Embed Size (px)
Citation preview

British Columbia Nutrition Survey: Report on Supplements
British Columbia Nutrition Survey:
Report on Supplements
Prepared by: Susan I. Barr, Ph.D.
Professor of Nutrition University of British Columbia
Prepared for: Prevention & Wellness Planning, B.C. Ministry of Health Services
February 2004

British Columbia Nutrition Survey: Report on Supplements
TABLE OF CONTENTS
List of Tables ..............................................................................................................................ii List of Figures ............................................................................................................................iii Executive Summary ................................................................................................................... iv Acknowledgements...................................................................................................................vii 1.0 INTRODUCTION.........................................................................................................1 2.0 METHODS .................................................................................................................... 3
2.1 Non-response Questionnaire............................................................................... 3 2.2 Supplement Intake .............................................................................................. 3
3.0 RESULTS and DISCUSSION ..................................................................................... 6
3.1 Response Rate..................................................................................................... 6 3.2 Comparison of Respondents and Non-respondents ............................................ 6 3.3 Prevalence of Use of Vitamin-Mineral and Other Supplements by
BC Adults............................................................................................................ 7 3.4 Number of Vitamin and/or Mineral Supplements Used ................................... 11 3.5 Use of Supplements Containing Specific Nutrients on the Day
Before the Survey ............................................................................................. 13 3.6 Use of Supplements Containing Specific Nutrients during the Month
Before the Survey ............................................................................................. 17 3.7 Nutrient Intakes from Supplements .................................................................. 20 3.8 Effect of Supplement Intake on the Prevalence of Nutrient Inadequacy.......... 29 3.9 Effect of Supplement Use on the Prevalence of Excessive Intakes.................. 35 3.10 Other Supplements Used................................................................................... 38
4.0 CONCLUSIONS ......................................................................................................... 41 5.0 REFERENCES............................................................................................................ 43
i

British Columbia Nutrition Survey: Report on Supplements
LIST OF TABLES Table 2.1 Observed and weighted sample sizes for the BC Nutrition Survey.................... 5
Table 3.1 Percent of BC adult population taking any supplement (vitamin-mineral and/or other).........................................................................................................7
Table 3.2 Percent of BC adult population taking vitamin and/or mineral supplements only, other supplements only, and both vitamin and/or mineral and other supplements ............................................................................9
Table 3.3 Number of vitamin and/or mineral supplements taken yesterday by BC adults taking one or more nutritional supplements.......................................................12
Table 3.4 Number of vitamin and/or mineral supplements taken yesterday by BC adults, by age and sex ........................................................................................13
Table 3.5 Percentage (and 95% confidence interval) of BC adults taking supplements containing various nutrients yesterday by age and sex......................................16
Table 3.6 Percentage (and 95% confidence interval) of BC adults taking supplements containing various nutrients last month by age and sex ....................................19
Table 3.7. Minimum, median and maximum nutrient intakes from supplements yesterday and during the last month by age and sex..........................................22
Table 3.8 Effect of supplement use on the apparent prevalence (and 95% confidence interval) of nutrient inadequacy in BC adults ....................................................30
Table 3.9 Effect of supplement use on median usual calcium intakes of BC adults ..................................................................................................................33
Table 3.10 Effect of supplement use on proportion of BC adults meeting the adequate intake (AI) for calcium .......................................................................34
Table 3.11 Effect of supplement use on median usual pantothenic acid intakes of BC adults............................................................................................................35
Table 3.12 Effect of supplement use on the proportion of BC adults meeting the adequate intake (AI) for pantothenic acid..........................................................35
Table 3.13 Effect of supplement use on the prevalence of BC adults with usual intakes above the tolerable upper intake level (UL) ..........................................37
Table 3.14 Percent of BC adult population using non-vitamin-mineral supplements .........39
Table 3.15 Other supplements used by participants in the BC Nutrition Survey ................40
ii

British Columbia Nutrition Survey: Report on Supplements
LIST OF FIGURES Figure 3.1. Percent of British Columbians consuming a vitamin and/or mineral
supplement by sex and age ................................................................................. 11 Figure 3.2. Prevalence of inadequate vitamin and mineral intakes from food alone,
and food from plus supplements, among British Columbia adults..................... 32
iii
British Columbia Nutrition Survey: Report on Supplements
Executive Summary
The British Columbia Nutrition Survey (BCNS) was conducted in 1999 by Health
Canada and the BC Ministry of Health Planning, in association with the University of British
Columbia, to obtain comprehensive up-to-date information on the eating habits and body weights
of adult British Columbians. The province-wide survey included 1823 participants aged 19 to 84
years, and involved 90-minute, in-home interviews by trained public health nurses and
nutritionists. Several questionnaires were used to assess food consumption and priority nutrition
issues, including a 24-hour recall, a food frequency questionnaire, and a general nutrition
questionnaire focusing on physical activity, healthy weight and body image, and food security.
Socio-demographic information and measured height, weight and waist circumference were also
collected from the participants.
Although the BCNS had several objectives, the data presented herein relate to only one;
namely, to assess the extent of supplement use and its impact on nutrient adequacy. The key
findings reported in this document are highlighted below.
• Supplement use is common among BC adults, with 46% of the population having taken one
or more supplements on the previous day, and 64% having done so within the previous
month. Although the majority of supplement users used only one or two supplements, almost
one in four supplement users had taken four or more supplements the previous day.
• Supplement use tended to be more common among women than men, and in adults over the
age of 50 compared to younger adults.
• Use of vitamin and/or mineral supplements was more common than use of other types of
supplements: Fifty-seven percent of the population had used one or more vitamin and/or
mineral supplements during the past month, while 33% had used one or more other
iv

British Columbia Nutrition Survey: Report on Supplements
supplements.
• Supplements containing vitamin C, vitamin E and calcium were the most commonly used
vitamin and/or mineral supplements. A wide variety of non-vitamin/mineral supplements was
used: Glucosamine and/or chondroitin sulphate, garlic, various oils, echniacea and gingko
biloba were reported most frequently.
• Although a synthetic source of vitamin B12 is recommended for adults over the age of 50,
over half the population of older adults had not consumed any supplemental vitamin B12
during the month before the survey.
• The recommended intakes for vitamin D are 400 mcg/d and 600 mcg/d for adults aged 51-70
and 71 and above, respectively. Although data on vitamin D intakes from food were not
available in the BCNS, these recommended intakes are very difficult to obtain from diet
alone. However, most older adults had not taken a supplement providing vitamin D in the
month before the survey.
• Consideration of supplement use significantly reduced the population prevalence of nutrient
inadequacy (as approximated by the percentage below the Estimated Average Requirement)
for folate, vitamin B12 and vitamin C, and differences were of borderline significance for
vitamin B6 and magnesium.
• Although supplement use increased median calcium intakes and the percentage of individuals
meeting the Adequate Intake (AI), median intakes remained below the AI for all age/sex
groups except young men, whose median intake exceeded the AI whether or not supplement
use was considered.
• Supplement use was associated with small increases (<1% - 7%) in the proportion of the
population with intakes above the Tolerable Upper Intake Level (UL) for calcium, vitamin
v

British Columbia Nutrition Survey: Report on Supplements
B6, folic acid, vitamin C, vitamin E, iron and zinc. For niacin, 10-37% of various age/sex
groups had intakes exceeding the UL.
Potential implications of these findings for health professionals and health planners
include the need to consider supplement use when assessing dietary intake; the likelihood that
future dietary guidance may need to include recommendations for supplement use; the need to
develop effective methods for educating the public about supplements; the need to monitor the
potential for adverse consequences arising from excessive supplement intake; and the need for
health professionals to inquire about their clients’ use of all types of supplements.
vi

British Columbia Nutrition Survey: Report on Supplements
Acknowledgements
In addition to myself, other members of the Investigative Team for the BCNS included
Lisa Forster-Coull (principle investigator) and Ryna Levy-Milne (co-investigator). I thank both
Lisa and Ryna for helpful comments and suggestions on earlier versions of this document. The
entire Investigative Team thanks Health Canada and the BC Ministry of Health Planning for
jointly funding the study, and the British Columbians who generously gave their time to
participate in the study. Many individuals contributed to the success of the BCNS, and are
acknowledged by name in the BC Nutrition Survey Nutrient Report (1).
vii

British Columbia Nutrition Survey: Report on Supplements
1.0 INTRODUCTION The British Columbia Nutrition Survey (BCNS) was conducted by Health Canada and the
BC Ministry of Health Planning, in association with the University of British Columbia, to
obtain comprehensive up-to-date information on the eating habits and body weights of adult
British Columbians. Similar provincial nutrition surveys have been conducted in all other
provinces beginning in 1988 with the Nova Scotia Nutrition Survey. This report is one of a
series arising from the BCNS, and as such, it relates to only one of the six objectives the survey
was designed to meet; namely “to determine the contribution of major food groups, food types
and dietary supplements to the diet”. Readers are referred to the BCNS Nutrient Report for a full
description of the rationale for the study, a literature review pertaining to the study’s objectives,
complete descriptions of study methodology, and data on response rates (1). The province-wide
survey involved 90-minute, in-home interviews conducted by trained public health nurses and
nutritionists utilizing several questionnaires to assess food consumption and priority nutrition
concerns. The questionnaires included a 24-hour recall that also ascertained supplement use, a
food frequency questionnaire, and a general nutrition questionnaire focusing on physical activity,
healthy weight and body image, and food security. Socio-demographic information, height,
weight and waist circumference measurements were also collected from the approximately 1800
participants, aged 19 to 84 years. The data reported herein were obtained from the 24-hr recall.
Assessment of the contribution of dietary supplements to the diets of British Columbians
is relevant, as increasing proportions of North Americans are using both nutritive and non-
nutritive supplements. For example, in the third National Health and Nutrition Examination
Survey (NHANES-III) study, 34.9% of men and 43.8% of women in the United States reported
using at least one supplement during the past month (2). Another national US sample found that
1

