Embed Size (px)
Citation preview

Mission Thrombectomy 2020 (MT 2020)
Global Executive Committee
Kickoff Meeting, Nov 21st, 2019
12th Annual SVIN Meeting, Atlanta, GA , Nov 21st, 2019

Agenda
12th Annual SVIN Meeting, Atlanta, GA , Nov 21st, 2019
1. Welcome, Introductions
2. MT 2020 – Mission, Scope, Initiatives
3. GEC – Charter, Structure, Scope
4. Project Management
5. Wrap Up – Thank You and Next Steps

12th Annual SVIN Meeting, Atlanta, GA , Nov 21st, 2019
Introductions
• Name
• Affiliation
• Years of Stroke Treatment Experience
• Number of thrombectomies in your practice/hospital

Agenda
12th Annual SVIN Meeting, Atlanta, GA , Nov 21st, 2019
1. Welcome, Introductions
2. MT 2020 – Mission, Scope, Initiatives
3. GEC – Charter, Structure, Scope
4. Project Management
5. Wrap Up – Thank You and Next Steps

Mission Thrombectomy 2020
(MT 2020) Global Alliance:
Accelerating Global Access to
Stroke Thrombectomy
Dileep R. Yavagal, MD, FSVIN, FAHA, FAANDirector of Interventional Neurology , Co-Director Neuroendovascular
SurgeryClinical Professor of Neurology & NeurosurgeryUniversity of Miami Miller School of Medicine,
Miami, FL, USAOn Behalf of the MT 2020 Leadership and Global Executive
Committees
MT2020 Kickoff Meeting, Atlanta, GA , Nov 21st, 2019

Disclosures
1. Consultant (Modest): Covidien/Medtronic, Neuralanalytics, Cerenovus, NMDDO
2. Steering Committee member:SWIFT Prime, RECOVER-Stroke , MR RESCUE ( Investigator Steering committee)
3. DSMB member: ESCAPE4. Supported by grants from:
Florida Biomedical CTSI, NIHAnderson Family Gift

MT 2020: Funding
2019 Funding
Unrestricted Grants:Gold Level
• Penumbra• Cerenovus• Microvention• Medtronic
Silver Level• IschemiaView
2018 Funding
Unrestricted Grants:
Gold Level
•Microvention
Silver Level
• Penumbra
• SVIN

Chairs Committee
Dr. Violiza InoaCoordinating
ChairUSA
Global Executive Committee (GEC)
Dr. Sheila MartinsCo-Chair
Brazil
Dr. Werner HackeCo-ChairGermany
Dr. Andrew DemchukCo-ChairCanada
Dr. Thomas LeungCo-Chair
Hong Kong
Country Liaison Regional Sub-Committees
Country Liaison
LeadershipCommittee
PMO
• Chair - Dileep R. Yavagal,
MD
• Vice-Chair - Ashutosh
Jadhav, MD, PhD
• Ameer Hassan, DO, FSVIN
• Vallabh Janardhan, MD,
FSVIN
• Violiza Inoa, MD
• Italo Linfante, MD, FAHA,
FSVIN
• Raul Nogueira, MD, FSVIN
• Robin Novakovic, MD,
FSVIN
• Osama (Sam) Zaidat, MD,
MSc, FSVIN
• Syed Zaidi, MD
• Ossama Yassin, MD
• Urs Fischer, MD
Chair, Stroke
Chair, MT
Board Member #1
Board Member #2
Board Member #3
•Orbees Medical
Anurag Mairal, PhD
Shyam Venkatesh,
PhD
- Project Management
- Strategy Consultant
•Asutosh Jadhav, PhD
- Consultant
• Jennifer Potter-Vig,
PhD
- Project Manager,
SVIN
Reg
ion
___
____
_
AdvisoryCommittee
• Society Liaisons
o ASA/AHA
o ESO
o MENA-SINO
o WSO
o SNIS
o WFITN
• Ralph Sacco
• Larry Goldstein
• Anne Alexandrov
• Endorsing Organizations
o ANZ – AN
o 5T-Stroke
o SISS
o KNANN
o NCS
o NVX
o SNVI
TBACo-Chair
China

MT 2020 Global Alliance: Partnerships
Partner Organizations1. American Stroke
Association/American Heart Association (ASA/AHA)
2. European Stroke Association (ESO): ResQ Registry
3. Middle East North Africa –Society (MENA-SINO)
4. World Stroke Organization (WSO)
5. SNIS6. WFITN
Endorsing Organizations1. Australian and New Zealand
Assn of Neurologists 2. Calgary Stroke Program (5T
Stroke)3. Italian Society for Study of
Stroke (SISS)4. Kazakhstan National Assn. of
Neurologists Neuroscience (KNANN)
5. Neurocritical Care Society (NCS)6. Neurovascular Exchange (NVX)7. SNVI: Society for Neurovascular
Intervention (India)

Global Burden of Stroke: Now Substantially Reversible!

