Embed Size (px)
Citation preview

1

Ministry Health Care 2
Communities We Serve
500 South Oakwood Road, Oshkosh, Wisconsin 54904

Ministry Health Care 3
TABLE OF CONTENTS Executive Summary………………………………………………………………………. 4 Organizational Commitment…………………………………………………………… 6 Community..………………………………………………………………………………. 9 Community Involvement ………………………………………………………………... 15 Community Needs Assessment Process……………………………………………….. 15 Health Priorities…………………………………………………………………………... 18 Community Assets ……………………………………………………………………….. 19 Data Gaps ………………………………………………………………………………... 20 Community Benefit and Economic Value…………………………………………….. 20 Next Steps………………………………………………………………………………… 22 Appendices
Appendix 1 _ Affinity Community Benefit Council Membership .………………… 22
Appendix 2 _ Fox Valley Regional Community Health Coalition Membership … 23
Appendix 3 _ re:Think Mental Health Shareshop Membership……………………. 24
Appendix 4 _ Mercy Medical Center Primary Service Area………………………... 26
Appendix 5 _ Educational Attainment/Age Distribution by Industry …………….. 27
Appendix 6 _ Wage Distribution/Employment .…………………………………….. 28
Appendix 7 _ Prominent Employers ………………………………………………….. 29
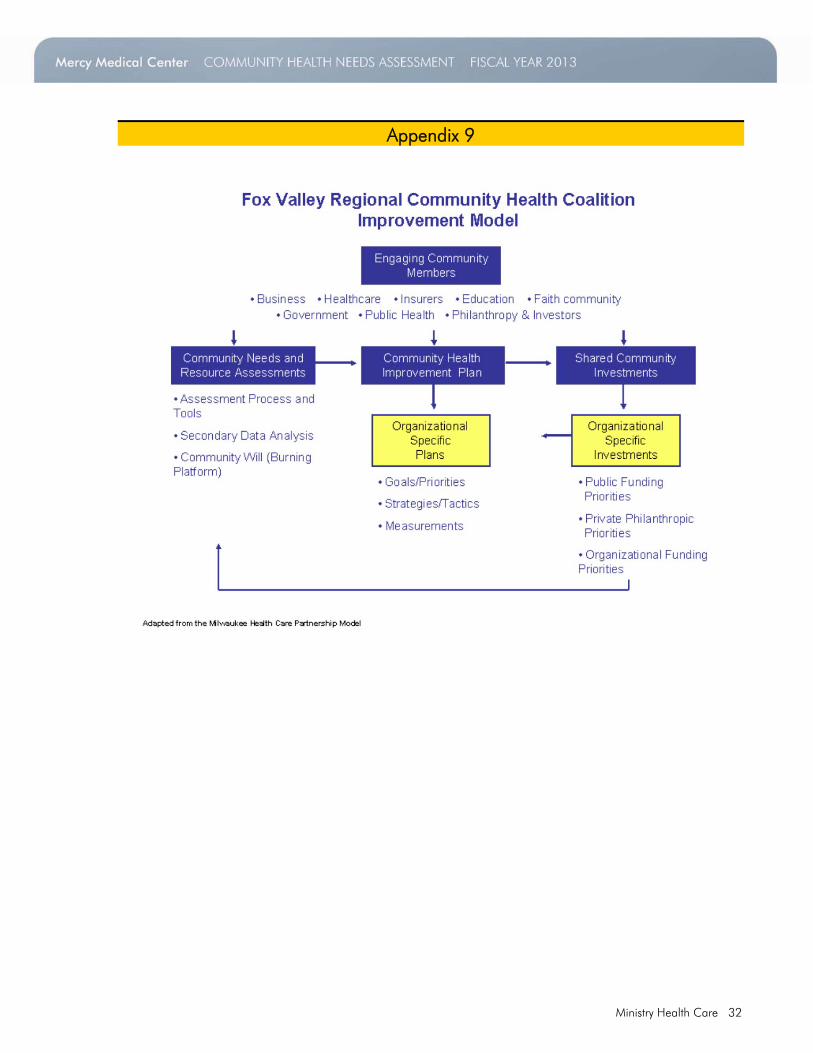
Appendix 8 _ Winnebago County Community Health Improvement Planning Membership………………………………………………….. 30 Appendix 9 _ Community Health Improvement Model ……………………………. 32
Appendix 10 _ Our Approach ………………………………………………………..… 33
Appendix 11 _ List of Sources ………………………………………………………..… 34
Appendix 12 _ Winnebago County Community Need Index ………………….. 36
Appendix 13 _ Summary of Identified Health Needs……………………………..... 37
Appendix 14 _ Mercy Medical Center FY12 Community Benefit Report ………… 38
Appendix 15 _ Behavioral Risk Factors Surveillance Study………………………… 39
Appendix 16 _ Winnebago County Health Rankings ………………………………. 40
Appendix 17 _ Mercy Medical Center Top 10 Diagnoses Codes/Affinity Medical Group Top 3 Diagnoses……………………………………………….. 41

Ministry Health Care 4
Mercy Medical Center Community Health Needs Assessment ______________________________________________________________________________________ Executive Summary
Mercy Medical Center is a member of Affinity Health System (Affinity). Affinity is one of the largest safety-net providers in the Fox Valley. The three Affinity hospitals, St. Elizabeth Hospital (Appleton, Wisconsin) Mercy Medical Center (Oshkosh, Wisconsin) and Calumet Medical Center (Chilton, Wisconsin), serve a diverse population of urban and rural residents.
Mercy Medical Center is proud to serve the Oshkosh community by providing quality patient care for more than a century. In 1891, Father Roman Scholter, pastor of St. Mary's Church in Oshkosh, convinced the Sisters of the Sorrowful Mother to come to Oshkosh and start a hospital. In response to the growing Oshkosh population, the hospital has expanded and grown over the years. Today, Mercy Medical Center provides total health care, including emergency/trauma care and surgical services, as well as many medical specialties, such as cardiology, oncology, orthopedics, intensive care, obstetrics and neurosurgery. Mercy is the home of the Kennedy Center for the Hip and Knee, a nationally-recognized program for hip replacement. In fiscal year 2012, Mercy Medical Center had 157 patient beds, 19,056 ER visits, 658 babies delivered and more than 106 skilled medical staff, 770 employees and 491 volunteers. Mercy Medical Center treats patients with dignity and compassion.
Mercy Medical Center’s Community Health Needs Assessment and Implementation Plan document our commitment to the health and improved quality of life in our community, evidenced by:
Written statements (e.g., mission and value statement; community benefit and outreach
plan; annual operating targets for community benefit and outreach) Organizational structures (e.g., Senior Vice President of Mission and Culture Integration
who reports directly to the CEO; the Community Benefit Council is interdivisional and includes Executive Members at its quarterly meetings)
Policies (e.g., financial assistance policy; billing and collection policy, expectations about community involvement and community benefit as part of performance evaluations)
Allocation of institutional resources (e.g., $6,077,664 million in FY2012 using state and federal mandated reporting guidelines).
The overarching goal of Mercy Medical Center’s community benefit and outreach is to respond to identified community health needs, increase access and improve health status, especially for the most vulnerable and underserved individuals and families in our community, and to be a leader and serve as an example to others in community service.
Every three years, Mercy Medical Center performs community needs assessments to evaluate the overall health status of the communities it serves. The information from these assessments is routinely used to guide the strategic planning processes of the organization-at-large.
Mercy Medical Center in collaboration with our local community health partners is pleased to present the following Community Health Needs Assessment to community residents, organizations and civic groups after engaging in a three year strategic planning process. Mercy Medical Center partnered with over 65 member organizations and individuals who represent a broad spectrum of the community and subscribe to a broad definition of health.