British Columbia Nutrition Survey: Report on Supplements
40% of adults had used one of more vitamin/mineral supplements during the past seven days (3),
while 14% reported using one or more herbal preparations. Fewer Canadian studies are
available, but the Food Habits of Canadians Study found that 41% of participants aged 18 to 65
used at least one supplement on the day prior to the survey: Thirty-eight percent used one or
more nutritive supplements, and 15% used one or more herbal preparations (4).
In the recently-released Dietary Reference Intakes (DRIs) (5-9), supplement use is
acknowledged to contribute to meeting nutrient requirements. When diets of populations are
assessed to determine the adequacy of nutrient intakes, assessment should be based on total
intake, including supplements (10). Furthermore, use of a supplement or fortified food is
explicitly or implicitly recommended for some age/sex groups: This includes folic acid for
women of child-bearing potential, and vitamins B12 and D for adults over 50. However,
supplement use also has the potential to lead to adverse effects from excessive nutrient intakes.
For some nutrients, such as niacin, magnesium, folic acid and vitamin E, the Tolerable Upper
Intake Level (UL) applies only to intakes from fortified foods and/or supplements. For these
reasons, current information on supplement use should be available to contribute to the
identification of priority areas for nutrition programming.
2

British Columbia Nutrition Survey: Report on Supplements
2.0 METHODS 2.1 Non-response Questionnaire
As discussed more completely in the British Columbia Nutrition Survey Report on
Energy and Nutrient Intakes (1), a low response rate suggests the potential for bias, as non-
responders may differ systematically from respondents. Accordingly, survey results may not be
generalizable to the general adult population in British Columbia. In an effort to assess the
direction and/or extent of potential bias associated with a low response rate, the non-responders
were asked to complete a short survey including questions on smoking, consumption of bread,
milk and supplements, and marital status. The question on supplement use asked “During the
past month, did you take any vitamin-mineral supplement?”.
2.2 Supplement Intake
Supplement data were obtained during the 24-hr recall portion of the in-home interview.
Participants were first asked whether they took any nutritional supplements, vitamins, minerals,
or herbal, botanical or homeopathic preparations yesterday, which was also the day used for the
24-hr recall of food intake. This was followed by a question about whether they took any other
supplements (i.e., that differed from the ones taken yesterday) within the past month. Next, for
each supplement, participants were asked to provide its specific name and DIN (drug
identification number). Because interviews were conducted in participants’ homes, in most cases
this information was recorded directly from the supplement label. Finally, participants indicated
how often they took the supplement (per day, per week or per month) as well as the number of
pills (or tablets, capsules, teaspoons) usually taken on each occasion.
3

British Columbia Nutrition Survey: Report on Supplements
Supplement data were entered into the Health Canada supplement database, using the
DIN when possible. For the purposes of analysis, vitamin and/or mineral supplements were
defined as supplements containing recognized vitamins and minerals, while other supplements
included supplements not containing recognized vitamins and minerals, but considered by the
respondent to be a supplement. Examples of non-nutritional supplements included herbs and
natural products (e.g., garlic, gingko, echinacea, homeopathic products, glucosamine). In some
cases this latter category also included substances containing known nutrients (e.g., oils that
contain vitamin A or D, but were not marketed as a vitamin A or D supplement).
For each individual who used nutritional supplements, nutrient intake from supplements
was expressed both as the intake “yesterday” and as the intake during the past month. Monthly
supplement intake data were expressed as daily amounts, and were combined with the adjusted
usual nutrient intake from food to yield the distribution of usual nutrient intake from food plus
supplements.
In most cases, data on the prevalence of supplement use are presented as the point
estimates for the sample, and the 95% confidence intervals (95% CI, the range within which the
population means could lie) are also presented. Whether subgroup means differ significantly can
be estimated by determining whether or not the 95% CIs overlap. For example, if the estimated
prevalence of use by men aged 19-30 was 24% (95% CI 12% - 31%), and was compared to an
estimated prevalence of 40% (95% CI 33% - 48%) for men aged 51-70, it could be concluded the
older men were more likely to use supplements than men aged 19-30, because the two sets of
confidence intervals do not overlap.
All data presented in this report have been weighted. Observed and weighted sample
sizes according to the Dietary Reference Intake age-sex groups are shown in Table 2.1.
4

British Columbia Nutrition Survey: Report on Supplements
Table 2.1 Observed and weighted sample sizes for the BC Nutrition Survey
Men (age in years) Women (age in years) Sample size
19-30 31-50 51-70 >71 19-30 31-50 51-70 >71
Observed 142 205 249 271 176 266 282 230
Weighted 235 366 217 84 229 371 221 99
From: BBCA Technical Document E451313-011B V1.
5

British Columbia Nutrition Survey: Report on Supplements
3.0 RESULTS AND DISCUSSION
3.1 Response Rate
In a large population survey such as the BCNS, the response rate depends on whether
unresolved cases (those individuals that couldn’t be contacted) were eligible to participate in the
survey. Lower and upper bounds for the response rate can be calculated based on the assumption
that all unresolved cases are eligible (lower bound), or that all unresolved cases are ineligible
(upper bound). The true rate lies somewhere between these two values. (Further details on the
response rate and its calculation are provided in the BCNS Report on Energy and Nutrient
Intakes [1]). In the BCNS, the lower and upper bounds of the response rate were 42% and 52%.
Thus, potential for non-response bias existed.
3.2 Comparison of Respondents and Non-respondents
About 66% of non-respondents completed the non-response survey, and their responses
were compared to those of study participants. Of relevance to this report was the finding that
respondents were significantly more likely than non-respondents to report use of a vitamin-
mineral supplement during the past month: For all adults, 66.2% of respondents had used a
supplement compared to 59.8% of non-respondents. Among men, 60.2% and 53.1% of
respondents and non-respondents, respectively, had used a supplement, and for women,
corresponding proportions were 71.7% and 66.4%. Accordingly, the true prevalence of
supplement use among BC adults is likely somewhat lower than the prevalence estimated in the
BCNS, and this should be kept in mind when interpreting the survey findings.
6

British Columbia Nutrition Survey: Report on Supplements
3.3 Prevalence of Use of Vitamin-Mineral and Other Supplements by BC Adults
Table 3.1 shows the proportions of BC men and women, by age group, who had taken
any type of supplement yesterday and during the past month. Overall, almost half of the
population took a supplement yesterday, and closed to two-thirds had taken a supplement within
the past month. Women appeared to be more likely than men to use supplements, both yesterday
and within the past month, and in some age groups the differences were significant (as assessed
by non-overlapping 95% Confidence Intervals). The proportions of adults using supplements
increased with age, particularly in adults over the age of 50. The BC Nutrition Survey findings
are generally comparable to those of the Food Habits of Canadians study, which found that 41%
of adults had used one or more supplements on the day before the survey (4). In that study,
women were also more likely than men to use supplements, and the prevalence of use increased
with age, from 28% of men and 35% of women aged 18 to 35, to 42% of men and 57% of
women aged 50 to 65. The Food Habits of Canadians study did not include individuals over the
age of 65, who were most likely to use supplements in the BCNS.
Table 3.1 Percent of BC adult population taking any supplement (Vitamin-mineral and/or other)
Supplement taken yesterday
Supplement taken in past month
Sex/Age Group
Percent (95% CI) Percent (95% CI) Men 19-30 28 (19 – 37) 54 (44 – 64) 31-50 35 (27 – 43) 52 (44 – 59) 51-70 44 (36 – 53) 59 (51 – 68) 71+ 65 (56 – 75) 70 (61 – 79) Women 19-30 38 (29 – 48) 62 (53 – 72) 31 – 50 46 (39 – 53) 69 (62 – 76) 51 – 70 72 (64 – 80) 79 (72 – 86) 71+ 80 (73 – 88) 84 (77 – 91) All Men and Women 46 64 Data from: BBCA Technical Document E451313-011C V3
7

British Columbia Nutrition Survey: Report on Supplements
Table 3.2 shows the proportions of BC adult men and women who took vitamin and/or
mineral supplements only, “other” supplements only, or both vitamin and/or mineral and “other”
supplements. As described earlier, the “other” supplement category includes some supplements
that contain nutrients (such as essential fatty acids and fat-soluble vitamins in oils), but consists
mainly of substances that are not recognized nutrients, although are believed by some to have
health benefits. Overall, it can be seen that more British Columbians used only vitamin and/or
mineral supplements as compared to only “other” supplements (e.g., for all adults, 24% used
only a vitamin and/or mineral supplement yesterday while 4% used only an “other” supplement
yesterday). Most of those who use “other” supplements also use a vitamin and/or mineral
supplement, as revealed by the fact that 18% of adults took both a vitamin and/or mineral
supplement and an “other” supplement yesterday. Similar observations were apparent for use of
supplements during the past month. Data from the Food Habits of Canadians Study were
consistent with the BC results. In that study, 26% took only a nutritional supplement yesterday,
11% took both nutritional and herbal supplements, and 4% used only herbal supplements (4).
8

