Embed Size (px)
DESCRIPTION
mid presentation
Citation preview

MINIMAL INTERVENTION DENTISTRY

“Life and health are God’s precious gifts to be treasured, nurtured and protected”.

Macro-dentistry‘Extension for prevention’
Micro dentistry‘Prevention of extension’





Terminology"minimal"
• very small in amount or extent; • smallest possible in amount or least possible in
extent; "intervention"
• an action undertaken in order to change what is happening or might happen in another’s affairs,especially in order to prevent something undesirable.
Minimal intervention (MI) in dentistryMount GJ.
Minim Interv Dent 2011; 4 (6)

DEFINITION
“philosophy of professional care concerned with the first occurrence, earliest detection, and earliest possible cure of disease on micro (molecular) levels, followed by minimally-invasive and patient-friendly treatment to repair irreversible damage caused by such disease”
Tyas MJ, Anusavice KJ, Frencken JE, Mount GJ. Minimal intervention dentistry --a review.
Int Dent J 2000 Feb; 50(1): 1-12.




Paradigm Shift
Dental caries as an infectious disease model involves focusing on treatment of the entire disease process not just surgically treating
cavities.

• ‘Drilling and filling’ a tooth is not the only solution to the damage caused by the caries process and is not an effective method to treat the Cariogenic infection.
• A comprehensive preventive and treatment program is necessary to manage dental caries.
• Minimal intervention is modern approach for management of caries
Minimally invasive dentistryCAROL ANNE MURDOCH-KINCH
JADA, Vol. 134, January 2003

CORE PRINCIPLES OF MID
Recognitionidentify and assess any potential
caries risk factors
eliminate or minimize caries risk factors, through altering DIET & increase pH of oral enviorment
To arrest and reverse incipient lesions, regenerating enamel subsurface lesions
Bioactive materials are used to restore the tooth and promote internal healing of the dentine
. Minimum intervention dentistry principles
and objectives.Walsh LJ, Brostek AM.
Aust.dent.jrnl 2013 Jun;58 Suppl 1:3-16

Patient Centred Management Cycle On Which MITP Is Based
MITP-PRACTICAL IMPLEMENTATION IN GENERAL PRACTICEMinim Interv Dent 2011; 4 (6)

IDENTIFY
MITP-PRACTICAL IMPLEMENTATION IN GENERAL PRACTICEMinim Interv Dent 2011; 4 (6)

PREVENT
MITP-PRACTICAL IMPLEMENTATION IN GENERAL PRACTICEMinim Interv Dent 2011; 4 (6)

RESTORE
MITP-PRACTICAL IMPLEMENTATION IN GENERAL PRACTICEMinim Interv Dent 2011; 4 (6)

A SYSTEM FOR TOTAL ENVIRONMENTAL MANAGEMENT
(STEM) OF THE ORAL CAVITY

Aspects Of The Oral Environment
A SYSTEM FOR TOTAL ENVIRONMENTAL MANAGEMENT(STEM) OF THE ORAL CAVITY, AND ITS APPLICATION TODENTAL CARIES CONTROL Laurence J Walsh
INTERNATIONAL DENTISTRY SA VOL. 10, NO. 1

Simplified scheme of how medical and lifestyle factors caninfluence resting salivary parameters.
A SYSTEM FOR TOTAL ENVIRONMENTAL MANAGEMENT(STEM) OF THE ORAL CAVITY, AND ITS APPLICATION TO DENTAL CARIES CONTROL Laurence J Walsh
INTERNATIONAL DENTISTRY SA VOL. 10, NO. 1

A SYSTEM FOR TOTAL ENVIRONMENTAL MANAGEMENT(STEM) OF THE ORAL CAVITY, AND ITS APPLICATION TODENTAL CARIES CONTROL Laurence J Walsh
INTERNATIONAL DENTISTRY SA VOL. 10, NO. 1

CONCEPTS OF MID
The focus is on maximum conservation of demineralized, noncavitated enamel and
dentin.

‘Golden triangle’ of MID
The histology of the dental substrate being treated
The chemistry/handling of the adhesive materials used
to restore the cavity
Consideration of the practical operative techniques available
to excavate caries minimally
Minimal intervention dentistry: part 7. Minimally invasive operative caries management: rationale and techniques
A. Banerjee

1) Early Caries Diagnosis2) The Assessment Of Individual Caries Risk
(high, moderate, low)3) The Classification Of Caries Depth And
Progression Using Radiographs4) The Reduction Of Cariogenic Bacteria To
Decrease The Risk Of Further Demineralization And Cavitation
5) The Arresting Of Active Lesion

6) The Remineralization And Monitoring Of Non Cavitated Arrested Lesions
7) The Placement Of Restorations In Teeth With Cavitated Lesions using Minimal Cavity Designs.
8) The Repair Rather Then The Replacement Of Defective Restorations
9) Assessing Disease Management Outcomes At Pre-established Levels.

EARLY DIAGNOSIS OF DENTAL CARIES

• G.V.Black – “ a sharp explorer should be used with some pressure & if a very slight pull is required to remove it i.e. ‘CATCH POINT’, the pit should be marked for restoration even if there are no signs of decay” .
CLINICAL EXAMINATION

• BASCD & WHO: “ if in the opinion of the examiner after visual
inspection a doubt exists, the surface should be investigated with a blunt probe & unless the point enters the lesion ,the surface will be regarded as sound. The blunt probe should have a tip of 0.5 mm”

Clinicians are forced to measure a dynamic process as a dichotomous variable of presence or absence of disease, using
i. Clinical criteria (e.g. color, softness or resistance to removal)
ii. Tools (Sharp explorer)

Healthy occlusal fissure
“ SHARP EYES BUT BLUNT PROBE”
The enamel is damaged by forceful probing with sharp sickle probes, so probes used to examine occlusal surfaces should beblunt and the probing forces light
Unaided caries diagnosisLess then 50% of caries incidences are correctly diagnosed!- occlusal caries = 41% diagnosed- approximal caries = 21% diagnosed
Caries diagnostic with magnification- occlusal caries = 53% diagnosed- approximal caries = 31% diagnosed