Ministry Health Care 5
Rather than focus on one isolated area of need, the needs assessment sought to create a comprehensive needs assessment for the community served using both quantitative and qualitative data. The needs assessment process involved assessment and understanding of demographics, health access, health care usage, health behaviors, health status, and social and environmental factors that ultimately affect health outcomes.
Input was gathered from residents through key informant interviews, focus groups and telephone surveys. Other assessments involved gathering data on the health status of the community through existing county and state surveys and the workings of the local public health system as well as an assessment of forces likely to impact the health of the public in the near future.
The review and evaluation of quantitative data combined with community consultation and feedback have enabled us to identify key priority areas in the community that require attention. The findings of this needs assessment are being used to facilitate strategic planning, decision-making, and resource investments and allocations.
The top seven priority areas of the 2013 needs assessment are: Alcohol consumption (frequency and amount) Asthma prevalence Mental health Newborn health and safety Obesity and diabetes Preventive health services Smoking
Goals and objectives relating to these issues, as well as strategies and asset inventory, comprise the community health improvement project (CHIP) plan. Task forces composed of individuals and groups committed to improving the identified health issues are being organized. Many task force members have been drawn from local CHIP committee organizations engaged in the process to date and other community residents are encouraged to step forward.
The CHIP process is an ambitious and bold effort at community engagement for a common good. No single organization has the depth of resources needed to raise community health to an optimal level or even to maintain it at its current level. CHIP is based on the idea that through collaboration and synergy, two plus two will equal a great deal more than four. Another important feature of CHIP is that the plan arises out of the community, which then has a greater investment in its implementation. In Winnebago County, CHIP merged with the established re:TH!NK coalition, which was already addressing drug and alcohol issues to quickly build additional action teams focused on identified lifestyle issues, such as nutrition, physical activity and access to health care, mental health and dental services, and taking a comprehensive approach to improving community health.
Residents and community groups are encouraged to join the CHIP process. For more information about this report, our action plans and/or how to get involved please contact Vicki Schorse, Mercy Health Foundation at 920.223.0521, or Carolyn Slavik at 920.223.0543.
By collaborating on priority health issues, local residents and community organizations will exhibit their deep commitment to maintaining our community as a healthy place to live and work.

Ministry Health Care 6
__________________________________________________________________________________________ Organizational Commitment
Catholic health care has its origins in a faith-based response to the health needs of those living in poverty and other vulnerable persons. This follows the example of Jesus, who had special affection for the poor and others at the margins of society. In this country, Catholic health care began a mission of responding to community need in 1727, when 12 Catholic sisters arrived in New Orleans to minister to persons who were ill or living in poverty.
The obligation to reach out to those in need and improve community health flows directly from Catholic health care’s identity. Mission-driven organizations provide community benefits because they are committed to: Promote and defend human dignity Care for persons living in poverty and vulnerable populations. Promote the common good. Steward resources
These organizations do not provide community benefits because of external pressures, such as challenges to tax-exempt status. They do it because it is right, because it arises from Catholic identity and because it ensures that they are who they say they are.
The Catholic Health Association
As a not-for-profit Catholic health care ministry, Mercy Medical Center embraces its responsibility to provide for the needs of the communities we serve. While Mercy Medical Center’s benefit program addresses the needs of the overall communities we serve, low income and other disadvantaged individuals and families deserve special attention and priority. Therefore, programs designed to improve access to health care and improve the health and lives of low-income persons and those who are marginalized are our top priority.
Affinity Health System operates as a regional integrated delivery system under a common board of directors and medical staff. The board is responsible for ensuring that community health is one of the major goals in the strategic planning process. The board of directors is a diverse group that includes community members, physicians and business executives who provide a broad spectrum of perspectives on plans presented for their approval. Affinity Health System hospitals’ presidents are committed to the Community Benefit process and accountable both to the vice president, of the eastern region of Ministry Health Care and to the senior vice president of hospital operations.
Community Benefit and Outreach Structure
The Affinity Health System Board of Directors provides oversight of the Affinity Community Benefit Council, who is responsible for the following areas regarding the community benefit activities:
Process
Completion and analysis of a three-year Community Health Needs Assessment. Discussion and analysis of information by Community Benefit sub-committees and Community
partners. Discussion and analysis of data and recommendations by Community Benefit Committee and
selection of priority focus areas. Discussion of Community Benefit Committee selections by the Affinity Executive Team. Final approval of Community Benefit Plan by Affinity Board of Directors. Annual updating of data through monitoring of Community Benefit activities and programs.

Ministry Health Care 7
Budgeting Decisions
Review community benefit budget for the Department of Community Benefit and Outreach with explicit understanding and assumption of their role to ensure that the hospitals fulfill their obligation to benefit the community.
Ensure long-term planning and budgeting to set multi-year goals and objectives. Budget adequate financial resources to hire competent employees to plan, develop, implement
and effectively manage community benefit initiatives.
Program Content Community needs are identified every three years and serve as a basis for developing Community Benefit programs and Healthy Community projects. Additional Community Benefit programs may be implemented, as the need arises. Community Benefit priority areas of focus are selected using the following criteria:
Congruency and relevance to Affinity’s Mission, Promise, Values and Strategic Goals. Alignment with Catholic Health Association (CHA) “A Guide for Planning & Reporting
Community Benefit”. Seriousness of the issue. Number of persons impacted by issue. Systemic and sustainable. Community “burning platform” to address the issue. Organizational “burning platform” to address the issue. Feasibility of addressing the issue (i.e., time commitment, financial resources,
community assets). Identified champion who is willing to lead the area of focus, who when necessary recruits
qualified committee members. Identified Senior Leader to serve as a leadership sponsor. Affinity’s experience with issue (available expertise).
Program Design The selection and design of community benefit activities are based on the following criteria:
Estimated effectiveness/efficiency (i.e. What is the track record to date on this approach? Are there adequate resources to implement this intervention strategy?)
Existing efforts (i.e. Who else is working on this? What is our role? Is it meaningful? How can we best complement/enhance an existing effort?)
Collaborative opportunities with local stakeholders in a community health assessment that establishes priorities, develops a plan to address identified needs, and integrates community health priorities into the strategic planning and annual budgeting process.
Program Targeting The targeting of specific project activities is based on the following criteria:
Target Population(s) (i.e. Will the intervention fit the needs and characteristics of the people we are trying to serve?)
Number of people (i.e. How many people will be helped by this intervention?) Degree of controversy (i.e. Is this intervention acceptable to the community? Will this
intervention offend important constituents?)
Program Continuation or Termination Schedule annual, detailed verbal and written reports of progress towards identified
performance targets by hospital community benefit and outreach leadership. Approve continuation or termination of community benefit and outreach programs after
receiving evaluation findings and other program information from community benefit and outreach employees and the Community Benefit Council.
Ministry Health Care 8
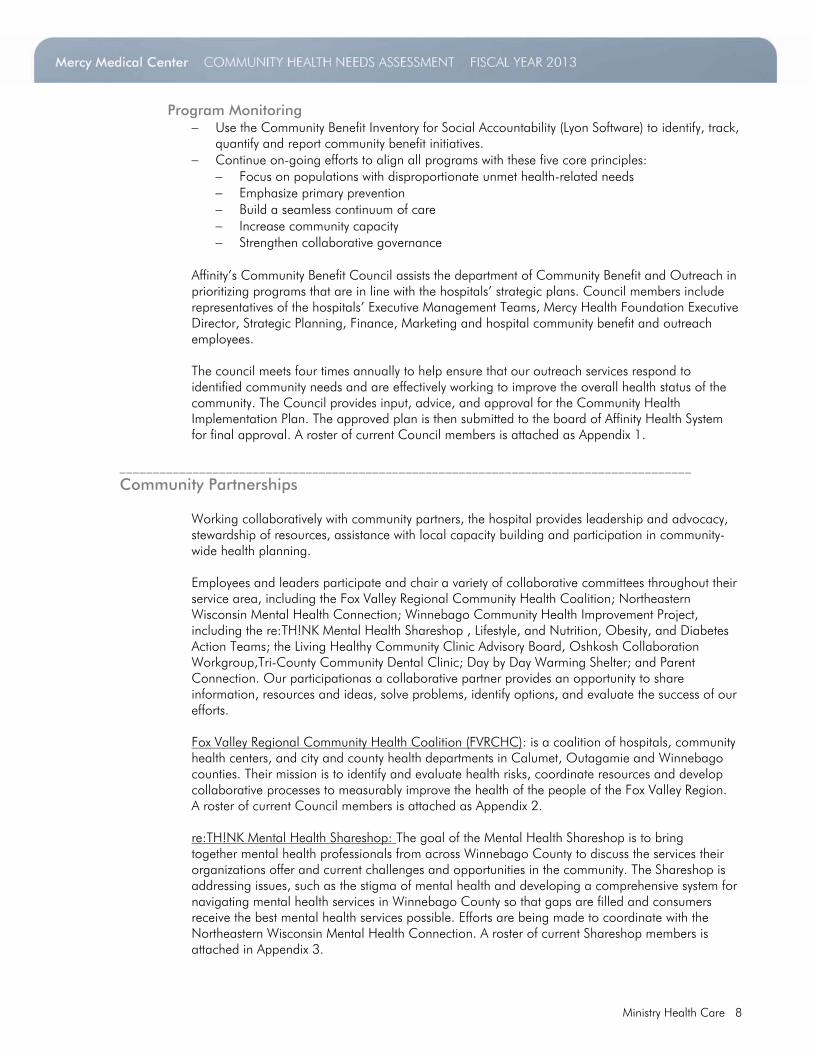
Program Monitoring
Use the Community Benefit Inventory for Social Accountability (Lyon Software) to identify, track, quantify and report community benefit initiatives.
Continue on-going efforts to align all programs with these five core principles: Focus on populations with disproportionate unmet health-related needs Emphasize primary prevention Build a seamless continuum of care Increase community capacity Strengthen collaborative governance
Affinity’s Community Benefit Council assists the department of Community Benefit and Outreach in prioritizing programs that are in line with the hospitals’ strategic plans. Council members include representatives of the hospitals’ Executive Management Teams, Mercy Health Foundation Executive Director, Strategic Planning, Finance, Marketing and hospital community benefit and outreach employees.
The council meets four times annually to help ensure that our outreach services respond to identified community needs and are effectively working to improve the overall health status of the community. The Council provides input, advice, and approval for the Community Health Implementation Plan. The approved plan is then submitted to the board of Affinity Health System for final approval. A roster of current Council members is attached as Appendix 1.
______________________________________________________________________________________ Community Partnerships
Working collaboratively with community partners, the hospital provides leadership and advocacy, stewardship of resources, assistance with local capacity building and participation in community-wide health planning. Employees and leaders participate and chair a variety of collaborative committees throughout their service area, including the Fox Valley Regional Community Health Coalition; Northeastern Wisconsin Mental Health Connection; Winnebago Community Health Improvement Project, including the re:TH!NK Mental Health Shareshop , Lifestyle, and Nutrition, Obesity, and Diabetes Action Teams; the Living Healthy Community Clinic Advisory Board, Oshkosh Collaboration Workgroup,Tri-County Community Dental Clinic; Day by Day Warming Shelter; and Parent Connection. Our participationas a collaborative partner provides an opportunity to share information, resources and ideas, solve problems, identify options, and evaluate the success of our efforts. Fox Valley Regional Community Health Coalition (FVRCHC): is a coalition of hospitals, community health centers, and city and county health departments in Calumet, Outagamie and Winnebago counties. Their mission is to identify and evaluate health risks, coordinate resources and develop collaborative processes to measurably improve the health of the people of the Fox Valley Region. A roster of current Council members is attached as Appendix 2. re:TH!NK Mental Health Shareshop: The goal of the Mental Health Shareshop is to bring together mental health professionals from across Winnebago County to discuss the services their organizations offer and current challenges and opportunities in the community. The Shareshop is addressing issues, such as the stigma of mental health and developing a comprehensive system for navigating mental health services in Winnebago County so that gaps are filled and consumers receive the best mental health services possible. Efforts are being made to coordinate with the Northeastern Wisconsin Mental Health Connection. A roster of current Shareshop members is attached in Appendix 3.

