Embed Size (px)
Citation preview

Missed Opportunities to Diagnose COPD
Daryl Freemanon behalf of the Study Collaborators

CollaboratorsResearch in Real Life, Cambridge
David Price
Julie von Ziegenweidt
Laurence Mascarenhas
Annie Burden
Alison Chisholm
Independent experts
David Halpin: Royal Devon and Exeter Foundation Trust, Exeter, UK
Eric Batemen: University of Cape Town, Cape Town, South Africa
Daryl Freeman: Mundesley Medical Practice, Norfolk, UK
Dermot Ryan: Woodbrook Medical Centre, Loughborough, UK
Rupert Jones: PeninsulaCollege of Medicine and Dentistry, University of Plymouth, UK
Respiratory Programme, Department of Health, UK
Robert Winter
Sue Hill
Kevin Holton
Anne Moger
Matthew Kearney

Diagnostic iceberg
• Among smokers with no prior history of obstructive lung disease, 18.7% have COPD1
• Amongst patients currently treated with asthma therapy and no diagnosis of COPD, 24.5% have COPD2
Tinkelman DG, Price DB, Nordyke RJ, Halbert RJ. Misdiagnosis of COPD and Asthma in Primary Care Patients 40 Years of Age and Over. J Asthma. 2006;43:75-80.

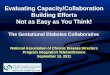
Population studies consistently demonstrate underdiagnosis of COPD is high
1. Soriano et al. Lancet 2009
Estimates of COPD underdiagnosis are substantially higher than those forhigh blood pressure, hypercholesterolemia and other similar disorders1
Cáceres,
Spain
Oviedo, S
pain
Sevil
le, Spain
Mexico
City, M
exico
Biscay,
Spain
IBERPOC, Spain
Poland
Madrid
, Spain
Burgos,
Spain
Caracas
, Venezu
ela
OLIN, S
weden
PLATIN
O, Lati
n America
Säo Paulo, B
razil
Santiag
o, Chile
Manlle
u, Spain
Montevideo, U
rugu
ay
Region
20
15
10
5
0
Prev
alen
ce (%
)
100
80
60
40
20
0
Underdiagnosis (%
)
DiagnosedUndiagnosed
% underdiagnosis

Dr Daryl Freeman
• Conflict of interests– DF has received honaria for speaking from
• AZ, BI, Napp, Novartis,Meda,Chiesi,Teva, Almirall
– DF has received educational support/grants/attendance at conferences from
• Napp, Teva, AZ, Pfizer

Daryl Freeman

Missed Opportunities
• Missed opportunities to identify patients in Primary Care
• Co- morbidities: should we screen for COPD in our CDM clinics?
• Questionnaires vs Opportunistic screening
How can we identify more patients with a COPD Diagnosis?

MISSED OPPORTUNITIES

COPD: mis- and under-diagnosed disease• UK Department of Health’s National COPD
Outcomes Strategy1, states that around:– 835,000 are currently diagnosed with COPD in England – 2,200,000 undiagnosed COPD
• Screening study in patients >40 years2
undiagnosed spirometrically-defined COPD in:– 1/5 of smokers – 1/4 of “asthma” patients
1. Department of Health. 2011. http://www.dh.gov.uk/publications 2. Tinkelman DG, Price DB, Nordyke RJ, Halbert RJ. J Asthma 2006;43(1):75–80

COPD in the UK: National Strategy• The Outcomes Strategy was published by the UK
Department of Health in July 2011.1
– Provides a framework for achieving improvements in COPD outcomes in England.
– Notes that too many people are being diagnosed too late in the disease to the detriment of the NHS and patients.
1. Department of Health 2011. http://www.dh.gov.uk/publications

Study rationale
• Early diagnosis and intervention in the management of symptomatic COPD may reduce:1
– Impact on patients • Exacerbation reduction• Lung function decline
– Rate of disease progression– Economic burden on health systems.
1. Price D, Freeman D, Cleland J, Kaplan A, Cerasoli F. Prim Care Resp J. 2011;20(1):15-22.

