Embed Size (px)
DESCRIPTION
Citation preview

Immunisation
Immunisation is second only to a clean drinking water supply as a way of improving and maintaining the health of the population. Whilst smallpox has been eradicated from the world, by immunisation, all other infectious diseases remain. The only way to protect children and adults from avoidable death and serious, often long-term, complications from such diseases is to maintain high levels of immunisation in the population.1
The risk we face
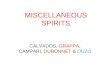
Barnet, in common with all other London boroughs, now faces the likelihood of a measles epidemic. In the last year or so the number of children and adults catching measles – the most contagious disease that there is – has been much higher than in past years and there have been several outbreaks, as shown in . Figure 1
Figure 2: The number of reported cases of measles in Barnet in recent years
The
reasons for the alarming increase in people catching measles in Barnet are outlined below demonstrating that MMR immunisation rates in Barnet are substantially below the level required for safety.
The reason that so many people have caught measles and the fact that we now face the very real risk of a measles epidemic is because there are now so many children whose parents have refused consent for them to be 1mmunizat with measles, mumps and rubella vaccine. The ‘herd immunity’ of the population is now sufficiently low to enable each person with measles to infect more than one other person. The problem of measles is more widespread in other parts of London, as shown below.
1 The main exception to this is TB. Whilst BCG vaccine is an important way to protect people most at risk the way this disease affects the population has changed.
0
10
20
30
40
50
60
70
80
90
2005/06 2006/07 2007/08
0
10
20
30
40
50
60
70
80
90
0
10
20
30
40
50
60
70
80
90
2005/06 2006/07 2007/082005/06 2006/07 2007/08

Source: Health Protection Agency. Measles and MMR uptake in London, 2008 Cover data and trends in vaccine uptake 2005-2008
MMR uptake at age 2 years for London and UK – January 1996 – March 2008* signify that immunisation rates are beginning to decline significantly
.

Immunisation rates in children in Barnet for:
first course of diphtheria, tetanus, pertussis and polio;
first dose of Haemophilus influenzae B;
meningococcus C;
first dose of measles, mumps and rubella (MMR);
second dose of MMR; and
diphtheria, tetanus and pertussis and inactivated polio booster.
This shows clearly that MMR 3mmunization rates in Barnet are very substantially below the level required for safety, i.e. to avoid measles outbreaks and to avoid a measles epidemic, although they are beginning to increase
Local targets
In common with other London PCTs, Barnet has agreed to increase all of its childhood immunisations to 90% by 2010/2011. The trajectory for immunisation rates for MMR by the age of two years shows the trajectory for MMR, which is the most challenging as all other childhood immunisation rates are currently in the high eighties and thus closer to the target.
The trajectory for immunisation rates for MMR by the age of two years
45.0
50.0
55.0
60.0
65.0
70.0
75.0
80.0
85.0
90.0
95.0
Q3 05/06 Q4 05/06 Q1 06/07 Q2 06/07 Q3 06/07 Q4 06/07 Q1 07/08 Q2 07/08 Q3 07/08 Q4 07/08 Q1 08/09
DTP/Polio primary
MMR 1st dose
Hib primary
MMR 2nd dose
MenC
DTaP/IPV booster
%
Quarter in each year
45.0
50.0
55.0
60.0
65.0
70.0
75.0
80.0
85.0
90.0
95.0
Q3 05/06 Q4 05/06 Q1 06/07 Q2 06/07 Q3 06/07 Q4 06/07 Q1 07/08 Q2 07/08 Q3 07/08 Q4 07/08 Q1 08/09
DTP/Polio primary
MMR 1st dose
Hib primary
MMR 2nd dose
MenC
DTaP/IPV boosterDTP/Polio primary
MMR 1st dose
Hib primary
MMR 2nd dose
MenC
DTaP/IPV booster
%
Quarter in each year
73.9 74.5 75.6 76.4 77 80
90
2004_05 2005_06 2006_07 2007_08 2008_09 2009_10 2010_20110
10
20
30
40
50
60
70
80
90
100
Pro
po
rtio
n (
%)
of
2-y
ear
old
s w
ith
fir
st
MM
R i
mm
un
isa
tio
n
actual trajectoryestimate
73.9 74.5 75.6 76.4 77 80
90
2004_05 2005_06 2006_07 2007_08 2008_09 2009_10 2010_20110
10
20
30
40
50
60
70
80
90
100
Pro
po
rtio
n (
%)
of
2-y
ear
old
s w
ith
fir
st
MM
R i
mm
un
isa
tio
n
actual trajectoryestimate