Ministry Health Care 9
S.A.N.E. (Sexual Assault Nurse Examiner): When the need for additional SANE nurses throughout the Fox Cities area was identified, Mercy Medical Center renewed efforts to train more nurses. Sexual assault victims often had to travel to other hospitals causing them additional stress and delaying the collection of evidence. A grant from Mercy Health Foundation made it possible to train five new SANE nurses and coverage is now available 24/7 at Mercy Medical Center and across the region.
Mercy Medical Center Community Health Needs Assessment An assessment conducted jointly by Calumet Medical Center, St. Elizabeth Hospital, Mercy Medical Center, ThedaCare, Aurora Health, Appleton, Neenah and Menasha Health Departments, Calumet, Outagamie and Winnebago County Health Departments. Mercy Medical Center’s community needs assessment was conducted with a wider community coalition. The similarity in population characteristics and cross-utilization of health care services in northeastern Wisconsin counties encourage collaborative efforts. Affinity Health System has three hospitals that serve communities in Calumet, Outagamie and Winnebago counties. These three rural counties are home to 387,391 residents. ______________________________________________________________________________________ Description of Community Served by the Hospital
Source: Community Commons
Winnebago County is located in east-central Wisconsin and covers a total area of 434 square miles. The county seat is Oshkosh. Mercy Medical Center is home to 165,032 Winnebago residents according to the 2010 census.
Mercy Medical Center primary serves Winnebago County and outlying rural communities such as Menasha identified by 80% of inpatient hospital discharges. A map is attached as Appendix 4. Discharges by city over the previous fiscal year were Oshkosh (65%), Omro (6%), Ripon (5%) and Winneconne (4%).

Ministry Health Care 10
According to the Winnebago County Workforce Profile, the population of Winnebago County in 2010 was 166,308, representing an increase of approximately 9,500 residents, or 6.1 percent of its population over the past decade. This growth rate is roughly equivalent to the 6.2 percent growth observed statewide, but lags significantly behind the national growth rate of 9.6 percent. Much of this growth can be attributed to the economic growth of the region, availability of land suitable for residential development, and relatively favorable housing costs.
The city demonstrating the greatest numerical population growth is the City of Oshkosh, the county’s largest municipality. In percentage terms, the Town of Clayton was the county’s fastest growing municipality. The City of Menasha spans two counties — Calumet and Winnebago — and grew by 7.8 percent over the past decade with a current population of 17,605.
Population growth in any area over any period of time can be decomposed into two distinct factors — natural increase, which is simply the balance between births and deaths, and net migration, which is the balance of residents moving into and out of an area over a period of time. Winnebago County’s natural increase and net migration lag behind the nation.
In comparing the educational attainment of Winnebago County’s population to that of the state and nation, we see that the county profiles closely to the state, but that a number of significant differences exist. Beginning at the lowest levels of attainment, we see that both the county and state have a significantly lower share of residents who have failed to complete a high school education. Conversely, Winnebago County has a significantly higher percentage of its population who count high school graduation as their highest level of attainment (35.5 percent as compared to 34.3 percent statewide and 29.3 percent nationally). This disparity has been supported historically through the importance of the manufacturing sector in the local economy, as seen in Appendix 5.
There is a strong correlation between a highly-educated and a highly-mobile population, as suggested. The presence of a large, regional job market and a robust transportation infrastructure allows residents the ability to live in one community and work in another, as indicated in Appendix 6. Much of this commuting activity is restricted to the U.S. Highway 41 corridor.
Prominent employers in Winnebago County are transportation equipment and manufacturing equipment, particularly Oshkosh Corporation and Pierce Manufacturing Inc. Another prominent industry sector that is represented in the tables is the education and health services sector, as represented by the educational services, ambulatory health care services, hospitals and nursing and residential care facilities industry subsectors and among employers including the Oshkosh Public School District, ThedaCare, and the University of Wisconsin — Oshkosh, as seen in Appendix 7. The region’s papermaking heritage is represented in the corporate headquarters of Kimberly Clark Global Sales. This sector has experienced marked decline statewide due to increased efficiency and firm consolidation.

Ministry Health Care 11
The gap between highest and lowest wage-earners was smaller in the northeast Wisconsin area than in the U.S. The median household income (2007-2011) in Winnebago County is $51,596, compared to Wisconsin ($52,347) and U.S. ($52,762).

Ministry Health Care 12
The challenges of poverty are difficult. Although the percentage of Southern Winnebago County residents in poverty has remained fairly stable, indicators show that there are segments of the community who are struggling. The number of homeless children has grown from 26 in 2003-2004 to 197 in 2009-2010, and the percentage of students eligible for free or reduced cost school lunches increased from 32% in 2008-2009 to 39% in 2009-2010. In the Oshkosh School District, 42% are now eligible. Several strong initiatives have begun to support the development of important life skills that will enable individuals to be self-sufficient, but much more support is needed to reach all who need these skills. (2011 Southern Winnebago County L.I. F.E. Study)
The composition of the Fox Cities community has changed. In Winnebago County, for example, the minority population has grown from just over 5% in 2000 to nearly 8% in 2010. In comparison, minorities composed nearly 28% of the U.S. population. (WI Department of Administration and U.S. Census)

Ministry Health Care 13
Source: Community Commons
The figure above displays the racial and ethnic diversity of Winnebago County by symbolizing each block group based on the population's racial/ethnic heterogeneity. The data used in this map are based on combined race and ethnicity data reported from the 2010 US Census. Block group racial diversity was calculated by the Center for Applied Research and Environmental Systems (CARES), and can be defined as the probability that two people chosen at random are of a different race or ethnicity. The most diverse group located in Winnebago County is identified by the beige zones (25.1-45.0), as seen in the above figure. An example of one of these zone compositions is: Source: Community Commons
Source: Mercy Medical Center