Aim
• To use large primary care clinical databases to:– Characterise the current COPD population– Ascertain the stage at presentation – Evaluate the consultation pattern prior to
diagnosis– Identify flags to aid in earlier diagnosis

Methods
• Retrospective observational study• Routine practice data (1990 - 2009) • Pooled from the databases
– General Practice Research Database (GPRD) www.gprd.com
– Optimum Patient Care Research Database (OPCRD) www.optimumpatientcare.org

Inclusion criteria
• Aged ≥40 years• Received a COPD diagnosis between 1990–
2009 (i.e. a Read Code for COPD)
• Minimum 3 year continuous practice data:– ≥2 years pre diagnosis– ≥1 year post diagnosis
• On current COPD therapy:– ≥2 COPD prescriptions in the year after COPD
diagnosis

Patient inclusion Flow Chart
Exclusion Criteria: 1) Age ≤40
1,220
2) Inadequate data12,458
3) ≤1 COPD prescription in the year after COPD diagnosis
13,655
Exclusion Criteria:1) Diagnosed prior 1990
2) <12 months of outcome data after diagnosis
9,452
FIRST COPD diagnosis after 1990 66,232
Meet inclusion criteria38,859
OPCRD 10,876GPRD 27,983
.
COPD Diagnosed patients 75,984
All Patients1,122,787
OPCRD 307,410GPRD 815,377

Study population = 38,859
Gender (male) 52.6%
Smoking status(data from 73%)
Non-smoker 8.9%
Current Smoker 45.7%
Ex-smoker 45.4%

Severity of COPD at time of diagnosis (available in 38%)
24% of all patients had FEV1/FVC ≥0.7:
– All had clinical diagnosis but not spirometrically confirmed
– Of these 54% have FEV1 % predicted 50–80%
FEV1 /FVC Ratio ≥ 0.7
Mild (FEV1 ≥ 80%)
Moderate (50% ≤ FEV1<
80%)
Severe (30% ≤ FEV1< 50%)
Very Severe (FEV1 ≤ 30%)
0
5
10
15
20
25
30
35
40
45
Pe
rce
nta
ge
of
pa
tie
nts

Severity at diagnosis over 20yrs
13 January 2011 COPD strategy database analysis 19
COPD CDM payment started

Age
40-49 50–59 60–69 70–79 80–89 90–99 ≥1000
5
10
15
20
25
30
35
4.9%
18.2%
32.6% 31.8%
11.6%
0.9% 0
Age distribution
Age category (years)
Pe
rce
nta
ge
of
pa
tie
nts
Median age 68 years (IQR 60-75 years)

Age of diagnosis over 20yrs
• Age of diagnosis is not changing in any severity category

Lower respiratory consultations in 2 years prior to COPD diagnosis
On average patients visited their general practitioner:
• For lower respiratory (LR) symptoms 2.8 times
• 56% had ≥2 consultations for LR symptoms
• 21% had at least 5 consultations
In our practice patients who have a smoking history and present with LRTI symptoms are referred for spirometry
when stable

Lower respiratory symptom consultations over time
•Mean number of LR symptom consultations / patient / year increased over 20 yrs before diagnosis:– 20 yrs: 0.01– 10 yrs: 0.25– 5 yrs: 0.53– 1 yr: 1.85
-20 -19 -18 -17 -16 -15 -14 -13 -12 -11 -10 -9 -8 -7 -6 -5 -4 -3 -2 -10
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
Years prior to receiving a COPD diagnosis
Me
an
nu
mb
er
of
LR
co
ns
ult
ati
on
s /
pt
/ y
ea
r