British Columbia Nutrition Survey: Report on Supplements
Table 3.2 Percent of BC adult population taking vitamin and/or mineral supplements only, other supplements only, and both vitamin and/or mineral and other supplements
Supplement taken yesterday
Supplement taken in past month
Sex/Age Group
Percent (95% CI) Percent (95% CI) Vitamin and/or Mineral Supplements Only
Men 19 – 30 yr 17 (9 – 25) 33 (23 – 42) 31 – 50 yr 19 (13 – 26) 27 (19 – 35) 51 – 70 yr 22 (16 – 28) 28 (20 – 35) >71 yr 30 (22 – 38) 29 (22 – 37)
Women 19 – 30 yr 24 (15 – 32) 34 (24 – 43) 31 – 50 yr 26 (19 – 33) 31 (24 – 39) 51 – 70 yr 27 (21 – 34) 29 (22 – 36) >71 yr 39 (29 – 49) 40 (30 – 50)
All Men and Women 24 (21 – 26) 31 (28 – 34) Other Supplements Only
Men 19 – 30 yr 4 (0.5 – 8) 9 (3 – 14) 31 – 50 yr 6 ( 2 – 10) 9 (5 – 13) 51 – 70 yr 6 (2 – 11) 9 (3 – 14) >71 yr 3 (0.6 – 5) 4 (1 – 6)
Women 19 – 30 yr 2 (0.4 – 3) 4 (0.8 – 8) 31 – 50 yr 3 (0.4 – 5) 6 (2 – 9) 51 – 70 yr 7 (2 – 11) 4 (2 – 7) >71 yr 5 (0.7 – 9) 4 (0 – 9)
All Men and Women 4 (3 – 6) 7 (5 – 8)
Both Vitamin and/or Mineral and Other Supplements
Men 19 – 30 yr 7 (2 – 12) 13 (6 – 19) 31 – 50 yr 10 (5 – 15) 16 (10 – 22) 51 – 70 yr 16 (10 – 22) 23 (16 – 30) >71 yr 33 (24 – 41) 37 (29 – 46)
Women 19 – 30 yr 13 (6 – 20) 24 (16 – 32) 31 – 50 yr 17 (12 – 22) 32 (25 – 40) 51 – 70 yr 38 (30 – 46) 45 (37 – 53) >71 yr 37 (27 – 47) 40 (30 – 50)
All Men and Women 18 (16 – 20) 26 (24 – 29) Data from: BBCA Technical Document E451313-011C V3
9

British Columbia Nutrition Survey: Report on Supplements
The total proportions of British Columbians using vitamin and/or mineral supplements
yesterday and during the past month are shown in Figure 3.1. Data shown in this figure were
obtained by adding together the proportions who used only a vitamin and/or mineral supplement
and who used both a vitamin and/or mineral supplement and an other supplement, as shown in
Table 3.2. It can be seen that within each age group, women appeared to be more likely to use
nutritional supplements than men, and that in general, the proportions using a supplement either
yesterday or within the past month increased with age. Also, in the oldest age group it appeared
that the proportions who used a supplement yesterday and who used a supplement within the past
month were quite similar, suggesting that most older adults who use nutritional supplements do
so on a daily basis. In contrast, in the youngest age group, for both men and women, the
proportion that had used a supplement within the past month was greater than the proportion that
had used a supplement yesterday. This suggests that among younger adults, occasional use of
supplements may be more common.
10

British Columbia Nutrition Survey: Report on Supplements
Figure 3.1. Percent of British Columbians consuming a vitamin and/or mineral supplement by sex and age
0102030405060708090
19-30
31-50
51-70
71+ 19-30
31-50
51-70
71+
Perc
ent
YesterdayPast month
Men, age group Women, age group
3.4 Number of Vitamin and/or Mineral Supplements Used
Table 3.3 shows the number of vitamin and/or mineral supplements used by BC adults
who used one or more supplements on the day prior to the survey. The largest proportions of
both men and women used only one supplement; however, for all age-sex groups except men
aged 19-30, more than 50% used two or more supplements. Finally, over 25% had taken four or
more vitamin and/or mineral supplements, and almost 9% had taken six or more. The prevalence
of multiple supplement use among BC adults appears similar to that reported for Canadians as a
whole. In the Food Habits of Canadians study, 57% of supplement users used more than one
supplement on the day prior to the survey (4), compared to 65% of British Columbian
supplement users.
11

British Columbia Nutrition Survey: Report on Supplements
Table 3.3 Number of vitamin and/or mineral supplements taken yesterday by BC adults taking one or more nutritional supplements
Number of vitamin and/or mineral supplements taken yesterday by those who took a supplement yesterday
Sex/age group Consumed supplement yesterday
(%) 1 (%) 2 (%) 3 (%) 4 (%) 5 (%) >6 (%)
Men 19 – 30 yr 24 67.9 14.3 3.6 10.7 3.6 - 31 – 50 yr 29 42.6 24.6 13.1 14.8 1.6 3.3 51 – 70 yr 38 41.9 26.5 13.7 8.6 2.6 6.8 >71 yr 63 34.7 24.4 14.8 12.5 7.8 5.7
Women 19 – 30 yr 37 48.4 26.6 14.1 6.2 - 4.7 31 – 50 yr 43 35.6 21.2 18.6 5.1 5.9 13.6 51 – 70 yr 65 23.4 24.0 22.8 12.2 7.2 12.6 >71 yr 76 34.8 23.4 16.5 10.8 5.9 8.7
All men and women 42 34.8 23.4 16.5 10.8 5.9 8.7 Data from: BBCA Technical Document E451313-011C V3
Table 3.4 also presents data on the numbers of vitamin and/or mineral supplements used,
but it includes those who did not use any supplements. For men and women combined, over half
did not use a supplement yesterday, but more than 10% of the BC population had used four or
more vitamin and/or mineral supplements. Use of multiple supplements increased with age: for
example, about 3-4% of those aged 19-30 used four or more supplements yesterday, compared to
16-19% of those aged 71 and above.
12

British Columbia Nutrition Survey: Report on Supplements
Table 3.4 Number of vitamin and/or mineral supplements taken yesterday by BC adults, by age and sex
Number of supplements taken yesterday Sex/age group 0 (%) 1 (%) 2 (%) 3 (%) 4 (%) 5 (%) >6 (%)
Men 19 – 30 yr 76 16.3 3.4 0.8 2.6 0.9 - 31 – 50 yr 71 12.4 7.1 3.8 4.3 0.5 1.0 51 – 70 yr 62 15.9 10.1 5.2 3.3 1.0 2.6 >71 yr 37 21.9 15.4 9.3 7.9 4.9 3.6
Women 19 – 30 yr 63 17.9 9.8 5.2 2.3 - 1.7 31 – 50 yr 57 15.3 9.1 8.0 2.2 2.5 5.8 51 – 70 yr 35 15.2 15.6 14.8 7.9 4.7 8.2 >71 yr 24 26.4 17.8 12.5 8.2 4.5 6.6
All men and women
58 14.6 9.8 6.9 4.5 2.5 3.7
Data from: BBCA Technical Document E451313-011C V3
3.5 Use of Supplements Containing Specific Nutrients on the Day Before the Survey
The proportion of BC adults who took supplements containing specific nutrients on the
day before their participation in the survey is shown in Table 3.5 by age group and sex. Overall,
the percent of the adult population taking a nutrient supplement ranged from 14% for phosphorus
to 31% for vitamin C. Vitamin C, calcium and vitamin E were each consumed by about 30% of
BC adults. These three nutrients were also the most commonly consumed in the Food Habits of
Canadians study (4) and in the Slone Survey of Americans (3).
The pattern of supplement use varied considerably by sex and age. Overall, women were
more likely than men to use supplements containing most nutrients. As assessed by non-
overlapping 95% confidence intervals, this sex difference was significant for women aged 31 and
above for calcium and vitamin D; for women 51 and above for riboflavin, thiamin, vitamin A
and vitamin B6; for women aged 51 –70 for folate, niacin, pantothenate, vitamin B12, vitamin C
13

British Columbia Nutrition Survey: Report on Supplements
and vitamin E; and for women aged 71 and above for potassium. Other studies did not report use
of specific nutrients by age and sex, so comparisons to other North American data cannot be
made.
Supplement use tended to increase with age. For men, those aged 71 and above were
significantly more likely to calcium and vitamin D supplements than all other age groups. They
were also more likely to use a vitamin C supplement than men aged 19-30, and a vitamin E
supplement than men aged 19-50. Among women, even more differences were apparent.
Compared to women aged 19-50, women aged 71 and above were significantly more likely to
use supplements containing calcium, magnesium, niacin, phosphorus, potassium, riboflavin,
thiamin, vitamin A, vitamin B6, vitamin B12, vitamin C, vitamin D, vitamin E and zinc. With the
exception of vitamin D, which was used by more women aged 71 and above than by women
aged 51-70, the prevalence of use by women aged 51-70 was intermediate and did not differ
from women aged 19-50 or women aged 71 and above. Finally, women aged 51-70 were more
likely than younger women to use a supplement containing calcium or vitamin E.
Use of a supplement containing vitamin B12 by adults over the age of 50 warrants
additional comment, as a synthetic source of this vitamin is recommended for this age group (6).
The reason for this recommendation is that gastric acid levels in 10-30% of older adults are too
low to cleave vitamin B12 from the protein to which it is bound in foods. If this does not occur,
vitamin B12 absorption is reduced. In contrast, synthetic vitamin B12 is present in the free form,
and its absorption is not affected by low gastric acid levels. Because few foods in the Canadian
food supply are fortified with vitamin B12, in most cases a supplement would be required to
obtain the synthetic form of the vitamin. For men and women aged 51-70, the proportions
consuming a supplement containing vitamin B12 on the day prior to the survey were 17% and
14

British Columbia Nutrition Survey: Report on Supplements
39% respectively, while for those aged 71 and above, corresponding values were 30% and 47%.
Some of these older adults who do not consume a supplement may be at risk for poor absorption
of vitamin B12, even if their dietary intake is adequate.
Use of vitamin D supplements by older adults also deserves consideration. Unlike
vitamin B12, a supplemental source is not specified. However, because the distribution of
vitamin D in the food supply is limited, it is probable that many older adults would fail to meet
the Adequate Intake (AI) through diet alone (unfortunately, dietary intakes of vitamin D could
not be assessed because the Canadian Nutrient File does not contain data on vitamin D). For
example, for those over age 70, meeting the AI of 15 mcg/d would require the consumption of
six glasses of milk on a daily basis. Thus, for practical purposes, many older adults would need
to consume a supplement to meet the AI, particularly during the winter months when
endogenous synthesis is limited (11). Yet only 17% and 35% of men aged 51-70 and 71 and
above took a supplement containing vitamin D on the day before the survey. Although women
were more likely than men to use a vitamin D supplement (41% and 60% of women aged 51-70
and >71, respectively, took a supplement), the proportions who did not take a supplement were
still substantial. Accordingly, some older adults who did not use a supplement may be at risk for
suboptimal vitamin D status.
15

