Embed Size (px)
DESCRIPTION
jurnal
Citation preview
www.elsevier.com/locate/ijgo
CLINICAL ARTICLE
Sublingual vs. vaginal misoprostol for inductionof labor
F.E.L. Feitosa a,*, Z.S. Sampaio a, C.A. Alencar Jr a,M.M.R. Amorim b, R. Passini Jr c
a Maternidade-Escola, Universidade Federal do Ceara,Fortaleza, State of Ceara, Brazilb Instituto Materno-Infantil de Pernambuco, Recife, State of Pernambuco, Brazilc Department of Obstetrics and Gynecology, School of Medicine fromUniversidade Estadual de Campinas (Unicamp), State of Sao Paulo, Brazil
Received 21 November 2005; received in revised form 10 April 2006; accepted 11 April 2006
0020-7292/$ - see front matter D 200All rights reserved.doi:10.1016/j.ijgo.2006.04.031
* Corresponding author. Address: Ruaapto. 1401-Bairro Coco, Fortaleza, Cea
E-mail address: edsonlucena@secre
KEYWORDSMisoprostol;Sublingualmisoprostol;Vaginal misoprostol;Induction of labor;Effectiveness;Safety
Abstract
Objective: To compare sublingual with vaginal misoprostol for the induction of labor.Methods: This double-blind clinical trial randomized 150 women to receive every 6h 25 Ag of sublingual misoprostol and vaginal placebo or 25 Ag of vaginal misoprostoland sublingual placebo. Maternal and neonatal outcomes were analyzed and riskratios (RRs) with 95% confidence intervals (CIs) calculated. The significance levelwas 5%. Results: Vaginal delivery rates were 57% in the sublingual group and 69% inthe vaginal group (RR, 0.8; 95% CI, 0.6—1.1). There were 11 cases of fetal distress inthe sublingual group and 4 cases in the vaginal group (RR, 2.7; 95% CI, 0.9—8.2).There were no significant differences in the number of doses needed, intervalbetween first dose and delivery, incidence of contractility disturbances, or neonatalresults. Conclusion: The administration of misoprostol 25 Ag by the sublingual routewas neither more effective nor safer than the same dose administered vaginally.D 2006 International Federation of Gynecology and Obstetrics. Published byElsevier Ireland Ltd. All rights reserved.
6 International Federation of
Batista de Oliveira, 1000ra, CEP 60176-030, Brazil.l.com.br (F.E.L. Feitosa).
1. Introduction
The use of misoprostol for labor induction with alive fetus was first described in 1992, in thepioneering study by Margulies et al. [1]. Since then,decreasing doses have been proposed and labor
International Journal of Gynecology and Obstetrics (2006) 94, 91—95
Gynecology and Obstetrics. Published by Elsevier Ireland Ltd.

F.E.L. Feitosa et al.92
induction with misoprostol has been favorablycompared with other methods [2,3].
Currently, to reduce the incidence of contractil-ity disturbances and neonatal complications, 25 Agis the recommended dose of vaginal misoprostol forinduction of labor [4]. Recent studies have sug-gested the possibility of sublingual administrationof misoprostol for labor induction [5—7]. In thesestudies Cytotec tablets (Searle Pharmaceuticals,Ontario, Canada) were used. Originally manufac-tured for oral use in 100 or 200 Ag doses, thesetablets had to be broken in smaller pieces toachieve the 25 Ag dosage. In Brazil, vaginal tabletscontaining 25 Ag of misoprostol have been com-mercially available since 1998.
Until recently, using the LILACS, Medline, Scielo,and Cochrane Library data bases, only 2 randomizedstudies comparing the sublingual and vaginal routesfor induction of term labor could be found [8,9]. Arecent meta-analysis comparing the effects of dif-ferent doses of misoprostol (50 Ag or higher) admin-istered orally, vaginally, and sublingually found nostatistically significant differences between theeffectiveness of these routes, and the authorssuggested that double-blind randomized studiesshould be performed, with sufficient sample sizes toallow for adequate extrapolation of the results [10].
The present study was carried out to test theeffectiveness and safety of 25 Ag tablets ofmisoprostol sublingually every 6 h for the inductionof term labor, compared with the same doseadministered vaginally.