Source: Barnet PCT Operating Plan
The key activities required are:
ensuring the accuracy of immunisation records – it is apparent that a lot of children have been immunised but the fact has not been recorded on the PCT’s child health surveillance system;
bolstering the immunisation call system to ensure that all children who need immunisation (because it is due or have, apparently, been missed) are invited for immunisation;
providing immunisations in various sites, e.g. GP surgeries, community pharmacies, A&E departments, walk-in centres, children’s centres, children’s outpatient departments;
promoting immunisation widely, using social marketing techniques, to better ensure that the right message is received; and
working with local community and religious leaders, and in schools, pre-school facilities, children’s centres, NHS facilities and other places to promote immunisation.
Data on ethnicity and religious belief are not currently routinely recorded in the context of childhood immunisation. However, it is apparent that in the North East and North central London area, the majority of people affected by measles have been Jewish. The reasons for this need to be explored further.

Teenage pregnancy
Barnet has one of the lowest rates of teenage pregnancy (TP) in London, and this is also lower than similar boroughs (including those matched for deprivation) such as Merton, Hounslow and Enfield. Not only is it lower than the London average, but it is also lower than the national average. The graph below summarises the his trend and the comparison between Barnet, London and England.
Approximately 68% of teenagers who conceived in Barnet in 2006 had a termination of pregnancy (TOP), the remainder having had either a live or still birth. Data on the residential postcodes of all TOPs performed by Marie Stopes, the PCT’s main provider of abortion services, on women in Barnet aged under 18 years show that 15.2% of teenage abortions were performed on young women who had had at least one previous TOP. Teenagers who have had one TOP are a high risk group for further unplanned pregnancy.
0 50 100 150 200 250 300
Asian: Pakistani
Black: Other
Mixed: White & Asian
Mixed: White & Black African
Not known
Chinese
Asian: Other
Asian: Indian
Mixed: Other Mixed
Black: Caribbean
Asian: Bangladeshi
White: Other
Any Other ethnic group
White: Irish
Black: African
White: Eastern European
White: British
Jewish
Number of reported measles cases
0 50 100 150 200 250 300
Asian: Pakistani
Black: Other
Mixed: White & Asian
Mixed: White & Black African
Not known
Chinese
Asian: Other
Asian: Indian
Mixed: Other Mixed
Black: Caribbean
Asian: Bangladeshi
White: Other
Any Other ethnic group
White: Irish
Black: African
White: Eastern European
White: British
Jewish
Number of reported measles cases