British Columbia Nutrition Survey: Report on Supplements
Table 3.5 Percentage (and 95% confidence interval) of BC adults taking supplements containing various nutrients yesterday by age and sex
Men (%) Women (%) Nutrient 19-30 yr 31-50 yr 51-70 yr >71 yr 19-30 yr 31-50 yr 51-70 yr >71 yr
All
Calcium (mg) 16 (8,24) 17 (11,22) 18 (12,24) 37 (28,46)# 21 (14,29) 34 (27,41) 52 (44,61)* 63 (52,72)* 29 (26,31)
Folic acid (mcg) 14 (7,22) 19 (13,25) 17 (11,22) 27 (19,35) 25 (16,33) 26 (20,33) 38 (30,45) 43 (33,53) 24 (21,27)
Iron (mg) 12 (5,19) 12 (7,17) 12 (7,17) 22 (15,29) 19 (11,26) 22 (16,27) 23 (17,29) 36 (26,46) 18 (16,20)
Magnesium (mg) 15 (8,24) 14 (9,19) 16 (10,21) 25 (18,33) 19 (12,27) 24 (18,30) 38 (30,46)* 42 (32,53)* 22 (20,25)
Niacin (mg NE) 14 (7,22) 19 (13,25) 18 (12,24) 30 (21,39) 25 (16,34) 29 (23,35) 40 (32,48) 50 (39,60) 26 (23,28)
Pantothenate (mg) 14 (7,22) 19 (13,24) 16 (10,22) 21 (14,28) 23 (14,31) 27 (21,33) 36 (28,44) 37 (27,47) 23 (20,26)
Phosphorus (mg) 11 (4,19) 9 (4,14) 11 (6,16) 18 (11,25) 9 (4,15) 13 (8,18) 20 (14,26) 32 (22,43)* 14 (11,16)
Potassium (mg) 10 (4,17) 10 (6,14) 11 (6,15) 20 (13,27) 13 (6,20) 16 (11,22) 21 (15,28) 34 (24,44)* 15 (13,17)
Riboflavin (mg) 15 (7,23) 19 (13,25) 17 (12,23) 26 (18,34) 25 (16,34) 29 (23,35) 39 (31,47) 50 (40,61)* 26 (23,28)
Thiamin (mg) 14 (7,22) 19 (13,25) 17 (11,23) 26 (18,34) 25 (16,34) 29 (23,35) 39 (31,47) 50 (40,61)* 25 (23,28)
Vitamin A (RE) 16 (3,25) 16 (10,21) 16 (11,22) 30 (21,38) 23 (15,31) 24 (18,30) 33 (26,41) 51 (41,61)* 23 (21,26)
Vitamin B6 (mg) 14 (7,22) 19 (14,25) 18 (12,24) 27 (19,35) 25 (16,34) 29 (23,36) 39 (32,47) 51 (40,61)* 26 (23,29)
Vitamin B12 (mcg) 14 (7,22) 19 (13,25) 17 (11,22) 30 (21,38) 24 (15,33) 28 (21,34) 39 (31,47) 47 (36,57)* 25 (22,28)
Vitamin C (mg) 20 (12,28) 24 (18,31) 24 (18,31) 39 (30,49)* 29 (21,38) 33 (26,39) 46 (38,54) 58 (48,68)* 31 (28,34)
Vitamin D (IU) 14 (7,22) 15 (10,21) 17 (12,23) 35 (26,43)# 21 (13,29) 28 (22,34) 41 (32,49) 60 (50,69)# 25 (23,28)
Vitamin E (eq) 18 (10,26) 18 (12,23) 29 (22,36) 45 (36,55)* 25 (17,34) 27 (21,33) 50 (42,58)* 63 (54,73)* 30 (27,32)
Zinc (mg) 13 (5,20) 13 (8,17) 14 (9,20) 23 (16,30) 18 (10,25) 20 (14,26) 29 (21,36) 41 (32,53)* 19 (17,21)
* Compared to at least one younger same-sex age group, a higher proportion of this age group took a supplement yesterday. # Compared to all younger same-sex age groups, a higher proportion of this age group took a supplement yesterday.
16

British Columbia Nutrition Survey: Report on Supplements
3.6 Use of Supplements Containing Specific Nutrients during the Month Before the Survey
The proportions of BC adults who took supplements containing specific nutrients on one
or more days in the month before their participation in the survey are shown in Table 3.6 by age
group and sex. Overall, the percent of the adult population taking a nutrient supplement ranged
from 19% for phosphorus to 46% for vitamin C. Similar to the findings for supplements taken
on the day before the survey, vitamin C, calcium and vitamin E were used by the largest
proportions of BC adults, in this case by more than 40%.
As was the case for use of supplements containing nutrients on the day prior to the
survey, women were more likely than men to use supplements of most nutrients during the
month before the survey. As assessed by non-overlapping 95% confidence intervals, this was
significant for those aged 31 – 50 for iron and pantothenate; for those aged 31 – 70 for vitamin E,
vitamin C and niacin; for those aged 31 and above for calcium, vitamin D, vitamin B6 and
riboflavin; for those aged 51 – 70 for folate, vitamin B12, and magnesium; for those aged 51 and
above for thiamin; and for those aged 71 and above for vitamin A.
Age differences were also apparent, but these were less common than was seen for use of
nutrient supplements on the day before the survey. For men, the only significant age difference
was for vitamin E, with men aged 71 and above more likely to use a supplement than men aged
31 – 50. For women, those aged 71 and above were more likely than those aged 19-30 to have
used supplements containing phosphorus, vitamin A and zinc. They were also more likely than
women aged 19-50 to have used a calcium supplement, and were more likely than all younger
women to have used a supplement with vitamin D. Women aged 51 –70 were more likely than
those aged 19 –30 to have used a calcium supplement, and women aged 51 and above were more
likely than those aged 19-30 to have used a supplement with vitamin E.
17

British Columbia Nutrition Survey: Report on Supplements
As mentioned with regard to supplement intake on the day before the survey, additional
comments about the use of supplements containing vitamin B12 by adults over 50 are warranted.
For men and women aged 51 to 70, 24% and 44% respectively had taken a supplement on one or
more days of the month preceding the survey, while for those aged 71 and above, corresponding
values were 33% and 49%. In other words, more than half the population of older adults had not
consumed any synthetic vitamin B12 in the month before the survey, suggesting that this may be
a nutrient of concern for this age group.
Similarly, Vitamin D may also be a nutrient of concern. Only 25% of men and 44% of
women aged 51-70 had taken a supplement containing vitamin D in the past month. For those
aged 71 and above, corresponding proportions were 37% and 66%. Without data on serum 25-
OH-Vitamin D levels, it is not possible to assess vitamin D status. However, recent reports
suggest that a majority of older Canadians who do not use supplements are at risk for suboptimal
vitamin D status (12).
18

British Columbia Nutrition Survey: Report on Supplements
Table 3.6 Percentage (and 95% confidence interval) of BC adults taking supplements containing various nutrients last month by age and sex
Men (%) Women (%)
Nutrient 19-30 yr 31-50 yr 51-70 yr >71 yr 19-30 yr 31-50 yr 51-70 yr >71 yr
All
Calcium (mg) 27 (18,36) 25 (18,32) 26 (19,34) 39 (30,48) 37 (28,46) 50 (42,58) 62 (54,70)* 69 (60,77)* 40 (36,43)
Folic acid (mcg) 29 (20,38) 29 (22,35) 24 (17,31) 30 (22,38) 42 (33,51) 42 (34,49) 42 (34,50) 45 (35,55) 35 (32,38)
Iron (mg) 23 (14,31) 21 (15,28) 19 (12,26) 24 (17,31) 28 (19,36) 36 (29,43) 24 (18,31) 40 (30,50) 27 (24,29)
Magnesium (mg) 26 (17,36) 22 (15,29) 23 (15,30) 28 (20,36) 28 (19,36) 40 (21,47) 42 (34,50) 46 (36,56) 31 (28,34)
Niacin (mg NE) 31 (21,40) 30 (23,37) 25 (18,32) 33 (24,42) 43 (34,52) 45 (38,52) 46 (38,54) 52 (42,62) 37 (34,40)
Pantothenate (mg) 27 (18,36) 27 (20,33) 23 (16,31) 23 (16,30) 36 (27,46) 41 (34,48) 38 (30,46) 39 (29,49) 32 (29,35)
Phosphorus (mg) 21 (12,29) 15 (9,20) 17 (11,24) 20 (13,27) 16 (9,23) 21 (15,27) 22 (16,29) 34 (25,44)* 19 (17,22)
Potassium (mg) 19 (11,27) 17 (11,23) 17 (11,24) 22 (15,29) 20 (13,28) 29 (22,36) 25 (19,32) 38 (28,48) 23 (20,25)
Riboflavin (mg) 32 (22,41) 30 (24,37) 25 (17,32) 30 (21,38) 43 (23,52) 45 (38,52) 45 (36,53) 52 (42,63) 37 (34,40)
Thiamin (mg) 29 (20,39) 30 (23,37) 24 (17,31) 29 (20,37) 43 (34,52) 45 (37,52) 45 (36,53) 52 (42,63) 37 (34,40)
Vitamin A (RE) 31 (22,41) 27 (20,34) 25 (18,32) 33 (25,42) 34 (25,43) 40 (33,47) 37 (30,45) 55 (45,65)* 34 (31,37)
Vitamin B6 (mg) 31 (22,41) 31 (24,37) 25 (18,33) 31 (22,39) 43 (34,52) 45 (38,52) 45 (37,53) 53 (43,63) 38 (35,41)
Vitamin B12 (mcg) 29 (20,39) 29 (22,36) 24 (17,31) 33 (24,41) 40 (31,50) 43 (36,50) 44 (36,53) 49 (39,59) 36 (33,39)
Vitamin C (mg) 41 (31,51) 38 (31,45) 35 (27,43) 44 (35,54) 50 (41,60) 53 (46,60) 55 (47,63) 60 (51,70) 46 (43,49)
Vitamin D (IU) 28 (19,37) 26 (19,32) 25 (18,33) 37 (28,46) 34 (25,44) 43 (36,50) 44 (36,53) 66 (58,75)# 36 (33,39)
Vitamin E (eq) 30 (21,40) 30 (23,37) 38 (29,46) 50 (40,60)* 37 (28,46) 45 (38,52) 56 (48,64)* 65 (56,75)* 41 (38,44)
Zinc (mg) 25 (16,33) 21 (15,28) 23 (16,30) 26 (19,33) 26 (18,34) 35 (28,42) 34 (26,42) 45 (35,55)* 28 (26,31)
* Compared to at least one younger same-sex age group, a higher proportion of this age group took a supplement in the previous month. # Compared to all younger same-sex age groups, a higher proportion of this age group took a supplement in the previous month.
19

