Embed Size (px)
Citation preview
Volume 38/Number 4/October 2016/Pages 360-374 /doi: 10 .17744/mehc.38.4.06
Mindfulness, Self-Compassion, and Counselor Characteristics and Session Variables
Cheryl L. Fulton Texas State University
Mindfulness has garnered interest as a counselor development tool for enhancing the therapeutic relationship and increasing counselor trainee effectiveness, yet empirical study o f counselor mindfulness is limited. A study o f the relationship between mindfulness and client perceived empathy among 55 client-counselor trainee dyads is reported. The relationships between counselor trainee mindfulness, self-compassion and ambiguity tolerance, experiential avoidance, and session depth were also examined in this exploratory study. Counselor trainee mindfulness was associated with client perceived empathy and both mindfulness and self-compassion were associated with lower experiential avoidance and greater session depth as rated by the counselor trainee. Self compassion was positively related to tolerance for ambiguity. Implications for counselors, educators, and supervisors and suggestions for practical application o f mindfulness for counselor development are discussed.
There are a number of counselor capabilities considered important to effective counseling including empathy (Rogers, 1957), tolerance for ambiguity (Bien, 2004; Levitt & Jacques, 2005), and affect tolerance, also called experiential avoidance in its negative form (Bien, 2004; Fulton, 2005). Counselor empathy is important to the development of the therapeutic relationship (Rogers, 1957), working alliance (Trusty, Ng, & Watts, 2005), and counseling outcomes (Elliott, Bohart, Watson, & Greenberg, 2011). Thus, empathic ability is an essential counselor training outcome. Empathy, as a counseling process, must first be experienced by the counselor, before it can be communicated and, in turn, received by the client (Barrett-Lennard, 1981). Although there are methods (e.g., microskills training) for teaching empathy skills (e.g., reflective listening), there are not equivalent methods for developing and maintaining one’s empathic capacity (e.g., Greason & Cashwell, 2009). Further, anxiety, which is inherent in counselor training, can impede the ability for empathy (Fliebert, Uhlemann, Marshall, & Lee, 1998).
Cheryl L. Fulton, D epartm ent o f Counseling, Leadership, Adult Education, and School Psychology, Texas
State University Correspondence concerning this artic le should be addressed to: Cheryl L. Fulton, 601
University Dr., EDUC 4026, San Marcos. TX, 78666. E-mail: c lfu lton@ txstate.edu.
360 0 Journal o f Mental Health Counseling
Mindfulness, Self-Compassion, and Session Variables
Affect tolerance and tolerance of ambiguity are purported to be important to empathic ability and effective counseling (Bien, 2004; Fulton, 2005; Levitt & Jacques, 2005). Bien (2004) proposed that tolerance of ambiguity be considered an addendum to Roger’s (1957) necessary conditions for therapeutic change because counselors must tolerate complex client situations without pushing for a premature solution, becoming apathetic, or sharing in the client’s despair. Ambiguity refers to being open to more than one interpretation, or being uncertain (Levitt & Jacques, 2005). Ambiguous situations are those that are complex, novel, and insoluble (conflicting information) and may promote stress, avoidance, delay, suppression, or denial (McClain, 2009). Clients are complex, often presenting contradictory feelings and concerns which can be challenging, particularly for trainees and novice counselors (Borders & Brown, 2005); ambiguity can be a barrier to understanding and promote frustration (McClain, 2009). Levitt and Jacques (2005) argued that ambiguity is inherent in counseling and the training process itself, therefore, educators need methods that support students to embrace ambiguity.
Experiential avoidance involves an unwillingness to remain in contact with sensations, emotions, thoughts, even when doing so is unproductive (Bond et ah, 2011). Experiential avoidance may be important to empathy as counselors are confronted with clients’ painful emotions which they must be present for, and empathize with, without personal distress, over-identification, or avoidance (Bien, 2004; Rogers, 1957); this may be difficult for trainees newly developing empathy skills. Further, because willingness to experience difficult thoughts, feelings, and sensations is central to many theoretical approaches, counselors must be able to model an appropriate relationship to these experiences (Bien, 2004). Bien (2004) recommended that counselors develop their inner life through practices such as meditation; however, empirical support for meditation as a means to develop affect tolerance among counselors is needed.
MINDFULNESS
Mindfulness has garnered attention as a potentially useful counselor training tool, particularly with regard to the development and maintenance of counselor empathy and the therapeutic relationship (e.g., Buser, Buser, Peterson, & Seraydarian, 2012; Fulton & Cashwell, 2015; Greason & Welfare, 2012). Mindfulness, rooted in the Buddhist tradition, is defined as intentional present moment awareness without judgment and requires an “affectionate attention” (Kabat-Zinn, 2012, p. 53) achieved by bringing kindness, compassion, equanimity, patience, curiosity, and trust to one’s awareness (Kabat-Zinn, 1994). Thus, mindfulness training typically includes both mindfulness practices that produce awareness and insight, and loving-kindness and compassion practices that foster compassion for both self and others. Self-compassion involves having feelings of concern for one’s own suffering and approaching one’s shortcomings with kindness, non-judgment, understanding, and awareness that shortcomings are part of the common human experience (Neff, 2003). Scholars have been uncertain as to whether compassion is considered an outcome of mindfulness
0 Journal of Mental Health Counseling 361
or a component of it (Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006). As a result, researchers often include study of both mindfulness and self-compassion, as they can be differentially or synergistically related to outcome variables such as empathy (Fulton & Cashwell, 2015).
Mindfulness, Self-compassion, and EmpathyBased on Buddhist psychology, empathy is viewed as a capacity that
can be cultivated through mental training, such as meditation (Greason & Cashwell, 2009). Neff and Pommier (2013) found that experienced meditators scored higher on measures of compassion for humanity and empathic concern than community or undergraduate samples. Based on controlled neuroscientific studies, researchers found mindfulness practices affected neural processes associated with enhanced empathic responses to social stimuli (Lutz, Brefczynski-Lewis, Johnstone, & Davidson, 2008) and increased grey-matter density in parts of the brain associated with empathy (Holzel et al., 2011). Likewise, based on self-report, self-compassion has been associated with social connection and empathy (Birnie, Speca, & Carlson, 2010; Neff, 2003).