Ministry Health Care 14
The community has made progress in the area of diversity, although there is still work to be done. In Southern Winnebago County, New North has an active diversity committee working with area companies, the University of Wisconsin-Oshkosh brings diverse people and ideas to the community, and the Hmong American Society provides support to the Hmong community. While there are local models of positive experiences with diversity, experts agreed that the community as a whole needs to do a better job promoting the involvement of diverse persons and supporting positive attitudes towards diversity of all types. (2011 Southern Winnebago County L.I.F.E. Study)
Source: U.S. Census Bureau, 2008-2010 American Community Survey

Ministry Health Care 15
______________________________________________________________________________________ Who Was Involved in Assessment
Mercy Medical Center participated in the assessment processes that gathered input from both private and public Winnebago, Calumet and Outagamie organization members including: medical staff, nurses and administrators; clinic personnel; public health nurses and educators; behavioral health staff and leaders; health insurance-health management staff, elementary, high school and post high school educators, nurses and administrators; police and emergency personnel; child, women's, family and senior social services; as well as interested community members in the health needs assessment process and service users.
Several Affinity representatives participated as a member of the Fox Valley and Southern Winnebago L.I.F.E. Study and/or Fox Valley Regional Community Health Coalition throughout the assessment process. Leona Whitman, manager of the Living Healthy Community Clinic, was consulted about the medically underserved community health needs. Appendix 8 lists additional individuals who participated in the community needs assessment process.
Winnebago County Public Health Experts
Doug Gieryn, Director/Health Officer, Winnebago County Health Department Twenty years public health experience, the last nine as Director/Health Officer for Winnebago County. Previous experience with the City of Milwaukee specializing in environmental health, communicable disease, tuberculosis and refugee health. Served as president of the Wisconsin Public Health Association in 2010. Provided oversight of the consolidation of three local public health agencies in Winnebago County in a two year process ending in 2012.
Denise Krueger, Public Health Nurse, Winnebago County Health Department Twenty-five years RN experience in Emergency, Home Health and Public Health. Thirteen years as public health nurse with the City of Oshkosh and served as interim health officer for Oshkosh, conducting and overseeing community needs assessments, from 2011 until consolidation with Winnebago County in May 2012.Brought together and served as the chair for what is now the re:TH!NK Nutrition, Diabetes and Obesity (NOD) Committee, currently serving as the public health liaison.
______________________________________________________________________________________ How the Assessment Was Conducted
Identification of Unmet Community Health Needs: Data Collection, Community Health Needs Assessment Findings and Assets Inventory
Mercy Medical Center recognizes that to have a meaningful effect on the populations we hope to help, we must consider how complex social factors such as poverty, education and housing affect people’s health. These factors that lead to poor health are often referred to as the social determinants of health and are documented by a significant body of research, see Appendix 9.
The community health improvement process has five key objectives:
(1) To establish a comprehensive set of indicators related to health processes, health
outcomes and social determinants of health in the communities we serve that incorporate a wide variety of county and sub-county information resources and utilize methods appropriate to their collection, analysis and application.

Ministry Health Care 16
(2) To identify and prioritize health needs in the communities served as a whole and in the
diverse communities served. (3) To assess current strengths within the communities we serve regarding the main health
priorities identified. (4) To foster projects to achieve health equity by addressing health and well-being needs,
improving health outcomes and reducing demographic, geographic and socioeconomic disparities in health and well-being.
(5) To coordinate and leverage resources to support the communities we serve with infrastructure and improvement projects.
Our work begins with an understanding that health cannot be defined simply as the absence of disease. A person’s health is affected by many factors including where the person lives, their income, educational status and other social circumstances Appendix 10.
The focus of Mercy Medical Center’s community health interventions is therefore based on overall determinants of health. We are committed to developing partnerships with community-based organizations who share our goals to improve health, as well as advocating for policies that improve the health of whole populations equitably.
This important work is a fulfillment of our mission, which calls us to advocate for the underserved and partner with others in the community to improve the quality of life. Therefore, the needs assessment is a collaborative effort by Mercy Medical Center, ThedaCare, Aurora Health Care, Winnebago County Health Department and other local partners.
Mercy Medical Center identifies unmet community health care needs in our community in a variety of ways. We used a range of quantitative and qualitative information based on review of health and quality of life data and interviews with community members and representatives of local agencies. We primarily utilized the following to assess community needs and the effectiveness of our response to these challenges: www.communitycommons.org, key informant interviews, http://www.dignityhealth.org/Who_We_Are/Community_Health/STGSS044508, www,countyhealthrankings.org, www.foxcitieslifestudy.org, http://www.lifestudy.info/life-studies-local/southern-winnebago-life-study/southern-winnebago-county-life-study-downloads, hospital and clinic utilization, Winnebago County Behavioral Risk Factor Surveillance System, Youth Risk Behavior Survey (YRBS), County Health Rankings, State of Wisconsin Best Practice Models and other published data from reliable secondary sources. For more details and links to specific reports see Appendix 11.
The choice of data utilized was:
Related to important community condition Useful for action Reliable Recent and historical Local, state, and national Available in future
The selection of priority needs involves collaboration with a variety of internal and external stakeholders. Each year, Mercy Medical Center’s Community Benefit and Outreach staff presented progress reports to the hospital President and Community Benefit Council. During FY11-12, the work concentrated on community benefit and outreach program review and quality.
As an adjunct to the organization’s Strategic Planning Process, community benefit and outreach planning derives input and guidance from the Community Benefit Council, as well as executive, management, and employees of the hospital. As a result, adjustments are made to

Ministry Health Care 17
programs, services and the Community Benefit Plan and Outreach. It is also their responsibility to ensure quality services are provided with each program and those we serve are satisfied with our services.
Other stakeholders involved in the selection of priorities are those organizations with which our hospital provides support to community benefit programs and outreach activities. Some include the Winnebago County Public Health Department, University of Wisconsin-Oshkosh, Oshkosh Area United Way, Community for Hope, Oshkosh Area Community Foundation and Mercy Health Foundation.
Community Need Index (CNI)
Mercy Medical Center utilizes a breakthrough approach to assess our community need and strategically allocate resources, as one means to identify disparities. The Community Need Index (CNI) http://www.dignityhealth.org/Who_We_Are/Community_Health/STGSS044508 assisted the hospital in understanding the public health needs of every zip code they serve, which in turn helps guide the development of community benefit programming.
To determine the severity of barriers to health care access in a given community, the CNI gathers data about that community’s socio-economy. For example, what percentage of the population is elderly and living in poverty; what percentage of the population is uninsured; what percentage of the population is unemployed, etc. Using this data, a score is assigned to each barrier condition (with 1 representing less community need and 5 representing more community need). The scores are then aggregated and averaged for a final CNI score (each barrier receives equal weight in the average). A score of 1.0 indicates a zip code (shown in blue) with the lowest socio-economic barriers, while a score of 5.0 represents a zip code (shown in red) with the most socio-economic barriers.
CNI demonstrates the link between community need, access to care and preventable hospitalization for conditions that, if effectively diagnosed and managed, should be treatable in an outpatient setting. Residents of communities with the highest CNI scores are twice as likely to be hospitalized for manageable conditions — such as asthma, pneumonia, or congestive heart failure — as communities with the lowest CNI scores.
The CNI for Winnebago County (Appendix 12) is used to further validate the identification of communities (by ZIP codes) that are the most socio-economically disadvantaged and thus most in need. Residents of these communities tend to have Disproportionate Unmet Health-Related Needs (DUHN): lack of education, lack of health care insurance, homelessness or transient lifestyles, no or limited access to quality health care, high prevalence of conditions such as diabetes, heart disease, obesity and substance abuse. Below are the CNI scores for a low need community (1.2) and a higher need community (3.4) within Winnebago County.
With this tool, Mercy Medical Center can focus quickly on the areas of most need and devote more time and resources to planning interventions that can assure health issues are addressed in sufficient time and in the most cost-effective settings.