Exacerbation frequency in 2 yrs before diagnosis and LR consultations over 10yrs
-10 -9 -8 -7 -6 -5 -4 -3 -2 -10
10
20
30
40
50
60
70
80
0–1 exacerbations in the 2 years prior to COPD diagnosis
≥2 exacerbations in the 2 years prior to COPD diagnosis
Years prior to COPD diagnosis
Pe
rce
nt
of
pa
tie
nts
wit
h ≥
2 a
nn
ua
l L
RT
I c
on
slu-
tati
on
s

Persistent exacerbation phenotype in COPD
For patients with multiple exacerbations in the year before diagnosis : • Odds ratio of ≥2 exacerbations in the:
• Further analyses planned to investigate whether treatment reduces the exacerbation frequency in such people
OR (95% CI)
First year after diagnosis 4.34 (4.13, 4.57)*
Second year after diagnosis 3.54 (3.36, 3.73)**
* Adjusted for age, gender, place of diagnosis & year of diagnosis ** Adjusted for age, gender & year of diagnosis

Chest X-rays over time
-20-19-18-17-16-15-14-13-12-11-10 -9 -8 -7 -6 -5 -4 -3 -2 -10
0.05
0.1
0.15
0.2
0.25
0.3
Years prior to COPD diagnosis
Me
an
nu
mb
er
of
Ch
es
t X
-ra
ys
/ p
a-
tie
nt
/ y
ea
r• Over the 20 years preceding their COPD diagnosis, Chest X-rays increase steadily• In 2 yrs before diagnosis:
o 22% had a Chest X-ray, 7% >1 chest X-rays

Primary vs secondary care diagnosis • The majority of patients are diagnosed in primary care:
99% (n=38,480) versus 1% (n=379)
• Multiple “COPD exacerbations” in the 2 yrs before diagnosis occurred in:– 41% diagnosed in secondary care – 35% diagnosed in primary care (p=0.007)
• Diagnosis in secondary care is usually late and represents delayed diagnosis

So has there been progress over 20 years?
• Early diagnosis is slowly improving.• In a large dataset we have shown in 2yrs before
diagnosis, there are opportunities to diagnose COPD– 56% consulted multiple times for LR symptoms– 26% consulted multiple times for LRTIs:– 22% of patients had a chest X-ray– Consultations increase in frequency prior to diagnosis– Diagnosis in secondary care is usually late

CO- MORBIDITIES: SHOULD WE SCREEN FOR COPD IN OUR CDM CLINICS?

Co-morbidities of COPD
COPD

Co-morbidities of COPD
COPD
UNRELATED
OsteoarthritisCirrhosis

Co-morbidities of COPD
COPD
UNRELATED
OsteoarthritisCirrhosis
SHARED RISK
Lung CancerCardiovascular

Co-morbidities of COPD
COPD
UNRELATED
OsteoarthritisCirrhosis
THERAPY
OsteoporosisDiabetes
SHARED RISK
Lung CancerCardiovascular

Co-morbidities of COPD
COPD
UNRELATED
OsteoarthritisCirrhosis
SYSTEMICCONSEQUENCES
CardiovascularMuscle Dysfunction
Metabolic Syndrome
THERAPY
OsteoporosisDiabetes
SHARED RISK
Lung CancerCardiovascular

Accelerated ageing may underlieboth COPD and co-morbidities
Cigarette smoke and other pollutants may accelerate lung aging
ROS = reactive oxygen species Ito et al. Chest 2009
Senescence ROS
mitochondria
InflammationStructural change
Increased risk of cancerCell death
Normal aged lung (senile lung) Accelerated aged lung (COPD lung)
Environmental ROS (Tobacco, kitchen smoke)
DNA damage Kinase activation (MAPK, PI3K
NFkB activation Oxidation/nitration of proteins,
Reduction of anti-aging molecules (sirtuin, HDAC etc.),
Telomere shortening, Defect of proteasome etc…

COPD is associated with a high prevalence of co-morbidities
Patie
nts
with
CO
PD re
porti
ng c
ondi
tion
(%)
Hypertension Hyper-cholesterolemia
Depression Cataracts Osteoporosis
Data from telephone survey carried out among 1,003 US patients with COPD in 2006
5357
54
49
44
2731 32
39
12
60
50
40
30
20
10
0
Barr et al. Am J Med 2009