Although sparse, there is evidence of a positive association between both mindfulness and self-compassion and empathy among counselors based on correlational studies (e.g., Fulton & Cashwell, 2015; Greason & Cashwell, 2009) and an early quasi-experimental study of mindfulness training among counselor trainees (Lesh, 1970). These studies, however, were based on a counselor’s self report of empathy. In a lone study, Greason and Welfare (2013) found mindfulness was related to client rated therapeutic factors (e.g., positive regard), however, it was not related to empathy. The researchers recommended that data on the length of the counseling relationship be included in future studies as this may have influenced the relationship between counselor mindfulness and empathy in their study.
Mindfulness, Experiential Avoidance, and Tolerance for AmbiguityMindfulness-based interventions are designed to help individuals attend
to aversive stimuli, including sensations, cognitions, and emotions, with open, non-reactive, non-judging, present-moment awareness (Baer, 2003). Bishop et al. (2004) posited that acceptance during mindfulness practice leads to decreased experiential avoidance and greater affect tolerance, coping, and increased self-observation which, in turn, leads to greater emotional awareness and cognitive complexity. Empirically, Farb et al. (2010) found that participants in an 8-week mindfulness training group (n = 18) had a similar sad reaction to watching a sad film as a control group (n = 18), however, those with mindfulness training had less neural activity (based on fMRI) while watching the sad film than the control group and compared to baseline. The researchers concluded that mindfulness meditation increased the ability to regulate emotion without necessarily avoiding or detaching from it. This has relevance for counselor trainees who must learn to sense and be present for a client’s affective state without becoming immersed in it (Rogers, 1957). Further, methods
362 0 Journal o f Mental Health Counseling

M in d f u ln e s s , S e l f - C o m p a s s io n , a n d S e s s io n V a r ia b le s
aimed at reducing experiential avoidance such as acceptance and commitment therapy incorporate mindfulness and have shown promise (Hayes, Luoma, Bond, Masuda, & Lillis, 2006), however, such approaches are designed for client concerns, and there is little study of how mindfulness may relate to experiential avoidance among counselors.
Tolerance of ambiguity is important, given the ambiguity' encountered in counselor training as well as in client presentations (Bien, 2004; Levitt & Jacques, 2005). Unfortunately, most studies of ambiguity tolerance in counseling are decades old and yielded few results (Levitt & Jacques, 2005). McClain (2009) created a new measure for ambiguity tolerance as he argued that older measures were weak conceptually and psychometrically; thus, the topic warrants reconsideration for study. Such studies are warranted, given that ambiguity tolerance is considered important for counselor trainees (Levitt & Jacques, 2005), and mindfulness is theorized to help individuals approach the present moment with equanimity (Kabat-Zinn, 1994) so they can remain open and flexible.
In sum, empathy, affect tolerance, and low experiential avoidance are important training variables. Mindfulness may be a potential means to address these variables, however, empirical study among counselors has been limited. The goal of this study was to extend previous studies in several ways. First, study of the relationship between counselor mindfulness and empathy among counselors has been based on counselor self report, and researchers have suggested that client feedback about this relationship is an important next step (Fulton & Cashwell, 2015; Greason & Cashwell, 2009). Further, Greason and Welfare (2013) recommended obtaining data regarding the length of the counseling relationship in future studies of counselor mindfulness and client perceived empathy, as this may have limited their ability' to find a relationship between counselor mindfulness and empathy in their study. Second, mindfulness outcomes such as affect tolerance and ambiguity tolerance have been theorized as important counselor attributes and associated with mindfulness, however, no current studies investigating these relationships among counselors were found. Third, because of the potential role of self-compassion and mindfulness outcomes, I included study of the relationship between self-compassion and study variables. Lastly, because there is limited knowledge of how counselor mindfulness impacts a counseling session, for both client and counselor trainee, session depth was examined. Session depth is the perceived power and value of the counseling session and the counselor’s perceived effectiveness (Reynolds et ah, 1996; Stiles & Snow, 1984). Fligher counselor- and client-rated session depth have been associated with greater client return rate (Tryon, 1990) and the perception that the session was a good vs. bad therapy hour (Reynolds et ah, 1996). Because mindfulness involves greater attention and patience in the present moment, it seems reasonable to explore its impact on both client-perceived empathy and session depth as session outcome variables.
The purpose of this study, therefore, was threefold: 1) to investigate the relationship between counselor mindfulness (and its facets) and client perceived empathy; 2) to determine the relationship between mindfulness and
4 Journal o f Mental Health Counseling 363
self-compassion and counselor attributes, including affect and ambiguity tolerance; and 3) to assess whether mindfulness and self-compassion are associated with session dynamics (i.e., session depth) as rated by both the client and the counselor. The following research questions were addressed: 1) Does mindfulness have a significant relationship with client perceived empathy? Which mindfulness facets best predict this relationship? 2) What are the respective relationships between mindfulness, self-compassion, and session depth? 3) What are the respective relationships between mindfulness and self-compassion and two counselor characteristics, experiential avoidance and ambiguity tolerance? Concordantly, I hypothesized that 1) there would be a positive relationship between mindfulness and client perceived empathy; no predictions were advanced regarding which facet would be most impactful; 2) mindfulness and self-compassion would be positively related to session depth (client and trainee); and 3) mindfulness and self-compassion would be negatively related to experiential avoidance and positively related to tolerance for ambiguity.