Ministry Health Care 18
______________________________________________________________________________________ Health Priorities Identified
It is clear that the communities served by Mercy Medical Center have many health and quality of life areas that need attention and concerted effort to improve. This 2013 Mercy Medical Center Community Needs Assessment is the beginning effort to address the most pressing needs. These needs will be addressed by the individual hospital, health and human service organizations within the community, as well as the collaborative efforts by the organizations gathered to prioritize the most significant needs summarized in this needs assessment.
While there is no precise definition of vulnerability, St. Elizabeth Hospital’s work focuses on people who don’t have the same kind of opportunities to make healthy decisions as others, and whose opportunities for good health are compromised by insufficient education, inadequate housing, racism or low income. Examples include the homeless, limited income families and children, the uninsured, ethnic minority groups, etc.
Mercy Medical Center, along with local community health improvement teams, reviewed qualitative and quantitative data sets. Each member voted on the top three focus areas. The health issues with the highest number of votes were identified as the key focus areas for the next 3-5 years:
Health priorities were selected using the following criteria:
Congruency and relevance to Affinity’s Mission, Promise, Values and Strategic Goals Addresses/Impact "multi" health issues Addresses the Disproportionate Unmet Health-Related Needs (DUHN) Number of persons impacted by health issue Community “burning platform” to address the issue. Organizational “burning platform” to address the issue. Aligned to Healthy WI 2020 Evidence-based practice (EVB) Likelihood of success Is it measurable?
Definitions Disproportionate Unmet Health-Related Needs (DUHN): seeks to accommodate the needs of communities/neighborhoods with socio-economic barriers that increase resident vulnerability to poorer health/health disparities.
Evidence-based practices (EVB): the practice of health care in which the practitioner systematically finds, appraises, and uses the most current and valid research findings as the basis for clinical decisions.
The 2013 needs assessment provided a listing of the health areas of focus that the Mercy Medical Center would need to address in order to create a healthier community. Of those, seven rose to the top of the list as critical to the immediate health crisis in our community. They include the following:
Alcohol consumption (frequency and amount) Asthma prevalence Mental health Newborn health and safety Obesity and diabetes Preventive health services Smoking
Ministry Health Care 19
Details of the identified health needs can be found in the http://www.foxcitieslifestudy.org/ and Appendix 13.
______________________________________________________________________________________ Community Assets Identified
In addition to identifying community need, the CHNA process also identified community assets and promising practices available in the community that respond to the needs. Also, by virtue of their frequent contact with residents of Winnebago County’s most disadvantaged communities, employees of the Department of Health are familiar with the community assets available to address health and human service issues that affect the residents.
Listed below are some of the promising practices in the community, see Fox Cities LIFE Study: Area Strengths and Southern Winnebago County LIFE Study for more detail.
Alcohol consumption (frequency and amount)
Winnebago County re:TH!NK alcohol prevention & control programming
Mental health Catalpa Health-proposed future satellite location in Oshkosh Winnebago County re:TH!NK Mental Health Shareshop Northeastern Wisconsin Mental Health Connection (NEWMHC)
Obesity and diabetes
Healthy Weight Fox Valley Community gardens and markets Walking and biking trails Eatsmart! N.E.W. program
Preventive Health Services Wisconsin Well Woman Program
Smoking Sustain “Call it Quits” Winnebago County re:TH!NK tobacco prevention and control programming
Others assets include:
Diversified economy, with strength in manufacturing, health care Variety of quality educational opportunities at all levels Growing Community Inclusiveness Libraries YMCA (multiple sites) Law enforcement and emergency response services Faith communities Miles of trails and parks Air quality is good with the exception of radon issues, more than half of homes test over
EPA action limit Drinking water is good for residents with city service but arsenic issues persist in well water Environmental Sustainability efforts by business Safety services seen as strong and collaborative Local civic organizations

Ministry Health Care 20
______________________________________________________________________________________ Data Gap Analysis
Where available, the most current and up-to-date data was used to determine the health needs of the community. Although the data set available is rich with information, not surprisingly, data gaps exist. Data, such as health insurance coverage data, obesity, heart disease and cancer screenings, and
incidence and mortality rates, are not available by zip code, within Winnebago County and/or surrounding communities.
Data is not available on all topics to evaluate health needs within each race/ethnicity by age-gender specific subgroups, especially Asian and Hispanic/Latino populations.
Diabetes prevalence is not available for children, a group that has had an increasing risk for type 2 diabetes in recent years due to increasing overweight/obesity rates.
Health risk behaviors that increase the risk for developing chronic diseases, like diabetes, are difficult to measure accurately in subpopulations, especially Asian and Hispanic/Latino populations, due to BRFSS methodology issues; particularly sample size for subpopulations.
County-wide data that characterize health risk and lifestyle behaviors like nutrition, exercise, and sedentary behaviors are not available for children.
Analysis of linked birth-death records (e.g. Fetal Infant Mortality Review team) would provide detailed information about characteristics and risk factors that contribute to fetal and infant losses in Winnebago County and/or surrounding communities among those populations that could be at elevated risk for poor birth outcomes.
An ongoing source of Pregnancy Risk Assessment Monitoring System (PRAMS) data at the county level at least every three years would improve policy and planning efforts in maternal, fetal and infant health.
______________________________________________________________________________________ Community Benefit and Economic Value Classified Summary of Unsponsored Community Benefit
Mercy Medical Center utilizes the Community Benefit Inventory for Social Accountability (CBISA) computer program created by Lyon Software to track Community Benefit activities. This software enhances our ability to capture data uniformly over a multiyear period and allows data to be updated as needed to develop trending information. The Classified Summary of Unsponsored Community Benefit Expense is included as Appendix 14.
Patient costs are determined by utilizing the HBOC Cost Accounting System.
Success Stories
Tri-County Community Dental Clinic 9 Tri Park Way, Appleton, WI 54915, 920.882.5500 With 13 employees (11 FTE), an annual budget of $1,336,644 and volunteer dentists, the clinic targets low-income, uninsured or underinsured individuals with unmet dental health needs, including migrant farm workers and other disenfranchised populations in Winnebago,
Outagamie and Calumet counties. In addition to the main office in Appleton, it has a mobile clinic that travels to schools to provide preventative and interventional care to elementary students onsite. The center frequently collaborates with more than 20 public, private, and nonprofit organizations. However, a gap remains in access to services for uninsured and Medicaid insured residents. Over 60,000 individuals in the three-county region are estimated to quality for services at the TCCDC; far more than can be served

Ministry Health Care 21
Living Healthy Community Clinic 510 Doctors Court, Oshkosh, WI 54901, 920.424.1242 The Living Healthy Community Clinic (LHCC) is a collaborative public/private program that provides confidential, cost-effective primary medical care to low–income and uninsured residents of Winnebago County. With 3.5 FTEs and an annual budget of $369,444, the LHCC provides over $1.8 million in health care services each year (based on Medicaid rates) including diagnostics, treatment and medication. Mercy Medical Center and other Oshkosh health care providers provide more advanced tests and hospital care when needed. In 2012, 1,052 patients made 4,435 visits to the LHCC. Many have chronic conditions, such as diabetes and cardiovascular disease that require ongoing medication and case management.
Parent Connection 36 Broad St., #150 Oshkosh, WI 54903, 920.223.6630 Parent Connection is a voluntary in-hospital readiness assessment for first-time parents with an offer of skilled home visitation services to medium and high stress families. Families commit to keep the child in program until age 3 (age four or five is ideal). Mercy Medical Center patients represent 95 percent of parents enrolled in the Oshkosh area program. Outcomes include: reduced abuse and neglect rates; improved parenting skills; school readiness; reduced second unplanned pregnancies; improved employability, etc. Outcome measures are already in place. Mercy Medical Center helped to establish the original newParent program in the mid 1990s and provided initial funding. Services are based on proven state and national models. Multiple community organizations collaborate, including Winnebago County and Family Services of Northeastern Wisconsin.
Winnebago County re:TH!NK Mental Health Shareshop Winnebago County Health Department, 112 Otter Street Oshkosh, WI 54903-2808, 920.232.3000 This is an emerging partnership resulting from the Southern Winnebago County CHIP that has drawn strong community interest and commitment. The current priority is on referral management and navigation for individuals and families from the first point of contact. The second focus is developing an anti-stigma campaign. The Winnebago County Health Department and health care and mental health organizations within the county are participating. Efforts are also being made to coordinate regionally.
Fitness for the Physically Challenged 2700 W. 9th Ave., Oshkosh, WI 54904, 920.236.1850 Fitness for the Physically Challenged has been providing free, guided exercise programming to Oshkosh area community members with disabilities for 20 years. The Outpatient Rehabilitation Department at Mercy Medical Center provides the facility without charge 15 hours per week and grants from Mercy Health Foundation fund the salary of the Physical Therapy Assistant (PTA). At any given time, up to 120 individuals participate in the program to help them gain or maintain strength in order to preserve optimum independence in the community.