Cardiovascular mortality in COPD
For every 10 % decrease in FEV1 in mild to moderate
COPD:
•Cardiovascular mortality increases by 28%
•Non-fatal coronary events increase by 20%
Anthonisen et al, AJRCCM 2002

Co-morbidities of COPD
COPD
UNRELATED
OsteoarthritisCirrhosis
SYSTEMICCONSEQUENCES
CardiovascularMuscle Dysfunction
Metabolic Syndrome
THERAPY
OsteoporosisDiabetes
SHARED RISK
Lung CancerCardiovascular

Diabetes
• Diabetes is highly prevalent among patients with COPD – Proportion of patients:
• 13–22%1 • 25–26%2
• Patients with COPD have a 2-fold greater risk of diabetes than individuals without COPD3
1. Sin et al. Circulation 2003; 2. Barr et al. Am J Med 2009; 3. Feary et al. Thorax 2010; 4. Mellbin et al. Eur J Cardiovasc Prev Rehabil 2010

Anxiety and Depression
• Both major comorbidities in COPD1–4
– Associated with poor prognosis4,5
• Estimates vary on prevalence of depression (8–80%) and anxiety (6–64%) in COPD2,6
– Lack of methodological consensus
• Abnormal (≥10 points) Hospital Anxiety and Depression Scale (HADS) scores in COPD patients (n=701) entering pulmonary rehabilitation:7
– Anxiety: 32%– Depression: 27%
1. Hanania et al. Am J Respi Crit Care Med 2011; 2. Kunik et al. Chest 2005; 3. Maurer et al. Chest 2008; 4. Ng et al. Arch Intern Med 2007; 5. Eiser et al. Thorax 2010;
6. Yohannes et al. Int J Geriatr Psychiatry 2010; 7. Janssen et al. Chron Respir Dis 2010

Active comorbidities at the time of diagnosis of COPD
A collaborative observational study carried out by the UK Department of Health and Research in Real Life collaborative
and independent respiratory experts

CollaboratorsDavid Price: Centre of Academic Primary Care, University of Aberdeen, UK; Research in Real Life, Cambridge, UK
David Halpin: Royal Devon and Exeter Foundation Trust, Exeter, UK
Robert Winter: Respiratory Programme, Department of Health, UK; East of England Strategic Health Authority, UK
Sue Hill: Respiratory Programme, Department of Health, UK
Eric Batemen: University of Cape Town, Cape Town, South Africa
Daryl Freeman: Mundwsley Medical Centre, Norfolk, UK
Dermot Ryan: Woodbrook Medical Centre, Loughborough,and University of Edinburgh, UK
Matthew Kearney: Respiratory Programme, Department of Health, UK;
Kevin Holton: Respiratory Programme, Department of Health, UK
Anne Moger: Respiratory Programme, Department of Health, UK
Julie von Ziegenweidt: Research in Real Life, Cambridge, UK
Laurence Mascarenhas: Research in Real Life, Cambridge, UK
Annie Burden: Research in Real Life, Cambridge, UK
Alison Chisholm: Research in Real Life, Cambridge, UK
Rupert Jones: Peninsula Medical School, University of Plymouth, UK

COPD in the UK: National Strategy• An Outcomes Strategy for Chronic Obstructive Pulmonary Disease
(COPD) and Asthma in England was published by the Department of Health in July 2011.1
• The Strategy:1
– Provides a framework for achieving a significant improvement in outcomes for the estimated three million people in England who live with COPD.
– Highlights that COPD is often associated with other conditions, e.g.:• ~40% of people with COPD also have heart disease• Significant numbers have depression and/or anxiety disorder
– Calls for:• Assessment and effective interventions using a holistic care approach where
comorbidities predate the COPD• A holistic approach to monitoring other conditions that may present after the COPD
diagnosis 1. Department of Health. An Outcomes Strategy for Chronic Obstructive Pulmonary Disease (COPD) and Asthma in England. 18 July 2011. Available online at: http://www.dh.gov.uk/publications