METHOD
ParticipantsFollowing institutional review board approval, a convenience sample of
master’s counseling students were recruited from practicum and intermediate methods courses in a CACREP-accredited counseling program at the researcher’s university. Intermediate methods courses differ from practicum primarily in that fewer clients are seen during the semester in the intermediate methods courses. The researcher obtained faculty support for the study and they agreed to have the researcher distribute and collect informed consent forms and questionnaires during class as well as to have trainees invite one client to participate. Eligible clients were university students and community members seeking services at the program’s clinic who were 18 years of age or older and able to voluntarily consent. Client-counselor trainee pairs participated in the study after at least three sessions so a therapeutic relationship could be established before client-perceived empathy was assessed. A total of 59 students from the total invited sample of 64 volunteered to participate yielding a 92% response rate. Four surveys were not useable due to incomplete data.
Based on the total sample, 48 (87.3%) were women, and 7 (12.7%) were men, with a mean age of 32.0 (SD = 7.3; Range = 23-50). Participants identified as European American (n = 43, 78.3 %), Hispanic/Latino/a (n = 7, 12.7%), and Biracial/Multiracial (n = 5, 9.0%). The majority of participants were in the clinical mental health track (n = 27, 49.1%), followed by couple and family (n = 12, 21.8%), school (n = 10, 18.2%), and dual track (n = 6, 10.9%). Seventy percent were in practicum classes and 30% in intermediate methods classes. Approximately 64.2% of trainees reported having a mindfulness practice, however, their practice was primarily described as yoga, occurring less than weekly; some meditation and prayer were also noted. Lastly, 39.6% of trainees reported exposure to mindfulness education, primarily yoga classes, personal counseling, or books. For client participants, 48 (87.3%) were women, and 7 (12.7%)
364 $ Journal o f Mental Health Counseling

Mindfulness, Self-Compassion, and Session Variables
were men; client mean age was 36.4 (SD = 13.3; Range = 19-61). Participants identified as European American (n = 34, 61.8%), Hispanic/Latino/a (n = 15, 27.2%), African American (n = 3,5.5%), and Biracial/Multiracial (n = 3,5.5%).
ProcedureCounselor trainees were provided with a script to read to their clients
inviting them to participate. The script included information that participation was voluntary and in no way tied to receiving services and was followed with obtaining client consent (100% of invited clients participated). Participants were blind to the study variables and both clients and counselor trainees were each given $3.00 as incentive for participation. Clients and trainees completed surveys in separate rooms and the majority of clients turned in surveys directly to the researcher as they exited the clinic. In the researcher’s absence, clients returned surveys via sealed envelope to their counselor; these were in turn collected by the instructor and returned to the researcher.
InstrumentationCounselor trainees completed the Five Facet Mindfulness Questionnaire
(FFMQ; Baer et ah, 2006), Self-Compassion Scale (SCS; Neff, 2003), Session Evaluation Questionnaire-Form 5 (SEQ; Stiles & Snow, 1984), Acceptance and Action Questionnaire - II (AAQ-II; Bond, et ah, 2011), and Multiple Stimulus Types Ambiguity Tolerance Scale-II (MSTATS; McClain, 2009). Counselors also completed the Therapeutic Presence Inventory (Geller, Greenberg, & Watson, 2010) which was used to answer research questions not addressed in this article. Clients completed a demographics questionnaire, tire SEQ, and the Barrett-Lennard Relationship Inventory-Client Form (BLRI; Barrett-Lennard, 1962).
Mindfulness. The FFMQ (Baer et ah, 2006) is a 39-itenr self-report questionnaire designed to measure mindfulness in daily life. The FFMQ consists of five mindfulness facets (subscales): Observe, Describe, Act with Awareness, Non-judge, and Non-react. Items are rated on a 5-point scale ranging from 1 (never or rarely true) to 5 (very often or always true) and each subscale is scored and the five factors combined to form a total score of mindfulness. The FFMQ has shown adequate construct validity and good internal consistency, with subscale alphas ranging from .75 to .91 and a full scale alpha of 0.96 (Baer et ah, 2006). The alpha coefficient in the current sample was .90 for the total scale and ranged from .80 to .92 for subscales.
Session depth. The SEQ (Stiles & Snow, 1984) is a 21-item questionnaire developed to measure client and counselor perspectives of immediate session impact. Specifically, the SEQ measures whether a counseling session was judged as good or bad based on two dimensions: 1) powerful and valuable versus weak and worthless (session Depth) and 2) relaxed and comfortable versus tense and distressing (session Smoothness). Two additional subscales measure participants’ post session mood, Positivity and Arousal. Participants endorse adjectives on a 7-point bipolar adjective format. The first 11 items measure
$ Journal o f Mental Health Counseling 365
session evaluation (depth and smoothness) using words such as “bad-good” and “valuable-worthless”. Ten items measure post-session mood and include adjectives such as “angr\’-pleased” and “calm-excited”. The authors reported that factor-analytic studies confirmed all four dimensions as underlying counselor-client session ratings. Internal consistency was high (ranging from .81-.93) for all dimensions across a variety of conditions and settings (Reynolds et al., 1996). In this study, the independent dimension of session Depth was used to evaluate participants’ most recent counseling session as this was deemed more theoretically relevant to counselor mindfulness. Greater ability to attend to a client’s experience should theoretically influence the client’s sense that the session was valuable, however, it may not necessarily equate with the perception that the session was relaxed. The alpha coefficient for session depth in the current sample was .77 (counselor) and .68 (client).
Client perceived empathy. The BLRI (Barrett-Lennard, 1962) comprises four subscales: Level of Regard, Empathy, Unconditionality, and Congruence, which are based on Rogers’s (1957) theory of the necessary conditions for promoting therapeutic change in the counseling relationship. Clients rate the extent to which they felt their counselor understood them in the session using a 6-point scale (e.g., “My counselor nearly always knows exactly what I mean”). Gurman (1977) reported that factor-analytic studies support the underlying dimensions of the BLRI and that the mean internal consistency was high (ranging from .74 - .91) across 14 studies. The Empathy subscale (16 items) was utilized as a measure of client perceived empathy in the current study. The alpha coefficient for the Empathy subscale was .75 for the study sample.