Ministry Health Care 22
______________________________________________________________________________________ Next Steps
Mercy Medical Center leadership will continue their work with their community health partners to use the information learned from the Needs Assessment process to develop a three-year Community Benefit Implementation Plan for addressing the prioritized community health needs.
Appendix 1 Affinity Community Benefit Council – Membership
Name Organization Title Expertise Area
Carolyn Slavik Affinity Health System Community Benefit and Outreach Coordinator
Nursing & Community Health
Carrie Hankes Ministry Health Care System Director Mission Integration
Nursing & Community Health
Cheryl Schmidt Affinity Health System Vice President Quality and Risk Services
Quality and Risk Management
Jennifer Wagner-Mauk Affinity Health System Vice President Marketing Operations
Public Relations
Jenny Konen Calumet Medical Center Coordinator Marketing & Public Relations
Community Health & Public Relations
Julia Salomon St. Elizabeth Hospital Community Health Improvement Leader
Dietetics, Nutrition Education, Community Nutrition
Kris Smith Affinity Health System Vice President Strategic Financial Planning
Finance
Linda Werner Mercy Medical Center Foundation Assistant Philanthropy, Grant Research and Writing
Liz Janzen St. Elizabeth Hospital Grant And Research Specialist
Philanthropy; Internal and External Grant management and research
Robert Gulig Affinity Health System Manager Reimbursement Finance Tom Veeser St. Elizabeth Hospital Chief Nursing Officer & VP
Patient Care Nursing
Tonya Dedering St. Elizabeth Hospital Executive Director Foundation and Volunteer Services
Philanthropy and Volunteer Services, Gift Shop
Vicki Schorse Mercy Medical Center Executive Director Foundation
Philanthropy; Gift Planning; Community and Project Development

Ministry Health Care 23
Appendix 2
Fox Valley Regional Community Health Coalition - Membership
NAME
ORGANIZATION TITLE EXPERTISE AREA
Becky Hovarter Shawano-Menominee Counties Health Department
Health Director/Officer Public health nursing Community health improvement, processes and plans
Bonnie Kolbe Calumet County Health and Human Services
Health Division Manager/Health Officer
Public health, Home Health and Hospice Nursing
Carrie Hankes Ministry Health Care System Director Mission Integration,
Nursing & Community Health
Christine Breunig Children’s Hospital of WI- Neenah
Operations and Projects Manager
Grants and program management
David Zerbe
Aurora Health Care Administrator Clinic Management
Denise Krueger
Winnebago County Health Department
Public Health Nurse Communicable Disease, Public Health/Nutrition & Diabetes
Douglas Gieryn
Winnebago County Health Department
Director/Health Officer Public Health
Ellen Koski Outagamie County, Department of Health and Human Services, Division of Public Health
Community Health Educator Public health program planning, Implementation & evaluation
Kristene Stacker Fox Cities Community Health Center
Executive Director Uninsured individuals’ health needs and are partners in providing services to this group.
Kurt Eggebrecht Appleton Health Department Health Officer Health Promotion, Disease Prevention and Population Health & Community Intervention
Leona Whitman UW-Oshkosh Living Healthy Community Clinic
Clinic Director Uninsured individuals’ health needs and are partners in providing services to this group
Mark Huber Aurora Health Care VP, Social Responsibility 40 years of experience in community health in the governmental, voluntary and health care sectors. Fellow of the National Public Health Leadership Institute, Past President of WI Public Health Association of Health Education Centers.
Mary Dorn Outagamie County Health and Human Services
Manager, Public Health Division Public Health
Paula Morgan ThedaCare Community Health Manager 25 years experience in community health in governmental and health care sectors
Sue Nett Menasha Health Department Public Health Director Public Health/Promotion of Community Health/Prevention of Chronic Disease

Ministry Health Care 24
Appendix 3 re:TH!NK Mental Health Shareshop - Membership
First Name
Last Name Organization/Agency Expertise
Linda Baeten Winnebago County Health Department Community Health
Amy Bertschausen Samaritan Counseling Center Mental Health
Lyn Beyer Reach Counseling Services, Inc. Mental Health
Kristen Biese Wisconsin Well Woman Program Community Health
Doug Bisbee Community for Hope of Greater Oshkosh Mental Health
Doug Brey Winnebago County Department of Human Services Community Health
Larry Cavanaugh Winnebago Mental Health Institute Mental Health
Kate Croskery-Jones A Home Within Foster Care
Stacey Davis Oshkosh Area School District Education
Jean Dekeyser ThedaCare Health Care
Marc Dosogne Boys & Girls Club of Oshkosh Youth Services
Diana Drew National Alliance on Mental Illness Mental Health
Faith Edwards UW Oshkosh Nursing Program Education
Julie Fevola UW Oshkosh Nursing Program Education
Lori Fields Boys & Girls Club of Oshkosh Youth Services
Cheryl Fowler Oshkosh Area Community Foundation Philanthropy
Joe Framke Oshkosh Police Department Law Enforcement
Irene Hans Franciscan Courts Aging Services
Mary Harp-Jirschele JJ Keller Foundation Philanthropy
Steve Herman Oshkosh City Council Government
Erin Hollister Northeast Regional Center Educator & Advocate for Children & Families
Sara Kaiser Winneconne School District Education
Don Karl Salvation Army Social Services
Heidi Keating re:TH!NK Community Health
Jeanine Knapp Lutheran Social Services of WI & Upper MI Mental Health
Cheryl Laabs Winnebago County Health Department
Community Health
Deb Lee Christine Ann Domestic Abuse Services, Inc. Domestic Abuse
Mary Lee Retired, Omro School District Education
Deborah Lee Christine Ann Domestic Abuse Services, Inc.
Domestic Abuse
Donna Lohry Winnebago County Supervisor Government

Ministry Health Care 25
Amanda Matthews NEW Mental Health Connection Mental Health
Angie McCarthy Day by Day Warming Shelter Social Services
Joy Mead-Meucci Aurora (Behavioral Health Services) Mental Health
Mike Norton Winnebago County Human Services Social Services
Sue Panek Oshkosh United Way Philanthropy
Teresa Paulus Winnebago County Health Department Community Health
Renee Raether Aurora (Behavioral Health Center) Mental Health
Tracey Ratzburg Northeast Regional Center Community Health
Erin Reismann Housing Authority Social Services
Susan Richards United Way Fox Cities Philanthropy
Brenna Root Winnebago County Health Department Community Health
Lynn Ryerson Oshkosh Area School District Education
Vicki Schorse Affinity Health System (Mercy Health Foundation)
Philanthropy & Community Health
Linda Schmidt-Goss Winnebago County Jail Law Enforcement
Wendy Schwalbe Family Services NEW Children's Services
Thomas Scofield UW Oshkosh College of Education & Human Services Education
Lindsay Sommerfeldt Affinity Health (Medical Group) Mental Health
Mark Stockli Oshkosh Family Mental Health
Paulette Stoltzmann Winnebago County Health Department Community Health
Mary Jo Turner Winnebago County Health Department Community Health
Lara Vendola-Messer Winnebago County Sheriff's Department Law Enforcement
Steve Vickman Oshkosh Area Community Pantry Social Services
Mark Weisensel Aging & Disability Resource Center of Winnebago County Aging Services
Becky Welhouse Lutheran Social Services of WI & Upper MI Mental Health
Leona Whitman UW Oshkosh Healthy Living Community Clinic Community Health
Rachel Williams Omro School District Education

Ministry Health Care 26
Appendix 4 Mercy Medical Center Primary Service Area Based on 80% Inpatient Discharges

Ministry Health Care 27
Appendix 5 Educational Attainment
Network Health Plan Community Health Advisory Team Age Distribution by Industry

Ministry Health Care 28
Appendix 6 Wage Distribution
Source: Winnebago County Workforce Profile Employment