2. Material and methods
A double-blind randomized clinical trial was con-ducted in 2 hospitals of the northeast region ofBrazil between June 2004 and March 2005. Theresearch ethic boards of both hospitals approvedthe study. All volunteers signed an informedconsent form.
Inclusion criteria were the following: singletonpregnancy, gestational age of 37 weeks or greater,live fetus, cephalic presentation, estimated sono-graphic fetal weight less than 4000 g, amnioticfluid index greater than 5 cm, normal antepartumnon-stress test results, and Bishop score of 6 orless.
Women were excluded in cases of fetal malfor-mations, intrauterine growth restriction, previousuterine scars, premature rupture of membranes, orany contraindication to vaginal delivery.
The tablets for sublingual administration contain-ing 25 Ag of misoprostol (Prostokos; Hebron S/A Ind.Quimicas e Farmaceuticas, Caruaru, Brazil) or place-
bo were specifically manufactured for the study.They had a pleasant taste and fast dissolution, andthey weremuch smaller than the vaginal tablets. Theplacebo vaginal tablets had the same appearance asthe marketed Prostokos vaginal tablets.
The tablets were placed in pouches identified assublingual (SL) or vaginal (V) and then stored inboxes numbered from 1 to 150. Each box containedone pouch with vaginal misoprostol and anotherwith sublingual placebo, or vice versa. Only theresponsible pharmacist had knowledge of thecontent of each pouch and each box. The boxeswere numbered according to previously generatedrandomization numbers using Epiinfo statisticalsoftware, version 6.04 (available from the Centersfor Disease Control, Atlanta, GA, USA). A blockedrandomization was made to assure that the groupswere of equal size [11].
Each participant received 1 sublingual and 1vaginal tablet, only 1 of them containing misopros-tol. The administration was repeated every 6 h until3 or more uterine contractions of 40 s durationoccurred over minutes, or when the maximum of 4doses (i.e., 100 Ag) was reached. In the absence ofactive labor 6 h after administration of the lastdose of misoprostol, failed induction was reportedand cesarean section was performed.
Fetal auscultation every 15 min was performedduring labor in all patients, before, during, andafter contractions. Cardiotocography was per-formed every 2 h or at shorter intervals at thediscretion of the attending obstetrician. The uter-ine activity was clinically assessed every 30 min.
The primary outcome measure was vaginaldelivery rate. Demographic characteristics andindications for the induction of labor were ana-lyzed. Secondary outcomes included the time fromfirst misoprostol administration to initiation oflabor and to delivery; duration of labor; numberof misoprostol doses administered, and need foraugmentation of labor with oxytocin.
Adverse effects included uterine contractilitydisturbances (tachysystole and hyperstimulationsyndrome), gastrointestinal symptoms such as nau-sea, vomiting, and diarrhea, and hyperthermia.Perinatal outcomes analyzed were fetal heart rate(FHR) changes during labor, intrapartum meconiumpassage, intrapartum fetal death, Apgar scores at 1and 5 min, and newborn admission in the intensivecare unit (NICU).
Tachysystole was defined by the presence of atleast 5 uterine contractions in 2 consecutive 10 minperiods. Hyperstimulation syndrome was defined astachysystole and/or hypertonus on cardiotocogra-phy, with fetal heart rate (FHR) alterations such asbradycardia (FHR b110 bpm), late decelerations,
Sublingual vs. vaginal misoprostol for induction of labor 93
and/or loss of fetal heart beat variability [12]. Theoccurrence of any of these abnormal eventsdefined fetal distress [13].
The 73.8% vaginal delivery rate with sublingualmisoprostol published in a 2002 study by Shetty etal. [6] was used for sample size calculation. With ana error of 5% and 80% power, a sample size of 138women was needed to detect a 20% differencebetween the groups [14]. A total of 150 womenwere randomized. All women underwent the laborinduction protocols at the participating hospitals.There were no withdrawals or exclusions postrandomization, and all women received the origi-nally assigned treatment.
Statistical analysis was performed using thestatistical package SAS/STAT, version 8.2 (SASInstitute, Cary, NC, USA). The statistician hadaccess to the groups’ denomination (A or B) butwas unaware of the kind of tablet used in eachgroup. The randomization code was broken onlyafter the results of the analysis were recorded. Asignificance level of 5% was adopted. Risk ratio (RR)and 95% confidence interval (CI 95%) were calcu-lated to assess the magnitude of the associationbetween outcomes and route of misoprostol ad-ministration, and vaginal misoprostol the referencecategory.
