and RA Cruz(coauthors) MS and Neuroimmunology Center The DellMedical School at The University of Texas at Austin
DisclosureE Meltzer served as a consultant for Genzyme and receivedhonoraria from Novartis S Campbell and B Ehrenfeld havenothing to disclose L Steinman is on the Editorial Boards ofthe Proceedings of the National Academy of Sciences and theJournal of Neuroimmunology He has served on the EditorialBoard of the Journal of Immunology and International Immu-nology He has served as a member of grant review committeesfor the NIH and the National MS Society He has served orserves as a consultant and received honoraria from AtaraBiotherapeutics Atreca Biogen-Idec Celgene CentocorCoherus EMD-Serono Genzyme Johnson and JohnsonNovartis RocheGenentech Teva Pharmaceuticals Incand TG Therapeutics He has served on the Data SafetyMonitoring Board for TG Therapeutics He serves on theBoard of Directors of Tolerion and Chairs the ScientificAdvisory Board for Atreca Currently L Steinman receivesresearch grant support from the NIH and Atara Bio-therapeutics MS Parsons has nothing to disclose SSZamvil is Deputy Editor ofNeurology Neuroimmunology andNeuroinflammation and is an Associate Editor for Frontiers inImmunology and Frontiers in Neurology He serves on theAdvisory Committee for the American Congress onTreatment and Research in Multiple Sclerosis (ACTRIMS)and is a standing member of the research grant reviewcommittee for the National Multiple Sclerosis Society(NMSS) He has served on the Editorial Board of theJournal of Clinical Investigation The Journal of Immunologyand The Journal of Neurological Sciences and has been acharter member of the grant review committee for the NIHClinical Neuroimmunology and Brain Tumors (CNBT)He has served or serves as a consultant and receivedhonoraria from Alexion Biogen-Idec EMD-SeronoGenzyme Novartis RocheGenentech and Teva Pharma-ceuticals Inc and has served on Data Safety MonitoringBoards for Lilly BioMS Teva and Opexa TherapeuticsCurrently SS Zamvil receives research grant support fromthe NIH NMSS Weill Institute Race to Erase MS and theMaisin Foundation TC Frohman has received advisoryboard fees from Alexion EM Frohman has receivedspeaker honoraria from Genzyme Novartis Alexion andAcorda Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationDecember 25 2019 Accepted in final form July 6 2020
References1 Coles AJ Twyman CL Arnold DL et al Alemtuzumab for patients with relapsing
multiple sclerosis after disease-modifying therapy a randomised controlled phase 3trial Lancet 20123801829ndash1839
2 Cohen JA Coles AJ Arnold DL et al Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis a randomisedcontrolled phase 3 trial Lancet 20123801819ndash1828
3 Coles AJ Cohen JA Fox EJ et al Alemtuzumab CARE-MS II 5-year follow-upNeurology 2017891117ndash1126
4 Havrdova E Arnold DL Cohen JA et al Alemtuzumab CARE-MS I 5-year follow-upNeurology 2017891107ndash1116
5 Sarvepalli D Rashid MU Ullah W Zafar Y Khan M Idiopathic thrombocytopenicpurpura a rare syndrome with alemtuzumab review of monitoring protocol Cureus201911e5715
6 Ruck T Schulte-Mecklenbeck A Pfeuffer S et al Pretreatment anti-thyroid auto-antibodies indicate increased risk for thyroid autoimmunity secondary to alemtuzu-mab a prospective cohort study EBioMedicine 201946381ndash386
Appendix Authors
Name Location Contribution
Ethan MeltzerMD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
SarahCampbell RN
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
BenjaminEhrenfeldMSW
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
Roberto ACruz MD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
LawrenceSteinman MD
Department ofNeurology StanfordUniversity School ofMedicine
Conception and criticalrevision of themanuscript forintellectual content
Matthew SParsons PhD
Division of Microbiologyand Immunology YerkesNational PrimateResearch CenterDepartment of Pathologyand Laboratory MedicineEmory University
Conception and criticalrevision of themanuscript forintellectual content
Scott S ZamvilMD PhD
Department ofNeurology amp Program inImmunology Universityof California SanFrancisco
Conception and criticalrevision of themanuscript forintellectual content
Elliot MFrohman MDPhD
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical SchoolUniversity of Texas atAustin
Conception and criticalrevision of themanuscript forintellectual content
Teresa CFrohmanMPAS MSCSPA-C FANA
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical School Universityof Texas at Austin
Conception and criticalrevision of themanuscript forintellectual content
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 9
7 Ruck T Pfeuffer S Schulte-Mecklenbeck A et al Vitiligo after alemtuzumab treat-ment secondary autoimmunity is not all about B cells Neurology 201891e2233ndashe2237
8 Zimmermann J Buhl T Muller M Alopecia universalis following alemtuzumabtreatment in multiple sclerosis a barely recognized manifestation of secondaryautoimmunity-report of a case and review of the literature Front Neurol 20178569
9 Rotondi M Molteni M Leporati P Capelli V Marino M Chiovato L Autoimmunethyroid diseases in patients treated with alemtuzumab for multiple sclerosis an ex-ample of selective anti-TSH-receptor immune response Front Endocrinol (Lau-sanne) 20178254
10 Costelloe L Jones J Coles A Secondary autoimmune diseases following alemtuzu-mab therapy for multiple sclerosis Expert Rev Neurother 201212335ndash341
11 Jones JL Phuah CL Cox AL et al IL-21 drives secondary autoimmunity in patientswith multiple sclerosis following therapeutic lymphocyte depletion with alemtuzu-mab (Campath-1H) J Clin Invest 20091192052ndash2061
12 Torino F Barnabei A Paragliola R Baldelli R Appetecchia M Corsello SM Thyroiddysfunction as an unintended side effect of anticancer drugs Thyroid 2013231345ndash1366
13 Azzopardi L Thompson SA Harding KE et al Predicting autoimmunity afteralemtuzumab treatment of multiple sclerosis J Neurol Neurosurg Psychiatry 201485795ndash798
14 Trinh T Haridas AS Sullivan TJ Ocular findings in alemtuzumab (Campath-1H)-induced thyroid eye disease Ophthalmic Plast Reconstr Surg 201632e128ndashe129
15 von Kutzleben S Pryce G Giovannoni G Baker D Depletion of CD52-positivecells inhibits the development of central nervous system autoimmune disease butdeletes an immune-tolerance promoting CD8 T-cell population Implications forsecondary autoimmunity of alemtuzumab in multiple sclerosis Immunology 2017150444ndash455
16 Wiendl H Carraro M Comi G et al Lymphocyte pharmacodynamics are not asso-ciated with autoimmunity or efficacy after alemtuzumab Neurol NeuroimmunolNeuroinflamm 201971ndash10 doi101212NXI0000000000000635
17 Kousin-Ezewu O Azzopardi L Parker RA et al Accelerated lymphocyte recoveryafter alemtuzumab does not predict multiple sclerosis activity Neurology 2014822158ndash2164
18 Jones J Thompson S Loh P et al Human autoimmunity after lymphocyte depletionis caused by homeostatic T-cell proliferation Proc Natl Acad Sci U S A 201311020200ndash20205
19 Costa DB Kobayashi SS Whacking a mole-cule clinical activity and mechanisms ofresistance to third generation EGFR inhibitors in EGFR mutated lung cancers withEGFR-T790M Transl Lung Cancer Res 20156809ndash815
20 Shin J MacCarthy T Antagonistic coevolution drives whack-a-mole sensitivity ingene regulatory networks PLoS Comput Biol 201511e1004432
21 Suzuki K Whack-a-mole strategy for multifocal ground glass opacities of the lungJ Thorac Dis 20179(suppl 3)S201ndashS207
22 Swanson DS Harrison CJ Playing Whack-a-Mole with pneumococcal serotypeeradication Pediatrics 2017140e20172034
23 Mestrovic T A microbial game of whack-a-mole clinical case series of the urethraluncloaking phenomenon caused by Corynebacterium glucuronolyticum in mentreated for Chlamydia trachomatis urethritis Infection 201947121ndash124
24 Gelfand JM Cree BAC Hauser SL Ocrelizumab and other CD20+ B-cell-depletingtherapies in multiple sclerosis Neurotherapeutics 201714835ndash841
25 Voog E Morschhauser F Solal-Celigny P Neutropenia in patients treated with rit-uximab N Engl J Med 20033482691ndash2694 discussion 2691ndash2694
26 Bar-Or A Fawaz L Fan B et al Abnormal B-cell cytokine responses a trigger of T-cell-mediated disease in MS Ann Neurol 201067452ndash461
27 Weber MS Prodrsquohomme T Patarroyo JC et al B-cell activation influences T-cellpolarization and outcome of anti-CD20 B-cell depletion in central nervous systemautoimmunity Ann Neurol 201068369ndash383
28 Monson NL Cravens P Hussain R et al Rituximab therapy reduces organ-specificT cell responses and ameliorates experimental autoimmune encephalomyelitis PLoSOne 20116e17103
29 Molnarfi N Schulze-Topphoff U Weber MS et al MHC class II-dependent B cellAPC function is required for induction of CNS autoimmunity independent of myelin-specific antibodies J Exp Med 20132102921ndash2937
30 Baker D Herrod SS Alvarez-Gonzalez C Giovannoni G Schmierer KInterpreting lymphocyte reconstitution data from the pivotal phase 3 trials of alem-tuzumab JAMA Neurol 201774961ndash969
31 Krupica T Fry TJ Mackall CL Autoimmunity during lymphopenia a two-hit modelClin Immunol 2006120121ndash128
32 Wilk EWitte TMarquardt N et al Depletion of functionally active CD20+ T cells byrituximab treatment Arthritis Rheum 2009603563ndash3571
33 Schuh E Berer K Mulazzani M et al Features of human CD3+CD20+ T cellsJ Immunol 20161971111ndash1117
34 Gingele S Kripuletz T Jacobs R Role of CD20+ T cells in multiple sclerosisimpli-cations for treatment with ocrelizumab Neural Regen Res 202015663ndash664
35 Palanichamy A Jahn S Nickles D et al Rituximab efficiently depletes increasedCD20-expressing T cells in multiple sclerosis patients J Immunol 2014193580ndash586
36 Holley JE Bremer E Kendall AC et al CD20+ inflammatory T-cells are present inblood and brain of multiple sclerosis patients and can be selectively targeted forapoptotic elimination Mult Scler Relat Disord 20143650ndash685
37 von Essen MR Ammitzboslashll C Hansen RH et al Proinflammatory CD20+ T cells inthe pathogenesis of multiple sclerosis Brain 2019142120ndash132
38 Lovett-Racke AE Gormley M Liu Y et al B cell depletion with ublituximab reshapesthe T cell profile in multiple sclerosis patients J Neuroimmunol 2019332187ndash197
39 Cross AH Stark JL Lauber J Ramsbottom MJ Lyons JA Rituximab reduces B cells andT cells in cerebrospinal fluid ofmultiple sclerosis patients J Neuroimmunol 200618063ndash70
40 Naismith RT Piccio L Lyons JA et al Rituximab add-on therapy for breakthroughrelapsing multiple sclerosis a 52-week phase II trial Neurology 2010741860ndash1867
41 Greenberg BM Graves D Remington G et al Rituximab dosing and monitoringstrategies in neuromyelitis optica patients creating strategies for therapeutic successMult Scler 2012181022ndash1026
42 Kim SH Jeong IH Hyun JW et al Treatment outcomes with rituximab in 100patients with neuromyelitis optica influence of FCGR3A polymorphisms on thetherapeutic response to rituximab JAMA Neurol 201572989ndash995
43 Steinman L Induction of new autoimmune diseases after alemtuzumab therapy formultiple sclerosis learning from adversity JAMA Neurol 201774907ndash908
44 Delcoigne B Manouchehrinia A Barro C et al Blood neurofilament light levelssegregate treatment effects in multiple sclerosis Neurology 202094e1201ndashe1212
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
DOI 101212NXI000000000000086820207 Neurol Neuroimmunol Neuroinflamm
Ethan Meltzer Sarah Campbell Benjamin Ehrenfeld et al depletion strategy
Mitigating alemtuzumab-associated autoimmunity in MS A whack-a-mole B-cell
This information is current as of August 7 2020
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

Alemtuzumab a humanized anti-CD52 monoclonal antibodythat depletes circulating B and T lymphocytes is approved inthe United States and Europe for the treatment of MS12
Patients who receive alemtuzumab have an estimated 60rate of attaining No Evidence of Disease Activity status whichis defined by no new clinical relapses disease progression ornew MRI activity in a 5-year follow-up period34 Antibody-mediated secondary autoimmune disease in patients with MStreated with alemtuzumab approaches an incidence of40ndash50 in prolonged follow-up with a peak incidence bythe third year following treatment initiation and waning in-cidence thereafter5ndash16
Themain adverse effect of alemtuzumab is the development ofpredominantly antibody-mediated secondary autoimmunedisorders The most common secondary autoimmune disor-der is antibody-mediated thyroid disease with autoimmunehyperthyroidism being the most common and exceeding thosedeveloping hypothyroidism56 Other antibody-mediated au-toimmune diseases have been reported including idiopathicthrombocytopenic purpura antindashglomerular basement mem-brane (GBM) disease neutropenia hemolytic anemia andvitiligo among others T cellndashmediated autoimmunity andgranulomatous inflammatory diseases (principally sarcoidosis)occur at a considerably lower incidence1ndash16 An increased riskof opportunistic infections continues to be an important andpotentially serious complication of all cell-depleting disease-modifying treatment strategies although there are a number ofsystematic risk-mitigating strategies
Cooperation between B cells and T cells is required for B-celldifferentiation and mature antibody formation and yet it isnow well established that following alemtuzumab disease-modifying therapy for MS that there is a marked discordancein B vs T lymphocyte reconstitution kinetics with the formerbeing detected earlier and in considerably greater proportionusing objective methods for characterizing peripheral bloodmononuclear cells
Some evidence suggests that lymphocyte repopulation pat-terns in patients treated with alemtuzumab are not neces-sarily associated with the risk of developing secondaryautoimmune diseases1617 Instead a compromise in the in-tegrity of cellular regulatory networks corroborated sto-chastically by diminution in the regulatory signature ratios(eg the clonal frequency of regulatory T cells (Tregs) toTH-17 proinflammatory cells) could influence the functionalthresholds that determine the ignition of dynamic immuneresponse oscillations and their disposition toward activationvs anergy11 Furthermore reduced thymopoiesis can result in
the restricted heterogeneity in the T-cell receptor repertoirecreating conditions that can predispose to a heightened risk ofsecondary autoimmunity18 Therefore the discrepancy be-tween humoral and cellular immune networks appears to bebeyond the simplistic stochastic considerations
The kinetic disparities in the development release andrecirculation of B and T lymphocytes may have implicationsfor the coordinate-regulatory mechanisms which representthe immune basis for self-tolerance and the correspondingmolecular check-point verification strategies which are im-perative for ensuring the perpetual fidelity to discriminatebetween self and non-self (ie tolerance and its durability inresponse to challenges fundamental to its integrity and withtime especially with advancing age and the emergence of theincreasingly recognized property of immune senescence)
We hypothesize that anti-CD20 B-cell depletion punctuallyadministered and temporally coinciding with the precociousB-cell hyperrepopulation may represent a viable strategy formitigating the risk of alemtuzumab-associated secondaryautoimmunity
Here we report a strategic approach along with pilot observa-tions suggesting that the risk of secondary autoimmunity canpotentially be mitigated when low-dose anti-CD20 therapy isadministered during B-cell repopulation (ie what is referred to asa ldquowhack-a-molerdquo strategy19ndash23) following alemtuzumab therapy
MethodsThe study was approved by the Investigational Review Boardof the Dell Medical School at the University of Texas atAustin All patients consented for the off-label use ofrituximab
Our primary research question was to ascertain whether thepunctuated administration of low-dose rituximab temporallylinked with the discordant B-cell hyperrepopulation (whenthe return of the CD19+ cells approximated 40ndash50 ofbaseline measures examined before alemtuzumab therapyintervention) represents an effective strategy for mitigatingalemtuzumab-associated secondary autoimmunity (Class IVevidence)
We examined 2 small cohorts of 5 patients each The firstcohort (see table 1 for demographics) which was originallytreated with alemtuzumab received at least 1 infusion of low-dose rituximab (range 1 to gt3 doses 50ndash150 mgm2) afterB-cell reconstitution began Follow-up of these individuals
GlossaryANC = absolute neutrophil count EAE = experimental autoimmune encephalitis GBM = glomerular basement membraneNMOSD = neuromyelitis optica spectrum disorder Tregs = regulatory T cells
2 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
occurred for more than 24 months All patients who receivedalemtuzumab for treatment of MS were eligible Patients werenot selected on the basis of prior immunotherapy Rituximabis an anti-CD20 monoclonal antibody therapeutic In additionto CD20 CD19 is also a pan B-cell marker Anti-CD20therapeutic monoclonal antibody interferes with the recog-nition of the CD20 antigen As such the CD19+ B-cell levelas measured by flow cytometry was used as a proxy to mea-sure extent of B-cell depletion following anti-CD20 therapy24
Alemtuzumab-treated patients were scheduled to receiverituximab when CD19+ B cells repopulated to 40ndash50 oftheir baseline levels Baseline B-cell frequency was de-termined before initiation of alemtuzumab treatments byperforming lymphocyte subset analysis on 3ndash4 weekly blooddraws Rituximab dosing was predicated on insurance cov-erage Some dosages were delayed due to difficultiesobtaining insurance approval
In addition to monthly monitoring of T- and B-cell(ie CD3+ and CD19+) lymphocyte subsets we also mea-sured thyroid function urinalysis and complete blood countsat baseline and monthly thereafter This was performed inaccordance with the Risk Evaluation andMitigation Strategies
program for alemtuzumab to identify evidence of autoim-mune thyroiditis anti-GBM antibody disease or immunethrombocytopenic purpura
The second cohort of 5 patients (demographics are shown intable 2) whichwas originally treatedwith alemtuzumab receivedat least 1 infusion of low-dose rituximab after B-cell re-constitution to 40ndash50 of baseline Follow-up of these indi-viduals occurred for less than 24 months Lymphocyte subsetsthyroid function urinalysis and complete blood counts weremeasured at baseline andmonthly thereafter as described above
Given the low number of patients in this retrospective caseseries and variations in protocol we did not have adequatepower to perform statistical tests to determine the efficacy ofanti-CD20 therapy in preventing alemtuzumab-mediatedsecondary autoimmunity
Data availabilityDeidentified data will be shared with other investigators fol-lowing requests made to the corresponding author
ResultsOf the 5 patients with follow-up greater than 24 months(table 1) who received low-dose rituximab infusions followingalemtuzumab 1 patient received 2 rituximab infusions and 1patient received greater than 3 rituximab infusions due toprolonged T-cell suppression Two of the patients receivedrituximab after a single cycle of alemtuzumab and 3 of thepatients received rituximab after 2 cycles of alemtuzumabNone of the patients received 3 cycles of alemtuzumab givenevidence of clinical remission and radiographic stabilizationas confirmed on follow-up MRI investigations
Table 1 Clinical characteristics and results of patientswith long-term follow-up
Characteristic Value
No of patients 5
Age mean (SD) y 47 (11)
Sex female 60
Cycles of alemtuzumab
1a 20
2 80
Follow-up mean (SD) mo 41 (5)
Rituximab doses individuals
1 3
2 1
3+ 1
Rituximab timing individuals
1st cycle 2
2nd cycle 3
Both 0
Secondary autoimmune disease 0
Shown are clinical characteristics of patients who received low-dose ritux-imab with follow-up duration greater than 24 months characterized by agesex cycles of alemtuzumab follow-up duration doses of rituximab timingof doses and development of secondary autoimmune diseasea One patient received only a single cycle of alemtuzumab at the patientrsquosrequest due to disease stability
Table 2 Clinical characteristics and results of patientswith short-term follow-up
Characteristic Value
No of patients 5
Age mean (SD) y 44 (13)
Sex female 80
Follow-up mean (SD) mo 14 (2)
Rituximab doses individuals
1 2
2 3
Median time to CD19 50 baseline mo 2
Median time to first rituximab dose mo 3
Shown are clinical characteristics of patients who received low-dose ritux-imabwith follow-up duration less than 24months characterized by age sexfollow-up duration doses of rituximab time to rise in CD19 count and timeto first rituximab dose
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 3
For all 5 patients the mean follow-up duration from the initialdose of alemtuzumab was 41 months (range 34ndash48 months)None of the patients developed secondary autoimmunecomplications as defined by the Comparison of Alemtuzumaband Rebif Efficacy in Multiple Sclerosis (CARE-MS) I and IItrials34 Based on the results of CARE-MS I we anticipatedthat 30ndash40 of patients with long-term follow-up wouldhave developed autoimmune thyroid disease34
Of the 5 additional patients with a follow-up duration of less than24 months (table 2) who received low-dose rituximab treatmentfollowing alemtuzumab 2 patients received 1 infusion of ritux-imab and 3 patients received 2 infusions of rituximab Themedian time to 40ndash50 recovery of the CD19+ cell count was2 months post-alemtuzumab and the median time to the firstrituximab dose administration was 3 months post-alemtuzumab
In this second cohort 1 patient developed transient neu-tropenia with an absolute neutrophil count (ANC) lt500μL2 months after the second dose of 100 mg of rituximab Thispatient was treated with granulocyte colony-stimulating factorand reconstituted the ANC within 1 month Another patientdeveloped a urinary tract infection and an additional patientdeveloped an upper respiratory tract infection after receivinglow-dose rituximab while both B- and T-cell lymphocyteswere suppressed
Late-onset neutropenia is a well-described phenomenon afterrituximab infusion which has been considered to be relatedto transient autoimmunity25 Alternately neutropenia hasalso been documented in postmarketing surveillance ofalemtuzumab-treated patients albeit at a much lower in-cident rate when compared with the frequency of the mostcommon alemtuzumab-induced secondary autoimmuneconditions particularly thyroiditis (eg Graves disease andHashimoto thyroiditis)34
All patients treated in both patient cohorts were on pro-phylactic valacyclovir or acyclovir for 24 consecutive monthsincluding during treatment with low-dose rituximab givenhigh rates of herpes reactivation in the clinical trials
DiscussionAlemtuzumab treatment in MS is associated with an earlyhyperrepopulation of B cells that emerge between 3 and 6months following treatment which precedes the repopulationof T cells that occurs between 12 and 24 months followingtreatment A fundamental discordance in the return of humoraland cellular networks is likely to play a role at least in part in theincidence of the adverse event most strikingly associated withalemtuzumab treatment secondary autoimmunity26ndash29
T-cell help is required for B-cell differentiation isotypeswitching and antibody secretion The interaction betweenB cells and T cells is bidirectional As such anti-CD20 B-cell
depletion in MS and experimental autoimmune encephalitis(EAE) promotes T-cell immune modulation characterizedby a significant reduction in proinflammatory Th1 and Th17cells which likely reflects a decrease in B-cell antigen-presenting cell function26 In this context selective de-ficiency of major histocompatibility complex (MHC) ClassII expression by B cells in mice eliminates both susceptibilityto EAE and the expansion of Th1 and Th17 cells29
In the absence of T-cell help B cells are rendered unable todifferentiate between the antigen presentation of self- vsnonndashself-epitopes at least in part secondary to a considerablylower threshold for presentation of low-magnitude antigenswhen compared with macrophages or dendritic cells Fur-thermore anti-CD20 treatment of MS and EAE promotesT-cell immune modulation characterized by a significant re-duction in the proinflammatory network at least in partmediated by Th1726ndash29 Conspicuously B cellndashspecific MHCClass IIndashdeficient mice are rendered resistant to the de-velopment of EAE28
Secondary humoral autoimmunity resulting in hyper- or hy-pothyroidism thrombocytopenia or renal disease are wellknown risks following alemtuzumab treatment of MS56 Wehypothesize that anti-CD20 B-cell depletion after alemtuzu-mab administration may mitigate the risk of secondary auto-immunity and have investigated this possibility Our initialresults suggest that anti-CD20 B-cell depletion is safe andpotentially efficacious However given the small sample sizeand unrandomized and unblinded cohort more rigorousstudies need to be pursued before making any declarationregarding efficacy
Several hypotheses attempt to delineate the cause of sec-ondary autoimmune disease associated with alemtuzumabMSdisease-modifying therapy Unlike traditional B-cell returnafter anti-CD20 therapies B-cell repopulation occurs rapidlyfollowing alemtuzumab treatment and is associated withhyperrepopulation of immature and mature B cells abovebaseline levels30 Following alemtuzumab treatment B-cellrepopulation occurs well in advance of T-cell repopulation(3ndash6 months compared with 12ndash24 months re-spectively) which may compromise the counterbalancing ofhumoral and cellular mechanisms that serve to maintain im-mune regulation
Notwithstanding these findings secondary autoimmune dis-ease after alemtuzumab treatment exhibits a long latencybefore presentation that is well beyond the observed B-cellhyperrepopulation and in fact coincides more closely withT-cell repopulation as autoantibody production is likely CD4T-cell dependent31
T-cell regeneration after depletion in adults is predominantlyachieved by thymic-independent homeostatic peripheral ex-pansion This process unlike T-cell regeneration in childrenwhich occurs primarily in the thymus is associated with
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
decreased self-tolerance a potential molecular scaffolding onwhich autoimmunity can result31
The goal of the temporally associated administration of low-doserituximab is not exclusively restricted to delaying the return ofthe CD19+ B-cell population or an attempt to solely synchronizethe reconstitution of B- and T-cell subsets Data from clinicaltrials that have analyzed the kinetics of humoral and cellularsubsets reveal no evidence of correlation that dichotomizes therisk predilection for alemtuzumab-mediated secondary autoim-munity16 Future work should also characterize the effect ofrituximab on a unique and proinflammatory mononuclear cellwhich coexpresses both CD20 andCD3 (ie CD20+ T cells andchimeric or C cells) which may serve to promote secondaryautoimmunity and would be expected to be deleted along withCD20+ B cells during our administration of low-dose rituximab
A uniquemember of the immune systemrsquosmononuclear cell poolis the CD20+ T cell (ie a chimeric lymphocyte or C cell figure1) which includes both CD4+ and CD8+ cells with the latterbeing the predominant of this cell type Its T-cell origin has beenconfirmed via the detection of CD3 encoded mRNA via reversetranscriptase-polymerase chain reaction (RT-PCR)3233 Thedistribution of these cells is broad and includes the primary andsecondary lymphoid tissue thymus bone marrow lymph nodeadenoids liver and cerebrospinal fluid (CSF) Conspicuously atresting conditions CD20+ T cells exhibit augmented release ofcytokines vs CD20minusT cells Specifically they release interferon γinterleukin (IL) 1 β IL-2 IL-4 IL-8 IL-10 transforming growthfactor β tumor necrosis factor α and c-c chemokine34
Under conditions of immune stimulation there is an escala-tion in cytokine production in CD20+ T cells32 Furthermoreenhanced expression of IL-17 is also characteristic of thissmall population of lymphocytes33 In patients with relapsing-remitting and primary progressive MS vs healthy controlsthere is an increased frequency of CD20+T cells in peripheralblood35
In those with MS there is an increased clonal frequency ofsuch cells in CSF when compared with the analysis of pe-ripheral blood mononuclear cells and the magnitude of thatclonal frequency is correlated with clinical disability in pa-tients with MS as measured by the long-validated ExpandedDisability Status Scale score36 Also CD20+ T cells areidentified within chronic white matter plaque lesions derivedfrom the MS brain36 In drastic contrast to the small pro-portion of such cells from the peripheral blood of controls theCD20+ T-cell fraction in patients with MS represents astriking 184 of all CD20+ cells including those mono-nuclear cells that are CD19+ B cells37
B-cell hyperrepopulation accompanied by a reduction ofT-cell help establishes circumstances whereby antigen pre-sentation coordinated by B cells renders them unable todifferentiate between self (whereby antigen presentation ofautoantigens stereotypically produces immune anergy) and
foreign epitopes (which appropriately culminates in immuneactivation) Alternately the B-cell depletion also comes withthe downregulation of inflammatory cytokines secondary toB-cell induction of T-cell activity and the eventual cytokinerelease syndrome
A detailed figure (figure 1) delineates our hypothetical con-stellation of features proposed as the basis for a low-dose anti-CD20 whack-a-mole strategy aimed at mitigating secondaryautoimmunity
If our proposed risk mitigation strategy were to be used morebroadly for feasibility there would need to be a straightfor-ward way of timing rituximab infusions As such figure 2illustrates a schematic for a potential protocol using a low-dose anti-CD20 (rituximab) whack-a-mole secondary auto-immunity mitigation strategy post-alemtuzumab treatmentand its effect on B-cell repopulation Specifically we timedlow-dose rituximab infusion with a CD19+ B-cell recovery of50 of normal baseline We chose this as a relatively easymarker to measure and to ensure that patients would receiverituximab synchronous to the B-cell hyperrepopulation phaseof postndashalemtuzumab-induced bone marrow mononuclearcell mobilization
Alternatively rituximab could be given at a fixed interval suchas 3 or 4 months after alemtuzumab infusion a commonalbeit not consistent duration for the bone marrow mobili-zation and peripheral repopulation of B cells However ifB-cell hyperrepopulation is delayed (eg until 4ndash6 months) afixed timing for whack-a-mole administration of low-doseanti-CD20 therapy could predispose a significant proportionof patients to harbor a temporal discordance between suchtreatment and its intended targets consequently producing anineffective depletion of both CD20+ B cells and CD20+CD3+ T cells (likely resulting in a potential type II error inefficacy analyses)