Disadvantages
• Still not all carious lesions are identified • Additional aids (Bitewing etc) needed • Costs • poor fit and adjustment - eye strain

• No longer consider to be an appropriate means of diagnosing occlusal caries because of the
i. possibility of extending the lesion or ii. inoculation of additional sites with cariogenic
microbes
Radiographic Assessment
• Minimal depth-500 micro meters• 2D image• Faulty angulation• Ionizing radiation

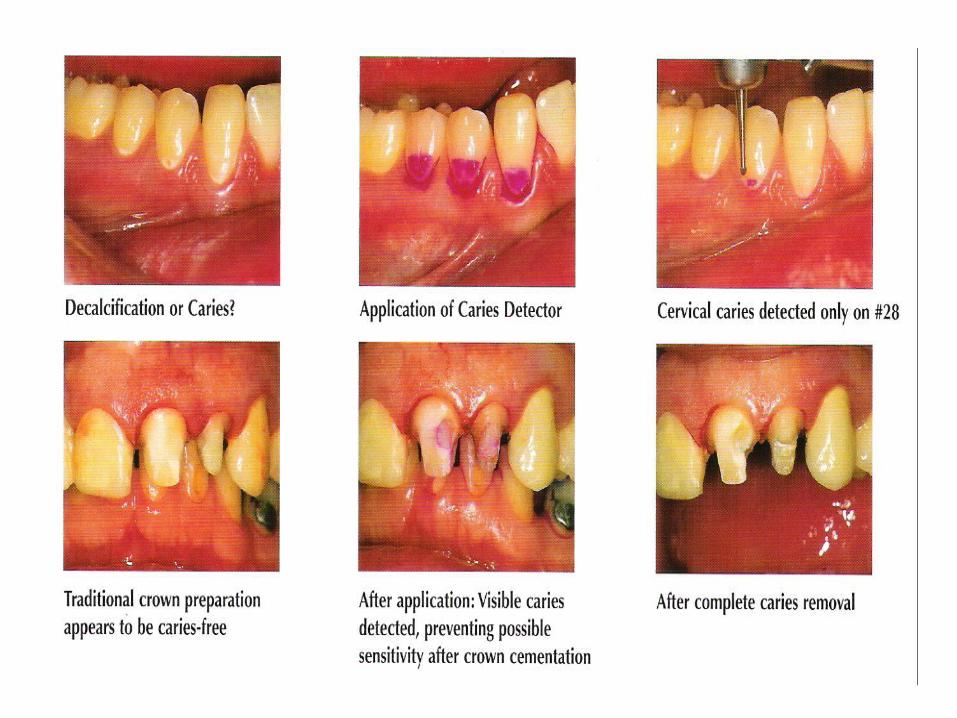
Caries Detecting Dyes

• Dyes for detection of enamel caries: Procion dye Calcein dye Fluorescent dye Brilliant blue• Dyes for detection of dentinal caries: Basic fuchsin Acid red Carbolan green Comassie blue Lissamin blue

DISADANTAGES:
Does not stain bacteria Risk of over treatment few are carcinogenic some may cause irreversible staining

Recent diagnostic methods
• Electrical Conductance Measurement (ECM)• Quantitative Light Induced Fluorescence (QLF)• Dye Enhanced Laser Fluorescence (DELF)• Diagnodent • Fibre optic Trans Illumination (FOTI)• Direct Magnification (DIMA)• Digital Subtraction Radiography• Optical Coherence Tomography (OCT)• Tuned Aperture Computed Tomography (TACT)• Electrical Impedence Tomography (EIT)• Digital Radiology (DR)
DIFOTI

Electronic Caries Monitor

DIAGNOdent
Diagnodent - dental caries laser detector - Minh Nguyen, D.D.S. - YouTube.flv
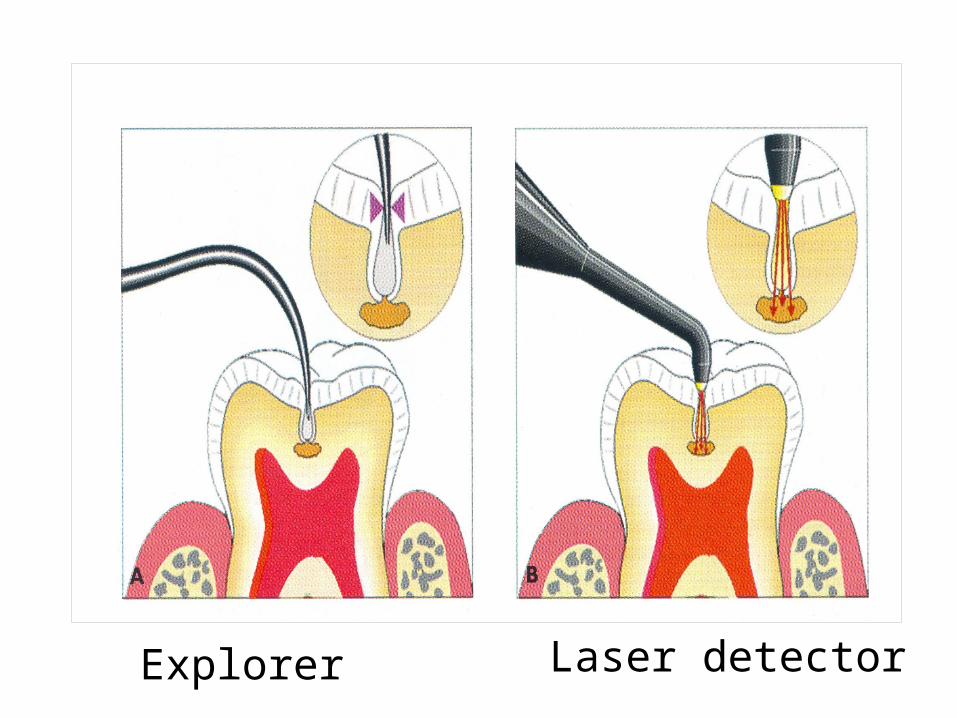
Laser detectorExplorer