3. Results
There were no significant differences betweengroups regarding maternal age, parity, gestational
Table 1 Doses and routes of misoprostol administration a
Variable Sublingual misoprostol
n (%)
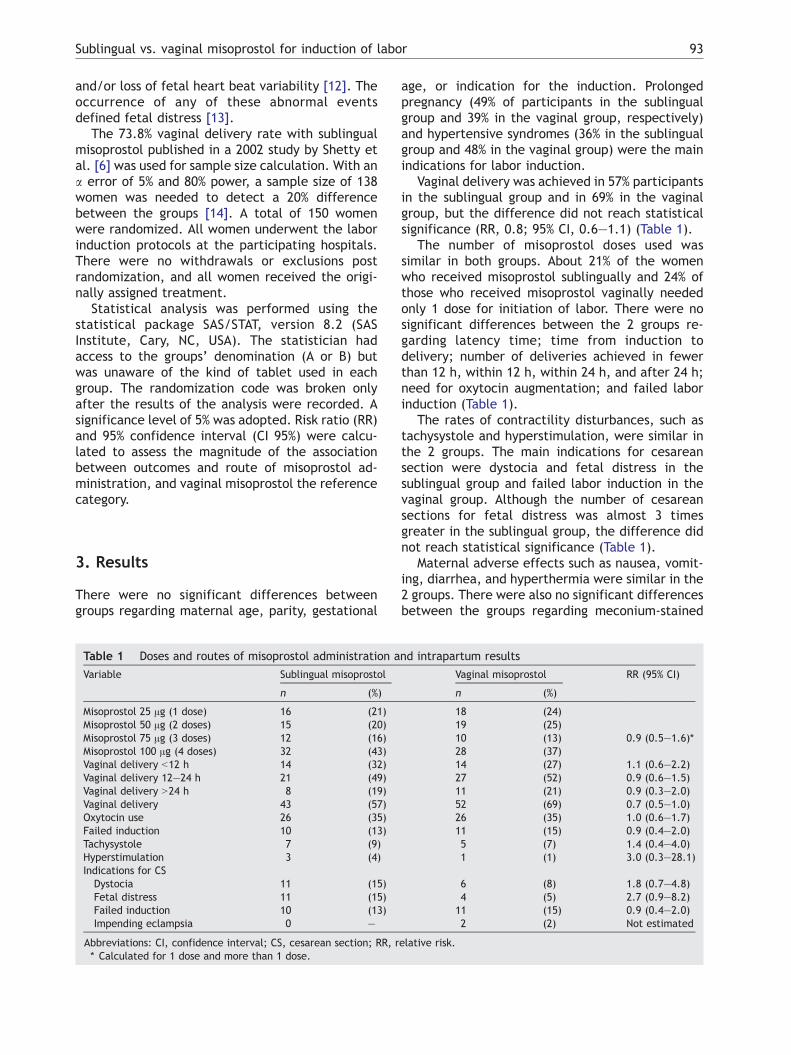
Misoprostol 25 Ag (1 dose) 16 (21)Misoprostol 50 Ag (2 doses) 15 (20)Misoprostol 75 Ag (3 doses) 12 (16)Misoprostol 100 Ag (4 doses) 32 (43)Vaginal delivery b12 h 14 (32)Vaginal delivery 12—24 h 21 (49)Vaginal delivery N24 h 8 (19)Vaginal delivery 43 (57)Oxytocin use 26 (35)Failed induction 10 (13)Tachysystole 7 (9)Hyperstimulation 3 (4)Indications for CS
Dystocia 11 (15)Fetal distress 11 (15)Failed induction 10 (13)Impending eclampsia 0 —
Abbreviations: CI, confidence interval; CS, cesarean section; RR, r* Calculated for 1 dose and more than 1 dose.
age, or indication for the induction. Prolongedpregnancy (49% of participants in the sublingualgroup and 39% in the vaginal group, respectively)and hypertensive syndromes (36% in the sublingualgroup and 48% in the vaginal group) were the mainindications for labor induction.
Vaginal delivery was achieved in 57% participantsin the sublingual group and in 69% in the vaginalgroup, but the difference did not reach statisticalsignificance (RR, 0.8; 95% CI, 0.6—1.1) (Table 1).