Given the heterogeneity in the kinetics of B-cell repopu-lation following alemtuzumab therapy coupled with theknown median half-life of rituximab at 22 days (with a rangeof 61ndash52 days as per package insert) we strongly advise formonthly lymphocyte subset analysis to precisely synchro-nize administration of a rituximab low-dose anti-CD20whack-a-mole therapy strategy to buffer against the dis-cordant B-cell hyperrepopulation in the absence of ade-quate T-cell help In addition this strategy will attenuatethe reemergence of the proinflammatory CD20+ T cellsIt remains to be seen if a single dose of rituximab willbe sufficient or whether multiple whack-a-mole cycleswill be required for a therapeutic effect of preventingalemtuzumab-associated secondary autoimmunity
It is of interest that anti-CD20 therapy achieves about a 99loss of peripheral blood B lymphocytes without affectingplasma cells or plasmablasts the principal antibody-secretingcells which are devoid of cell surface CD20 expression In
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 5
Figure 1 A model for the mitigation of secondary autoimmunity in patients with MS post-alemtuzumab
In the upper portion of the figure we illustrate alemtuzumab treatment and its effect on elimination of antindashself-lymphocytes by 2 principal mechanismsclearance through the reticular endothelial system (RES on the left) and assembly of themembrane attack complex (MAC) facilitating the passage of C9 whichcompromises cell membrane integrity thereby culminating in cytotoxicity and cell death The lower middle illustration emphasizes post-alemtuzumabtreatment-inducedmobilization of bonemarrow stem cells reconstituting the immune system B cells undergo a discordant hyperrepopulation approachingpretreatment baseline numbers 3ndash6 months following alemtuzumab treatment whereas T-cell reconstitution is considerably delayed (12ndash24 months)Hypothetically the highly discordant hyperrepopulation of B cells plays a role in the development of secondary autoimmunity Post-alemtuzumab treatmentcirculatingmononuclear cells are principally CD3+-naive T cells CD19+ CD20+-naive B cells as well as a unique population of cells that express both the B-cellantigen CD20 and the T-cell antigen CD3 These latter cells we refer to as Chimeric lymphocytes (C cells) and they are known to express proinflammatorycytokines which in the absence of adequate T-cell help can foment the production of antindashself-antibodies This can initiate corresponding autoantibody-mediated disorders such as those designated by green labels in the figure as well as to T cells capable of orchestrating cellularmechanisms of autoimmunity(designated by purple labels) To the lower left of the lower diagram one can see an enrichment in the CD3+ CD20+ C cells simultaneouswith the discordant B-cell hyperrepopulation (generally emerging approximately 3ndash6 months following alemtuzumab treatment) in the context of a deficiency in the clonalfrequency of regulatory T cells (Tregs) (ie identified as CD4+CD25hiFoxP3+) In the absence of T-cell help such B cells are rendered incapable of discriminatingbetween self and foreign epitopes to both other B cells thereby coordinating the development of antibodies as well as to T cells leading to T-cell receptormaturation with elaboration of cytokine and chemokine expression profiles commensurate to foment cellular autoimmunemechanisms The central portionof the diagram serves to illustrate the potential diversity of antibody-mediated secondary autoimmune states (green line paths) We also see activation ofT cells which can mediate secondary autoimmunity (purple line paths) and granulomatous inflammatory disease most specifically sarcoidosis Monitoringmonthly lymphocyte subsets facilitates detection of the discordant B-cell hyperrepopulation phase of bone marrow mononuclear cell mobilization afteralemtuzumab therapy and thereby provides for the discrete and temporally punctuated administration of an anti-CD20 ldquowhack-a-molerdquo strategy formitigating secondary autoimmunity Specifically we administered low-dose rituximab to orchestrate the deletionof bothCD20+B cells in conjunctionwith theCD20+CD3+ C cells along with their B-cell activation capabilities via the elaboration of proinflammatory cytokine and chemokine cascades The net effect isseen approximately 4months later (in the upper circle on the right lower side of the diagram) when there is amarked diminution of both effectormemory Bcells and autoimmunity-inducing C cells with a corresponding expansion in the clonal frequency of Tregs
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
keeping with this observation anti-CD20 therapy appears toexert no impact on CSF antibody indices such as oligoclonalbanding increased immuno gamma globulin (IgG) indexandor an elevation in IgG synthesis rates characteristic ab-normalities identified in approximately 90 of patients withMS when using isoelectric focusing techniques Alternatelythe peripheral loss of B cells does correspond to a markedreduction in the development of both T1 gadolinium-enhancing and combined unique MS plaque lesions3839
In a recent study the third-generation glycoengineered chi-meric anti-CD20 therapy ublituximab was shown to reduceboth effector and memory CD8 T-cell populations while alsoaugmenting the clonal frequency of naive CD8+ T cells38 Oneof the most conspicuous observations was the identification ofa population of lymphocytes with cell surface expression ofboth CD20+ and CD3+ (those designated as chimeric or Ccells in our hypothetical model figure 1) with further char-acterization revealing that such cells exhibit features inkeeping with memory CD8+ T cells40
The functionally chimeric lymphocytes produce proin-flammatory mediators which may play a key role in thepromiscuous antigen presentation of self-motifs during thediscordant hyperrepopulation of B cells following alemtuzu-mab treatment (figure 1) Lovett-Racke et al categoricallycharacterized both the cellular identification and cytokinechemokine expression profiles using flow cytometric tech-niques from 47 patients withMS treated with ublituximab and
confirmed that such treatment resulted in significantly at-tenuated expression of proinflammatory cytokines reducedantigen presentation a shift from the effectormemory phe-notype to repopulation of naive lymphocytes and importantlyaugmentation in the clonal frequency of regulatory T cells(Tregs)33
A primary immune defect in patients with MS is a deficiencyin Tregs Efficacy in treating the disorder at least in partinvolves reconstitution of the immune networkrsquos regulatorycapabilities through the expansion of Tregs specificallyidentified as CD4+CD25hiFoxP3+2838 The observationsfrom this investigation suggest that anti-CD20 therapy is ca-pable of provoking a skewing or immune deviation that maybe secondary perhaps at least in part to the deletion ofCD20+CD3+ C cells thereby resulting in reduced B cellndashmediated degenerate antigen presentation of self-motifsalong with a broadening in the clonal frequency of Tregs all ofwhich may be germane to our understanding of how we canuse alemtuzumab while actively reducing (vis a vis with theapplication of a lsquowhack-a-molersquo cell depletion strategy) theincidence of secondary autoimmunity (figures 1 and 2)33
We successfully used low-dose rituximab 100 mg (50ndash75mgm2) for patients with neuromyelitis optica spectrumdisorder (NMOSD) who could not afford access to higherdoses of rituximab A 100-mg infusion depletes the CD19population of B cells to less than 2 for an average of 99 days(in essence B-cell suppression is highly titratable analogous
Figure 2 Low-dose anti-CD20 therapy post-alemtuzumab schematic illustrating a potential pilot protocol
This schematic depicts normal CD4+ and CD19+ cell reconstitution9 as well as the theoretical CD19+ reconstitution with our proposed low-dose rituximabprotocol Low-dose rituximab (eg 100 mg) is given subsequent to the detection of the precociously discordant B-cell hyperrepopulation phase of bonemarrow mononuclear cell mobilization following alemtuzumab treatment an intervention which attenuates promiscuous antigen presentation by B cellscapable of activating antindashself-humoral and cellular networks while also serving to promote a more synchronized repopulation across the bone marrowmobilization of mononuclear cell heterogeneity (ie achieving a more balanced return of B and T lymphocyte populations with the added dividend ofamplifying the clonal frequency of Tregs and observation akin to tolerance induction in patients with MS)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 7
to immunologic labetalol the latter commonly used as ahighly titratable agent for management of hypertensive crisessuch as hypertensive encephalopathy where loss of cerebro-vascular autoregulation precludes the employment of long-acting agents which could result in a protracted compromisein cerebral blood flow dynamics predisposing to a hypoxic-ischemic insult) in patients with NMOSD compared with 184days for a 1000 mg dose of rituximab41
Low-dose rituximab is a more attractive alternative to stan-dard doses of 1000 mg or 375 mgm2 First doses of ritux-imab as low as 1 mgm2 suppress B cells by 97 in healthycontrols and B cells remain suppressed to 75 of baselinelevels at 12 weeks after infusion4243
Second low-dose anti-CD20 therapy does not result in pro-longed B-cell depletion so as not to interfere with repeatcycles of alemtuzumab therapy41
Third low-dose rituximab may facilitate greater control ofB-cell repopulation and improved temporal synchronizationwith T-cell repopulation
Last reduced dosing magnitude reduces the duration of im-munosuppression compared with conventional doses of rit-uximab and may eventually be shown in evidence-basedstudies to demonstrate both safety and cost advantages if fewcomplications are identified with the low-dose regimen
A more robust clinical trial with a primary outcome of thedevelopment of secondary autoimmunity would not likelyrequire a large number of participants given the incidence rateof 40 of autoimmune thyroid disease in patients with MSwho have received alemtuzumab34 Hence we would esti-mate an incidence of 40 in the control group ofalemtuzumab-only treated patients and with an assumption ofan incidence of 10 in patients who would receive adjunctrituximab If we assign the probability of a type I error of 5and a power of 80 a trial would need approximately 80patients total (40 in each arm) accounting for drop-outs
In addition to our small sample size and an unrandomizedand unblended cohort many physicians prescribe steroidswith rituximab infusion (methylprednisolone 250 mg beforeeach and every alemtuzumab infusion in our center) to pre-vent infusion reactions It is possible that the potential positiveeffects of secondary autoimmunity prevention attributed torituximab are instead or at least in part due to steroid usageIn addition treatment may simply delay secondary autoim-munity rather than preventing it and longer periods of as-certainment will be required to assess for this prospect
An alternate explanation concerning the impact of rituximabon secondary autoimmunity is that some individuals mayrespond differently to low-dose anti-CD20 therapy due to theeffects of the FCGR3A polymorphism42 We do not know theeffect of the polymorphism on low-dose rituximab kinetics
however binding affinity may play a larger role in low-doserituximab compared with conventional doses given the lowerabsolute concentration of rituximab Such issues should becarefully considered in the design of a larger trial particularlygiven potential effects of such factors on response character-istics as well as on study cost
As the field of neurology shifts from amodel of step escalationto induction therapy for the treatment of MS strategies thatare aimed at mitigating the risks of potent disease modifyingtherapies are urgently needed43
Only through the scientific method of subjecting our hy-pothesis to the rigors of a controlled adequately blindedprospective and adequately powered clinical trial can weconfirm or refute the hypothesis-driven question can theapplication of low-dose anti-CD20 therapy temporally syn-chronized with objective confirmation of B-cell hyper-repopulation serve to adequately reduce or even preventalemtuzumab-associated secondary autoimmunity
Furthermore the addition of anti-CD20 therapy could po-tentially confer benefits on immune deviation that would exertadded efficacy in synergy with the alemtuzumab-mediatedmechanisms of action in the establishment of disease re-mission while constituting augmented and durable regulatoryproperties in keeping with those achieved during the criticalperiod that we now recognize collectively as self-tolerance
Buffeted by the broad dissemination of bone marrow mobili-zation of stem cells following alemtuzumab treatment maypromote the process of restoration and neurologic functionalreconstitution Recent evidence has demonstrated that anemerging biomarker for assessing tissue damage in the CNS ofpatients withMS the neurofilament light chain is reducedmostmarkedly following the administration of alemtuzumab whencompared with other disease-modifying therapies and that suchlevels remain reduced to the greatest magnitude over time44
It was once thought that a proposition such as repair andfunctional recovery from MS was wholly enigmatic and un-likely However we have arrived at a point in the history of ourunderstanding of the disorderrsquos pathobiology in concert withthe corresponding derangements in immune regulatory in-fluences and how to remediate them We believe our work torepresent but a single small step toward this constellation ofgoals that are so important to our deserving patients theirfamilies our community and those of us who serve on thoseteams who care for and about them
AcknowledgmentThe authors thank Mr Jason Ooi and Dr Matthew Parsonsfor their transformation and production of Elliot andTeresa Frohmanrsquos formulation of the figure 1 medicalillustration which showcases alemtuzumabrsquos mechanism ofaction the pathobiological underpinnings for treatment-associated secondary autoimmunity and the hypothetical
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
mechanisms germane to our ldquowhack-a-molerdquo B-cell de-letion strategy aimed at mitigating alemtuzumab-associatedautoimmunity in MS
Study fundingThe National Multiple Sclerosis Society 5-Year InstitutionalFellowship Training Grant Awarded to TC Frohman andEM Frohman Fellows funded E Meltzer and RA Cruz(coauthors) MS and Neuroimmunology Center The DellMedical School at The University of Texas at Austin
DisclosureE Meltzer served as a consultant for Genzyme and receivedhonoraria from Novartis S Campbell and B Ehrenfeld havenothing to disclose L Steinman is on the Editorial Boards ofthe Proceedings of the National Academy of Sciences and theJournal of Neuroimmunology He has served on the EditorialBoard of the Journal of Immunology and International Immu-nology He has served as a member of grant review committeesfor the NIH and the National MS Society He has served orserves as a consultant and received honoraria from AtaraBiotherapeutics Atreca Biogen-Idec Celgene CentocorCoherus EMD-Serono Genzyme Johnson and JohnsonNovartis RocheGenentech Teva Pharmaceuticals Incand TG Therapeutics He has served on the Data SafetyMonitoring Board for TG Therapeutics He serves on theBoard of Directors of Tolerion and Chairs the ScientificAdvisory Board for Atreca Currently L Steinman receivesresearch grant support from the NIH and Atara Bio-therapeutics MS Parsons has nothing to disclose SSZamvil is Deputy Editor ofNeurology Neuroimmunology andNeuroinflammation and is an Associate Editor for Frontiers inImmunology and Frontiers in Neurology He serves on theAdvisory Committee for the American Congress onTreatment and Research in Multiple Sclerosis (ACTRIMS)and is a standing member of the research grant reviewcommittee for the National Multiple Sclerosis Society(NMSS) He has served on the Editorial Board of theJournal of Clinical Investigation The Journal of Immunologyand The Journal of Neurological Sciences and has been acharter member of the grant review committee for the NIHClinical Neuroimmunology and Brain Tumors (CNBT)He has served or serves as a consultant and receivedhonoraria from Alexion Biogen-Idec EMD-SeronoGenzyme Novartis RocheGenentech and Teva Pharma-ceuticals Inc and has served on Data Safety MonitoringBoards for Lilly BioMS Teva and Opexa TherapeuticsCurrently SS Zamvil receives research grant support fromthe NIH NMSS Weill Institute Race to Erase MS and theMaisin Foundation TC Frohman has received advisoryboard fees from Alexion EM Frohman has receivedspeaker honoraria from Genzyme Novartis Alexion andAcorda Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationDecember 25 2019 Accepted in final form July 6 2020
References1 Coles AJ Twyman CL Arnold DL et al Alemtuzumab for patients with relapsing
multiple sclerosis after disease-modifying therapy a randomised controlled phase 3trial Lancet 20123801829ndash1839
2 Cohen JA Coles AJ Arnold DL et al Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis a randomisedcontrolled phase 3 trial Lancet 20123801819ndash1828
3 Coles AJ Cohen JA Fox EJ et al Alemtuzumab CARE-MS II 5-year follow-upNeurology 2017891117ndash1126
4 Havrdova E Arnold DL Cohen JA et al Alemtuzumab CARE-MS I 5-year follow-upNeurology 2017891107ndash1116
5 Sarvepalli D Rashid MU Ullah W Zafar Y Khan M Idiopathic thrombocytopenicpurpura a rare syndrome with alemtuzumab review of monitoring protocol Cureus201911e5715
6 Ruck T Schulte-Mecklenbeck A Pfeuffer S et al Pretreatment anti-thyroid auto-antibodies indicate increased risk for thyroid autoimmunity secondary to alemtuzu-mab a prospective cohort study EBioMedicine 201946381ndash386
Appendix Authors
Name Location Contribution
Ethan MeltzerMD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
SarahCampbell RN
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
BenjaminEhrenfeldMSW
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
Roberto ACruz MD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
LawrenceSteinman MD
Department ofNeurology StanfordUniversity School ofMedicine
Conception and criticalrevision of themanuscript forintellectual content
Matthew SParsons PhD
Division of Microbiologyand Immunology YerkesNational PrimateResearch CenterDepartment of Pathologyand Laboratory MedicineEmory University
Conception and criticalrevision of themanuscript forintellectual content
Scott S ZamvilMD PhD
Department ofNeurology amp Program inImmunology Universityof California SanFrancisco
Conception and criticalrevision of themanuscript forintellectual content
Elliot MFrohman MDPhD
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical SchoolUniversity of Texas atAustin
Conception and criticalrevision of themanuscript forintellectual content
Teresa CFrohmanMPAS MSCSPA-C FANA
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical School Universityof Texas at Austin
Conception and criticalrevision of themanuscript forintellectual content
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 9
7 Ruck T Pfeuffer S Schulte-Mecklenbeck A et al Vitiligo after alemtuzumab treat-ment secondary autoimmunity is not all about B cells Neurology 201891e2233ndashe2237
8 Zimmermann J Buhl T Muller M Alopecia universalis following alemtuzumabtreatment in multiple sclerosis a barely recognized manifestation of secondaryautoimmunity-report of a case and review of the literature Front Neurol 20178569
9 Rotondi M Molteni M Leporati P Capelli V Marino M Chiovato L Autoimmunethyroid diseases in patients treated with alemtuzumab for multiple sclerosis an ex-ample of selective anti-TSH-receptor immune response Front Endocrinol (Lau-sanne) 20178254
10 Costelloe L Jones J Coles A Secondary autoimmune diseases following alemtuzu-mab therapy for multiple sclerosis Expert Rev Neurother 201212335ndash341
11 Jones JL Phuah CL Cox AL et al IL-21 drives secondary autoimmunity in patientswith multiple sclerosis following therapeutic lymphocyte depletion with alemtuzu-mab (Campath-1H) J Clin Invest 20091192052ndash2061
12 Torino F Barnabei A Paragliola R Baldelli R Appetecchia M Corsello SM Thyroiddysfunction as an unintended side effect of anticancer drugs Thyroid 2013231345ndash1366
13 Azzopardi L Thompson SA Harding KE et al Predicting autoimmunity afteralemtuzumab treatment of multiple sclerosis J Neurol Neurosurg Psychiatry 201485795ndash798
14 Trinh T Haridas AS Sullivan TJ Ocular findings in alemtuzumab (Campath-1H)-induced thyroid eye disease Ophthalmic Plast Reconstr Surg 201632e128ndashe129
15 von Kutzleben S Pryce G Giovannoni G Baker D Depletion of CD52-positivecells inhibits the development of central nervous system autoimmune disease butdeletes an immune-tolerance promoting CD8 T-cell population Implications forsecondary autoimmunity of alemtuzumab in multiple sclerosis Immunology 2017150444ndash455
16 Wiendl H Carraro M Comi G et al Lymphocyte pharmacodynamics are not asso-ciated with autoimmunity or efficacy after alemtuzumab Neurol NeuroimmunolNeuroinflamm 201971ndash10 doi101212NXI0000000000000635
17 Kousin-Ezewu O Azzopardi L Parker RA et al Accelerated lymphocyte recoveryafter alemtuzumab does not predict multiple sclerosis activity Neurology 2014822158ndash2164
18 Jones J Thompson S Loh P et al Human autoimmunity after lymphocyte depletionis caused by homeostatic T-cell proliferation Proc Natl Acad Sci U S A 201311020200ndash20205
19 Costa DB Kobayashi SS Whacking a mole-cule clinical activity and mechanisms ofresistance to third generation EGFR inhibitors in EGFR mutated lung cancers withEGFR-T790M Transl Lung Cancer Res 20156809ndash815
20 Shin J MacCarthy T Antagonistic coevolution drives whack-a-mole sensitivity ingene regulatory networks PLoS Comput Biol 201511e1004432
21 Suzuki K Whack-a-mole strategy for multifocal ground glass opacities of the lungJ Thorac Dis 20179(suppl 3)S201ndashS207
22 Swanson DS Harrison CJ Playing Whack-a-Mole with pneumococcal serotypeeradication Pediatrics 2017140e20172034
23 Mestrovic T A microbial game of whack-a-mole clinical case series of the urethraluncloaking phenomenon caused by Corynebacterium glucuronolyticum in mentreated for Chlamydia trachomatis urethritis Infection 201947121ndash124
24 Gelfand JM Cree BAC Hauser SL Ocrelizumab and other CD20+ B-cell-depletingtherapies in multiple sclerosis Neurotherapeutics 201714835ndash841
25 Voog E Morschhauser F Solal-Celigny P Neutropenia in patients treated with rit-uximab N Engl J Med 20033482691ndash2694 discussion 2691ndash2694
26 Bar-Or A Fawaz L Fan B et al Abnormal B-cell cytokine responses a trigger of T-cell-mediated disease in MS Ann Neurol 201067452ndash461
27 Weber MS Prodrsquohomme T Patarroyo JC et al B-cell activation influences T-cellpolarization and outcome of anti-CD20 B-cell depletion in central nervous systemautoimmunity Ann Neurol 201068369ndash383
28 Monson NL Cravens P Hussain R et al Rituximab therapy reduces organ-specificT cell responses and ameliorates experimental autoimmune encephalomyelitis PLoSOne 20116e17103
29 Molnarfi N Schulze-Topphoff U Weber MS et al MHC class II-dependent B cellAPC function is required for induction of CNS autoimmunity independent of myelin-specific antibodies J Exp Med 20132102921ndash2937
30 Baker D Herrod SS Alvarez-Gonzalez C Giovannoni G Schmierer KInterpreting lymphocyte reconstitution data from the pivotal phase 3 trials of alem-tuzumab JAMA Neurol 201774961ndash969
31 Krupica T Fry TJ Mackall CL Autoimmunity during lymphopenia a two-hit modelClin Immunol 2006120121ndash128
32 Wilk EWitte TMarquardt N et al Depletion of functionally active CD20+ T cells byrituximab treatment Arthritis Rheum 2009603563ndash3571
33 Schuh E Berer K Mulazzani M et al Features of human CD3+CD20+ T cellsJ Immunol 20161971111ndash1117
34 Gingele S Kripuletz T Jacobs R Role of CD20+ T cells in multiple sclerosisimpli-cations for treatment with ocrelizumab Neural Regen Res 202015663ndash664
35 Palanichamy A Jahn S Nickles D et al Rituximab efficiently depletes increasedCD20-expressing T cells in multiple sclerosis patients J Immunol 2014193580ndash586
36 Holley JE Bremer E Kendall AC et al CD20+ inflammatory T-cells are present inblood and brain of multiple sclerosis patients and can be selectively targeted forapoptotic elimination Mult Scler Relat Disord 20143650ndash685
37 von Essen MR Ammitzboslashll C Hansen RH et al Proinflammatory CD20+ T cells inthe pathogenesis of multiple sclerosis Brain 2019142120ndash132
38 Lovett-Racke AE Gormley M Liu Y et al B cell depletion with ublituximab reshapesthe T cell profile in multiple sclerosis patients J Neuroimmunol 2019332187ndash197
39 Cross AH Stark JL Lauber J Ramsbottom MJ Lyons JA Rituximab reduces B cells andT cells in cerebrospinal fluid ofmultiple sclerosis patients J Neuroimmunol 200618063ndash70
40 Naismith RT Piccio L Lyons JA et al Rituximab add-on therapy for breakthroughrelapsing multiple sclerosis a 52-week phase II trial Neurology 2010741860ndash1867
41 Greenberg BM Graves D Remington G et al Rituximab dosing and monitoringstrategies in neuromyelitis optica patients creating strategies for therapeutic successMult Scler 2012181022ndash1026
42 Kim SH Jeong IH Hyun JW et al Treatment outcomes with rituximab in 100patients with neuromyelitis optica influence of FCGR3A polymorphisms on thetherapeutic response to rituximab JAMA Neurol 201572989ndash995
43 Steinman L Induction of new autoimmune diseases after alemtuzumab therapy formultiple sclerosis learning from adversity JAMA Neurol 201774907ndash908
44 Delcoigne B Manouchehrinia A Barro C et al Blood neurofilament light levelssegregate treatment effects in multiple sclerosis Neurology 202094e1201ndashe1212
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
DOI 101212NXI000000000000086820207 Neurol Neuroimmunol Neuroinflamm
Ethan Meltzer Sarah Campbell Benjamin Ehrenfeld et al depletion strategy
Mitigating alemtuzumab-associated autoimmunity in MS A whack-a-mole B-cell
This information is current as of August 7 2020
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

occurred for more than 24 months All patients who receivedalemtuzumab for treatment of MS were eligible Patients werenot selected on the basis of prior immunotherapy Rituximabis an anti-CD20 monoclonal antibody therapeutic In additionto CD20 CD19 is also a pan B-cell marker Anti-CD20therapeutic monoclonal antibody interferes with the recog-nition of the CD20 antigen As such the CD19+ B-cell levelas measured by flow cytometry was used as a proxy to mea-sure extent of B-cell depletion following anti-CD20 therapy24
Alemtuzumab-treated patients were scheduled to receiverituximab when CD19+ B cells repopulated to 40ndash50 oftheir baseline levels Baseline B-cell frequency was de-termined before initiation of alemtuzumab treatments byperforming lymphocyte subset analysis on 3ndash4 weekly blooddraws Rituximab dosing was predicated on insurance cov-erage Some dosages were delayed due to difficultiesobtaining insurance approval
In addition to monthly monitoring of T- and B-cell(ie CD3+ and CD19+) lymphocyte subsets we also mea-sured thyroid function urinalysis and complete blood countsat baseline and monthly thereafter This was performed inaccordance with the Risk Evaluation andMitigation Strategies
program for alemtuzumab to identify evidence of autoim-mune thyroiditis anti-GBM antibody disease or immunethrombocytopenic purpura
The second cohort of 5 patients (demographics are shown intable 2) whichwas originally treatedwith alemtuzumab receivedat least 1 infusion of low-dose rituximab after B-cell re-constitution to 40ndash50 of baseline Follow-up of these indi-viduals occurred for less than 24 months Lymphocyte subsetsthyroid function urinalysis and complete blood counts weremeasured at baseline andmonthly thereafter as described above
Given the low number of patients in this retrospective caseseries and variations in protocol we did not have adequatepower to perform statistical tests to determine the efficacy ofanti-CD20 therapy in preventing alemtuzumab-mediatedsecondary autoimmunity
Data availabilityDeidentified data will be shared with other investigators fol-lowing requests made to the corresponding author
ResultsOf the 5 patients with follow-up greater than 24 months(table 1) who received low-dose rituximab infusions followingalemtuzumab 1 patient received 2 rituximab infusions and 1patient received greater than 3 rituximab infusions due toprolonged T-cell suppression Two of the patients receivedrituximab after a single cycle of alemtuzumab and 3 of thepatients received rituximab after 2 cycles of alemtuzumabNone of the patients received 3 cycles of alemtuzumab givenevidence of clinical remission and radiographic stabilizationas confirmed on follow-up MRI investigations
Table 1 Clinical characteristics and results of patientswith long-term follow-up
Characteristic Value
No of patients 5
Age mean (SD) y 47 (11)
Sex female 60
Cycles of alemtuzumab
1a 20
2 80
Follow-up mean (SD) mo 41 (5)
Rituximab doses individuals
1 3
2 1
3+ 1
Rituximab timing individuals
1st cycle 2
2nd cycle 3
Both 0
Secondary autoimmune disease 0
Shown are clinical characteristics of patients who received low-dose ritux-imab with follow-up duration greater than 24 months characterized by agesex cycles of alemtuzumab follow-up duration doses of rituximab timingof doses and development of secondary autoimmune diseasea One patient received only a single cycle of alemtuzumab at the patientrsquosrequest due to disease stability
Table 2 Clinical characteristics and results of patientswith short-term follow-up
Characteristic Value
No of patients 5
Age mean (SD) y 44 (13)
Sex female 80
Follow-up mean (SD) mo 14 (2)
Rituximab doses individuals
1 2
2 3
Median time to CD19 50 baseline mo 2
Median time to first rituximab dose mo 3
Shown are clinical characteristics of patients who received low-dose ritux-imabwith follow-up duration less than 24months characterized by age sexfollow-up duration doses of rituximab time to rise in CD19 count and timeto first rituximab dose
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 3
For all 5 patients the mean follow-up duration from the initialdose of alemtuzumab was 41 months (range 34ndash48 months)None of the patients developed secondary autoimmunecomplications as defined by the Comparison of Alemtuzumaband Rebif Efficacy in Multiple Sclerosis (CARE-MS) I and IItrials34 Based on the results of CARE-MS I we anticipatedthat 30ndash40 of patients with long-term follow-up wouldhave developed autoimmune thyroid disease34
Of the 5 additional patients with a follow-up duration of less than24 months (table 2) who received low-dose rituximab treatmentfollowing alemtuzumab 2 patients received 1 infusion of ritux-imab and 3 patients received 2 infusions of rituximab Themedian time to 40ndash50 recovery of the CD19+ cell count was2 months post-alemtuzumab and the median time to the firstrituximab dose administration was 3 months post-alemtuzumab