Self-compassion. Counselor trainees were given the 26-item SCS (Neff, 2003) which assesses positive and negative aspects of three components of self-compassion: Self-Kindness (e.g., “I try to be loving towards myself when I’m feeling emotional pain”) versus Self-Judgment (reverse-coded; e.g., “I’m disapproving and judgmental about my own flaws and inadequacies”); Common Humanity (e.g., “I try to see my failings as part of the human condition”) versus Isolation (reverse-coded; e.g., “When I fail at something that’s important to me, I tend to feel alone in my failure”); and Mindfulness (e.g., “When something upsets me I try to keep my emotions in balance”) versus Over-Identification (reverse-coded; e.g., “When something upsets me I get carried away with my feelings”). Responses are given on a 5-point scale ranging from 1 (almost never) to 5 (almost always). Neff and Germer (2012) suggested that the mindfulness subscale of the SCS is distinct from general mindfulness (e.g., FFMQ) in two ways. First, mindfulness as an aspect of self-compassion is narrower, referring to awareness of negative thoughts and feelings associated with personal suffering as opposed to a full range of experience (positive, negative, or neutral) with acceptance and equanimity. Second, mindfulness in self-compassion is more person-focused than experience-focused. Neff (2003) found evidence of adequate construct validity and high internal consistency (Cronbach’s alpha of .92). In the current study, the alpha coefficient for the SCS was .94.
Experiential avoidance. The AAQ-II (Bond et al., 2011) is a seven-item questionnaire used to measure psychological flexibility and experiential avoid-
366 $ Journal o f Mental Health Counseling
Mindfulness, Self-Compassion, and Session Variables
ance. Counselor trainees respond to a 7-point scale ranging from 1 (never true) to 7 (always true) on items such as “I’m afraid of my feelings” and “Worries get in the way of my success”. Bond, et al., (2011) found support for construct validity and high internal consistency (Cronbach’s alpha of .88). In the current study, the alpha coefficient for the AAQ-11 was .82.
Ambiguity tolerance. Counselor trainees were given the 13-item MSTATS (McClain, 2009) which assesses ambiguity tolerance defined as an orientation ranging from aversion to attraction, toward stimuli that are complex, unfamiliar, and unsolvable. Responses are given on a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree) on items such as “1 don’t tolerate ambiguous situations well” and “I would rather avoid solving a problem that must be viewed from several different perspectives”. McClain found support for construct validity and high internal consistency (Cronbach’s alpha of .83). In this study the alpha coefficient was .88.
Demographics. Counselor trainees were queried about age, gender, race/ ethnicity, program track, field experience, meditation practice (and what type), and exposure to mindfulness training in their counseling program (and what type). Counselors also indicated the number of counseling sessions completed at the time of the study. Clients were queried about age, gender, and race/ ethnicity.
RESULTS
Preliminary AnalysesAn a priori sample size (Soper, 2016) was calculated and 55 dyads were
deemed sufficient for a medium effect size of .3 (Cohen, 1988) and power of .80 at the .05 level for F-tests for linear and multiple regressions. Preliminary analysis of the data indicated that there were no outliers and data approximated normal distributions for all instruments. Mean item replacement was used for five items missing across the dataset.
Although the majority of students (70%) were in practicum classes, as a preliminary analysis, the difference in mean scores for session related variables (i.e., client perceived empathy and session depth) between students in the practicum and intermediate methods courses were calculated to assess whether developmental level would predict results. Based on f-tests, no statistically significant differences were found between practicum and intermediate methods students for session related variables, thus students were combined for analyses. However, a non-significant difference between practicum and intermediate methods courses does not necessarily mean they are equivalent (Weigold, Weigold, & Russell, 2013). Additionally, at least three completed sessions were required to participate and the average number of sessions at the data collection point was 6.0 (SD = 2.0; Range = 3-8). There was no significant relationship between client perceived empathy and session number (r = .22, p = .11) possibly reducing the likelihood that more than the three minimum required sessions for participation impacted results for client perceived empathy; however, it is still possible results may have been different with more
0 Journal of Mental Health Counseling 367
sessions. Lastly, there was concordance between client and counselor ratings on se ss io n d e p th (r = .28, p = .04). Further, there was no significant difference in counselor vs. client ratings of session depth (f = .86, d f = 108, p = .39) and the effect size was small (C o h e n ’s d - .17).
Main AnalysesAn alpha level of .05 was used for all main analyses. For research question
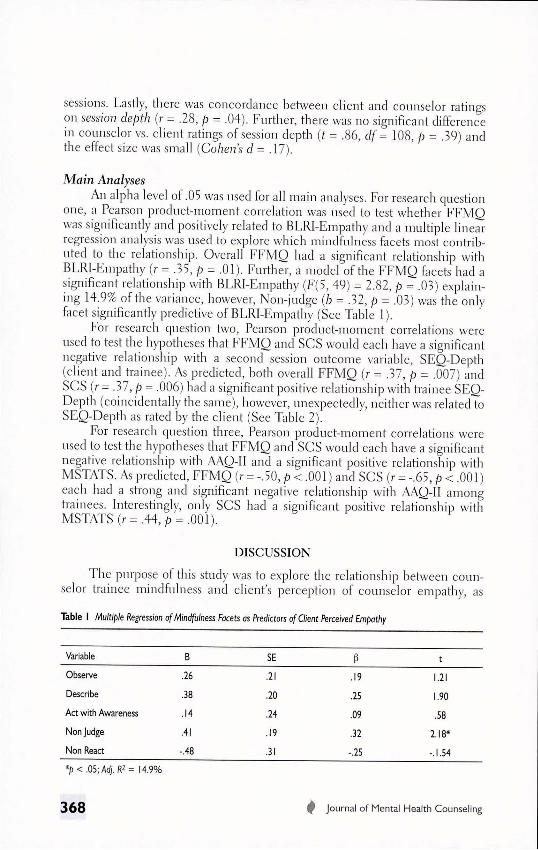
one, a Pearson product-moment correlation was used to test whether FFMO was significantly and positively related to BLRI-Empathy and a multiple linear regression analysis was used to explore which mindfulness facets most contributed to the relationship. Overall FFMQ had a significant relationship with BLRI-Empathy (r = .35, p = .01). Further, a model of the FFMQ facets had a significant relationship with BLRI-Empathy (F(5, 49) = 2.82, p = .03) explaining 14.9% of the variance, however, Non-judge (b = .32, p = .03) was the only facet significantly predictive of BLRI-Empathy (See Table 1).
