Embed Size (px)
Citation preview

Misplaced Nasogastric Tube: A Serious Preventable Error
By Daniel Haslam, Dr Michael Parris, Nutritional Team

Content• Problem
• Quantifying the problem
• Addressing issues
• Discussion

Problem
• Increasing use of chest radiograph as first line check for NG tube position [2]. Implications include:
- unnecessary radiation exposure - unnecessary expenditure - risk of interpretation errors - Treatment delays
• 2005-2010: 21 deaths, 79 causes of harm due to feeding into the lungs [1].
• Feeding from a misplaced nasogastric tube is a Never Event [1].

Problem
• Training varies between Trusts – A National audit suggests only 31% junior doctors receive
training on use of chest radiograph for interpreting NG tube position [3].

Case Studies• Patient requiring NG feeding.• NG tube resited through night.• Portable chest x ray was viewed by nightshift ITU CT2 who then advised
the nurses to commence feeding. • Patient was fed for approximately 1.5 hours giving 200 ml of feed. • 0850: patient became very distressed, hypertensive, desaturating and
coughed up NG feed into ventilator tubing.• The NG feed was stopped. • Duty ITU doctors were alerted to the problem and patient was reviewed. • The CXR was reviewed and the NG tube was found to be positioned in the
left lung.

Case Studies
• The NPSA is aware of two patient deaths since March 2011 where staff had flushed nasogastric tubes with water before initial placement had been confirmed [4]. – Staff then aspirated back the water (including the
lubricant within the tube).– The mix of water and the lubricant gave a pH
reading below 5.5, and assumed it was in correct position, although the tube was actually in the patient’s lung.

Design
• Questionnaire – Assessed level of training and knowledge
• 1st and 2nd line methods of confirming NG placement
• Three landmarks on a chest radiograph confirming NG placement
Bisects Carina
Crosses hemi-diaphragm
NG tube deviates left
• Quiz• Assessed clinical judgement of 7 random chest radiographs of NG
tube placement [5]• 2 NG tube in correct position• 5 NG tube not in correct position

Baseline measurements (1)61.7% [29/47] response rate.
- 13.8% [4/29] were aware of the National Patient Safety Agency (NPSA) guidelines
- 6.9% [2/29] received training, both informally.

Baseline measurement (2)1st line check for NGT placement
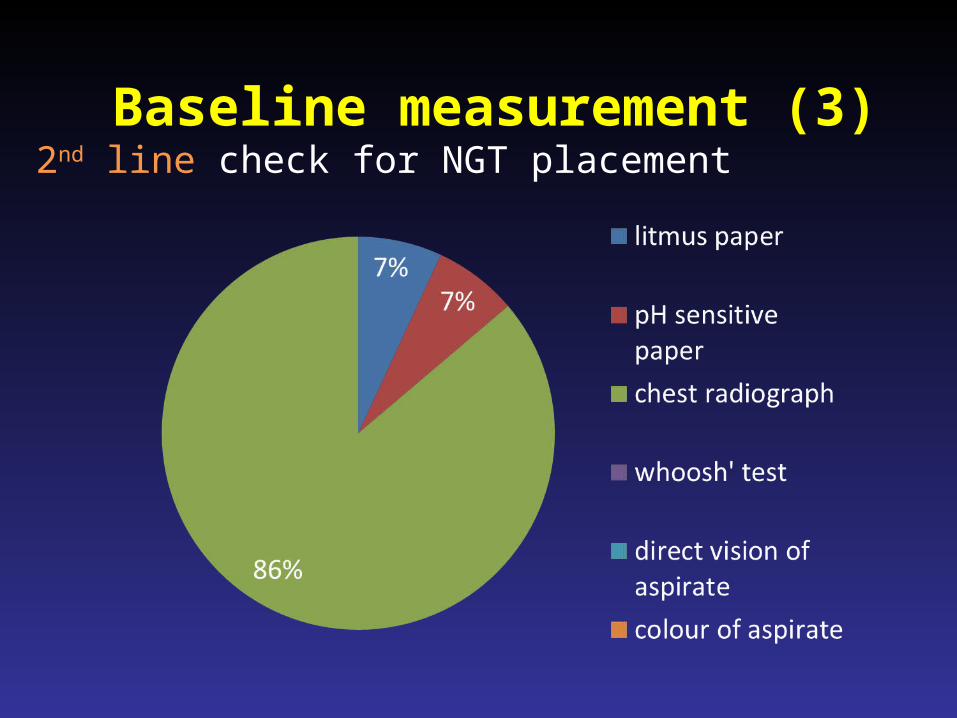
2nd line check for NGT placementBaseline measurement (3)
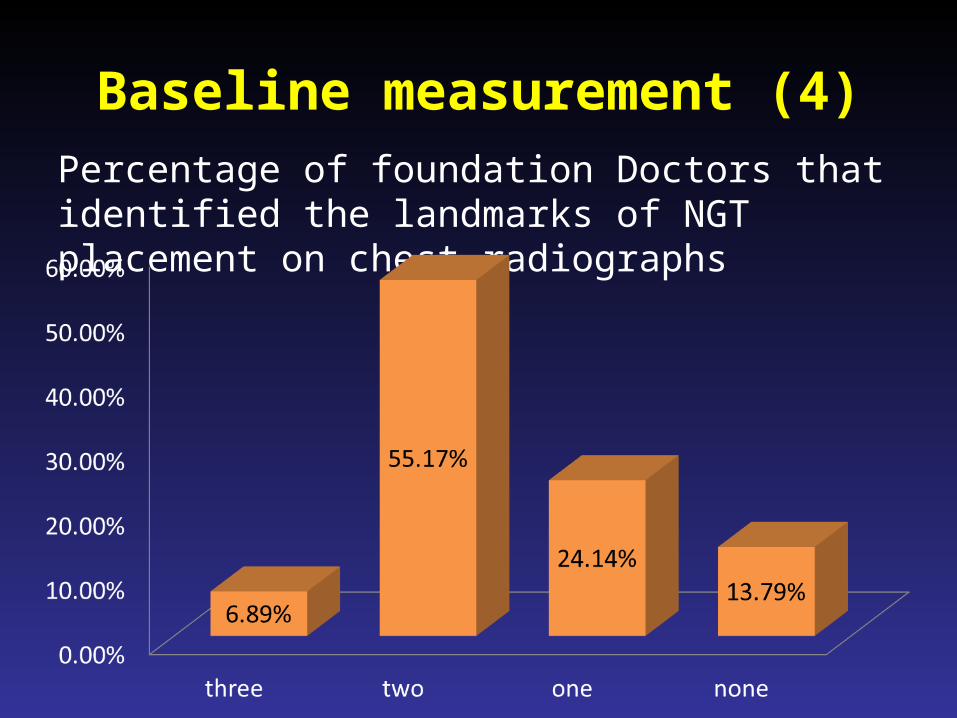
Baseline measurement (4)Percentage of foundation Doctors that identified the landmarks of NGT placement on chest radiographs