Mechanical Thrombectomy is highly Costly but Cost-Effective
• Health-economic analysis• Quantify the impact of
developing stroke care in the country
• Estimates the impact of
gradually increasing uptake
of more effective treatments
over 10 years
• estimated cost savings of
$602 million over 15 years
($255 million direct costs,
$348 million indirect costs).

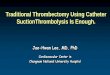
Major inequalities in acute stroke treatment between and
within 44 European countries
Figure 1. Choropleth map showing number of stroke units per million population
in 42 European countries (mean 2.9, 95% CI 2.3–3.6).
A need to implement tailored stroke care
programs for reducing stroke-related
morbidity and mortality in Europe.
• Rate of IV t-PA=18%
• Rate of EVT=5%
Delivery target
• 3 stroke units / 1.000.000
• 1 comprehensive stroke centre / 1.000.000
Access target

SVIN: MT2020 Global Alliance

• In 2012, Zaidat et al1 estimated LVO to be • 4% to 14% of the total of 675,000 ischemic strokes in the US
• Thus MT eligible patients is the US may range from • 27,000 to 97,000 patients annually
• Other estimates of LVOs are approximately • 9% to 27% of the total, yielding estimates of 60,750 to 182,250 total LVO in the US
• Total MTs in USA estimated in 2016 was estimated to be under 20,000, a large gap between the need and MT performed.
• Worldwide estimate of 10% LVO yields a staggering 1.7M LVO annually
• Total MTs worldwide in 2016: <100,000
The Access Gap in MT: 2016-
1. Zaidat OO, Lazzaro M, McGinley E, et al. Demand-supply of neurointerventionalists for
endovascular ischemic stroke therapy. Neurology 2012;79:S35–41.

MT 2020: Current US & World MT Procedure Estimates
• US Device Industry estimates– 2015: 10,000– 2016: 20,000– 2017: 32,000– 2018: 45,000– 2020:? 70,000-80,000
• Worldwide Device Industry estimates– 2016: 79,000
• 22k US, 27k Europe, 30k Asia, Australia
– 2017: 106,000• 32k US , 30k Europe, 43k: Asia,
Australia
– 2018: 156,000– 2019: Projected 198,000
– 2020: Goal 3020,000
• MT total numbers tracking by “triangulation” method– Sales– Independent research
organizations– Public Hospital and Procedure
Statistic Databases

Physical Access to MT in USA: Travel Distance to Thrombectomy
• Access to acute stroke intervention for LVO patients in the US in evolution over last decade1.
• 2011: 56% of the U.S. population had access within 60 min by ground to endovascular stroke treatment-capable hospitals2
• Recent modeling data3, with an assumption of addition of 20 optimally located CSCs per state, estimate that – 63% of the U.S. population would have 60-min ground
access and 83% would have 60-min ground/ air access to a CSC (57).
1. Khandelwal et al. J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6 Acute Ischemic Stroke Intervention June 7 2016 : 2631 – 4 42642
2. Adeoye O, Albright KC, Carr BG, et al. Geographic access to acute stroke care in the United States. Stroke 2014;45:3019–24.
3. Mullen MT, Branas CC, Kasner SE, et al. Optimization modeling to maximize population access to comprehensive stroke centers. Neurology 2015; 84:1196–205.

MT2020: Vision & Goals
• To be a global, metric-driven, umbrella campaignto reduce death and disability associated with LVO ischemic stroke by accelerating access to Mechanical Thrombectomy through:1. Integrating the disparate knowledge of barriers to
MT access worldwide
2. Unify multiple efforts by local and specialty societies to accelerate MT access globally.
3. Globally double the access to MT every 2 years
4. Aim for a goal of 302,000 MT worldwide in 2020

MT 2020: Outcome Metrics
1. Global Total MT = or >3020,00 in 2020
2. Double access to MT every 2 years