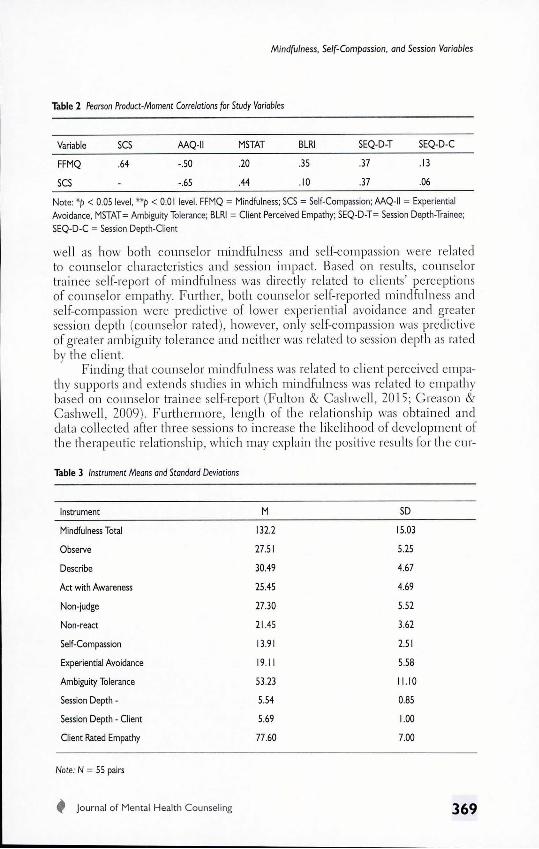
For research question two, Pearson product-moment correlations were used to test the hypotheses that FFMQ and SCS would each have a significant negative relationship with a second session outcome variable, SEQ-Depth (client and trainee). As predicted, both overall FFMQ (r = .37, p = .007) and SCS (r = .37, p = .006) had a significant positive relationship with trainee SEQ- Depth (coincidentally the same), however, unexpectedly, neither was related to SEQ-Depth as rated by the client (See Table 2).
For research question three, Pearson product-moment correlations were used to test the hypotheses that FFMQ and SCS would each have a significant negative relationship with AAQ-II and a significant positive relationship with MSTATS. As predicted, FFMQ (r = -.50, p < .001) and SCS (r = -.65, p < .001) each had a strong and significant negative relationship with AAQ-II among trainees. Interestingly, only SCS had a significant positive relationship with MSTATS (r = .44, p = .001).
DISCUSSION
The purpose of this study was to explore the relationship between counselor trainee mindfulness and client’s perception of counselor empathy, as
Table I M u lt ip le Regression o f M in d fu ln e s s Face ts as P red ic to rs o f C lie n t Perceived E m p a th y
Variable B SE P t
Observe .26 .21 .19 1.21
Describe .38 .20 .25 1.90
Act with Awareness .14 .24 .09 .58
Non Judge .41 .19 .32 2.18*
Non React -.48 .31 -.25 -.1.54
* p < .05; A d j. R2 = 14.9%
368 0 Journal o f M ental Health Counseling
M indfu lness, Self-Com passion, and Session Variables
Table 2 Pearson Product-Moment Correlations for Study Variables
Variable SCS AAQ-II MSTAT BLRI SEQ-D-T SEQ-D-C
FFMQ .64 -.50 .20 .35 .37 .13
SCS - -.65 .44 .10 .37 .06
Note: *p < 0.05 level, **p < 0.01 level. FFMQ = Mindfulness; SCS = Self-Compassion; M Q - ll = Experiential Avoidance, MSTAT= Ambiguity Tolerance; BLRI = Client Perceived Empathy; SEQ-D-T= Session Depth-Trainee;
SEQ-D-C = Session Depth-Client
well as how both counselor mindfulness and self-compassion were related to counselor characteristics and session impact. Based on results, counselor trainee self-report of mindfulness was directly related to clients’ perceptions of counselor empathy. Further, both counselor self-reported mindfulness and self-compassion were predictive of lower experiential avoidance and greater session depth (counselor rated), however, only self-compassion was predictive of greater ambiguity tolerance and neither was related to session depth as rated by the client.