ULTRASONOGRAPHY

ENDOSCOPE• Fluorescence• Blue light
• White light endoscopy• Small carious lesion• Camera + endoscope = VIDEOSCOPE

CARIES RISK ASSESSMENT
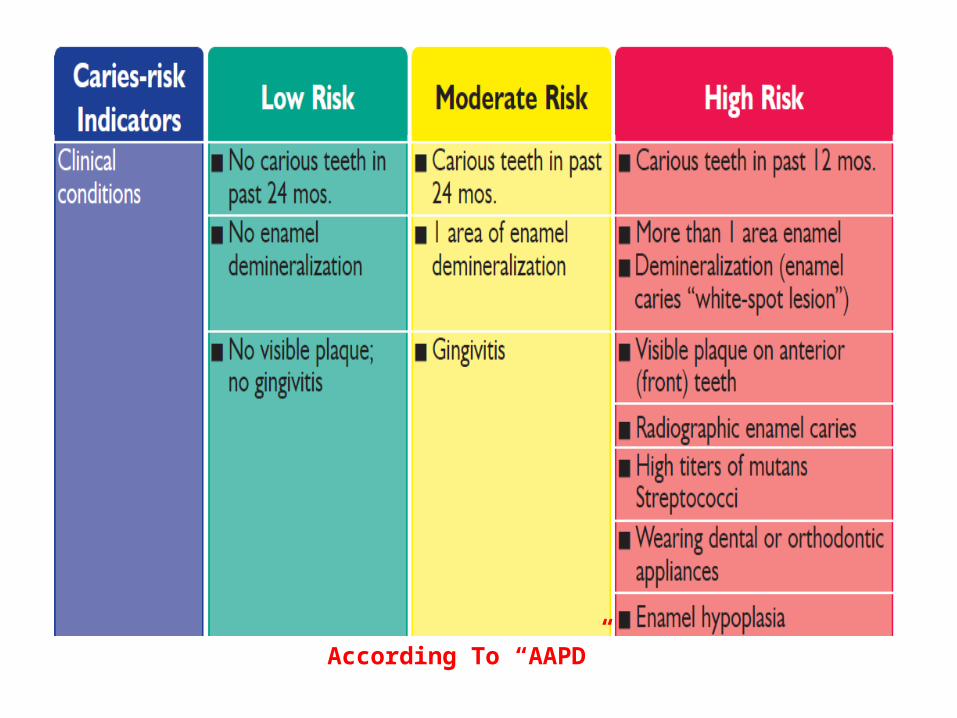
According To “AAPD”



The Caries Balance
Pathological Factors Acid-producing bacteria• Sub-normal saliva flow and/or function Frequent eating/drinking of fermentable carbohydrate
Protective Factors Saliva flow and components Fluoride: remineralizationAntibacterials: - chlorhexidine, iodine?, xylitol, new?Ph controling rinses
Caries No Caries
Featherstone JD 2000

Cariogram is a new way in which to illustrate the interaction between caries related factors
CARIOGRAM - THE FIVE SECTORS

AIMS • Illustrates the interaction of caries related factors. • Illustrates the chance to avoid caries. • Expresses caries risk graphically. • Recommends targeted preventive actions. • Can be used in the clinic. • Can be used as an educational programme.

CARIES MANAGEMENT BY RISK ASSESSMENT (CAMBRA)

2002 FDI BASIC CAMBRA PRINCIPLES• Modification of the oral flora to favor health.• Patient education and informed participation.• Remineralization of non-cavitated lesions of
enamel and dentin/cementum• Minimal operative intervention of cavitated
lesions and defective restorations.• Repair of defective restorations

1. Modification of the oral flora
Dental caries is an infectious disease, and the primary focus should therefore be on-
i. control of the infection,ii. plaque control and iii. reduced carbohydrate intake.

2. Patient education
The etiology of dental caries should be explained to the patient, together with the means of prevention through dietary and oral hygiene measures.

3. Remineralization of non-cavitated lesions of enamel and dentine
• Saliva plays a critical role in the demineralization/remineralization cycle, and its quantity and quality should therefore be assessed.
• There is strong evidence that ‘white spot’ lesions of enamel and non-cavitated lesions of dentine can be arrested or reversed.
• Such lesions should therefore be managed initially by remineralization techniques.
• The extent of the lesion should be objectively recorded such that any progression can be identified at recall.

4. Minimal operative intervention of cavitated lesions
Operative intervention should focus on the preservation of natural tooth structure and be limited to the removal of friable enamel and infected dentine.
This can be done with hand, rotary, sonic, ultrasonic, air abrasive or laser instruments, depending on the circumstances.
Preparation of minimal cavities enables their restoration with adhesive materials such as glass-ionomer cement and/or resin composite.
5. Repair of defective restorations
Removal of restorations results in an inevitable increase in cavity size as a consequence of removal of sound tooth structure.
Depending on the clinical judgment of the dentist, repair could be considered as an alternative to replacement in some circumstances.