How Do Treatments Diffuse?Everett Rodgers Model
19Access is constrained by information, facilities and physicians and financial access. Will there be enough specialists for early majority and late majority stages. How will the association control growth and be relevant?
Nu
mb
er
of
Ne
w P
atie
nts
wit
h A
cce
ss
Time and Increase in Access (percentage of population)
Area Under Graph Shows Percentage of Population with Access

Developed Country Access
0.00
2.00
4.00
6.00
8.00
10.00
Acc
ess
Sco
re
Time
Developed Countries Normal Developed Countries MT2020
20
MT2020

Developing Country Access and MT2020 Goals
0.00
2.00
4.00
6.00
8.00
10.00
Acc
ess
Sco
re (
0-1
0)
Time
Developing Countries Normal Developing Countries MT2020
21
MT2020

Barriers to Thrombectomy Access
• Information and Diagnostic Access– availability of information about LVO and triage,
• to specialists; general and emergency care physicians; health care professionals (EMT, nurses); hospitals; clinics; insurance firms; policy-makers; and, patients.
• Physical Access– ability to access Mechanical Thrombectomy procedure for LVO
• distance to facilities; availability of specialty/expertise in the local area; availability of equipment/devices; and, driven by increased volume of patients (through protocols).
• Financial Access– insurance (private or public); ability to pay for MT; speed of
access to payment; and, payment lag (before/at service/after service).
22

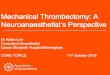
MT 2020 2018 Pilot Survey Project: MT Access Scores 2018
6.71
8.68.23
7.29
9.08
8.5
4.29
6.577.1
0
1
2
3
4
5
6
7
8
9
10
Number of LVO's Rx with MT Physical Access Financial Access
Combined Urban (80.7% of Population) Rural (19.3% of Population)
LVO MT Access and Physical Access; Difference Between Urban and Rural p<0.01Financial Access: Difference Between Urban and Rural p<0.05

MT 2020 GA Overall Approach: Regional MT Access Scoring based Public Health
InterventionsMT Access Score: 3 Pillars (IPF) with
0-10 score1. Information and Diagnostic Access
– availability of information about LVO and triage, • to specialists; general and emergency care
physicians; health care professionals (EMT, nurses); hospitals; clinics; insurance firms; policy-makers; and, patients.
2. Physical Access– ability to access Mechanical Thrombectomy
procedure for LVO • distance to facilities; availability of
specialty/expertise in the local area; availability of equipment/devices; and, driven by increased volume of patients (through protocols).
3. Financial Access– insurance (private or public); ability to pay for MT;
speed of access to payment; and, payment lag (before/at service/after service).
MT Access Interventions: IPF Interventions
1. Accelerate LVO Diagnosis and Treatment Information & Awareness
2. Accelerate Physical Infrastructure for MT
3. Accelerate Financial Ecosystem for LVO MT treatment
24

MT2020 : 2019 Interventions#1 Global Intervention—
White Paper for Health Policy Makers :• Objective :
– Develop a White Paper that provides policy-makers with data on LVOs and why a global/national/regional and local strategy to increase Mechanical Thrombectomy is needed. There will be three versions of the report for High-Income, Low-Income and Very Low-Income Countries.
• White Paper :“Building Stroke Thrombectomy Systems of Care In Your Region: Why & How “
– Executive Summary– Strokes and Mission Thrombectomy
• The Basics of LVO• The Context of the Problem• Delivery of Mechanical Thrombectomy
– The Health Economics of Treating LVOs• Cost of Non-treatment—Compare to the Cost of Treatment
– Goals and Objectives for Global/National/Regional and Local governmental and other institutions.
– Proposed Strategies– Conclusion
25

MT2020 : 2019 #2. Global Intervention—
• OBJECTIVE– Develop strategies to increase Mechanical
Thrombectomies in High-Income, Low-Income and Very Low-Income Countries. The focus will be on information, training,
1. Patient Journey Educational Materials: (HI,LI, VLI Countries) – Develop a Patient Journey (will aid policymakers and
infrastructure development). – SVIN will develop the new model.
26

MT2020 : 2019 #3 Global Intervention—Increase Infrastructure and
Payment (LI, VLI countries)
i. International Thrombectomy Stroke Certification Programs: SNVI-SVIN Self Attestation TSC Certification
ii. Develop Innovative MT Payment Methods for Low-Income Countries and Very Low-Income Countries.
27

Stroke Thrombectomy Center Certification for Low Income Countries
(LIC): To be finalized

MT2020 : 2020 Interventions In Planning
• White Paper in Collaboration with SNIS:
– Rural Access to Stroke Thrombectomy in the US
• White paper in collaboration with WFITN:
– Global Demand for Mechanical Thrombectomy and Supply

MT 2020 Smartphone App:Real-time Global and Individual Thrombectomy Tracker
• MT2020 App tracks & stores de-identified MTs
performed throughout the world by individual
neurointerventionalists
• Users can keep a track of their case log with getting
details of the procedures performed in their region
and around the globe.