Study objective• The research team’s objective was to evaluate the presence of active
comorbidities at the time of patients’ COPD diagnosis. Namely, comorbid:– Asthma– Ischaemic heart disease (IHD)
• Heart Failure, or• Angina, or • Myocardial Infarction
– Gastro-oesophageal reflux disease (GERD) – Diabetes mellitus (DM) – Osteoporosis– Sinusitis– Allergic Rhinitis– Depression and anxiety– Chronic pain

Study rationale
• Comorbidities can potentiate the morbidity of COPD, and vice versa.
• Patients with COPD often die as a result of a comorbidities.
• Understanding the prevalence of comorbidities will help quantify the extent of disease burden of patients living with COPD.

Study design and data• Retrospective observational study using routine
practice data (between 1990 and 2009) pooled from: – General Practice (GPRD)
• Well-validated Primary care database• Anonymised, longitudinal data • Routine clinical data
– Optimum Patient Care Research Databases (OPCRD)• Anonymised data extracted from practices during records-based clinical reviews,
contains: Routine clinical data Patient reported data
• Has been approved by Trent Multi Centre Research Ethics Committee for clinical research use

Inclusion criteria
• Included in the dataset were all patients who were:– Aged ≥40 years– Received a COPD diagnosis between 1990–2009 (i.e. a Read
Code for COPD)
• Minimum 3 year continuous practice data:– ≥2 years pre diagnosis– 1 year post diagnosis
• On current COPD therapy:– ≥2 COPD prescriptions in the year after COPD diagnosis

Data extraction CONSORT
Exclusion Criteria: 1) Age ≤40 OPCRD (n = 660) GPRD (n = 560)
2) Patients without 2 years’ data prior to and 1 year’s data after diagnosis. OPCRD (n=3,391) GPRD (n = 9,107)
3) ≤1 COPD prescription in the year after COPD diagnosis (any of SABA / LABA / ICS / SAAC / LAAC / LTRA / THEO) OPCRD (n= 3,884) GPRD (n = 9,771)
Valid COPD Patients(n = 38,859)
OPCRD (n = 10,876)GPRD (n = 27,983)
Exclusion Criteria:1) Patients whose COPD was diagnosed prior 1990
2) Patients without ≥12 months of outcome data after their COPD diagnosis OPCRD (n = 4,291) GPRD (n = 5,161) FIRST COPD diagnosis after 1990
OPCRD (n = 18,811)GPRD (n =47,421)
Identify patients with valid inclusion criteria
1)Age >402)At least 2 years’ of data pre diagnosis and 1 year’s data post diagnosis 3)At least 2 prescriptions for COPD therapy after COPD diagnosis.
COPD Diagnosed patients
OPCRD (n = 23,102)GPRD (n =52,582)
All PatientsOPCRD (n = 307,410)GPRD (n = 815,377)

Study population• Active comorbidities at the time of COPD diagnosis were defined
as follows:
Comorbidity Defined as
Asthma
Diagnostic Code ever prior to COPD diagnosisIschaemic Heart Disease
Osteoporosis
Diabetes Mellitus Diagnostic Code ever prior OR drugs ever prior to COPD diagnosis
GERD
Diagnostic Code in 2 years prior to COPD diagnosis OR diagnostic code ever prior plus drugs in the 2 years prior to COPD diagnosis
Allergic Rhinitis
Sinusitis
Depression / Anxiety
Chronic Pain ≥3 analgesic prescriptions in the 2 years prior to COPD diagnosis