• LANIMA-lesions for which appropriate non-invasive management is advised.
• LOCA-lesions for which operative care is advised

• Five treatment categories for the protocol:1. Caries-Balanced Low-Risk2. Caries-Balanced Moderate-Risk3. Caries-Active Moderate-Risk4. Caries-Active High-Risk5. Caries-Active Extreme-Risk




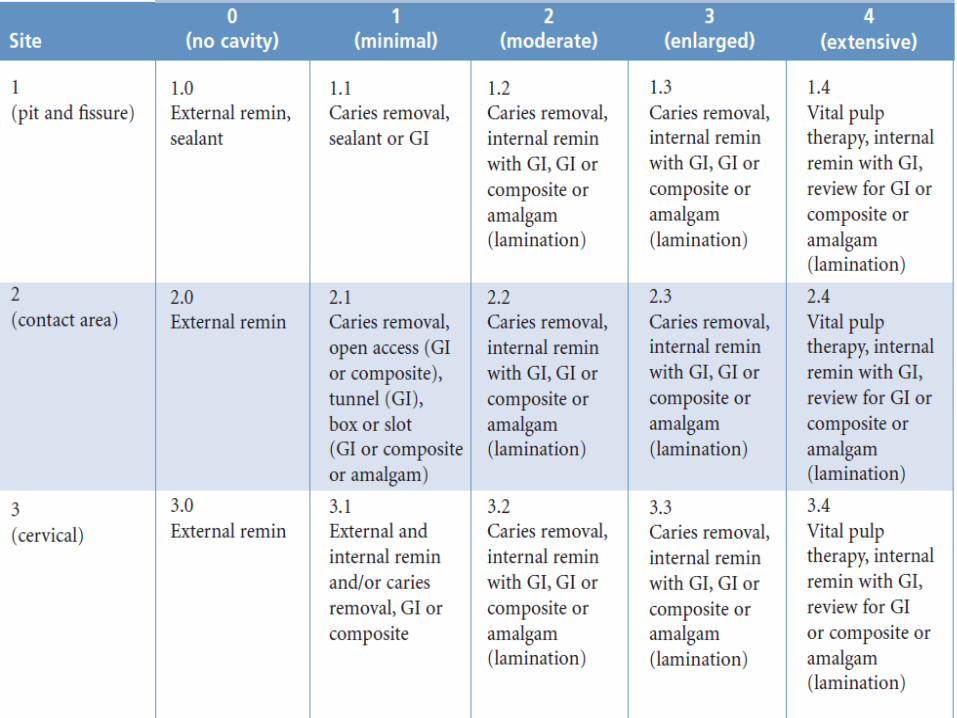
NEW CARIES CLASSIFICATION


MOUNT AND HUME CLASSIFICATION

SITE 1

SITE 2

SITE 3
4.REMINERALIZATION OF EARLY LESIONSAND REDUCTION OF CARIOGENIC BACTERIA

• Enamel and dentin demineralization is not a continuous, irreversible process.
• Through a series of demineralization and remineralization cycles, the tooth alternately loses and gains calcium and phosphate ions, depending on the microenvironment
Minimally invasive dentistryCAROL ANNE MURDOCH-KINCH
JADA, Vol. 134, January 2003

When the pH is less than 5.5, subsurface enamel or dentin will demineralize.
Fluoride enhances the uptake of calcium and phosphate ions and can form fluoroapatite.
Fluorapatite demineralizes at a pH less than 4.5, making it more resistant to demineralization from an acid challenge than hydroxylapatite.
In early carious lesions, there is subsurface demineralization of the enamel.
As caries progresses into dentin, the surface of the enamel eventually cavitates.
Minimally invasive dentistryCAROL ANNE MURDOCH-KINCH
JADA, Vol. 134, January 2003


surgical treatment— caries removal and restoration—is indicated for the cavitated lesion
In the noncavitated lesion, to take advantage of the tooth’s capacity to remineralize, one must first alter the oral environment, to tip the balance in favor of remineralization and away from demineralization.
Minimally invasive dentistryCAROL ANNE MURDOCH-KINCH
JADA, Vol. 134, January 2003

This is achieved by:1. Rebalancing the oral environment2. Approach to remineralization3. Surface protection• Changing the microflora, using agents such as topical
chlorhexidine and topical F• Reducing the amount of dietary sucrose• Decreasing the intake of fermentable carbohydrates• Adding fluoride, particularly through daily application
during tooth brushing• Increasing salivary flow, using mechanical stimulation
during vigorous chewing to enhance flow, by changing drugs which reduce flow, or by using drugs to enhance flow.
• Fissure protection by use of sealants.

Rebalancing the Oral Environment
i. Use a chlorhexidine mouthwash twice a day, ii. Limit intake of fermentable carbohydrates, iii. Ensure an optimum salivary flow,iv. Use buffering agents to control oral ph, v. And practice good oral hygiene to prevent plaque
accumulation.
The goal is to change the local biochemistry so that the patient is no longer losing tooth mineral and further cavitation does not occur

Approach to Remineralization
Fluoride is widely known molecule that enhanceremineralization.
It is used in various forms, topical application ofgel/foam, mouthwash, varnish, in toothpastes.
Fluoride combines with hydroxyapatite to formfluorapatite layer that is resistant to dissolution inacid produced bymicroorganisms.

Non-Fluoride Remineralizing Agents
CPP-ACP complex
Demineralized EnamelRemineralized enamel using fluoride and CPP-ACP
Body of lesion remineralized with CPPACP

NovaMin® (calcium sodium phosphosilicate)
is a bioactive glass composed of minerals that naturally occur in the body and reacts when it comes into contact with water, saliva or other body fluids.
This reaction releases calcium, phosphorus, sodium and silicon ions in a way that results in the formation of new hydroxycarbonate apatite (HCA) crystals.
NovaMin forms a mineralized layer that is mechanically strong and more resistant to acid

Xylitol containing chewing gums increase salivary flowrate and enhance protective properties of saliva by increasing the buffering activity.
The concentration of bicarbonate and phosphates ions in stimulated saliva is high which help in preventing demineralizationXylitol containing chewing gums increase salivary flow rate and enhance protective properties of saliva by increasing the buffering activity.
The concentration of bicarbonate and phosphates ions in stimulated saliva is high which help in preventing demineralization

7.MINIMAL INTERVENTION TOOTH PREPARATION

Conventional caries removal and cavity preparation entail the use of the burs.
Disadvantages of this system include:(1) The perception by patients that drilling is
unpleasant.(2) Local anesthesia is frequently required.(3) Drilling can cause deleterious thermal effect
combined with the use of pressure for caries removal, causing pulpal effects.
(4) The use of a hand piece may result in removal ofsoftened, but affected dentine, resulting in an
excessive loss of sound tooth tissue.