The number of misoprostol doses used wassimilar in both groups. About 21% of the womenwho received misoprostol sublingually and 24% ofthose who received misoprostol vaginally neededonly 1 dose for initiation of labor. There were nosignificant differences between the 2 groups re-garding latency time; time from induction todelivery; number of deliveries achieved in fewerthan 12 h, within 12 h, within 24 h, and after 24 h;need for oxytocin augmentation; and failed laborinduction (Table 1).
The rates of contractility disturbances, such astachysystole and hyperstimulation, were similar inthe 2 groups. The main indications for cesareansection were dystocia and fetal distress in thesublingual group and failed labor induction in thevaginal group. Although the number of cesareansections for fetal distress was almost 3 timesgreater in the sublingual group, the difference didnot reach statistical significance (Table 1).
Maternal adverse effects such as nausea, vomit-ing, diarrhea, and hyperthermia were similar in the2 groups. There were also no significant differencesbetween the groups regarding meconium-stained
nd intrapartum results
Vaginal misoprostol RR (95% CI)
n (%)
18 (24)19 (25)10 (13) 0.9 (0.5—1.6)*28 (37)14 (27) 1.1 (0.6—2.2)27 (52) 0.9 (0.6—1.5)11 (21) 0.9 (0.3—2.0)52 (69) 0.7 (0.5—1.0)26 (35) 1.0 (0.6—1.7)11 (15) 0.9 (0.4—2.0)5 (7) 1.4 (0.4—4.0)1 (1) 3.0 (0.3—28.1)
6 (8) 1.8 (0.7—4.8)4 (5) 2.7 (0.9—8.2)11 (15) 0.9 (0.4—2.0)2 (2) Not estimated
elative risk.
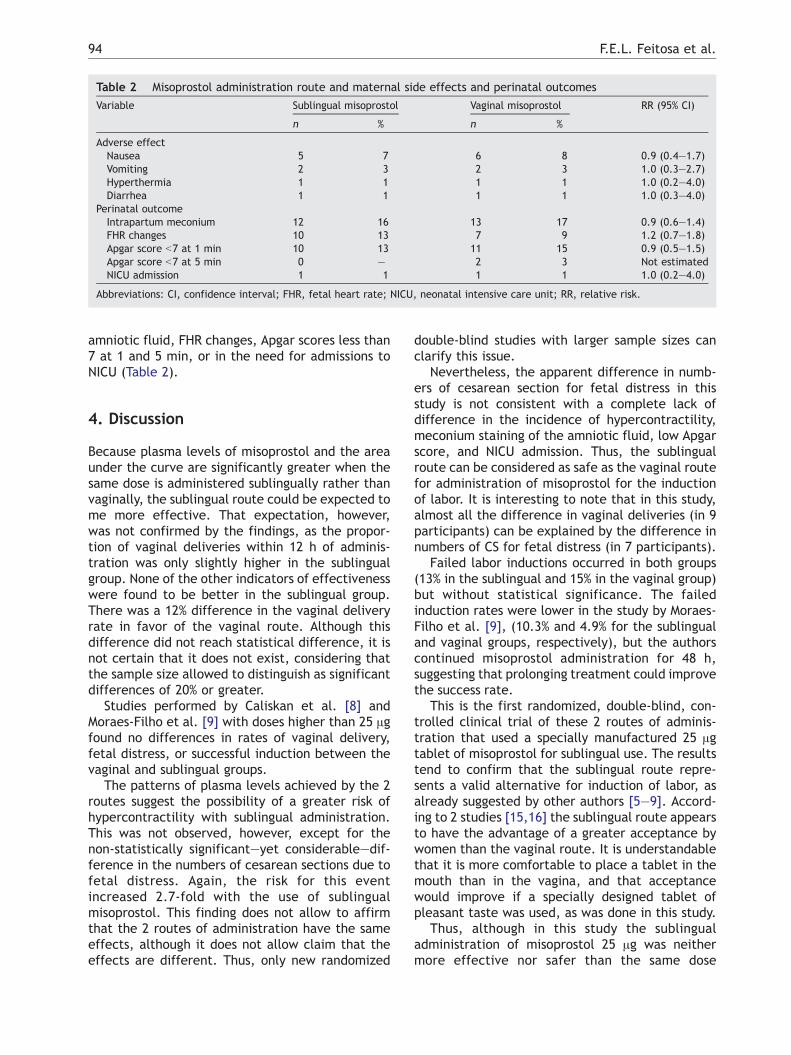
Table 2 Misoprostol administration route and maternal side effects and perinatal outcomes
Variable Sublingual misoprostol Vaginal misoprostol RR (95% CI)
n % n %
Adverse effectNausea 5 7 6 8 0.9 (0.4—1.7)Vomiting 2 3 2 3 1.0 (0.3—2.7)Hyperthermia 1 1 1 1 1.0 (0.2—4.0)Diarrhea 1 1 1 1 1.0 (0.3—4.0)
Perinatal outcomeIntrapartum meconium 12 16 13 17 0.9 (0.6—1.4)FHR changes 10 13 7 9 1.2 (0.7—1.8)Apgar score b7 at 1 min 10 13 11 15 0.9 (0.5—1.5)Apgar score b7 at 5 min 0 — 2 3 Not estimatedNICU admission 1 1 1 1 1.0 (0.2—4.0)
Abbreviations: CI, confidence interval; FHR, fetal heart rate; NICU, neonatal intensive care unit; RR, relative risk.