In this second cohort 1 patient developed transient neu-tropenia with an absolute neutrophil count (ANC) lt500μL2 months after the second dose of 100 mg of rituximab Thispatient was treated with granulocyte colony-stimulating factorand reconstituted the ANC within 1 month Another patientdeveloped a urinary tract infection and an additional patientdeveloped an upper respiratory tract infection after receivinglow-dose rituximab while both B- and T-cell lymphocyteswere suppressed
Late-onset neutropenia is a well-described phenomenon afterrituximab infusion which has been considered to be relatedto transient autoimmunity25 Alternately neutropenia hasalso been documented in postmarketing surveillance ofalemtuzumab-treated patients albeit at a much lower in-cident rate when compared with the frequency of the mostcommon alemtuzumab-induced secondary autoimmuneconditions particularly thyroiditis (eg Graves disease andHashimoto thyroiditis)34
All patients treated in both patient cohorts were on pro-phylactic valacyclovir or acyclovir for 24 consecutive monthsincluding during treatment with low-dose rituximab givenhigh rates of herpes reactivation in the clinical trials
DiscussionAlemtuzumab treatment in MS is associated with an earlyhyperrepopulation of B cells that emerge between 3 and 6months following treatment which precedes the repopulationof T cells that occurs between 12 and 24 months followingtreatment A fundamental discordance in the return of humoraland cellular networks is likely to play a role at least in part in theincidence of the adverse event most strikingly associated withalemtuzumab treatment secondary autoimmunity26ndash29
T-cell help is required for B-cell differentiation isotypeswitching and antibody secretion The interaction betweenB cells and T cells is bidirectional As such anti-CD20 B-cell
depletion in MS and experimental autoimmune encephalitis(EAE) promotes T-cell immune modulation characterizedby a significant reduction in proinflammatory Th1 and Th17cells which likely reflects a decrease in B-cell antigen-presenting cell function26 In this context selective de-ficiency of major histocompatibility complex (MHC) ClassII expression by B cells in mice eliminates both susceptibilityto EAE and the expansion of Th1 and Th17 cells29
In the absence of T-cell help B cells are rendered unable todifferentiate between the antigen presentation of self- vsnonndashself-epitopes at least in part secondary to a considerablylower threshold for presentation of low-magnitude antigenswhen compared with macrophages or dendritic cells Fur-thermore anti-CD20 treatment of MS and EAE promotesT-cell immune modulation characterized by a significant re-duction in the proinflammatory network at least in partmediated by Th1726ndash29 Conspicuously B cellndashspecific MHCClass IIndashdeficient mice are rendered resistant to the de-velopment of EAE28
Secondary humoral autoimmunity resulting in hyper- or hy-pothyroidism thrombocytopenia or renal disease are wellknown risks following alemtuzumab treatment of MS56 Wehypothesize that anti-CD20 B-cell depletion after alemtuzu-mab administration may mitigate the risk of secondary auto-immunity and have investigated this possibility Our initialresults suggest that anti-CD20 B-cell depletion is safe andpotentially efficacious However given the small sample sizeand unrandomized and unblinded cohort more rigorousstudies need to be pursued before making any declarationregarding efficacy
Several hypotheses attempt to delineate the cause of sec-ondary autoimmune disease associated with alemtuzumabMSdisease-modifying therapy Unlike traditional B-cell returnafter anti-CD20 therapies B-cell repopulation occurs rapidlyfollowing alemtuzumab treatment and is associated withhyperrepopulation of immature and mature B cells abovebaseline levels30 Following alemtuzumab treatment B-cellrepopulation occurs well in advance of T-cell repopulation(3ndash6 months compared with 12ndash24 months re-spectively) which may compromise the counterbalancing ofhumoral and cellular mechanisms that serve to maintain im-mune regulation
Notwithstanding these findings secondary autoimmune dis-ease after alemtuzumab treatment exhibits a long latencybefore presentation that is well beyond the observed B-cellhyperrepopulation and in fact coincides more closely withT-cell repopulation as autoantibody production is likely CD4T-cell dependent31
T-cell regeneration after depletion in adults is predominantlyachieved by thymic-independent homeostatic peripheral ex-pansion This process unlike T-cell regeneration in childrenwhich occurs primarily in the thymus is associated with
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
decreased self-tolerance a potential molecular scaffolding onwhich autoimmunity can result31
The goal of the temporally associated administration of low-doserituximab is not exclusively restricted to delaying the return ofthe CD19+ B-cell population or an attempt to solely synchronizethe reconstitution of B- and T-cell subsets Data from clinicaltrials that have analyzed the kinetics of humoral and cellularsubsets reveal no evidence of correlation that dichotomizes therisk predilection for alemtuzumab-mediated secondary autoim-munity16 Future work should also characterize the effect ofrituximab on a unique and proinflammatory mononuclear cellwhich coexpresses both CD20 andCD3 (ie CD20+ T cells andchimeric or C cells) which may serve to promote secondaryautoimmunity and would be expected to be deleted along withCD20+ B cells during our administration of low-dose rituximab
A uniquemember of the immune systemrsquosmononuclear cell poolis the CD20+ T cell (ie a chimeric lymphocyte or C cell figure1) which includes both CD4+ and CD8+ cells with the latterbeing the predominant of this cell type Its T-cell origin has beenconfirmed via the detection of CD3 encoded mRNA via reversetranscriptase-polymerase chain reaction (RT-PCR)3233 Thedistribution of these cells is broad and includes the primary andsecondary lymphoid tissue thymus bone marrow lymph nodeadenoids liver and cerebrospinal fluid (CSF) Conspicuously atresting conditions CD20+ T cells exhibit augmented release ofcytokines vs CD20minusT cells Specifically they release interferon γinterleukin (IL) 1 β IL-2 IL-4 IL-8 IL-10 transforming growthfactor β tumor necrosis factor α and c-c chemokine34
Under conditions of immune stimulation there is an escala-tion in cytokine production in CD20+ T cells32 Furthermoreenhanced expression of IL-17 is also characteristic of thissmall population of lymphocytes33 In patients with relapsing-remitting and primary progressive MS vs healthy controlsthere is an increased frequency of CD20+T cells in peripheralblood35
In those with MS there is an increased clonal frequency ofsuch cells in CSF when compared with the analysis of pe-ripheral blood mononuclear cells and the magnitude of thatclonal frequency is correlated with clinical disability in pa-tients with MS as measured by the long-validated ExpandedDisability Status Scale score36 Also CD20+ T cells areidentified within chronic white matter plaque lesions derivedfrom the MS brain36 In drastic contrast to the small pro-portion of such cells from the peripheral blood of controls theCD20+ T-cell fraction in patients with MS represents astriking 184 of all CD20+ cells including those mono-nuclear cells that are CD19+ B cells37
B-cell hyperrepopulation accompanied by a reduction ofT-cell help establishes circumstances whereby antigen pre-sentation coordinated by B cells renders them unable todifferentiate between self (whereby antigen presentation ofautoantigens stereotypically produces immune anergy) and
foreign epitopes (which appropriately culminates in immuneactivation) Alternately the B-cell depletion also comes withthe downregulation of inflammatory cytokines secondary toB-cell induction of T-cell activity and the eventual cytokinerelease syndrome
A detailed figure (figure 1) delineates our hypothetical con-stellation of features proposed as the basis for a low-dose anti-CD20 whack-a-mole strategy aimed at mitigating secondaryautoimmunity
If our proposed risk mitigation strategy were to be used morebroadly for feasibility there would need to be a straightfor-ward way of timing rituximab infusions As such figure 2illustrates a schematic for a potential protocol using a low-dose anti-CD20 (rituximab) whack-a-mole secondary auto-immunity mitigation strategy post-alemtuzumab treatmentand its effect on B-cell repopulation Specifically we timedlow-dose rituximab infusion with a CD19+ B-cell recovery of50 of normal baseline We chose this as a relatively easymarker to measure and to ensure that patients would receiverituximab synchronous to the B-cell hyperrepopulation phaseof postndashalemtuzumab-induced bone marrow mononuclearcell mobilization
Alternatively rituximab could be given at a fixed interval suchas 3 or 4 months after alemtuzumab infusion a commonalbeit not consistent duration for the bone marrow mobili-zation and peripheral repopulation of B cells However ifB-cell hyperrepopulation is delayed (eg until 4ndash6 months) afixed timing for whack-a-mole administration of low-doseanti-CD20 therapy could predispose a significant proportionof patients to harbor a temporal discordance between suchtreatment and its intended targets consequently producing anineffective depletion of both CD20+ B cells and CD20+CD3+ T cells (likely resulting in a potential type II error inefficacy analyses)
Given the heterogeneity in the kinetics of B-cell repopu-lation following alemtuzumab therapy coupled with theknown median half-life of rituximab at 22 days (with a rangeof 61ndash52 days as per package insert) we strongly advise formonthly lymphocyte subset analysis to precisely synchro-nize administration of a rituximab low-dose anti-CD20whack-a-mole therapy strategy to buffer against the dis-cordant B-cell hyperrepopulation in the absence of ade-quate T-cell help In addition this strategy will attenuatethe reemergence of the proinflammatory CD20+ T cellsIt remains to be seen if a single dose of rituximab willbe sufficient or whether multiple whack-a-mole cycleswill be required for a therapeutic effect of preventingalemtuzumab-associated secondary autoimmunity
It is of interest that anti-CD20 therapy achieves about a 99loss of peripheral blood B lymphocytes without affectingplasma cells or plasmablasts the principal antibody-secretingcells which are devoid of cell surface CD20 expression In
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 5
Figure 1 A model for the mitigation of secondary autoimmunity in patients with MS post-alemtuzumab
In the upper portion of the figure we illustrate alemtuzumab treatment and its effect on elimination of antindashself-lymphocytes by 2 principal mechanismsclearance through the reticular endothelial system (RES on the left) and assembly of themembrane attack complex (MAC) facilitating the passage of C9 whichcompromises cell membrane integrity thereby culminating in cytotoxicity and cell death The lower middle illustration emphasizes post-alemtuzumabtreatment-inducedmobilization of bonemarrow stem cells reconstituting the immune system B cells undergo a discordant hyperrepopulation approachingpretreatment baseline numbers 3ndash6 months following alemtuzumab treatment whereas T-cell reconstitution is considerably delayed (12ndash24 months)Hypothetically the highly discordant hyperrepopulation of B cells plays a role in the development of secondary autoimmunity Post-alemtuzumab treatmentcirculatingmononuclear cells are principally CD3+-naive T cells CD19+ CD20+-naive B cells as well as a unique population of cells that express both the B-cellantigen CD20 and the T-cell antigen CD3 These latter cells we refer to as Chimeric lymphocytes (C cells) and they are known to express proinflammatorycytokines which in the absence of adequate T-cell help can foment the production of antindashself-antibodies This can initiate corresponding autoantibody-mediated disorders such as those designated by green labels in the figure as well as to T cells capable of orchestrating cellularmechanisms of autoimmunity(designated by purple labels) To the lower left of the lower diagram one can see an enrichment in the CD3+ CD20+ C cells simultaneouswith the discordant B-cell hyperrepopulation (generally emerging approximately 3ndash6 months following alemtuzumab treatment) in the context of a deficiency in the clonalfrequency of regulatory T cells (Tregs) (ie identified as CD4+CD25hiFoxP3+) In the absence of T-cell help such B cells are rendered incapable of discriminatingbetween self and foreign epitopes to both other B cells thereby coordinating the development of antibodies as well as to T cells leading to T-cell receptormaturation with elaboration of cytokine and chemokine expression profiles commensurate to foment cellular autoimmunemechanisms The central portionof the diagram serves to illustrate the potential diversity of antibody-mediated secondary autoimmune states (green line paths) We also see activation ofT cells which can mediate secondary autoimmunity (purple line paths) and granulomatous inflammatory disease most specifically sarcoidosis Monitoringmonthly lymphocyte subsets facilitates detection of the discordant B-cell hyperrepopulation phase of bone marrow mononuclear cell mobilization afteralemtuzumab therapy and thereby provides for the discrete and temporally punctuated administration of an anti-CD20 ldquowhack-a-molerdquo strategy formitigating secondary autoimmunity Specifically we administered low-dose rituximab to orchestrate the deletionof bothCD20+B cells in conjunctionwith theCD20+CD3+ C cells along with their B-cell activation capabilities via the elaboration of proinflammatory cytokine and chemokine cascades The net effect isseen approximately 4months later (in the upper circle on the right lower side of the diagram) when there is amarked diminution of both effectormemory Bcells and autoimmunity-inducing C cells with a corresponding expansion in the clonal frequency of Tregs
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
keeping with this observation anti-CD20 therapy appears toexert no impact on CSF antibody indices such as oligoclonalbanding increased immuno gamma globulin (IgG) indexandor an elevation in IgG synthesis rates characteristic ab-normalities identified in approximately 90 of patients withMS when using isoelectric focusing techniques Alternatelythe peripheral loss of B cells does correspond to a markedreduction in the development of both T1 gadolinium-enhancing and combined unique MS plaque lesions3839
In a recent study the third-generation glycoengineered chi-meric anti-CD20 therapy ublituximab was shown to reduceboth effector and memory CD8 T-cell populations while alsoaugmenting the clonal frequency of naive CD8+ T cells38 Oneof the most conspicuous observations was the identification ofa population of lymphocytes with cell surface expression ofboth CD20+ and CD3+ (those designated as chimeric or Ccells in our hypothetical model figure 1) with further char-acterization revealing that such cells exhibit features inkeeping with memory CD8+ T cells40
The functionally chimeric lymphocytes produce proin-flammatory mediators which may play a key role in thepromiscuous antigen presentation of self-motifs during thediscordant hyperrepopulation of B cells following alemtuzu-mab treatment (figure 1) Lovett-Racke et al categoricallycharacterized both the cellular identification and cytokinechemokine expression profiles using flow cytometric tech-niques from 47 patients withMS treated with ublituximab and
confirmed that such treatment resulted in significantly at-tenuated expression of proinflammatory cytokines reducedantigen presentation a shift from the effectormemory phe-notype to repopulation of naive lymphocytes and importantlyaugmentation in the clonal frequency of regulatory T cells(Tregs)33
A primary immune defect in patients with MS is a deficiencyin Tregs Efficacy in treating the disorder at least in partinvolves reconstitution of the immune networkrsquos regulatorycapabilities through the expansion of Tregs specificallyidentified as CD4+CD25hiFoxP3+2838 The observationsfrom this investigation suggest that anti-CD20 therapy is ca-pable of provoking a skewing or immune deviation that maybe secondary perhaps at least in part to the deletion ofCD20+CD3+ C cells thereby resulting in reduced B cellndashmediated degenerate antigen presentation of self-motifsalong with a broadening in the clonal frequency of Tregs all ofwhich may be germane to our understanding of how we canuse alemtuzumab while actively reducing (vis a vis with theapplication of a lsquowhack-a-molersquo cell depletion strategy) theincidence of secondary autoimmunity (figures 1 and 2)33
We successfully used low-dose rituximab 100 mg (50ndash75mgm2) for patients with neuromyelitis optica spectrumdisorder (NMOSD) who could not afford access to higherdoses of rituximab A 100-mg infusion depletes the CD19population of B cells to less than 2 for an average of 99 days(in essence B-cell suppression is highly titratable analogous
Figure 2 Low-dose anti-CD20 therapy post-alemtuzumab schematic illustrating a potential pilot protocol
This schematic depicts normal CD4+ and CD19+ cell reconstitution9 as well as the theoretical CD19+ reconstitution with our proposed low-dose rituximabprotocol Low-dose rituximab (eg 100 mg) is given subsequent to the detection of the precociously discordant B-cell hyperrepopulation phase of bonemarrow mononuclear cell mobilization following alemtuzumab treatment an intervention which attenuates promiscuous antigen presentation by B cellscapable of activating antindashself-humoral and cellular networks while also serving to promote a more synchronized repopulation across the bone marrowmobilization of mononuclear cell heterogeneity (ie achieving a more balanced return of B and T lymphocyte populations with the added dividend ofamplifying the clonal frequency of Tregs and observation akin to tolerance induction in patients with MS)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 7
to immunologic labetalol the latter commonly used as ahighly titratable agent for management of hypertensive crisessuch as hypertensive encephalopathy where loss of cerebro-vascular autoregulation precludes the employment of long-acting agents which could result in a protracted compromisein cerebral blood flow dynamics predisposing to a hypoxic-ischemic insult) in patients with NMOSD compared with 184days for a 1000 mg dose of rituximab41
Low-dose rituximab is a more attractive alternative to stan-dard doses of 1000 mg or 375 mgm2 First doses of ritux-imab as low as 1 mgm2 suppress B cells by 97 in healthycontrols and B cells remain suppressed to 75 of baselinelevels at 12 weeks after infusion4243
Second low-dose anti-CD20 therapy does not result in pro-longed B-cell depletion so as not to interfere with repeatcycles of alemtuzumab therapy41
Third low-dose rituximab may facilitate greater control ofB-cell repopulation and improved temporal synchronizationwith T-cell repopulation
Last reduced dosing magnitude reduces the duration of im-munosuppression compared with conventional doses of rit-uximab and may eventually be shown in evidence-basedstudies to demonstrate both safety and cost advantages if fewcomplications are identified with the low-dose regimen
A more robust clinical trial with a primary outcome of thedevelopment of secondary autoimmunity would not likelyrequire a large number of participants given the incidence rateof 40 of autoimmune thyroid disease in patients with MSwho have received alemtuzumab34 Hence we would esti-mate an incidence of 40 in the control group ofalemtuzumab-only treated patients and with an assumption ofan incidence of 10 in patients who would receive adjunctrituximab If we assign the probability of a type I error of 5and a power of 80 a trial would need approximately 80patients total (40 in each arm) accounting for drop-outs
In addition to our small sample size and an unrandomizedand unblended cohort many physicians prescribe steroidswith rituximab infusion (methylprednisolone 250 mg beforeeach and every alemtuzumab infusion in our center) to pre-vent infusion reactions It is possible that the potential positiveeffects of secondary autoimmunity prevention attributed torituximab are instead or at least in part due to steroid usageIn addition treatment may simply delay secondary autoim-munity rather than preventing it and longer periods of as-certainment will be required to assess for this prospect
An alternate explanation concerning the impact of rituximabon secondary autoimmunity is that some individuals mayrespond differently to low-dose anti-CD20 therapy due to theeffects of the FCGR3A polymorphism42 We do not know theeffect of the polymorphism on low-dose rituximab kinetics
however binding affinity may play a larger role in low-doserituximab compared with conventional doses given the lowerabsolute concentration of rituximab Such issues should becarefully considered in the design of a larger trial particularlygiven potential effects of such factors on response character-istics as well as on study cost
As the field of neurology shifts from amodel of step escalationto induction therapy for the treatment of MS strategies thatare aimed at mitigating the risks of potent disease modifyingtherapies are urgently needed43
Only through the scientific method of subjecting our hy-pothesis to the rigors of a controlled adequately blindedprospective and adequately powered clinical trial can weconfirm or refute the hypothesis-driven question can theapplication of low-dose anti-CD20 therapy temporally syn-chronized with objective confirmation of B-cell hyper-repopulation serve to adequately reduce or even preventalemtuzumab-associated secondary autoimmunity
Furthermore the addition of anti-CD20 therapy could po-tentially confer benefits on immune deviation that would exertadded efficacy in synergy with the alemtuzumab-mediatedmechanisms of action in the establishment of disease re-mission while constituting augmented and durable regulatoryproperties in keeping with those achieved during the criticalperiod that we now recognize collectively as self-tolerance
Buffeted by the broad dissemination of bone marrow mobili-zation of stem cells following alemtuzumab treatment maypromote the process of restoration and neurologic functionalreconstitution Recent evidence has demonstrated that anemerging biomarker for assessing tissue damage in the CNS ofpatients withMS the neurofilament light chain is reducedmostmarkedly following the administration of alemtuzumab whencompared with other disease-modifying therapies and that suchlevels remain reduced to the greatest magnitude over time44
It was once thought that a proposition such as repair andfunctional recovery from MS was wholly enigmatic and un-likely However we have arrived at a point in the history of ourunderstanding of the disorderrsquos pathobiology in concert withthe corresponding derangements in immune regulatory in-fluences and how to remediate them We believe our work torepresent but a single small step toward this constellation ofgoals that are so important to our deserving patients theirfamilies our community and those of us who serve on thoseteams who care for and about them
AcknowledgmentThe authors thank Mr Jason Ooi and Dr Matthew Parsonsfor their transformation and production of Elliot andTeresa Frohmanrsquos formulation of the figure 1 medicalillustration which showcases alemtuzumabrsquos mechanism ofaction the pathobiological underpinnings for treatment-associated secondary autoimmunity and the hypothetical
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
mechanisms germane to our ldquowhack-a-molerdquo B-cell de-letion strategy aimed at mitigating alemtuzumab-associatedautoimmunity in MS
Study fundingThe National Multiple Sclerosis Society 5-Year InstitutionalFellowship Training Grant Awarded to TC Frohman andEM Frohman Fellows funded E Meltzer and RA Cruz(coauthors) MS and Neuroimmunology Center The DellMedical School at The University of Texas at Austin
DisclosureE Meltzer served as a consultant for Genzyme and receivedhonoraria from Novartis S Campbell and B Ehrenfeld havenothing to disclose L Steinman is on the Editorial Boards ofthe Proceedings of the National Academy of Sciences and theJournal of Neuroimmunology He has served on the EditorialBoard of the Journal of Immunology and International Immu-nology He has served as a member of grant review committeesfor the NIH and the National MS Society He has served orserves as a consultant and received honoraria from AtaraBiotherapeutics Atreca Biogen-Idec Celgene CentocorCoherus EMD-Serono Genzyme Johnson and JohnsonNovartis RocheGenentech Teva Pharmaceuticals Incand TG Therapeutics He has served on the Data SafetyMonitoring Board for TG Therapeutics He serves on theBoard of Directors of Tolerion and Chairs the ScientificAdvisory Board for Atreca Currently L Steinman receivesresearch grant support from the NIH and Atara Bio-therapeutics MS Parsons has nothing to disclose SSZamvil is Deputy Editor ofNeurology Neuroimmunology andNeuroinflammation and is an Associate Editor for Frontiers inImmunology and Frontiers in Neurology He serves on theAdvisory Committee for the American Congress onTreatment and Research in Multiple Sclerosis (ACTRIMS)and is a standing member of the research grant reviewcommittee for the National Multiple Sclerosis Society(NMSS) He has served on the Editorial Board of theJournal of Clinical Investigation The Journal of Immunologyand The Journal of Neurological Sciences and has been acharter member of the grant review committee for the NIHClinical Neuroimmunology and Brain Tumors (CNBT)He has served or serves as a consultant and receivedhonoraria from Alexion Biogen-Idec EMD-SeronoGenzyme Novartis RocheGenentech and Teva Pharma-ceuticals Inc and has served on Data Safety MonitoringBoards for Lilly BioMS Teva and Opexa TherapeuticsCurrently SS Zamvil receives research grant support fromthe NIH NMSS Weill Institute Race to Erase MS and theMaisin Foundation TC Frohman has received advisoryboard fees from Alexion EM Frohman has receivedspeaker honoraria from Genzyme Novartis Alexion andAcorda Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationDecember 25 2019 Accepted in final form July 6 2020
References1 Coles AJ Twyman CL Arnold DL et al Alemtuzumab for patients with relapsing
multiple sclerosis after disease-modifying therapy a randomised controlled phase 3trial Lancet 20123801829ndash1839
2 Cohen JA Coles AJ Arnold DL et al Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis a randomisedcontrolled phase 3 trial Lancet 20123801819ndash1828
3 Coles AJ Cohen JA Fox EJ et al Alemtuzumab CARE-MS II 5-year follow-upNeurology 2017891117ndash1126
4 Havrdova E Arnold DL Cohen JA et al Alemtuzumab CARE-MS I 5-year follow-upNeurology 2017891107ndash1116
5 Sarvepalli D Rashid MU Ullah W Zafar Y Khan M Idiopathic thrombocytopenicpurpura a rare syndrome with alemtuzumab review of monitoring protocol Cureus201911e5715
6 Ruck T Schulte-Mecklenbeck A Pfeuffer S et al Pretreatment anti-thyroid auto-antibodies indicate increased risk for thyroid autoimmunity secondary to alemtuzu-mab a prospective cohort study EBioMedicine 201946381ndash386
Appendix Authors
Name Location Contribution
Ethan MeltzerMD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
SarahCampbell RN
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
BenjaminEhrenfeldMSW
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
Roberto ACruz MD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
LawrenceSteinman MD
Department ofNeurology StanfordUniversity School ofMedicine
Conception and criticalrevision of themanuscript forintellectual content
Matthew SParsons PhD
Division of Microbiologyand Immunology YerkesNational PrimateResearch CenterDepartment of Pathologyand Laboratory MedicineEmory University
Conception and criticalrevision of themanuscript forintellectual content
Scott S ZamvilMD PhD
Department ofNeurology amp Program inImmunology Universityof California SanFrancisco
Conception and criticalrevision of themanuscript forintellectual content
Elliot MFrohman MDPhD
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical SchoolUniversity of Texas atAustin
Conception and criticalrevision of themanuscript forintellectual content
Teresa CFrohmanMPAS MSCSPA-C FANA
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical School Universityof Texas at Austin
Conception and criticalrevision of themanuscript forintellectual content
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 9
7 Ruck T Pfeuffer S Schulte-Mecklenbeck A et al Vitiligo after alemtuzumab treat-ment secondary autoimmunity is not all about B cells Neurology 201891e2233ndashe2237
8 Zimmermann J Buhl T Muller M Alopecia universalis following alemtuzumabtreatment in multiple sclerosis a barely recognized manifestation of secondaryautoimmunity-report of a case and review of the literature Front Neurol 20178569
9 Rotondi M Molteni M Leporati P Capelli V Marino M Chiovato L Autoimmunethyroid diseases in patients treated with alemtuzumab for multiple sclerosis an ex-ample of selective anti-TSH-receptor immune response Front Endocrinol (Lau-sanne) 20178254
10 Costelloe L Jones J Coles A Secondary autoimmune diseases following alemtuzu-mab therapy for multiple sclerosis Expert Rev Neurother 201212335ndash341
11 Jones JL Phuah CL Cox AL et al IL-21 drives secondary autoimmunity in patientswith multiple sclerosis following therapeutic lymphocyte depletion with alemtuzu-mab (Campath-1H) J Clin Invest 20091192052ndash2061
12 Torino F Barnabei A Paragliola R Baldelli R Appetecchia M Corsello SM Thyroiddysfunction as an unintended side effect of anticancer drugs Thyroid 2013231345ndash1366
13 Azzopardi L Thompson SA Harding KE et al Predicting autoimmunity afteralemtuzumab treatment of multiple sclerosis J Neurol Neurosurg Psychiatry 201485795ndash798
14 Trinh T Haridas AS Sullivan TJ Ocular findings in alemtuzumab (Campath-1H)-induced thyroid eye disease Ophthalmic Plast Reconstr Surg 201632e128ndashe129
15 von Kutzleben S Pryce G Giovannoni G Baker D Depletion of CD52-positivecells inhibits the development of central nervous system autoimmune disease butdeletes an immune-tolerance promoting CD8 T-cell population Implications forsecondary autoimmunity of alemtuzumab in multiple sclerosis Immunology 2017150444ndash455
16 Wiendl H Carraro M Comi G et al Lymphocyte pharmacodynamics are not asso-ciated with autoimmunity or efficacy after alemtuzumab Neurol NeuroimmunolNeuroinflamm 201971ndash10 doi101212NXI0000000000000635
17 Kousin-Ezewu O Azzopardi L Parker RA et al Accelerated lymphocyte recoveryafter alemtuzumab does not predict multiple sclerosis activity Neurology 2014822158ndash2164
18 Jones J Thompson S Loh P et al Human autoimmunity after lymphocyte depletionis caused by homeostatic T-cell proliferation Proc Natl Acad Sci U S A 201311020200ndash20205
19 Costa DB Kobayashi SS Whacking a mole-cule clinical activity and mechanisms ofresistance to third generation EGFR inhibitors in EGFR mutated lung cancers withEGFR-T790M Transl Lung Cancer Res 20156809ndash815
20 Shin J MacCarthy T Antagonistic coevolution drives whack-a-mole sensitivity ingene regulatory networks PLoS Comput Biol 201511e1004432