An Introduction To MinimalIntervention Dentistry (MI)
S Mickenautsch
DENTAL NEWS, VOLUME XIV, NUMBER IV, 2007


1.MECHANICAL ROTARYi. BURS
2.MECHANICAL,NON ROTARYii. AIR ABRASIONiii. AIR POLISHING
iv. ATRAUMATIC RESTORATIVE TECHNIQUEv. ULTRASONICS
vi. SONIC ABRASION3.CHEMO-MECHANICAL
vii. CARISOLV,CARIDEXviii. ENZYMES
4.PHOTOABLATIONix. LASER

MECHANICAL ROTARY BURS

The Fissurotomy® Bur1. It can be used to progressively explore suspect fissure
systems or portions of fissure systems.
2. The bur can be used to create one pass cutting to theDEJ, when its depth is accurately judged by knowingthe bur head length (2.5 mm) and gauging depth byrelating the bur head/neck junction to the cavosurfacecavity preparation margin.
3. The bur can be used to remove very small amounts of carious dentin..

• The bur can be used to gain access to larger dentin carious lesions by efficiently removing overlying enamel
• Finally, the bur can be used for enameloplasty procedures to remove irregular surface and fissurerelated defects, and to prepare an area for restoration or sealing.

The goals of ultraconservative preparation are quite simple:
1. Recontouring the fissure and pit anatomy for access and visibility.
2. Exploration of the cavity to ensure that no decay remains undetected.
3. Ultraconservative (but complete) caries removal.

Variations In Dealing With AProximal Lesion

Smart Polymer Burs !!!
Dream or Reality ?


SMART PREP KIT


KNOOP HARDNESS NUMBER



ATRAUMATIC RESTORATIVE
TREATMENT

“No Needle, No Drill,
No Noise”

The correct use of the ART approachJo E. FRENCKEN1, Soraya Coelho LEAL
J Appl Oral Sci. 2010;18(1):1-4

DEFINITION
• Elementary technique of caries removal using hand instruments only ,combined with the use of modern restorative material with adhesive characteristics
PioneersFrencken Joe, Makoni F. in Tanzania 1980

PRINCIPLE
• Removal of cariogenic biomass
• Seal & protect tooth
• Place an adhesive restorative material


ART Indications
• Limited access to traditional care• Pediatric & Geriatric care• High caries risk management• Extreme dental fear/anxiety
management

ADVANTAGES OF ART• Easy Caries Removal • Conserve tooth structure• Hand Instruments• Limitation of Pain, Non threatening• Restore with an adhesive material• No local anesthesia• No high/low speed hand piece• No suction• No water• Simple infection control• Prevent secondary caries(Fluoride)• Ease of repair• Low cost

Procedure• Isolate• Access• Excavate• Condition• Insert• Press• Remove excess
….Instruct patient not to eat for at least an hour

Atraumatic restorative treatment (ART)
The most common failures are:-
Partial material lossComplete material lossCaries related to restoration marginMaterial wear >0.5 mm
Atraumatic restorative treatment (ART) – factors affecting successMickenautsch S and Grossman E S
Journal Of Minimum Intervention In Dentistry2008; 1 (2)

ART failures may occur in combination or lead to each other.
• Hand excavation, as a mechanical form of selective caries removal, is capable to remove most of the infected dentin.
• However, research showed that bacteria remain present after complete hand excavation within the tubuli of affected dentine
Bönecker M, Grossman E, Cleaton-Jones PE, Parak R. Clinical, histological and microbiological study of hand-excavated carious dentine in
extracted permanent teeth. South Afric Dent J 2003; 58: 273-8.

Caries activity can be reduced through- effective nutrient deprivation by sealing the
cavity using filling materials which chemically bond to the cavity walls
assist remineralisation of affected dentine through long-time fluoride and mineral release
Weerheijm KL, Groen HJ. The residual caries dilemma.
Community Dent Oral Epidemiol 1999; 27: 436-41
• Clinical factors responsible for ART failures are
1. Material Factor 2. Operator Factor
3. Technique Factor
Atraumatic restorative treatment (ART) – factors affecting successMickenautsch S and Grossman E S
Journal Of Minimum Intervention In Dentistry

Atraumatic restorative treatment (ART) – factors affecting successMickenautsch S and Grossman E S
Journal Of Minimum Intervention In Dentistry

WHAT IS UNDERSTOOD BY‘MODIFIED ART’?
• Modification is most often associated with theuse of rotary equipment: the drill, to open thetooth cavity, followed by the normal ARTprocedure in cleaning and restoring the cavity
• It has been suggested that the use of rotaryequipment would make the total procedurequicker and easier.
The correct use of the ART approachJo E. FRENCKEN1, Soraya Coelho LEAL