Summary characteristic• A total of 38,859 patients were included in the study
PATIENT CHARACTERISTIC
Sex (male) 52.6%
AgeMean 67.5 (10.4) yearsMedian (IQR) 68 (60, 75) years
Severity of COPD at diagnosis*(data available in 37.8% of patients)
FEV1/FVC ≥ 0.7** 24.3%Mild (FEV1 ≥ 80%) 6.6%Moderate (50% ≤ FEV1< 80%) 38.4%Severe (30% ≤ FEV1< 50%) 24.3%Very Severe (FEV1 ≤ 30%) 5.8%
Smoking status(data available for 73.1% of patients)
Non-smoker 8.9%Current Smoker 45.7%Ex-smoker 45.4%
*Based on FEV1 and GOLD criteria; over the period of this study (1999–2009), CAT scores were recorded in only 4.1% of patients**Of the 24.3% of patients with FEV1/FVC ≥0.7: 65% have ratios between 0.7–0.8 and 54% have FEV1 percent predicted of 50–80%, i.e. would be classified as moderate

Prevalenceof comorbidities(I)
COMORBIDITY Percent of patients
GERD 6.5%
Depression and Anxiety 15.8%
Sinusitis 5.7%
Allergic rhinitis 6.6%
Diabetes Mellitus 18.3%
Ischaemic Heart Disease Diagnosis* 14.9%
Osteoporosis 3.4%
Asthma Diagnosis 33.9%
Chronic Pain Diagnosis 39.8%*Heart failure, Angina or Myocardial Infarction; drugs for IHD drugs indistinguishable from drugs for hypertension

Prevalence of comorbidities (II)• At the time of their COPD diagnosis:
– ~1/3 of patients been diagnosed with asthma at some point– Nearly 40% of patients had received multiple (≥3) prescriptions
for analgesics in the preceding 2 years– ~15% had been diagnosed with ischaemic heart disease in the
prior 2 years– ~16% had received medication for depression and/or anxiety in
the prior 2 years– ~18% of patients had comorbid diabetes

Active comorbidities over time (II)
• Prevalence of asthma remained steady at approximately 30%• Prevalence of all other active comorbidities increased over the 20 years of the
study (see table).
Year of COPD
diagnosis GERD
Depression and
AnxietySinusitis
Allergic rhinitis
Diabetes Mellitus
Ischaemic Heart
Disease
Osteo-porosis Asthma
Chronic Pain
1990 0.6% 7.4% 0% 4.0% 12.6% 6.5% 0.5% 33.4% 17.2%
1995 5.3% 11.9% 1.1% 7.7% 14.2% 13.2% 0.4% 38.7% 34.5%
2000 6.0% 15.4% 2.4% 6.5% 17.0% 16.7% 3.4% 36.0% 40.8%
2001 6.7% 16.8% 2.4% 6.7% 17.0% 17.8% 2.5% 32.7% 40.6%
2005 7.8% 17.2% 3.7% 5.9% 20.5% 16.0% 5.2% 33.2% 46.4%
2009 7.7% 14.6% 2.8% 7.0% 28.9% 11.5% 8.7% 31.0% 40.8%
p-value* <0.001 <0.001 <0.001 0.019 <0.001 <0.001 <0.001 <0.001 <0.001
*Chi squared

Active comorbidities by COPD severity at diagnosis (II)
FVC Ratio >=0.7 Mild Moderate Severe Very Severe.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0
COPD Patients with Co-morbid Diagnoses by GOLD Severity
Asthma IHD Osteoporosis Diabetes Mellitus GERDRhinitis Sinusitis Depression Chronic Pain
GOLD Severity
Pe
rce
nta
ge

Conclusions• These data confirm that active comorbidities are common at the
time of COPD diagnosis.
• Trends over the study period suggest:– Constant diagnosis of asthma– Increased prevalence of active comorbidities– Association between presence of comorbidities and milder COPD at
time of diagnosis
• The increased prevalence of active comorbidities at the time of COPD diagnosis may indicate:– Increased awareness of comorbidities– Improved diagnosis of COPD in patients treated for comorbidities– Effects of national targets, e.g. UK Quality and Outcomes Framework.