Finding that counselor mindfulness was related to client perceived empathy supports and extends studies in which mindfulness was related to empathy based on counselor trainee self-report (Fulton & Cashwell, 2015; Greason & Cashwell, 2009). Furthermore, length of the relationship was obtained and data collected after three sessions to increase the likelihood of development of the therapeutic relationship, which may explain the positive results for the cur-
Table 3 Instrument Means and Standard Deviations
Instrument M SD
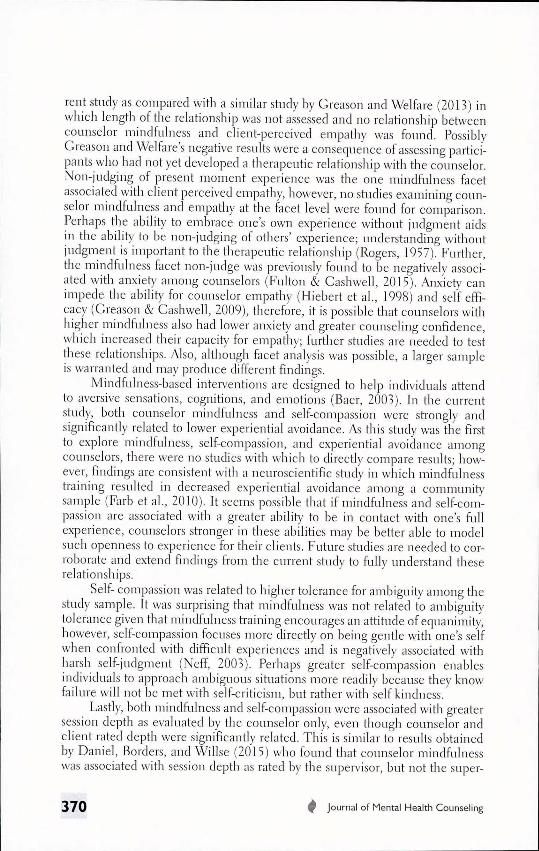
Mindfulness Total 132.2 15.03
Observe 27.51 5.25
Describe 30.49 4.67
Act with Awareness 25.45 4.69
Non-judge 27.30 5.52
Non-react 21.45 3.62
Self-Compassion 13.91 2.51
Experiential Avoidance 19.11 5.58
Ambiguity Tolerance 53.23 11.10
Session Depth - 5.54 0.85
Session Depth - Client 5.69 1.00
Client Rated Empathy 77.60 7.00
Note: N = 55 pairs
^ Journal o f M ental H ea lth Counseling 369
rent study as compared with a similar study by Greason and Welfare (2013) in which length of the relationship was not assessed and no relationship between counselor mindfulness and client-perceived empathy was found. Possibly Greason and Welfare’s negative results were a consequence of assessing participants who had not yet developed a therapeutic relationship with the counselor. Non-judging of present moment experience was the one mindfulness facet associated with client perceived empathy, however, no studies examining counselor mindfulness and empathy at the facet level were found for comparison. Perhaps the ability to embrace one’s own experience without judgment aids in the ability to be non-judging of others’ experience; understanding without judgment is important to the therapeutic relationship (Rogers, 1957). Further, the mindfulness facet non-judge was previously found to be negatively associated with anxiety among counselors (Fulton & Cashwell, 2015). Anxiety can impede the ability for counselor empathy (Hiebert et al., 1998) and self efficacy (Greason & Cashwell, 2009), therefore, it is possible that counselors with higher mindfulness also had lower anxiety and greater counseling confidence, which increased their capacity for empathy; further studies are needed to test these relationships. Also, although facet analysis was possible, a larger sample is warranted and may produce different findings.
Mindfulness-based interventions are designed to help individuals attend to aversive sensations, cognitions, and emotions (Baer, 2003). In the current study, both counselor mindfulness and self-compassion were strongly and significantly related to lower experiential avoidance. As this study was the first to explore mindfulness, self-compassion, and experiential avoidance among counselors, there were no studies with which to directly compare results; however, findings are consistent with a neuroscientific study in which mindfulness training resulted in decreased experiential avoidance among a community sample (Farb et al., 2010). It seems possible that if mindfulness and self-compassion are associated with a greater ability to be in contact with one’s full experience, counselors stronger in these abilities may be better able to model such openness to experience for their clients. Future studies are needed to corroborate and extend findings from the current study to fully understand these relationships.
Self- compassion was related to higher tolerance for ambiguity among the study sample. It was surprising that mindfulness was not related to ambiguity tolerance given that mindfulness training encourages an attitude of equanimity, however, self-compassion focuses more directly on being gentle with one’s self when confronted with difficult experiences and is negatively associated with harsh self-judgment (Neff, 2003). Perhaps greater self-compassion enables individuals to approach ambiguous situations more readily because they know failure will not be met with self-criticism, but rather with self kindness.
Lastly, both mindfulness and self-compassion were associated with greater session depth as evaluated by the couuselor only, even though counselor and client rated depth were significantly related. This is similar to results obtained by Daniel, Borders, and Willse (2015) who found that counselor mindfulness was associated with session depth as rated by the supervisor, but not the super-
370 0 Journal o f Mental Health Counseling

M in d fu ln e s s , S e lf - C o m p a s s io n , a n d S e s s io n V a r ia b le s
visee. It seems both more mindful counselors and supervisors perceive greater session depth than do their clients or supervisees. This may not be surprising because sessions that involve collaborative engagement are associated with higher ratings of depth, particularly by the counselor; although there is also evidence that both counselor and client rated session depth is important to a good counseling hour (Tryon, 1990).
Implications for Counselors, Educators, and SupervisorsMindfulness has been associated with empathy based on client-perceived
empathy in the current study and previously with counselor trainee self-reported empathy (Fulton & Cashwell, 2015; Greason & Cashwell, 2009), development of the therapeutic relationship (Buser et ah, 2012), and positive client outcomes (Grepnrair et ah, 2007). Taken together, there is growing evidence that mindfulness training may be a useful method for developing qualities important to an effective therapeutic relationship, and in turn, positive client outcomes. Further, the mindfulness skill, non-judging present moment experience, was most predictive of client-rated empathy. Activities (e.g., compassion meditations) that enhance a counselor’s ability to maintain a non-judgmental stance toward their own internal experience may be particularly apt for experiencing empathy toward a client. Randomized controlled studies of the effect of mindfulness on non-judging within the counselor, and in turn, within the counseling process, are needed to investigate this possibility.