Sexual health
Sexual health is an important aspect of physical and mental well-being. Poor sexual health can have a long-lasting and severe impact on people’s lives, for example through unintended pregnancies and abortions causing physical disease and poor educational, social and economic opportunities; Sexually transmitted infections (STIs) and HIV/AIDS; ectopic pregnancies leading to infertility; cervical and other genital cancers; and hepatitis, chronic liver disease and liver cancer.
The risk we face
Sexually transmitted infections
Nationally, diagnoses of sexually transmitted infections (STIs) have been steadily rising in the UK since 2001. The most recent Health Protection Agency (HPA) data indicate that this trend is continuing: between 2005 and 2006 there was a 2% rise in both new diagnoses and total numbers of STIs (recurrent and follow-up presentations) in genito-urinary medicine (GUM)
0
10
20
30
40
50
60M
arch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
1999 2000 2001 2002 2003 2004 2005 2006 2007
Un
de
r 1
8 c
on
cep
tio
n r
ate
per
100
0
Barnet rolling average
London
England
1998
0
10
20
30
40
50
60M
arch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
1999 2000 2001 2002 2003 2004 2005 2006 2007
Un
de
r 1
8 c
on
cep
tio
n r
ate
per
100
0
Barnet rolling averageBarnet rolling average
LondonLondon
EnglandEngland
1998
0
5
10
15
20
25
30
35
40
45
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
1999 2000 2001 2002 2003 2004 2005 2006 2007
Un
de
r 1
8 c
on
cep
tio
n r
ate
per
10
00
Quarterly rate
Rolling average
1998
0
5
10
15
20
25
30
35
40
45
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
Sep
t
Dec
Mar
ch
Jun
e
1999 2000 2001 2002 2003 2004 2005 2006 2007
Un
de
r 1
8 c
on
cep
tio
n r
ate
per
10
00
Quarterly rate
Rolling average
1998

clinics. The overall increase in STIs masks a more complicated picture for specific infections and in specific age and other risk groups.i
The incidence of Genital Chlamydia, Gonorrhoea and other STI’s are explored further in Appendix 8.
The true incidence of STIs in Barnet is not known, since figures on the numbers of people with a STI are rarely presented on the basis of a person’s residence. Most data are reported at GUM clinic level, but since these clinics see people regardless of their place of residence, figures from clinics include diagnoses made on people living outside of the ‘host’ PCT area where the clinic is situated. Data can also be distorted when the place of residence of a patient attending a clinic is unknown and this varies between GUM clinics. Appendix 8 discusses the GUM clinics most likely to be attended by Barnet residents and the types of STI’s which are presented at the GUM clinics.
Although local GUM clinic data are a poor indication of the local incidence and prevalence of STI, they do give a reasonable idea of trends and these continue to rise in Barnet, as elsewhere.
HIV/AIDS
The number of people in Barnet known to have HIV infection has increased steadily since 2002. Appendix 8 contains data showing this increase, as well as the ethnicity and age of HIV/AIDS patients
In common with many other areas, HIV is more common in people in Black African and African Caribbean ethnic groups. However, unlike most of the other PCTs in the north central part of London, especially the inner-city ones, HIV infection is becoming increasingly common in Black women in Barnet rather than in the Black MSM group. It is possible that the male partners of many of these women contract the infection abroad. But the important point is that it is heterosexual transmission of HIV that is becoming a larger issue that it is in MSM in Barnet. In 2005, 132/504 (26.2%) of known cases of HIV in Barnet were in MSM, 316/504 (62.7%) were in heterosexual men or women, 26/504 (5.2%) were acquired by mother-to-child transmission, and the remainder were acquired through other or unknown means.
Abortion services
In terms of access to abortion services for all women of child-bearing age, there were 2444 TOPs performed on Barnet residents in 2006. This is above the national average rate and probably reflects either better access to termination services or lack of access to contraception services. As Barnet has such a low number of teenage conceptions (which include abortions as well as births) relative to most other PCTs in London, this latter possible explanation is unlikely.