21 Suzuki K Whack-a-mole strategy for multifocal ground glass opacities of the lungJ Thorac Dis 20179(suppl 3)S201ndashS207
22 Swanson DS Harrison CJ Playing Whack-a-Mole with pneumococcal serotypeeradication Pediatrics 2017140e20172034
23 Mestrovic T A microbial game of whack-a-mole clinical case series of the urethraluncloaking phenomenon caused by Corynebacterium glucuronolyticum in mentreated for Chlamydia trachomatis urethritis Infection 201947121ndash124
24 Gelfand JM Cree BAC Hauser SL Ocrelizumab and other CD20+ B-cell-depletingtherapies in multiple sclerosis Neurotherapeutics 201714835ndash841
25 Voog E Morschhauser F Solal-Celigny P Neutropenia in patients treated with rit-uximab N Engl J Med 20033482691ndash2694 discussion 2691ndash2694
26 Bar-Or A Fawaz L Fan B et al Abnormal B-cell cytokine responses a trigger of T-cell-mediated disease in MS Ann Neurol 201067452ndash461
27 Weber MS Prodrsquohomme T Patarroyo JC et al B-cell activation influences T-cellpolarization and outcome of anti-CD20 B-cell depletion in central nervous systemautoimmunity Ann Neurol 201068369ndash383
28 Monson NL Cravens P Hussain R et al Rituximab therapy reduces organ-specificT cell responses and ameliorates experimental autoimmune encephalomyelitis PLoSOne 20116e17103
29 Molnarfi N Schulze-Topphoff U Weber MS et al MHC class II-dependent B cellAPC function is required for induction of CNS autoimmunity independent of myelin-specific antibodies J Exp Med 20132102921ndash2937
30 Baker D Herrod SS Alvarez-Gonzalez C Giovannoni G Schmierer KInterpreting lymphocyte reconstitution data from the pivotal phase 3 trials of alem-tuzumab JAMA Neurol 201774961ndash969
31 Krupica T Fry TJ Mackall CL Autoimmunity during lymphopenia a two-hit modelClin Immunol 2006120121ndash128
32 Wilk EWitte TMarquardt N et al Depletion of functionally active CD20+ T cells byrituximab treatment Arthritis Rheum 2009603563ndash3571
33 Schuh E Berer K Mulazzani M et al Features of human CD3+CD20+ T cellsJ Immunol 20161971111ndash1117
34 Gingele S Kripuletz T Jacobs R Role of CD20+ T cells in multiple sclerosisimpli-cations for treatment with ocrelizumab Neural Regen Res 202015663ndash664
35 Palanichamy A Jahn S Nickles D et al Rituximab efficiently depletes increasedCD20-expressing T cells in multiple sclerosis patients J Immunol 2014193580ndash586
36 Holley JE Bremer E Kendall AC et al CD20+ inflammatory T-cells are present inblood and brain of multiple sclerosis patients and can be selectively targeted forapoptotic elimination Mult Scler Relat Disord 20143650ndash685
37 von Essen MR Ammitzboslashll C Hansen RH et al Proinflammatory CD20+ T cells inthe pathogenesis of multiple sclerosis Brain 2019142120ndash132
38 Lovett-Racke AE Gormley M Liu Y et al B cell depletion with ublituximab reshapesthe T cell profile in multiple sclerosis patients J Neuroimmunol 2019332187ndash197
39 Cross AH Stark JL Lauber J Ramsbottom MJ Lyons JA Rituximab reduces B cells andT cells in cerebrospinal fluid ofmultiple sclerosis patients J Neuroimmunol 200618063ndash70
40 Naismith RT Piccio L Lyons JA et al Rituximab add-on therapy for breakthroughrelapsing multiple sclerosis a 52-week phase II trial Neurology 2010741860ndash1867
41 Greenberg BM Graves D Remington G et al Rituximab dosing and monitoringstrategies in neuromyelitis optica patients creating strategies for therapeutic successMult Scler 2012181022ndash1026
42 Kim SH Jeong IH Hyun JW et al Treatment outcomes with rituximab in 100patients with neuromyelitis optica influence of FCGR3A polymorphisms on thetherapeutic response to rituximab JAMA Neurol 201572989ndash995
43 Steinman L Induction of new autoimmune diseases after alemtuzumab therapy formultiple sclerosis learning from adversity JAMA Neurol 201774907ndash908
44 Delcoigne B Manouchehrinia A Barro C et al Blood neurofilament light levelssegregate treatment effects in multiple sclerosis Neurology 202094e1201ndashe1212
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
DOI 101212NXI000000000000086820207 Neurol Neuroimmunol Neuroinflamm
Ethan Meltzer Sarah Campbell Benjamin Ehrenfeld et al depletion strategy
Mitigating alemtuzumab-associated autoimmunity in MS A whack-a-mole B-cell
This information is current as of August 7 2020
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

For all 5 patients the mean follow-up duration from the initialdose of alemtuzumab was 41 months (range 34ndash48 months)None of the patients developed secondary autoimmunecomplications as defined by the Comparison of Alemtuzumaband Rebif Efficacy in Multiple Sclerosis (CARE-MS) I and IItrials34 Based on the results of CARE-MS I we anticipatedthat 30ndash40 of patients with long-term follow-up wouldhave developed autoimmune thyroid disease34
Of the 5 additional patients with a follow-up duration of less than24 months (table 2) who received low-dose rituximab treatmentfollowing alemtuzumab 2 patients received 1 infusion of ritux-imab and 3 patients received 2 infusions of rituximab Themedian time to 40ndash50 recovery of the CD19+ cell count was2 months post-alemtuzumab and the median time to the firstrituximab dose administration was 3 months post-alemtuzumab
In this second cohort 1 patient developed transient neu-tropenia with an absolute neutrophil count (ANC) lt500μL2 months after the second dose of 100 mg of rituximab Thispatient was treated with granulocyte colony-stimulating factorand reconstituted the ANC within 1 month Another patientdeveloped a urinary tract infection and an additional patientdeveloped an upper respiratory tract infection after receivinglow-dose rituximab while both B- and T-cell lymphocyteswere suppressed
Late-onset neutropenia is a well-described phenomenon afterrituximab infusion which has been considered to be relatedto transient autoimmunity25 Alternately neutropenia hasalso been documented in postmarketing surveillance ofalemtuzumab-treated patients albeit at a much lower in-cident rate when compared with the frequency of the mostcommon alemtuzumab-induced secondary autoimmuneconditions particularly thyroiditis (eg Graves disease andHashimoto thyroiditis)34
All patients treated in both patient cohorts were on pro-phylactic valacyclovir or acyclovir for 24 consecutive monthsincluding during treatment with low-dose rituximab givenhigh rates of herpes reactivation in the clinical trials
DiscussionAlemtuzumab treatment in MS is associated with an earlyhyperrepopulation of B cells that emerge between 3 and 6months following treatment which precedes the repopulationof T cells that occurs between 12 and 24 months followingtreatment A fundamental discordance in the return of humoraland cellular networks is likely to play a role at least in part in theincidence of the adverse event most strikingly associated withalemtuzumab treatment secondary autoimmunity26ndash29
T-cell help is required for B-cell differentiation isotypeswitching and antibody secretion The interaction betweenB cells and T cells is bidirectional As such anti-CD20 B-cell
depletion in MS and experimental autoimmune encephalitis(EAE) promotes T-cell immune modulation characterizedby a significant reduction in proinflammatory Th1 and Th17cells which likely reflects a decrease in B-cell antigen-presenting cell function26 In this context selective de-ficiency of major histocompatibility complex (MHC) ClassII expression by B cells in mice eliminates both susceptibilityto EAE and the expansion of Th1 and Th17 cells29
In the absence of T-cell help B cells are rendered unable todifferentiate between the antigen presentation of self- vsnonndashself-epitopes at least in part secondary to a considerablylower threshold for presentation of low-magnitude antigenswhen compared with macrophages or dendritic cells Fur-thermore anti-CD20 treatment of MS and EAE promotesT-cell immune modulation characterized by a significant re-duction in the proinflammatory network at least in partmediated by Th1726ndash29 Conspicuously B cellndashspecific MHCClass IIndashdeficient mice are rendered resistant to the de-velopment of EAE28
Secondary humoral autoimmunity resulting in hyper- or hy-pothyroidism thrombocytopenia or renal disease are wellknown risks following alemtuzumab treatment of MS56 Wehypothesize that anti-CD20 B-cell depletion after alemtuzu-mab administration may mitigate the risk of secondary auto-immunity and have investigated this possibility Our initialresults suggest that anti-CD20 B-cell depletion is safe andpotentially efficacious However given the small sample sizeand unrandomized and unblinded cohort more rigorousstudies need to be pursued before making any declarationregarding efficacy
Several hypotheses attempt to delineate the cause of sec-ondary autoimmune disease associated with alemtuzumabMSdisease-modifying therapy Unlike traditional B-cell returnafter anti-CD20 therapies B-cell repopulation occurs rapidlyfollowing alemtuzumab treatment and is associated withhyperrepopulation of immature and mature B cells abovebaseline levels30 Following alemtuzumab treatment B-cellrepopulation occurs well in advance of T-cell repopulation(3ndash6 months compared with 12ndash24 months re-spectively) which may compromise the counterbalancing ofhumoral and cellular mechanisms that serve to maintain im-mune regulation
Notwithstanding these findings secondary autoimmune dis-ease after alemtuzumab treatment exhibits a long latencybefore presentation that is well beyond the observed B-cellhyperrepopulation and in fact coincides more closely withT-cell repopulation as autoantibody production is likely CD4T-cell dependent31
T-cell regeneration after depletion in adults is predominantlyachieved by thymic-independent homeostatic peripheral ex-pansion This process unlike T-cell regeneration in childrenwhich occurs primarily in the thymus is associated with
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
decreased self-tolerance a potential molecular scaffolding onwhich autoimmunity can result31
The goal of the temporally associated administration of low-doserituximab is not exclusively restricted to delaying the return ofthe CD19+ B-cell population or an attempt to solely synchronizethe reconstitution of B- and T-cell subsets Data from clinicaltrials that have analyzed the kinetics of humoral and cellularsubsets reveal no evidence of correlation that dichotomizes therisk predilection for alemtuzumab-mediated secondary autoim-munity16 Future work should also characterize the effect ofrituximab on a unique and proinflammatory mononuclear cellwhich coexpresses both CD20 andCD3 (ie CD20+ T cells andchimeric or C cells) which may serve to promote secondaryautoimmunity and would be expected to be deleted along withCD20+ B cells during our administration of low-dose rituximab
A uniquemember of the immune systemrsquosmononuclear cell poolis the CD20+ T cell (ie a chimeric lymphocyte or C cell figure1) which includes both CD4+ and CD8+ cells with the latterbeing the predominant of this cell type Its T-cell origin has beenconfirmed via the detection of CD3 encoded mRNA via reversetranscriptase-polymerase chain reaction (RT-PCR)3233 Thedistribution of these cells is broad and includes the primary andsecondary lymphoid tissue thymus bone marrow lymph nodeadenoids liver and cerebrospinal fluid (CSF) Conspicuously atresting conditions CD20+ T cells exhibit augmented release ofcytokines vs CD20minusT cells Specifically they release interferon γinterleukin (IL) 1 β IL-2 IL-4 IL-8 IL-10 transforming growthfactor β tumor necrosis factor α and c-c chemokine34
Under conditions of immune stimulation there is an escala-tion in cytokine production in CD20+ T cells32 Furthermoreenhanced expression of IL-17 is also characteristic of thissmall population of lymphocytes33 In patients with relapsing-remitting and primary progressive MS vs healthy controlsthere is an increased frequency of CD20+T cells in peripheralblood35
In those with MS there is an increased clonal frequency ofsuch cells in CSF when compared with the analysis of pe-ripheral blood mononuclear cells and the magnitude of thatclonal frequency is correlated with clinical disability in pa-tients with MS as measured by the long-validated ExpandedDisability Status Scale score36 Also CD20+ T cells areidentified within chronic white matter plaque lesions derivedfrom the MS brain36 In drastic contrast to the small pro-portion of such cells from the peripheral blood of controls theCD20+ T-cell fraction in patients with MS represents astriking 184 of all CD20+ cells including those mono-nuclear cells that are CD19+ B cells37
B-cell hyperrepopulation accompanied by a reduction ofT-cell help establishes circumstances whereby antigen pre-sentation coordinated by B cells renders them unable todifferentiate between self (whereby antigen presentation ofautoantigens stereotypically produces immune anergy) and
foreign epitopes (which appropriately culminates in immuneactivation) Alternately the B-cell depletion also comes withthe downregulation of inflammatory cytokines secondary toB-cell induction of T-cell activity and the eventual cytokinerelease syndrome
A detailed figure (figure 1) delineates our hypothetical con-stellation of features proposed as the basis for a low-dose anti-CD20 whack-a-mole strategy aimed at mitigating secondaryautoimmunity
If our proposed risk mitigation strategy were to be used morebroadly for feasibility there would need to be a straightfor-ward way of timing rituximab infusions As such figure 2illustrates a schematic for a potential protocol using a low-dose anti-CD20 (rituximab) whack-a-mole secondary auto-immunity mitigation strategy post-alemtuzumab treatmentand its effect on B-cell repopulation Specifically we timedlow-dose rituximab infusion with a CD19+ B-cell recovery of50 of normal baseline We chose this as a relatively easymarker to measure and to ensure that patients would receiverituximab synchronous to the B-cell hyperrepopulation phaseof postndashalemtuzumab-induced bone marrow mononuclearcell mobilization
Alternatively rituximab could be given at a fixed interval suchas 3 or 4 months after alemtuzumab infusion a commonalbeit not consistent duration for the bone marrow mobili-zation and peripheral repopulation of B cells However ifB-cell hyperrepopulation is delayed (eg until 4ndash6 months) afixed timing for whack-a-mole administration of low-doseanti-CD20 therapy could predispose a significant proportionof patients to harbor a temporal discordance between suchtreatment and its intended targets consequently producing anineffective depletion of both CD20+ B cells and CD20+CD3+ T cells (likely resulting in a potential type II error inefficacy analyses)
Given the heterogeneity in the kinetics of B-cell repopu-lation following alemtuzumab therapy coupled with theknown median half-life of rituximab at 22 days (with a rangeof 61ndash52 days as per package insert) we strongly advise formonthly lymphocyte subset analysis to precisely synchro-nize administration of a rituximab low-dose anti-CD20whack-a-mole therapy strategy to buffer against the dis-cordant B-cell hyperrepopulation in the absence of ade-quate T-cell help In addition this strategy will attenuatethe reemergence of the proinflammatory CD20+ T cellsIt remains to be seen if a single dose of rituximab willbe sufficient or whether multiple whack-a-mole cycleswill be required for a therapeutic effect of preventingalemtuzumab-associated secondary autoimmunity
It is of interest that anti-CD20 therapy achieves about a 99loss of peripheral blood B lymphocytes without affectingplasma cells or plasmablasts the principal antibody-secretingcells which are devoid of cell surface CD20 expression In
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 5
Figure 1 A model for the mitigation of secondary autoimmunity in patients with MS post-alemtuzumab
In the upper portion of the figure we illustrate alemtuzumab treatment and its effect on elimination of antindashself-lymphocytes by 2 principal mechanismsclearance through the reticular endothelial system (RES on the left) and assembly of themembrane attack complex (MAC) facilitating the passage of C9 whichcompromises cell membrane integrity thereby culminating in cytotoxicity and cell death The lower middle illustration emphasizes post-alemtuzumabtreatment-inducedmobilization of bonemarrow stem cells reconstituting the immune system B cells undergo a discordant hyperrepopulation approachingpretreatment baseline numbers 3ndash6 months following alemtuzumab treatment whereas T-cell reconstitution is considerably delayed (12ndash24 months)Hypothetically the highly discordant hyperrepopulation of B cells plays a role in the development of secondary autoimmunity Post-alemtuzumab treatmentcirculatingmononuclear cells are principally CD3+-naive T cells CD19+ CD20+-naive B cells as well as a unique population of cells that express both the B-cellantigen CD20 and the T-cell antigen CD3 These latter cells we refer to as Chimeric lymphocytes (C cells) and they are known to express proinflammatorycytokines which in the absence of adequate T-cell help can foment the production of antindashself-antibodies This can initiate corresponding autoantibody-mediated disorders such as those designated by green labels in the figure as well as to T cells capable of orchestrating cellularmechanisms of autoimmunity(designated by purple labels) To the lower left of the lower diagram one can see an enrichment in the CD3+ CD20+ C cells simultaneouswith the discordant B-cell hyperrepopulation (generally emerging approximately 3ndash6 months following alemtuzumab treatment) in the context of a deficiency in the clonalfrequency of regulatory T cells (Tregs) (ie identified as CD4+CD25hiFoxP3+) In the absence of T-cell help such B cells are rendered incapable of discriminatingbetween self and foreign epitopes to both other B cells thereby coordinating the development of antibodies as well as to T cells leading to T-cell receptormaturation with elaboration of cytokine and chemokine expression profiles commensurate to foment cellular autoimmunemechanisms The central portionof the diagram serves to illustrate the potential diversity of antibody-mediated secondary autoimmune states (green line paths) We also see activation ofT cells which can mediate secondary autoimmunity (purple line paths) and granulomatous inflammatory disease most specifically sarcoidosis Monitoringmonthly lymphocyte subsets facilitates detection of the discordant B-cell hyperrepopulation phase of bone marrow mononuclear cell mobilization afteralemtuzumab therapy and thereby provides for the discrete and temporally punctuated administration of an anti-CD20 ldquowhack-a-molerdquo strategy formitigating secondary autoimmunity Specifically we administered low-dose rituximab to orchestrate the deletionof bothCD20+B cells in conjunctionwith theCD20+CD3+ C cells along with their B-cell activation capabilities via the elaboration of proinflammatory cytokine and chemokine cascades The net effect isseen approximately 4months later (in the upper circle on the right lower side of the diagram) when there is amarked diminution of both effectormemory Bcells and autoimmunity-inducing C cells with a corresponding expansion in the clonal frequency of Tregs
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
keeping with this observation anti-CD20 therapy appears toexert no impact on CSF antibody indices such as oligoclonalbanding increased immuno gamma globulin (IgG) indexandor an elevation in IgG synthesis rates characteristic ab-normalities identified in approximately 90 of patients withMS when using isoelectric focusing techniques Alternatelythe peripheral loss of B cells does correspond to a markedreduction in the development of both T1 gadolinium-enhancing and combined unique MS plaque lesions3839
In a recent study the third-generation glycoengineered chi-meric anti-CD20 therapy ublituximab was shown to reduceboth effector and memory CD8 T-cell populations while alsoaugmenting the clonal frequency of naive CD8+ T cells38 Oneof the most conspicuous observations was the identification ofa population of lymphocytes with cell surface expression ofboth CD20+ and CD3+ (those designated as chimeric or Ccells in our hypothetical model figure 1) with further char-acterization revealing that such cells exhibit features inkeeping with memory CD8+ T cells40
The functionally chimeric lymphocytes produce proin-flammatory mediators which may play a key role in thepromiscuous antigen presentation of self-motifs during thediscordant hyperrepopulation of B cells following alemtuzu-mab treatment (figure 1) Lovett-Racke et al categoricallycharacterized both the cellular identification and cytokinechemokine expression profiles using flow cytometric tech-niques from 47 patients withMS treated with ublituximab and
confirmed that such treatment resulted in significantly at-tenuated expression of proinflammatory cytokines reducedantigen presentation a shift from the effectormemory phe-notype to repopulation of naive lymphocytes and importantlyaugmentation in the clonal frequency of regulatory T cells(Tregs)33
A primary immune defect in patients with MS is a deficiencyin Tregs Efficacy in treating the disorder at least in partinvolves reconstitution of the immune networkrsquos regulatorycapabilities through the expansion of Tregs specificallyidentified as CD4+CD25hiFoxP3+2838 The observationsfrom this investigation suggest that anti-CD20 therapy is ca-pable of provoking a skewing or immune deviation that maybe secondary perhaps at least in part to the deletion ofCD20+CD3+ C cells thereby resulting in reduced B cellndashmediated degenerate antigen presentation of self-motifsalong with a broadening in the clonal frequency of Tregs all ofwhich may be germane to our understanding of how we canuse alemtuzumab while actively reducing (vis a vis with theapplication of a lsquowhack-a-molersquo cell depletion strategy) theincidence of secondary autoimmunity (figures 1 and 2)33
We successfully used low-dose rituximab 100 mg (50ndash75mgm2) for patients with neuromyelitis optica spectrumdisorder (NMOSD) who could not afford access to higherdoses of rituximab A 100-mg infusion depletes the CD19population of B cells to less than 2 for an average of 99 days(in essence B-cell suppression is highly titratable analogous
Figure 2 Low-dose anti-CD20 therapy post-alemtuzumab schematic illustrating a potential pilot protocol
This schematic depicts normal CD4+ and CD19+ cell reconstitution9 as well as the theoretical CD19+ reconstitution with our proposed low-dose rituximabprotocol Low-dose rituximab (eg 100 mg) is given subsequent to the detection of the precociously discordant B-cell hyperrepopulation phase of bonemarrow mononuclear cell mobilization following alemtuzumab treatment an intervention which attenuates promiscuous antigen presentation by B cellscapable of activating antindashself-humoral and cellular networks while also serving to promote a more synchronized repopulation across the bone marrowmobilization of mononuclear cell heterogeneity (ie achieving a more balanced return of B and T lymphocyte populations with the added dividend ofamplifying the clonal frequency of Tregs and observation akin to tolerance induction in patients with MS)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 7
to immunologic labetalol the latter commonly used as ahighly titratable agent for management of hypertensive crisessuch as hypertensive encephalopathy where loss of cerebro-vascular autoregulation precludes the employment of long-acting agents which could result in a protracted compromisein cerebral blood flow dynamics predisposing to a hypoxic-ischemic insult) in patients with NMOSD compared with 184days for a 1000 mg dose of rituximab41
Low-dose rituximab is a more attractive alternative to stan-dard doses of 1000 mg or 375 mgm2 First doses of ritux-imab as low as 1 mgm2 suppress B cells by 97 in healthycontrols and B cells remain suppressed to 75 of baselinelevels at 12 weeks after infusion4243
Second low-dose anti-CD20 therapy does not result in pro-longed B-cell depletion so as not to interfere with repeatcycles of alemtuzumab therapy41
Third low-dose rituximab may facilitate greater control ofB-cell repopulation and improved temporal synchronizationwith T-cell repopulation
Last reduced dosing magnitude reduces the duration of im-munosuppression compared with conventional doses of rit-uximab and may eventually be shown in evidence-basedstudies to demonstrate both safety and cost advantages if fewcomplications are identified with the low-dose regimen
A more robust clinical trial with a primary outcome of thedevelopment of secondary autoimmunity would not likelyrequire a large number of participants given the incidence rateof 40 of autoimmune thyroid disease in patients with MSwho have received alemtuzumab34 Hence we would esti-mate an incidence of 40 in the control group ofalemtuzumab-only treated patients and with an assumption ofan incidence of 10 in patients who would receive adjunctrituximab If we assign the probability of a type I error of 5and a power of 80 a trial would need approximately 80patients total (40 in each arm) accounting for drop-outs
In addition to our small sample size and an unrandomizedand unblended cohort many physicians prescribe steroidswith rituximab infusion (methylprednisolone 250 mg beforeeach and every alemtuzumab infusion in our center) to pre-vent infusion reactions It is possible that the potential positiveeffects of secondary autoimmunity prevention attributed torituximab are instead or at least in part due to steroid usageIn addition treatment may simply delay secondary autoim-munity rather than preventing it and longer periods of as-certainment will be required to assess for this prospect
An alternate explanation concerning the impact of rituximabon secondary autoimmunity is that some individuals mayrespond differently to low-dose anti-CD20 therapy due to theeffects of the FCGR3A polymorphism42 We do not know theeffect of the polymorphism on low-dose rituximab kinetics
however binding affinity may play a larger role in low-doserituximab compared with conventional doses given the lowerabsolute concentration of rituximab Such issues should becarefully considered in the design of a larger trial particularlygiven potential effects of such factors on response character-istics as well as on study cost
As the field of neurology shifts from amodel of step escalationto induction therapy for the treatment of MS strategies thatare aimed at mitigating the risks of potent disease modifyingtherapies are urgently needed43
Only through the scientific method of subjecting our hy-pothesis to the rigors of a controlled adequately blindedprospective and adequately powered clinical trial can weconfirm or refute the hypothesis-driven question can theapplication of low-dose anti-CD20 therapy temporally syn-chronized with objective confirmation of B-cell hyper-repopulation serve to adequately reduce or even preventalemtuzumab-associated secondary autoimmunity
Furthermore the addition of anti-CD20 therapy could po-tentially confer benefits on immune deviation that would exertadded efficacy in synergy with the alemtuzumab-mediatedmechanisms of action in the establishment of disease re-mission while constituting augmented and durable regulatoryproperties in keeping with those achieved during the criticalperiod that we now recognize collectively as self-tolerance
Buffeted by the broad dissemination of bone marrow mobili-zation of stem cells following alemtuzumab treatment maypromote the process of restoration and neurologic functionalreconstitution Recent evidence has demonstrated that anemerging biomarker for assessing tissue damage in the CNS ofpatients withMS the neurofilament light chain is reducedmostmarkedly following the administration of alemtuzumab whencompared with other disease-modifying therapies and that suchlevels remain reduced to the greatest magnitude over time44
It was once thought that a proposition such as repair andfunctional recovery from MS was wholly enigmatic and un-likely However we have arrived at a point in the history of ourunderstanding of the disorderrsquos pathobiology in concert withthe corresponding derangements in immune regulatory in-fluences and how to remediate them We believe our work torepresent but a single small step toward this constellation ofgoals that are so important to our deserving patients theirfamilies our community and those of us who serve on thoseteams who care for and about them
AcknowledgmentThe authors thank Mr Jason Ooi and Dr Matthew Parsonsfor their transformation and production of Elliot andTeresa Frohmanrsquos formulation of the figure 1 medicalillustration which showcases alemtuzumabrsquos mechanism ofaction the pathobiological underpinnings for treatment-associated secondary autoimmunity and the hypothetical
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
mechanisms germane to our ldquowhack-a-molerdquo B-cell de-letion strategy aimed at mitigating alemtuzumab-associatedautoimmunity in MS
Study fundingThe National Multiple Sclerosis Society 5-Year InstitutionalFellowship Training Grant Awarded to TC Frohman andEM Frohman Fellows funded E Meltzer and RA Cruz(coauthors) MS and Neuroimmunology Center The DellMedical School at The University of Texas at Austin
DisclosureE Meltzer served as a consultant for Genzyme and receivedhonoraria from Novartis S Campbell and B Ehrenfeld havenothing to disclose L Steinman is on the Editorial Boards ofthe Proceedings of the National Academy of Sciences and theJournal of Neuroimmunology He has served on the EditorialBoard of the Journal of Immunology and International Immu-nology He has served as a member of grant review committeesfor the NIH and the National MS Society He has served orserves as a consultant and received honoraria from AtaraBiotherapeutics Atreca Biogen-Idec Celgene CentocorCoherus EMD-Serono Genzyme Johnson and JohnsonNovartis RocheGenentech Teva Pharmaceuticals Incand TG Therapeutics He has served on the Data SafetyMonitoring Board for TG Therapeutics He serves on theBoard of Directors of Tolerion and Chairs the ScientificAdvisory Board for Atreca Currently L Steinman receivesresearch grant support from the NIH and Atara Bio-therapeutics MS Parsons has nothing to disclose SSZamvil is Deputy Editor ofNeurology Neuroimmunology andNeuroinflammation and is an Associate Editor for Frontiers inImmunology and Frontiers in Neurology He serves on theAdvisory Committee for the American Congress onTreatment and Research in Multiple Sclerosis (ACTRIMS)and is a standing member of the research grant reviewcommittee for the National Multiple Sclerosis Society(NMSS) He has served on the Editorial Board of theJournal of Clinical Investigation The Journal of Immunologyand The Journal of Neurological Sciences and has been acharter member of the grant review committee for the NIHClinical Neuroimmunology and Brain Tumors (CNBT)He has served or serves as a consultant and receivedhonoraria from Alexion Biogen-Idec EMD-SeronoGenzyme Novartis RocheGenentech and Teva Pharma-ceuticals Inc and has served on Data Safety MonitoringBoards for Lilly BioMS Teva and Opexa TherapeuticsCurrently SS Zamvil receives research grant support fromthe NIH NMSS Weill Institute Race to Erase MS and theMaisin Foundation TC Frohman has received advisoryboard fees from Alexion EM Frohman has receivedspeaker honoraria from Genzyme Novartis Alexion andAcorda Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationDecember 25 2019 Accepted in final form July 6 2020