Self-compassion was strongly associated with greater ambiguity tolerance in the current study and has been associated with many other potential benefits to counselors such as less anxiety and emotional exhaustion (Birnie et ah, 2010). Thus, incorporating self-compassion exercises into training and/ or supervision may be fruitful, particularly given the difficulty students have coping with the ambiguity inherent in counselor training (Levitt & Jacques, 2005). Self-compassion practices may also be useful to counselor trainees as tolerance for ambiguity is important to promoting deep exploration and change during counseling (Bien, 2004). Both mindfulness and self-compassion were strongly negatively associated with experiential avoidance in the current study. Educators and trainees may find mindfulness worth exploring as a way to lower experiential avoidance so that students can better tolerate the feelings and thoughts that arise when confronted with the range of difficult emotions and concerns expressed by clients and during the training process overall.
Mindfulness can be incorporated into counseling training and ongoing development in a number of ways. For example, Hahn (1975) suggested that mindfulness can be practiced informally, such as by taking a moment to focus on the breath or giving any activity one’s full attention, in the present moment without judgment or elaboration. Formal mindfulness practice involves an “activity” used to cultivate mindfulness such as sitting meditation (Baer, 2003). Both formal and informal practices could be incorporated into class or supervision. Educators could also adapt the well-established mindfulness-based stress reduction program (MBSR; Kabat-Zinn, 1990) for use across the curriculum,
0 Journal o f Mental Health Counseling 371
however, additional research is needed to determine the best timing and context for this training (e.g., supervision, class, practicum). MBSR courses are readily available online and in-person so that any practicing counselor could benefit from such training. Lastly, supervisors may encourage mindfulness and self-compassion through modeling and skill-building (e.g., practice observing one’s self without judgment or modeling self-compassion).
Limitations and Future ResearchResults, while promising, need to be considered within the context of
limitations of the study design and sample. Participants were mostly female, European American trainees from a single CACREP-accredited program; results may not generalize to other programs, non-accredited programs, men, or other ethnicities. A larger, more diverse sample is recommended for future studies. Session data were based on trainees’ relationship with one client in one session, limiting the range and variability of client responses. It is possible that session depth may have been atypical, thus, researchers should consider collecting evaluative session data over several sessions. Additionally, all instruments were self-report measures which can be influenced by degree of self-knowledge and social desirability. Lastly, because this study was correlational, causation cannot be determined. Randomized controlled studies designed to measure specific changes as a result of mindfulness training are needed so educators and supervisors can confidently use mindfulness training to improve counselor performance and client outcomes.
In conclusion, despite the study limitations, the current study offers support for the suggestion that both mindfulness and self-compassion are associated with important counselor variables such as client-perceived empathy, affect tolerance, ambiguity tolerance, and session dynamics. Further studies are needed to corroborate these findings and to further explore the role of affect tolerance and tolerance for ambiguity in the counseling process. Ultimately, if mindfulness is to be considered a useful counselor development method, researchers must demonstrate that such training will improve counseling performance and client outcomes.
REFERENCESBaer, R. A. (2003). Mindfulness training as a clinical intervention: A conceptual and empirical
review. Clinical Psychology: Science and Practice, 10, 125-143. doi: 10.1093/clipsy.bpgO 15 Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J.,&Toney, L. (2006). Using self-report assessment
methods to explore facets of mindfulness. Assessment, 13, 27-45. doi: 10.1177/1073191105283504 Barrett-Lennard, G.T. (1981). The empathy cycle: Refinement of a nuclear concept. Journal of
Counseling Psychology, 28, 91-100. doi: 10.1037//0022-0167.28.2.91 Barrett-Lennard, G. T. (1962). Dimensions of therapist response as causal factors in therapeutic
change. Psychological Monographs, 76(43). doi: 10.1037/h0093918 Bien, T. (2004). Quantum change and psychotherapy. Journal o f Clinical Psychology tin Session, 60,
493-501. doi: 10.1002/jclp.20003
372 0 Journal o f Mental Health Counseling

Mindfulness, Self-Compassion, and Session Variables
Birnie, K., Speca, M , & Carlson, L. E. (2010). Exploring self-compassion and empathy in the context of mindfulness-based stress reduction (MBSR). Stress and Health 26, 359-371. doi: 10.1002/smi. 1305
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., . . . Devins, G. (2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice, 11, 230-241. doi: 10.1093/clipsy.bph077
Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K.,...Zettle, R. D. (2011). Preliminary psychometric properties of the Acceptance and Action Questionnaire - II: A revised measure of psychological inflexibility and experiential avoidance. Behavior Therapy, 42, 676-688. doi:10.1016/j.beth.2011.03.007
Borders, L. D., & Brown, L. L. (2005). The new handbook of counseling supervision. New York, NY: Routledge.
Buser, T., Buser, J., Peterson, C. H., & Seraydarian, D. G. (2012). Influence of mindfulness practice on counseling skill development. Journal of Preparation and Supervision, 4, 20-36. doi: 10.7729/41.0019
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Earlbaum Associates.
Daniel, L., Borders, L. D., & Willse, J. (2015). The role of supervisors’ and supervisees’ mindfulness in clinical supervision. Counselor Education & Supervision, 54, 221-232. doi:10.1002/ceas.l2015
Elliott, R., Bohart, A. C., Watson, ]. C., & Greenberg, L. S. (2011). Empathy. Psychotherapy, 48, 43-49. doi:10.1037/a0022187
Farb, N. S., Anderson, A. K., Mayberg, H., Bean, ]., McKeon, D., & Segal, Z. V. (2010). Minding one’s emotions: Mindfulness training alters the neural expression of sadness. Emotion, 10, 25- 33. doi: 10.1037/a0017151
Fulton, P. R. (2005). Mindfulness as clinical training. In C. K. Germer, R. D. Siegel, & P. R. Fulton (Eds.), Mindfulness and psychotherapy (pp. 55-72). New York, NY: Guilford.