MT 2020 Smartphone App: Download from App store
• Find it on your smartphone in iPhone or Android
APP store: Search for “MT2020”
• Compatibility: Requires iOS 8.0 or later.
Compatible with iPhone, iPad, and iPod touch.
• Website for app: www.mt2020.org
• Email: [email protected]

Physician Log In

Account Registration

You will receive activation email / password shortly …

Home Page – you are able to view thrombectomy centers within your
region

Add New Case – Fill basic patient info


Download case log as pdf for your personal record

Surrogate Account
• Your assistants (PA / Nurse Practitioner / Trainee Fellow) can add cases under your name through a separate login
• You assistant can add cases under multiple supervisors

Assistant Log In

Account Registration

You will receive activation email / password shortly …

First time log in … select your center … you can choose multiple centers

Select your supervising physician

Click the request icon

Your supervising physician will need to accept your request

MT2020 Website Launched (Dr. Aroor): World Stroke Day, October 29th, 2019
https://missionthrombectomy2020.org/

MT2020 FB Page

MT 2020: Conclusions
1. MT 2020 is a global multi-stakeholder public health campaign to accelerate thrombectomy access for LVO stroke patients with the ultimate goal to lower the death and disability from acute ischemic stroke worldwide
2. The campaign hopes to see a goal of >3020,00MT in one year by end of 2020– A feasible goal, in light of the near doubling of the
number of MT from 2016 to 2018 to 100,000

MT 2020 GEC In Person Meeting
• GEC in-person Meeting planned at ISC 2020
• White Paper to be finalized and discussed at the meeting
• Roundtable discussion on best practices to increase access to high quality mechanical thrombectomy.

MT 2020: Conclusions
3. The MT 2020 US Pilot survey of Interventional Neurologists (IN) in the US found:
1. As expected, estimated MT Access scores are significantly lower in rural US as compared to urban areas on all three pillars of MT access
2. MT experts appear to overestimate the the number of LVO’s getting thrombectomy in the US by several fold.
1. Develop strategies to inform.
3. Physician and facility payment for MT in the US is perceived as inadequate by MT experts.
1. Develop strategies for informing payers.
4. 2019 efforts in the MT 2020 campaign will focus on1. White Paper on Cost-effectiveness for Health Policy Makers at 3 country
levels.a. Patient Journey Materials, b. Thrombectomy Center Certification for LI and VLI countries c. Innovative Payment Models for payment models for LI and VLI countries

Thank you for your support for MT2020 Global Alliance!!

GLOBAL EXECUTIVE COMMITTEE

DISCLOSURES
CONSULTANT:
SIEMENS
CERENOVUS
PENUMBRA

GLOBAL BURDEN OF STROKE
STROKE
SECOND LEADING CAUSE OF DEATH WORLDWIDE
THIRD LEADING CAUSE OF DISABILITY
LEADING CAUSE OF DEMENTIA
PRIMARY CAUSE OF DEPRESSION
Global Burden of Diseases report 2013:
GLOBAL STROKE INCIDENCE: 10.3 MILLION (>14 MILL NOW)
MORTALITY: 6.5 MILLION
STROKE SURVIVORS: 25.7 MILLION
3-5% OF ALL HEALTH EXPENDITURE ($183 billion by 2030 in the US)
Feigin VL, Krishnamurthi RV, Parmar P, Norrving B, Mensah GA, Bennett DA, et al. Update on the Global Burden of Ischemic and Hemorrhagic Stroke in 1990-2013: The GBD 2013 Study. Neuroepidemiology. 2015;45(3):161-76.
Walter Johnson, Oyere Onuma, Mayowa Owolabi, Sonal Sachdev. Stroke: A Global Response is Needed. Bulletin of the World Health Organization 2016;94:634-634A. doi: http://dx.doi.org/10.2471/BLT.16.181636


WHO DATA
70% of strokes and 87% of both stroke-related deaths and disability-adjusted life years occur in low-
and middle-income countries
The stroke incidence in low- and middle-income countries has more than doubled over the last 40
years
Stroke occurs 15 years earlier in people living in low- and middle-income countries