Ministry Health Care 29
Appendix 7

Ministry Health Care 30
Appendix 8
Winnebago County Community Health Improvement Planning Membership
First name Last
name Organization Expertise
Kari Arkins YMCA Fitness and Prevention
Ken Arneson Evergreen Retirement Community Aging Services
Linda Baeten Winnebago County Health Dept Community Health
Sister Pam Biehl St. Mary's Winneconne Faith Community
John Casper Oshkosh Chamber of Commerce Economic Development
Jill Collier Winnebago Board of Health (Also UW-O) Community Health
Tom Davies Land and Water Conservation Environment
Emily Dieringer Winnebago County Health Dept Community Health
Marc Dosogne Boys and Girls Club Youth Services
Cindy Draws Winnebago County Health Dept Community Health
Julie Fevola Christine Ann Center Domestic Abuse
Doug Gieryn Winnebago County Health Dept Community Health
Bob Glass Tri-County Community Dental Clinic Dental Health
Rose Goyke Peace Lutheran (Parish Nurse) Community Health
Jennifer Greeninger Oshkosh City Government
Mark Harris County Executive Government
Steve Herman Winnebago County Sheriff Law Enforcement
Mike Hert Aurora Health Care
Stan Kline Oshkosh Board of Health Community Health
Christine Kneip UW Extension Education
Melissa Kohn Fox Valley Technical College Education
Melissa Kraemer Badtke East Central Regional Planning Community Development
Cheryl Laabs Winnebago County Health Dept Community Health
Melanie Leet Land and Water Conservation Environment
Nancy Leipzig Southwest Rotary Civic Organizations
Danica Lewis/Robt Geigle Oshkosh Area School District Education
Paula McNiel UW-Oshkosh Education
Dave Morton Morton Pharmacy Health Care
Tracy Mrochek Oshkosh Health Services Division Community Health
Catherine Neiswender UW Extension Education
Mary Olson Oshkosh Area Community Pantry Social Services
Susan Phillips Town of Menasha FD Safety
Jeff Phillips Winnebago County Health Dept Community Health
Mark Rohloff Oshkosh City Manager Government

Ministry Health Care 31
Tom Saari Winnebago County Human Services Mental Health
Vicki Schorse Mercy Health Foundation/MMC
Philanthropy and Community Health Planning
Paul Spiegel Oshkosh Health Services Division Community Health
Ken Stoffel Winnebago County Human Services Mental Health
Deb Tauer ADVOCAP Social Services
Jayne Tebon Oshkosh Health Services Division Community Health
Mary Jo Turner Winnebago County Health Dept Community Health
Dave Wellhofer Omro School District Education
Leona Whitman Living Healthy Community Clinic Community Health
Kelly Zdanovec Davis Child Care Center Child Care
Mark Ziemer Oshkosh Director of Senior Services Aging Services
Ministry Health Care 32
Appendix 9

Ministry Health Care 33
Appendix 10 Our Approach
Mercy Medical Center measures community health based on the County Health Rankings Model, “a model of
population health that emphasizes the many factors that, if improved, can help make communities healthier
places to live, learn, work and play”.

Ministry Health Care 34
Appendix 11
List of Sources
The following sources, woven together within each section, comprise the data: Community Commons http://www.communitycommons.org/ CHNA.org is a free web-based platform designed to assist hospitals (with particular attention to critical access and other smaller facilities), non-profit organizations, state and local health departments, financial institutions, and other organizations seeking to better understand the needs and assets of their communities, and to collaborate to make measurable improvements in community health and well-being. Community Focus Groups with vulnerable population subgroups of our community to gauge their perceptions of quality of life. These groups were held due to the fact that they may be under-represented in surveys, and in the case of older adults, are an important community segment with growing needs. 2011 Southern Winnebago County L.I.F.E. Study http://www.lifestudy.info/life-stories-local/southern-winnebago-life-study/southern-winnebago-county-life-study-online Information is gathered from surveys of community and leaders, a health risk behavior survey, focus groups, interviews with experts, secondary data compilation, agency and provider data, and the Youth Risk Behavior survey. Community Need Index (CNI) http://www.dignityhealth.org/Who_We_Are/Community_Health/STGSS044508 CNI is an online mapping tool which pinpoints the level of community need for every zip code in the United States. County Health Rankings http://www.countyhealthrankings.org/#app/ Nearly every county in the country is ranked on health outcomes (how healthy we are) and on health factors (how healthy we can be). In 2012, Outagamie County ranked 16th in the state for our health outcomes and 13th in the state for our health factors (out of 72 counties). Fox Cities L.I.F.E. Study http://www.foxcitieslifestudy.org/ The Fox Cities L.I.F.E. Study included three surveys, community focus groups, interviews with experts and a look at statistical data published by the state and others (Appendix 5). We considered all data sources together to look for convergence on important issues. Hospital and clinic utilization, including emergency department services, were reviewed. Appropriate inclusion of key elements of this hospital utilization data was then shared during related discussions by members of St. Elizabeth Hospital Advisory team and Affinity Community Health Improvement partners regarding community health needs. Key Informant Interviews with leaders within a specific vulnerable population to obtain information of challenges and strengths in the area related to their fields of expertise.

Ministry Health Care 35
Published Data from reliable secondary sources such as the state, U.S. Census, counties, Centers for Disease Control, Annie E. Casey Foundation and other reputable and objective sources.
U.S. Census dataset: 2005-2007 and 2007-2009 three year estimates from the American Community Surveys (ACS) were used because of the greater accuracy they provided. One year ACS estimates have much larger margins of error and are not available for areas with smaller populations (i.e., Calumet County). Data from the 2010
U.S. Census are only partially released as of this printing. When we could, we have incorporated actual 2010 Census data. Both sources have high credibility.
Whenever possible, we have used rates rather than actual number of cases or reports to adjust for changes in the size of the population over time.
Occasionally, a source we are using has changed its data reporting methods. Our report notes when these changes have occurred between years of data. When comparing two data points from different counties or time periods, it is important to keep in mind the fact that the difference may be due to sampling and may not be statistically significant. However, large differences, although not statistically significant, are still important to investigate.
United States Census Bureau http://www.census.gov/ One source for current population data and the latest Economic Indicators. Youth Risk Behavior Survey (YRBS) http://www.co.winnebago.wi.us/health/units/administration/community-health-data/youth-risk-behavior-survey-yrbs Administered by the Winnebago County Health Department in even-numbered years to all middle and high school students in the five school districts in Winnebago County. Winnebago County Behavioral Risk Factor Surveillance System http://www.co.winnebago.wi.us/health/units/administration/community-health-data/behavioral-risk-factor-surveillance-system-2011-br Included 400 telephone interviews, random selection of persons 18 years old and older – data weighted by age to align 2010 census results for comparison and low margin of error, 95% confidence obtained in survey. Winnebago County Workforce Profile http://worknet.wisconsin.gov/worknet_info/downloads/CP/winnebago_profile.pdf To assist with identifying priorities, comparisons are made to other Wisconsin counties, as well as to national benchmarks such as Healthy People 2020, which is a set of key national health objectives.

Ministry Health Care 36
Appendix 12 Winnebago County Community Need Index CNI provides a focus for Mercy Medical Center to increase the health and quality of life of residents in Winnebago County and outlying rural communities served.

Ministry Health Care 37
Appendix 13 Summary of Identified Health needs
2011 Fox Cities L.I.F.E Study (Calumet, Outagamie and Winnebago counties)
Identified Health Needs
2011 L.I.F.E. Southern Winnebago County Identified Health Needs
1. Low birth weights 1. Obesity & lifestyle habits 2. Teen birth rate up 2. Binge drinking & tobacco use 3. Suicide rate up 3. Access to medical & dental care (adult & children) 4. Adult tobacco, drug & alcohol use up 4. Health outcomes rank declined 5. Adult obesity rate & diabetes up 5. Abuse of prescription drugs 6. Youth tobacco, drug & alcohol use up 6. Diabetes up 7. Access to health care, esp. mental health care 7. Community needs to do a better job with diversity relating to
income & racial/ethnic issues 8. Access to dental care 8. Growing water loss & inability to handle water runoff during
severe storms 9. High cost of child care 9. Need broader access to preventive & primary care services 10. Increased gaps in care management for people with disabilities of all ages
10. Low awareness of “healthy lifestyles”
11. Youth – fear for safety at schools/bullying 11. Increase in infant mortality rate 12. Increase in low income students 12. Increase in low birth weight babies (single mothers & low
income mothers) 13. Decreased water quality 13. Increase in suicide rate 14. Increased child abuse & neglect/bullying 14. Increase in mental illness 15. Increased teen dating violence 15. Increase in asthma 16. Increased elder abuse 16. Increased tobacco use and exposure 17. Increase in violent crime esp. drug-related 17. Increased abuse of alcohol 18. Increased drug abuse & gang activities 18. High cost of child care 19. Increased homelessness r/t unemployment (more children)
19. Inadequate transportation
20. Increased FoodShare recipients 20. Increased percentage of older adults living at home alone in poverty
21. Increased food insecurity & hunger 21. Older adults have housing concerns as well as transportation & technology concerns (feel isolated)
22. Transportation challenges 22. Increase in homelessness, including children 23. Availability of jobs with health care benefits 23. Increase in violence at school/bullying 24. Increase in gang activity & use of drugs 25. Decrease in area’s ability to address emerging environmental
problems (ozone as a major pollutant) 26. Lake & river quality/poor clarity 27. Poor walkability in certain parts of the area 28. Increase in reported cases of child abuse & neglect 29. Increase in total youth arrests including drug arrests 30. Increase in elder abuse & neglect 31. Increase in sexual assaults/domestic abuse/violent
crime/property crime rates 32. Increase in abuse of marijuana, oxycontin, & pharmaceutical
drugs 33. Decrease in affordable housing 34. Increase in FoodShare recipients 35. Increase in transportation, utilities & health care costs