British Columbia Nutrition Survey: Report on Supplements
3.7 Nutrient Intake from Supplements
Table 3.7 presents data on the minimum, median and maximum intake of
nutrients from supplements by those using supplements on the day before the survey
(‘yesterday’) and during the month before the survey (‘last month’). To facilitate
comparisons, the table also lists the recommended intake (Recommended Dietary
Allowance [RDA] or Adequate Intake [AI]) as well as the Tolerable Upper Intake Level
[UL]. Several observations may be made from the data presented in the table:
• For many nutrients, the median intake taken ‘yesterday’ corresponds to the
amounts found in typical “1-a-day” multivitamin/mineral supplements. These
amounts are below the recommended intakes for nutrients such as calcium,
phosphorus and magnesium, while they approximate (~1-3 times) the
recommended intakes for Vitamin D, thiamin, riboflavin, niacin, folic acid,
pantothenate, vitamin A, iron and zinc. Median supplemental intakes of
vitamin B12, vitamin B6, vitamin C and vitamin E in several age/sex groups
were well above the RDA.
• When the usual intakes over the past month are examined, similar patterns are
evident, although usual intakes of vitamin C fall to within 1-3 times the RDA
for most age-sex groups. This may reflect the tendency for some people to take
large doses of vitamin C only when they feel unwell, rather than on a daily
basis.
• Because the UL applies to usual intake, it is most informative to examine
intakes over the past month against the UL. When considering nutrient intake
from supplements alone, it can be seen that most maximum intakes of age-sex
20

British Columbia Nutrition Survey: Report on Supplements
groups did not exceed the UL for calcium, phosphorus, vitamin D, and vitamin
E. In contrast, maximum intakes of several age-sex groups were above the ULs
for folic acid, iron, magnesium, vitamin B6, vitamin C, and zinc. For niacin, the
median intakes of several age-sex groups and the maximal intakes of all age-sex
groups exceeded the UL. It is not possible to determine whether maximal
vitamin A intakes are above the UL, since the supplemental intakes include
vitamin A contributions from both β-carotene and preformed retinol, while the
UL applies only to preformed retinol. Further information on the role of
supplements in contributing to intakes above the UL is presented in Section 3.9.
21

British Columbia Nutrition Survey: Report on Supplements
Table 3.7 Minimum, median and maximum nutrient intakes from supplements yesterday and during the last month by age and sex
Yesterday Last monthNutrient
DRI group RDA1/AI2 UL3
Minimum Median Maximum Minimum Median Maximum
M 19-30 1000 2500 87.5 175 1219 0.3 125 1192
M 31-50 1000 2500 6.2 175 1815 4.1 99 1645
M 51-70 1200 2500 5.1 200 1500 2.9 200 2311
M 71+ 1200 2500 1.6 300 1282 1.6 223 1201
F 19-30 1000 2500 15.5 200 1175 0.2 132 3579
F 31-50 1000 2500 3.1 453 1516 1.5 196 1500
F 51-70 1200 2500 3.1 500 4203 0.3 375 4201
Calcium (mg)
F 71+ 1200 2500 3.1 490 2500 3.1 405 1725
M 19-30 4007 10005 100 600 2400 38 250 2400
M 31-50 4007 10005 10 400 5400 63 263 5400
M 51-70 4007 10005 100 400 2000 67 400 2000
M 71+ 4007 10005 50 407 5000 89 400 5000
F 19-30 4007 10005 7 600 3021 70 329 1200
F 31-50 4007 10005 14 400 2000 110 300 1992
F 51-70 4007 10005 50 400 4000 120 400 2760
Folic acid (mcg)
F 71+ 4007 10005 80 500 3500 94 500 3500
M 19-30 8 45 5.0 10 60 0.1 6.6 60
M 31-50 8 45 2.5 10 33 0.3 3.9 31
M 51-70 8 45 4.0 5.0 40 0.2 4.0 36
Iron (mg)
M 71+ 8 45 3.3 10.0 122 0.4 9.0 122
22

British Columbia Nutrition Survey: Report on Supplements
Table 3.7 (Cont’d) Yesterday Last monthNutrient
DRI group RDA/AI UL
Minimum Median Maximum Minimum Median Maximum
F 19-30 18 45 2.6 18.0 81 0.2 8.2 85
F 31-50 18 45 1.4 10.0 221 0.3 7.1 221
F 51-70 8 45 4.0 4.0 59 0.7 4.0 30
Iron (mg)
F 71+ 8 45 4.0 4.0 221 0.3 4.0 101
M 19-30 400 3504 26.7 63 600 0.9 50 600
M 31-50 420 3504 5.6 100 750 0.2 38 750
M 51-70 420 3504 5.6 100 668 1.6 82 488
M 71+ 420 3504 5.6 100 1000 5.1 100 821
F 19-30 310 3504 17.0 100 740 4.5 43 740
F 31-50 320 3504 5.6 100 1500 0.2 66 1500
F 51-70 320 3504 5.6 167 837 1.6 150 837
Magnesium (mg)
F 71+ 320 3504 5.6 100 600 5.6 100 60099
M 19-30 16 355 20.0 40 120 0.1 20.5 120
M 31-50 16 355 1.0 40 100 0.2 24.6 100
M 51-70 16 355 6.0 40 1500 3.9 34.3 1500
M 71+ 16 355 10.0 40 1500 1.6 40.0 1500
F 19-30 14 355 0.7 40 200 1.6 19.5 90
F 31-50 14 355 0.1 50 240 0.5 27.6 240
F 51-70 14 355 0.4 40 4057 0.4 40.0 4952
Niacin (mg NE)
F 71+ 14 355 6.6 40 615 0.6 40.0 424
23

British Columbia Nutrition Survey: Report on Supplements
Table 3.7 (Cont’d) Yesterday Last monthNutrient
DRI group RDA/AI UL
Minimum Median Maximum Minimum Median Maximum
M 19-30 5 - 5.0 10 60 0.1 8 60
M 31-50 5 - 0.1 20 90 0.1 10 90
M 51-70 5 - 5.0 10 450 0.2 10 450
M 71+ 5 - 5.0 10 500 1.5 10 500
F 19-30 5 - 0.1 10 100 1.0 8 60
F 31-50 5 - 0.1 12 275 0.1 10 275
F 51-70 5 - 1.4 10 310 0.8 10 300
Pantothenate (mg)
F 71+ 5 - 5.0 10 110 0.7 10 110
M 19-30 700 4000 62 125 750 4 94 750
M 31-50 700 4000 50 125 210 2 62 210
M 51-70 700 4000 50 125 250 2 125 250
M 71+ 700 3000 50 125 265 2 125 265
F 19-30 700 4000 25 125 420 5 82 345
F 31-50 700 4000 25 125 500 2 103 500
F 51-70 700 4000 50 125 471 4 125 471
Phosphorus (mg)
F 71+ 700 3000 48 125 500 8 125 500
M 19-30 1.3 - 1.6 3.2 51 0.1 2.4 51
M 31-50 1.3 - 0.3 15 100 0.1 3.2 100
M 51-70 1.3 - 1.6 3.2 100 0.3 3.2 100
Riboflavin(mg)
M 71+ 1.3 - 0.8 3.2 100 0.7 3.2 148
24

British Columbia Nutrition Survey: Report on Supplements
Table 3.7 (Cont’d) Yesterday Last monthNutrient
DRI group RDA/AI UL
Minimum Median Maximum Minimum Median Maximum
F 19-30 1.1 - 0.2 5 100 0.3 3.6 50
F 31-50 1.1 - 0.1 10 200 0.1 5.9 200
F 51-70 1.1 - 0.2 3.2 300 0.1 4.9 300
Riboflavin (mg)
F 71+ 1.1 - 1.2 3.2 100 0.1 3.2 100
M 19-30 1.2 - 1.2 2.2 52 0.1 2.1 54
M 31-50 1.2 - 0.9 15 100 0.2 2.2 100
M 51-70 1.2 - 1.2 2.2 101 0.2 2.2 101
M 71+ 1.2 - 0.8 2.2 100 0.4 2.2 148
F 19-30 1.1 - 0.6 4.5 100 0.2 4.1 50
F 31-50 1.1 - 0.1 15 200 0.1 5.9 200
F 51-70 1.1 - 0.3 3 300 0.1 4.9 300
Thiamin (mg)
F 71+ 1.1 - 1.2 2.2 100 0.1 2.2 100
M 19-30 900 30008 672 988 10320 32 909 10320
M 31-50 900 30008 255 2220 7500 16 983 6899
M 51-70 900 30008 375 1500 34880 22 1332 34880
M 71+ 900 30008 255 1332 7000 71 1332 7000
F 19-30 700 30008 289 1476 5690 29 970 5500
F 31-50 700 30008 56 1110 16500 32 988 16500
F 51-70 700 30008 255 1332 6000 49 1332 6000
Vitamin A (RAE)
F 71+ 700 30008 375 1332 7500 39 1332 7500
25