MAJOR CHALLENGES
Lack of stroke centers (comprehensive/stroke care centers)
Improper/inefficient transport systems
Lack of stroke expertise
Deficient health infrastructure, man power and logistic facilities
Travel times
Financial crisis
Vivek Nambiar. Growing Burden of Stroke, Recent Advancements in Management and Global Commitments: The Way Forward. Editorial, Journal of Pharmacy
Practice and Community Medicine.2018

MT2020 GLOBAL EXECUTIVE COMMITTEE
GEC: MT2020 GLOBAL NETWORK
GOAL: to facilitate outreach to regions around the world with annual public health interventions
that will accelerate access to stroke thrombectomy
Implementation of top 5 public health interventions each year
Evaluation of local/regional structures
Synergistic work with other stroke health organizations

Chairs Committee
Dr. Violiza
Inoa
Coordinating
Chair, USA
Global Executive Committee (GEC)
Dr. Sheila
Martins
Co-Chair
Brazil
Dr. Werner
Hacke
Co-Chair
Germany
Dr. Andrew
Demchuk
Co-Chair
Canada
Dr. Thomas
Leung
Co-Chair
Hong Kong
Country Liaison Regional Sub-Committees
Country
Liaison
Leadership
CommitteePMO
• Chair - Dileep R.
Yavagal, MD
• Vice-Chair - Ashutosh
Jadhav, MD, PhD
• Ameer Hassan, DO,
FSVIN
• Vallabh Janardhan, MD,
FSVIN
• Violiza Inoa, MD
• Italo Linfante, MD,
FAHA, FSVIN
• Raul Nogueira, MD,
FSVIN
• Robin Novakovic, MD,
FSVIN
• Osama (Sam) Zaidat,
MD, MSc, FSVIN
• Syed Zaidi, MD
• Ossama Yassin, MD
• Urs Fischer, MD
Chair, Stroke
Chair, MT
Board Member #1
Board Member #2
Board Member #3
•Orbees Medical
Anurag Mairal, PhD
Shyam Venkatesh, PhD
- Project Management
- Strategy Consultant
•Asutosh Jadhav, PhD
- Consultant
• Jennifer Potter-Vig, PhD
- Project Manager, SVIN
Regi
on _
__
_____
Advisory
Committee
• Society
Liaisons
o ASA/AHA
o ESO
o MENA-SINO
o WSO
o SNIS
o WFITN
• Ralph Sacco
• Larry Goldstein
• Anne
Alexandrov
• Endorsing
Organizations
o ANZ – AN
o 5T-Stroke
o SISS
o KNANN
o NCS
o NVX
o SNVI
TBA
Co-Chair
China

GEC STRUCTURE
Chairs Committee. The GEC Chair committee will provide the overall leadership for this global outreach
by coordinating with regional committees throughout the globe.
The Chairs Committee will be constituted of the coordinating chairperson and four-five co-chairs
Regional Sub-Committees. MT 2020 GEC public health interventions will be deployed globally with
specific local-level actions led by a regional committee of five members
Stroke Chair: heads region-specific actions addressing the stroke landscape including barriers and drivers
to treatment
MT Chair: heads region-specific actions addressing the increase of patient access to MT
Board Members: three board members who will support the execution of the initiatives at the local level
Country Liaison. The regional-level activities will be managed by a country-based liaison representing the
various regions at the country level

GEC SUPPORT
Leadership Committee. The MT 2020 leadership committee will have a “think-tank” role and will be
responsible for developing and planning the initiatives in collaboration with the GEC and the Advisory
Board
Project Management Office: The project management office will coordinate and provide overall
support to the activities of the GEC and MT 2020
Advisory Board. The advisory board will be comprised of clinical, industry, and society/policy thought
leaders that will provide overarching advice and direction to the GEC and MT 2020

GEC CHAIRS
Dr. Werner Hacke Dr. Sheila Martins
Dr. Andrew Demchuk
Dr. Thomas Leung Dr. Violiza Inoa