Ministry Health Care 38
Appendix 14
Mercy Medical Center Fiscal Year 2012 Community Benefit Report
Community Health Improvement Services …………………………………………………..… $264,453 Activities carried out by Affinity Health System for the express purpose of improving community health. They extend beyond patient care activities and are subsidized by Affinity. Included in this category are the unreimbursed costs associated with community education and outreach, screenings conducted in the community, support groups, counseling services, self-help and wellness programs, immunizations, and support for community clinics. Health Professions Education ……………………………………………………………………...$501,152 Clinical training of interns and residents, nurses, technicians and other health professionals. Included in this category are scholarships provided by Affinity and the unreimbursed cost associated with opening clinical training programs. Subsidized Health Services ……………………………………………………………………….. $123,980 Provides for non-governmental program recipients with incomplete or no financial reimbursement. Included are services such as emergency services, neonatal intensive care, obstetrics and newborn care, and behavioral health services. Cash and In-kind Contributions ………………………………………………………………….. $363,295 Funds and in-kind donations to the community at large. Included are cash contributions to nonprofit organizations, sponsorships of health-related activities, food donations, contributions of supplies and equipment, and provision of meeting room space to community groups. Charity Care ………………………………………………………………………………………… $1,083,588 Free or discounted health-related services provided to people who cannot afford to pay, including uninsured and other low-income patients. Unreimbursed Cost of Government-Sponsored Programs …………………………………… $3,679,103 Shortfall experienced when payments received are below the cost of treating public beneficiaries through Medicaid and other local public programs. Community Building/Benefit Activities and Operations ……………………………………… $62,095 Activities such as physical improvements and housing, economic development, coalition building, community health improvement advocacy, workforce development, community health needs, and health assessments. Total Community Benefits ………………………………………………………………………… $6,077,664 *We are not including the gap in Medicare reimbursement, which totaled $6,616,053. This is in accordance with the Catholic Health Association Community Benefit Reporting Guidelines. Including the Medicare shortfall, our total would be $12,693,717.

Ministry Health Care 39
Appendix 15 Behavioral Risk Factors Surveillance Study Highlights The following data was provided by the Fox Cities L.I.F.E. Study.

Ministry Health Care 40
Appendix 16
Winnebago County Health Rankings
* 90th percentile, i.e., only 10% are better Note: Blank values reflect unreliable or missing data
2012
WinnebagoCounty
Error Margin
NationalBenchmark*
Iowa Trend Rank
(of 99)
Health Outcomes 76Mortality 87
Premature death 7,322 5,153-9,490 5,466 6,012
Morbidity 50 Poor or fair health 10% 5-17% 10% 12% Poor physical health days 1.7 1.0-2.4 2.6 2.8 Poor mental health days 1.8 0.8-2.8 2.3 2.7 Low birth weight 8.1% 6.3-10.0% 6.0% 6.8% Health Factors 19Health Behaviors 10 Adult smoking 14% 9-22% 14% 19% Adult obesity 26% 20-32% 25% 29% Physical inactivity 24% 19-31% 21% 25% Excessive drinking 20% 13-29% 8% 20% Motor vehicle crash death rate 30 18-43 12 15 Sexually-transmitted infections 184 84 313 Teen birth rate 24 18-29 22 33 Clinical Care 13 Uninsured 9% 8-10% 11% 10% Primary care physicians 2,672:1 631:1 1,492:1 Preventable hospital stays 54 44-63 49 63 Diabetic screening 88% 75-100% 89% 88% Mammography screening 79% 65-93% 74% 71% Social & Economic Factors 52 High school graduation 88% 89% Some college 67% 58-76% 68% 67% Unemployment 7.1% 5.4% 6.1% Children in poverty 16% 11-20% 13% 16% Inadequate social support 12% 7-19% 14% 16% Children in single-parent households 21% 13-29% 20% 27% Violent crime rate 73 291 Physical Environment 30
Air pollution-particulate matter days 0 0 1
Air pollution-ozone days 0 0 0 Access to recreational facilities 9 16 11 Limited access to healthy foods 6% 0% 6% Fast food restaurants 31% 25% 44%
Ministry Health Care 41
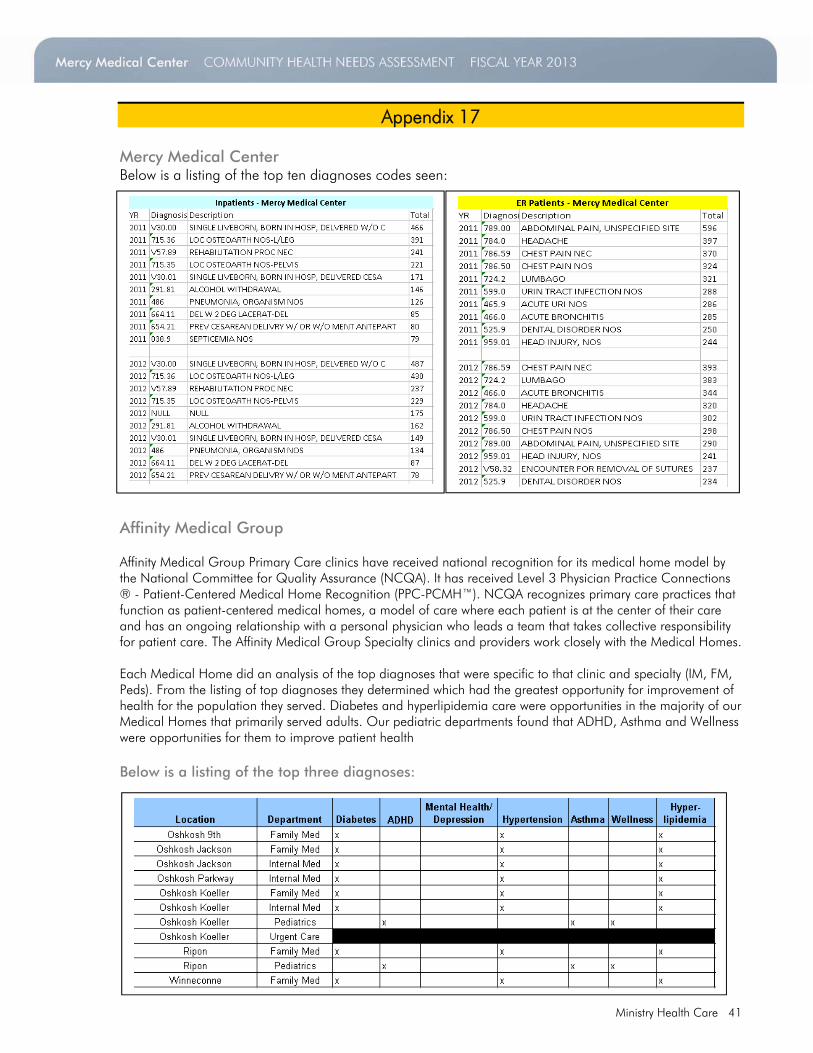
Appendix 17 Mercy Medical Center Below is a listing of the top ten diagnoses codes seen:
Affinity Medical Group Affinity Medical Group Affinity Medical Group Primary Care clinics have received national recognition for its medical home model by the National Committee for Quality Assurance (NCQA). It has received Level 3 Physician Practice Connections ® - Patient-Centered Medical Home Recognition (PPC-PCMH™). NCQA recognizes primary care practices that function as patient-centered medical homes, a model of care where each patient is at the center of their care and has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The Affinity Medical Group Specialty clinics and providers work closely with the Medical Homes. Each Medical Home did an analysis of the top diagnoses that were specific to that clinic and specialty (IM, FM, Peds). From the listing of top diagnoses they determined which had the greatest opportunity for improvement of health for the population they served. Diabetes and hyperlipidemia care were opportunities in the majority of our Medical Homes that primarily served adults. Our pediatric departments found that ADHD, Asthma and Wellness were opportunities for them to improve patient health Below is a listing of the top three diagnoses: