-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
1/21
SANDY KARTIKA P C11108214
NURUL AINI C11108785
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
2/21
Patients IdentityName : Mrs. S
Gender : Female
Age : 56 years old
Marital Status : Married
Address : Jl. Vet. Utara LR 41/39
Admission Date : 3 February 2012
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
3/21
History TakingChief complaint : rupture of blisters on the
back,
chest, arms, abdomen, and lipatan paha
Happen 1 week ago, starts with appear blisters
on the left armpit and ruptured later. Shortlythereafter, the
patient develops widespreadbullae that are easily ruptured.
Post operation of mammae (7 days before)Medication History :
Tamopen, Dexamethasone,
Pirolesicam,
Fever (+) 1 day before bulla presented
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
4/21
Physical ExaminationAnemic (-), icterus (-), cyanoses (-)
Erosion covering
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
5/21
Current Status General status
Composmentis
Severe Sickness
Adequate nutrition Moderate Hygiene
Vital sign
Blood pressure : 110/90mmHg
Pulse rate : 80x/min
Respiration rate : 24x/min
Temperature : 36C
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
6/21
Dermato-venerology StatusLocation 1 : Regio Mammae dextra,
abdomen sinistra
Effloresensi : Bulla
Location 2 : Regio extremities superior et
inferior,truncusposteriorEffloresensi : Bulla, vesicle,
excoriation,
erosion, epidermolysis
Location 3 : Regio Mammae sinistra,Effloresensi : Ulcus post op
Ca mammae
Location 4 : Regio oralis
Effloresensi : Stomatitis, crust
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
7/21
Laboratory Result
Ureum : 129 mg/dl
Creatinin : 1,7 mg/dl
GDS : 66 mg/dl SGOT : 67 U/l
SGPT : 172 U/l
Natrium : 129,50 mmol/l
Kalium : 4,33 mmol/l
Chloride : 102,30 mmol/l
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
8/21
Recommended examination
Consult diet
Consult ENT Chest X-ray examination
Punch biopsy
Immunofluorescence microscopy
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
9/21
ResumeA 56 years old woman came to the hospital with
complain rupture of blisters on the back, chest, arms,abdomen,
and lipatan paha. Happen 1 week ago, starts
with appear blisters on the left armpit and ruptured
later. Shortly thereafter, the patient developswidespread bullae
that are easily ruptured. Pasien
mengeluh susah menelan. Nyeri pada lesi (+), gatal
pada lesi (+).
Post operation of mammae (7 days before). MedicationHistory :
Tamofen, Dexamethasone, Piroxicam. Fever
(+) 1 day before bulla presented. Family medical
history with the same complain (-).
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
10/21
DiagnosisStevens-Johnson Syndrome
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
11/21
Treatment
1. Dexamethasone inj. 1 amp/ 6 h./ iv
2. Gentamicin 1 amp/12 h./ iv
3. Afucid cr.
4. Compress NaCl 0.3%
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
12/21
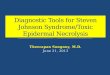
PICTURES (9-02-2012)
Fig. 1 Fig.2
Figure 1: Stomatitis and crust on the upper and lower lips
Figure 2: Ulcus post op Ca mammae at the upper chest ofthe
patient.
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
13/21
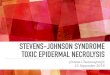
Fig.3 Fig.4
Figure 3 and 4: SJS with bulla, vesicle, excoriation, erosion,
and
epidermolysis on the armpit and arms.
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
14/21
Fig.5 Fig.6
Figure 5: Bulla on the whole abdomen of the patient
Figure 6: Erosion, bulla, and excoration on the
thighintertrigo
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
15/21
STEVENS JOHNSON SYNDROME
Acute life-threatening mucocutaneousreactions characterized
byextensive necrosis
and detachment of the epidermis.
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
16/21
Idiopathic - 25%
Drug allergy 50%
- Analgesic- Antipyretic
- Anticonvulsan
- Traditional drug
And the other are Infections
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
17/21
TRIAS:
Skin abnormality : The initial skin lesions are
characterized by erythematous, dusky
red, purpuric macules, irregularly shaped,
which progressively coalesce.Mucous membrane involvement :
The
oral cavity and the vermilion border of the
lips are almost invariably affected and feature
painful hemorrhagic erosions coated
by grayish white pseudomembranes andcrusts of the lips
Extra-Cutaneous Symptoms : associated with high fever, pain,
and weakness
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
18/21
Pathogenesis
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
19/21
DiagnosisAnamnesis & history taking
Physical examination
Laboratory examinationo Low serum albumin and increase in
gammaglobulins;
electrolyte imbalance; acute-phase proteins increased.
o
Leukocytosis (+) means the causes is infectiono Eosinofilia (+)
means the causes is allergy
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
20/21
Treatment
Remove any potential offending and unnecessary
medications
Address nutrition, fluid and electrolyte balance
Oral corticosteroid
Local skin care with compression to weeping orcrusted sites,
bland emollients and mid-potencytopical corticosteroids
For secondary infection with systemic antibiotics
-
7/29/2019 Mini Poster - Stevens Johnson Syndrome
21/21
Prognosis If the management is fast and adequate, the
prognosis
is better.
The mortality rate is 5-12%. The prognosis is notaffected by the
type or dose of the responsible drug orthe presence of human
immunodeficiency virusinfection but depending on the severity of
the disease
and the prior general condition of the patient.