References1 Coles AJ Twyman CL Arnold DL et al Alemtuzumab for patients with relapsing
multiple sclerosis after disease-modifying therapy a randomised controlled phase 3trial Lancet 20123801829ndash1839
2 Cohen JA Coles AJ Arnold DL et al Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis a randomisedcontrolled phase 3 trial Lancet 20123801819ndash1828
3 Coles AJ Cohen JA Fox EJ et al Alemtuzumab CARE-MS II 5-year follow-upNeurology 2017891117ndash1126
4 Havrdova E Arnold DL Cohen JA et al Alemtuzumab CARE-MS I 5-year follow-upNeurology 2017891107ndash1116
5 Sarvepalli D Rashid MU Ullah W Zafar Y Khan M Idiopathic thrombocytopenicpurpura a rare syndrome with alemtuzumab review of monitoring protocol Cureus201911e5715
6 Ruck T Schulte-Mecklenbeck A Pfeuffer S et al Pretreatment anti-thyroid auto-antibodies indicate increased risk for thyroid autoimmunity secondary to alemtuzu-mab a prospective cohort study EBioMedicine 201946381ndash386
Appendix Authors
Name Location Contribution
Ethan MeltzerMD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
SarahCampbell RN
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
BenjaminEhrenfeldMSW
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
Roberto ACruz MD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
LawrenceSteinman MD
Department ofNeurology StanfordUniversity School ofMedicine
Conception and criticalrevision of themanuscript forintellectual content
Matthew SParsons PhD
Division of Microbiologyand Immunology YerkesNational PrimateResearch CenterDepartment of Pathologyand Laboratory MedicineEmory University
Conception and criticalrevision of themanuscript forintellectual content
Scott S ZamvilMD PhD
Department ofNeurology amp Program inImmunology Universityof California SanFrancisco
Conception and criticalrevision of themanuscript forintellectual content
Elliot MFrohman MDPhD
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical SchoolUniversity of Texas atAustin
Conception and criticalrevision of themanuscript forintellectual content
Teresa CFrohmanMPAS MSCSPA-C FANA
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical School Universityof Texas at Austin
Conception and criticalrevision of themanuscript forintellectual content
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 9
7 Ruck T Pfeuffer S Schulte-Mecklenbeck A et al Vitiligo after alemtuzumab treat-ment secondary autoimmunity is not all about B cells Neurology 201891e2233ndashe2237
8 Zimmermann J Buhl T Muller M Alopecia universalis following alemtuzumabtreatment in multiple sclerosis a barely recognized manifestation of secondaryautoimmunity-report of a case and review of the literature Front Neurol 20178569
9 Rotondi M Molteni M Leporati P Capelli V Marino M Chiovato L Autoimmunethyroid diseases in patients treated with alemtuzumab for multiple sclerosis an ex-ample of selective anti-TSH-receptor immune response Front Endocrinol (Lau-sanne) 20178254
10 Costelloe L Jones J Coles A Secondary autoimmune diseases following alemtuzu-mab therapy for multiple sclerosis Expert Rev Neurother 201212335ndash341
11 Jones JL Phuah CL Cox AL et al IL-21 drives secondary autoimmunity in patientswith multiple sclerosis following therapeutic lymphocyte depletion with alemtuzu-mab (Campath-1H) J Clin Invest 20091192052ndash2061
12 Torino F Barnabei A Paragliola R Baldelli R Appetecchia M Corsello SM Thyroiddysfunction as an unintended side effect of anticancer drugs Thyroid 2013231345ndash1366
13 Azzopardi L Thompson SA Harding KE et al Predicting autoimmunity afteralemtuzumab treatment of multiple sclerosis J Neurol Neurosurg Psychiatry 201485795ndash798
14 Trinh T Haridas AS Sullivan TJ Ocular findings in alemtuzumab (Campath-1H)-induced thyroid eye disease Ophthalmic Plast Reconstr Surg 201632e128ndashe129
15 von Kutzleben S Pryce G Giovannoni G Baker D Depletion of CD52-positivecells inhibits the development of central nervous system autoimmune disease butdeletes an immune-tolerance promoting CD8 T-cell population Implications forsecondary autoimmunity of alemtuzumab in multiple sclerosis Immunology 2017150444ndash455
16 Wiendl H Carraro M Comi G et al Lymphocyte pharmacodynamics are not asso-ciated with autoimmunity or efficacy after alemtuzumab Neurol NeuroimmunolNeuroinflamm 201971ndash10 doi101212NXI0000000000000635
17 Kousin-Ezewu O Azzopardi L Parker RA et al Accelerated lymphocyte recoveryafter alemtuzumab does not predict multiple sclerosis activity Neurology 2014822158ndash2164
18 Jones J Thompson S Loh P et al Human autoimmunity after lymphocyte depletionis caused by homeostatic T-cell proliferation Proc Natl Acad Sci U S A 201311020200ndash20205
19 Costa DB Kobayashi SS Whacking a mole-cule clinical activity and mechanisms ofresistance to third generation EGFR inhibitors in EGFR mutated lung cancers withEGFR-T790M Transl Lung Cancer Res 20156809ndash815
20 Shin J MacCarthy T Antagonistic coevolution drives whack-a-mole sensitivity ingene regulatory networks PLoS Comput Biol 201511e1004432
21 Suzuki K Whack-a-mole strategy for multifocal ground glass opacities of the lungJ Thorac Dis 20179(suppl 3)S201ndashS207
22 Swanson DS Harrison CJ Playing Whack-a-Mole with pneumococcal serotypeeradication Pediatrics 2017140e20172034
23 Mestrovic T A microbial game of whack-a-mole clinical case series of the urethraluncloaking phenomenon caused by Corynebacterium glucuronolyticum in mentreated for Chlamydia trachomatis urethritis Infection 201947121ndash124
24 Gelfand JM Cree BAC Hauser SL Ocrelizumab and other CD20+ B-cell-depletingtherapies in multiple sclerosis Neurotherapeutics 201714835ndash841
25 Voog E Morschhauser F Solal-Celigny P Neutropenia in patients treated with rit-uximab N Engl J Med 20033482691ndash2694 discussion 2691ndash2694
26 Bar-Or A Fawaz L Fan B et al Abnormal B-cell cytokine responses a trigger of T-cell-mediated disease in MS Ann Neurol 201067452ndash461
27 Weber MS Prodrsquohomme T Patarroyo JC et al B-cell activation influences T-cellpolarization and outcome of anti-CD20 B-cell depletion in central nervous systemautoimmunity Ann Neurol 201068369ndash383
28 Monson NL Cravens P Hussain R et al Rituximab therapy reduces organ-specificT cell responses and ameliorates experimental autoimmune encephalomyelitis PLoSOne 20116e17103
29 Molnarfi N Schulze-Topphoff U Weber MS et al MHC class II-dependent B cellAPC function is required for induction of CNS autoimmunity independent of myelin-specific antibodies J Exp Med 20132102921ndash2937
30 Baker D Herrod SS Alvarez-Gonzalez C Giovannoni G Schmierer KInterpreting lymphocyte reconstitution data from the pivotal phase 3 trials of alem-tuzumab JAMA Neurol 201774961ndash969
31 Krupica T Fry TJ Mackall CL Autoimmunity during lymphopenia a two-hit modelClin Immunol 2006120121ndash128
32 Wilk EWitte TMarquardt N et al Depletion of functionally active CD20+ T cells byrituximab treatment Arthritis Rheum 2009603563ndash3571
33 Schuh E Berer K Mulazzani M et al Features of human CD3+CD20+ T cellsJ Immunol 20161971111ndash1117
34 Gingele S Kripuletz T Jacobs R Role of CD20+ T cells in multiple sclerosisimpli-cations for treatment with ocrelizumab Neural Regen Res 202015663ndash664
35 Palanichamy A Jahn S Nickles D et al Rituximab efficiently depletes increasedCD20-expressing T cells in multiple sclerosis patients J Immunol 2014193580ndash586
36 Holley JE Bremer E Kendall AC et al CD20+ inflammatory T-cells are present inblood and brain of multiple sclerosis patients and can be selectively targeted forapoptotic elimination Mult Scler Relat Disord 20143650ndash685
37 von Essen MR Ammitzboslashll C Hansen RH et al Proinflammatory CD20+ T cells inthe pathogenesis of multiple sclerosis Brain 2019142120ndash132
38 Lovett-Racke AE Gormley M Liu Y et al B cell depletion with ublituximab reshapesthe T cell profile in multiple sclerosis patients J Neuroimmunol 2019332187ndash197
39 Cross AH Stark JL Lauber J Ramsbottom MJ Lyons JA Rituximab reduces B cells andT cells in cerebrospinal fluid ofmultiple sclerosis patients J Neuroimmunol 200618063ndash70
40 Naismith RT Piccio L Lyons JA et al Rituximab add-on therapy for breakthroughrelapsing multiple sclerosis a 52-week phase II trial Neurology 2010741860ndash1867
41 Greenberg BM Graves D Remington G et al Rituximab dosing and monitoringstrategies in neuromyelitis optica patients creating strategies for therapeutic successMult Scler 2012181022ndash1026
42 Kim SH Jeong IH Hyun JW et al Treatment outcomes with rituximab in 100patients with neuromyelitis optica influence of FCGR3A polymorphisms on thetherapeutic response to rituximab JAMA Neurol 201572989ndash995
43 Steinman L Induction of new autoimmune diseases after alemtuzumab therapy formultiple sclerosis learning from adversity JAMA Neurol 201774907ndash908
44 Delcoigne B Manouchehrinia A Barro C et al Blood neurofilament light levelssegregate treatment effects in multiple sclerosis Neurology 202094e1201ndashe1212
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
DOI 101212NXI000000000000086820207 Neurol Neuroimmunol Neuroinflamm
Ethan Meltzer Sarah Campbell Benjamin Ehrenfeld et al depletion strategy
Mitigating alemtuzumab-associated autoimmunity in MS A whack-a-mole B-cell
This information is current as of August 7 2020
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

decreased self-tolerance a potential molecular scaffolding onwhich autoimmunity can result31
The goal of the temporally associated administration of low-doserituximab is not exclusively restricted to delaying the return ofthe CD19+ B-cell population or an attempt to solely synchronizethe reconstitution of B- and T-cell subsets Data from clinicaltrials that have analyzed the kinetics of humoral and cellularsubsets reveal no evidence of correlation that dichotomizes therisk predilection for alemtuzumab-mediated secondary autoim-munity16 Future work should also characterize the effect ofrituximab on a unique and proinflammatory mononuclear cellwhich coexpresses both CD20 andCD3 (ie CD20+ T cells andchimeric or C cells) which may serve to promote secondaryautoimmunity and would be expected to be deleted along withCD20+ B cells during our administration of low-dose rituximab
A uniquemember of the immune systemrsquosmononuclear cell poolis the CD20+ T cell (ie a chimeric lymphocyte or C cell figure1) which includes both CD4+ and CD8+ cells with the latterbeing the predominant of this cell type Its T-cell origin has beenconfirmed via the detection of CD3 encoded mRNA via reversetranscriptase-polymerase chain reaction (RT-PCR)3233 Thedistribution of these cells is broad and includes the primary andsecondary lymphoid tissue thymus bone marrow lymph nodeadenoids liver and cerebrospinal fluid (CSF) Conspicuously atresting conditions CD20+ T cells exhibit augmented release ofcytokines vs CD20minusT cells Specifically they release interferon γinterleukin (IL) 1 β IL-2 IL-4 IL-8 IL-10 transforming growthfactor β tumor necrosis factor α and c-c chemokine34
Under conditions of immune stimulation there is an escala-tion in cytokine production in CD20+ T cells32 Furthermoreenhanced expression of IL-17 is also characteristic of thissmall population of lymphocytes33 In patients with relapsing-remitting and primary progressive MS vs healthy controlsthere is an increased frequency of CD20+T cells in peripheralblood35
In those with MS there is an increased clonal frequency ofsuch cells in CSF when compared with the analysis of pe-ripheral blood mononuclear cells and the magnitude of thatclonal frequency is correlated with clinical disability in pa-tients with MS as measured by the long-validated ExpandedDisability Status Scale score36 Also CD20+ T cells areidentified within chronic white matter plaque lesions derivedfrom the MS brain36 In drastic contrast to the small pro-portion of such cells from the peripheral blood of controls theCD20+ T-cell fraction in patients with MS represents astriking 184 of all CD20+ cells including those mono-nuclear cells that are CD19+ B cells37
B-cell hyperrepopulation accompanied by a reduction ofT-cell help establishes circumstances whereby antigen pre-sentation coordinated by B cells renders them unable todifferentiate between self (whereby antigen presentation ofautoantigens stereotypically produces immune anergy) and
foreign epitopes (which appropriately culminates in immuneactivation) Alternately the B-cell depletion also comes withthe downregulation of inflammatory cytokines secondary toB-cell induction of T-cell activity and the eventual cytokinerelease syndrome
A detailed figure (figure 1) delineates our hypothetical con-stellation of features proposed as the basis for a low-dose anti-CD20 whack-a-mole strategy aimed at mitigating secondaryautoimmunity
If our proposed risk mitigation strategy were to be used morebroadly for feasibility there would need to be a straightfor-ward way of timing rituximab infusions As such figure 2illustrates a schematic for a potential protocol using a low-dose anti-CD20 (rituximab) whack-a-mole secondary auto-immunity mitigation strategy post-alemtuzumab treatmentand its effect on B-cell repopulation Specifically we timedlow-dose rituximab infusion with a CD19+ B-cell recovery of50 of normal baseline We chose this as a relatively easymarker to measure and to ensure that patients would receiverituximab synchronous to the B-cell hyperrepopulation phaseof postndashalemtuzumab-induced bone marrow mononuclearcell mobilization
Alternatively rituximab could be given at a fixed interval suchas 3 or 4 months after alemtuzumab infusion a commonalbeit not consistent duration for the bone marrow mobili-zation and peripheral repopulation of B cells However ifB-cell hyperrepopulation is delayed (eg until 4ndash6 months) afixed timing for whack-a-mole administration of low-doseanti-CD20 therapy could predispose a significant proportionof patients to harbor a temporal discordance between suchtreatment and its intended targets consequently producing anineffective depletion of both CD20+ B cells and CD20+CD3+ T cells (likely resulting in a potential type II error inefficacy analyses)
Given the heterogeneity in the kinetics of B-cell repopu-lation following alemtuzumab therapy coupled with theknown median half-life of rituximab at 22 days (with a rangeof 61ndash52 days as per package insert) we strongly advise formonthly lymphocyte subset analysis to precisely synchro-nize administration of a rituximab low-dose anti-CD20whack-a-mole therapy strategy to buffer against the dis-cordant B-cell hyperrepopulation in the absence of ade-quate T-cell help In addition this strategy will attenuatethe reemergence of the proinflammatory CD20+ T cellsIt remains to be seen if a single dose of rituximab willbe sufficient or whether multiple whack-a-mole cycleswill be required for a therapeutic effect of preventingalemtuzumab-associated secondary autoimmunity
It is of interest that anti-CD20 therapy achieves about a 99loss of peripheral blood B lymphocytes without affectingplasma cells or plasmablasts the principal antibody-secretingcells which are devoid of cell surface CD20 expression In
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 5
Figure 1 A model for the mitigation of secondary autoimmunity in patients with MS post-alemtuzumab
In the upper portion of the figure we illustrate alemtuzumab treatment and its effect on elimination of antindashself-lymphocytes by 2 principal mechanismsclearance through the reticular endothelial system (RES on the left) and assembly of themembrane attack complex (MAC) facilitating the passage of C9 whichcompromises cell membrane integrity thereby culminating in cytotoxicity and cell death The lower middle illustration emphasizes post-alemtuzumabtreatment-inducedmobilization of bonemarrow stem cells reconstituting the immune system B cells undergo a discordant hyperrepopulation approachingpretreatment baseline numbers 3ndash6 months following alemtuzumab treatment whereas T-cell reconstitution is considerably delayed (12ndash24 months)Hypothetically the highly discordant hyperrepopulation of B cells plays a role in the development of secondary autoimmunity Post-alemtuzumab treatmentcirculatingmononuclear cells are principally CD3+-naive T cells CD19+ CD20+-naive B cells as well as a unique population of cells that express both the B-cellantigen CD20 and the T-cell antigen CD3 These latter cells we refer to as Chimeric lymphocytes (C cells) and they are known to express proinflammatorycytokines which in the absence of adequate T-cell help can foment the production of antindashself-antibodies This can initiate corresponding autoantibody-mediated disorders such as those designated by green labels in the figure as well as to T cells capable of orchestrating cellularmechanisms of autoimmunity(designated by purple labels) To the lower left of the lower diagram one can see an enrichment in the CD3+ CD20+ C cells simultaneouswith the discordant B-cell hyperrepopulation (generally emerging approximately 3ndash6 months following alemtuzumab treatment) in the context of a deficiency in the clonalfrequency of regulatory T cells (Tregs) (ie identified as CD4+CD25hiFoxP3+) In the absence of T-cell help such B cells are rendered incapable of discriminatingbetween self and foreign epitopes to both other B cells thereby coordinating the development of antibodies as well as to T cells leading to T-cell receptormaturation with elaboration of cytokine and chemokine expression profiles commensurate to foment cellular autoimmunemechanisms The central portionof the diagram serves to illustrate the potential diversity of antibody-mediated secondary autoimmune states (green line paths) We also see activation ofT cells which can mediate secondary autoimmunity (purple line paths) and granulomatous inflammatory disease most specifically sarcoidosis Monitoringmonthly lymphocyte subsets facilitates detection of the discordant B-cell hyperrepopulation phase of bone marrow mononuclear cell mobilization afteralemtuzumab therapy and thereby provides for the discrete and temporally punctuated administration of an anti-CD20 ldquowhack-a-molerdquo strategy formitigating secondary autoimmunity Specifically we administered low-dose rituximab to orchestrate the deletionof bothCD20+B cells in conjunctionwith theCD20+CD3+ C cells along with their B-cell activation capabilities via the elaboration of proinflammatory cytokine and chemokine cascades The net effect isseen approximately 4months later (in the upper circle on the right lower side of the diagram) when there is amarked diminution of both effectormemory Bcells and autoimmunity-inducing C cells with a corresponding expansion in the clonal frequency of Tregs
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
keeping with this observation anti-CD20 therapy appears toexert no impact on CSF antibody indices such as oligoclonalbanding increased immuno gamma globulin (IgG) indexandor an elevation in IgG synthesis rates characteristic ab-normalities identified in approximately 90 of patients withMS when using isoelectric focusing techniques Alternatelythe peripheral loss of B cells does correspond to a markedreduction in the development of both T1 gadolinium-enhancing and combined unique MS plaque lesions3839
In a recent study the third-generation glycoengineered chi-meric anti-CD20 therapy ublituximab was shown to reduceboth effector and memory CD8 T-cell populations while alsoaugmenting the clonal frequency of naive CD8+ T cells38 Oneof the most conspicuous observations was the identification ofa population of lymphocytes with cell surface expression ofboth CD20+ and CD3+ (those designated as chimeric or Ccells in our hypothetical model figure 1) with further char-acterization revealing that such cells exhibit features inkeeping with memory CD8+ T cells40
The functionally chimeric lymphocytes produce proin-flammatory mediators which may play a key role in thepromiscuous antigen presentation of self-motifs during thediscordant hyperrepopulation of B cells following alemtuzu-mab treatment (figure 1) Lovett-Racke et al categoricallycharacterized both the cellular identification and cytokinechemokine expression profiles using flow cytometric tech-niques from 47 patients withMS treated with ublituximab and
confirmed that such treatment resulted in significantly at-tenuated expression of proinflammatory cytokines reducedantigen presentation a shift from the effectormemory phe-notype to repopulation of naive lymphocytes and importantlyaugmentation in the clonal frequency of regulatory T cells(Tregs)33
A primary immune defect in patients with MS is a deficiencyin Tregs Efficacy in treating the disorder at least in partinvolves reconstitution of the immune networkrsquos regulatorycapabilities through the expansion of Tregs specificallyidentified as CD4+CD25hiFoxP3+2838 The observationsfrom this investigation suggest that anti-CD20 therapy is ca-pable of provoking a skewing or immune deviation that maybe secondary perhaps at least in part to the deletion ofCD20+CD3+ C cells thereby resulting in reduced B cellndashmediated degenerate antigen presentation of self-motifsalong with a broadening in the clonal frequency of Tregs all ofwhich may be germane to our understanding of how we canuse alemtuzumab while actively reducing (vis a vis with theapplication of a lsquowhack-a-molersquo cell depletion strategy) theincidence of secondary autoimmunity (figures 1 and 2)33
We successfully used low-dose rituximab 100 mg (50ndash75mgm2) for patients with neuromyelitis optica spectrumdisorder (NMOSD) who could not afford access to higherdoses of rituximab A 100-mg infusion depletes the CD19population of B cells to less than 2 for an average of 99 days(in essence B-cell suppression is highly titratable analogous
Figure 2 Low-dose anti-CD20 therapy post-alemtuzumab schematic illustrating a potential pilot protocol
This schematic depicts normal CD4+ and CD19+ cell reconstitution9 as well as the theoretical CD19+ reconstitution with our proposed low-dose rituximabprotocol Low-dose rituximab (eg 100 mg) is given subsequent to the detection of the precociously discordant B-cell hyperrepopulation phase of bonemarrow mononuclear cell mobilization following alemtuzumab treatment an intervention which attenuates promiscuous antigen presentation by B cellscapable of activating antindashself-humoral and cellular networks while also serving to promote a more synchronized repopulation across the bone marrowmobilization of mononuclear cell heterogeneity (ie achieving a more balanced return of B and T lymphocyte populations with the added dividend ofamplifying the clonal frequency of Tregs and observation akin to tolerance induction in patients with MS)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 7
to immunologic labetalol the latter commonly used as ahighly titratable agent for management of hypertensive crisessuch as hypertensive encephalopathy where loss of cerebro-vascular autoregulation precludes the employment of long-acting agents which could result in a protracted compromisein cerebral blood flow dynamics predisposing to a hypoxic-ischemic insult) in patients with NMOSD compared with 184days for a 1000 mg dose of rituximab41
Low-dose rituximab is a more attractive alternative to stan-dard doses of 1000 mg or 375 mgm2 First doses of ritux-imab as low as 1 mgm2 suppress B cells by 97 in healthycontrols and B cells remain suppressed to 75 of baselinelevels at 12 weeks after infusion4243
Second low-dose anti-CD20 therapy does not result in pro-longed B-cell depletion so as not to interfere with repeatcycles of alemtuzumab therapy41
Third low-dose rituximab may facilitate greater control ofB-cell repopulation and improved temporal synchronizationwith T-cell repopulation
Last reduced dosing magnitude reduces the duration of im-munosuppression compared with conventional doses of rit-uximab and may eventually be shown in evidence-basedstudies to demonstrate both safety and cost advantages if fewcomplications are identified with the low-dose regimen
A more robust clinical trial with a primary outcome of thedevelopment of secondary autoimmunity would not likelyrequire a large number of participants given the incidence rateof 40 of autoimmune thyroid disease in patients with MSwho have received alemtuzumab34 Hence we would esti-mate an incidence of 40 in the control group ofalemtuzumab-only treated patients and with an assumption ofan incidence of 10 in patients who would receive adjunctrituximab If we assign the probability of a type I error of 5and a power of 80 a trial would need approximately 80patients total (40 in each arm) accounting for drop-outs
In addition to our small sample size and an unrandomizedand unblended cohort many physicians prescribe steroidswith rituximab infusion (methylprednisolone 250 mg beforeeach and every alemtuzumab infusion in our center) to pre-vent infusion reactions It is possible that the potential positiveeffects of secondary autoimmunity prevention attributed torituximab are instead or at least in part due to steroid usageIn addition treatment may simply delay secondary autoim-munity rather than preventing it and longer periods of as-certainment will be required to assess for this prospect
An alternate explanation concerning the impact of rituximabon secondary autoimmunity is that some individuals mayrespond differently to low-dose anti-CD20 therapy due to theeffects of the FCGR3A polymorphism42 We do not know theeffect of the polymorphism on low-dose rituximab kinetics
however binding affinity may play a larger role in low-doserituximab compared with conventional doses given the lowerabsolute concentration of rituximab Such issues should becarefully considered in the design of a larger trial particularlygiven potential effects of such factors on response character-istics as well as on study cost
As the field of neurology shifts from amodel of step escalationto induction therapy for the treatment of MS strategies thatare aimed at mitigating the risks of potent disease modifyingtherapies are urgently needed43
Only through the scientific method of subjecting our hy-pothesis to the rigors of a controlled adequately blindedprospective and adequately powered clinical trial can weconfirm or refute the hypothesis-driven question can theapplication of low-dose anti-CD20 therapy temporally syn-chronized with objective confirmation of B-cell hyper-repopulation serve to adequately reduce or even preventalemtuzumab-associated secondary autoimmunity
Furthermore the addition of anti-CD20 therapy could po-tentially confer benefits on immune deviation that would exertadded efficacy in synergy with the alemtuzumab-mediatedmechanisms of action in the establishment of disease re-mission while constituting augmented and durable regulatoryproperties in keeping with those achieved during the criticalperiod that we now recognize collectively as self-tolerance
Buffeted by the broad dissemination of bone marrow mobili-zation of stem cells following alemtuzumab treatment maypromote the process of restoration and neurologic functionalreconstitution Recent evidence has demonstrated that anemerging biomarker for assessing tissue damage in the CNS ofpatients withMS the neurofilament light chain is reducedmostmarkedly following the administration of alemtuzumab whencompared with other disease-modifying therapies and that suchlevels remain reduced to the greatest magnitude over time44
It was once thought that a proposition such as repair andfunctional recovery from MS was wholly enigmatic and un-likely However we have arrived at a point in the history of ourunderstanding of the disorderrsquos pathobiology in concert withthe corresponding derangements in immune regulatory in-fluences and how to remediate them We believe our work torepresent but a single small step toward this constellation ofgoals that are so important to our deserving patients theirfamilies our community and those of us who serve on thoseteams who care for and about them
AcknowledgmentThe authors thank Mr Jason Ooi and Dr Matthew Parsonsfor their transformation and production of Elliot andTeresa Frohmanrsquos formulation of the figure 1 medicalillustration which showcases alemtuzumabrsquos mechanism ofaction the pathobiological underpinnings for treatment-associated secondary autoimmunity and the hypothetical
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
mechanisms germane to our ldquowhack-a-molerdquo B-cell de-letion strategy aimed at mitigating alemtuzumab-associatedautoimmunity in MS
Study fundingThe National Multiple Sclerosis Society 5-Year InstitutionalFellowship Training Grant Awarded to TC Frohman andEM Frohman Fellows funded E Meltzer and RA Cruz(coauthors) MS and Neuroimmunology Center The DellMedical School at The University of Texas at Austin
DisclosureE Meltzer served as a consultant for Genzyme and receivedhonoraria from Novartis S Campbell and B Ehrenfeld havenothing to disclose L Steinman is on the Editorial Boards ofthe Proceedings of the National Academy of Sciences and theJournal of Neuroimmunology He has served on the EditorialBoard of the Journal of Immunology and International Immu-nology He has served as a member of grant review committeesfor the NIH and the National MS Society He has served orserves as a consultant and received honoraria from AtaraBiotherapeutics Atreca Biogen-Idec Celgene CentocorCoherus EMD-Serono Genzyme Johnson and JohnsonNovartis RocheGenentech Teva Pharmaceuticals Incand TG Therapeutics He has served on the Data SafetyMonitoring Board for TG Therapeutics He serves on theBoard of Directors of Tolerion and Chairs the ScientificAdvisory Board for Atreca Currently L Steinman receivesresearch grant support from the NIH and Atara Bio-therapeutics MS Parsons has nothing to disclose SSZamvil is Deputy Editor ofNeurology Neuroimmunology andNeuroinflammation and is an Associate Editor for Frontiers inImmunology and Frontiers in Neurology He serves on theAdvisory Committee for the American Congress onTreatment and Research in Multiple Sclerosis (ACTRIMS)and is a standing member of the research grant reviewcommittee for the National Multiple Sclerosis Society(NMSS) He has served on the Editorial Board of theJournal of Clinical Investigation The Journal of Immunologyand The Journal of Neurological Sciences and has been acharter member of the grant review committee for the NIHClinical Neuroimmunology and Brain Tumors (CNBT)He has served or serves as a consultant and receivedhonoraria from Alexion Biogen-Idec EMD-SeronoGenzyme Novartis RocheGenentech and Teva Pharma-ceuticals Inc and has served on Data Safety MonitoringBoards for Lilly BioMS Teva and Opexa TherapeuticsCurrently SS Zamvil receives research grant support fromthe NIH NMSS Weill Institute Race to Erase MS and theMaisin Foundation TC Frohman has received advisoryboard fees from Alexion EM Frohman has receivedspeaker honoraria from Genzyme Novartis Alexion andAcorda Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationDecember 25 2019 Accepted in final form July 6 2020