British Columbia Nutrition Survey: Report on Supplements
Table 3.7 (Cont’d) Yesterday Last monthNutrient
DRI group RDA/AI UL
Minimum Median Maximum Minimum Median Maximum
M 19-30 1.3 100 2.0 5 51 0.1 2.8 51
M 31-50 1.3 100 0.5 5 200 0.1 3.0 200
M 51-70 1.7 100 2.0 8 102 0.3 6.5 102
M 71+ 1.7 100 1.0 5 125 0.3 5.0 148
F 19-30 1.3 100 0.3 6 100 0.3 4.3 55
F 31-50 1.3 100 0.1 8 200 0.1 5.0 200
F 51-70 1.5 100 0.4 8 400 0.2 7.1 300
Vitamin B6 (mg)
F 71+ 1.5 100 1.0 8 600 0.1 6.9 600
M 19-30 2.4 - 6.0 20 267 0.2 8.3 236
M 31-50 2.4 - 3.0 20 209 0.2 12 4849
M 51-70 2.46 - 6.0 24 510 1.0 16 436
M 71+ 2.46 - 3.0 25 1200 1.4 20 1200
F 19-30 2.4 - 1.7 18 232 0.9 12 184
F 31-50 2.4 - 0.8 20 3070 0.3 13 5999
F 51-70 2.46 - 2.0 25 9210 0.5 25 9210
Vitamin B12 (mcg)
F 71+ 2.46 - 2.0 25 1250 0.3 25 1100
M 19-30 90 2000 60 125 2150 3 90 2150
M 31-50 90 2000 81 650 2300 3 180 2116
M 51-70 90 2000 50 500 2722 16 230 2722
Vitamin C (mg)
M 71+ 90 2000 15 500 4200 5 391 4200
26

British Columbia Nutrition Survey: Report on Supplements
Table 3.7 (Cont’d)
Yesterday Last monthNutrient
DRI group RDA/AI UL
Minimum Median Maximum Minimum Median Maximum
F 19-30 75 2000 50 180 2000 8 99 2171
F 31-50 75 2000 45 500 5145 3 209 4090
F 51-70 75 2000 20 500 9000 10 200 5320
Vitamin C (mg)
F 71+ 75 2000 50 120 12000 6 120 12000
M 19-30 200 2000 200 400 2400 5 286 2400
M 31-50 200 2000 36 400 1800 6 171 1343
M 51-70 400 2000 67 400 1400 7 381 1380
M 71+ 600 2000 85 400 1748 13 383 1748
F 19-30 200 2000 24 400 1400 1 263 874
F 31-50 200 2000 48 400 1200 9 279 1600
F 51-70 400 2000 50 400 1400 18 400 1720
Vitamin D (IU)
F 71+ 600 2000 50 400 2472 6 400 2472
M 19-30 1510 100011 6.7 34 311 0.2 20 454
M 31-50 1510 100011 16.8 40 670 0.1 27 670
M 51-70 1510 100011 20.1 268 1071 4.3 153 1071
M 71+ 1510 100011 6.7 268 1139 1.0 268 1139
F 19-30 1510 100011 6.7 34 733 0.9 20 1006
F 31-50 1510 100011 0.5 80 840 0.5 20 840
F 51-70 1510 100011 6.7 268 1097 3.3 268 1097
Vitamin E (eq)9
F 71+ 1510 100011 6.7 268 2412 0.4 268 2412
27

British Columbia Nutrition Survey: Report on Supplements
Table 3.7 (Cont’d)
Yesterday Last monthNutrient
DRI group RDA/AI UL
Minimum Median Maximum Minimum Median Maximum
Zinc (mg) 11 40 7.5 15 90 0.1 11 90
M 31-50 11 40 0.4 15 60 0.1 6 60
M 51-70 11 40 5.0 15 108 0.2 15 100
M 71+ 11 40 1.1 15 100 0.7 15 100
F 19-30 8 40 0.3 15 150 0.7 13 150
F 31-50 8 40 0.6 15 68 0.2 9 68
F 51-70 8 40 0.3 15 55 0.3 15 50
F 71+ 8 40 1.0 15 75 1.0 15 75
M 19-30
Data obtained from BBCA E451311-011CV1 – Supplement Tables, Stephen Hayward, January 2003 1. RDA = Recommended Dietary Allowance 2. AI = Adequate Intake 3. UL = Tolerable Upper Intake Level 4. The UL for magnesium applies only to intake from supplements and pharmacologic agents 5. The UL for niacin and folic acid apply only to intake from supplements and fortified foods 6. Adults over 50 are advised to meet their RDA for vitamin B12 mainly by consuming fortified foods or a supplement 7. The RDA for folate is expressed as dietary folate equivalents (DFE), where 1 DFE = 1 µg food folate, or 0.6 µg from fortified food, or 0.5 µg from a
supplement taken on an empty stomach. 8. The UL for vitamin A applies only to intake from preformed retinol. 9. Vitamin E intakes from supplements are expressed as α-tocopherol equivalents. This older nomenclature also included a vitamin E value for tocopherols
other than α-tocopherol and for some tocotrienols, while the current RDA applies only to α-tocopherol 10. The RDA for vitamin E is expressed in mg α-tocopherol. This includes the RRR-α-tocopherol found in founds and the 2R stereoisomers that occur in
fortified foods and supplements. 11. The UL for vitamin E applies to any form of supplemental vitamin E (i.e., both the 2R and the 2S stereoisomers).
28

British Columbia Nutrition Survey: Report on Supplements
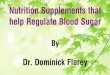
3.8 Effect of Supplement Intake on the Prevalence of Nutrient Inadequacy
The effect of supplement use on the prevalence of nutrient inadequacy among BC adults
is shown in Table 3.8 and Figure 3.2. This was assessed by comparing the proportions with
usual intakes below the EAR from food alone and from the combination of food plus
supplements. For all nutrients except niacin (which had a “zero” prevalence of inadequacy from
food alone) consideration of supplement use reduced the population prevalence of inadequacy,
although the reduction was not significant for thiamin, riboflavin, phosphorus and zinc.
Supplement use was associated with significant reductions in the population prevalence of
inadequacy for folate, vitamin B12 and vitamin C, and the differences approached significance
for vitamin B6 and magnesium. When the data were examined by sex and age group, similar
trends were observed, but in most cases, the differences were not significant because of broad
confidence intervals. However, supplement use significantly decreased the prevalence of dietary
folate inadequacy for women aged 31-50, 51-70, and 71 and above. Use of supplemental folic
acid also increased the proportion of women aged 19-50 who met the recommendation to
consume 400 mcg folic acid per day to prevent neural tube defects. No women met the
recommendation from food alone, compared to 16% from food plus supplements (data not
shown in Table).
29

British Columbia Nutrition Survey: Report on Supplements
Table 3.8 Effect of supplement use on the apparent prevalence (and 95% confidence interval) of nutrient inadequacy in BC adults
Men (age in years) Women (age in years) 19-30 31-50 51-70 >71 19-30 31-50 51-70 >71
All
Thiamin <EAR (food) 3%
(0,6) 0.7% (0,2)
5% (2,9)
3% (0.4,6)
7% (2,11)
14% (8,20)
14% (8,20)
5% (0.7,10)
7% (5,9)
<EAR (fd/supp) 2% (0,5)
0.5% (0,1)
4% (0.9,7)
1% (0.2,3)
5% (0,9)
11% (6,16)
7% (3,11)
1% (0,3)
5% (3,6)
Riboflavin <EAR (food) 3%
(0,7) 3%
(0,5) 3%
(0.5,5) 5%
(1,8) 2%
(0,5) 8%
(3,12) 4%
(0.2,8) 3%
(1,5) 4%
(3,5) <EAR (fd/supp) 2%
(0,5) 3%
(0,5) 3%
(0.3,5) 4%
(0.7,7) 2%
(0,5) 6%
(2,10) 0.5% (0,1)
1% (0.5,2)
3% (2,4)
Niacin <EAR (food) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) <EAR (fd/supp) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) 0%
(0,0) Vitamin B6 <EAR (food) 2%
(0.2,4) 0.3%
(0,0.8) 21%
(14,29) 19%
(12,25) 16%
(9,23) 19%
(13,25) 29%
(22,37) 36%
(26,45) 15%
(13,17) <EAR (fd/supp) 2%
(0,30 0.3%
(0,0.8) 19%
(12,26) 15%
(9,21) 13%
(6,19) 15%
(10,20) 16%#
(11,22) 20%
(12,28) 11%# (9,13)
Folate <EAR (food) 2%
(0,6) 5%
(2,8) 20%
(14,27) 35%
(26,44) 32%
(23,41) 40%
(33,47) 47%
(39,56) 67%
(58,76) 27%
(24,30) <EAR (fd/supp) 2%
(0,6) 3%
(1,5) 16%
(10,23) 27%
(18,36) 19%
(11,27) 23%*
(17,29) 29%*
(22,37) 39%*
(29,49) 17%*
(15,19) Vitamin B12 <EAR (food) 7%
(2,13) 10%
(5,16) 8%
(4,12) 13%
(6,19) 38%
(28,48) 25%
(18,32) 20%
(14,27) 18%
(11,25) 18%
(15,20) <EAR (fd/supp) 5%
(0.6,10) 9%
(4,14) 7%
(4,11) 12%
(5,18) 21%
(13,29) 16%
(11,22) 13%
(8,18) 10%
(4,15) 12%*
(10,14) Vitamin C <EAR (food) 31%
(22,41) 42%
(33,50) 34%
(26,43) 27%
(19,34) 33%
(24,42) 32%
(25,39) 20%
(13,26) 26%
(18,35) 32%
(29,35) <EAR (fd/supp) 25%
(16,35) 34%
(26,41) 26%
(18,34) 16%
(10,23) 23%
(15,32) 21%
(15,28) 11%
(5,16) 13%
(7,19) 23%*
(20,26) Magnesium <EAR (food) 32%
(21,42) 33%
(24,42) 44%
(35,53) 62%
(53,72) 37%
(28,46) 43%
(35,50) 40%
(32,48) 45%
(35,56) 39%
(36,43) <EAR (fd/supp) 31%
(20,41) 31%
(22,39) 37%
(28,45) 52%
(43,61) 31%
(22,39) 36%
(29,44) 27%
(19,34) 26%#
(18,35) 33%#
(29,36)
30