1.1.1 The relationship between diversity and deprivation and sexual health problems
There is a clear relationship between rates of sexual ill-health, poverty and social exclusion. Certain groups are particularly at risk of poor sexual health, including:
young people, especially those in, or leaving, care;
people from Black and ethnic minority groups;
gay and bisexual men;
injecting-drug users;
adults and children living with HIV and other people affected by HIV;
sex workers; and
people in prisons and youth offending establishment.
People in these groups are not only more likely to engage in sexually risky behaviour, but will often make only poor use of existing services and are therefore hard to reach.ii
Ethnicity is relevant to the planning of sexual health services in several ways. First, certain communities are more likely to experience a high incidence of specific STIs, for example HIV is much more common in the Black African community, and the majority of women with HIV in Barnet are from this community. Secondly, services may need to be modified so that that can be made religiously and/or culturally acceptable to certain communities, for example sex and relationships education (SRE) programmes for young people from certain orthodox Jewish and Islamic communities. Thirdly, cultural values and ethnicity may affect health beliefs and behaviours and health-seeking activities and can be important influences on health and well-being. There is limited evidence on this issue, but for instance there is some indication that men from the Black African community are less likely to attend GUM clinics.iii,iv,v
Knowing people’s ethnicity is also important in terms of designing services: there is evidence that many people from the African community are uncomfortable visiting GUM clinics, and that in this community a different approach is needed. Since in general sexually active women of all communities are more likely to attend health services, increasing testing in these settings is an important method for increasing uptake of HIV screening in women, for example in antenatal or family planning clinics. For men, however, a more community-orientated approach is most likely to achieve results.
In terms of age and general sexual health services, the greatest numbers of people seen in the main GUM clinics serving Barnet’s population are aged 15-35 years (77% of attendees) and 60% of attendees are women.
i HPA (2007). Testing Times - HIV and other Sexually Transmitted Infections in the United Kingdom: 2007 London: Health Protection Agency, Centre for Infections. November 2007.
ii Downing J, Jones L, Cook PA et al (2006) Prevention of sexually transmitted infections (STIs): a review of reviews into the effectiveness of non-clinical interventions. Evidence Briefing Update. London: National Institute for Health and Clinical Evidence.
iii National Survey of Sexual Attitudes and Lifestyles II, National Centre for Social Researchiv Sadler KE, McGarrigle CA, Elam G et al (2007) Sexual behaviour and HIV infection in black-Africans in England:
results from the Mayisha II survey of sexual attitudes and lifestyles. Sexually Transmitted Infections 2007;83:523-529.
v Fenton KA et al. Ethnic variations in sexual behaviour in Great Britain and risk of sexually transmitted infections: a probability survey. The Lancet 365: 1246 - 1255, 2005.

1.1.2 Local targets
There are two main targets. The first is to screen people aged 15-24 years for genital Chlamydia infection. The target for 2008/09 is to screen 6,699 people.
The other main target is to reduce the number of teenage pregnancies. The trajectory for this is shown in Figure 2.
Figure 2: Teenage pregnancy rates in Barnet – current and future trajectory
1.1.3 Key things that need to be done
The key activities required are:
increasing the provision of sexual health services in GP practices;
increasing the number of young people screened for genital Chlamydia infection; and
ensuring that all sexual health services (including sexual health promotion and sexual relationship education) are designed to enable access by people from different ethnic and religious backgrounds.
1.1.4 Key things that need to be done
The key activities required are:
enabling more people with mental health problems to give up smoking;
identifying and acting on any common factors that there may be in people who are currently receiving or who have recently received care from mental health services and who attempt or succeed in killing themselves;
9mmunizatio that there will be an increased need for services to care for people with dementia in the coming years.
1.1.5 Over the next few years, in terms of health services, Barnet needs to:
.
Co
nc
ep
tio
n r
ate
pe
r 1
,000
fem
ale
s a
ge
d 1
5-17
0
5
10
15
20
25
30
35
2005 2006 2007 2008 2009 2010
actual trajectoryestimate
167 168 149
131 107 84
Co
nc
ep
tio
n r
ate
pe
r 1
,000
fem
ale
s a
ge
d 1
5-17
0
5
10
15
20
25
30
35
Co
nc
ep
tio
n r
ate
pe
r 1
,000
fem
ale
s a
ge
d 1
5-17
0
5
10
15
20
25
30
35
0
5
10
15
20
25
30
35
2005 2006 2007 2008 2009 20102005 2006 2007 2008 2009 2010
actualactual trajectorytrajectoryestimateestimate
167 168 149167 168167 168 149
131 107 84131 107 84