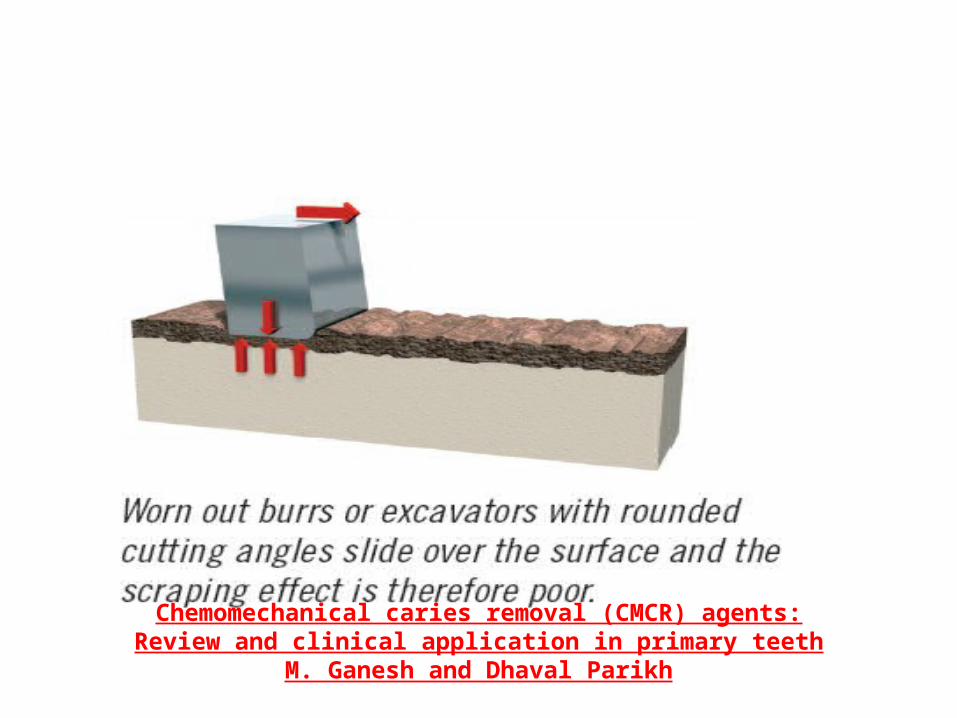
CHEMO MECHANICAL CARIES REMOVAL (CMCR)
Chemical softening of carious dentin followed by its removal by gentle excavation

• Softened the outer dentin• Solution 1: NaOCl• Solution 2: glycine+amino butyric acid+ NaCl+NaOH• pH = 11
CARIDEX
Chemomechanical caries removal (CMCR) agents:Review and clinical application in primary teeth
M. Ganesh and Dhaval Parikh


MediTeam – Sweden-1998
carisolvChemomechanical caries removal (CMCR) agents:Review and clinical application in primary teeth
M. Ganesh and Dhaval Parikh
2 Syringes
NaOCl
Pink Viscous gel ( Lysine, Leucine, Glutamic Acid +Carboxymethyl cellulose + Erythrosine )
Time Required – 10 – 15 mins
Max Volume of Gel – 0.2 – 1 ml
Cloudy - frosty
‘A silent revolution’

Procedure
Chemomechanical caries removal (CMCR) agents:Review and clinical application in primary teeth
M. Ganesh and Dhaval Parikh

Chemomechanical caries removal (CMCR) agents:Review and clinical application in primary teeth
M. Ganesh and Dhaval Parikh
Chemomechanical caries removal (CMCR) agents:Review and clinical application in primary teeth
M. Ganesh and Dhaval Parikh

ADVANTAGES• Painless• No need of local anesthesia• Conservation of sound tooth structure• Reduced risk of pulp exposure• Well suited for anxious patient
LIMITATION
• Rotary and hand instruments may still be needed
Chemomechanical caries removal (CMCR) agents:Review and clinical application in primary teeth
M. Ganesh and Dhaval Parikh

ENZYMES

Enzymes for removal of caries !!!!!! • Achromobacter collagenase- In 1989 Goldsberg and
Keil• Enzyme Pronase –non specific proteolytic enzyme –
Streptomyces griseus
• Pepsin- carboxylic protease enzyme ,acts only on non-helical and denatured collagen segments.

PAPACARIE
MAIN COMPONENTS –•PAPAIN- Enzyme•CHLORAMINE- Bactericidal and disinfectant•TOLUIDINE BLUE- Coloring agent
Chemomechanical caries removal (CMCR) agents:Review and clinical application in primary teeth
M. Ganesh and Dhaval ParikhJournal of Dentistry and Oral Hygiene Vol. 3(3)34-45, 2011

MODE OF ACTION
Chemomechanical caries removal (CMCR) agents:Review and clinical application in primary teeth
M. Ganesh and Dhaval Parikh

AIR ABRASION (Kinetic Cavity Preparation)

• Air abrasion utilizes kinetic energy from alumina particles entrained in high velocity stream of air to remove tooth structure

Kavo Rondo Flex
KCP 100
Prep Start

Comparison between drill and air abrasion
High Speed Drills Air Abrasion
Rotary bur cause micro fractures No micro fractures
Excessive destruction of tooth structure
Less destruction of tooth structure
Heat,vibration,bone conducted noise-patient discomfort
Heatless,vibrasion less, minimal sound
Patient Anxiety Patient friendly

Abrasive particles
• Aluminum oxide• Alumina particles – alpha alumina, pure,
biocompatible, used in food and medicine, prime ingredient in tooth paste
• Particle size – 27 micro meter• Polycarbonate resin alumina- hydroxyapatite
mixtures-selective in removal of caries• Sodium bicarbonate-remove surface stains ,plaque

Dental Air Abrasion - YouTube.flv

Applications of Air Abrasion
• Cavity preparations• Removal of temporary cement• Micro abrasion of white spot enamel
hypoplasia• Stains removal• Repair of acrylic ,composite, porcelain

Air abrasion cannot be used for …
• Crown preparation• Large-deep carious defects• Amalgam removal• Class II Cavity preparations

ADVANTAGES
• Non traumatic treatment• Biocompatibility• No Chipping• No micro fracturing• Decreased thermal build up• smooth margins• Less invasive procedure• No anesthesia• Less discomfort

DISADVANTAGES
• Lack of tactile sensation• Non contact based modality• Messy –Spread of aluminium oxide• Danger of air embolism and emphysema• Impaired indirect view

Contraindications
• Asthma patients• Severe dust allergy• Chronic pulmonary disease• Recent extraction• Open wound in oral cavity• Sub gingival caries removal

Safety Issues
• Masks• Rubber dam• Dry vaccum systems• Eye glasses• Disposable mouth mirror• High speed suction

OZONE THERAPY

THE MOST BEAUTIFUL THINGS ON EARTH ARE ALSO THE MOST SIMPLEST AND MOST NATURAL !!!!!