References1 Coles AJ Twyman CL Arnold DL et al Alemtuzumab for patients with relapsing
multiple sclerosis after disease-modifying therapy a randomised controlled phase 3trial Lancet 20123801829ndash1839
2 Cohen JA Coles AJ Arnold DL et al Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis a randomisedcontrolled phase 3 trial Lancet 20123801819ndash1828
3 Coles AJ Cohen JA Fox EJ et al Alemtuzumab CARE-MS II 5-year follow-upNeurology 2017891117ndash1126
4 Havrdova E Arnold DL Cohen JA et al Alemtuzumab CARE-MS I 5-year follow-upNeurology 2017891107ndash1116
5 Sarvepalli D Rashid MU Ullah W Zafar Y Khan M Idiopathic thrombocytopenicpurpura a rare syndrome with alemtuzumab review of monitoring protocol Cureus201911e5715
6 Ruck T Schulte-Mecklenbeck A Pfeuffer S et al Pretreatment anti-thyroid auto-antibodies indicate increased risk for thyroid autoimmunity secondary to alemtuzu-mab a prospective cohort study EBioMedicine 201946381ndash386
Appendix Authors
Name Location Contribution
Ethan MeltzerMD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
SarahCampbell RN
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
BenjaminEhrenfeldMSW
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
Roberto ACruz MD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
LawrenceSteinman MD
Department ofNeurology StanfordUniversity School ofMedicine
Conception and criticalrevision of themanuscript forintellectual content
Matthew SParsons PhD
Division of Microbiologyand Immunology YerkesNational PrimateResearch CenterDepartment of Pathologyand Laboratory MedicineEmory University
Conception and criticalrevision of themanuscript forintellectual content
Scott S ZamvilMD PhD
Department ofNeurology amp Program inImmunology Universityof California SanFrancisco
Conception and criticalrevision of themanuscript forintellectual content
Elliot MFrohman MDPhD
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical SchoolUniversity of Texas atAustin
Conception and criticalrevision of themanuscript forintellectual content
Teresa CFrohmanMPAS MSCSPA-C FANA
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical School Universityof Texas at Austin
Conception and criticalrevision of themanuscript forintellectual content
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 9
7 Ruck T Pfeuffer S Schulte-Mecklenbeck A et al Vitiligo after alemtuzumab treat-ment secondary autoimmunity is not all about B cells Neurology 201891e2233ndashe2237
8 Zimmermann J Buhl T Muller M Alopecia universalis following alemtuzumabtreatment in multiple sclerosis a barely recognized manifestation of secondaryautoimmunity-report of a case and review of the literature Front Neurol 20178569
9 Rotondi M Molteni M Leporati P Capelli V Marino M Chiovato L Autoimmunethyroid diseases in patients treated with alemtuzumab for multiple sclerosis an ex-ample of selective anti-TSH-receptor immune response Front Endocrinol (Lau-sanne) 20178254
10 Costelloe L Jones J Coles A Secondary autoimmune diseases following alemtuzu-mab therapy for multiple sclerosis Expert Rev Neurother 201212335ndash341
11 Jones JL Phuah CL Cox AL et al IL-21 drives secondary autoimmunity in patientswith multiple sclerosis following therapeutic lymphocyte depletion with alemtuzu-mab (Campath-1H) J Clin Invest 20091192052ndash2061
12 Torino F Barnabei A Paragliola R Baldelli R Appetecchia M Corsello SM Thyroiddysfunction as an unintended side effect of anticancer drugs Thyroid 2013231345ndash1366
13 Azzopardi L Thompson SA Harding KE et al Predicting autoimmunity afteralemtuzumab treatment of multiple sclerosis J Neurol Neurosurg Psychiatry 201485795ndash798
14 Trinh T Haridas AS Sullivan TJ Ocular findings in alemtuzumab (Campath-1H)-induced thyroid eye disease Ophthalmic Plast Reconstr Surg 201632e128ndashe129
15 von Kutzleben S Pryce G Giovannoni G Baker D Depletion of CD52-positivecells inhibits the development of central nervous system autoimmune disease butdeletes an immune-tolerance promoting CD8 T-cell population Implications forsecondary autoimmunity of alemtuzumab in multiple sclerosis Immunology 2017150444ndash455
16 Wiendl H Carraro M Comi G et al Lymphocyte pharmacodynamics are not asso-ciated with autoimmunity or efficacy after alemtuzumab Neurol NeuroimmunolNeuroinflamm 201971ndash10 doi101212NXI0000000000000635
17 Kousin-Ezewu O Azzopardi L Parker RA et al Accelerated lymphocyte recoveryafter alemtuzumab does not predict multiple sclerosis activity Neurology 2014822158ndash2164
18 Jones J Thompson S Loh P et al Human autoimmunity after lymphocyte depletionis caused by homeostatic T-cell proliferation Proc Natl Acad Sci U S A 201311020200ndash20205
19 Costa DB Kobayashi SS Whacking a mole-cule clinical activity and mechanisms ofresistance to third generation EGFR inhibitors in EGFR mutated lung cancers withEGFR-T790M Transl Lung Cancer Res 20156809ndash815
20 Shin J MacCarthy T Antagonistic coevolution drives whack-a-mole sensitivity ingene regulatory networks PLoS Comput Biol 201511e1004432
21 Suzuki K Whack-a-mole strategy for multifocal ground glass opacities of the lungJ Thorac Dis 20179(suppl 3)S201ndashS207
22 Swanson DS Harrison CJ Playing Whack-a-Mole with pneumococcal serotypeeradication Pediatrics 2017140e20172034
23 Mestrovic T A microbial game of whack-a-mole clinical case series of the urethraluncloaking phenomenon caused by Corynebacterium glucuronolyticum in mentreated for Chlamydia trachomatis urethritis Infection 201947121ndash124
24 Gelfand JM Cree BAC Hauser SL Ocrelizumab and other CD20+ B-cell-depletingtherapies in multiple sclerosis Neurotherapeutics 201714835ndash841
25 Voog E Morschhauser F Solal-Celigny P Neutropenia in patients treated with rit-uximab N Engl J Med 20033482691ndash2694 discussion 2691ndash2694
26 Bar-Or A Fawaz L Fan B et al Abnormal B-cell cytokine responses a trigger of T-cell-mediated disease in MS Ann Neurol 201067452ndash461
27 Weber MS Prodrsquohomme T Patarroyo JC et al B-cell activation influences T-cellpolarization and outcome of anti-CD20 B-cell depletion in central nervous systemautoimmunity Ann Neurol 201068369ndash383
28 Monson NL Cravens P Hussain R et al Rituximab therapy reduces organ-specificT cell responses and ameliorates experimental autoimmune encephalomyelitis PLoSOne 20116e17103
29 Molnarfi N Schulze-Topphoff U Weber MS et al MHC class II-dependent B cellAPC function is required for induction of CNS autoimmunity independent of myelin-specific antibodies J Exp Med 20132102921ndash2937
30 Baker D Herrod SS Alvarez-Gonzalez C Giovannoni G Schmierer KInterpreting lymphocyte reconstitution data from the pivotal phase 3 trials of alem-tuzumab JAMA Neurol 201774961ndash969
31 Krupica T Fry TJ Mackall CL Autoimmunity during lymphopenia a two-hit modelClin Immunol 2006120121ndash128
32 Wilk EWitte TMarquardt N et al Depletion of functionally active CD20+ T cells byrituximab treatment Arthritis Rheum 2009603563ndash3571
33 Schuh E Berer K Mulazzani M et al Features of human CD3+CD20+ T cellsJ Immunol 20161971111ndash1117
34 Gingele S Kripuletz T Jacobs R Role of CD20+ T cells in multiple sclerosisimpli-cations for treatment with ocrelizumab Neural Regen Res 202015663ndash664
35 Palanichamy A Jahn S Nickles D et al Rituximab efficiently depletes increasedCD20-expressing T cells in multiple sclerosis patients J Immunol 2014193580ndash586
36 Holley JE Bremer E Kendall AC et al CD20+ inflammatory T-cells are present inblood and brain of multiple sclerosis patients and can be selectively targeted forapoptotic elimination Mult Scler Relat Disord 20143650ndash685
37 von Essen MR Ammitzboslashll C Hansen RH et al Proinflammatory CD20+ T cells inthe pathogenesis of multiple sclerosis Brain 2019142120ndash132
38 Lovett-Racke AE Gormley M Liu Y et al B cell depletion with ublituximab reshapesthe T cell profile in multiple sclerosis patients J Neuroimmunol 2019332187ndash197
39 Cross AH Stark JL Lauber J Ramsbottom MJ Lyons JA Rituximab reduces B cells andT cells in cerebrospinal fluid ofmultiple sclerosis patients J Neuroimmunol 200618063ndash70
40 Naismith RT Piccio L Lyons JA et al Rituximab add-on therapy for breakthroughrelapsing multiple sclerosis a 52-week phase II trial Neurology 2010741860ndash1867
41 Greenberg BM Graves D Remington G et al Rituximab dosing and monitoringstrategies in neuromyelitis optica patients creating strategies for therapeutic successMult Scler 2012181022ndash1026
42 Kim SH Jeong IH Hyun JW et al Treatment outcomes with rituximab in 100patients with neuromyelitis optica influence of FCGR3A polymorphisms on thetherapeutic response to rituximab JAMA Neurol 201572989ndash995
43 Steinman L Induction of new autoimmune diseases after alemtuzumab therapy formultiple sclerosis learning from adversity JAMA Neurol 201774907ndash908
44 Delcoigne B Manouchehrinia A Barro C et al Blood neurofilament light levelssegregate treatment effects in multiple sclerosis Neurology 202094e1201ndashe1212
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
DOI 101212NXI000000000000086820207 Neurol Neuroimmunol Neuroinflamm
Ethan Meltzer Sarah Campbell Benjamin Ehrenfeld et al depletion strategy
Mitigating alemtuzumab-associated autoimmunity in MS A whack-a-mole B-cell
This information is current as of August 7 2020
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

Figure 1 A model for the mitigation of secondary autoimmunity in patients with MS post-alemtuzumab
In the upper portion of the figure we illustrate alemtuzumab treatment and its effect on elimination of antindashself-lymphocytes by 2 principal mechanismsclearance through the reticular endothelial system (RES on the left) and assembly of themembrane attack complex (MAC) facilitating the passage of C9 whichcompromises cell membrane integrity thereby culminating in cytotoxicity and cell death The lower middle illustration emphasizes post-alemtuzumabtreatment-inducedmobilization of bonemarrow stem cells reconstituting the immune system B cells undergo a discordant hyperrepopulation approachingpretreatment baseline numbers 3ndash6 months following alemtuzumab treatment whereas T-cell reconstitution is considerably delayed (12ndash24 months)Hypothetically the highly discordant hyperrepopulation of B cells plays a role in the development of secondary autoimmunity Post-alemtuzumab treatmentcirculatingmononuclear cells are principally CD3+-naive T cells CD19+ CD20+-naive B cells as well as a unique population of cells that express both the B-cellantigen CD20 and the T-cell antigen CD3 These latter cells we refer to as Chimeric lymphocytes (C cells) and they are known to express proinflammatorycytokines which in the absence of adequate T-cell help can foment the production of antindashself-antibodies This can initiate corresponding autoantibody-mediated disorders such as those designated by green labels in the figure as well as to T cells capable of orchestrating cellularmechanisms of autoimmunity(designated by purple labels) To the lower left of the lower diagram one can see an enrichment in the CD3+ CD20+ C cells simultaneouswith the discordant B-cell hyperrepopulation (generally emerging approximately 3ndash6 months following alemtuzumab treatment) in the context of a deficiency in the clonalfrequency of regulatory T cells (Tregs) (ie identified as CD4+CD25hiFoxP3+) In the absence of T-cell help such B cells are rendered incapable of discriminatingbetween self and foreign epitopes to both other B cells thereby coordinating the development of antibodies as well as to T cells leading to T-cell receptormaturation with elaboration of cytokine and chemokine expression profiles commensurate to foment cellular autoimmunemechanisms The central portionof the diagram serves to illustrate the potential diversity of antibody-mediated secondary autoimmune states (green line paths) We also see activation ofT cells which can mediate secondary autoimmunity (purple line paths) and granulomatous inflammatory disease most specifically sarcoidosis Monitoringmonthly lymphocyte subsets facilitates detection of the discordant B-cell hyperrepopulation phase of bone marrow mononuclear cell mobilization afteralemtuzumab therapy and thereby provides for the discrete and temporally punctuated administration of an anti-CD20 ldquowhack-a-molerdquo strategy formitigating secondary autoimmunity Specifically we administered low-dose rituximab to orchestrate the deletionof bothCD20+B cells in conjunctionwith theCD20+CD3+ C cells along with their B-cell activation capabilities via the elaboration of proinflammatory cytokine and chemokine cascades The net effect isseen approximately 4months later (in the upper circle on the right lower side of the diagram) when there is amarked diminution of both effectormemory Bcells and autoimmunity-inducing C cells with a corresponding expansion in the clonal frequency of Tregs
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
keeping with this observation anti-CD20 therapy appears toexert no impact on CSF antibody indices such as oligoclonalbanding increased immuno gamma globulin (IgG) indexandor an elevation in IgG synthesis rates characteristic ab-normalities identified in approximately 90 of patients withMS when using isoelectric focusing techniques Alternatelythe peripheral loss of B cells does correspond to a markedreduction in the development of both T1 gadolinium-enhancing and combined unique MS plaque lesions3839
In a recent study the third-generation glycoengineered chi-meric anti-CD20 therapy ublituximab was shown to reduceboth effector and memory CD8 T-cell populations while alsoaugmenting the clonal frequency of naive CD8+ T cells38 Oneof the most conspicuous observations was the identification ofa population of lymphocytes with cell surface expression ofboth CD20+ and CD3+ (those designated as chimeric or Ccells in our hypothetical model figure 1) with further char-acterization revealing that such cells exhibit features inkeeping with memory CD8+ T cells40
The functionally chimeric lymphocytes produce proin-flammatory mediators which may play a key role in thepromiscuous antigen presentation of self-motifs during thediscordant hyperrepopulation of B cells following alemtuzu-mab treatment (figure 1) Lovett-Racke et al categoricallycharacterized both the cellular identification and cytokinechemokine expression profiles using flow cytometric tech-niques from 47 patients withMS treated with ublituximab and
confirmed that such treatment resulted in significantly at-tenuated expression of proinflammatory cytokines reducedantigen presentation a shift from the effectormemory phe-notype to repopulation of naive lymphocytes and importantlyaugmentation in the clonal frequency of regulatory T cells(Tregs)33
A primary immune defect in patients with MS is a deficiencyin Tregs Efficacy in treating the disorder at least in partinvolves reconstitution of the immune networkrsquos regulatorycapabilities through the expansion of Tregs specificallyidentified as CD4+CD25hiFoxP3+2838 The observationsfrom this investigation suggest that anti-CD20 therapy is ca-pable of provoking a skewing or immune deviation that maybe secondary perhaps at least in part to the deletion ofCD20+CD3+ C cells thereby resulting in reduced B cellndashmediated degenerate antigen presentation of self-motifsalong with a broadening in the clonal frequency of Tregs all ofwhich may be germane to our understanding of how we canuse alemtuzumab while actively reducing (vis a vis with theapplication of a lsquowhack-a-molersquo cell depletion strategy) theincidence of secondary autoimmunity (figures 1 and 2)33
We successfully used low-dose rituximab 100 mg (50ndash75mgm2) for patients with neuromyelitis optica spectrumdisorder (NMOSD) who could not afford access to higherdoses of rituximab A 100-mg infusion depletes the CD19population of B cells to less than 2 for an average of 99 days(in essence B-cell suppression is highly titratable analogous
Figure 2 Low-dose anti-CD20 therapy post-alemtuzumab schematic illustrating a potential pilot protocol
This schematic depicts normal CD4+ and CD19+ cell reconstitution9 as well as the theoretical CD19+ reconstitution with our proposed low-dose rituximabprotocol Low-dose rituximab (eg 100 mg) is given subsequent to the detection of the precociously discordant B-cell hyperrepopulation phase of bonemarrow mononuclear cell mobilization following alemtuzumab treatment an intervention which attenuates promiscuous antigen presentation by B cellscapable of activating antindashself-humoral and cellular networks while also serving to promote a more synchronized repopulation across the bone marrowmobilization of mononuclear cell heterogeneity (ie achieving a more balanced return of B and T lymphocyte populations with the added dividend ofamplifying the clonal frequency of Tregs and observation akin to tolerance induction in patients with MS)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 7
to immunologic labetalol the latter commonly used as ahighly titratable agent for management of hypertensive crisessuch as hypertensive encephalopathy where loss of cerebro-vascular autoregulation precludes the employment of long-acting agents which could result in a protracted compromisein cerebral blood flow dynamics predisposing to a hypoxic-ischemic insult) in patients with NMOSD compared with 184days for a 1000 mg dose of rituximab41
Low-dose rituximab is a more attractive alternative to stan-dard doses of 1000 mg or 375 mgm2 First doses of ritux-imab as low as 1 mgm2 suppress B cells by 97 in healthycontrols and B cells remain suppressed to 75 of baselinelevels at 12 weeks after infusion4243
Second low-dose anti-CD20 therapy does not result in pro-longed B-cell depletion so as not to interfere with repeatcycles of alemtuzumab therapy41
Third low-dose rituximab may facilitate greater control ofB-cell repopulation and improved temporal synchronizationwith T-cell repopulation
Last reduced dosing magnitude reduces the duration of im-munosuppression compared with conventional doses of rit-uximab and may eventually be shown in evidence-basedstudies to demonstrate both safety and cost advantages if fewcomplications are identified with the low-dose regimen
A more robust clinical trial with a primary outcome of thedevelopment of secondary autoimmunity would not likelyrequire a large number of participants given the incidence rateof 40 of autoimmune thyroid disease in patients with MSwho have received alemtuzumab34 Hence we would esti-mate an incidence of 40 in the control group ofalemtuzumab-only treated patients and with an assumption ofan incidence of 10 in patients who would receive adjunctrituximab If we assign the probability of a type I error of 5and a power of 80 a trial would need approximately 80patients total (40 in each arm) accounting for drop-outs
In addition to our small sample size and an unrandomizedand unblended cohort many physicians prescribe steroidswith rituximab infusion (methylprednisolone 250 mg beforeeach and every alemtuzumab infusion in our center) to pre-vent infusion reactions It is possible that the potential positiveeffects of secondary autoimmunity prevention attributed torituximab are instead or at least in part due to steroid usageIn addition treatment may simply delay secondary autoim-munity rather than preventing it and longer periods of as-certainment will be required to assess for this prospect
An alternate explanation concerning the impact of rituximabon secondary autoimmunity is that some individuals mayrespond differently to low-dose anti-CD20 therapy due to theeffects of the FCGR3A polymorphism42 We do not know theeffect of the polymorphism on low-dose rituximab kinetics
however binding affinity may play a larger role in low-doserituximab compared with conventional doses given the lowerabsolute concentration of rituximab Such issues should becarefully considered in the design of a larger trial particularlygiven potential effects of such factors on response character-istics as well as on study cost
As the field of neurology shifts from amodel of step escalationto induction therapy for the treatment of MS strategies thatare aimed at mitigating the risks of potent disease modifyingtherapies are urgently needed43
Only through the scientific method of subjecting our hy-pothesis to the rigors of a controlled adequately blindedprospective and adequately powered clinical trial can weconfirm or refute the hypothesis-driven question can theapplication of low-dose anti-CD20 therapy temporally syn-chronized with objective confirmation of B-cell hyper-repopulation serve to adequately reduce or even preventalemtuzumab-associated secondary autoimmunity
Furthermore the addition of anti-CD20 therapy could po-tentially confer benefits on immune deviation that would exertadded efficacy in synergy with the alemtuzumab-mediatedmechanisms of action in the establishment of disease re-mission while constituting augmented and durable regulatoryproperties in keeping with those achieved during the criticalperiod that we now recognize collectively as self-tolerance
Buffeted by the broad dissemination of bone marrow mobili-zation of stem cells following alemtuzumab treatment maypromote the process of restoration and neurologic functionalreconstitution Recent evidence has demonstrated that anemerging biomarker for assessing tissue damage in the CNS ofpatients withMS the neurofilament light chain is reducedmostmarkedly following the administration of alemtuzumab whencompared with other disease-modifying therapies and that suchlevels remain reduced to the greatest magnitude over time44
It was once thought that a proposition such as repair andfunctional recovery from MS was wholly enigmatic and un-likely However we have arrived at a point in the history of ourunderstanding of the disorderrsquos pathobiology in concert withthe corresponding derangements in immune regulatory in-fluences and how to remediate them We believe our work torepresent but a single small step toward this constellation ofgoals that are so important to our deserving patients theirfamilies our community and those of us who serve on thoseteams who care for and about them
AcknowledgmentThe authors thank Mr Jason Ooi and Dr Matthew Parsonsfor their transformation and production of Elliot andTeresa Frohmanrsquos formulation of the figure 1 medicalillustration which showcases alemtuzumabrsquos mechanism ofaction the pathobiological underpinnings for treatment-associated secondary autoimmunity and the hypothetical
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
mechanisms germane to our ldquowhack-a-molerdquo B-cell de-letion strategy aimed at mitigating alemtuzumab-associatedautoimmunity in MS
Study fundingThe National Multiple Sclerosis Society 5-Year InstitutionalFellowship Training Grant Awarded to TC Frohman andEM Frohman Fellows funded E Meltzer and RA Cruz(coauthors) MS and Neuroimmunology Center The DellMedical School at The University of Texas at Austin
DisclosureE Meltzer served as a consultant for Genzyme and receivedhonoraria from Novartis S Campbell and B Ehrenfeld havenothing to disclose L Steinman is on the Editorial Boards ofthe Proceedings of the National Academy of Sciences and theJournal of Neuroimmunology He has served on the EditorialBoard of the Journal of Immunology and International Immu-nology He has served as a member of grant review committeesfor the NIH and the National MS Society He has served orserves as a consultant and received honoraria from AtaraBiotherapeutics Atreca Biogen-Idec Celgene CentocorCoherus EMD-Serono Genzyme Johnson and JohnsonNovartis RocheGenentech Teva Pharmaceuticals Incand TG Therapeutics He has served on the Data SafetyMonitoring Board for TG Therapeutics He serves on theBoard of Directors of Tolerion and Chairs the ScientificAdvisory Board for Atreca Currently L Steinman receivesresearch grant support from the NIH and Atara Bio-therapeutics MS Parsons has nothing to disclose SSZamvil is Deputy Editor ofNeurology Neuroimmunology andNeuroinflammation and is an Associate Editor for Frontiers inImmunology and Frontiers in Neurology He serves on theAdvisory Committee for the American Congress onTreatment and Research in Multiple Sclerosis (ACTRIMS)and is a standing member of the research grant reviewcommittee for the National Multiple Sclerosis Society(NMSS) He has served on the Editorial Board of theJournal of Clinical Investigation The Journal of Immunologyand The Journal of Neurological Sciences and has been acharter member of the grant review committee for the NIHClinical Neuroimmunology and Brain Tumors (CNBT)He has served or serves as a consultant and receivedhonoraria from Alexion Biogen-Idec EMD-SeronoGenzyme Novartis RocheGenentech and Teva Pharma-ceuticals Inc and has served on Data Safety MonitoringBoards for Lilly BioMS Teva and Opexa TherapeuticsCurrently SS Zamvil receives research grant support fromthe NIH NMSS Weill Institute Race to Erase MS and theMaisin Foundation TC Frohman has received advisoryboard fees from Alexion EM Frohman has receivedspeaker honoraria from Genzyme Novartis Alexion andAcorda Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationDecember 25 2019 Accepted in final form July 6 2020
References1 Coles AJ Twyman CL Arnold DL et al Alemtuzumab for patients with relapsing
multiple sclerosis after disease-modifying therapy a randomised controlled phase 3trial Lancet 20123801829ndash1839
2 Cohen JA Coles AJ Arnold DL et al Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis a randomisedcontrolled phase 3 trial Lancet 20123801819ndash1828
3 Coles AJ Cohen JA Fox EJ et al Alemtuzumab CARE-MS II 5-year follow-upNeurology 2017891117ndash1126
4 Havrdova E Arnold DL Cohen JA et al Alemtuzumab CARE-MS I 5-year follow-upNeurology 2017891107ndash1116
5 Sarvepalli D Rashid MU Ullah W Zafar Y Khan M Idiopathic thrombocytopenicpurpura a rare syndrome with alemtuzumab review of monitoring protocol Cureus201911e5715
6 Ruck T Schulte-Mecklenbeck A Pfeuffer S et al Pretreatment anti-thyroid auto-antibodies indicate increased risk for thyroid autoimmunity secondary to alemtuzu-mab a prospective cohort study EBioMedicine 201946381ndash386
Appendix Authors
Name Location Contribution
Ethan MeltzerMD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
SarahCampbell RN
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
BenjaminEhrenfeldMSW
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
Roberto ACruz MD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
LawrenceSteinman MD
Department ofNeurology StanfordUniversity School ofMedicine
Conception and criticalrevision of themanuscript forintellectual content
Matthew SParsons PhD
Division of Microbiologyand Immunology YerkesNational PrimateResearch CenterDepartment of Pathologyand Laboratory MedicineEmory University
Conception and criticalrevision of themanuscript forintellectual content
Scott S ZamvilMD PhD
Department ofNeurology amp Program inImmunology Universityof California SanFrancisco
Conception and criticalrevision of themanuscript forintellectual content
Elliot MFrohman MDPhD
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical SchoolUniversity of Texas atAustin
Conception and criticalrevision of themanuscript forintellectual content
Teresa CFrohmanMPAS MSCSPA-C FANA
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical School Universityof Texas at Austin
Conception and criticalrevision of themanuscript forintellectual content
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 9
7 Ruck T Pfeuffer S Schulte-Mecklenbeck A et al Vitiligo after alemtuzumab treat-ment secondary autoimmunity is not all about B cells Neurology 201891e2233ndashe2237
8 Zimmermann J Buhl T Muller M Alopecia universalis following alemtuzumabtreatment in multiple sclerosis a barely recognized manifestation of secondaryautoimmunity-report of a case and review of the literature Front Neurol 20178569
9 Rotondi M Molteni M Leporati P Capelli V Marino M Chiovato L Autoimmunethyroid diseases in patients treated with alemtuzumab for multiple sclerosis an ex-ample of selective anti-TSH-receptor immune response Front Endocrinol (Lau-sanne) 20178254
10 Costelloe L Jones J Coles A Secondary autoimmune diseases following alemtuzu-mab therapy for multiple sclerosis Expert Rev Neurother 201212335ndash341
11 Jones JL Phuah CL Cox AL et al IL-21 drives secondary autoimmunity in patientswith multiple sclerosis following therapeutic lymphocyte depletion with alemtuzu-mab (Campath-1H) J Clin Invest 20091192052ndash2061
12 Torino F Barnabei A Paragliola R Baldelli R Appetecchia M Corsello SM Thyroiddysfunction as an unintended side effect of anticancer drugs Thyroid 2013231345ndash1366
13 Azzopardi L Thompson SA Harding KE et al Predicting autoimmunity afteralemtuzumab treatment of multiple sclerosis J Neurol Neurosurg Psychiatry 201485795ndash798
14 Trinh T Haridas AS Sullivan TJ Ocular findings in alemtuzumab (Campath-1H)-induced thyroid eye disease Ophthalmic Plast Reconstr Surg 201632e128ndashe129
15 von Kutzleben S Pryce G Giovannoni G Baker D Depletion of CD52-positivecells inhibits the development of central nervous system autoimmune disease butdeletes an immune-tolerance promoting CD8 T-cell population Implications forsecondary autoimmunity of alemtuzumab in multiple sclerosis Immunology 2017150444ndash455
16 Wiendl H Carraro M Comi G et al Lymphocyte pharmacodynamics are not asso-ciated with autoimmunity or efficacy after alemtuzumab Neurol NeuroimmunolNeuroinflamm 201971ndash10 doi101212NXI0000000000000635
17 Kousin-Ezewu O Azzopardi L Parker RA et al Accelerated lymphocyte recoveryafter alemtuzumab does not predict multiple sclerosis activity Neurology 2014822158ndash2164
18 Jones J Thompson S Loh P et al Human autoimmunity after lymphocyte depletionis caused by homeostatic T-cell proliferation Proc Natl Acad Sci U S A 201311020200ndash20205
19 Costa DB Kobayashi SS Whacking a mole-cule clinical activity and mechanisms ofresistance to third generation EGFR inhibitors in EGFR mutated lung cancers withEGFR-T790M Transl Lung Cancer Res 20156809ndash815
20 Shin J MacCarthy T Antagonistic coevolution drives whack-a-mole sensitivity ingene regulatory networks PLoS Comput Biol 201511e1004432
21 Suzuki K Whack-a-mole strategy for multifocal ground glass opacities of the lungJ Thorac Dis 20179(suppl 3)S201ndashS207
22 Swanson DS Harrison CJ Playing Whack-a-Mole with pneumococcal serotypeeradication Pediatrics 2017140e20172034
23 Mestrovic T A microbial game of whack-a-mole clinical case series of the urethraluncloaking phenomenon caused by Corynebacterium glucuronolyticum in mentreated for Chlamydia trachomatis urethritis Infection 201947121ndash124
24 Gelfand JM Cree BAC Hauser SL Ocrelizumab and other CD20+ B-cell-depletingtherapies in multiple sclerosis Neurotherapeutics 201714835ndash841
25 Voog E Morschhauser F Solal-Celigny P Neutropenia in patients treated with rit-uximab N Engl J Med 20033482691ndash2694 discussion 2691ndash2694
26 Bar-Or A Fawaz L Fan B et al Abnormal B-cell cytokine responses a trigger of T-cell-mediated disease in MS Ann Neurol 201067452ndash461
27 Weber MS Prodrsquohomme T Patarroyo JC et al B-cell activation influences T-cellpolarization and outcome of anti-CD20 B-cell depletion in central nervous systemautoimmunity Ann Neurol 201068369ndash383
28 Monson NL Cravens P Hussain R et al Rituximab therapy reduces organ-specificT cell responses and ameliorates experimental autoimmune encephalomyelitis PLoSOne 20116e17103
29 Molnarfi N Schulze-Topphoff U Weber MS et al MHC class II-dependent B cellAPC function is required for induction of CNS autoimmunity independent of myelin-specific antibodies J Exp Med 20132102921ndash2937
30 Baker D Herrod SS Alvarez-Gonzalez C Giovannoni G Schmierer KInterpreting lymphocyte reconstitution data from the pivotal phase 3 trials of alem-tuzumab JAMA Neurol 201774961ndash969
31 Krupica T Fry TJ Mackall CL Autoimmunity during lymphopenia a two-hit modelClin Immunol 2006120121ndash128
32 Wilk EWitte TMarquardt N et al Depletion of functionally active CD20+ T cells byrituximab treatment Arthritis Rheum 2009603563ndash3571
33 Schuh E Berer K Mulazzani M et al Features of human CD3+CD20+ T cellsJ Immunol 20161971111ndash1117
34 Gingele S Kripuletz T Jacobs R Role of CD20+ T cells in multiple sclerosisimpli-cations for treatment with ocrelizumab Neural Regen Res 202015663ndash664
35 Palanichamy A Jahn S Nickles D et al Rituximab efficiently depletes increasedCD20-expressing T cells in multiple sclerosis patients J Immunol 2014193580ndash586
36 Holley JE Bremer E Kendall AC et al CD20+ inflammatory T-cells are present inblood and brain of multiple sclerosis patients and can be selectively targeted forapoptotic elimination Mult Scler Relat Disord 20143650ndash685
37 von Essen MR Ammitzboslashll C Hansen RH et al Proinflammatory CD20+ T cells inthe pathogenesis of multiple sclerosis Brain 2019142120ndash132
38 Lovett-Racke AE Gormley M Liu Y et al B cell depletion with ublituximab reshapesthe T cell profile in multiple sclerosis patients J Neuroimmunol 2019332187ndash197
39 Cross AH Stark JL Lauber J Ramsbottom MJ Lyons JA Rituximab reduces B cells andT cells in cerebrospinal fluid ofmultiple sclerosis patients J Neuroimmunol 200618063ndash70
40 Naismith RT Piccio L Lyons JA et al Rituximab add-on therapy for breakthroughrelapsing multiple sclerosis a 52-week phase II trial Neurology 2010741860ndash1867
41 Greenberg BM Graves D Remington G et al Rituximab dosing and monitoringstrategies in neuromyelitis optica patients creating strategies for therapeutic successMult Scler 2012181022ndash1026
42 Kim SH Jeong IH Hyun JW et al Treatment outcomes with rituximab in 100patients with neuromyelitis optica influence of FCGR3A polymorphisms on thetherapeutic response to rituximab JAMA Neurol 201572989ndash995
43 Steinman L Induction of new autoimmune diseases after alemtuzumab therapy formultiple sclerosis learning from adversity JAMA Neurol 201774907ndash908
44 Delcoigne B Manouchehrinia A Barro C et al Blood neurofilament light levelssegregate treatment effects in multiple sclerosis Neurology 202094e1201ndashe1212
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
DOI 101212NXI000000000000086820207 Neurol Neuroimmunol Neuroinflamm
Ethan Meltzer Sarah Campbell Benjamin Ehrenfeld et al depletion strategy
Mitigating alemtuzumab-associated autoimmunity in MS A whack-a-mole B-cell
This information is current as of August 7 2020
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

keeping with this observation anti-CD20 therapy appears toexert no impact on CSF antibody indices such as oligoclonalbanding increased immuno gamma globulin (IgG) indexandor an elevation in IgG synthesis rates characteristic ab-normalities identified in approximately 90 of patients withMS when using isoelectric focusing techniques Alternatelythe peripheral loss of B cells does correspond to a markedreduction in the development of both T1 gadolinium-enhancing and combined unique MS plaque lesions3839
In a recent study the third-generation glycoengineered chi-meric anti-CD20 therapy ublituximab was shown to reduceboth effector and memory CD8 T-cell populations while alsoaugmenting the clonal frequency of naive CD8+ T cells38 Oneof the most conspicuous observations was the identification ofa population of lymphocytes with cell surface expression ofboth CD20+ and CD3+ (those designated as chimeric or Ccells in our hypothetical model figure 1) with further char-acterization revealing that such cells exhibit features inkeeping with memory CD8+ T cells40
The functionally chimeric lymphocytes produce proin-flammatory mediators which may play a key role in thepromiscuous antigen presentation of self-motifs during thediscordant hyperrepopulation of B cells following alemtuzu-mab treatment (figure 1) Lovett-Racke et al categoricallycharacterized both the cellular identification and cytokinechemokine expression profiles using flow cytometric tech-niques from 47 patients withMS treated with ublituximab and
confirmed that such treatment resulted in significantly at-tenuated expression of proinflammatory cytokines reducedantigen presentation a shift from the effectormemory phe-notype to repopulation of naive lymphocytes and importantlyaugmentation in the clonal frequency of regulatory T cells(Tregs)33
A primary immune defect in patients with MS is a deficiencyin Tregs Efficacy in treating the disorder at least in partinvolves reconstitution of the immune networkrsquos regulatorycapabilities through the expansion of Tregs specificallyidentified as CD4+CD25hiFoxP3+2838 The observationsfrom this investigation suggest that anti-CD20 therapy is ca-pable of provoking a skewing or immune deviation that maybe secondary perhaps at least in part to the deletion ofCD20+CD3+ C cells thereby resulting in reduced B cellndashmediated degenerate antigen presentation of self-motifsalong with a broadening in the clonal frequency of Tregs all ofwhich may be germane to our understanding of how we canuse alemtuzumab while actively reducing (vis a vis with theapplication of a lsquowhack-a-molersquo cell depletion strategy) theincidence of secondary autoimmunity (figures 1 and 2)33
We successfully used low-dose rituximab 100 mg (50ndash75mgm2) for patients with neuromyelitis optica spectrumdisorder (NMOSD) who could not afford access to higherdoses of rituximab A 100-mg infusion depletes the CD19population of B cells to less than 2 for an average of 99 days(in essence B-cell suppression is highly titratable analogous
Figure 2 Low-dose anti-CD20 therapy post-alemtuzumab schematic illustrating a potential pilot protocol
This schematic depicts normal CD4+ and CD19+ cell reconstitution9 as well as the theoretical CD19+ reconstitution with our proposed low-dose rituximabprotocol Low-dose rituximab (eg 100 mg) is given subsequent to the detection of the precociously discordant B-cell hyperrepopulation phase of bonemarrow mononuclear cell mobilization following alemtuzumab treatment an intervention which attenuates promiscuous antigen presentation by B cellscapable of activating antindashself-humoral and cellular networks while also serving to promote a more synchronized repopulation across the bone marrowmobilization of mononuclear cell heterogeneity (ie achieving a more balanced return of B and T lymphocyte populations with the added dividend ofamplifying the clonal frequency of Tregs and observation akin to tolerance induction in patients with MS)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 7
to immunologic labetalol the latter commonly used as ahighly titratable agent for management of hypertensive crisessuch as hypertensive encephalopathy where loss of cerebro-vascular autoregulation precludes the employment of long-acting agents which could result in a protracted compromisein cerebral blood flow dynamics predisposing to a hypoxic-ischemic insult) in patients with NMOSD compared with 184days for a 1000 mg dose of rituximab41
Low-dose rituximab is a more attractive alternative to stan-dard doses of 1000 mg or 375 mgm2 First doses of ritux-imab as low as 1 mgm2 suppress B cells by 97 in healthycontrols and B cells remain suppressed to 75 of baselinelevels at 12 weeks after infusion4243
Second low-dose anti-CD20 therapy does not result in pro-longed B-cell depletion so as not to interfere with repeatcycles of alemtuzumab therapy41
Third low-dose rituximab may facilitate greater control ofB-cell repopulation and improved temporal synchronizationwith T-cell repopulation
Last reduced dosing magnitude reduces the duration of im-munosuppression compared with conventional doses of rit-uximab and may eventually be shown in evidence-basedstudies to demonstrate both safety and cost advantages if fewcomplications are identified with the low-dose regimen
A more robust clinical trial with a primary outcome of thedevelopment of secondary autoimmunity would not likelyrequire a large number of participants given the incidence rateof 40 of autoimmune thyroid disease in patients with MSwho have received alemtuzumab34 Hence we would esti-mate an incidence of 40 in the control group ofalemtuzumab-only treated patients and with an assumption ofan incidence of 10 in patients who would receive adjunctrituximab If we assign the probability of a type I error of 5and a power of 80 a trial would need approximately 80patients total (40 in each arm) accounting for drop-outs
In addition to our small sample size and an unrandomizedand unblended cohort many physicians prescribe steroidswith rituximab infusion (methylprednisolone 250 mg beforeeach and every alemtuzumab infusion in our center) to pre-vent infusion reactions It is possible that the potential positiveeffects of secondary autoimmunity prevention attributed torituximab are instead or at least in part due to steroid usageIn addition treatment may simply delay secondary autoim-munity rather than preventing it and longer periods of as-certainment will be required to assess for this prospect
An alternate explanation concerning the impact of rituximabon secondary autoimmunity is that some individuals mayrespond differently to low-dose anti-CD20 therapy due to theeffects of the FCGR3A polymorphism42 We do not know theeffect of the polymorphism on low-dose rituximab kinetics
however binding affinity may play a larger role in low-doserituximab compared with conventional doses given the lowerabsolute concentration of rituximab Such issues should becarefully considered in the design of a larger trial particularlygiven potential effects of such factors on response character-istics as well as on study cost
As the field of neurology shifts from amodel of step escalationto induction therapy for the treatment of MS strategies thatare aimed at mitigating the risks of potent disease modifyingtherapies are urgently needed43
Only through the scientific method of subjecting our hy-pothesis to the rigors of a controlled adequately blindedprospective and adequately powered clinical trial can weconfirm or refute the hypothesis-driven question can theapplication of low-dose anti-CD20 therapy temporally syn-chronized with objective confirmation of B-cell hyper-repopulation serve to adequately reduce or even preventalemtuzumab-associated secondary autoimmunity
Furthermore the addition of anti-CD20 therapy could po-tentially confer benefits on immune deviation that would exertadded efficacy in synergy with the alemtuzumab-mediatedmechanisms of action in the establishment of disease re-mission while constituting augmented and durable regulatoryproperties in keeping with those achieved during the criticalperiod that we now recognize collectively as self-tolerance
Buffeted by the broad dissemination of bone marrow mobili-zation of stem cells following alemtuzumab treatment maypromote the process of restoration and neurologic functionalreconstitution Recent evidence has demonstrated that anemerging biomarker for assessing tissue damage in the CNS ofpatients withMS the neurofilament light chain is reducedmostmarkedly following the administration of alemtuzumab whencompared with other disease-modifying therapies and that suchlevels remain reduced to the greatest magnitude over time44
It was once thought that a proposition such as repair andfunctional recovery from MS was wholly enigmatic and un-likely However we have arrived at a point in the history of ourunderstanding of the disorderrsquos pathobiology in concert withthe corresponding derangements in immune regulatory in-fluences and how to remediate them We believe our work torepresent but a single small step toward this constellation ofgoals that are so important to our deserving patients theirfamilies our community and those of us who serve on thoseteams who care for and about them
AcknowledgmentThe authors thank Mr Jason Ooi and Dr Matthew Parsonsfor their transformation and production of Elliot andTeresa Frohmanrsquos formulation of the figure 1 medicalillustration which showcases alemtuzumabrsquos mechanism ofaction the pathobiological underpinnings for treatment-associated secondary autoimmunity and the hypothetical
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
mechanisms germane to our ldquowhack-a-molerdquo B-cell de-letion strategy aimed at mitigating alemtuzumab-associatedautoimmunity in MS
Study fundingThe National Multiple Sclerosis Society 5-Year InstitutionalFellowship Training Grant Awarded to TC Frohman andEM Frohman Fellows funded E Meltzer and RA Cruz(coauthors) MS and Neuroimmunology Center The DellMedical School at The University of Texas at Austin
DisclosureE Meltzer served as a consultant for Genzyme and receivedhonoraria from Novartis S Campbell and B Ehrenfeld havenothing to disclose L Steinman is on the Editorial Boards ofthe Proceedings of the National Academy of Sciences and theJournal of Neuroimmunology He has served on the EditorialBoard of the Journal of Immunology and International Immu-nology He has served as a member of grant review committeesfor the NIH and the National MS Society He has served orserves as a consultant and received honoraria from AtaraBiotherapeutics Atreca Biogen-Idec Celgene CentocorCoherus EMD-Serono Genzyme Johnson and JohnsonNovartis RocheGenentech Teva Pharmaceuticals Incand TG Therapeutics He has served on the Data SafetyMonitoring Board for TG Therapeutics He serves on theBoard of Directors of Tolerion and Chairs the ScientificAdvisory Board for Atreca Currently L Steinman receivesresearch grant support from the NIH and Atara Bio-therapeutics MS Parsons has nothing to disclose SSZamvil is Deputy Editor ofNeurology Neuroimmunology andNeuroinflammation and is an Associate Editor for Frontiers inImmunology and Frontiers in Neurology He serves on theAdvisory Committee for the American Congress onTreatment and Research in Multiple Sclerosis (ACTRIMS)and is a standing member of the research grant reviewcommittee for the National Multiple Sclerosis Society(NMSS) He has served on the Editorial Board of theJournal of Clinical Investigation The Journal of Immunologyand The Journal of Neurological Sciences and has been acharter member of the grant review committee for the NIHClinical Neuroimmunology and Brain Tumors (CNBT)He has served or serves as a consultant and receivedhonoraria from Alexion Biogen-Idec EMD-SeronoGenzyme Novartis RocheGenentech and Teva Pharma-ceuticals Inc and has served on Data Safety MonitoringBoards for Lilly BioMS Teva and Opexa TherapeuticsCurrently SS Zamvil receives research grant support fromthe NIH NMSS Weill Institute Race to Erase MS and theMaisin Foundation TC Frohman has received advisoryboard fees from Alexion EM Frohman has receivedspeaker honoraria from Genzyme Novartis Alexion andAcorda Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationDecember 25 2019 Accepted in final form July 6 2020
References1 Coles AJ Twyman CL Arnold DL et al Alemtuzumab for patients with relapsing
multiple sclerosis after disease-modifying therapy a randomised controlled phase 3trial Lancet 20123801829ndash1839
2 Cohen JA Coles AJ Arnold DL et al Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis a randomisedcontrolled phase 3 trial Lancet 20123801819ndash1828
3 Coles AJ Cohen JA Fox EJ et al Alemtuzumab CARE-MS II 5-year follow-upNeurology 2017891117ndash1126
4 Havrdova E Arnold DL Cohen JA et al Alemtuzumab CARE-MS I 5-year follow-upNeurology 2017891107ndash1116
5 Sarvepalli D Rashid MU Ullah W Zafar Y Khan M Idiopathic thrombocytopenicpurpura a rare syndrome with alemtuzumab review of monitoring protocol Cureus201911e5715
6 Ruck T Schulte-Mecklenbeck A Pfeuffer S et al Pretreatment anti-thyroid auto-antibodies indicate increased risk for thyroid autoimmunity secondary to alemtuzu-mab a prospective cohort study EBioMedicine 201946381ndash386
Appendix Authors
Name Location Contribution
Ethan MeltzerMD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
SarahCampbell RN
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
BenjaminEhrenfeldMSW
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
Roberto ACruz MD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
LawrenceSteinman MD
Department ofNeurology StanfordUniversity School ofMedicine
Conception and criticalrevision of themanuscript forintellectual content
Matthew SParsons PhD
Division of Microbiologyand Immunology YerkesNational PrimateResearch CenterDepartment of Pathologyand Laboratory MedicineEmory University
Conception and criticalrevision of themanuscript forintellectual content
Scott S ZamvilMD PhD
Department ofNeurology amp Program inImmunology Universityof California SanFrancisco
Conception and criticalrevision of themanuscript forintellectual content
Elliot MFrohman MDPhD
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical SchoolUniversity of Texas atAustin
Conception and criticalrevision of themanuscript forintellectual content
Teresa CFrohmanMPAS MSCSPA-C FANA
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical School Universityof Texas at Austin
Conception and criticalrevision of themanuscript forintellectual content
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 9
7 Ruck T Pfeuffer S Schulte-Mecklenbeck A et al Vitiligo after alemtuzumab treat-ment secondary autoimmunity is not all about B cells Neurology 201891e2233ndashe2237
8 Zimmermann J Buhl T Muller M Alopecia universalis following alemtuzumabtreatment in multiple sclerosis a barely recognized manifestation of secondaryautoimmunity-report of a case and review of the literature Front Neurol 20178569
9 Rotondi M Molteni M Leporati P Capelli V Marino M Chiovato L Autoimmunethyroid diseases in patients treated with alemtuzumab for multiple sclerosis an ex-ample of selective anti-TSH-receptor immune response Front Endocrinol (Lau-sanne) 20178254
10 Costelloe L Jones J Coles A Secondary autoimmune diseases following alemtuzu-mab therapy for multiple sclerosis Expert Rev Neurother 201212335ndash341
11 Jones JL Phuah CL Cox AL et al IL-21 drives secondary autoimmunity in patientswith multiple sclerosis following therapeutic lymphocyte depletion with alemtuzu-mab (Campath-1H) J Clin Invest 20091192052ndash2061
12 Torino F Barnabei A Paragliola R Baldelli R Appetecchia M Corsello SM Thyroiddysfunction as an unintended side effect of anticancer drugs Thyroid 2013231345ndash1366
13 Azzopardi L Thompson SA Harding KE et al Predicting autoimmunity afteralemtuzumab treatment of multiple sclerosis J Neurol Neurosurg Psychiatry 201485795ndash798
14 Trinh T Haridas AS Sullivan TJ Ocular findings in alemtuzumab (Campath-1H)-induced thyroid eye disease Ophthalmic Plast Reconstr Surg 201632e128ndashe129
15 von Kutzleben S Pryce G Giovannoni G Baker D Depletion of CD52-positivecells inhibits the development of central nervous system autoimmune disease butdeletes an immune-tolerance promoting CD8 T-cell population Implications forsecondary autoimmunity of alemtuzumab in multiple sclerosis Immunology 2017150444ndash455
16 Wiendl H Carraro M Comi G et al Lymphocyte pharmacodynamics are not asso-ciated with autoimmunity or efficacy after alemtuzumab Neurol NeuroimmunolNeuroinflamm 201971ndash10 doi101212NXI0000000000000635
17 Kousin-Ezewu O Azzopardi L Parker RA et al Accelerated lymphocyte recoveryafter alemtuzumab does not predict multiple sclerosis activity Neurology 2014822158ndash2164
18 Jones J Thompson S Loh P et al Human autoimmunity after lymphocyte depletionis caused by homeostatic T-cell proliferation Proc Natl Acad Sci U S A 201311020200ndash20205
19 Costa DB Kobayashi SS Whacking a mole-cule clinical activity and mechanisms ofresistance to third generation EGFR inhibitors in EGFR mutated lung cancers withEGFR-T790M Transl Lung Cancer Res 20156809ndash815
20 Shin J MacCarthy T Antagonistic coevolution drives whack-a-mole sensitivity ingene regulatory networks PLoS Comput Biol 201511e1004432
21 Suzuki K Whack-a-mole strategy for multifocal ground glass opacities of the lungJ Thorac Dis 20179(suppl 3)S201ndashS207
22 Swanson DS Harrison CJ Playing Whack-a-Mole with pneumococcal serotypeeradication Pediatrics 2017140e20172034
23 Mestrovic T A microbial game of whack-a-mole clinical case series of the urethraluncloaking phenomenon caused by Corynebacterium glucuronolyticum in mentreated for Chlamydia trachomatis urethritis Infection 201947121ndash124
24 Gelfand JM Cree BAC Hauser SL Ocrelizumab and other CD20+ B-cell-depletingtherapies in multiple sclerosis Neurotherapeutics 201714835ndash841
25 Voog E Morschhauser F Solal-Celigny P Neutropenia in patients treated with rit-uximab N Engl J Med 20033482691ndash2694 discussion 2691ndash2694
26 Bar-Or A Fawaz L Fan B et al Abnormal B-cell cytokine responses a trigger of T-cell-mediated disease in MS Ann Neurol 201067452ndash461
27 Weber MS Prodrsquohomme T Patarroyo JC et al B-cell activation influences T-cellpolarization and outcome of anti-CD20 B-cell depletion in central nervous systemautoimmunity Ann Neurol 201068369ndash383
28 Monson NL Cravens P Hussain R et al Rituximab therapy reduces organ-specificT cell responses and ameliorates experimental autoimmune encephalomyelitis PLoSOne 20116e17103
29 Molnarfi N Schulze-Topphoff U Weber MS et al MHC class II-dependent B cellAPC function is required for induction of CNS autoimmunity independent of myelin-specific antibodies J Exp Med 20132102921ndash2937
30 Baker D Herrod SS Alvarez-Gonzalez C Giovannoni G Schmierer KInterpreting lymphocyte reconstitution data from the pivotal phase 3 trials of alem-tuzumab JAMA Neurol 201774961ndash969
31 Krupica T Fry TJ Mackall CL Autoimmunity during lymphopenia a two-hit modelClin Immunol 2006120121ndash128
32 Wilk EWitte TMarquardt N et al Depletion of functionally active CD20+ T cells byrituximab treatment Arthritis Rheum 2009603563ndash3571
33 Schuh E Berer K Mulazzani M et al Features of human CD3+CD20+ T cellsJ Immunol 20161971111ndash1117
34 Gingele S Kripuletz T Jacobs R Role of CD20+ T cells in multiple sclerosisimpli-cations for treatment with ocrelizumab Neural Regen Res 202015663ndash664
35 Palanichamy A Jahn S Nickles D et al Rituximab efficiently depletes increasedCD20-expressing T cells in multiple sclerosis patients J Immunol 2014193580ndash586
36 Holley JE Bremer E Kendall AC et al CD20+ inflammatory T-cells are present inblood and brain of multiple sclerosis patients and can be selectively targeted forapoptotic elimination Mult Scler Relat Disord 20143650ndash685
37 von Essen MR Ammitzboslashll C Hansen RH et al Proinflammatory CD20+ T cells inthe pathogenesis of multiple sclerosis Brain 2019142120ndash132
38 Lovett-Racke AE Gormley M Liu Y et al B cell depletion with ublituximab reshapesthe T cell profile in multiple sclerosis patients J Neuroimmunol 2019332187ndash197
39 Cross AH Stark JL Lauber J Ramsbottom MJ Lyons JA Rituximab reduces B cells andT cells in cerebrospinal fluid ofmultiple sclerosis patients J Neuroimmunol 200618063ndash70
40 Naismith RT Piccio L Lyons JA et al Rituximab add-on therapy for breakthroughrelapsing multiple sclerosis a 52-week phase II trial Neurology 2010741860ndash1867
41 Greenberg BM Graves D Remington G et al Rituximab dosing and monitoringstrategies in neuromyelitis optica patients creating strategies for therapeutic successMult Scler 2012181022ndash1026
42 Kim SH Jeong IH Hyun JW et al Treatment outcomes with rituximab in 100patients with neuromyelitis optica influence of FCGR3A polymorphisms on thetherapeutic response to rituximab JAMA Neurol 201572989ndash995
43 Steinman L Induction of new autoimmune diseases after alemtuzumab therapy formultiple sclerosis learning from adversity JAMA Neurol 201774907ndash908
44 Delcoigne B Manouchehrinia A Barro C et al Blood neurofilament light levelssegregate treatment effects in multiple sclerosis Neurology 202094e1201ndashe1212
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
DOI 101212NXI000000000000086820207 Neurol Neuroimmunol Neuroinflamm
Ethan Meltzer Sarah Campbell Benjamin Ehrenfeld et al depletion strategy
Mitigating alemtuzumab-associated autoimmunity in MS A whack-a-mole B-cell
This information is current as of August 7 2020
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

to immunologic labetalol the latter commonly used as ahighly titratable agent for management of hypertensive crisessuch as hypertensive encephalopathy where loss of cerebro-vascular autoregulation precludes the employment of long-acting agents which could result in a protracted compromisein cerebral blood flow dynamics predisposing to a hypoxic-ischemic insult) in patients with NMOSD compared with 184days for a 1000 mg dose of rituximab41
Low-dose rituximab is a more attractive alternative to stan-dard doses of 1000 mg or 375 mgm2 First doses of ritux-imab as low as 1 mgm2 suppress B cells by 97 in healthycontrols and B cells remain suppressed to 75 of baselinelevels at 12 weeks after infusion4243
Second low-dose anti-CD20 therapy does not result in pro-longed B-cell depletion so as not to interfere with repeatcycles of alemtuzumab therapy41
Third low-dose rituximab may facilitate greater control ofB-cell repopulation and improved temporal synchronizationwith T-cell repopulation
Last reduced dosing magnitude reduces the duration of im-munosuppression compared with conventional doses of rit-uximab and may eventually be shown in evidence-basedstudies to demonstrate both safety and cost advantages if fewcomplications are identified with the low-dose regimen
A more robust clinical trial with a primary outcome of thedevelopment of secondary autoimmunity would not likelyrequire a large number of participants given the incidence rateof 40 of autoimmune thyroid disease in patients with MSwho have received alemtuzumab34 Hence we would esti-mate an incidence of 40 in the control group ofalemtuzumab-only treated patients and with an assumption ofan incidence of 10 in patients who would receive adjunctrituximab If we assign the probability of a type I error of 5and a power of 80 a trial would need approximately 80patients total (40 in each arm) accounting for drop-outs
In addition to our small sample size and an unrandomizedand unblended cohort many physicians prescribe steroidswith rituximab infusion (methylprednisolone 250 mg beforeeach and every alemtuzumab infusion in our center) to pre-vent infusion reactions It is possible that the potential positiveeffects of secondary autoimmunity prevention attributed torituximab are instead or at least in part due to steroid usageIn addition treatment may simply delay secondary autoim-munity rather than preventing it and longer periods of as-certainment will be required to assess for this prospect
An alternate explanation concerning the impact of rituximabon secondary autoimmunity is that some individuals mayrespond differently to low-dose anti-CD20 therapy due to theeffects of the FCGR3A polymorphism42 We do not know theeffect of the polymorphism on low-dose rituximab kinetics
however binding affinity may play a larger role in low-doserituximab compared with conventional doses given the lowerabsolute concentration of rituximab Such issues should becarefully considered in the design of a larger trial particularlygiven potential effects of such factors on response character-istics as well as on study cost
As the field of neurology shifts from amodel of step escalationto induction therapy for the treatment of MS strategies thatare aimed at mitigating the risks of potent disease modifyingtherapies are urgently needed43
Only through the scientific method of subjecting our hy-pothesis to the rigors of a controlled adequately blindedprospective and adequately powered clinical trial can weconfirm or refute the hypothesis-driven question can theapplication of low-dose anti-CD20 therapy temporally syn-chronized with objective confirmation of B-cell hyper-repopulation serve to adequately reduce or even preventalemtuzumab-associated secondary autoimmunity
Furthermore the addition of anti-CD20 therapy could po-tentially confer benefits on immune deviation that would exertadded efficacy in synergy with the alemtuzumab-mediatedmechanisms of action in the establishment of disease re-mission while constituting augmented and durable regulatoryproperties in keeping with those achieved during the criticalperiod that we now recognize collectively as self-tolerance
Buffeted by the broad dissemination of bone marrow mobili-zation of stem cells following alemtuzumab treatment maypromote the process of restoration and neurologic functionalreconstitution Recent evidence has demonstrated that anemerging biomarker for assessing tissue damage in the CNS ofpatients withMS the neurofilament light chain is reducedmostmarkedly following the administration of alemtuzumab whencompared with other disease-modifying therapies and that suchlevels remain reduced to the greatest magnitude over time44
It was once thought that a proposition such as repair andfunctional recovery from MS was wholly enigmatic and un-likely However we have arrived at a point in the history of ourunderstanding of the disorderrsquos pathobiology in concert withthe corresponding derangements in immune regulatory in-fluences and how to remediate them We believe our work torepresent but a single small step toward this constellation ofgoals that are so important to our deserving patients theirfamilies our community and those of us who serve on thoseteams who care for and about them
AcknowledgmentThe authors thank Mr Jason Ooi and Dr Matthew Parsonsfor their transformation and production of Elliot andTeresa Frohmanrsquos formulation of the figure 1 medicalillustration which showcases alemtuzumabrsquos mechanism ofaction the pathobiological underpinnings for treatment-associated secondary autoimmunity and the hypothetical
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
mechanisms germane to our ldquowhack-a-molerdquo B-cell de-letion strategy aimed at mitigating alemtuzumab-associatedautoimmunity in MS
Study fundingThe National Multiple Sclerosis Society 5-Year InstitutionalFellowship Training Grant Awarded to TC Frohman andEM Frohman Fellows funded E Meltzer and RA Cruz(coauthors) MS and Neuroimmunology Center The DellMedical School at The University of Texas at Austin