BOARD MEMBERS FROM 40 COUNTRIES SO FAR…

Country Liaisons
Dr. Thanh Nguyen Canada
Dr. Edgar Samaniego Ecuador
Dr. Diogo Haussen Brazil
Dr. Alberto Maud Argentina
Dr. Alex B. Chebl Lebanon
Dr. Ali Alaraj Lebanon
Dr. Mohammad Jumaa Syria
Dr. Jeffrey Katz Israel
Dr. Wondwossen Tekle Ethiopia
Dr. Sherman Chen Taiwan
Dr. Thanh Nguyen Vietnam
Dr. Jawaad Kirmani Pakistan
Dr. Qaisar Shah Pakistan
Dr. Tanzila Shams Bangladesh
Dr. Thomas Oxley Australia
Dr. Andrei Alexandrov Russia
Dr. Osman Kozak Turkey
Dr. Marc Ribo Spain
Country LiaisonsDr. Tibor Becske Hungary
Dr. Tudor Jovin Romania
Dr. Viktor Szedor Czech Republic
Dr. Alexander Venizelos Greece
Dr. Yafel Serulle Dominican Republic
D. Stelios Smirnakis Greece
Dr. Luis Suazo Dominican republic
Regional Board Members
Dr. Pedro Lylek Argentina
Dr. Jin Soo Lee South Korea
Dr. Bernard Yan Australia
Dr. Monika Killer Austria
Dr.Tommy Anderson Belgium
Dr. Francisco
Montalverne Brazil
Dr. Mayank Goyal Canada
Regional Board Members
Dr. Bijoy Menon Canada
Dr.Thomas Leung China
Dr.Vladimir Kalousek Croatia
Dr. Olav Jansen Denmark
Dr. Swarup Chawla England
Dr. Sanjeev Nayak England
Dr. Mikael Mazighi France
Dr. Michel Poitin France
Dr. Marius Hartmann Germany
Dr. Istvan Szikora Hungary
Dr. Gigy Kurutukulam India
Dr. Chandril Chugh India
Dr.Vikram Huded India
Dr. P.N Sylaja India
Dr. Mathew Cherian India
Dr.Vipul Gupta India
Global Executive Committee Board Members – Work In Progress

Regional Board Members
Dr.Vivek Gupta India
Dr.Ajay Kumar India
Dr. Paritosh Pandey India
Dr. Guy Raphaeli Israel
Dr. Salvatore Mangiafico Italy
Dr. Noboyuki Sakai Japan
Dr. Michel Mawad Jordan
Dr. Geert Lycklama Netherlands
Dr. Manuel Moquillaza Peru
Dr.Adam Kobayashi Poland
Dr. Mario Martinez Galdamez Spain
Dr. Michael Soderman Sweden
Dr. Paolo Machi Switzerland
Dr. Zsolt Kulcsarz Switzerland
Dr. Erol Akgul Turkey
Dr. Saruhan Cekirge Turkey
Global Executive Committee Board Members – Work In Progress

GEC IMMEDIATE NEXT STEPS
Request to all GEC members to develop regional sub-committees – recruitment and invitations
Physician stakeholders
Other stakeholders (allied healthcare workers)
Finalize regional committees
Launch a survey to obtain regional level feedback
GEC board member meeting at ISC 2020 (February 19-21)
Discussion and implementation of the White Paper: “Building Stroke Thrombectomy Systems in
your Region: Why and How?”
Plan: regional committee members would take the white paper and communicate to local
health policy makers
White paper could be customized to regional needs

GEC RESOURCES FOR REGIONAL SUBCOMMITTEES
CONTINUED INTERACTION AND SUPPORT
Bidirectional feedback and brainstorming on local stroke systems of care
Stroke education/training – facilitating clinical observerships
Resources for plan implementation
Grant writing support

GEC COMMUNICATION
WhatsApp – MT2020 GEC
Email – [email protected]
MT2020 Website – www.missionthrombectomy2020.org
Facebook – https://www.facebook.com/MT2020Stroke/

THANK YOU

Agenda
12th Annual SVIN Meeting, Atlanta, GA , Nov 21st, 2019
1. Welcome, Introductions
2. MT 2020 – Mission, Scope, Initiatives
3. GEC – Charter, Structure, Scope
4. Project Management
5. Wrap Up – Thank You and Next Steps

San Francisco Bay Area management and strategy consulting firm focused on Healthcare
50+ cumulative years experience in the Neurovascular space
Closely track the evolution of stroke treatment across the globe
Experience with 30+ countries – with focus on improving Patient Access to interventional
therapies

ROLE OF ORBEES MEDICAL
Coordination
Project Management
Communication Strategy

Agenda
12th Annual SVIN Meeting, Atlanta, GA , Nov 21st, 2019
1. Welcome, Introductions
2. MT 2020 – Mission, Scope, Initiatives
3. GEC – Charter, Structure, Scope
4. Project Management
5. Wrap Up – Thank You and Next Steps