OZONE
NATURE’S MOST POWERFUL OXIDANT
CARIOUS LESIONS NOT ONLY BECOME STERILE AFTER EXPOSURE TO OZONE BUT ALSO TEND TO RE-MINERALIZE AFTER SOMETIME
Kills bacteria,spores and viruses….

ozone to the rescue ….• completely eliminates acidophilic
bacteria ,fungi and viruses • Sterile environment • 10 secs of 2200 ppm ozone
eliminates 99 % of the carious micro flora
• Niche is very unlikely to re-develop

Effects of ozone
• kills microbes
• Plaque• Little influence on alloys
Ozone A powerful biocide

Heal ozone Tec3 ( Curosone, USA)
POLYURETHANE CONSOLE HAND PIECE PATIENT KIT
•Ozone Generator•Vacuums pump •Flow sensors •Peristaltic pump• Desiccant •Ozone destructor•Back-lit LCD Display
•Hand piece•Disposable sealing cup•Push button
•Re-Mineralizing tooth paste•Oral rinse•Travel spray



Clinical steps Polymer Cup is adapted to carious lesion and air is sucked to create a vacuum
Ozone gas is delivered at a preset conc. ,for 10 secs if the seal is good
If the seal is defective the unit switches off
Suction activated for 10 secs to remove debris from the surface
Suction system passes gas through Granular activated carbon filter to remove all traces of ozone
Reductant fluid is pumped for 5 secs onto treatment site to start the remineralization process
Patient is instructed to use ‘home care kit’ and recalled after 3 months for check up ,when a cosmetic restoration can be placed if needed

OZONE THERAPY

Indications for Ozone Therapy
• Primary root carious lesions• Early carious lesions• Pit and Fissure caries• Caries around crowns and bridges

Advantages• Kills 99%micro organisms• Oxidizes caries and speeds up re-
mineralization• Removes organic debris on carious lesions• Removes volatile sulphur which cause halitosis• Decrease treatment time• Microbes don’t become resistant• Non –allergic, noiseless, painless and Phobic
friendly and pedo friendly

BIDDING A FINAL FAREWELL TO OUR DRILL,
FILL AND BILL PHILOSOPHY !!!!

LASER THERAPY

Efficacy of laser depends on •Wavelength characteristics•Pulse energy•Optical properties of incident tissue
Applications•Selective Hard Tissue Ablation•Selective Carious Dentin Removal•Destroy S.Mutans•Sealing of Fissures•Cut Dental Hard Tissue•Adjunctive treatment in caries prophylaxis•Modify structures of dentin and enamel

Lasers used for selective hard tissue ablation•Er:YAG :Yttrium –Aluminium-Garnet and Nd:YAG – Neodymium-YAG-IR Emission•C02 Laser – IR Emission•Excimer Lasers (ArF- Argon: Freon and XeCl – Xenon : Chlorine – U.V.Emission•Holomium lasers•Dye enhanced laser ablation – Indocyanine Green & Diode Laser
Carious Dentin Removal – UV Excimer (377nm)Destroy S.Mutans – Excimer with Dye
Sealing of fissures – CO2


Laser Caries Removal Technique - YouTube_2.flv

Advantages
• Effect of vibrations,pressure and unfavorable temperatures associated with rotary cutting instruments –avoided
• Safe and efficacious modality of caries removal and cavity preparation
Limitations•Expensive•Size of the instrument

POINTS TO REMEMBER…
• GENTLY TOUCH TARGET TISSUE • CUTTING RADIATION ONLY FROM THE END OF
TIP• WATER STREAM TO TARGET TISSUE• OPERATION AREA SHOULD BE WET• KEEP TIP MOVING• WIDE CUT- TIP OVER THE SURFACE• DEEP CUT- TIP UP & DOWN

Laser safety

SONIC OSCILLATION (SONOABRASION)

SONO ABRASION• Removal of carious dentin using high
frequency ,sonic air scaler with modified abrasive tips
First Design
•Sonic micro unit deigned by Dr.Hugo Unterbrink and Mosele•Based on Soniflex Air scaler Hand piece •Oscillations - < 6.5 KHZ

Mechanics
Elliptical motion Transverse 0.08 - 0.15mm Longitudinal - 0.055 -0.135mm
Diamond Coated – 40 micro meter grit Water irrigation 20-30ml/minAir pressure 3.5 bar

• Torque Applied – 2N • More pressure - dampens oscillations
Indications
•Carious dentin removal•Finishing cavity preparations
More studies needed to prove its efficiency

Principals of Minimally Invasive Restoration1. Shape of cavity is dictated by the caries and unique
foreach carious lesion (conservative cavity preparation).2. Only demineralized enamel and infected dentine isremoved, affected dentine can be left.3. Macromechanical retention not required.4. Undermined enamel cavity can be restored with
adhesive materials.

BIOMIMETIC MATERIALS

CPP-ACP
• Casein phosphopeptide- amorphous calcium phosphate
releases Ca and Phosphate ions
GC tooth mousse,ACP composite

• Remineralization effect of 0.5 - 1.0% CPP-ACP solution, equivalent to 500 ppm of Fluoride
• GC TOOTH MOUSSE
• flavor helps stimulate salivary flow



ARISTON pHc • Introduced by ivoclar-vivadent in 1998• Light activated alkaline –glass restorative material• Intelligent restorative material as it releases
calcium,flouride and hydroxyl ions when intraoral pH values dropes below critical 5.5 level
• Restoration of class I and II lesions.

BIODENTINE
• Bio-active dentin substitute• All-in-one, biocompatible, bulk filling material.• Ca3SiO5 based cement• A supra plasticizing admixture to reduce the water
content to the mix and retain its workability.• Improved handling properties.• Setting time - 10 min.• Helps in re-mineralization of dentin.