Baseline measurement (5)
• 6.9% [2/29] answered the correct pH cut off of NG aspirates (pH 5.5).
• 3.4% [1/29] would correctly ‘wait and aspirate later’ if the pH aspirate was outside the range.

Baseline measurement (6)
• 59.6% [28/47] responded– 7 radiographs • 2 correctly placed NG tubes (89.3% - 50/56 potential
correct answers)• 5 incorrectly placed NG tubes (75% - 105/140)
– 3 F1s answer all questions correctly– Out of the incorrect answers• 83% [34/41] commence feeding when not suitable• 17% [7/41] would not commence feeding when
suitable

Intervention (1)
1. Educating junior doctors through a formal lecture– Including 8 chest
radiographs from PACS system.
2. Introduction of a compulsory electronic-module [6]

Intervention (2)
3. Posterpresentation
4. Engaging with nursing team– Electronic-module available for nurses– Additional comments in competency Framework
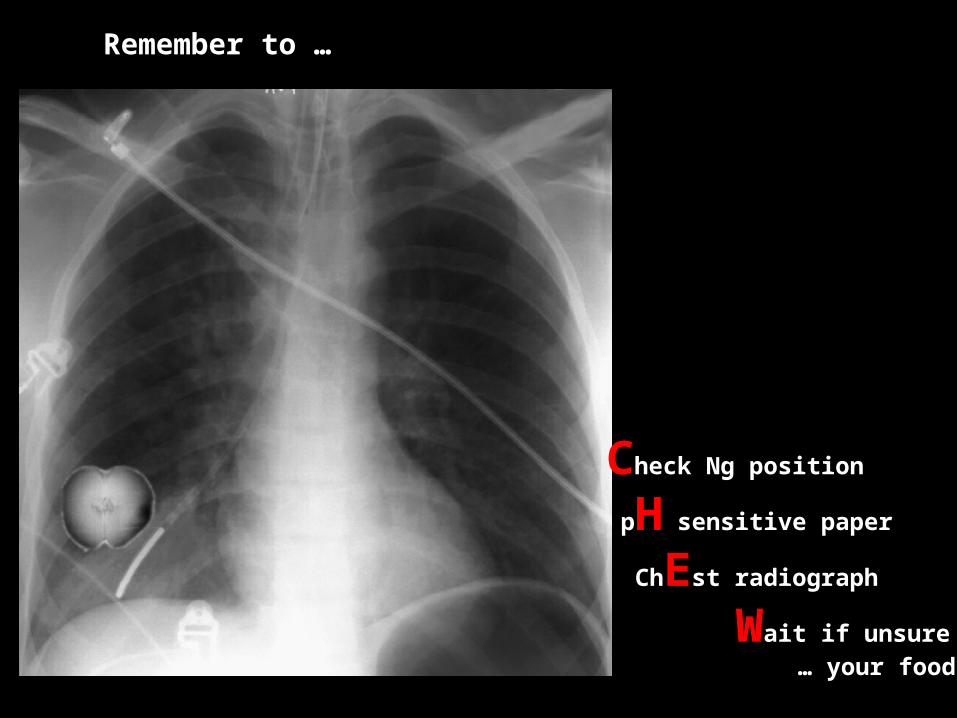
Remember to …
Check Ng position
pH sensitive paper
ChEst radiograph
Wait if unsure … your food!
Results (1)
• The response rate 57.4% [27/47] was similar to that of baseline measurements.
• 100% rating of ‘training was beneficial’.