F.E.L. Feitosa et al.94
amniotic fluid, FHR changes, Apgar scores less than7 at 1 and 5 min, or in the need for admissions toNICU (Table 2).
4. Discussion
Because plasma levels of misoprostol and the areaunder the curve are significantly greater when thesame dose is administered sublingually rather thanvaginally, the sublingual route could be expected tome more effective. That expectation, however,was not confirmed by the findings, as the propor-tion of vaginal deliveries within 12 h of adminis-tration was only slightly higher in the sublingualgroup. None of the other indicators of effectivenesswere found to be better in the sublingual group.There was a 12% difference in the vaginal deliveryrate in favor of the vaginal route. Although thisdifference did not reach statistical difference, it isnot certain that it does not exist, considering thatthe sample size allowed to distinguish as significantdifferences of 20% or greater.
Studies performed by Caliskan et al. [8] andMoraes-Filho et al. [9] with doses higher than 25 Agfound no differences in rates of vaginal delivery,fetal distress, or successful induction between thevaginal and sublingual groups.
The patterns of plasma levels achieved by the 2routes suggest the possibility of a greater risk ofhypercontractility with sublingual administration.This was not observed, however, except for thenon-statistically significant—yet considerable—dif-ference in the numbers of cesarean sections due tofetal distress. Again, the risk for this eventincreased 2.7-fold with the use of sublingualmisoprostol. This finding does not allow to affirmthat the 2 routes of administration have the sameeffects, although it does not allow claim that theeffects are different. Thus, only new randomized
double-blind studies with larger sample sizes canclarify this issue.
Nevertheless, the apparent difference in numb-ers of cesarean section for fetal distress in thisstudy is not consistent with a complete lack ofdifference in the incidence of hypercontractility,meconium staining of the amniotic fluid, low Apgarscore, and NICU admission. Thus, the sublingualroute can be considered as safe as the vaginal routefor administration of misoprostol for the inductionof labor. It is interesting to note that in this study,almost all the difference in vaginal deliveries (in 9participants) can be explained by the difference innumbers of CS for fetal distress (in 7 participants).
Failed labor inductions occurred in both groups(13% in the sublingual and 15% in the vaginal group)but without statistical significance. The failedinduction rates were lower in the study by Moraes-Filho et al. [9], (10.3% and 4.9% for the sublingualand vaginal groups, respectively), but the authorscontinued misoprostol administration for 48 h,suggesting that prolonging treatment could improvethe success rate.
This is the first randomized, double-blind, con-trolled clinical trial of these 2 routes of adminis-tration that used a specially manufactured 25 Agtablet of misoprostol for sublingual use. The resultstend to confirm that the sublingual route repre-sents a valid alternative for induction of labor, asalready suggested by other authors [5—9]. Accord-ing to 2 studies [15,16] the sublingual route appearsto have the advantage of a greater acceptance bywomen than the vaginal route. It is understandablethat it is more comfortable to place a tablet in themouth than in the vagina, and that acceptancewould improve if a specially designed tablet ofpleasant taste was used, as was done in this study.