8.REPAIR VS. REPLACEMENT OF DEFECTIVE RESTORATIONS
caries under well-sealed restorations fails toprogress and that caries progresses slowly Inmost populations, repairing defective
restorations rather than replacing them is a valid and more conservative option for treatment
Minimally invasive dentistryCAROL ANNE MURDOCH-KINCH
JADA, Vol. 134, January 2003

PEDIATRIC MINIMAL INTERVENTION DENTISTRY

Caries Management Protocol for 1-2 Year Olds

Caries Management Protocol for 3-5 Year Olds

Caries Management Protocol for ≥6 Year-Olds

GERIATRIC MINIMAL INTERVENTION DENTISTRY
COMPLEXRESTORATIVE CHALLENGES IN OLDER
PATIENTS

• Erosion, • Abrasion,• Demineralization,• Rampant coronal and root caries, • Sound and decayed retained roots, • Recurrent caries (necessitating crowns and other
repairs),• Subgingival caries, • “wet” oral environments

• Salivary gland hypofunction,• Disruptive behaviours, • Poor compliance with preventive care, • High plaque levels,• Bleeding and swollen gingival tissues, and • Financial and• Other restrictions on care options

• The use of a blunt or periodontal probe is advocated for exploring root-surface caries in older adults

TECHNIQUES
• Placement of Glass Ionomers• Sandwich Technique• Remineralization and Restoration to Counteract
Erosion and Abrasion• Tunnel and Slot Preparations• Techniques for “Wet” Subgingival Environments• Vital Pulp Therapy• Geriatric Atraumatic Restorative Technique

Placement of Glass Ionomers

Sandwich Technique
• 2 direct restorative materials can be used to “make the most of the biological, physical and/or aesthetic properties of each material, and in the presence of adhesion, to achieve as close as possible to a single monolithic reconstruction of a tooth.
• useful in situations when strength and pleasing esthetics are essential

• FULL SANDWICH TECHNIQUE
• PARTIAL SANDWICH TECHNIQUE
Remineralization and Restoration to Counteract Erosion and Abrasion
Remineralization involves the use of products such as-
Topical fluorides and Amorphous calcium phosphatesMI Paste (GC America)

Restoration of cervical lesions may beundertaken when esthetics is an issue or when
soft caries and cavitation have occurred. The use of glass ionomers and composite
resins either alone or in combination (with a sandwich technique) is generally recommended

Tunnel and Slot Preparations
• Slot preparations are indicated for lesions that are less than 2.5 mm from the marginal ridge.
• The lesion is more than 2.5 mm from the marginal ridge, a tunnel preparation can be used.


Techniques for “Wet” Subgingival Environments
In many older patients it can be extremely challenging to control bleeding and saliva during restoration of subgingival carious lesions, which tend to recur around large restorations and crowns.
A glass ionomer such as Fuji Triage works well in these “wet” environments because it has low viscosity and does not “run”

Caries Classification And Treatment Options For Geriatric Minimal Intervention Dentistry

STRATEGIES FOR ADDRESSING THE NEW CARIESCHALLENGE IN OLDER PATIENTS



• For older patients, the practitioner may need to assess modifying factors such as those
i. Social support,ii. Transportationiii. Fear and anxiety, iv. Consent,v. Restraint andvi. Perceived need

Chemoprophylactics

CATIONIC
• chlorhexidine gluconate (CHX),• cetylpyridinium chloride (CPC), • benzalkonium chloride, • hexetidine and • metal salts;
ANIONIC
• sodium lauryl sulfate;
NONIONIC• Phenolic compounds (essential oils) and
triclosan.

OXYGENATING AGENTS
• hydrogen peroxide and • surface-modifying agents(e.g., delmopinol).

Treatment of xerostomia and salivary gland hypofunction

General treatment
• Change medications to classes that are less anticholinergic lead to less fluid retention
• Increase water intake (if not contraindicated bymedications and medical conditions).• Avoid dental products with additives (e.g., sodium
lauryl sulfate) or alcohol (e.g., mouthrinses)• Use a room humidifier during the day and at night.

Saliva substitutes and oral lubricants
• Oral Balance Gel,• Denture Grip,• Biotene Range (mouthrinse, toothpaste and gum) • MI Paste (GC America, Alsip, Ill; • Range of other products such as Moi-Stir(Kingswood Laboratories, Indianapolis, Ind.),• MouthKote • XeroLube
Saliva stimulants
• Sugar-free gum and candy several times daily (e.g.,xylitol gum and candy products, • Trident White with Recaldent gum (Cadbury Adams
USA LLC, Parsippany, N.J.)• SalivaSure tablets (Scandanavian Formulas,
Sellersville, Penn.) Place near major salivary ducts several times daily and suck.
• Contains fruit acid which is pH buffered. • Systemic sialogogue therapy with pilocarpine or
cevimeline;


Future of
Minimal Intervention Techniques …

NANOTECHNOLOGY
Richard.P.Feynman
Think twice before you pick up that hand piece ……. ….Because the cutting edge is not a dental bur anymore !!!
CONCLUSION

Thank you…

Types of caries lesions
Cavitated caries lesions
Non-cavitated caries lesions
Causes structural alteration of the surface of the tooth enamel, without loss of macroscopic
substance and
led to structural alterations to such a
degree that there is loss of dental substance
and the formation of a cavity, whether shallow
or deep
Tooth restoration – Non Invasive TechniquesBasso M
J Minim Interv Dent 2011; 4 (3)

As a rule of thumb, it can be said – cavitated lesions we have no choice but to carry outinvasive restorative procedures, while with non-cavitated surface lesions we caninstead opt for restorative solutions that do notinvolve working with abrasives and hence, do notentail procedures of a locally invasive nature.
Tooth restoration – Non Invasive TechniquesBasso M
J Minim Interv Dent 2011; 4 (3)




![Evidence based Compendium – [Database] - midentistry.com · Evidence based Compendium – [Database] handbook Plus+ Minimum Intervention (MI) in Dentistry Edition 1.3](https://img.pdfslide.us/doc/110x75/5c8d639209d3f218598b69aa/evidence-based-compendium-database-evidence-based-compendium-database.jpg)