Results (2)Percentage of F1’s who could correctly identify the first line check for NG tube placement
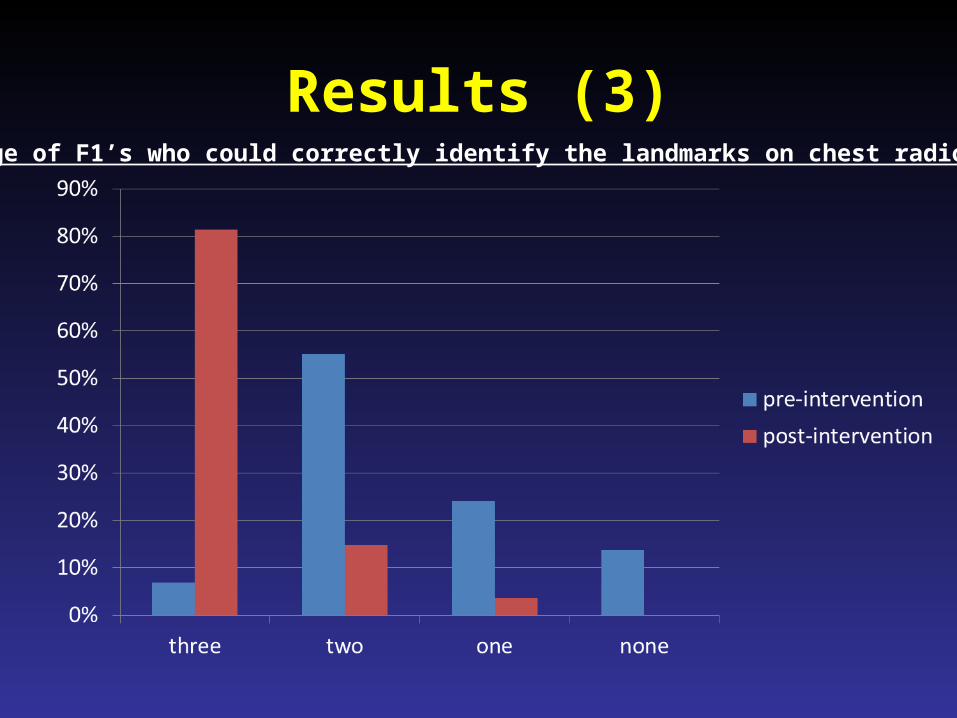
Results (3)Percentage of F1’s who could correctly identify the landmarks on chest radiographs

Results (4)
• 48.15% [13/27] answered the correct pH cut off of NG aspirates.
• 40.7% (11/27) would correctly ‘wait and
aspirate later’ if the pH aspirate was outside the range.

Key points
• There is large discrepancy in the knowledge on the guidance NG tube placement
• Highlights the importance of continuous training amongst health professionals
• Simple, cost-effective, reproducible, modifiable interventions

Discussion
• Should there be universal training across all Trust Sites?
• If so, in what training format?
• Should the training be aimed at grade-specific doctors?
References1. Patient Safety Alert NPSA/2011/PSA002: Reducing the harm caused by misplaced
nasogastric feeding tubes in adults, children and infants . 2011. http://www.nrls.npsa.nhs.uk/alerts/?entryid45=129640 (accessed 22.01.2014).
2. Nasogastric feeding tube placement: changing culture. www.nursingtimes.net/Journals/2011/10/17/j/u/c/Innov-ng-tubes.pdf (accessed on the 10/05/14)
3. National Patient Safety Agency. Nasogastric tubes audit. Available online at: www.nrls.npsa.nhs.uk/resources/?entryid45=66675
4. Harm from flushing of nasogastric tubes before confirmation of placement. http://www.nrls.npsa.nhs.uk/resources/type/alerts/?entryid45=133441 (accessed on the 10.03.2015)
5. http://www.trainingngt.co.uk/site/home.aspx (accessed on the 23.01.2014)6. http://asph.trainingtracker.co.uk/training-slides.asp?5C1B4B404F4141 (accessed
on the 25/04/2014

Thank you for listening.
Questions?