British Columbia Nutrition Survey: Report on Supplements
Table 3.8 (cont’d) Men (age in years) Women (age in years)
19-30 31-50 51-70 >71 19-30 31-50 51-70 >71 All
Phosphorus <EAR (food) 0.2%
(0,0.6) 0.2%
(0,0.6) 2%
(0,4) 0.1%
(0.0.2) 0.3%
(0,0.8) 2%
(0,5) 3%
(0.8,6) 2%
(0.5,4) 1%
(0.6,2) <EAR (fd/supp) 0.2%
(0,0.6) 0.2%
(0,0.6) 2%
(0,4) 0.1%
(0,0.2) 0.3%
(0,0.8) 2%
(0,5) 3%
(0.6,6) 2%
(0.5,4) 1%
(0.6,2) Zinc <EAR (food) 7%
(2,12) 11%
(6,17) 26%
(18,33) 42%
(34,51) 11%
(4,18) 11%
(6,15) 20%
(13,27) 19%
(11,27) 15%
(13,18) <EAR (fd/supp) 7%
(2,12) 11%
(5,16) 18%
(12,24) 33%
(24,41) 8%
(2,14) 10%
(5,15) 13%
(8,19) 10%
(5,15) 12%
(10,14) EAR = Estimated Average Requirement. The proportion of a group with usual intakes below the EAR approximates the population prevalence of inadequate intakes. * 95% Confidence intervals do not overlap; P < 0.05 # 95% Confidence intervals do not overlap, but upper boundary of CI for food alone is the same as lower boundary of CI for food plus supplements; significance thus approximates P = 0.05. Source: BBCA E451311-011CV1 – Supplement Tables, Stephen Hayward, January 2003
31

British Columbia Nutrition Survey: Report on Supplements
Figure 3.2. Prevalence of inadequate vitamin and mineral intakes from food alone, and food from plus supplements, among British Columbia adults.
#
0 5 10
Thiamin
Riboflavin
Niacin
Vitamin B6
Folate
Vitamin B12
Vitamin C
Magnesium
Phosphorus
Zinc
Food + Supplements
Supplement use significantly reVitamin B12 and folate (p<0.05vitamin B6 approached signific(Source: BBCA E451311-011C For nutrients that do n
supplement use on the prevalen
does not have an EAR, the d
requirement distribution is re
comparisons can be made that
supplements can be compared,
median intake meets or excee
15 20 25
Prevalence of inadequa
Food
duced the prevalence o), while the reduction iance (p~0.05).
V1 – Supplement Tab
ot have an EAR (cal
ce of inadequacy cann
istribution of requirem
quired to assess the p
may provide some insi
as a population can b
ds the AI. This is pa
30
cy (%)
f inaden inade
les, Ste
cium a
ot be q
ents is
revalen
ght. Fi
e assum
rticular
35 4
quate intakquate intak
phen Hayw
nd pantoth
uantitativel
not known
ce of inad
rst, median
ed to hav
ly true whe
0 45
es of Vitamin C, es of magnesium and
ard, January 2003)
enic acid), the effect of
y assessed. (If a nutrient
, and knowledge of the
equacy.) However, two
intakes with and without
e adequate intakes if the
n the AI was set as the
32

British Columbia Nutrition Survey: Report on Supplements
median intake of a healthy population, which is the case for pantothenic acid but not for calcium.
Second, the proportion of the population with intakes that meet the AI can be examined.
Although an intake below the AI cannot be assumed to be inadequate, intakes at or above the AI
can be assumed to be adequate.
Tables 3.9 and 3.10 provide data on the effect of supplement use on calcium intakes of
BC adults. As shown in Table 3.9, supplement use increased median intakes in all age/sex
groups, but in no case did it change the median intake from below the AI to at or above the AI.
Young men were the only age group with a median intake that met the AI, and this occurred
whether or not supplement use was considered.
Table 3.9 Effect of supplement use on median usual calcium intakes of BC adults Age/sex group Adequate Intake
(mg/d) Median Intake, Food
(mg/d) Median Intake, Food
plus Supplements (mg/d)
Men 19-30 yr 1000 1044 1050 31-50 yr 1000 883 906 51-70 yr 1200 772 885 >71 yr 1200 727 847 Women 19-30 yr 1000 761 852 31-50 yr 1000 679 827 51-70 yr 1200 667 863 >71 yr 1200 662 948 Source: BBCA E451311-011CV1 – Supplement Tables, Stephen Hayward, January 2003
Table 3.10 shows the impact of supplement use on the proportion of adults with calcium
intakes at or above the AI. For men aged 50 or less, supplement use had essentially no impact on
the proportion meeting the AI, although for older men, there were modest increases. In contrast,
consideration of supplement use increased the proportion of women of all ages that met the AI.
33

British Columbia Nutrition Survey: Report on Supplements
This was particularly apparent for those over the age of 50, among whom the proportions
meeting the AI increased from 4% to 40% (age 51-70) and from 8% to 44% (age >71).
Table 3.10 Effect of supplement use on the proportion of BC adults meeting the adequate intake (AI) for calcium Age/sex group Adequate Intake
(mg/d) Proportion Meeting
AI from Food Proportion Meeting AI from Food plus
Supplements Men 19-30 yr 1000 53% 54% 31-50 yr 1000 42% 42% 51-70 yr 1200 12% 19% >71 yr 1200 9% 22% Women 19-30 yr 1000 26% 33% 31-50 yr 1000 13% 31% 51-70 yr 1200 4% 40% >71 yr 1200 8% 44% Source: BBCA E451311-011CV1 – Supplement Tables, Stephen Hayward, January 2003 Similar comparisons are made in Tables 3.11 and 3.12 for pantothenic acid. Table 3.11
shows that median intakes of men were at or above the AI whether or not supplement use was
considered. In contrast, women’s median intakes increased from below the AI to meet or almost
meet the AI when supplements were considered. Table 3.12 shows that consideration of
supplement use increased the proportions who met the AI for all age/sex groups, and that the
increases were greater in women than men.
34

British Columbia Nutrition Survey: Report on Supplements
Table 3.11 Effect of supplement use on the median usual pantothenic acid intakes of B.C. adults Age/sex group Adequate Intake
(mg/d) Median Intake, Food
(mg/d) Median Intake, Food
plus Supplements (mg/d)
Men 19-30 yr 5 6.7 7.1 31-50 yr 5 5.6 5.9 51-70 yr 5 5.3 6.0 >71 yr 5 4.9 5.4 Women 19-30 yr 5 4.0 4.9 31-50 yr 5 4.0 5.0 51-70 yr 5 4.2 5.0 >71 yr 5 3.9 4.6 Source: BBCA E451311-011CV1 – Supplement Tables, Stephen Hayward, January 2003 Table 3.12 Effect of supplement use on the proportion of BC adults meeting the adequate intake (AI) for pantothenic acid Age/sex group Adequate Intake
(mg/d) Proportion Meeting
AI from Food Proportion Meeting AI from Food plus
Supplements Men 19-30 yr 5 81.3% 85.1% 31-50 yr 5 73.0% 77.9% 51-70 yr 5 58.5% 66.7% >71 yr 5 48.8% 59.5% Women 19-30 yr 5 19.7% 48.0% 31-50 yr 5 20.8% 49.3% 51-70 yr 5 19.5% 49.8% >71 yr 5 15.0% 45.5% Source: BBCA E451311-011CV1 – Supplement Tables, Stephen Hayward, January 2003 3.9 Effect of Supplement Use on the Prevalence of Excessive Intakes In addition to reducing the prevalence of inadequate nutrient intakes, supplement use can
increase the potential risk of adverse effects from excessive intakes, and this can be assessed by
examining the prevalence of intakes that exceed the Tolerable Upper Intake Level (UL). (Note
that this could not be assessed for vitamin A, as the UL applies to preformed retinol only, and
35

British Columbia Nutrition Survey: Report on Supplements
these values were not available in the BCNS). As shown in Table 3.13, the prevalence of intakes
above the UL was close to zero for most nutrients for both men and women when intakes from
food alone were considered. Supplement use was associated with a substantial prevalence of
intakes above the UL for niacin (10-37%, depending on age/sex group). The adverse effect
associated with excessive intakes of niacin is flushing, which although uncomfortable, does not
appear to be medically dangerous and is easily terminated by reducing or stopping the
supplement dose (6). Supplement use was associated with smaller increases in the prevalence of
intakes above the UL for calcium, vitamin B6, folic acid, vitamin C, vitamin E, iron and zinc (<1
– 7%). Although the prevalence of intakes above the UL for vitamin B6 was relatively low, it is
nevertheless of potential concern since the adverse effect (peripheral neuropathy) is serious and
may not be reversible. The finding that depending on the age/sex group, between 2% and 7% of
BC adults were above the UL for folic acid also warrants comment. Here, the concern is that
excessive folate intakes may mask development of vitamin B12 deficiency. However, 84% of
those with folic acid intakes above the UL were also using a vitamin B12 supplement, suggesting
that very few individuals are at risk of deficiency.
36

British Columbia Nutrition Survey: Report on Supplements
Table 3.13 Effect of supplement use on the prevalence of BC adults with usual intakes above the tolerable upper intake level (UL) Men Women Nutrient
Age group (yr)
UL (mg/d)
>UL, food alone (%)
>UL, food and supplements
(%)
>UL, food alone (%)
>UL, food and supplements
(%) Calcium 19-30 2500 1 1 0 <1 31-50 2500 0 0 0 0 51-70 2500 0 0 0 3 >71 2500 0 0 0 1 Folic acid1 19-30 1 0 3 0 4 31-50 1 0 4 0 4 51-70 1 0 2 0 5 >71 1 0 7 0 5
Iron 19-30 45 0 1 0 3 31-50 45 0 <1 0 3 51-70 45 0 <1 0 0 >71 45 0 5 0 1
Niacin1 19-30 35 N/A 10 N/A 11 31-50 35 N/A 12 N/A 20 51-70 35 N/A 12 N/A 27 >71 35 N/A 19 N/A 37
Phosphorus 19-30 4000 <1 <1 0 0 31-50 4000 0 0 0 0 51-70 4000 0 0 0 0 >71 3000 <1 <1 0 0 Vitamin B6 19-30 100 0 0 0 0 31-50 100 0 <1 0 3 51-70 100 0 2 0 5 >71 100 0 2 0 5
Vitamin C 19-30 2000 0 2 0 <1 31-50 2000 0 <1 0 3 51-70 2000 0 1 0 2 >71 2000 0 1 0 1
37