Conclusions• Close monitoring of patients with existing conditions present opportunity
for earlier COPD identification and diagnosis.
• Decision support prompts: – Patients with a positive smoking history and either:
• IHD and/or
• Diabetes – should be evaluated for presence of COPD as part of their
reviews
• Integrated, holistic management of patients with COPD (≥GOLD II) is required to optimise care and minimse the morbidity and mortality of patients with COPD (e.g. reduce myocardial infractions and strokes for those COPD patients with comorbid IHD).

QUESTIONNAIRES VS OPPORTUNISTIC SCREENING

Screening in primary care.
• Smoker + cough : – 27 % had COPD.– Have to test 4 patients to find one with COPD.
• Smoker + cough + 1 other risk factor: – 35 % had COPD– Must test 3 patients to find one with COPD.
C P van Schayck BMJ. 2002 June 8; 324 (7350): 1370

So how should we do it?
Soriano J, Price D et al Lancet 2009

Can we target spirometry better in case finding?

Case finding questions– Age group (40-49, 50-59, 60-69, 70+)– Pack-years smoked (0-14, 15-24, 25-49, 50+)– Body mass index– “Does the weather affect your cough?” (Yes/No)– “Do you ever cough up phlegm [sputum] from your chest
when you don’t have a cold?” (Yes/No)– “Do you usually cough up phlegm [sputum] from your chest
first thing in the morning?” (Yes/No: negative association)– “How frequently do you wheeze?” (Ever/Never)– “Do you have or have you had any allergies?” (Yes/No:
negative association)


COPD QuestionnaireQUESTION RESPONSE POINTS
What is your age? 40-49 years50-59 years60-69 years70 + years
048
10
How many cigarettes do you currently smoke each day (if you are an ex-smoker how many did you smoke)? What is the total number of years you have smoked cigarettes?Packs per day = cigarettes per day / 20 per packPacks-year = packs per day x years smoked
0-14 packs-year15-24 packs-year25-49 packs-year50+ packs-year
0237
What is your weight in kg? What is your height in m?BMI = weight / (height x height)
BMI <25.4BMI 25.4–29.7BMI >29.7
510
Does the weather affect your cough? YesNoI do not have a cough
300
Do you ever cough up sputum (phlegm) from your chest when you do not have a cold? YesNo
30
Do you usually cough up sputum (phlegm) from your chest first thing in the morning? YesNo
03
How frequently do you wheeze? NeverOccasionally
04
Do you or have you had any allergies? YesNo
03

Add up the total points based on the patient’s responses.• 17 or more points suggests a moderate to high risk of COPD:
go to COPD Diagnosis Guide .• 16 or fewer points suggest a low risk of COPD:
– consider other diagnoses, including asthma: proceed to the Adult Asthma Questionnaire
– or consider specialist referral.
Interpreting the COPD Questionnaire
- 16 17 18 19 +
Consider other diagnoses (proceed to the Adult
Asthma Questionnaire), or specialist referral
Proceed to COPD Diagnosis Guide

SUMMARY
• Missed opportunities– In Primary Care
• CXRs rather than spirometry
– Secondary Care• Admissions – diagnosis
not being made effectively
• Opportunities– Use other CDM clinics to
identify patients– Educate staff doing
minor illness clinics– Use questionnaires– Use sophisticated
computer interrogation tools
• E.g OPC, GRASP, iCOPD

SCN East of England
• IT tools – http://www.respiratoryfutures.org.uk/regions-and-nations/east-of-
england/announcements/summary-of-it-tools-to-support-respiratory-care-published-by-eoe-rscn-and-pcrs-uk/
• Our priorities with CCGs– Identify patients with COPD– Identify patients at risk of exacerbations– Set up respiratory pathways according to the
needs of their populations– Encourage an holistic approach to breathlessness

The SCN breathlessness algorithm

Questions?