Thus, although in this study the sublingualadministration of misoprostol 25 Ag was neithermore effective nor safer than the same dose

Sublingual vs. vaginal misoprostol for induction of labor 95
administered vaginally, the limited sample sizedoes not allow reaching definitive conclusions.Given the proven feasibility of using the sublingualroute and the preference of the women, similartrials with a larger sample size should be carriedout in the near future.
Acknowledgments
The misoprostol tablets used in this clinical trialwere donated by the Hebron S/A Ind. Quimicas eFarmaceuticas, Caruaru, Brazil.
References
[1] Margulies M, Campos Perez G, Voto LS. Misoprostol toinduce labor. Lancet 1992;339:64.
[2] Alfirevic Z. Oral misoprostol for induction of labor.Cochrane Database Syst Rev 2001;2:CD001338.
[3] Hofmeyr GJ, Gulmezoglu AM. Vaginal misoprostol forcervical ripening and induction of labour. Cochrane Data-base Syst Rev 2003;1:CD000941.
[4] ACOG Committee Opinion. Number 283, May 2003. NewU.S. Food and Drug Administration labeling on Cytotec(misoprostol) use and pregnancy. Obstet Gynecol2003;101:1049–51.
[5] Shetty A, Mackie L, Danielian P, Rice P, Templeton A.Sublingual compared with oral misoprostol in term labour: arandomized controlled trial. BJOG 2002;109:645–50.
[6] Shetty A, Danielian P, Templeton A. Sublingual misoprostolfor the induction of labor at term. Am J Obstet Gynecol2002;186:72–6.
[7] Wolf SB, Sanchez-Ramos L, Kaunitz AM. Sublingual miso-prostol for labor induction: a randomized clinical trial.Obstet Gynecol 2005;105:365–71.
[8] Caliskan E, Bodur H, Ozeren S, Corakci A, Ozkan S, YucesoyI. Misoprostol 50 Ag sublingually versus vaginally for laborinduction at term. Gynecol Obstet Invest 2005;59:155–61.
[9] Moraes-Filho OB, Albuquerque RM, Pacheco AJC, RibeiroRH, Cecatti JG, Welkovic S. Sublingual versus vaginalmisoprostol for labor induction of term pregnancies. RevBras Ginecol Obstet 2005;27:20–3.
[10] Muzonzini G, Hofmeyr GJ. Buccal or sublingual misoprostolfor cervical ripening and induction of labour. CochraneDatabase Syst Rev 2004;18(4):CD004221.
[11] Friedman LM, Furberg CD, DeMets DL. The randomizationprocess. In: Friedman LM, Furberg CD, DeMets DL, editors.Fundamentals of Clinical Trials, 3rd ed. New York, NY7Springer-Verlag, 1998. p. 61–81.
[12] Royal College of Obstetricians and Gynaecologists. Inductionof labour: evidence-based. London, England: RCOG ClinicalEffectiveness Support Unit; Jun2 2001. Clinical GuidelineNo. 9. Avaliable at: http://www.rcog.uk/resources/public/rcog_induction_of_labour.pdf.
[13] Royal College of Obstetricians and Gynaecologists. The useof electronic fetal monitoring: the use and interpretationof cardiotocography in intrapartum fetal surveillance:evidence-based. London, England: RCOG Clinical Effective-ness Support Unit; May 2001. Clinical Guideline No. 8.Available at: http://www.rcog.uk/resources/public/pdf/efm_guideline_final_2may2001.pdf.
[14] Friedman LM, Furberg CD, DeMets DL. Sample size. In:Friedman LM, Furberg CD, DeMets DL, editors. Fundamen-tals of clinical trials, 3rd ed. New York, NY7 Springer-Verlag,1998. p. 94–125.
[15] Arvidson C, Hellborg M, Gemzel-Daniellson K. Preferenceand acceptability of oral versus vaginal administration ofmisoprostol in medical abortion with mifepristone. Eur JObstet Gynecol Reprod Biol 2005;123:87–91.
[16] Saxena P, Salhan S, Sara N. Sublingual versus vaginal routeof misoprostol for cervical ripening prior to surgicaltermination of first trimester abortions. Eur J ObstetGynecol Reprod Biol 2006;125:109–13.





