Fulton, C. L., & Cashwell, C. S. (2015). Mindfulness-based awareness and compassion: Predictors of counselor empathy and anxiety. Counselor Education & Supervision, 54,122-133. doi: 10.1002/ ceas. 12009
Geller, S. M., Greenberg, L. S., & Watson, J. C. (2010). Therapist and client perceptions of therapeutic presence: The development of a measure. Psychotherapy Research, 20, 599-610. doi:10.1080/10503307.2010.495957
Greason, P. B., & Cashwell, C. S. (2009). Mindfulness and counseling self-efficacy: The mediating role of attention and empathy. Counselor Education and Supervision, 49, 2-18. doi: 10.1002/j. 15 56-6978.2009,tb00083.x
Greason, P. B., & Welfare, L. E. (2013). The impact of mindfulness and meditation practice on client perceptions of common therapeutic factors. Journal of Humanistic Counseling, 52, 235- 253. doi: 10.1002/j.2161-1939.2013.00045.x
Grepmair, L., Mitterlehner, F., Loew, T., Bachler, E., Rother, W., & Nickel, M. (2007). Promoting mindfulness in psychotherapists in training influences the treatment results of their patients: A randomized, double-blind, controlled study. Psychotherapy and Psychosomatics, 76, 332-338. doi: 10.1159/000107560
Gurman, A. S. (1977). The patient’s perception of the therapeutic relationship. In A. S. Gurnman & A. M. Razin (Eds.), Effective psychotherapy: A handbook of research (pp. 503-543). New York, NY: Pergamon.
Hahn, T. N. (1975). Miracle of mindfulness. Boston, MA: Beacon Press.Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Lillis, J. (2006). Acceptance and
commitment therapy: Model, processes, and outcomes. Behavior Research and Therapy, 44, 1-25. doi: 10.1016/j.brat,2005.06.006
Hiebert, B., Uhlemann, M. R., Marshall, A., & Lee, D. Y. (1998). The relationship between selftalk, anxiety, and counseling skill. Canadian Journal of Counseling, 32, 163-171.
Holzel, B. K., Carmody, J., Vangel, M., Congleton, C., Yerramsetti, S. M., Card, T., & Lazar, S. W. (2011). Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Research: Neuroimaging, 191, 36-43. doi:10.1016/j.pscychresns.2010.08.006
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. New York, NY: Delacorte.
0 Journal of Mental Health Counseling 373
Kabat-Zinn, J. (1994). Wherever you go, there you are: mindfulness meditation in everyday life. New York, NY: Hyperion.
Kabat-Zinn, J. (2012). Mindfulness for beginners. Boulder, CO: Sounds True, Inc.Lesh, T. (1970). Zen meditation and development of empathy in counselors. Journal of Humanistic
Psychology, 10, 39-74. doi: 10.1177/00221678700100010 5 Levitt, D. H., & Jacques, J. D. (2005). Promoting tolerance for ambiguity in counselor training
programs. Journal of Humanistic Counseling, Education and Development 44 46-54 doi: 10.1002/J.2164-490x.2005.tb0005 5.x
Lutz, A., Brefczynski-Lewis, J., Johnstone, 1., & Davidson, R. J. (2008). Regulation of the neural circuitry of emotion by compassion meditation: Effects of meditative expertise. PLoS ONE, 3, 1-10. doi: 10.1371/journal.pone.0001897
McClain, D. L. (2009). Evidence of the properties of an ambiguity tolerance measure: The multiple stimulus types ambiguity tolerance scale-II (MSTAT-ll). Psychological Reports 105 975-988. doi: 10.2466/prO.105.3.975-988
Neff, K. D. (2003). The development and validation of a scale to measure self-compassion. Self and Identity, 2, 223-250. doi: 10.1080/15298860309027
Neff, K. D., & Germer, K. G. (2012). A pilot study and randomized controlled trial of die Mindful Self-Compassion program. Journal of Clinical Psychology, 69, 28-44. doi: 10.1002/jclp. 2192 3
Neff, k., & Pommier, E. (2013). The relationship between self-compassion and other-focused concern among college undergraduates, community adults, and practicing meditators. Self and Identity, 12, 160-176. doi: 10.1080/15298868.2011.649546
Reynolds, S., Stiles, W. B„ Barkham, M., Shapiro, D. A., Hardy, G. E., & Rees, A. (1996). Acceleration of changes in session impact during contrasting time-limited psychotherapies. Journal of Consulting and Clinical Psychology, 64, 577-586. doi: 10.1037/0022- 006X.64.3.577
Rogers, C. R. (1957). The necessary and sufficient conditions of therapeutic personality change.Journal of Consulting Psychology, 21, 95-103. doi:10.1037/h0045357
Soper, D. (2016). Free statistics calculators (Version 4.0) [Software]. Available from http://www. danielsoper.com/statcalc3/default.aspx.
Stiles, W. B., & Snow, J. S. (1984). Counseling session impact as viewed by novice counselors and their clients. Journal of Counseling Psychology, 31, 3-12. doi: 10.1037/0022-0167.31.1.3
I rusty, J., Ng, K., & Watts, R. E. (2005). Model of effects of adult attachment on emotional empathy of counseling students. Journal of Counseling 6 Development, 83, 66-77. doi: 10.1002/j. 15 56-6678.2005.tb00581 .x
Tryon, G. S. (1990). Session depth and smoothness in relation to the concept of engagement in counseling. Journal of Counseling Psychology, 37, 248-253. doi: 10.1037/0022-0167.37.3.248
Weigold, A., Weigold, I. K., & Russell, E. ]. (2013). Examination of the equival ence of self-report survey-based papcr-and-pencil and Internet data collection methods. Psychological Methods 18 53-70. doi: 10.1037/a0031607
374 0 Journal o f Mental Health Counseling
Copyright of Journal of Mental Health Counseling is the property of American Mental HealthCounselors Association and its content may not be copied or emailed to multiple sites orposted to a listserv without the copyright holder's express written permission. However, usersmay print, download, or email articles for individual use.