British Columbia Nutrition Survey: Report on Supplements
Table 3.13 (Cont’d) Men Women Nutrient
Age group (yr)
UL (mg/d)
>UL, food alone (%)
>UL, food and supplements
(%)
>UL, food alone (%)
>UL, food and supplements
(%) Vitamin E2 19-30 1000 N/A 0 N/A <1 31-50 1000 N/A 0 N/A 0 51-70 1000 N/A <1 N/A <1 >71 1000 N/A 1 N/A 0
Zinc 19-30 40 0 4 0 3 31-50 40 <1 2 0 1 51-70 40 3 6 <1 3 >71 40 0 6 0 6 1. The UL for niacin and folate apply only to intake from supplements and/or fortified foods. For niacin, data on intake from fortified foods were not available. 2. The UL for vitamin E applies only to intake from supplements. 3.10 Other Supplements Used
Table 3.14 shows the proportions of BC adults who took one or more non-vitamin-
mineral supplements on the day before the survey and in the previous month. Overall, just over
a fifth had used a supplement yesterday, while about one-third had used a supplement during the
previous month. Confidence intervals were not available for these data, so the significance of
differences between sexes and across age groups cannot be determined. However, it appears that
women were somewhat more likely than men to have taken a non-vitamin-mineral supplement,
and that the prevalence of use tended to increase with age.
These observations are generally similar to those of a survey of members of a group
health maintenance organization in northern California, among whom 33% had used at least one
non-vitamin-mineral supplement during the past year (13). In that survey, use of all non-
vitamin-mineral supplements was highest among women aged 45-64 years of age who were
college graduates.
38

British Columbia Nutrition Survey: Report on Supplements
Table 3.14 Percent of BC adult population using non-vitamin-mineral supplements Supplement Consumed Sex/Age Group
Yesterday (%) Past Month (%) Men 19 – 30 yr 11 22 31 – 50 yr 16 25 51 – 70 yr 22 32 >71 yr 36 41
Women 19 – 30 yr 15 28 31 – 50 yr 20 38 51 – 70 yr 45 49 >71 yr 42 44
All Men and Women 22 33 Data from: BBCA Technical Document E451313-011C V3
A wide variety of non-vitamin/mineral supplements was used by study participants, and
these are listed in Table 3.15. The most commonly-cited substances were glucosamine and/or
chondroitin sulfate, garlic, various oils, echinacea and gingko biloba. In the Food Habits of
Canadians Study, the most frequently-cited non-vitamin-mineral supplements were garlic, an
herbal mix, evening primrose oil and Echinacea (4), while in the study of members of a health
maintenance organization in California, echinacea, gingko biloba and glucosamine were the most
frequently used products (13).
39

British Columbia Nutrition Survey: Report on Supplements
Table 3.15 Other supplements used by participants in the BC Nutrition Survey
Type of supplement Number using Glucosamine and/or chondroitin sulfate 208 Garlic 141 Oils (including flaxseed, evening primrose, oil blends, gamma-linolenic acid, borage)
125
Echinacea 121 Gingko biloba 112 Lecithin 57 Ginseng 45 Coenzyme Q10 43 Greens 37 St. John’s Wort 36 Lactic acid bacteria 34 Algae 34 Saw palmetto 25 Protein or amino acids 22 Grape seed extract 22 Cayenne 15 Cranberry 13 Prostate care 11 Devil’s claw 8 Milk thistle 7 Alfalfa 7 Royal jelly 7 Kava kava 7 Creatine monohydrate 6 Bee pollen 5 Other (unspecified) 308 Other (used by <4) 37 Data from: BBCA Technical Document E451313-011C V3References. Unweighted data. A discussion of the potential health benefits and/or adverse effects of these substances is
beyond the scope of this report. However, the potential of some of these products to interact
with certain prescription medications has been recognized (14-16), suggesting that it is important
for health professionals to ascertain their use by patients.
40

British Columbia Nutrition Survey: Report on Supplements
4.0 CONCLUSIONS
Data obtained in the British Columbia Nutrition Survey indicate that supplement use is
common among BC adults, particularly among seniors and women. The high prevalence of
supplement use emphasizes the importance of considering the contribution of supplements when
assessing dietary intake, whether that assessment is occurring at an individual level (e.g., a
dietitian assessing a client’s diet) or at a population level (e.g., using survey data to formulate
public policy recommendations). In the BCNS, consideration of supplement use reduced the
population prevalence of inadequacy for all nutrients except niacin (which had a “zero”
prevalence of inadequacy from food alone). Although the reductions were not significant for
thiamin, riboflavin, phosphorus and zinc, significant reductions were observed in the population
prevalence of inadequacy for folate, vitamin B12 and vitamin C, and the differences approached
significance for vitamin B6 and magnesium. The impact of supplementation of nutrient
adequacy cannot be quantitatively assessed for nutrients (such as calcium) that have an AI rather
than an EAR. However, use of calcium supplements did increase the proportions of individuals
(especially women) with intakes at or above the AI, although it did not increase median intakes
to meet the AI.
The new Dietary Reference Intakes reflect advances in our knowledge of nutrient
physiology and the role of nutrients in chronic disease prevention. In the past, dietary guidance
was based on the assumption that healthy individuals consuming a varied diet could meet all
their nutrient needs through food alone, and that supplementation was therefore not required.
Given current levels of fortification of the Canadian food supply, this assumption no longer
applies to some nutrients and some age/sex groups. Specifically, the DRIs recommend that all
women of child-bearing potential obtain 400 mcg of folic acid per day, and that adults over the
41

British Columbia Nutrition Survey: Report on Supplements
age of 50 obtain the majority of their RDA for vitamin B12 through synthetic sources.
Furthermore, although a specific recommendation for supplementation is not made, for practical
purposes most adults over the age of 50 will require a supplement to meet the AI for vitamin D.
In the BCNS, most individuals to whom these recommendations apply were not using the
appropriate supplement. Future dietary guidance may therefore need to include advice on
supplement use. In this regard, there may be a need to develop effective methods of educating
the public about supplements.
In addition to recognizing the positive contributions of supplements, it is also important
to consider their potential to lead to excessive nutrient intakes. In the BCNS, the prevalence of
nutrient intakes above the UL increased when supplement use was considered. In many cases,
the increases were modest (e.g., from 2% with diet alone to 5% with supplements), and although
the prevalence of excessive intakes of niacin was high at 10-37%, the health implications do not
appear to be serious. Nevertheless, particularly if current trends in supplement use continue,
monitoring this situation is warranted, as excessive intakes of some nutrients are associated with
serious and/or irreversible adverse effects.
Supplements used by BC adults included a wide variety of substances other than vitamins
and minerals. Because some of these substances interact with prescription medications, it may
become increasingly important for health professionals to inquire about their clients’ use of these
supplements.
42

British Columbia Nutrition Survey: Report on Supplements
5.0 REFERENCES 1. British Columbia Ministry of Health Planning. British Columbia Nutrition Survey: Nutrient
Report. Victoria BC: Ministry of Health Planning, 2004.
2. Balluz LS, Kieszak SM, Philen RM, Mulinare J. Vitamin and mineral supplement use in the
United States. Results from the Third National Health and Nutrition Examination Survey.
Arch Fam Med 2000;9:258-262.
3. Kaufman DW, Kelly JP, Rosenberg L, Anderson TE, Mitchell AA. Recent patterns of
medication use in the ambulatory adult population of the United States. The Slone Survey.
JAMA 2002;287:337-344.
4. Troppmann L, Johns T, Gray-Donald K. Natural health product use in Canada. Can J Public
Health 2002;93:426-430.
5. Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Calcium,
Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington DC: National Academy
Press, 1997.
6. Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Thiamin,
Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline.
Washington DC: National Academy Press, 1998.
7. Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Vitamin C,
Vitamin E, Selenium, and Carotenoids. Washington DC: National Academy Press, 2000.
8. Food and Nutrition Board, Institute of Medicine Dietary Reference Intakes for Vitamin A,
Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum,
Nickel, Silicon, Vanadium, and Zinc. Washington DC: National Academy Press, 2001.
43

British Columbia Nutrition Survey: Report on Supplements
9. Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Energy,
Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids
(Macronutrients). Washington DC: National Academy Press, 2002.
10. Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes. Applications in
Dietary Assessment. Washington DC: National Academy Press, 2000.
11. Webb AR, Kline L, Holick MF. Influence of season and latitude on the cutaneous synthesis
of vitamin D3: exposure to winter sunlight in Boston and Edmonton will not promote vitamin
D3 synthesis in human skin. J Clin Endocrinol Metab 1988;67: 373-378.
12. Rucker D, Allan JA, Fick GH, Hanley DA. Vitamin D insufficiency in a population of
healthy western Canadians. Can Med Assoc J 2002;166:1517-1524.
13. Schaffer DM, Gordon NP, Jensen CD, Avins AL. Nonvitamin, nonmineral supplement use
over a 12-month period by adult members of a large health maintenance organization. J Am
Diet Assoc 2003;103:1500-1505.
14. Abebe W. An overview of herbal supplement utilization with particular emphasis on possible
interactions with dental drugs and oral manifestations. J Dent Hygiene 2003; 77(1):37-46.
15. Tessier DJ, Bash DS. A surgeon's guide to herbal supplements. J Surg Res 2003;114:30-36.
16. Dasgupta A. Review of abnormal laboratory test results and toxic effects due to use of herbal
medicines. Am J Clin Pathol 2003;120:127-137.
44