DisclosureE Meltzer served as a consultant for Genzyme and receivedhonoraria from Novartis S Campbell and B Ehrenfeld havenothing to disclose L Steinman is on the Editorial Boards ofthe Proceedings of the National Academy of Sciences and theJournal of Neuroimmunology He has served on the EditorialBoard of the Journal of Immunology and International Immu-nology He has served as a member of grant review committeesfor the NIH and the National MS Society He has served orserves as a consultant and received honoraria from AtaraBiotherapeutics Atreca Biogen-Idec Celgene CentocorCoherus EMD-Serono Genzyme Johnson and JohnsonNovartis RocheGenentech Teva Pharmaceuticals Incand TG Therapeutics He has served on the Data SafetyMonitoring Board for TG Therapeutics He serves on theBoard of Directors of Tolerion and Chairs the ScientificAdvisory Board for Atreca Currently L Steinman receivesresearch grant support from the NIH and Atara Bio-therapeutics MS Parsons has nothing to disclose SSZamvil is Deputy Editor ofNeurology Neuroimmunology andNeuroinflammation and is an Associate Editor for Frontiers inImmunology and Frontiers in Neurology He serves on theAdvisory Committee for the American Congress onTreatment and Research in Multiple Sclerosis (ACTRIMS)and is a standing member of the research grant reviewcommittee for the National Multiple Sclerosis Society(NMSS) He has served on the Editorial Board of theJournal of Clinical Investigation The Journal of Immunologyand The Journal of Neurological Sciences and has been acharter member of the grant review committee for the NIHClinical Neuroimmunology and Brain Tumors (CNBT)He has served or serves as a consultant and receivedhonoraria from Alexion Biogen-Idec EMD-SeronoGenzyme Novartis RocheGenentech and Teva Pharma-ceuticals Inc and has served on Data Safety MonitoringBoards for Lilly BioMS Teva and Opexa TherapeuticsCurrently SS Zamvil receives research grant support fromthe NIH NMSS Weill Institute Race to Erase MS and theMaisin Foundation TC Frohman has received advisoryboard fees from Alexion EM Frohman has receivedspeaker honoraria from Genzyme Novartis Alexion andAcorda Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationDecember 25 2019 Accepted in final form July 6 2020
References1 Coles AJ Twyman CL Arnold DL et al Alemtuzumab for patients with relapsing
multiple sclerosis after disease-modifying therapy a randomised controlled phase 3trial Lancet 20123801829ndash1839
2 Cohen JA Coles AJ Arnold DL et al Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis a randomisedcontrolled phase 3 trial Lancet 20123801819ndash1828
3 Coles AJ Cohen JA Fox EJ et al Alemtuzumab CARE-MS II 5-year follow-upNeurology 2017891117ndash1126
4 Havrdova E Arnold DL Cohen JA et al Alemtuzumab CARE-MS I 5-year follow-upNeurology 2017891107ndash1116
5 Sarvepalli D Rashid MU Ullah W Zafar Y Khan M Idiopathic thrombocytopenicpurpura a rare syndrome with alemtuzumab review of monitoring protocol Cureus201911e5715
6 Ruck T Schulte-Mecklenbeck A Pfeuffer S et al Pretreatment anti-thyroid auto-antibodies indicate increased risk for thyroid autoimmunity secondary to alemtuzu-mab a prospective cohort study EBioMedicine 201946381ndash386
Appendix Authors
Name Location Contribution
Ethan MeltzerMD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
SarahCampbell RN
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
BenjaminEhrenfeldMSW
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
Roberto ACruz MD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
LawrenceSteinman MD
Department ofNeurology StanfordUniversity School ofMedicine
Conception and criticalrevision of themanuscript forintellectual content
Matthew SParsons PhD
Division of Microbiologyand Immunology YerkesNational PrimateResearch CenterDepartment of Pathologyand Laboratory MedicineEmory University
Conception and criticalrevision of themanuscript forintellectual content
Scott S ZamvilMD PhD
Department ofNeurology amp Program inImmunology Universityof California SanFrancisco
Conception and criticalrevision of themanuscript forintellectual content
Elliot MFrohman MDPhD
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical SchoolUniversity of Texas atAustin
Conception and criticalrevision of themanuscript forintellectual content
Teresa CFrohmanMPAS MSCSPA-C FANA
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical School Universityof Texas at Austin
Conception and criticalrevision of themanuscript forintellectual content
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 9
7 Ruck T Pfeuffer S Schulte-Mecklenbeck A et al Vitiligo after alemtuzumab treat-ment secondary autoimmunity is not all about B cells Neurology 201891e2233ndashe2237
8 Zimmermann J Buhl T Muller M Alopecia universalis following alemtuzumabtreatment in multiple sclerosis a barely recognized manifestation of secondaryautoimmunity-report of a case and review of the literature Front Neurol 20178569
9 Rotondi M Molteni M Leporati P Capelli V Marino M Chiovato L Autoimmunethyroid diseases in patients treated with alemtuzumab for multiple sclerosis an ex-ample of selective anti-TSH-receptor immune response Front Endocrinol (Lau-sanne) 20178254
10 Costelloe L Jones J Coles A Secondary autoimmune diseases following alemtuzu-mab therapy for multiple sclerosis Expert Rev Neurother 201212335ndash341
11 Jones JL Phuah CL Cox AL et al IL-21 drives secondary autoimmunity in patientswith multiple sclerosis following therapeutic lymphocyte depletion with alemtuzu-mab (Campath-1H) J Clin Invest 20091192052ndash2061
12 Torino F Barnabei A Paragliola R Baldelli R Appetecchia M Corsello SM Thyroiddysfunction as an unintended side effect of anticancer drugs Thyroid 2013231345ndash1366
13 Azzopardi L Thompson SA Harding KE et al Predicting autoimmunity afteralemtuzumab treatment of multiple sclerosis J Neurol Neurosurg Psychiatry 201485795ndash798
14 Trinh T Haridas AS Sullivan TJ Ocular findings in alemtuzumab (Campath-1H)-induced thyroid eye disease Ophthalmic Plast Reconstr Surg 201632e128ndashe129
15 von Kutzleben S Pryce G Giovannoni G Baker D Depletion of CD52-positivecells inhibits the development of central nervous system autoimmune disease butdeletes an immune-tolerance promoting CD8 T-cell population Implications forsecondary autoimmunity of alemtuzumab in multiple sclerosis Immunology 2017150444ndash455
16 Wiendl H Carraro M Comi G et al Lymphocyte pharmacodynamics are not asso-ciated with autoimmunity or efficacy after alemtuzumab Neurol NeuroimmunolNeuroinflamm 201971ndash10 doi101212NXI0000000000000635
17 Kousin-Ezewu O Azzopardi L Parker RA et al Accelerated lymphocyte recoveryafter alemtuzumab does not predict multiple sclerosis activity Neurology 2014822158ndash2164
18 Jones J Thompson S Loh P et al Human autoimmunity after lymphocyte depletionis caused by homeostatic T-cell proliferation Proc Natl Acad Sci U S A 201311020200ndash20205
19 Costa DB Kobayashi SS Whacking a mole-cule clinical activity and mechanisms ofresistance to third generation EGFR inhibitors in EGFR mutated lung cancers withEGFR-T790M Transl Lung Cancer Res 20156809ndash815
20 Shin J MacCarthy T Antagonistic coevolution drives whack-a-mole sensitivity ingene regulatory networks PLoS Comput Biol 201511e1004432
21 Suzuki K Whack-a-mole strategy for multifocal ground glass opacities of the lungJ Thorac Dis 20179(suppl 3)S201ndashS207
22 Swanson DS Harrison CJ Playing Whack-a-Mole with pneumococcal serotypeeradication Pediatrics 2017140e20172034
23 Mestrovic T A microbial game of whack-a-mole clinical case series of the urethraluncloaking phenomenon caused by Corynebacterium glucuronolyticum in mentreated for Chlamydia trachomatis urethritis Infection 201947121ndash124
24 Gelfand JM Cree BAC Hauser SL Ocrelizumab and other CD20+ B-cell-depletingtherapies in multiple sclerosis Neurotherapeutics 201714835ndash841
25 Voog E Morschhauser F Solal-Celigny P Neutropenia in patients treated with rit-uximab N Engl J Med 20033482691ndash2694 discussion 2691ndash2694
26 Bar-Or A Fawaz L Fan B et al Abnormal B-cell cytokine responses a trigger of T-cell-mediated disease in MS Ann Neurol 201067452ndash461
27 Weber MS Prodrsquohomme T Patarroyo JC et al B-cell activation influences T-cellpolarization and outcome of anti-CD20 B-cell depletion in central nervous systemautoimmunity Ann Neurol 201068369ndash383
28 Monson NL Cravens P Hussain R et al Rituximab therapy reduces organ-specificT cell responses and ameliorates experimental autoimmune encephalomyelitis PLoSOne 20116e17103
29 Molnarfi N Schulze-Topphoff U Weber MS et al MHC class II-dependent B cellAPC function is required for induction of CNS autoimmunity independent of myelin-specific antibodies J Exp Med 20132102921ndash2937
30 Baker D Herrod SS Alvarez-Gonzalez C Giovannoni G Schmierer KInterpreting lymphocyte reconstitution data from the pivotal phase 3 trials of alem-tuzumab JAMA Neurol 201774961ndash969
31 Krupica T Fry TJ Mackall CL Autoimmunity during lymphopenia a two-hit modelClin Immunol 2006120121ndash128
32 Wilk EWitte TMarquardt N et al Depletion of functionally active CD20+ T cells byrituximab treatment Arthritis Rheum 2009603563ndash3571
33 Schuh E Berer K Mulazzani M et al Features of human CD3+CD20+ T cellsJ Immunol 20161971111ndash1117
34 Gingele S Kripuletz T Jacobs R Role of CD20+ T cells in multiple sclerosisimpli-cations for treatment with ocrelizumab Neural Regen Res 202015663ndash664
35 Palanichamy A Jahn S Nickles D et al Rituximab efficiently depletes increasedCD20-expressing T cells in multiple sclerosis patients J Immunol 2014193580ndash586
36 Holley JE Bremer E Kendall AC et al CD20+ inflammatory T-cells are present inblood and brain of multiple sclerosis patients and can be selectively targeted forapoptotic elimination Mult Scler Relat Disord 20143650ndash685
37 von Essen MR Ammitzboslashll C Hansen RH et al Proinflammatory CD20+ T cells inthe pathogenesis of multiple sclerosis Brain 2019142120ndash132
38 Lovett-Racke AE Gormley M Liu Y et al B cell depletion with ublituximab reshapesthe T cell profile in multiple sclerosis patients J Neuroimmunol 2019332187ndash197
39 Cross AH Stark JL Lauber J Ramsbottom MJ Lyons JA Rituximab reduces B cells andT cells in cerebrospinal fluid ofmultiple sclerosis patients J Neuroimmunol 200618063ndash70
40 Naismith RT Piccio L Lyons JA et al Rituximab add-on therapy for breakthroughrelapsing multiple sclerosis a 52-week phase II trial Neurology 2010741860ndash1867
41 Greenberg BM Graves D Remington G et al Rituximab dosing and monitoringstrategies in neuromyelitis optica patients creating strategies for therapeutic successMult Scler 2012181022ndash1026
42 Kim SH Jeong IH Hyun JW et al Treatment outcomes with rituximab in 100patients with neuromyelitis optica influence of FCGR3A polymorphisms on thetherapeutic response to rituximab JAMA Neurol 201572989ndash995
43 Steinman L Induction of new autoimmune diseases after alemtuzumab therapy formultiple sclerosis learning from adversity JAMA Neurol 201774907ndash908
44 Delcoigne B Manouchehrinia A Barro C et al Blood neurofilament light levelssegregate treatment effects in multiple sclerosis Neurology 202094e1201ndashe1212
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
DOI 101212NXI000000000000086820207 Neurol Neuroimmunol Neuroinflamm
Ethan Meltzer Sarah Campbell Benjamin Ehrenfeld et al depletion strategy
Mitigating alemtuzumab-associated autoimmunity in MS A whack-a-mole B-cell
This information is current as of August 7 2020
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

mechanisms germane to our ldquowhack-a-molerdquo B-cell de-letion strategy aimed at mitigating alemtuzumab-associatedautoimmunity in MS
Study fundingThe National Multiple Sclerosis Society 5-Year InstitutionalFellowship Training Grant Awarded to TC Frohman andEM Frohman Fellows funded E Meltzer and RA Cruz(coauthors) MS and Neuroimmunology Center The DellMedical School at The University of Texas at Austin
DisclosureE Meltzer served as a consultant for Genzyme and receivedhonoraria from Novartis S Campbell and B Ehrenfeld havenothing to disclose L Steinman is on the Editorial Boards ofthe Proceedings of the National Academy of Sciences and theJournal of Neuroimmunology He has served on the EditorialBoard of the Journal of Immunology and International Immu-nology He has served as a member of grant review committeesfor the NIH and the National MS Society He has served orserves as a consultant and received honoraria from AtaraBiotherapeutics Atreca Biogen-Idec Celgene CentocorCoherus EMD-Serono Genzyme Johnson and JohnsonNovartis RocheGenentech Teva Pharmaceuticals Incand TG Therapeutics He has served on the Data SafetyMonitoring Board for TG Therapeutics He serves on theBoard of Directors of Tolerion and Chairs the ScientificAdvisory Board for Atreca Currently L Steinman receivesresearch grant support from the NIH and Atara Bio-therapeutics MS Parsons has nothing to disclose SSZamvil is Deputy Editor ofNeurology Neuroimmunology andNeuroinflammation and is an Associate Editor for Frontiers inImmunology and Frontiers in Neurology He serves on theAdvisory Committee for the American Congress onTreatment and Research in Multiple Sclerosis (ACTRIMS)and is a standing member of the research grant reviewcommittee for the National Multiple Sclerosis Society(NMSS) He has served on the Editorial Board of theJournal of Clinical Investigation The Journal of Immunologyand The Journal of Neurological Sciences and has been acharter member of the grant review committee for the NIHClinical Neuroimmunology and Brain Tumors (CNBT)He has served or serves as a consultant and receivedhonoraria from Alexion Biogen-Idec EMD-SeronoGenzyme Novartis RocheGenentech and Teva Pharma-ceuticals Inc and has served on Data Safety MonitoringBoards for Lilly BioMS Teva and Opexa TherapeuticsCurrently SS Zamvil receives research grant support fromthe NIH NMSS Weill Institute Race to Erase MS and theMaisin Foundation TC Frohman has received advisoryboard fees from Alexion EM Frohman has receivedspeaker honoraria from Genzyme Novartis Alexion andAcorda Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationDecember 25 2019 Accepted in final form July 6 2020
References1 Coles AJ Twyman CL Arnold DL et al Alemtuzumab for patients with relapsing
multiple sclerosis after disease-modifying therapy a randomised controlled phase 3trial Lancet 20123801829ndash1839
2 Cohen JA Coles AJ Arnold DL et al Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis a randomisedcontrolled phase 3 trial Lancet 20123801819ndash1828
3 Coles AJ Cohen JA Fox EJ et al Alemtuzumab CARE-MS II 5-year follow-upNeurology 2017891117ndash1126
4 Havrdova E Arnold DL Cohen JA et al Alemtuzumab CARE-MS I 5-year follow-upNeurology 2017891107ndash1116
5 Sarvepalli D Rashid MU Ullah W Zafar Y Khan M Idiopathic thrombocytopenicpurpura a rare syndrome with alemtuzumab review of monitoring protocol Cureus201911e5715
6 Ruck T Schulte-Mecklenbeck A Pfeuffer S et al Pretreatment anti-thyroid auto-antibodies indicate increased risk for thyroid autoimmunity secondary to alemtuzu-mab a prospective cohort study EBioMedicine 201946381ndash386
Appendix Authors
Name Location Contribution
Ethan MeltzerMD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
SarahCampbell RN
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
BenjaminEhrenfeldMSW
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
Roberto ACruz MD
MS amp NeuroimmunologyCTR Department ofNeurology Dell MedicalSchool University ofTexas at Austin
Conception and criticalrevision of themanuscript forintellectual content
LawrenceSteinman MD
Department ofNeurology StanfordUniversity School ofMedicine
Conception and criticalrevision of themanuscript forintellectual content
Matthew SParsons PhD
Division of Microbiologyand Immunology YerkesNational PrimateResearch CenterDepartment of Pathologyand Laboratory MedicineEmory University
Conception and criticalrevision of themanuscript forintellectual content
Scott S ZamvilMD PhD
Department ofNeurology amp Program inImmunology Universityof California SanFrancisco
Conception and criticalrevision of themanuscript forintellectual content
Elliot MFrohman MDPhD
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical SchoolUniversity of Texas atAustin
Conception and criticalrevision of themanuscript forintellectual content
Teresa CFrohmanMPAS MSCSPA-C FANA
MS amp NeuroimmunologyCTR Department ofNeurology Neurosurgeryamp Ophthalmology DellMedical School Universityof Texas at Austin
Conception and criticalrevision of themanuscript forintellectual content
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 9
7 Ruck T Pfeuffer S Schulte-Mecklenbeck A et al Vitiligo after alemtuzumab treat-ment secondary autoimmunity is not all about B cells Neurology 201891e2233ndashe2237
8 Zimmermann J Buhl T Muller M Alopecia universalis following alemtuzumabtreatment in multiple sclerosis a barely recognized manifestation of secondaryautoimmunity-report of a case and review of the literature Front Neurol 20178569
9 Rotondi M Molteni M Leporati P Capelli V Marino M Chiovato L Autoimmunethyroid diseases in patients treated with alemtuzumab for multiple sclerosis an ex-ample of selective anti-TSH-receptor immune response Front Endocrinol (Lau-sanne) 20178254
10 Costelloe L Jones J Coles A Secondary autoimmune diseases following alemtuzu-mab therapy for multiple sclerosis Expert Rev Neurother 201212335ndash341
11 Jones JL Phuah CL Cox AL et al IL-21 drives secondary autoimmunity in patientswith multiple sclerosis following therapeutic lymphocyte depletion with alemtuzu-mab (Campath-1H) J Clin Invest 20091192052ndash2061
12 Torino F Barnabei A Paragliola R Baldelli R Appetecchia M Corsello SM Thyroiddysfunction as an unintended side effect of anticancer drugs Thyroid 2013231345ndash1366
13 Azzopardi L Thompson SA Harding KE et al Predicting autoimmunity afteralemtuzumab treatment of multiple sclerosis J Neurol Neurosurg Psychiatry 201485795ndash798
14 Trinh T Haridas AS Sullivan TJ Ocular findings in alemtuzumab (Campath-1H)-induced thyroid eye disease Ophthalmic Plast Reconstr Surg 201632e128ndashe129
15 von Kutzleben S Pryce G Giovannoni G Baker D Depletion of CD52-positivecells inhibits the development of central nervous system autoimmune disease butdeletes an immune-tolerance promoting CD8 T-cell population Implications forsecondary autoimmunity of alemtuzumab in multiple sclerosis Immunology 2017150444ndash455
16 Wiendl H Carraro M Comi G et al Lymphocyte pharmacodynamics are not asso-ciated with autoimmunity or efficacy after alemtuzumab Neurol NeuroimmunolNeuroinflamm 201971ndash10 doi101212NXI0000000000000635
17 Kousin-Ezewu O Azzopardi L Parker RA et al Accelerated lymphocyte recoveryafter alemtuzumab does not predict multiple sclerosis activity Neurology 2014822158ndash2164
18 Jones J Thompson S Loh P et al Human autoimmunity after lymphocyte depletionis caused by homeostatic T-cell proliferation Proc Natl Acad Sci U S A 201311020200ndash20205
19 Costa DB Kobayashi SS Whacking a mole-cule clinical activity and mechanisms ofresistance to third generation EGFR inhibitors in EGFR mutated lung cancers withEGFR-T790M Transl Lung Cancer Res 20156809ndash815
20 Shin J MacCarthy T Antagonistic coevolution drives whack-a-mole sensitivity ingene regulatory networks PLoS Comput Biol 201511e1004432
21 Suzuki K Whack-a-mole strategy for multifocal ground glass opacities of the lungJ Thorac Dis 20179(suppl 3)S201ndashS207
22 Swanson DS Harrison CJ Playing Whack-a-Mole with pneumococcal serotypeeradication Pediatrics 2017140e20172034
23 Mestrovic T A microbial game of whack-a-mole clinical case series of the urethraluncloaking phenomenon caused by Corynebacterium glucuronolyticum in mentreated for Chlamydia trachomatis urethritis Infection 201947121ndash124
24 Gelfand JM Cree BAC Hauser SL Ocrelizumab and other CD20+ B-cell-depletingtherapies in multiple sclerosis Neurotherapeutics 201714835ndash841
25 Voog E Morschhauser F Solal-Celigny P Neutropenia in patients treated with rit-uximab N Engl J Med 20033482691ndash2694 discussion 2691ndash2694
26 Bar-Or A Fawaz L Fan B et al Abnormal B-cell cytokine responses a trigger of T-cell-mediated disease in MS Ann Neurol 201067452ndash461
27 Weber MS Prodrsquohomme T Patarroyo JC et al B-cell activation influences T-cellpolarization and outcome of anti-CD20 B-cell depletion in central nervous systemautoimmunity Ann Neurol 201068369ndash383
28 Monson NL Cravens P Hussain R et al Rituximab therapy reduces organ-specificT cell responses and ameliorates experimental autoimmune encephalomyelitis PLoSOne 20116e17103
29 Molnarfi N Schulze-Topphoff U Weber MS et al MHC class II-dependent B cellAPC function is required for induction of CNS autoimmunity independent of myelin-specific antibodies J Exp Med 20132102921ndash2937
30 Baker D Herrod SS Alvarez-Gonzalez C Giovannoni G Schmierer KInterpreting lymphocyte reconstitution data from the pivotal phase 3 trials of alem-tuzumab JAMA Neurol 201774961ndash969
31 Krupica T Fry TJ Mackall CL Autoimmunity during lymphopenia a two-hit modelClin Immunol 2006120121ndash128
32 Wilk EWitte TMarquardt N et al Depletion of functionally active CD20+ T cells byrituximab treatment Arthritis Rheum 2009603563ndash3571
33 Schuh E Berer K Mulazzani M et al Features of human CD3+CD20+ T cellsJ Immunol 20161971111ndash1117
34 Gingele S Kripuletz T Jacobs R Role of CD20+ T cells in multiple sclerosisimpli-cations for treatment with ocrelizumab Neural Regen Res 202015663ndash664
35 Palanichamy A Jahn S Nickles D et al Rituximab efficiently depletes increasedCD20-expressing T cells in multiple sclerosis patients J Immunol 2014193580ndash586
36 Holley JE Bremer E Kendall AC et al CD20+ inflammatory T-cells are present inblood and brain of multiple sclerosis patients and can be selectively targeted forapoptotic elimination Mult Scler Relat Disord 20143650ndash685
37 von Essen MR Ammitzboslashll C Hansen RH et al Proinflammatory CD20+ T cells inthe pathogenesis of multiple sclerosis Brain 2019142120ndash132
38 Lovett-Racke AE Gormley M Liu Y et al B cell depletion with ublituximab reshapesthe T cell profile in multiple sclerosis patients J Neuroimmunol 2019332187ndash197
39 Cross AH Stark JL Lauber J Ramsbottom MJ Lyons JA Rituximab reduces B cells andT cells in cerebrospinal fluid ofmultiple sclerosis patients J Neuroimmunol 200618063ndash70
40 Naismith RT Piccio L Lyons JA et al Rituximab add-on therapy for breakthroughrelapsing multiple sclerosis a 52-week phase II trial Neurology 2010741860ndash1867
41 Greenberg BM Graves D Remington G et al Rituximab dosing and monitoringstrategies in neuromyelitis optica patients creating strategies for therapeutic successMult Scler 2012181022ndash1026
42 Kim SH Jeong IH Hyun JW et al Treatment outcomes with rituximab in 100patients with neuromyelitis optica influence of FCGR3A polymorphisms on thetherapeutic response to rituximab JAMA Neurol 201572989ndash995
43 Steinman L Induction of new autoimmune diseases after alemtuzumab therapy formultiple sclerosis learning from adversity JAMA Neurol 201774907ndash908
44 Delcoigne B Manouchehrinia A Barro C et al Blood neurofilament light levelssegregate treatment effects in multiple sclerosis Neurology 202094e1201ndashe1212
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
DOI 101212NXI000000000000086820207 Neurol Neuroimmunol Neuroinflamm
Ethan Meltzer Sarah Campbell Benjamin Ehrenfeld et al depletion strategy
Mitigating alemtuzumab-associated autoimmunity in MS A whack-a-mole B-cell
This information is current as of August 7 2020
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

7 Ruck T Pfeuffer S Schulte-Mecklenbeck A et al Vitiligo after alemtuzumab treat-ment secondary autoimmunity is not all about B cells Neurology 201891e2233ndashe2237
8 Zimmermann J Buhl T Muller M Alopecia universalis following alemtuzumabtreatment in multiple sclerosis a barely recognized manifestation of secondaryautoimmunity-report of a case and review of the literature Front Neurol 20178569
9 Rotondi M Molteni M Leporati P Capelli V Marino M Chiovato L Autoimmunethyroid diseases in patients treated with alemtuzumab for multiple sclerosis an ex-ample of selective anti-TSH-receptor immune response Front Endocrinol (Lau-sanne) 20178254
10 Costelloe L Jones J Coles A Secondary autoimmune diseases following alemtuzu-mab therapy for multiple sclerosis Expert Rev Neurother 201212335ndash341
11 Jones JL Phuah CL Cox AL et al IL-21 drives secondary autoimmunity in patientswith multiple sclerosis following therapeutic lymphocyte depletion with alemtuzu-mab (Campath-1H) J Clin Invest 20091192052ndash2061
12 Torino F Barnabei A Paragliola R Baldelli R Appetecchia M Corsello SM Thyroiddysfunction as an unintended side effect of anticancer drugs Thyroid 2013231345ndash1366
13 Azzopardi L Thompson SA Harding KE et al Predicting autoimmunity afteralemtuzumab treatment of multiple sclerosis J Neurol Neurosurg Psychiatry 201485795ndash798
14 Trinh T Haridas AS Sullivan TJ Ocular findings in alemtuzumab (Campath-1H)-induced thyroid eye disease Ophthalmic Plast Reconstr Surg 201632e128ndashe129
15 von Kutzleben S Pryce G Giovannoni G Baker D Depletion of CD52-positivecells inhibits the development of central nervous system autoimmune disease butdeletes an immune-tolerance promoting CD8 T-cell population Implications forsecondary autoimmunity of alemtuzumab in multiple sclerosis Immunology 2017150444ndash455
16 Wiendl H Carraro M Comi G et al Lymphocyte pharmacodynamics are not asso-ciated with autoimmunity or efficacy after alemtuzumab Neurol NeuroimmunolNeuroinflamm 201971ndash10 doi101212NXI0000000000000635
17 Kousin-Ezewu O Azzopardi L Parker RA et al Accelerated lymphocyte recoveryafter alemtuzumab does not predict multiple sclerosis activity Neurology 2014822158ndash2164
18 Jones J Thompson S Loh P et al Human autoimmunity after lymphocyte depletionis caused by homeostatic T-cell proliferation Proc Natl Acad Sci U S A 201311020200ndash20205
19 Costa DB Kobayashi SS Whacking a mole-cule clinical activity and mechanisms ofresistance to third generation EGFR inhibitors in EGFR mutated lung cancers withEGFR-T790M Transl Lung Cancer Res 20156809ndash815
20 Shin J MacCarthy T Antagonistic coevolution drives whack-a-mole sensitivity ingene regulatory networks PLoS Comput Biol 201511e1004432
21 Suzuki K Whack-a-mole strategy for multifocal ground glass opacities of the lungJ Thorac Dis 20179(suppl 3)S201ndashS207
22 Swanson DS Harrison CJ Playing Whack-a-Mole with pneumococcal serotypeeradication Pediatrics 2017140e20172034
23 Mestrovic T A microbial game of whack-a-mole clinical case series of the urethraluncloaking phenomenon caused by Corynebacterium glucuronolyticum in mentreated for Chlamydia trachomatis urethritis Infection 201947121ndash124
24 Gelfand JM Cree BAC Hauser SL Ocrelizumab and other CD20+ B-cell-depletingtherapies in multiple sclerosis Neurotherapeutics 201714835ndash841
25 Voog E Morschhauser F Solal-Celigny P Neutropenia in patients treated with rit-uximab N Engl J Med 20033482691ndash2694 discussion 2691ndash2694
26 Bar-Or A Fawaz L Fan B et al Abnormal B-cell cytokine responses a trigger of T-cell-mediated disease in MS Ann Neurol 201067452ndash461
27 Weber MS Prodrsquohomme T Patarroyo JC et al B-cell activation influences T-cellpolarization and outcome of anti-CD20 B-cell depletion in central nervous systemautoimmunity Ann Neurol 201068369ndash383
28 Monson NL Cravens P Hussain R et al Rituximab therapy reduces organ-specificT cell responses and ameliorates experimental autoimmune encephalomyelitis PLoSOne 20116e17103
29 Molnarfi N Schulze-Topphoff U Weber MS et al MHC class II-dependent B cellAPC function is required for induction of CNS autoimmunity independent of myelin-specific antibodies J Exp Med 20132102921ndash2937
30 Baker D Herrod SS Alvarez-Gonzalez C Giovannoni G Schmierer KInterpreting lymphocyte reconstitution data from the pivotal phase 3 trials of alem-tuzumab JAMA Neurol 201774961ndash969
31 Krupica T Fry TJ Mackall CL Autoimmunity during lymphopenia a two-hit modelClin Immunol 2006120121ndash128
32 Wilk EWitte TMarquardt N et al Depletion of functionally active CD20+ T cells byrituximab treatment Arthritis Rheum 2009603563ndash3571
33 Schuh E Berer K Mulazzani M et al Features of human CD3+CD20+ T cellsJ Immunol 20161971111ndash1117
34 Gingele S Kripuletz T Jacobs R Role of CD20+ T cells in multiple sclerosisimpli-cations for treatment with ocrelizumab Neural Regen Res 202015663ndash664
35 Palanichamy A Jahn S Nickles D et al Rituximab efficiently depletes increasedCD20-expressing T cells in multiple sclerosis patients J Immunol 2014193580ndash586
36 Holley JE Bremer E Kendall AC et al CD20+ inflammatory T-cells are present inblood and brain of multiple sclerosis patients and can be selectively targeted forapoptotic elimination Mult Scler Relat Disord 20143650ndash685
37 von Essen MR Ammitzboslashll C Hansen RH et al Proinflammatory CD20+ T cells inthe pathogenesis of multiple sclerosis Brain 2019142120ndash132
38 Lovett-Racke AE Gormley M Liu Y et al B cell depletion with ublituximab reshapesthe T cell profile in multiple sclerosis patients J Neuroimmunol 2019332187ndash197
39 Cross AH Stark JL Lauber J Ramsbottom MJ Lyons JA Rituximab reduces B cells andT cells in cerebrospinal fluid ofmultiple sclerosis patients J Neuroimmunol 200618063ndash70
40 Naismith RT Piccio L Lyons JA et al Rituximab add-on therapy for breakthroughrelapsing multiple sclerosis a 52-week phase II trial Neurology 2010741860ndash1867
41 Greenberg BM Graves D Remington G et al Rituximab dosing and monitoringstrategies in neuromyelitis optica patients creating strategies for therapeutic successMult Scler 2012181022ndash1026
42 Kim SH Jeong IH Hyun JW et al Treatment outcomes with rituximab in 100patients with neuromyelitis optica influence of FCGR3A polymorphisms on thetherapeutic response to rituximab JAMA Neurol 201572989ndash995
43 Steinman L Induction of new autoimmune diseases after alemtuzumab therapy formultiple sclerosis learning from adversity JAMA Neurol 201774907ndash908
44 Delcoigne B Manouchehrinia A Barro C et al Blood neurofilament light levelssegregate treatment effects in multiple sclerosis Neurology 202094e1201ndashe1212
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 6 | November 2020 NeurologyorgNN
DOI 101212NXI000000000000086820207 Neurol Neuroimmunol Neuroinflamm
Ethan Meltzer Sarah Campbell Benjamin Ehrenfeld et al depletion strategy
Mitigating alemtuzumab-associated autoimmunity in MS A whack-a-mole B-cell
This information is current as of August 7 2020
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

DOI 101212NXI000000000000086820207 Neurol Neuroimmunol Neuroinflamm
Ethan Meltzer Sarah Campbell Benjamin Ehrenfeld et al depletion strategy
Mitigating alemtuzumab-associated autoimmunity in MS A whack-a-mole B-cell
This information is current as of August 7 2020
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

ServicesUpdated Information amp
httpnnneurologyorgcontent76e868fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent76e868fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionall_immunologyAll Immunology
httpnnneurologyorgcgicollectionall_demyelinating_disease_cnsAll Demyelinating disease (CNS)
httpnnneurologyorgcgicollectionall_clinical_trialsAll Clinical trialsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm